When it comes to the body, many factors can cause low back pain without a person knowing they encounter it. Simple actions like sitting, standing, and walking can be difficult or helpful, depending on the person’s actions. Since low back pain tends to vary from person to person and the possible factors that can cause low back pain make diagnosing a bit difficult. Fortunately, there are available treatments that can help manage low back pain symptoms and can help alleviate its associated symptoms in the body. Today’s article examines the causes and symptoms of low back pain, aqua therapy for low back pain, and how chiropractic care goes hand in hand with aqua therapy. We refer patients to certified providers specializing in musculoskeletal treatments and hydrotherapy to help many individuals with low back pain. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
The Causes Of Low Back Pain
Have you been feeling aches along the sides of your back? Do you feel stiff when hunched over for an extended period? Or does sitting down make the pain go away or worsen? Many of these factors are associated with signs that you could be suffering from low back pain. Low back pain is considered the leading disability causes worldwide, as studies reveal, which can be influenced by many factors that a person is going through. Anyone can risk developing low back pain as it can derive from different sources that overlap many potential issues. Some of the causes associated with low back pain vary depending on how severely the factors affect the individual, which includes:
Muscle and ligament sprain (Overused muscles and ligaments from injuries, poor posture, or lifting heavy objects)
When it comes to the symptoms of low back pain, many individuals will experience pain ranging from a dull ache to a sudden shooting burning pain that travels down the legs. Many individuals often feel pain from one location of the lower half of the body; instead, it is located on the other side, known as referred pain. Low back pain can potentially mean that another issue is affecting the body. Some of the symptoms associated with low back pain include:
Muscle stiffness
Sciatica
Muscle spasms
Limited mobility on the hips and pelvis
Inflammation
Muscle tenderness
All is not lost, as treatments are available to manage low back pain symptoms and alleviate the body’s pain.
Aqua Therapy For Spine Health-Video
Have you been experiencing muscle stiffness in your lower back? Do hip pain and sciatic symptoms cause mobility issues in your legs? Or does it hurt when you are bending down to pick something up? You could be dealing with low back pain associated with chronic symptoms affecting the body, so why not try aqua therapy? The video above demonstrates what aqua therapy does to the body and the exercises used to relieve low back pain. Studies reveal that the therapeutic purposes of water have dated back to ancient Egypt, Greek, and Roman civilization; that helps cleanse the body from ailments. Many physical therapists utilize aqua therapy to enable individuals with low back pain. Aqua therapy engages the waters, buoyancy, resistance, and hydrostatic pressure that helps rehabilitate injuries and maintain health.
Aqua Therapy For Low Back Pain
Many individuals that suffer from low back pain will try to find ways to alleviate the pain. Aqua therapy is one available treatment that doesn’t strain the lower back and has therapeutic properties. Studies reveal that the beneficial properties of aqua therapy allow the body to improve muscle strength and range of motion while reducing muscle fatigue by using water buoyancy to take the pressure off the spine. Since low back pain is a common health issue associated with environmental factors for many individuals, studies reveal that water buoyancy can eliminate the gravitational forces impacting the body weight by counteracting it. To that point, this reduces joint stress on the body to perform the water aerobic exercises with ease. Individuals who incorporate aqua therapy in their health and wellness journey may be more motivated to exercise in the water without worrying about constant pain.
Aqua Therapy Goes Hand In Hand With Chiropractic Care
Like any treatment, chiropractic care and aqua therapy have an excellent relationship as they work together to assess and analyze the individual’s problem and devise a plan for them. Chiropractors utilize spinal manipulation to determine where the pain is located. So when a person is dealing with low back pain due to spinal subluxation or misalignment, a chiropractor can help the individual by loosening the stiff muscles and increasing the range of motion back to the spine. At the same time, aqua therapy incorporates the same benefits associated with land-based physical therapy, including a treatment plan tailored to the individual. Chiropractors and physical therapists work together to determine the best possible action to speed up the recovery process when it comes to a person’s pain, giving them the best chance to get back their quality of life.
Conclusion
Low back pain is one of many individuals’ most common complaints worldwide. The many factors associated with low back pain vary and range from a dull ache to a sharp pain radiating down the legs as part of the symptoms of low back pain. Treatments like aqua therapy can help take the load off the spine through water buoyancy and can help reduce the stress on the joints in the lumbar spine while reducing muscle fatigue. Combined with chiropractic care, many individuals can recover faster from their low back pain and bring back their quality of life without being in so much pain.
References
Abadi, Fariba Hossein, et al. “The Effect of Aquatic Exercise Program on Low-Back Pain Disability in Obese Women.” Journal of Exercise Rehabilitation, Korean Society of Exercise Rehabilitation, 31 Dec. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6944883/.
Allegri, Massimo, et al. “Mechanisms of Low Back Pain: A Guide for Diagnosis and Therapy.” F1000Research, F1000Research, 28 June 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4926733/.
Carayannopoulos, Alexios G, et al. “The Benefits of Combining Water and Land-Based Therapy.” Journal of Exercise Rehabilitation, Korean Society of Exercise Rehabilitation, 26 Feb. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7056478/.
Cole, Andrew, and Bruce Becker. “Water Therapy Exercise Program.” Spine, Spine-Health, 26 Feb. 2010, https://www.spine-health.com/wellness/exercise/water-therapy-exercise-program.
Many people worldwide know that exercising has impressive benefits that help improve the body’s overall wellness. The body has different muscle groups that have a casual relationship with the vital organs inside the body. Organs like the heart, lungs, gut, and bladder correlate with the different muscles through the nerve roots that connect them. When the body suffers from various factors that affect it, it causes referred pain to the body where one pain is at one location but radiates from the other side. Exercising can help the body recover through physical rehabilitation by reducing inflammation and scarring on the muscle tissues. One of the many exercises that helps strengthen the muscles, increase flexibility, and even improve posture is Pilates. Today’s article looks at Pilates, its benefits, and how it can help alleviate back pain. We refer patients to certified providers specializing in musculoskeletal treatments to help many individuals with low back pain issues affecting their bodies. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Pilates?
Have you been feeling sluggish or having low energy throughout the entire day? What about experiencing pain in your lower back? Have you experienced muscle stiffness in certain areas around your body? Many of these symptoms are associated with musculoskeletal issues that correlate with different factors that affect the body; why not try an exercise regime like Pilates? Pilates is a system of exercises that uses a particular machine or body to improve a person’s physical strength and posture while increasing the body’s flexibility and enhancing mental awareness. Joseph Pilates developed Pilates in the early 20th century as an exercise program to help World War I soldiers improve their physical fitness levels. Pilates was used as rehabilitation therapy for injured individuals by incorporating resistance, stretching, and target muscle strengthening. Pilates is now utilized for all individuals with different bodies and fitness levels and can provide tremendous benefits.
What Are The Benefits?
Pilates, like any other form of exercise, has many beneficial properties that help improve a person’s health and wellness. Studies reveal that Pilates helps many individuals, including older adults, by improving their posture by decreasing thoracic flexion while increasing lumbar extension for pain relief. Some of the beneficial properties that Pilates offer to the body include:
Increasing core strength: The deep muscles in the abdomen, back, and pelvic regions become stronger and help stabilize the body more.
Strengthen muscle groups: Pilates helps make the muscles not only strong but also helps stretch them so that they can look long and lean. This makes the individual look toned.
It’s a whole body workout: As many exercises work on specific body parts, Pilates focuses on each muscle part of the body and helps muscle development.
Posture Improvement: Pilates help keep the spine aligned while strengthening the body and core. Over time a person’s posture will improve naturally, making them stand taller, stronger, and even more graceful.
Increases energy: Like all exercises, Pilates will give a person the energy boost they need. This is due to the focused breathing and increased blood circulation that stimulates the muscles and the spine.
Pilates Exercises For Back Pain-Video
Are you looking for a new exercise to tone your muscles? Have you been dealing with pain in your lower back? Do you have muscle weakness in some regions of your body? If you have been experiencing pain-related issues, why not try Pilates? The video above goes through a 10-minute Pilates workout for back pain. Studies reveal that non-specific low back pain is a highly prevalent condition many individuals associate with disability and work absence worldwide. Many environmental factors affect many individuals, causing them to suffer back issues. Pilates can help encourage many individuals to regain their health and wellness by incorporating core strength and stability while improving their posture.
Pilates Alleviate Back Pain
Many people don’t realize that some low back pain symptoms are related to poor posture. Poor posture can lead to associated symptoms of headaches, back pain, improper balance, and pelvic issues. What Pilates does is that it creates body awareness and helps improve the lower back muscles by strengthening them and relaxing the stiff muscles. Studies reveal that incorporating Pilates as physical therapy for individuals suffering from low back pain can help address the mental and physical pain aspects with core strengthening, flexibility, and relaxing the tense muscles. Many individuals should never put off exercising when it comes to back pain. Incorporating an exercise routine can benefit the body and prevent future injuries.
Conclusion
An exercise regime can provide many beneficial results for those looking for ways to be healthy, those suffering from injuries, or those who want to add something else to their workout routine. Pilates is one of those exercises that incorporates resistance, stretching, and muscle targeting as it is a full-body workout. Pilates is used in rehabilitation therapy for injured individuals and can provide tremendous benefits. Pilates can help many individuals with back issues associated with environmental factors like poor posture. Many individuals that utilize Pilates as part of their exercise regime will begin to feel stronger and healthier as their backs will thank them.
References
Baker, Sara. “Pilates Exercise for a Healthy Spine – Spineuniverse.” Spineuniverse, 28 Dec. 2019, https://www.spineuniverse.com/wellness/exercise/pilates-exercise-healthy-spine.
Kuo, Yi-Liang, et al. “Sagittal Spinal Posture after Pilates-Based Exercise in Healthy Older Adults.” Spine, U.S. National Library of Medicine, 1 May 2009, https://pubmed.ncbi.nlm.nih.gov/19404180/.
Sorosky, Susan, et al. “Yoga and Pilates in the Management of Low Back Pain.” Current Reviews in Musculoskeletal Medicine, Humana Press Inc, Mar. 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2684152/.
Yamato, Tiê P, et al. “Pilates for Low Back Pain.” The Cochrane Database of Systematic Reviews, John Wiley & Sons, Ltd, 2 July 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8078578/.
When the weather becomes hot, and everyone begins to plan fun activities to enjoy, one of the many activities that come to mind is hanging out in the pool. Swimming is an excellent way to combat the summer heat, but it can provide much more for the body. For athletes, it provides another form of cardio exercise to improve their quality performance when they are competing. While for individuals looking for an affordable exercise regimeor just some fun activity to do, swimming can become a form of therapy and be beneficial for them if they were previously injured. Today’s article looks at how swimming causes an impact on the musculoskeletal system, its beneficial properties to the heart, and how aqua therapy combined with chiropractic care helps optimize full-body health. We refer patients to certified providers specializing in musculoskeletal treatments and hydrotherapy to help those with musculoskeletal disorders. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Swimming & Its Impact On The Musculoskeletal System
Water exercises or swimming can benefit those looking for different cardio exercises to build muscle endurance or have a clear sense of mind. Swimming is fantastic for all body sizes, and when it is done correctly, it can be highly recognized as a form of rehabilitation and injury recovery known as aquatic therapy. Research studies reveal that aquatic treatments and exercises can significantly reduce pain in individuals that suffer from low back pain while increasing physical function. Some of the impacts that swimming/aquatic therapy provides on the musculoskeletal system include:
Builds muscle strength
Improves endurance
Stabilizes joints
Improves poor posture
Swimming/ hydrotherapy is an excellent low-impact exercise that is easy on the back and spine, especially for individuals suffering from low back pain or spinal misalignments. Studies reveal that the efficacy of aquatic activities helps strengthen the abdominals and legs and stretch the back while managing musculoskeletal issues.
When individuals suffer from back pain associated with chronic issues can become concerning for the vital organs that have a causal relationship with the muscle as they are affected as well. When spinal joints and muscles begin to suffer from abnormal weight increases, the muscles and ligaments become misaligned. Misalignment or subluxation is defined as spinal vertebrates that are out of place and cause pressure on the surrounding nerves exiting the spinal cord. These spinal issues then become a risk of developing musculoskeletal disorders in the body. Unlike many aerobic exercises like running or cycling that may be hard on the spine, swimming has little to no impact on the spinal structures. So when individuals begin to take up swimming, they realize that the water buoyancy helps support their body weight while relieving stress on all joints and decompressing the spine. This gives the individual a greater range of motion, while the water gives off a sense of purification as it helps the body relax. Hence, hydrotherapy helps relax people who suffer from obesity or muscle injuries associated with muscle and joint pain as the water provides gentle resistance while relaxing the muscles to promote longer exercise sessions.
The Benefits Of Swimming For The Heart
Swimming or any form of water aerobics is not only beneficial to the musculoskeletal system but can help improve cardiac function in the heart and even the lungs. Studies reveal that swimming is an effective option for maintaining and enhancing cardiovascular fitness. Some of the benefits swimming provides for the cardiovascular system include:
Lowers blood pressure
Improve circulation
Reduces heart rate
But how does swimming improve cardiovascular function in the body? Individuals submerge themselves underwater; they hold their breath until the air is needed. Being submerged underwater may help lung capacity while gaining control of how a person breathes. Breathing exercises associated with aqua therapy help promote stronger lungs and heart while increasing their capacity for blood and airflow to the heart and lungs. Say, for example, a person is having trouble breathing due to restrictive blood and air flow associated with cardiopulmonary issues, which potentially be involved in experiencing an asthma attack associated with obesity.
The Benefits Of Swimming-Video
Have you wanted to try a different form of cardio exercise? Have you been experiencing a limited range of motion in your arms, shoulders, back, and neck? Do you feel tightness across your chest? The video above gives an overview explanation of the health benefits of swimming. Swimming or aquatic therapy allows the individual experiencing chronic pain issues to do cardio activities without increasing or worsening pain, which is very therapeutic for the body. Many people are either training for an athletic event or finding a leisure activity that will benefit them in the long run. Swimming is considered an important factor in a person’s quality of life as it helps them become motivated to make small changes to better their health. Additionally, regular cardiovascular exercises/activities like swimming benefit pain reduction in a therapeutic sense. When individuals are trying to figure out and determine the proper training or therapy that can help alleviate their specific ailments, their goal is to see how those exercises should be done in a certain amount of time without causing fatigue or increased pain as the primary objective.
Aqua Therapy & Chiropractic Care
When looking for the proper exercise regime or treatment for pain issues, it can be challenging to see what works and doesn’t. For those with musculoskeletal disorders related to chronic issues, aqua therapy and chiropractic care go hand in hand in alleviating pain. Aqua therapy exercises can range from simple routines in shallow waters to high-tech equipment like underwater treadmills for muscle conditioning. Active water therapy exercises that are diverse in relieving musculoskeletal pain should be tailored to the person and the specific conditions that are ailing them.
But how does chiropractic care work hand in hand with aqua therapy? Well, chiropractic care and exercise have a casual relationship when it comes to treating musculoskeletal disorders. Many individuals do suffer from spinal misalignment, which becomes a risk of developing musculoskeletal issues that cause discomfort. Since many individuals associate chiropractic care with back issues, the reality shows that chiropractic care not only helps with back issues but various issues that affect the muscles, joints, and organs related to each other. An example would be an individual with low back problems who cannot do any activities for long periods while triggering gut issues. This is defined as somato-visceral pain where affected muscles associated with internal organs trigger pain. So for a chiropractor to adjust an individual dealing with back pain associated with gut or heart issues can slowly restore the person’s natural alignment by reducing the irritated nerve roots between the vertebrae and strengthening the surrounding muscles and tissues. Afterward, a chiropractor may recommend exercises like aquatic therapy to speed up the rehabilitation process, as studies reveal that physical activities are perceived to have a positive impact on health while being associated with perceived symptom reductions in musculoskeletal and injuries, as well as cardiovascular and blood conditions. Once a chiropractic regimen and exercise routine are in place, injury prevention kicks in, keeping the individual moving pain-free.
Conclusion
Whether it is having fun in the sun or finding a new exercise, swimming is not only for just playing but can be therapeutic for individuals dealing with chronic issues. Any aquatic exercise provides little to no impact on the body as it helps strengthen the musculoskeletal and cardiovascular systems with gentle force. Combined with chiropractic care, many individuals that are dealing with musculoskeletal issues associated with chronic organ issues will begin to become motivated to better themselves in the long run.
References
Ariyoshi, Mamoru, et al. “Efficacy of Aquatic Exercises for Patients with Low-Back Pain.” The Kurume Medical Journal, Kurume University School of Medicine, 11 Aug. 2009, https://www.jstage.jst.go.jp/article/kurumemedj1954/46/2/46_2_91/_article.
Lazar, Jason M, et al. “Swimming and the Heart.” International Journal of Cardiology, U.S. National Library of Medicine, 18 Apr. 2013, https://pubmed.ncbi.nlm.nih.gov/23602872/.
Massey, Heather, et al. “Perceived Impact of Outdoor Swimming on Health: Web-Based Survey.” Interactive Journal of Medical Research, JMIR Publications, 4 Jan. 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8767464/.
Shi, Zhongju, et al. “Aquatic Exercises in the Treatment of Low Back Pain: A Systematic Review of the Literature and Meta-Analysis of Eight Studies.” American Journal of Physical Medicine & Rehabilitation, U.S. National Library of Medicine, Feb. 2018, https://pubmed.ncbi.nlm.nih.gov/28759476/.
Everyone wants to be healthier at some point in their lives. Some individuals train to be athletes and must follow procedures to maintain their health. In comparison, others want to get healthier by eating the right food, exercising for at least 30 minutes to an hour, meditating or doing yoga to relieve stress, and maintaining a healthy weight. However, many environmental factors do affect the human body. They can alter how a person looks, weight, levels of physical activity, and how different foods affect the body’s metabolism. When environmental factors start to take hold of a person’s health, it can trigger unwanted issues that affect not only the muscles in the body but the associated internal organs that help provide the functionality to the body. Today’s article focuses on the musculoskeletal system, how different issues affect the musculoskeletal system and associate with other problems in the body, and various treatments to improve musculoskeletal health. We refer patients to certified providers specializing in musculoskeletal therapies that help those with musculoskeletal disorders. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
The Musculoskeletal System & Its Function
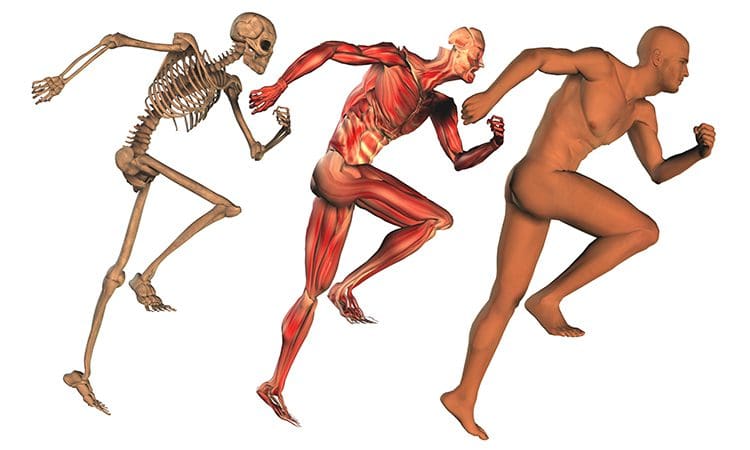
How does the musculoskeletal system play its role in the human body? The body is considered a complex being that consists of various organs, muscles, tissues, ligaments, and joints that help move a person from one place to another, resting while needed, and doing multiple activities in a casual relationship. Studies reveal that the musculoskeletal system is controlled by the central nervous system that interconnects the motor-sensory function for the body’s ability to move and rest.
The three main muscle groups that make up the musculoskeletal system are:
Skeletal muscle- Muscle tendons that are connected to the bones
Cardiac muscle- Muscles associated with the heart
Smooth muscle- Muscles that line with blood vessels and specific organs (ex. intestines)
Each muscle group provides different functions that correlate to how the body moves. Skeletal muscles make the legs and arms move. Cardiac muscles help the heart pump blood to the various muscles, organs, and tissues. Smooth muscles help specific organs (intestines, stomach, and urinary tract) digest, collect nutrients, and eliminate toxins in the body.
Issues That Affect The Musculoskeletal System
These factors are related to different issues that can not only disrupt the musculoskeletal system but can be an overlap of profiles affecting the cardiovascular system, spinal health, and gut system. The different factors that are associated with the musculoskeletal system are:
Obesity
Lack of physical activity
Poor Posture
Inflammation
Unhealthy Diet
How would various factors implicate musculoskeletal issues while triggering different bodily problems? Well, let’s use obesity as an example. Obesity is associated with issues like back and joint pain as studies reveal that these musculoskeletal issues make up pain and disability as a dominant source. A poor diet of processed foods high in fats and sugars can be associated with the risk of developing obesity.
Not only that, but obesity could potentially be involved in the thoracic spine and upper back pain due to the result of physical inactivity and poor dieting. The weight on the body can strain the muscles and ligaments in the back, causing the spinal vertebrae to become misaligned and pressure the nerves exiting the spinal cord. The misalignment of the vertebrae is called a subluxation. When a person is suffering from upper back pain, it can overlap with chest pain, which can be a concerning issue to vital organs like the heart, which potentially involved in the risk of cardiovascular disease. It is related to subluxation that may affect the heart contraction rate, rhythm, and power through the sympathetic efferent pathways originating from the thoracic region.
An Overview Of The Musculoskeletal System-Video
Are you experiencing pain in your upper back or chest? How about cardiac issues associated with shouldering and arming pain? Many of these issues are related to factors that affect the musculoskeletal system that might potentially be involved with chronic issues. The video above summarizes the musculoskeletal system’s role in the body. When environmental factors become a risk of developing musculoskeletal disorders that can potentially be involved in different bodily problems, studies reveal that musculoskeletal disorders associated with abnormal functions may cause a significant impact on regular performances. An example would be a person dealing with bad hip pain and cannot do any exercises triggering heart issues. This is defined as somato-visceral pain where the affected muscle is associated with an internal organ being a pain mediator.
Treatments For Improving Musculoskeletal System
In most treatments, many individuals utilize the following to improve not only the musculoskeletal system but other issues that affect the body:
Exercise
Healthy Diet
Stress Management Treatments
Chiropractic Therapy
No matter what affliction or health problem a person is dealing with, having the best treatment solution possible is a start on a person’s health and wellness journey. The first step is to have a precise diagnosis to the doctor while giving as much information as possible is critical. Providing them with a complete health history is an essential first step. After a manual examination of the issues causing them pain, the primary physician could refer the individual for chiropractic care to relieve issues affecting their musculoskeletal system.
Many people usually only associate chiropractic care with back problems. Still, the reality is that chiropractic therapy can be helpful for the musculoskeletal system and various issues related to the muscles and organs. A chiropractor can provide therapeutic stretches and recommend exercises to individuals to help them avoid the same problems later on. Many chiropractors offer recommendations and nutrition that individuals can utilize to help improve their condition. For the musculoskeletal system, a healthy diet may help achieve and maintain a healthy body weight while reducing the risk of chronic disease. Eating the right amount of healthy greens, fruits, beneficial carbs, and healthy fats can help reduce the risk of developing chronic issues in the body like cardiovascular diseases. However, if primary cardiac problems affect the body, it is best to seek medical attention as soon as possible.
Conclusion
The body is considered a complex being that consists of various organs, muscles, tissues, ligaments, and joints that provide various activities to the host. The musculoskeletal system has three muscle groups: skeletal, cardiac, and smooth muscles provide different functions that correlate to how the body moves. When various factors begin to cause issues to the musculoskeletal system, they can potentially be involved with pain issues that affect more than the body. Treatments like chiropractic care, a healthy diet, exercise, and stress management may be the stepping stones to alleviating various issues that are affecting the musculoskeletal system and a great start in achieving health and wellness.
References
Kennel, Peter J, et al. “Skeletal Muscle Changes in Chronic Cardiac Disease and Failure.” Comprehensive Physiology, U.S. National Library of Medicine, 20 Sept. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6752037/.
Malik, Khalid M, et al. “Musculoskeletal Disorders a Universal Source of Pain and Disability Misunderstood and Mismanaged: A Critical Analysis Based on the U.S. Model of Care.” Anesthesiology and Pain Medicine, Kowsar, 15 Dec. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6348332/.
Murphy, Andrew C, et al. “Structure, Function, and Control of the Human Musculoskeletal Network.” PLoS Biology, Public Library of Science, 18 Jan. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5773011/.
Stochkendahl, Mette J, et al. “Diagnosis and Treatment of Musculoskeletal Chest Pain: Design of a Multi-Purpose Trial.” BMC Musculoskeletal Disorders, BioMed Central, 31 Mar. 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2315652/.
The digestive system in the body helps with the process of digesting food that the host consumes. The food being digested goes through a bio-transformation where it turns into nutrients and is stored in the intestines, liver, and gallbladder, where it turns into bile to be excreted out of the system to ensure a healthy functional gut system and body. But when disruptive factors like poor eating habits or gut issues start to affect the body and gallbladder, this causes many problems that can make an individual miserable. This affects their quality of life since they are dealing with painful issues in their bodies that overlap the primary source risk profiles. Today’s article looks at the gallbladder, how it functions with the body and parasympathetic nervous system, and how referred shoulder pain and gallbladder dysfunction are connected. We refer patients to certified providers specializing in gastroenterology and chiropractic treatments that help those with issues that affect their shoulders and gallbladder. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is The Gallbladder?
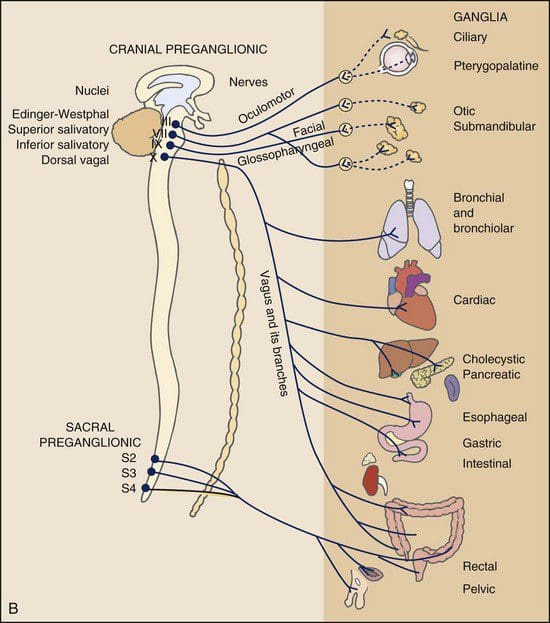
The digestive system comprises the mouth, the internal organs from the GI tract, the liver, the gallbladder, and the anus, where food is consumed, digested, and excreted out of the body to keep it healthy. The gallbladder is a small organ that store and releases bile at the appropriate time into the intestines to be mixed with the digested foods to be excreted out of the body. This pear-shaped organ inflates and deflates like a balloon when it stores and releases bile while having a casual relationship with the nerves and hormones that help regulate the gallbladder functioning properly. Studies reveal that the ganglia become the target of causing the hormone cholecystokinin and the parasympathetic nerve to up or downregulate the neurotransmission to the gallbladder. This causes the gallbladder to be functional in the body.
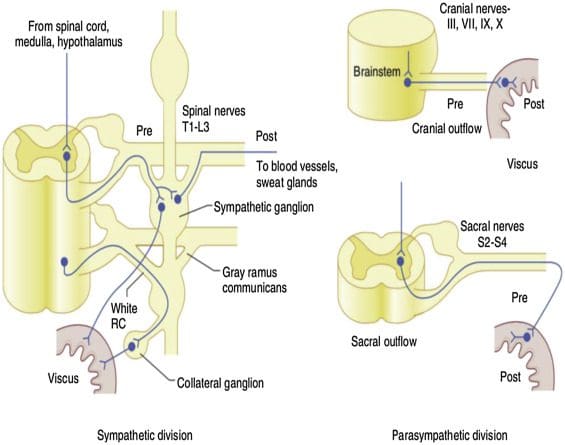
What Are Its Functions In The Parasympathetic Nervous System?
So what are the functions that the gallbladder provides to the body? For starters, the parasympathetic nervous system allows the body to rest and digest the consumed food to be turned into nutrients. The parasympathetic nervous system also provides gallbladder stimulation as studies reveal that the gallbladder receives innervation from the parasympathetic nervous system connected to the vagus nerve that transmits information to the spine and the brain. Keeping and releasing bile from this pear-shaped organ helps regulate the gastrointestinal tract. This causal relationship between the gallbladder and the parasympathetic nerve is essential because the body needs to know when to store and release bile from the gallbladder, or it might trigger some issues that can do more harm to the body and even affect the gallbladder itself.
Do You Have Shoulder Pain?- Video
Have you been experiencing gut issues causing a sharp or dull ache in your back or sides? How about questionable shoulder pain that seems to come out of nowhere? Or are your experiencing inflammation in your digestive system? Many of these symptoms are signs of visceral-somatic pain affecting the gallbladder. Visceral-somatic pain is defined when there is damage to the organ, and it starts to affect the muscles in a different location in the body. The video above gives an excellent example of visceral-somatic pain in the gallbladder and the shoulder. Now many people wonder how shoulder pain is the mediator of the gallbladder? Well, inflammation in the liver and gallbladder causes the nerve roots to be hypersensitive and compressed. This leads to overlapping profiles, triggering pain in the shoulder muscles and associated with upper mid-back pain.
Referred Shoulder Pain & Gallbladder Dysfunction
Now say the individual is experiencing shoulder pain; however, when they rotate their shoulder, there is no pain? Where is the source of shoulder pain localized, and what is causing the issue? And why is it correlating to the gallbladder? This is known as referred pain, where the source of pain is poorly localized when it is located elsewhere. Studies reveal that gallbladder dysfunctions like cholecystitis might be associated with acute thoracolumbar shoulder pain. So what does this mean? It means that any referred pain that is the causation of shoulder pain gives the impression that something is wrong with the gallbladder. This would provide much-needed information when individuals are being examined by their physicians.
Conclusion
The body needs the digestive system to help process food the host consumes and excretes for a healthy functioning system. The gallbladder stores and releases bile to the digested food. This ensures that the nutrients and bile are transported and passed out of the body. When disruptive factors cause gut issues and affect the gallbladder, it can correlate to different problems impacting the body. An example would be gallbladder issues associated with shoulder pain. This is referred to as pain, which is from an affected organ and associated with the muscle in a different location. This can make the individual feel miserable and wonder what is going on with their shoulders when it might be something associated with their gallbladder. Available treatments can provide better knowledge to determine the problem and how to alleviate the issues.
References
Carter, Chris T. “Acute Thoracolumbar Pain Due to Cholecystitis: A Case Study.” Chiropractic & Manual Therapies, BioMed Central, 18 Dec. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4683782/.
Jones, Mark W, et al. “Anatomy, Abdomen and Pelvis, Gallbladder.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 8 Nov. 2021, https://www.ncbi.nlm.nih.gov/books/NBK459288/.
Mawe, Gary M., et al. “Nerves and Hormones Interact to Control Gallbladder Function.” Physiology, 1 Apr. 1998, https://journals.physiology.org/doi/full/10.1152/physiologyonline.1998.13.2.84.
Medical Professional, Cleveland Clinic. “Gallbladder: What Is It, Function, Location & Anatomy.” Cleveland Clinic, 28 July 2021, https://my.clevelandclinic.org/health/body/21690-gallbladder.
Everyone around the world has dealt with pain that makes them feel uncomfortable and has them place their hands on the location where the pain is originating in their bodies. Many factors can become issues in the body, like a poor, unhealthy lifestyle that causes problems in the gut system and develop painful symptoms that affect the intestines. Stressful events that cause headaches that affect the neck and upper back muscles or gut issues that cause discomfort in the abdominal and back region. All these issues are known as referred pain, where a person feels pain in one part of their body, but it is caused by a different source of pain in a different location. An example would be an individual with back pain, but the pain is originating in their abdominal organs. Today’s article looks at various issues that mask low back pain in the body, how organ issues mimic low back pain, and how to alleviate these issues affecting the body. We refer patients to certified providers specializing in gastroenterology and chiropractic treatments that help those with issues that affect their back and gut system. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Different Issues Masking Low Back Pain
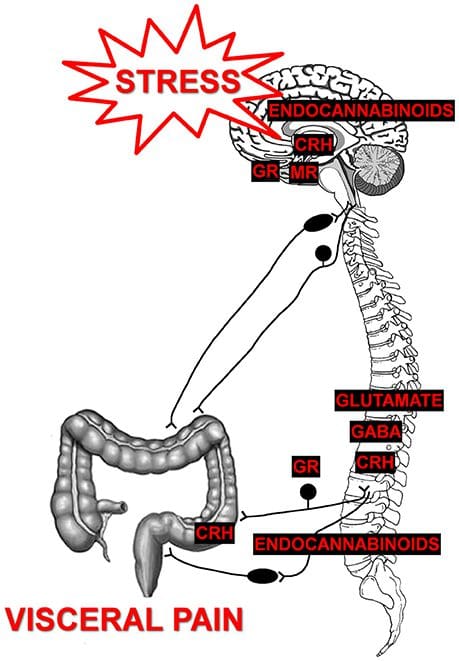
Have you experienced discomfort in your abdominal region causing pain in your lower back? How about pelvic issues that are causing bowel discomfort? Or constipation issues that are compressing the nerves in your lower back? These signs and symptoms correlate to visceral-somatic pain, defined as poorly localized pain characterized by irritated internal organs that cause muscle hypersensitivity from the same nerve. So what does this mean for a person experiencing back issues affecting their quality of life? Well, this might be an indication of the individual that might be suffering from gastrointestinal problems that are correlating to low back pain. Studies reveal any disturbances causing musculoskeletal or gastrointestinal complaints that could induce referred pain through the sympathetic nervous system. An example will be if the body suffers from infections from the kidneys that are associated with low back pain.
So how would the kidneys be associated with low back pain? What is the correlation? For example, a person is constantly eating foods with either a high salt content or a high protein in their system. These high food contents begin to form kidney stones in one or both organs, thus causing a sharp pain that triggers low back pain. As the kidney stones pass through the urinary tract, it administrates radiating pain to the body’s lower abdominal and pelvic region. Another example of issues that can mask low back is constipation in the abdominal area associated with pelvic dysfunction. How does this correlate to the lower back? Think of your abdominal organs overlapped by risk profiles associated with gut disorders. Signs like hypothyroidism, SIBO, celiac disease, or IBS can increase the risk associated with pelvic floor dysfunction, which causes bloating and constipation to the abdominal organs. These issues are co-morbidities to IBS as studies reveal that the pelvic floor and abdominal muscles are co-activated to increase spine stability and intra-abdominal pressure. Now it may seem not a bad thing to the body unless the individual is constantly standing for an extended period or is obese, thus becoming a mediator for the host to suffer from low back pain while being associated with pelvic dysfunction.
Organ Issues Mimicking Low Back Pain- Video
Have you been feeling muscle tenderness in the lower extremities of your body? How about gut issues that are associated with low back pain? Or are you feeling bowel dysfunction in your pelvic region? All these issues correlate to viscerosomatic pain, where the infected organ is causing issues to the muscle in a different location. The video above explains how various organ issues can mimic spinal and back pain in the body. One of the examples that the video explains is how kidney infections are associated with back pain. Studies reveal that visceral pain originating from the upper urinary tract coincidently correlates with the characteristics of referred pain and changes in the somatic tissues of the body.
Alleviating Issues Affecting The Body
Say an individual is suffering from low back pain issues; as they get their mandatory examination, they explain to their physician about their low back pain and what is happening. Once the suffering individual is situated, the physician begins to look over the body where the pain is located, either by physical examination or through the intake form they are looking over. So what does this implicates in the body? Well, studies have revealed that systemic pathologies of the visceral organs can mimic or mask musculoskeletal pain. An example would be someone who is experiencing gastrointestinal issues in their gut, and it’s triggering muscle spasms in the back. This causes the nerve roots to be hypersensitive to the visceral organs and increases the risk associated with low back pain.
Conclusion
Dealing with pain is no joke, primarily when the pain is located in a different body region. Sometimes the pain can be an organ issue that mimics muscle pain in the back. This is known as viscero-somatic pain, defined where infected organs are either mimicking or triggering muscle issues in different body locations. This causation is usually due to various factors like unhealthy lifestyle habits affecting the visceral organs and affecting the muscles that correspond to the organs, like IBS issues affecting the lower back. Available treatments are there to figure out what problems affect the body and provide a better understanding to alleviate them.
References
Basso, Francesca Lo, et al. “Manual Treatment for Kidney Mobility and Symptoms in Women with Nonspecific Low Back Pain and Urinary Infections.” De Gruyter, De Gruyter, 1 May 2021, https://www.degruyter.com/document/doi/10.1515/jom-2020-0288/html.
Bussey, Melanie Dawn, et al. “Is Pelvic Floor Dysfunction Associated with Development of Transient Low Back Pain during Prolonged Standing? A Protocol.” Clinical Medicine Insights. Women’s Health, SAGE Publications, 27 May 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6537301/.
J;, Stowell T;Cioffredi W;Greiner A;Cleland. “Abdominal Differential Diagnosis in a Patient Referred to a Physical Therapy Clinic for Low Back Pain.” The Journal of Orthopaedic and Sports Physical Therapy, U.S. National Library of Medicine, Nov. 2005, https://pubmed.ncbi.nlm.nih.gov/16355918/.
Lacy, Brian E, et al. “Management of Chronic Abdominal Distension and Bloating.” Clinical Gastroenterology and Hepatology : the Official Clinical Practice Journal of the American Gastroenterological Association, 1 Apr. 2020, https://www.cghjournal.org/article/S1542-3565(20)30433-X/fulltext.
PJ;, Pedersen KV;Drewes AM;Frimodt-Møller PC;Osther. “Visceral Pain Originating from the Upper Urinary Tract.” Urological Research, U.S. National Library of Medicine, 16 May 2010, https://pubmed.ncbi.nlm.nih.gov/20473661/.
The spine has three areas: cervical, thoracic, and lumbar in the back, encased with muscles, tissues, ligaments, and joints that help protect the spinal cord from injuries. With the spinal cord being part of the central nervous system, this long cord has many nerve roots that are spread all over the body and help function each section of the body. When the back muscles become damaged or injured in the thoracic region of the spine, it can cause painful symptoms and other issues that correspond with the thoracic spine. Today’s article will look at the thoracic spine, how back pain in the upper-mid section of the back, and how visceral referred pain affects the thoracic region in the body. We refer patients to certified, skilled providers specializing in osteopathic and chiropractic treatments that help those suffering from chest pains and thoracic back pain. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is critical for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
The Thoracic Spine
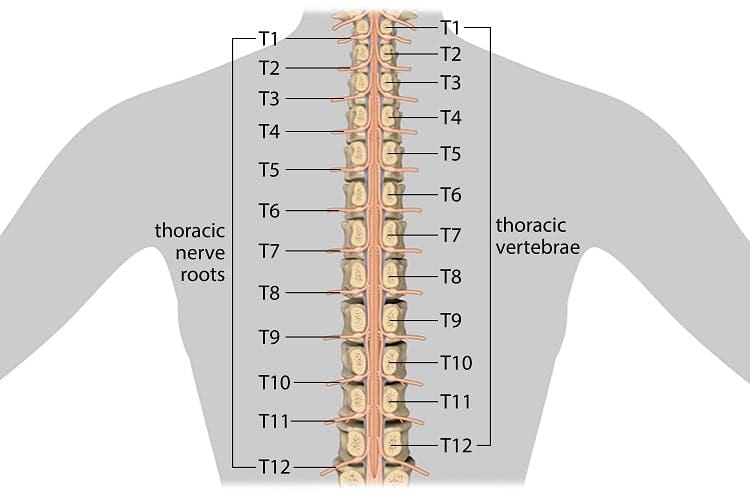
Have you been experiencing herniation in the upper-mid section of your back? Have you felt chest pain occur frequently? Do your back muscles feel stiff or constantly ache even after you stretch? All these symptoms are signs that affect the thoracic region of the spine. Research studies have defined the three spinal areas: the cervical, thoracic, and lumbar help keep the upper half of the body upright. The thoracic area of the spine has added support from the rib cage and allows the body to rotate and flex the upper body. The thoracic region of the spine is also the first curvature that is tight enough to protect the vital organs and loose enough to allow respiratory movement in the body. Additional research studies have also mentioned that the thoracic segments in the spine are susceptible to injuries that can affect the back entirely. The thoracic segments can succumb to structural alterations, disc herniation, and even trauma in the spine from environmental factors like lifting or carrying heavy objects, muscle strain, and forceful impact.
How Thoracic Pain Affect The Body
When the thoracic region of the spine begins to suffer from environmental factors or traumatic events, it can affect the body and aggravate the nerves that encase the spinal column. Research studies have found that when the thoracic spine has succumbed to injuries, it can affect the upper half of the body. Structural changes in the thoracic T 1 through 3 regions of the spine can cause the cervical area to develop neck pain. This causes restricted segmental mobility in the cervical and thoracic regions of the spine. Another research study has mentioned that individuals suffering from thoracic pain will often complain about paravertebral pain aggravated by prolonged standing, hyperextension, and even hyper rotation in the thoracic spinal column. When this happens, it can cause discomfort to the individual and limit their range of motion since their muscles are stiff. Thoracic pain can even affect the corresponding muscles connected to the body’s internal organs.
Referred Pain Affect The Thoracic Spine-Video
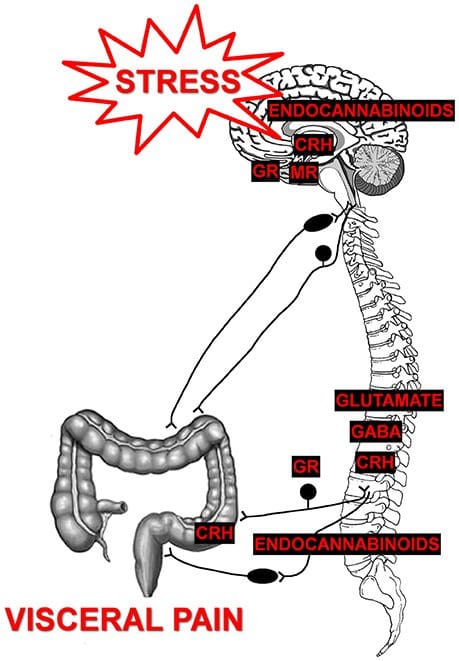
Have you felt muscle stiffness in your upper-middle back? Have you been dealing with neck or chest pain? Have inflammatory issues affecting your esophagus? Many of these are signs and symptoms of visceral referred pain affecting the thoracic region of the spine. The video above explains how visceral referred pain can affect the thoracic spine and the corresponding muscle and organs in the area. Research studies have defined pain as damaged nociceptive sensory nerves that affect the peripheral tissues in the face. The broken nerve roots can affect one portion of the body but also a different section of the body. Additional research studies have also found that visceral pain affecting the thoracic regions of the spine can impact the cardiovascular system. This is due to hypertension caused by chronic stress from environmental factors.
Visceral Referred Pain Affecting The Thoracic Region
Research studies have noticed that thoracic spinal pain can become a common site for inflammation, degenerative discs, and other issues contributing to pain and disability in the spine. Visceral pain is a complex disorder that can cause the surrounding muscles and organs in the thoracic region to be compromised. When the body is suffering from visceral referred pain, the thoracic region of the spine will also begin to suffer. Additional research studies have found that visceral referred pain that affects the thoracic neurons will also affect the esophageal and cardiac input to the cardiovascular and gut systems. When the affected thoracic neurons begin to cause heart and esophageal problems, these two organs become hypersensitive due to noxious stimulation.
Conclusion
The spine has three areas: the cervical, thoracic, and lumbar, which help keep the body upright and is encased with muscles, tissues, and ligaments that protect the spinal cord from injuries. Injuries that affect the thoracic regions of the back can cause problems to the corresponding muscles and the internal organs, especially in the gut and cardiovascular systems. These organs become hyper-sensitive and can make the body develop hypertension and other issues that can make the body dysfunctional. When individuals realize that their upper-middle back pain in the thoracic region can affect their cardiovascular system, they can find ways to treat their back pain and prevent cardiovascular issues from forming.
References
Briggs, Andrew M, et al. “Thoracic Spine Pain in the General Population: Prevalence, Incidence and Associated Factors in Children, Adolescents and Adults. A Systematic Review.” BMC Musculoskeletal Disorders, BioMed Central, 29 June 2009, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2720379/.
Brumovsky, P R, and G F Gebhart. “Visceral Organ Cross-Sensitization – an Integrated Perspective.” Autonomic Neuroscience: Basic & Clinical, U.S. National Library of Medicine, 16 Feb. 2010, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2818077/.
Gkasdaris, Grigorios, et al. “Clinical Anatomy and Significance of the Thoracic Intervertebral Foramen: A Cadaveric Study and Review of the Literature.” Journal of Craniovertebral Junction & Spine, Medknow Publications & Media Pvt Ltd, 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5111324/.
Joshi, Shriya, et al. “Thoracic Posture and Mobility in Mechanical Neck Pain Population: A Review of the Literature.” Asian Spine Journal, Korean Society of Spine Surgery, 3 June 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6773982/.
Murray, Greg M. “Guest Editorial: Referred Pain.” Journal of Applied Oral Science : Revista FOB, Faculdade De Odontologia De Bauru Da Universidade De São Paulo, 2009, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4327510/.
van Kleef , Maarten, et al. “10. Thoracic Pain.” Pain Practice : the Official Journal of World Institute of Pain, U.S. National Library of Medicine, 2010, https://pubmed.ncbi.nlm.nih.gov/20492577/.
Ward, John, et al. “Immediate Effects of Upper Thoracic Spine Manipulation on Hypertensive Individuals.” The Journal of Manual & Manipulative Therapy, Maney Publishing, Feb. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4459143/.
Waxenbaum, Joshua A, et al. “Anatomy, Back, Thoracic Vertebrae – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 12 Aug. 2021, https://www.ncbi.nlm.nih.gov/books/NBK459153/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine