Can incorporating these 7 exercises help individuals dealing with back pain help promote a healthy spine and functionality?
Introduction
Many individuals have dealt with back pain in their body’s upper, middle, and lower portions, which can correlate with other issues in the upper and lower body extremities. This is due to how many environmental factors affect a person’s daily routine. From stressful days that impact a person’s day to physical inactivity or even spinal issues that have developed over time can cause back pain. When individuals decide to make changes in their health and wellness journey to not only reduce back pain but also improve how they present themselves. Many individuals can start with exercises to reduce back pain and help their spinal health by making sure that they are doing it correctly to prevent injuries. Today’s article looks at how spinal issues correlate with back pain and how these seven simple exercises and stretches can help reduce lower back pain and help you have a healthy spine. We talk with certified associated medical providers who provide our patients’ information to assess back pain correlated with their spine. We also inform patients while asking their associated medical provider intricate questions to formulate customized treatment plans to reduce back pain by integrating exercises to help reduce the pain and promote wellness. Dr. Alex Jimenez, D.C., includes this information as an academic service. Disclaimer.
Spinal Issues Correlating To Back Pain
Do you feel stiffness or muscle aches in your back’s upper, middle, or lower areas? Have you noticed that your posture is hunched more than normal when looking at the phone or being on the computer for an extended period? Or does your back ache from lifting a heavy object or sleeping incorrectly? More often than not, these pain-related scenarios are associated with back pain combined with spinal issues. As one of the leading causes of disability, loss of productivity, and more visits to a health clinic, back pain can impact the body and cause individuals to be miserable. (Bang et al., 2021) Back pain can be specific or non-specific and can cause a person’s spine to degenerate through the spinal disc. The spinal disc provides stability, flexibility, and mobility to the spine, which then helps keep the host upright. However, as the body ages, so does the spine, as lower back pain is multifactorial. When the spinal disc degenerates, the spine has a reduced capacity for intrinsic self-repair within the tissues. (Mohd Isa et al., 2022)
At the same time, when many individuals are dealing with low back pain, depending on the severity of the issue, theywill often change their gait mechanics by adapting different strategies to mitigate the loading on the primary muscles associated with the locomotion that protects the pain-producing tissues. (Smith et al., 2022) When that happens, the pain from the lower back muscles can aggravate the spine further and lead to more chronic issues; however, there are ways to reduce the effects of lower back pain and to help keep the spine healthy.
Can Core Exercises Help with Back Pain?-Video
The 7 Exercises To Incorporate For Back Pain
When it comes to making sure that lower back pain can be reduced and to help with keeping a healthy spine, many people often seek out physical therapy to reduce the pain. Since low back pain is costly in a clinical approach, physical therapy is cost-effective, non-invasive, and can help individuals get a kick start in their health journey. Physical therapy involves whole-body movement that emphasizes breathing coordination, reducing pain from the lower back, and helping stabilize the lumbar spine to improve physical function. (Li et al., 2023) By going through a treatment plan that incorporates physical therapy, many individuals will begin to notice their pain is improving and their quality of life is getting better. (Fischer et al., 2021) Additionally, stretching and core stability exercises can activate the deep and superficial spinal muscles by strengthening them and help stretch out sore muscles affected by low back pain to help many individuals recover. (Calatayud et al., 2019) Below are seven exercises that can help reduce back pain and, when done correctly and consecutively, can help many individuals have a healthier spine while being more mindful of their bodies.
Knee-To-Chest Exercise
This knee-to-chest exercise can help stretch the lower back muscles and can be done in the morning or evening.
Lying on your back with knees bent and feet flat for stability.
Pull one knee up with both hands and press it towards your chest.
Keep the stomach muscles tight while pressing your spine to the floor, holding for at least 30 seconds before returning to position.
Repeat with the other knee and do each stretch 2-3 times.
Lower Back Rotational Stretch (On the Floor)
This lower back rotational stretch can help stretch tight muscles in the lower back.
Laying on the mat, ensure you are on your back with knees bent and feet flat.
Make sure the shoulders are firmly on the floor, and slowly roll the knees to one side until 45 degrees.
Hold that position for 30 seconds before slowly rotating the knees back to the starting position.
Repeat on the other side and do each stretch 2-3 times.
Lower Back Flexibility Exercise
This lower back flexibility will help stretch and strengthen the lower back and core muscles.
Lay flat on the mat. For stability, make sure that the knees are bent with feet are flat on the floor.
Tighten the stomach muscles so the lower back can be pulled away from the floor.
Hold the position for 5 seconds and relax, slowly lowering to the floor.
Flatten the back as your belly button starts to go towards the floor, and hold the position for 5 seconds before relaxing.
Do five repetitions a day to slowly work up to 30 reps.
Bridge Exercise
The bridge exercise can help with core stability and help strengthen core muscles.
Laying flat on your back on the floor, with knees bent and feet flat. Make sure that your shoulders and head are relaxed.
Tighten the core and glute muscles while slowly raising from the hips to form a straight line from the knees to the shoulders.
Stay in that position for 30 seconds while taking deep breaths.
Slowly go down to the floor and relax.
Do five repetitions a day to slowly work up to 30 reps.
Cat-To-Cow Stretch
The cat-to-cow stretch helps with shoulders, upper back, and lower back muscles.
On your hands and knees, hip-width apart on the mat, be in a neutral spine position.
Slowly arch your back by pulling your belly towards the ceiling and your head down for 30 seconds.
Then, slowly let the back and belly sag towards the floor as the head rises for 30 seconds.
Return to the neutral spine position and repeat about 3-5 times twice daily.
Lower Back Rotational Stretch (Seated)
This lower back rotational stretch is seated if the floor is uncomfortable for individuals with severe back pain.
Sitting in an armless chair or stool in a seated upright position, cross one leg over the other.
Then, place the left elbow against the outside of the right knee and twist and stretch the side.
Hold the postion for 10 seconds before slowly returning to a seated position.
Repeat the stretch on the opposite side.
Do this stretch 3-5 times on each side to stretch tight back muscles about twice daily.
Shoulder Blade Squeeze
This shoulder blade squeeze helps individuals properly posture while stretching and strengthening tight upper back and shoulder muscles.
Start in a seated upright position on an armless chair or stool.
Slowly pull the shoulder blades together in the upright position and hold for 5-30 seconds.
Relax, return to the upright position, and repeat 3-5 times twice daily.
References
Bang, A. A., Bhojraj, S. Y., & Bang, A. T. (2021). Back pain and musculoskeletal pain as public health problems: Rural communities await solution. J Glob Health, 11, 01007. https://doi.org/10.7189/jogh.11.01007
Calatayud, J., Escriche-Escuder, A., Cruz-Montecinos, C., Andersen, L. L., Perez-Alenda, S., Aiguade, R., & Casana, J. (2019). Tolerability and Muscle Activity of Core Muscle Exercises in Chronic Low-back Pain. Int J Environ Res Public Health, 16(19). https://doi.org/10.3390/ijerph16193509
Fischer, S. C., Calley, D. Q., & Hollman, J. H. (2021). Effect of an Exercise Program That Includes Deadlifts on Low Back Pain. J Sport Rehabil, 30(4), 672-675. https://doi.org/10.1123/jsr.2020-0324
Li, Y., Yan, L., Hou, L., Zhang, X., Zhao, H., Yan, C., Li, X., Li, Y., Chen, X., & Ding, X. (2023). Exercise intervention for patients with chronic low back pain: a systematic review and network meta-analysis. Front Public Health, 11, 1155225. https://doi.org/10.3389/fpubh.2023.1155225
Mohd Isa, I. L., Teoh, S. L., Mohd Nor, N. H., & Mokhtar, S. A. (2022). Discogenic Low Back Pain: Anatomy, Pathophysiology and Treatments of Intervertebral Disc Degeneration. Int J Mol Sci, 24(1). https://doi.org/10.3390/ijms24010208
Smith, J. A., Stabbert, H., Bagwell, J. J., Teng, H. L., Wade, V., & Lee, S. P. (2022). Do people with low back pain walk differently? A systematic review and meta-analysis. J Sport Health Sci, 11(4), 450-465. https://doi.org/10.1016/j.jshs.2022.02.001
Individuals who have experienced spinal or back trauma, suffered fractures, are going through spinal degeneration, or are dealing with a spinal condition have an increased risk of anterolisthesis, where a vertebra slips forward relative to the vertebra below it. Can healthcare providers help prevent and treat the condition?
Anterolisthesis
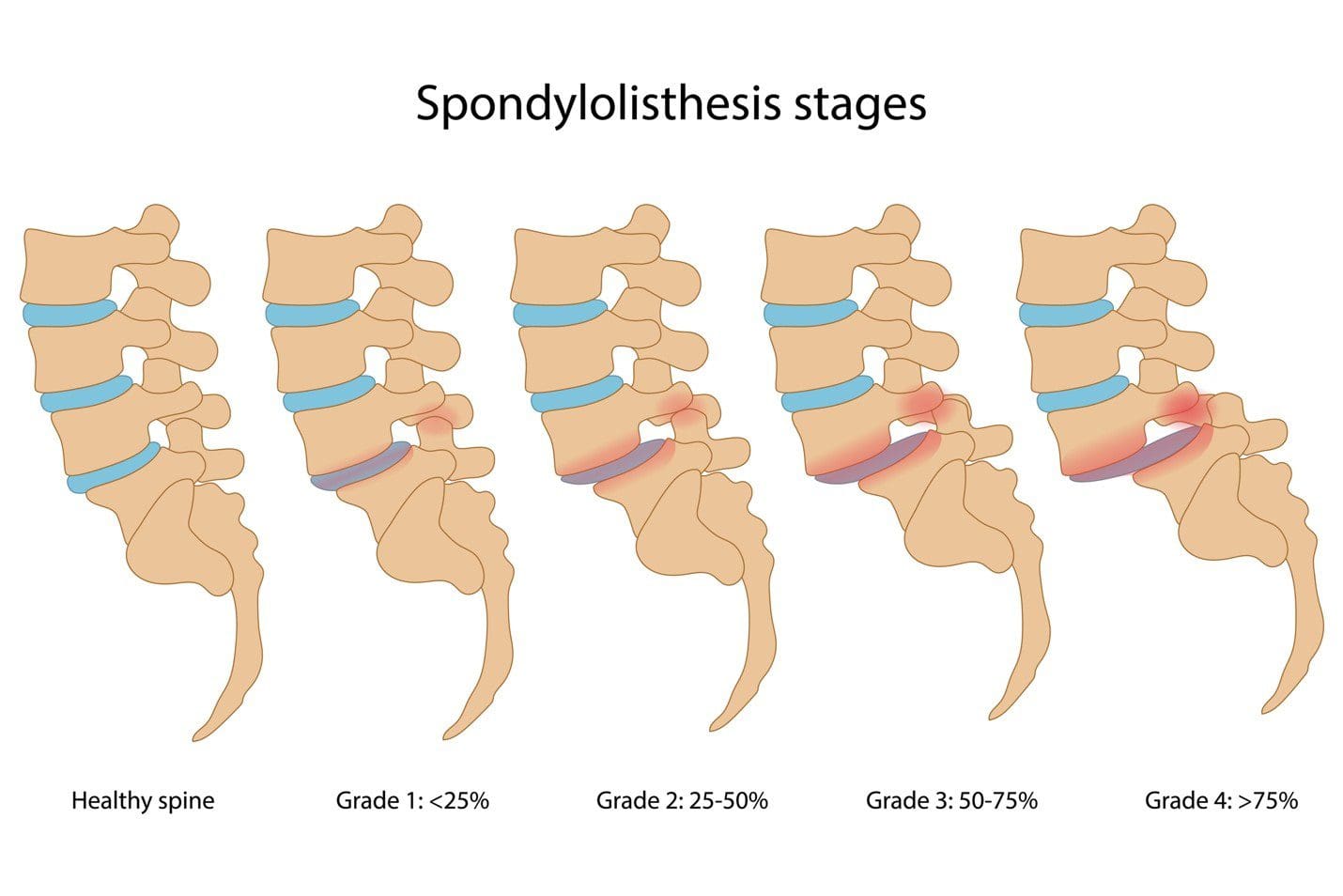
The spine consists of 33 individual bones or vertebrae stacked on one another. Anterolisthesis occurs when one vertebral segment slips forward over another. The condition can be mild, asymptomatic, or cause significant pain and neurological symptoms. Many different things, including osteoarthritis, osteoporosis, trauma, or a fracture, can cause this vertebral shifting. (Cedars Sinai, 2022) Spondylolisthesis is a general term for shifting a spinal vertebra over the one below it. It includes anterolisthesis, forward moving, and the less common retrolisthesis, or backward shifting.
Grades
Anterolisthesis is typically graded using the Meyerding scale, which assigns one of five grades according to how much slippage has occurred. These grades include:
Anterolisthesis can lead to various symptoms, depending on the severity and if the surrounding spinal nerves have been affected. The most common complaints include:
Diagnosis begins with a subjective evaluation and a physical examination. During these, the healthcare provider will assess sensation, strength, and reflexes and will order one of several diagnostic tests, including:
X-rays
Visualizes the vertebrae in the spine and their position relative to those above and below.
Also provides a clear picture of spinal arthritis or disc degeneration.
Magnetic Resonance Imaging – MRI
Allows the spinal cord, nerves, muscles, and discs to be assessed for compression or damage.
Several factors determine how the condition is treated, including:
The grade of the slippage.
The cause.
The symptoms.
The presence of instability on a diagnostic test such as an X-ray.
Stable and mildly symptomatic cases are usually treated with a combination that can involve:
Physical therapy
Activity modification
Bracing
Nonsteroidal anti-inflammatory medications/NSAIDs like ibuprofen.
Spinal injections
In more severe cases in which spinal instability or significant neurological symptoms are present, surgery may be recommended. This commonly involves a spinal decompression or fusion procedure. The technique varies based on the surgeon’s preferences and anatomy. (Koslosky E., and Gendelberg D. 2020)
Prognosis
Most individuals with this condition don’t know they have it until it is found accidentally on an X-ray or an MRI for something else. Mild cases can cause minimal symptoms and can be well-managed with conservative treatments. Cases of unstable anterolisthesis or those with neurological compression often require surgical intervention. These surgeries restore stability to the spine and alleviate any pressure on the nerves. More than 85% of individuals who need surgery have a successful outcome. (American Academy of Orthopaedic Surgeons, 2021)
Self-Care and Management
For individuals experiencing pain, numbness, or tingling from anterolisthesis, getting symptoms evaluated by a healthcare provider is an important first step. The healthcare provider may suggest one of several management strategies, which include:
Core Strengthening
To alleviate symptoms, exercises targeting the core muscles in the hips, pelvis, abdomen, and lower back are recommended.
Formal physical therapy may also be recommended.
Over-the-counter Meds
A healthcare provider may suggest pain-relieving medications like ibuprofen or naproxen to reduce soreness.
Activity Modification
Sticking to gentle, pain-free activities and avoiding excessive or repetitive extension of the spine can help prevent symptom aggravation. (American Academy of Orthopaedic Surgeons, 2021)
Injury Medical Chiropractic and Functional Medicine Clinic
At Injury Medical Chiropractic and Functional Medicine Clinic, our areas of practice include Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Wellness & Nutrition, Functional Medicine Treatments, and in-scope care protocols. We focus on what works for you to relieve pain and restore function. If other treatment is needed, individuals will be referred to a clinic or physician best suited to their injury, condition, and/or ailment.
Koslosky, E., & Gendelberg, D. (2020). Classification in Brief: The Meyerding Classification System of Spondylolisthesis. Clinical orthopaedics and related research, 478(5), 1125–1130. https://doi.org/10.1097/CORR.0000000000001153
American Academy of Orthopaedic Surgeons. (2021). Adult spondylolisthesis in the low back. https://orthoinfo.aaos.org/en/diseases–conditions/adult-spondylolisthesis-in-the-low-back
Hospital for Special Surgery. (2023). Spondylolisthesis. https://www.hss.edu/condition-list_spondylolisthesis.asp
Can knowing the characteristics of each stage of healing help expedite recovery for individuals who are healing after neck and back injuries?
Back or Neck Injury Healing Stages
At each stage, different things happen at the injury site. This means recommended exercises and activity levels will vary depending on how long it’s been since the injury. The stages to know about when healing from a neck or back injury. (Brumitt J., and Cuddeford T. 2015)
Inflammation or Acute Stage
Also known as the inflammatory stage, the acute stage occurs during the injury and can continue for 72 hours. The body releases repair chemicals in response to tissue damage, causing inflammation and pain. Symptoms of inflammation, including redness, swelling, pain at rest, and diminished function, are expected. Inflammation and pain during the inflammation stage are caused by the body’s repair chemicals released in response to tissue damage. (Wu, Y. S. and Chen S. N. 2014) The biological reaction decreases mobility so the injured area can rest and heal, but the substances that promote healing also cause pain and swelling. (Shah A. and Amini-Nik S. 2017) Scar tissue also begins to form during the inflammatory stage. (Wilgus T. A. 2020) Initial treatment focuses on reducing pain, swelling, and muscle spasms. Individuals are encouraged to use ice packs, compression, and over-the-counter anti-inflammatory medications like ibuprofen or naproxen. (Duchesne E., Dufresne S. S., and Dumont N. A. 2017)
Subacute Stage
Inflammation decreases, and new connective tissue and capillaries grow to help repair damaged structures. The subacute phase generates new connective tissue and capillary growth and reduced inflammation. (Brumitt J., and Cuddeford T. 2015) Scar tissue continues to grow during this time, as well. The tissues are still fragile at this stage, stressing the injured area should be limited to when the therapist or doctor is examining or working with the patient. Most physical therapists recommend beginning with gentle movement during the subacute phase and gradually building up the intensity of exercise. Mild isometric and low-intensity exercises are often used. Because activity is restricted, the muscles may seem weak. Depending on the severity of the injury and the type of tissue that was injured (i.e., tendons have less blood circulation and tend to heal more slowly, it can take a few days to several weeks. (Brumitt J., and Cuddeford T. 2015)
The Chronic Stage or Maturation
The inflammation disappears entirely during the chronic or maturation stage of neck or back injury healing. The new collagen fibers build strength, and the wound shrinks. (Brumitt J., and Cuddeford T. 2015) During this stage, pain associated with the injury tends to be limited to the end joint’s range of motion. The first ten weeks of the chronic stage are essential for engaging in exercises that enhance healing and help remodel the fibers so they will function as close as possible to the way they did before the injury. (Azevedo P. S. et al., 2016) Exercises during the ten weeks are important because otherwise, individuals can permanently lose some of their ability to move and function.
After around ten weeks, the scar tissue can permanently change, so re-acquiring strength and flexibility may necessitate surgery or manual release treatment from a physical therapist or chiropractor. During this time, the scar tissue can be remodeled with exercise, meaning that the activities and motions performed on the injured area will affect the formation of new tissue fibers. The chronic stage of healing begins after 21 days and doesn’t end after the 10-week prime time (Brumitt J., and Cuddeford T. 2015). It can continue for quite some time.
Treatment
Treatment focuses on engaging the injured muscles in light isometric contractions to help align new collagen fibers. Physical therapy helps rebuild mobility, strength, balance, and flexibility and can also help learn about injury and how to recover. A treatment that may also help during these phases is massage therapy. Extended bed rest or immobility can prolong symptoms and delay recovery. Tips to manage pain and recovery:
When sitting for long periods, get up and move around frequently.
Wear comfortable shoes.
When driving long distances, stop frequently to stand up and walk around.
Sleep on the side with a small pillow between the knees.
Limit how much weight is carried.
Add exercises gradually.
Most symptoms of back strain or sprain improve in about two weeks. Individuals may need additional treatment if symptoms continue for longer than two weeks. Maintaining exercises will continue to make the body stronger, more flexible, more functional, and pain-free.
Chiropractic Care for Healing After Trauma
References
Brumitt, J., & Cuddeford, T. (2015). CURRENT CONCEPTS OF MUSCLE AND TENDON ADAPTATION TO STRENGTH AND CONDITIONING. International journal of sports physical therapy, 10(6), 748–759.
Wu, Y. S., & Chen, S. N. (2014). Apoptotic cell: linkage of inflammation and wound healing. Frontiers in pharmacology, 5, 1. https://doi.org/10.3389/fphar.2014.00001
Shah, A., & Amini-Nik, S. (2017). The Role of Phytochemicals in the Inflammatory Phase of Wound Healing. International journal of molecular sciences, 18(5), 1068. https://doi.org/10.3390/ijms18051068
Wilgus T. A. (2020). Inflammation as an orchestrator of cutaneous scar formation: a review of the literature. Plastic and aesthetic research, 7, 54. https://doi.org/10.20517/2347-9264.2020.150
Duchesne, E., Dufresne, S. S., & Dumont, N. A. (2017). Impact of Inflammation and Anti-inflammatory Modalities on Skeletal Muscle Healing: From Fundamental Research to the Clinic. Physical therapy, 97(8), 807–817. https://doi.org/10.1093/ptj/pzx056
Azevedo, P. S., Polegato, B. F., Minicucci, M. F., Paiva, S. A., & Zornoff, L. A. (2016). Cardiac Remodeling: Concepts, Clinical Impact, Pathophysiological Mechanisms and Pharmacologic Treatment. Arquivos brasileiros de cardiologia, 106(1), 62–69. https://doi.org/10.5935/abc.20160005
It can be challenging for individuals trying to keep their homes clean with chronic back pain. Can learning and proper body mechanics help manage household responsibilities without aggravating pain symptoms?
Household Chores
Household-related back problems usually occur because we don’t take the time to consider how to move and perform the tasks from a musculoskeletal perspective to avoid and prevent injuries. Most ergonomic tips for household chores revolve around the same ideas for athletes and fitness enthusiasts: maintain a neutral spine, avoid twisting when possible, strengthen the body’s core, take regular breaks, stretch, and don’t overdo it. A healthy body mechanics system works for those who garden as well. Using strategies like cleaning a little here and there instead of taking an entire day whenever possible and organizing tools ahead of time along with training oneself how to perform them in a way that the spine, back muscles, and the entire body are protected from injury, pain, sciatica, or re-injury. However, implementing proper body mechanics requires a willingness to become aware of how each task is performed and to retrain the body where necessary to a healthier method/technique and a happier household.
Vacuuming
Vacuuming is one of those chores that can quickly lead to a habitual bent-over posture. This is not recommended for the spine’s health; slouching, whether from a position held for a sustained period of time or an activity that requires repetition, can lead to problems with the intervertebral discs and pain symptoms. (Nazari J., Pope M. H., and Graveling R. A. 2012) Another posture that individuals tend to engage in is vacuuming with an overly straight back. Like slouching, keeping the spine rigidly over-extended while vacuuming can irritate the spine and cause muscle spasms. It can also increase the normal low back curve, which, in turn, may lead to extra tightness and a painful back.
Vacuuming with healthy body mechanics includes employing a minimal lunge that stays in a pain-free position that does not extend beyond the comfortable position. Individuals should place one foot in front of the other for a short distance. The stance is similar to the way fencers position themselves. This allows a shift forward and back during the vacuuming process instead of bending or rounding over at the spine. For those with sacroiliac joint issues, the forward placement of one leg may be more comfortable than the forward placement of the other. Try out and use the side that feels comfortable, and stick with that. Do not work in pain or through the pain. Switching legs and/or arms can help avoid muscle fatigue or injury triggers. Place the non-vacuuming hand on the thigh in front to help take the weight and pressure off the back. Maintain the pelvis in a level position when working. Another strategy for those who can get up and down from the floor without trouble is to vacuum while kneeling on one knee. This brings the body’s center of mass closer to the floor, reducing the degree to which the body has to deal with the force of gravity. Kneeling while vacuuming may also help prevent rounding over at the spine.
Dusting
When dusting, reduce the load off the back by propping the inactive arm on the item or area being cleaned. Alternatively, prop the arm on the thigh.
Laundry
In a large household, it is very easy to overdo laundry and trying to finish up as much as possible can lead to pain symptoms and injuries. If possible, break up the loads that have to be lifted or carried into smaller bundles that weigh less. This can mean more loads, but the strategy protects the back and spine. Avoid extremes in the spinal position; don’t round over at the spine or keep it rigid and over-extended. Lift with the legs and protect the discs. Adjustments that can be made to the basic lift with the leg and not the back strategy include putting the laundry basket on a table or chair that is preferably the same height as the washer or dryer. This will minimize bending. To relieve pressure on the back, use one hand to load the washer, dryer, or laundry basket while using one of the appliances to prop the other hand.
Dishes
During dishwashing, use a small step stool or box to help prevent injury and/or relieve pain. Place it in the cabinet under the sink and rest one foot on it. This strategy can work well for those with sacroiliac joint problems, especially if the foot on the pain-free side is the one placed on the box or stool. Ensuring foot placement reduces pain and discomfort and does not cause pain. Using a box or stool can also help with core stability. Core stability is one of the best ways, in general, to prevent injury and keep low back pain away. (Coulombe B. J., Games K. E., Neil E. R., and Eberman L. E. 2017) As the box is directly under the sink, the body has to firmly position itself against the counter, providing stability during the task. The box or stool will contract the pelvic and hip muscles and strengthen the core.
Sweeping
Many sweep, mop, and rake with their spines, which can be counterproductive to health, as twisting and bending simultaneously is a known risk factor for a herniated disc. (Shimia, M. et al., 2013) Use the arms and legs instead of overly involving the back during sweeping and raking. The idea is to reach and pull the broom or sweeper with the arms rather than twisting around to reach all the areas working with one leg in front of the other. When needing to change directions, pivot on the back leg, keeping the trunk relaxed, equivalent to a tai chi movement. Or, turn the whole body in different directions by taking small steps. Taking small steps or pivoting on the back leg to change the direction of the trunk and arms protects from overuse and extensive wear and tear.
Adjustments for a new method of household sweeping and raking include:
Sweeping or raking about 1 to 2 feet in front to avoid overreaching and strain.
Maintaining the spine in one long, flexible, but unbroken line.
The head, shoulders, rib cage, pelvis, knees, and feet should always face the same direction and be vertically balanced relative to one another.
This will mean changing directions by pivoting the back leg or moving the whole body around, taking small steps.
Consider using an ergonomically designed broom, sweeper, mop, rake, and other household tools. This will be a bend in the handle or stem to help avoid bending.
Injury Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop personalized treatment programs. We focus on what works for you and use an integrated approach to treating injuries and chronic pain syndromes to improve flexibility, mobility, and agility, relieve pain, and help individuals return to normal activities. Our providers use Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles. Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers if other treatments are needed.
Heel Spurs
References
Nazari, J., Pope, M. H., & Graveling, R. A. (2012). Reality about migration of the nucleus pulposus within the intervertebral disc with changing postures. Clinical biomechanics (Bristol, Avon), 27(3), 213–217. https://doi.org/10.1016/j.clinbiomech.2011.09.011
Coulombe, B. J., Games, K. E., Neil, E. R., & Eberman, L. E. (2017). Core Stability Exercise Versus General Exercise for Chronic Low Back Pain. Journal of athletic training, 52(1), 71–72. https://doi.org/10.4085/1062-6050-51.11.16
Shimia, M., Babaei-Ghazani, A., Sadat, B. E., Habibi, B., & Habibzadeh, A. (2013). Risk factors of recurrent lumbar disk herniation. Asian journal of neurosurgery, 8(2), 93–96. https://doi.org/10.4103/1793-5482.116384
An annular fissure is caused by age-related changes to the spine, which often do not cause symptoms but can cause back pain. Can understanding the causes help individuals manage lower back pain and help healthcare providers develop an effective treatment program?
Annular Fissure
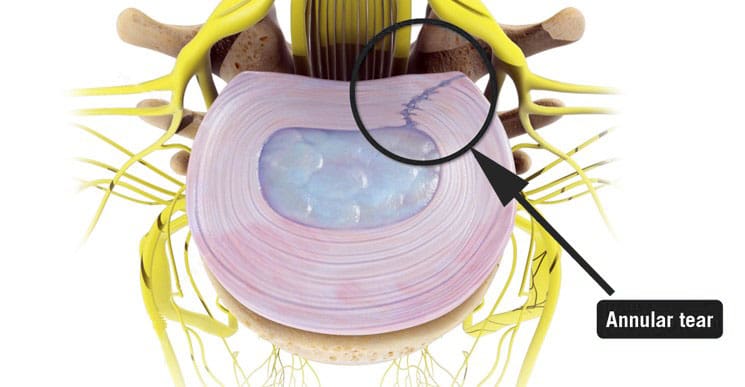
An annular fissure is a discogenic condition that affects the spine and can cause lower back pain. Also called an annular tear, it’s usually a wear-and-tear condition that happens over time rather than a condition caused by trauma. It usually happens when the fibers that make up the annulus or the tough outer covering of the intervertebral disc break or separate. To manage it, healthcare providers may recommend:
Making lifestyle changes.
Staying aware of how you go about daily activities and take steps to make adjustments, such as being mindful of unhealthy posture.
Start doing exercises that help make the back stronger.
Medical care if pain and other symptoms need to be managed.
Symptoms
Lower back pain may be a sign of an annular fissure, or there may be no symptoms. Symptoms can include:
Pain
Weakness
Numbness
Electrical sensations travel down one leg or arm if a cervical/neck tear is present.
Numbness and weakness may be caused by the nerves getting irritated or compressed near an annular tear. (Stadnik, T. W. et al., 1998)
These symptoms can also be similar to a herniated disc, which can be a complication of an annular fissure.
However, studies have shown that annular tears and herniated discs often go unnoticed because they have few obvious symptoms. (Jarvik, J. G. et al., 2005)
Annulus Function
The annulus comprises several layers of tough fibers/fibrocartilage that surround, contain, and protect the soft, liquid nucleus inside the disc. The layers of the annulus fibrosus crisscross to provide support. The nucleus is a shock absorber cushions the body’s weight on the spinal joints when sitting, standing, or moving. Its strength also allows the disc to buffer the jolts and jars it experiences. It also helps maintain the integrity of the intervertebral joint by supporting the space between the two vertebrae. When an annular fissure occurs, the fibers separate or tear off from insertion on the nearby spinal bone. A fissure can also be a break in the fibers of one or more layers. (Jarvik, J. G. et al., 2005)
Causes
An annular tear is not the standard term medical professionals use to describe or diagnose a fissure because the word tear suggests that trauma has led to the separation or break in the fibers. While an injury can cause an annular fissure, it’s usually caused by long-term wear and tear. (Guterl, C. C. et al., 2013) The tears are typically caused by age-related degenerative changes in the disc, which can also lead to degeneration in other areas of the spine. Wear and tear are caused by annular fissures due to an individual’s daily living habits, such as sitting, standing, walking, climbing stairs, and performing other routine movements.
Treatment
While a large annular fissure is not likely to improve without treatment, a small one could heal independently. However, once an area has torn, it becomes more likely to continue tearing. (Virginia Spine Institute, N.D.) Conservative treatment is usually enough to control pain and symptoms. Physical therapy and anti-inflammatory medication are the first line of treatment. (Cheng, J. et al., 2019) Medication can be over-the-counter or prescription. Physical therapy treatment includes exercises, traction, and other therapies. If these do not help with the symptoms, the provider may suggest a steroid injection to reduce inflammation and pain. It can take three to six months to recover from degenerative disc problems if doing a standard treatment plan that includes rest, low-impact therapy exercises, and anti-inflammatory treatments. (Cheng, J. et al., 2019)
In severe cases, surgery may be recommended, including disc replacement surgery. An annular tear is not a reason to have disc replacement surgery alone; it is only when there are degenerative changes in the vertebral disc that surgery might be necessary. (Yue, J. J. et al., 2012)
Improving Body Alignment
Not paying attention and being aware of how the body performs everyday activities can, over time, set the stage for an annular fissure and other musculoskeletal injuries. However, fixing daily movement and posture habits to prevent injuries can be done through simple adjustments. For example, strengthening the core and back muscles can reduce pressure on the spine and help prevent injuries. (Camp, C. L. et al., 2016) The idea is to improve joint and overall body alignment. Activities can include:
Strength training
Walking
Pilates classes
Yoga
Tai chi
Somatic exercises
These activities help with muscle balance and joint alignment, which are recommended prevention strategies that physical therapists use when working with individuals who need help with spinal problems.
Visiting a chiropractic and physical therapy team can help treat injuries and chronic pain syndromes, relieve pain, resolve musculoskeletal issues, and prevent future symptoms. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a personalized care program for each patient through an integrated approach to treating injuries, improving flexibility, mobility, and agility to help return to normal and optimal function. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Back Pain Specialist
References
Stadnik, T. W., Lee, R. R., Coen, H. L., Neirynck, E. C., Buisseret, T. S., & Osteaux, M. J. (1998). Annular tears and disk herniation: prevalence and contrast enhancement on MR images in the absence of low back pain or sciatica. Radiology, 206(1), 49–55. https://doi.org/10.1148/radiology.206.1.9423651
Jarvik, J. G., Hollingworth, W., Heagerty, P. J., Haynor, D. R., Boyko, E. J., & Deyo, R. A. (2005). Three-year incidence of low back pain in an initially asymptomatic cohort: clinical and imaging risk factors. Spine, 30(13), 1541–1549. https://doi.org/10.1097/01.brs.0000167536.60002.87
Guterl, C. C., See, E. Y., Blanquer, S. B., Pandit, A., Ferguson, S. J., Benneker, L. M., Grijpma, D. W., Sakai, D., Eglin, D., Alini, M., Iatridis, J. C., & Grad, S. (2013). Challenges and strategies in the repair of ruptured annulus fibrosus. European cells & materials, 25, 1–21. https://doi.org/10.22203/ecm.v025a01
Virginia Spine Institute. (N.D.). Annular disc tear Understanding the Symptoms, Causes, and Treatments. https://www.spinemd.com/conditions/annular-disc-tear/
Cheng, J., Santiago, K. A., Nguyen, J. T., Solomon, J. L., & Lutz, G. E. (2019). Treatment of symptomatic degenerative intervertebral discs with autologous platelet-rich plasma: follow-up at 5-9 years. Regenerative medicine, 14(9), 831–840. https://doi.org/10.2217/rme-2019-0040
Yue, J. J., Telles, C., Schlösser, T. P., Hermenau, S., Ramachandran, R., & Long, W. D., 3rd (2012). Do presence and location of annular tear influence clinical outcome after lumbar total disc arthroplasty? A prospective 1-year follow-up study. International journal of spine surgery, 6, 13–17. https://doi.org/10.1016/j.ijsp.2011.09.001
Camp, C. L., Conti, M. S., Sgroi, T., Cammisa, F. P., & Dines, J. S. (2016). Epidemiology, Treatment, and Prevention of Lumbar Spine Injuries in Major League Baseball Players. American journal of orthopedics (Belle Mead, N.J.), 45(3), 137–143.
Individuals dealing with pain in the buttocks can make life difficult to sit, walk, or perform simple, everyday tasks. Can understanding the anatomy, location, and function of the gluteus maximus muscle help in muscle rehabilitation and avoid potential injuries?
Gluteus Maximus
The gluteus maximus is the largest human body muscle responsible for hip extension, external rotation, adduction, and abduction, as well as the ability to stand upright. The primary muscle extends laterally and keeps the body upright by supporting the bony pelvis and trunk. (Neto W. K. et al., 2020) When the gluteus maximus is strained, injured, or weak, it can lead to pain and inflammation.
Common symptoms can include:
Stiffness in the buttock
Discomfort while sitting
Difficulty standing up from sitting
Difficulty bending over
Pain when walking, especially upstairs or on a hill
Pain in the lower back and/or tailbone
Anatomy and Structure
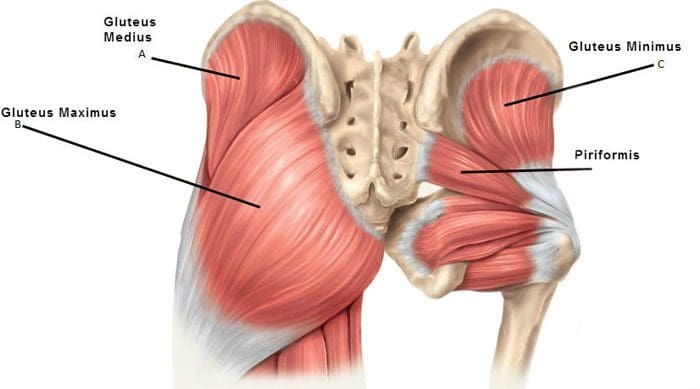
The muscles that comprise the glutes are the gluteus maximus, gluteus medius, and gluteus minimus. The gluteus medius runs underneath the gluteus maximus, and the gluteus minimus is underneath the gluteus medius.
The gluteus maximus is one of the strongest muscles. Fibers from the muscle connect to different body parts, including the femur/thighbone and the iliotibial band, which comprises connective tissue that runs up the thigh. The superior gluteal artery transports blood from the heart to the glutes.
Nerve Supply
The inferior gluteal nerve, part of the sacral plexus branch, innervates the maximus muscle. The sacral plexus nerves support motor and sensory function in the thighs, lower legs, feet, and pelvis. The sciatic nerve runs under the gluteus maximus, from the lower back down to the leg, and is often the cause of nerve pain in and around the area. (Carro L. P. et al., 2016) The main nerve of the perineum is the pudendal nerve, which runs under the gluteus maximus muscle.
Location
The gluteus maximus muscle defines the buttocks. It can be called a superficial muscle, sometimes referred to muscles that help provide shape. The origin of the gluteus maximus connects to the sacrum, the ilium, or the large upper part of the hip bone, the thoracolumbar fascia tissue, and the sacrotuberous ligaments attached to the posterior superior iliac spine. The gluteus maximus has a 45-degree angle from the pelvis to the buttocks and then inserts at the gluteal tuberosity of the femur and the iliotibial tract.
Variations
Sometimes, a duplicate muscle may originate from the gluteus maximus muscle in rare cases. However, it is more common that the gluteus maximus muscle fibers may be inserted into different body parts than where they are typically inserted. (Taylor, V. G., Geoffrey & Reeves, Rustin. 2015) This can cause a condition called greater trochanteric pain syndrome or GTPS. Inflammation of the gluteus medius, minimum tendons, and bursa inflammation can also cause GTPS. Individuals with GTPS will have tenderness or a pulsing feeling on the outer side of the hip and thigh when lying on the side, along with other symptoms.
Function
The gluteus maximus extends and externally rotates the hip joint, stabilizing the body. It is highly engaged during running and hiking activities. Regular walking does not typically target gluteus maximus strength training. However, the gluteus maximus promotes balance when walking and other activities by helping keep the pelvis and posture upright.
Conditions
The most common condition associated with the gluteus maximus is muscle strain, and deep gluteus maximus syndrome is another condition that can cause pain and involves the muscles.
Muscle Strain
A muscle strain can result from stretching and working the muscle too much that it becomes overstretched or tears. (Falótico G. G. et al., 2015) This can happen from not warming up or cooling down properly, repetitive use injury, and over-exercising. Alternatively, not exercising and not utilizing your gluteus maximus can weaken it, leading to lower back pain, hip pain, and stability and posture issues. (Jeong U. C. et al., 2015)
Deep Gluteus Maximus Syndrome
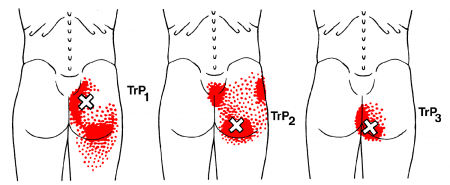
This syndrome causes pain in the buttocks when the sciatic nerve becomes entrapped. (Martin, H. D. et al., 2015) The location of the pain can help healthcare providers determine where the nerve is trapped. Those with deep gluteus maximus syndrome may experience various types of discomfort, including (Martin, H. D. et al., 2015)
Numbness and tingling in the leg
Pain when sitting
Pain when walking
Pain that radiates down the back and hips and into the thigh
To diagnose the condition, a healthcare provider may perform a physical examination and various tests to rule out other conditions that can cause similar symptoms.
Treatment and Rehabilitation
If there is pain in the buttocks and/or lower extremities, it’s important to consult a primary doctor, chiropractor, or physical therapist. They will evaluate the strength of the gluteus muscles to diagnose any strain or weakness. From there, they will develop a personalized treatment plan to help heal the injury, strengthen the muscles, and restore function. Treatment will include stretches once the strain is rested and improves.
Recommendations can include taking a few days off to rest the muscle or, at the very least, stop performing the work or activity that caused the strain.
Ice and over-the-counter medication like ibuprofen can help reduce inflammation.
For weak gluteus maximus, a physical therapist will strengthen and retrain the muscle with a tailored program of exercises. (Jeong U. C. et al., 2015)
Treatment for deep gluteus maximus syndrome may include conservative treatment, such as chiropractic decompression and realignment, physical therapy, medications for pain and inflammation, and injections.
If conservative treatments do not relieve the pain, a primary healthcare provider may recommend surgery. (Martin, H. D. et al., 2015)
Working with a chiropractic physical therapy team can help individuals return to normal function and expedite healing. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a customized treatment program through an integrated approach to treating injuries and chronic pain syndromes, improving flexibility, mobility, and agility to relieve pain and help individuals return to normal activities. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
The Science of Motion and Chiropractic Care
References
Neto, W. K., Soares, E. G., Vieira, T. L., Aguiar, R., Chola, T. A., Sampaio, V. L., & Gama, E. F. (2020). Gluteus Maximus Activation during Common Strength and Hypertrophy Exercises: A Systematic Review. Journal of sports science & medicine, 19(1), 195–203.
Carro, L. P., Hernando, M. F., Cerezal, L., Navarro, I. S., Fernandez, A. A., & Castillo, A. O. (2016). Deep gluteal space problems: piriformis syndrome, ischiofemoral impingement and sciatic nerve release. Muscles, ligaments and tendons journal, 6(3), 384–396. https://doi.org/10.11138/mltj/2016.6.3.384
Taylor, Victor & Guttmann, Geoffrey & Reeves, Rustin. (2015). A variant accessory muscle of the gluteus maximus. International Journal of Anatomical Variations. 8. 10-11.
Falótico, G. G., Torquato, D. F., Roim, T. C., Takata, E. T., de Castro Pochini, A., & Ejnisman, B. (2015). Gluteal pain in athletes: how should it be investigated and treated?. Revista brasileira de ortopedia, 50(4), 462–468. https://doi.org/10.1016/j.rboe.2015.07.002
Jeong, U. C., Sim, J. H., Kim, C. Y., Hwang-Bo, G., & Nam, C. W. (2015). The effects of gluteus muscle strengthening exercise and lumbar stabilization exercise on lumbar muscle strength and balance in chronic low back pain patients. Journal of physical therapy science, 27(12), 3813–3816. https://doi.org/10.1589/jpts.27.3813
Martin, H. D., Reddy, M., & Gómez-Hoyos, J. (2015). Deep gluteal syndrome. Journal of hip preservation surgery, 2(2), 99–107. https://doi.org/10.1093/jhps/hnv029
For individuals wanting to try Pilates for back pain and exercise, can learning how to find their neutral spine help improve flexibility and increase the range of motion in the joints?
Pilates Neutral Spine
Pilates is a functional exercise modality emphasizing core stability, which is fundamental to developing a balanced body. The exercises strengthen the muscles, improve flexibility, and increase the range of motion in the joints. (Kloubec J. 2011) It is considered a functional fitness method because its principles work to establish more graceful, efficient movements from everyday life, such as improving posture. Pilates has shown its effectiveness in that it is often used in physical therapy and rehabilitation settings. (Byrnes, K., Wu, P. J., and Whillier, S. 2018) However, knowing how to find the neutral spine is essential for performing various Pilates exercises correctly. (Barbosa, A. C. et al., 2018) This subtle adjustment during practice may help prevent injury and increase overall performance. A neutral spine is the natural position of the spine when all three curves:
Cervical (neck)
Thoracic (middle)
Lumbar (lower)
Are active and in healthy alignment.
This is the strongest position for the spine when standing or sitting, allowing the body to move more naturally.
Alignment
The following exercise can help find the Pilates neutral spine.
Basic Position
Lie on the back with knees bent and feet flat on the floor.
Ensure the legs are parallel to the hips, knees, heels, and toes.
Let the arms rest at your sides.
Relax
Relax the body, including the shoulders, neck, and jaw.
Allow the back to melt into the floor.
The rib cage will drop when the lower ribs are released to the floor.
Breathe Deep
Inhale all the way into the body, allowing it to move into the back and sides of the rib cage and all the way to the pelvis.
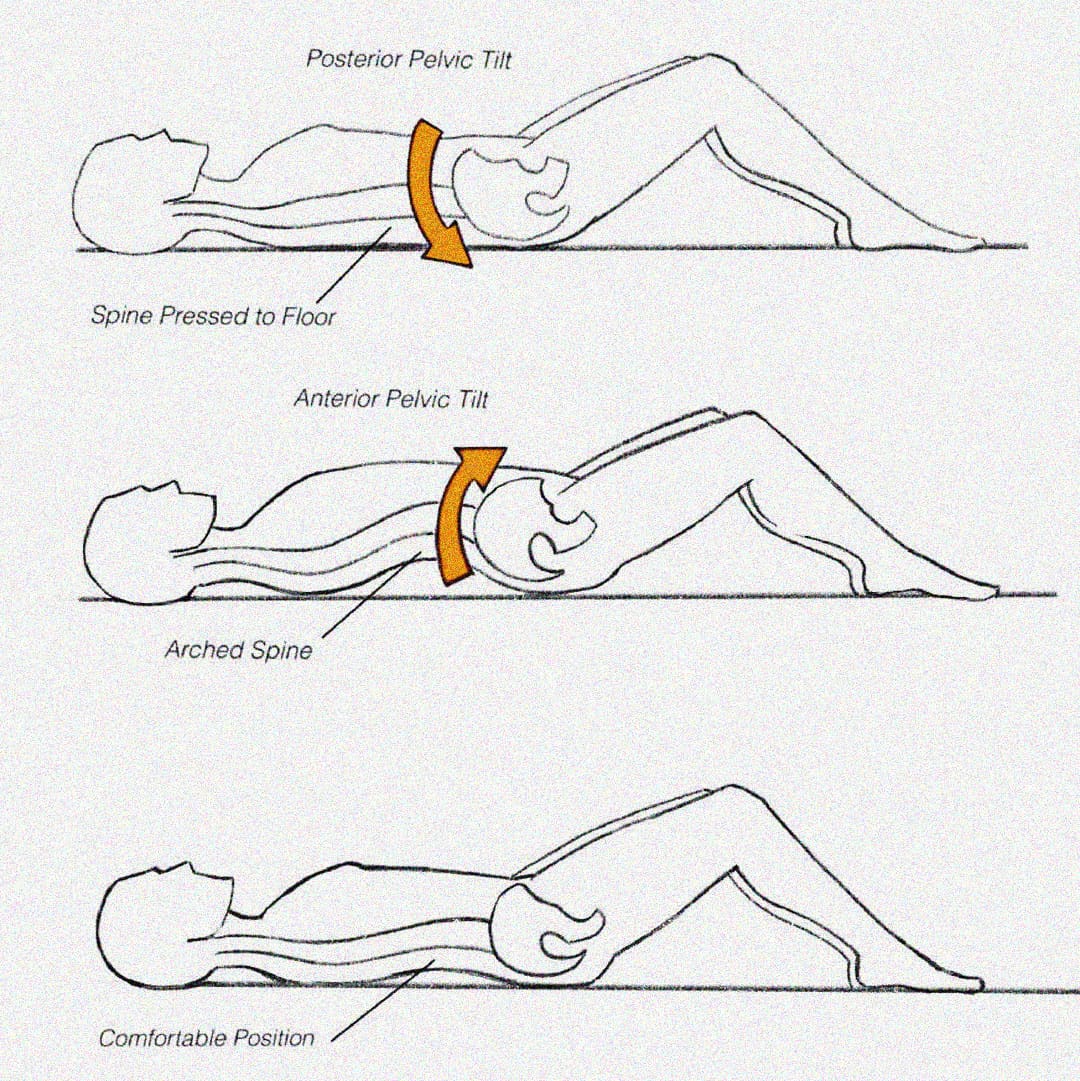
Pelvic Tilt
Exhale and use the abdominals to press the lower spine into the floor in a pelvic tuck. (Eickmeyer S. M. 2017)
Inhale to release.
Exhale and pull the lower spine off the floor, creating a pelvic tilt.
Inhale to release.
Pilates exercises don’t use excess energy or tension. Proper alignment and a neutral spine position can ensure that tension is released and excess energy is not exerted. (Byrnes, K., Wu, P. J., and Whillier, S. 2018) When performing the exercise, ensure that the shoulders, neck, and legs are relaxed and not involved in the movement.
When Exercising
Once a neutral spine is achieved, the goal is to maintain this spinal position during the exercises and when changing positions.
Start by lifting the right leg and placing it back down without letting the hips move.
Then, repeat the motion with the left leg.
Engage the abdominal muscles to help stabilize the pelvis, keeping it from moving and maintaining a neutral spine.
Repeat this process with each leg.
Once each leg can be lifted easily, test with both legs.
Exhale deeply and lift the legs while keeping the core and pelvis stable.
Then, lower them back down.
When performing this progression, there may be a want to release the abs and let the back arch.
This will cause a tuck and tilt position away from the neutral spine position.
If this progression is difficult, keep practicing until you can maintain a neutral spine.
Once this basic progression feels easy, try additional progressions and positioning.
Visualization Tips
Most people have their spines in one of two positions: tucked or tilted. A neutral spine requires individuals to be in between, with the lower abdominals flat and the lower spine’s natural curve slightly off the floor. The following visualization can help establish a neutral spine.
Balanced Pelvic Placement
Imagine a cup of water sitting on the lower abdomen, a couple of inches below the belly button.
Allow the abdominal muscles to drop toward the spine, flattening the belly.
You don’t want the water to spill, so the pelvis cannot be tipped forward or tucked under.
Body Scan Meditation
Once the body is relaxed with a balanced alignment on the floor.
Allow breathing to become deep and full and the abdominals to drop toward the floor.
The natural neck and lower spine curves should be off the floor.
Ensure the lower spine is not pressed into the floor, as this indicates a pelvic tilt.
If there is any discomfort or pain when working to increase endurance, seek advice from a healthcare professional. Injury Medical Chiropractic and Functional Medicine Clinic uses an integrated approach to treating injuries and chronic pain syndromes. It offers personalized care plans that improve ability through flexibility, mobility, and agility programs to relieve pain. Our providers use an integrated approach to create personalized care plans for each patient, including Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles. Our goal is to relieve pain naturally by restoring health and function to the body. If other treatment is needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Is Motion Key to Healing?
References
Kloubec J. (2011). Pilates: how does it work and who needs it?. Muscles, ligaments and tendons journal, 1(2), 61–66.
Byrnes, K., Wu, P. J., & Whillier, S. (2018). Is Pilates an effective rehabilitation tool? A systematic review. Journal of bodywork and movement therapies, 22(1), 192–202. https://doi.org/10.1016/j.jbmt.2017.04.008
Barbosa, A. C., Vieira, E. R., Silva, A. F., Coelho, A. C., Martins, F. M., Fonseca, D. S., Barbosa, M. A., & Bordachar, D. (2018). Pilates experience vs. muscle activation during abdominal drawing-in maneuver. Journal of bodywork and movement therapies, 22(2), 467–470. https://doi.org/10.1016/j.jbmt.2017.05.002
Eickmeyer S. M. (2017). Anatomy and Physiology of the Pelvic Floor. Physical medicine and rehabilitation clinics of North America, 28(3), 455–460. https://doi.org/10.1016/j.pmr.2017.03.003
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine