Mobility Challenges in Mexican and Mexican American Communities: Insights from El Paso Back Clinic®
Mexican-American with back pain at a construction site.
At El Paso Back Clinic® in El Paso, TX, we see many patients from Mexican and Mexican American backgrounds facing mobility issues. These problems often stem from tough jobs, health factors like obesity, and aging. Our wellness chiropractic care focuses on pain relief and improved movement. This article discusses common issues such as arthritis and back pain, supported by studies. We’ll explain how our team, including Dr. Alexander Jimenez, DC, APRN, FNP-BC, uses integrative approaches to help. If you’re in El Paso dealing with these, our clinic is here for you.
Common Musculoskeletal Mobility Issues We Treat
Musculoskeletal problems affect your bones, muscles, and joints, making it difficult to move freely. At our clinic, we see these issues often in our community, where many work in demanding fields like farming or construction.
Arthritis, especially in the knees, is a top concern. It causes joint wear-related swelling and pain. In Mexico, about 20-25% of adults aged 40+ have it, with higher rates among women (Villarreal Rizzo et al., 2025). Mexican Americans in the U.S. also face risks, like osteoporosis weakening bones in 16% of women (Wright et al., n.d.). At El Paso Back Clinic®, we help ease this with gentle adjustments and exercises.
Chronic low back pain hits hard, too. It comes from prolonged lifting or standing. In Mexico, it’s the leading cause of disability, with 840.6 cases per 100,000 in 2021 (Clark et al., 2023). Among farmworkers here in Texas, 46.9% report back issues affecting daily life (Weigel et al., 2013). Our chiropractic care targets this to get you moving again.
Work injuries often involve the shoulders, wrists, and legs. Repetitive tasks in jobs cause rotator cuff problems in 19.1% and elbow pain in 20.2% of Latino workers (Mora et al., 2014). Older adults in our area are at risk of frailty due to ongoing pain, leading to reduced mobility (National Institutes of Health, n.d.). Women face more disability in tasks like walking, with arthritis raising risks by 35% over time (Rodriguez et al., 2021).
Here are key facts we see in our patients:
Arthritis rates: 19.6% for knee issues in Mexicans over 40, up to 24.2% in women (Ciampi de Andrade et al., 2022).
Back pain: Affects 16.9% of farmworkers from repetitive strain (Mora et al., 2014).
Craft-related injuries: Neck and knee pain from activities like weaving (Jeanson et al., 2025).
Disability trends: Physical function declines by 0.18 points per year with arthritis (Rodriguez et al., 2021).
Jobs in agriculture and construction drive these, plus obesity adds joint stress. In our Mexican American patients, higher BMI initially slows strength loss but worsens it later (Davis & Al Snih, 2025). About 83% of Hispanic men are overweight, linked to less activity (Valdez et al., 2019). At El Paso Back Clinic®, we address this with personalized plans.
Neuromusculoskeletal Issues Addressed at Our Clinic
These issues combine nerve problems with muscle and bone pain, leading to numbness or weakness. Our wellness approach helps restore nerve function and reduce discomfort.
Chronic low back pain is common, often due to nerve compression. It’s the main cause of disability in Mexico (Alva Staufert et al., 2021). Knee and foot arthritis affects movement, with 25.5% showing joint changes (Ciampi de Andrade et al., 2022). We treat foot pain from standing jobs, seen in 4.8% of workers (Mora et al., 2014).
Shoulder injuries, such as rotator cuff tears, are associated with overhead work and affect 19.1% (Mora et al., 2014). Elbow issues, or epicondylitis, affected 20.2% due to tool use (Mora et al., 2014). MSDs in Mexico rose 57.3% over 30 years (Clark et al., 2023). Obesity plays a role, with 40% of Hispanic men affected (Valdez et al., 2019).
In border areas like El Paso, women report 29.8% low back and 38.3% upper back pain from factory jobs (Harlow et al., 1999). Older patients walk more slowly due to leg pain (Quiben & Hazuda, 2015).
Common issues we handle:
Low back pain: Top disability driver, tied to work and weight (Alva Staufert et al., 2021).
Knee/foot arthritis: More in women, causing stiffness (Ciampi de Andrade et al., 2022).
Rotator cuff: From arm overuse in construction (Mora et al., 2014).
Epicondylitis: Elbow strain, common in 20% (Mora et al., 2014).
How El Paso Back Clinic® Helps with Integrative Care
Our clinic combines nurse practitioners (NPs) and chiropractic methods for culturally sensitive help. We focus on pain management and rehab to fit our community’s needs.
NPs at our clinic offer full check-ups that consider culture and history. They suggest diets rich in veggies and yoga for detox and pain relief (Jimenez, 2026a). We team up for whole-body care (Jimenez, 2026b).
Chiropractic adjustments realign the spine to ease nerve compression. For sitting-related back pain, we restore curves and strengthen the core (El Paso Back Pain Clinic, n.d.). Access to this care is key, though Hispanics use it less (Roseen, 2023).
Dr. Alexander Jimenez shares from his experience: Chronic back pain worsens with poor posture, but adjustments and exercises help (Jimenez, n.d.). For sciatica, decompression relieves pressure on nerves, which is common in laborers. Neuropathy gets therapy for tingling (Jimenez, n.d.). He uses functional medicine to tackle stress, diet, and job factors in our Mexican American patients.
We include mindfulness and natural remedies. Cultural factors, such as family support, help recovery, but delays worsen pain (Arthritis Foundation, n.d.). Our NPs create home plans (Pérez-Stable et al., 2003).
Rehab strengthens areas such as the legs and shoulders (Mora et al., 2014). It cuts frailty risks (National Institutes of Health, n.d.). For farmworkers, it reduces disability (Weigel et al., 2013).
Our care benefits:
Cultural match: Understanding barriers like work migration (Harlow et al., 1999).
Strength building: Targeted exercises (Mora et al., 2014).
Prevention: Nutrition against obesity (Valdez et al., 2019).
Why Choose El Paso Back Clinic® for Your Mobility Needs
In El Paso, with our diverse community, these issues are common but treatable. Our clinic specializes in wellness chiropractic to help you stay active. Contact us for a consultation with Dr. Jimenez and our team.
Natural Detox Support at El Paso Back Clinic®: Enhancing Your Body’s Wellness in El Paso, TX
A Chiropractor/Nurse Practitioner points to various organs on a computer screen.
In the busy city of El Paso, Texas, staying healthy means helping your body naturally cleanse itself. Organs like the liver and kidneys handle detoxification every day, removing waste from food, air, and daily life. But factors like stress, poor diet, or injuries can slow this down. At El Paso Back Clinic®, a top wellness chiropractic care clinic in El Paso, TX, we focus on supporting your body’s own detox processes. Our team, led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, combines nurse practitioner expertise with integrative chiropractic care for a whole-body approach. We avoid quick fixes and instead promote lasting health through nutrition, adjustments, and lifestyle tips.
Many folks chase trendy detoxes like juice cleanses, but experts agree the body doesn’t need them if it’s working well. The liver breaks down toxins, and the kidneys filter them out (MD Anderson Cancer Center, n.d.). Risky methods like colon cleanses can harm your gut balance (Lehigh Valley Health Network, n.d.). At our clinic, we guide patients toward safe, natural ways to support detoxification, drawing on over 30 years of Dr. Jimenez’s experience in functional medicine and injury recovery.
Dr. Jimenez’s clinical work at El Paso Back Clinic® demonstrates how gentle methods help reset the body, especially after holidays or other sources of stress. We address root causes, such as gut issues or pain, that affect detox, using personalized plans for El Paso residents (Jimenez, n.d.a; Jimenez, n.d.b).
How Nurse Practitioners at El Paso Back Clinic® Aid Natural Detox
At El Paso Back Clinic®, our nurse practitioners (NPs) are key to detox support. As advanced nurses, they diagnose and manage health needs, focusing on liver and kidney function with everyday habits. Located at 11860 Vista Del Sol Dr, Suite 128, in El Paso, TX, we offer convenient care for locals dealing with pain, fatigue, or toxin buildup.
Boosting Liver and Kidney Health
The liver and kidneys are detox powerhouses. Our NPs help by recommending simple nutrition and hydration changes tailored to your life in El Paso, where dry weather can make staying hydrated tough.
Choose colorful produce: Fruits and veggies full of antioxidants protect your liver (Whole Family Health Care, n.d.).
Drink plenty of water: This flushes the kidneys and fights dehydration common in our desert climate (Care and, n.d.).
Balance protein intake: Opt for plant-based options to avoid overloading the kidneys (Care and, n.d.).
Add fiber: Whole grains and beans help gut detox by binding waste (University of Wisconsin Department of Family Medicine and Community Health, n.d.).
We monitor your health to spot early signs of strain, like from meds or local pollution. Dr. Jimenez uses functional tests at the clinic to check for toxins and suggest nutrient boosts (Jimenez, n.d.a).
Hydration is extra important here in El Paso. Our NPs teach that water supports sleep and that much detox occurs (Comprehensive Cancer Centers of Nevada, n.d.). We swap soda for herbal teas to keep things natural.
Handling Substance Withdrawal Safely
For those in El Paso facing addiction, detox means safe withdrawal. Our NPs manage this with meds and checks, easing symptoms in a supportive setting.
Prescribe calming meds: Like lorazepam for alcohol withdrawal (National Center for Biotechnology Information, n.d.a).
Track health signs: Watch blood pressure to avoid risks (Pine Rest Christian Mental Health Services, n.d.).
Offer comfort: Counseling helps through emotional ups and downs (Health eCareers, n.d.).
As certified addictions experts, our team customizes detox protocols, using tapers for substances like opioids (Mississippi Drug and Alcohol Treatment Center, n.d.). We stabilize patients medically and mentally first (National Center for Biotechnology Information, n.d.b). Family involvement builds strong support, key in our community-focused clinic (Health eCareers, n.d.).
Dr. Jimenez’s neuropathy and addiction care at El Paso Back Clinic® blends NP skills for symptom relief without over-relying on drugs (Jimenez, n.d.b).
Using Holistic Techniques for Stress Relief
Stress is a big detox blocker, raising hormones that slow liver work (Richmond Functional Medicine, n.d.). At our El Paso clinic, NPs use whole-person methods to calm the mind and body.
Safe herbs: Like milk thistle for liver aid, chosen just for you (Natural Healers, n.d.).
Relaxing therapies, such as massage or acupuncture, promote peace (Collaborating Docs, n.d.).
Dr. Jimenez notes stress management is vital for chronic pain patients here, using clinic tools to balance emotions (Jimenez, n.d.a).
Promoting Lasting Lifestyle Shifts
We stress habits that stick, not fads. Our NPs create plans fitting El Paso’s active lifestyle, from border walks to mountain hikes.
Healthy eating: Focus on whole foods to fuel detox (Whole Family Health Care, n.d.).
Quality rest: 7-9 hours lets your body clean house (Comprehensive Cancer Centers of Nevada, n.d.).
Move daily: Exercise boosts blood flow and sweat (University of Wisconsin Department of Family Medicine and Community Health, n.d.).
Handle stress: Yoga classes at our clinic keep systems smooth (Richmond Functional Medicine, n.d.).
Plans are personal, taking into account your job or family. We collaborate with other pros to resolve issues like stress from long commutes. Education empowers you—learn why changes help (Natural Healers, n.d.). In addiction recovery, we cover triggers (Health eCareers, n.d.).
At El Paso Back Clinic®, Dr. Jimenez’s integrative NP role uses nutrition science to support detoxification without judgment (Jimenez, n.d.b). This builds natural health for our community.
How Integrative Chiropractors at El Paso Back Clinic® Enhance Detox
Our integrative chiropractors at El Paso Back Clinic® look at the whole you, starting with spine health. They improve nerve function, flow, and organ work for better detox, all in our welcoming El Paso spaces.
Fine-Tuning the Nervous System
Nerves control detox organs. Spine misalignments block signals, slowing cleanup. Our adjustments fix this gently.
Realign spine: Eases nerve pressure for optimal function (DC Labs, n.d.).
Support organs: Better signals help the liver and kidneys (Impact Chiropractic, n.d.a).
Dr. Jimenez’s clinic observations indicate that chiropractic aids detoxification in functional medicine (Jimenez, n.d.a).
Adjustments enhance natural waste removal, not myths about toxin release (Dr. Chris Harlan, n.d.).
Boosting Lymph and Blood Flow
Lymph drains waste; blood carries nutrients. Chiropractors promote this for efficient detox.
Increase movement: Adjustments get fluids circulating (Impact-Chiropractic, n.d.).
Cut swelling: Less inflammation eases detox (Dallas Accident and Injury Rehab, n.d.).
We add exercise tips, like stretches for El Paso’s warm days (Mountain Movement Center, n.d.).
Dr. Jimenez sees adjustments as helping circulation during sports recovery, aiding detox (Jimenez, n.d.b).
Holistic Support for Organs
Our chiropractors combine adjustments with nutrition and lifestyle advice for comprehensive detox support.
Eat smart: Anti-inflammatory foods for organ health (Hutsell Chiropractic, n.d.).
Hydrate well: Water supports the kidneys in our dry area (Cascades Chiropractors, n.d.).
Daily habits: Exercise and relaxation improve waste exit (Mountain Movement Center, n.d.).
We relieve pressure through alignment, no harsh flushes (DC Labs, n.d.).
Dr. Jimenez combines this with NP care for conditions such as sciatica (Jimenez, n.d.b).
Steering Clear of Quick Fixes
We guide away from extremes, toward steady changes for El Paso lifestyles.
Fix posture: Reduces organ stress (Impact Chiropractic, n.d.b).
Pair with nutrition: Boosts adjustment benefits (Hutsell Chiropractic, n.d.).
Patients often feel happier and more energetic post-care (Dr. Chris Harlan, n.d.).
Dr. Jimenez’s gentle resets align with our clinic’s philosophy (Jimenez, n.d.b).
The Benefits for Your Long-Term Wellness in El Paso
At El Paso Back Clinic®, NPs and chiropractors team up for top detox support, avoiding the risks of fad diets. We enhance the liver, kidneys, nerves, and flow for true wellness.
Dr. Jimenez’s expertise ensures smart, non-invasive care (Jimenez, n.d.a; Jimenez, n.d.b). Call 915-850-0900 to start your journey.
Natural detox thrives on support, not shortcuts. Our clinic empowers El Pasoans for healthier lives.
Fun Ways to Stay Active: Alternatives to Boring Workouts for Better Health
Friends play table tennis as a way to start making fitness fun and as a doable health goal.
Many people start the new year with big fitness goals. They promise to hit the gym every day or run miles each week. But often, these plans fall apart quickly. Life gets busy, motivation fades, and suddenly, exercise feels like a chore. If this sounds like you, don’t worry. Giving up on strict resolutions doesn’t mean giving up on health. Instead, shift to activities that feel more like play than work. Fun sports and easy movements can keep you moving without the dread of traditional workouts. This approach makes staying active sustainable and enjoyable, leading to better long-term habits (Bayou Bend Health System, n.d.).
Research shows that making physical activity fun boosts your chances of sticking with it. For example, choosing things you enjoy turns exercise into a hobby. This can improve your mood, reduce stress, and even help with weight management. Health experts recommend at least 150 minutes of moderate activity per week for adults, but it doesn’t have to be in a gym (NHS, n.d.). Simple swaps like walking in nature or dancing to music can meet these goals while feeling effortless.
In this article, we’ll explore ways to restart your fitness journey with joy. We’ll cover fun sports, social options, and relaxing practices. We’ll also discuss low-impact choices for those who struggle with standard routines. Plus, learn how professionals like integrative chiropractors and nurse practitioners can guide you. Drawing from expert insights, including clinical observations from Dr. Alexander Jimenez, DC, APRN, FNP-BC, this guide offers practical tips to get back on track.
Restarting After a Failed New Year’s Resolution
If your resolution crashed early, it’s time for a fresh start. The key is picking activities that excite you. Fun, easy sports like hiking, dancing, swimming, or biking can make movement feel rewarding. These options build fitness without the pressure of sets and reps.
Hiking: Head to a trail for fresh air and views. It’s a great way to explore while getting your heart rate up. Start with short paths and build up. Hiking strengthens legs and improves balance, all while enjoying nature (MultiCare Clinic, n.d.).
Dancing: Put on your favorite tunes and move freely. Whether alone or in a class, dancing boosts cardio and coordination. It’s low-pressure and can burn calories without feeling like exercise (Whispering Oaks Senior Living, n.d.).
Swimming: Water supports your body, making it gentle on joints. Swim laps or just splash around for fun. It’s ideal for all ages and helps with endurance (Vista Springs Living, n.d.).
Biking: Ride a bike around your neighborhood or on paths. It’s easy to adjust speed and distance. Biking tones muscles and can be a social outing (Blue Cross NC, n.d.).
These activities trick your brain into thinking you’re playing, not working out. Studies support this: enjoyable exercise leads to better adherence and health outcomes (Exercise is Medicine, n.d.).
Beyond solo sports, join social activities to add fun. Pickleball, tennis, or team sports bring people together, making commitment easier.
Pickleball: A mix of tennis and ping-pong, it’s easy to learn and play. Courts are popping up everywhere, and it’s great for quick games with friends (Nerd Fitness, n.d.).
Tennis: Hit the court for rallies that improve agility. Doubles makes it less intense and more chatty (Athlean-X, n.d.).
Team Sports: Join a recreational league for soccer, basketball, or volleyball. The group vibe keeps you motivated, and games feel like events, not drills (Quora, n.d.).
Social exercise can reduce feelings of isolation while building strength. One study notes that group activities enhance mental health alongside physical benefits (Reddit, n.d.).
For a calmer approach, try mind-body practices like yoga or Tai Chi. These are low-impact and focus on relaxation.
Yoga: Gentle poses improve flexibility and reduce stress. Start with beginner videos at home. It helps with breathing and mindfulness (Piedmont Wellness Center, n.d.).
Tai Chi: Slow, flowing movements build balance and calm the mind. It’s perfect for easing into activity without strain (Care Insurance, n.d.).
These practices are adaptable for any fitness level. They promote relaxation, which can lower blood pressure and improve sleep (NHLBI, n.d.).
To build habits, start small. Aim for 10–15 minute sessions a few times a week. Gradually increase as you gain confidence. This prevents burnout and lets your body adjust (Bayou Bend Health System, n.d.). Track progress in a journal to see improvements, like feeling more energetic.
Options for Those Who Dislike Traditional Workouts
Not everyone loves the gym or running. If weights and treadmills bore you, low-impact or sociable sports offer alternatives. These keep you active without the monotony, focusing on enjoyment and variety.
Swimming and biking stand out as low-impact favorites. Swimming provides a full-body workout in a supportive environment, reducing joint stress (Seniors Helping Seniors, n.d.). Biking lets you control the pace, making it accessible for beginners (MultiCare Clinic, n.d.).
Hiking and dancing add adventure. Hiking varies with terrain, keeping things interesting, while dancing lets you express yourself creatively (Blue Cross NC, n.d.; Whispering Oaks Senior Living, n.d.).
For a challenge, try rock climbing. It’s low-impact but builds strength and problem-solving skills. You can start indoors at a gym with easy walls (The Telegraph, n.d.).
Joining a recreational sports league brings community. Options like softball or ultimate frisbee emphasize fun over competition (Nerd Fitness, n.d.).
Benefits of These Activities:
More engaging than repetitive workouts.
Build social connections.
Adaptable to your energy level.
Improve mood through endorphins (Sanguina, n.d.).
These choices make the activity feel natural. For instance, walking briskly counts as exercise and can be done anywhere (Quora, n.d.). Or jump rope for short bursts—it’s simple and effective for cardio (MCU, n.d.).
If mobility is an issue, modify exercises. Chair-based routines or water aerobics allow movement without strain (ParentGiving, n.d.; Care.com, n.d.). The goal is consistency over intensity.
Experts agree: low-impact options like these support heart health and flexibility, especially for those with limits (Gaddis Premier, n.d.; Prairie Hills at Independence, n.d.).
How Integrative Professionals Can Help
When starting or restarting activity, professional guidance ensures safety. Integrative chiropractors and nurse practitioners offer tailored care, especially if you have physical limits.
Integrative chiropractors focus on the whole body. They use adjustments to align the spine, reducing pain and improving movement. This holistic approach addresses root causes rather than just symptoms (Integral Chiropractic, n.d.; Impastato Chiropractic, n.d.).
For example, if joint pain stops you from hiking, a chiropractor can ease stiffness through manipulations and exercises (Elysian Wellness Centre, n.d.; De Integrative Healthcare, n.d.). They often include nutrition and lifestyle advice for better results (AFP Fitness, n.d.; Together4Health Wellness, n.d.).
Nurse practitioners add medical expertise. They assess your health and create plans that address limits, such as suggesting low-impact swimming for arthritis (Buckner Parkway Place, n.d.; Cor Health Ontario, n.d.).
Together, these pros provide personalized care. They work with your abilities to help you enjoy activities again (Wellness Center FW, n.d.; Fortitude Health, n.d.).
Dr. Alexander Jimenez, DC, APRN, FNP-BC, embodies this integrated approach. With over 30 years in practice, he combines chiropractic and nursing for comprehensive care. His clinical observations highlight non-invasive methods for pain management and mobility.
In his work, Dr. Jimenez notes that tailored programs, like resistance band exercises, strengthen muscles without high impact. This helps people with injuries return to fun activities like biking or dancing. He emphasizes flexibility for joint health, noting that restricted movement can lead to pain, but gentle practices like yoga can restore it.
On LinkedIn, Dr. Jimenez shares insights on sciatica and back pain, recommending core exercises like modified squats for those with limitations. He advocates stretching to prevent stiffness, noting, “If you don’t stretch, your body ‘pays interest'” in reduced mobility.
His practice includes functional medicine, addressing nutrition and the environment for wellness. For example, he uses assessments to create plans that fit patients’ lifestyles, helping them stay active despite chronic conditions (All Injury Rehab, n.d.; Motus Integrative Health, n.d.).
How They Help:
Assess limits and set realistic goals.
Provide exercises like water aerobics for joint relief (Activ Therapy, n.d.).
Offer advice on enjoyable activities to build habits (Nepute Wellness Center, n.d.).
Monitor progress to adjust plans.
This support makes returning to movement less daunting. Integrative care focuses on harmony in physical, mental, and emotional health (Wellness Center FW, n.d.).
Wrapping Up: Make Movement Joyful
Staying active doesn’t require grueling workouts. By choosing fun options like hiking or yoga and seeking professional help when needed, you can rebuild habits. Remember Dr. Jimenez’s observation: personalized, holistic care unlocks better mobility. Start small, stay consistent, and enjoy the process. Your health will thank you.
Dr. Alex Jimenez at El Paso Back Clinic®: Beating Back Pain from Long Desk Hours
Businesswoman experiences worsening back pain while sitting at her desk.
If your back pain gets worse the longer you sit at your desk, you are not alone. Many people in El Paso face this issue due to long hours spent in sedentary jobs. Sitting for extended periods can put pressure on the spine, tighten muscles, and reduce blood flow, leading to stiffness, aches, and, in some cases, chronic problems (Colorado Pain Care, n.d.). The positive news is that you can take simple steps to reduce the pain and prevent it from worsening. At El Paso Back Clinic® in El Paso, TX, the wellness chiropractic care team, led by Dr. Alex Jimenez, DC, APRN, FNP-BC, focuses on helping people just like you find natural, long-term relief through personalized plans.
Prolonged sitting stresses the lower back by increasing disc pressure by up to 90% compared to standing. It flattens the spine’s natural curve, strains muscles, and creates imbalances (Colorado Pain Care, n.d.). Slouching or leaning forward adds extra load to the neck and upper back. Over time, this can lead to tight hips, weak core muscles, and ongoing discomfort that affects daily life.
At El Paso Back Clinic®, our experts understand these issues caused by sedentary work. They use a holistic approach that combines chiropractic adjustments, functional medicine, and rehab to address root causes like poor posture and muscle imbalances from desk jobs (Jimenez, n.d.-a).
Here are practical changes to start today:
Move often: Get up every 30 minutes to stand, walk, or shift positions. Short 1-2 minute breaks improve circulation and ease tension (Huntsville Hospital Health System, n.d.; Sydney West Physio, n.d.).
Use regular breaks: Set a timer for quick walks to get water or to stretch. This habit prevents stiffness from building up throughout the day.
Add dynamic movement: While sitting, shift weight, uncross legs periodically, or use a footrest to change angles. These small actions keep the spine mobile (Colorado Pain Care, n.d.).
A proper ergonomic setup supports optimal posture and reduces strain.
Follow these key tips:
Set your chair so that your feet are flat on the floor, your knees are at 90 degrees, and your hips are level with or above your knees.
Add lumbar support (a small pillow or rolled towel works) to maintain the lower back’s curve.
Place your screen at eye level to avoid looking down or up too much.
Keep the keyboard and mouse close so elbows bend at 90 degrees and shoulders stay relaxed.
Avoid crossing legs for long, as it can tilt the pelvis (Senara Chiropractic & Med Spa, n.d.; Huntsville Hospital Health System, n.d.).
Consider alternating between sitting and standing with a standing desk. Even partial standing reduces spinal pressure.
Stretches help loosen tight spots from sitting, such as the hips, shoulders, and neck.
Try these simple ones:
Hip flexor stretch: Kneel on one knee, gently push hips forward, and hold 20-30 seconds per side.
Chest and shoulder opener: Clasp hands behind your back or use a wall to stretch forward.
Neck tilts: Slowly tilt the head side to side or forward/back; hold for 10-15 seconds.
Upper back extension: Hands behind head, gently arch upper back (Sydney West Physio, n.d.).
Do them hourly or during breaks for better flexibility.
Strengthening the core supports the spine and improves posture long-term.
Include these:
Planks: Hold forearm plank 20-30 seconds.
Cat-camel: On hands and knees, arch and round back slowly.
Bridges: Lie back, lift hips while squeezing glutes.
Walking or gentle yoga: Build overall strength (Huntsville Hospital Health System, n.d.; Sydney West Physio, n.d.).
Aim for 20-30 minutes of activity most days.
For lasting relief, professional care targets alignment, mobility, and personalized fixes. At El Paso Back Clinic®, Dr. Alex Jimenez leads a team offering integrated chiropractic care. This includes spinal adjustments to correct misalignments, non-surgical spinal decompression for disc relief, acupuncture, functional medicine for nutrition and stress, and rehab exercises tailored to desk-related issues.
Dr. Jimenez, with dual expertise as a chiropractor and nurse practitioner, emphasizes posture correction, mobility training, and the prevention of sedentary pain through evidence-based methods. The clinic helps restore function without drugs or surgery, focusing on root causes like imbalances from prolonged sitting (Jimenez, n.d.-a; Jimenez, n.d.-b).
Other options in El Paso exist, but El Paso Back Clinic® stands out for its comprehensive wellness approach, advanced diagnostics, and patient-centered plans that go beyond basic adjustments.
If pain includes numbness, tingling, or weakness in the legs, or persists despite changes, seek evaluation to rule out serious conditions (University of Maryland Medical System, n.d.).
Start small: improve movement, setup, and stretches. If needed, contact El Paso Back Clinic® for expert help. Many in El Paso regain comfort and stay active with this care.
Spinal Hygiene Explained: Daily Habits to Keep Your Spine Strong and Pain-Free
A woman performs spinal hygiene exercises on a fitness ball at home, strengthening her back muscles.
Spinal hygiene is the practice of caring for your spine every day to keep it strong, flexible, and healthy. Just like brushing your teeth helps prevent cavities, spinal hygiene helps avoid back problems and keeps your body moving well. The spine supports your whole body, protects the nervous system, and lets you bend, twist, and stand tall. Good habits can make a big difference in how you feel now and as you get older.
What Spinal Hygiene Means
Spinal hygiene includes simple daily actions to protect the spine’s natural shape and movement. The spine has gentle curves that help absorb shock and allow smooth motion. When these curves stay balanced, and the spine moves freely, you feel better overall.
Proper posture: Sit and stand with your shoulders back, head aligned over your spine, and pelvis in a neutral position to avoid extra strain.
Regular movement and exercise: Stay active with walking, swimming, or stretching to keep joints loose and muscles strong.
Proper body mechanics: Lift things by bending your knees, keeping objects close to your body, and avoiding twists to prevent injury.
Core strength: Build muscles around your midsection for better support and stability.
Hydration and nutrition: Drink plenty of water to keep spinal discs cushioned, and eat foods rich in calcium, vitamin D, magnesium, and omega-3 fatty acids to support bone and tissue health.
Stress management: Use deep breathing, meditation, or yoga to reduce tension that tightens back muscles.
These steps help maintain the spine’s integrity and prevent issues like stiffness or pain (Spinenpain.org, n.d.; Lifemovesmt.com, n.d.).
Neglecting spinal hygiene can lead to problems over time. Poor habits can cause muscle imbalances, joint wear, reduced motion, and conditions such as herniated discs or chronic back pain. This can affect your nervous system, since the spine houses nerves that control body functions. When the spine is out of alignment, it may press on nerves, leading to pain, weakness, or other issues (Servinglifedallas.com, n.d.; Drmmalone.com, n.d.).
Benefits of Good Spinal Hygiene
Taking care of your spine brings many advantages. It reduces the chance of back pain, improves how easily you move, and supports better posture. A healthy spine also helps the nervous system function smoothly, boosting energy, coordination, and overall well-being. Regular care can slow age-related changes, lower injury risk, and help you stay active longer.
Prevents muscle tightness and joint problems
Improves blood flow and nutrient delivery to spinal tissues
Enhances balance and reduces fall risk
Supports better sleep and less daily discomfort
Studies and experts note that these habits promote long-term health and vitality (Illinoisspinalcare.com, n.d.; Spinehealth.org, n.d.).
How Chiropractic Care Fits In
Chiropractic care plays a key role in spinal hygiene. Chiropractors use gentle adjustments to fix misalignments, called subluxations, that can stress the spine and nerves. These adjustments restore proper movement, reduce pain, and improve function. Regular chiropractic visits act as preventive maintenance, catching small issues before they grow.
Many people combine chiropractic with other habits for the best results. Adjustments improve alignment, while daily posture and exercise help maintain gains. This approach helps address common complaints such as neck or low back pain and supports recovery from injuries (Illinoisspinalcare.com, n.d.; Eastportlandchiropractor.com, n.d.).
The Power of Integrative Care with Chiropractors and Nurse Practitioners
An integrative approach brings together diverse experts to achieve stronger results. Chiropractors focus on the spine’s structure, alignment, and movement through adjustments and rehab. Nurse practitioners (NPs), especially those with advanced training, address broader health needs such as nutrition, stress management, hormone balance, and lifestyle changes.
This team effort addresses both the physical spine and daily habits that affect it. For example, a chiropractor might correct alignment after an injury, while an NP guides on anti-inflammatory foods or stress reduction to aid healing. Together, they create personalized plans that work better than one alone, especially for complex pain, chronic issues, or recovery from accidents.
Dr. Alexander Jimenez, DC, APRN, FNP-BC, stands out in this field. As a Doctor of Chiropractic and board-certified Family Nurse Practitioner, he combines spinal adjustments, decompression therapy, and functional medicine. His practice emphasizes root-cause care, using nutrition, lifestyle tweaks, and advanced diagnostics for musculoskeletal problems, personal injuries, and overall wellness. Clinical observations from his work show that integrative methods restore mobility, reduce pain, and improve quality of life by treating the whole person—not just symptoms (Dralexjimenez.com, n.d.; A4m.com, n.d.).
Simple Ways to Start Spinal Hygiene Today
You can begin with easy changes that fit into daily life.
Posture checks: Set reminders to sit tall and take breaks from sitting every 30 minutes.
Daily stretches: Try cat-cow pose, child’s pose, or seated twists for 5-10 minutes.
Safe lifting: Always bend at the knees and use your legs.
Stay hydrated: Drink water throughout the day to keep your discs healthy.
Eat spine-friendly foods: Include leafy greens, fish, nuts, and dairy or alternatives for key nutrients.
Move often: Walk or do low-impact activity for at least 30 minutes most days.
Manage stress: Practice deep breathing or short meditation sessions.
Adding regular chiropractic check-ups can help monitor and maintain progress (Lifemovesmt.com, n.d.; Newlifefamilychiropractic.net, n.d.).
Final Thoughts
Spinal hygiene is a smart, everyday way to protect one of your body’s most important parts. By focusing on posture, movement, nutrition, and professional care when needed, you support a strong spine, healthy nerves, and a better quality of life. Small habits add up to big benefits, helping you stay active and pain-free for years.
A physiotherapist works on a patient’s foot as part of their neuropathy treatment in the clinic
A Local, Integrative Approach from El Paso Back Clinic
Peripheral neuropathy is a common concern for many people in El Paso. Questions usually center on why symptoms are happening, how diabetes and spine health are connected, and what can be done beyond medication. At El Paso Back Clinic, care focuses on non-invasive, whole-person strategies that improve nerve function, movement, and daily quality of life.
This article answers the most common local questions in clear language and explains how integrative chiropractic care—coordinated with nurse practitioner (NP) oversight—addresses neuropathy by treating both symptoms and root causes. Clinical insights reflect the experience of Dr. Alexander Jimenez, DC, APRN, FNP-BC.
What Is Peripheral Neuropathy?
Peripheral neuropathy happens when nerves outside the brain and spinal cord are damaged or irritated. These nerves help you feel sensation, move muscles, and regulate automatic body functions like sweating and digestion. When nerve signals are disrupted, symptoms can feel burning, sharp, numb, or electric (West Texas Pain Institute, n.d.; Frontier Neurology, n.d.).
Most Common Neuropathy Symptoms We See in El Paso
People in El Paso often describe similar patterns:
Burning or throbbing pain (especially at night)
Tingling or “pins and needles”
Numbness in the feet or hands
Electric or shooting pain
Muscle weakness or cramping
Balance problems or frequent trips
Sensitivity to touch
In more advanced cases, symptoms can involve digestion, bladder control, or sweating (Frontier Neurology, n.d.).
Why Neuropathy Is So Common in This Region
A major driver locally is diabetes and prediabetes. High blood sugar can injure small blood vessels that feed nerves, leading to poor nerve signaling over time.
Other contributors include:
Spine and posture problems that stress nerve roots
Vitamin deficiencies (especially B vitamins)
Circulation issues
Prior injuries or repetitive strain
Certain medications or alcohol overuse
Inflammatory or autoimmune conditions
Many patients have multiple contributing factors, which is why a full evaluation is important (Medicos Family Clinic, n.d.; West Texas Pain Institute, 2023).
How Diabetic Neuropathy Affects Daily Life
Diabetic neuropathy often begins in the feet and slowly progresses upward. Common concerns include:
Burning feet at night
Loss of protective sensation
Higher risk of cuts, sores, and ulcers
Changes in walking or posture
Increased fall risk
Early integrative care can slow progression and reduce complications (El Paso Feet, n.d.; iVascular Center, n.d.).
How Neuropathy Is Evaluated at El Paso Back Clinic
Diagnosis is not based solely on symptoms. A complete assessment looks at the whole person.
Evaluation commonly includes:
Detailed health and symptom history
Review of blood sugar control and medications
Neurological and sensory testing
Posture and movement analysis
Spinal and joint evaluation
Imaging when nerve compression is suspected
Dr. Jimenez emphasizes that neuropathy symptoms often overlap with spinal nerve irritation or biomechanical stress, making dual-scope evaluation especially valuable (Jimenez, n.d.-a; Nonsurgical Spine Center, n.d.).
Can Neuropathy Improve Without Surgery?
For many people, yes. Most patients want conservative options before considering surgery or long-term medication use.
Non-surgical strategies may include:
Chiropractic care
Targeted exercise and physical therapy
Lifestyle and nutrition guidance
Laser therapy
Nerve stimulation techniques
Footwear and balance support
Stress and sleep optimization
Combining approaches is often more effective than relying on just one method (P3 Physical Therapy, n.d.; El Paso Feet, n.d.).
How Chiropractic Care Supports Nerve Health
Chiropractic care focuses on restoring healthy movement in the spine and joints, thereby reducing stress on nerves.
At El Paso Back Clinic, care may include:
Gentle spinal adjustments
Joint mobilization
Postural correction
Nerve decompression strategies
Soft tissue techniques
Guided movement and mobility work
Clinical observations show that improving spinal mechanics can enhance nerve signaling and reduce irritation—especially when neuropathy overlaps with back or neck problems (Jimenez, n.d.-b; El Paso Back Clinic, n.d.).
The Role of Nurse Practitioners in Neuropathy Care
Nurse practitioners (NPs) are essential for addressing medical and metabolic contributors to nerve damage.
NP-guided support may involve:
Lab testing and result interpretation
Diabetes and metabolic management
Identifying vitamin or nutrient deficiencies
Reviewing medication side effects
Monitoring nerve-related complications
Dr. Jimenez’s dual licensure allows structural findings and medical factors to be evaluated together, helping patients understand why symptoms are happening—not just where they hurt (Jimenez, n.d.-c).
Why an Integrative Approach Works Best
Neuropathy rarely has a single cause. Integrative care addresses multiple systems at once.
Benefits include:
More accurate diagnosis
Personalized care plans
Reduced dependence on pain medications
Improved balance, strength, and confidence
Better long-term nerve health
This approach is especially helpful for people with diabetes, chronic back pain, or long-standing symptoms (HealthCoach Clinic, n.d.; Pain and Wellness Institute, n.d.).
Physical Therapy and Movement for Nerve Recovery
Physical therapy complements chiropractic care by retraining safe movement and improving circulation.
Physical therapy may help by:
Strengthening supportive muscles
Improving balance and coordination
Reducing fall risk
Teaching nerve-friendly movement patterns
When coordinated with chiropractic and NP care, recovery is often faster and more sustainable (P3 Physical Therapy, n.d.).
Lifestyle Habits That Matter for Neuropathy
Daily habits can either protect or irritate nerves.
Helpful habits include:
Keeping blood sugar stable
Wearing supportive footwear
Limiting alcohol and avoiding smoking
Staying physically active
Managing stress
Prioritizing sleep
Small, consistent changes can reduce flare-ups and improve comfort over time (Modern Pain Houston, n.d.; Dr. Dennis Harris, n.d.).
Emotional and Community Support
Living with nerve pain can affect mood and sleep. Support makes a difference.
Education and coaching
Stress-management strategies
Peer or virtual support groups
Family involvement in care plans
Support resources help patients feel informed and empowered (Foundation for Peripheral Neuropathy, n.d.).
When to Seek Professional Help
Consider an evaluation if you notice:
Persistent tingling or numbness
Burning or electric pain
Muscle weakness
Balance problems or frequent falls
Foot wounds that heal slowly
Early care can help prevent progression and complications (West Texas Pain Institute, n.d.; Frontier Neurology, n.d.).
The El Paso Back Clinic Difference
At El Paso Back Clinic, neuropathy care is centered on conservative, patient-focused solutions. By combining chiropractic care with nurse practitioner oversight and lifestyle strategies, patients receive practical, non-invasive options designed to improve nerve function and daily life.
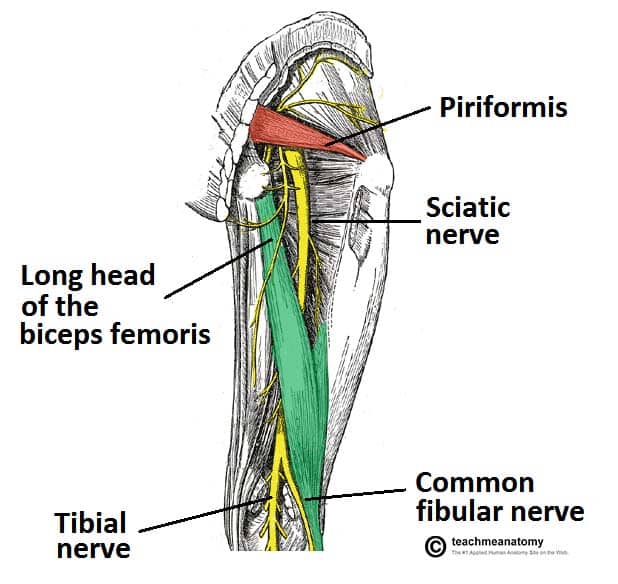
Innovations in Sciatica Treatment in 2026: A Shift Toward Targeted, Minimally Invasive, and Integrative Care
Sciatica is one of the most common causes of chronic lower back and leg pain. It occurs when the sciatic nerve—the longest nerve in the body—is irritated or compressed, often due to disc herniation, spinal degeneration, inflammation, or biomechanical imbalance. For years, treatment options focused mainly on pain medications, steroid injections, or surgery when symptoms became severe.
In 2026, sciatica care has entered a new phase. Treatment is no longer just about “blocking pain.” Instead, the focus is on precision diagnosis, nerve healing, inflammation reduction, and functional recovery, with fewer complications and faster healing times. These advances also emphasize integrated, interdisciplinary care, combining chiropractic treatment with the diagnostic and clinical oversight of nurse practitioners (NPs).
This article explains the most important innovations shaping sciatica treatment in 2026, using easy-to-understand language while staying grounded in current clinical research and real-world outcomes.
Understanding Sciatica: Why Better Solutions Were Needed
Sciatica is not a single disease. It is a symptom caused by pressure or irritation along the sciatic nerve, usually beginning in the lower spine and traveling into the buttock and leg. Pain can feel sharp, burning, electric, or aching and may include numbness or weakness.
Common contributors include:
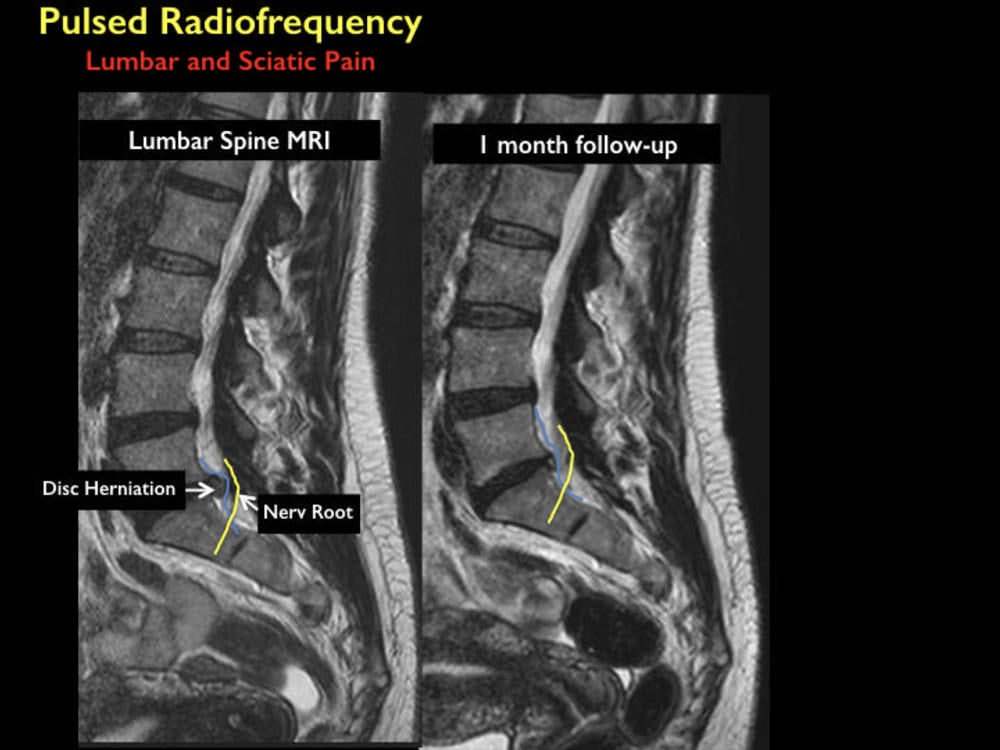
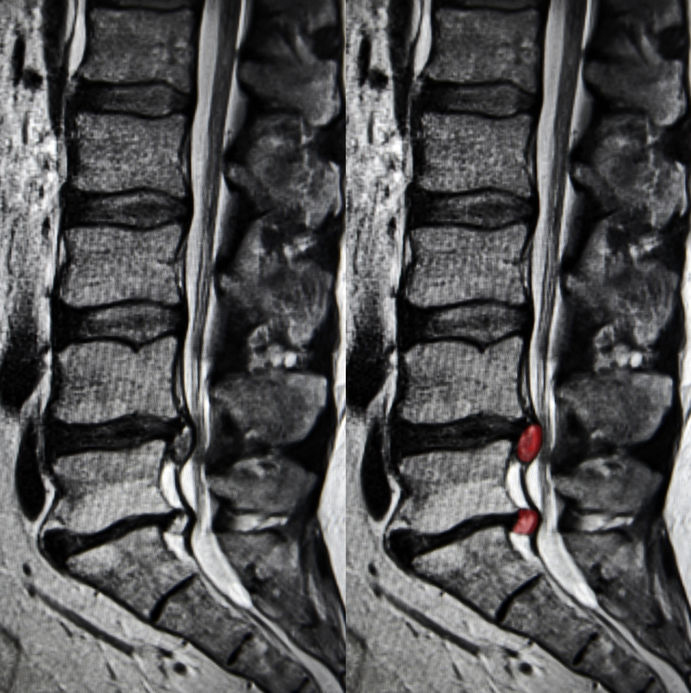
Herniated or bulging lumbar discs
Spinal stenosis
Degenerative disc disease
Muscle imbalance or pelvic instability
Inflammation around nerve roots
Traditional treatments often relied on:
Long-term anti-inflammatory or pain medications
Opioids for severe cases
Epidural steroid injections
Surgery as a last resort
While these approaches helped some patients, they did not always address the underlying cause, and many carried risks such as dependency, complications, or prolonged recovery (Stanford Health Care, n.d.).
What Has Changed in 2026?
By 2026, sciatica treatment emphasizes early, targeted, and minimally invasive care. Research and clinical experience now show that addressing nerve irritation early and restoring healthy movement patterns can prevent chronic pain and disability (BioSpace, 2025).
Key changes include:
Improved imaging and diagnostics
Precision-guided nerve procedures
Regenerative medicine options
Advanced neuromodulation technologies
Integrated chiropractic and NP-led care models
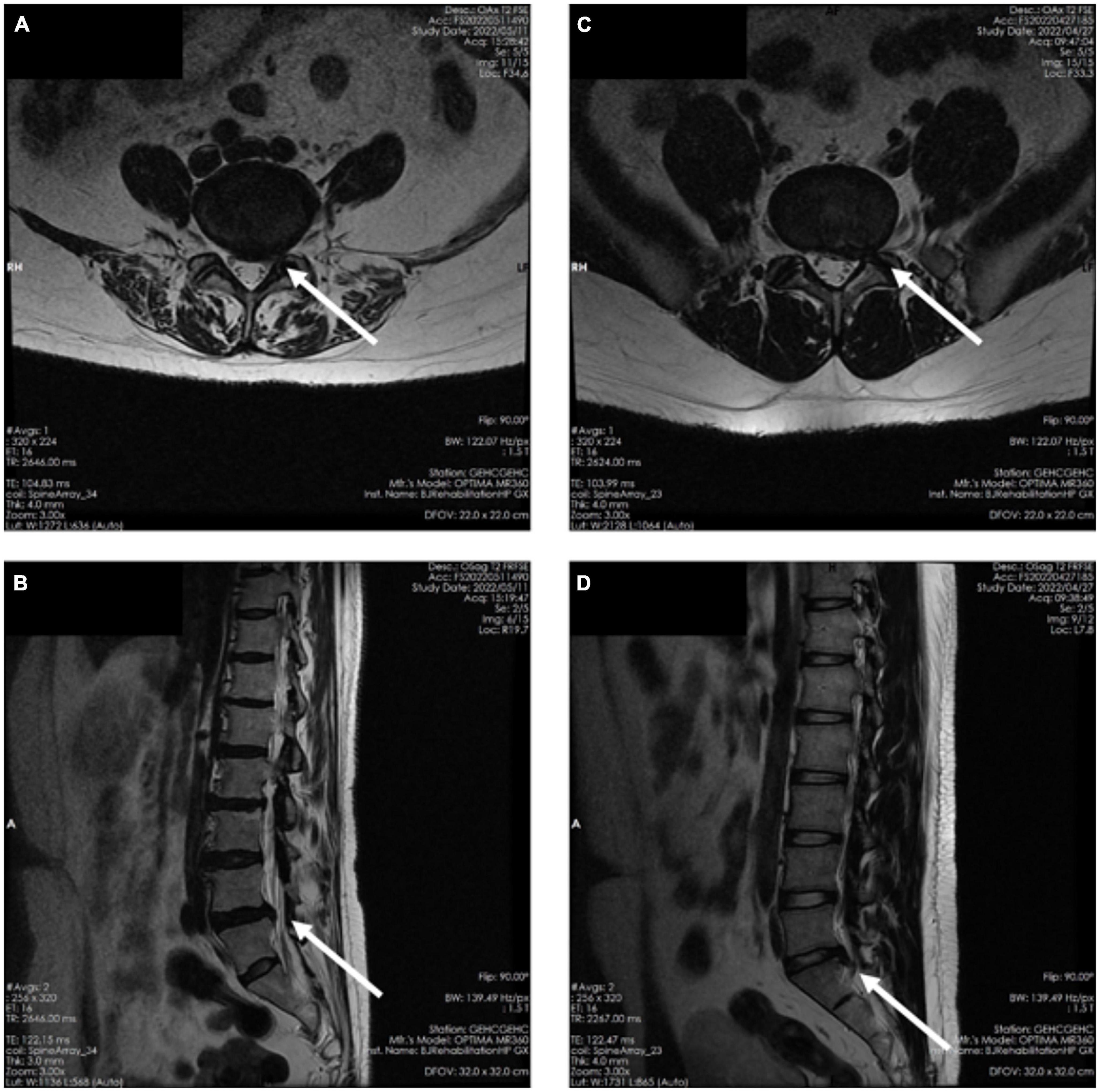
Advanced Diagnostic Imaging: Seeing the True Source of Pain
One of the biggest improvements in sciatica care is high-resolution MRI technology. Modern imaging allows clinicians to:
Identify the exact nerve root involvement
Distinguish disc-related pain from muscular or inflammatory causes
Detect subtle nerve inflammation missed in earlier imaging methods
Enhanced MRI protocols now guide treatment decisions more accurately, reducing unnecessary procedures and improving outcomes (Stanford Health Care, n.d.).
Nurse practitioners play a critical role here by:
Ordering and interpreting imaging
Correlating findings with physical symptoms
Coordinating referrals and follow-up care
Minimally Invasive Pain Procedures: Precision Without Surgery
Improved Nerve Blocks
Modern nerve blocks are no longer “blind injections.” In 2026, they are image-guided and highly targeted, delivering medication exactly where inflammation and irritation occur.
Benefits include:
Faster pain relief
Reduced medication dosage
Improved diagnostic clarity
Lower complication risk
Nerve blocks are now often used as diagnostic tools to help clinicians determine whether pain is mechanical, inflammatory, or neuropathic in origin (Apollo Spine & Pain, 2026a).
Radiofrequency Ablation (RFA)
Radiofrequency ablation uses controlled heat to disrupt pain signals traveling through irritated nerves. Newer RFA systems are more precise and selective than earlier versions.
Key advantages:
Long-lasting pain relief
Minimal tissue damage
Short recovery time
Reduced reliance on medications
RFA is especially helpful for chronic sciatica that does not respond to conservative care (Apollo Spine & Pain, 2026b).
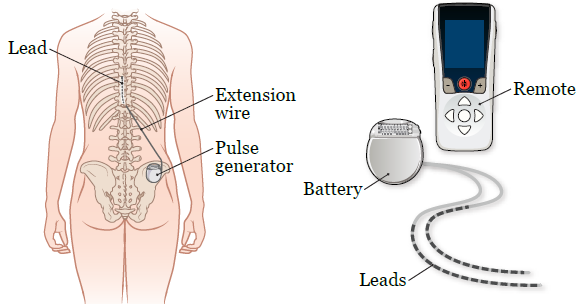
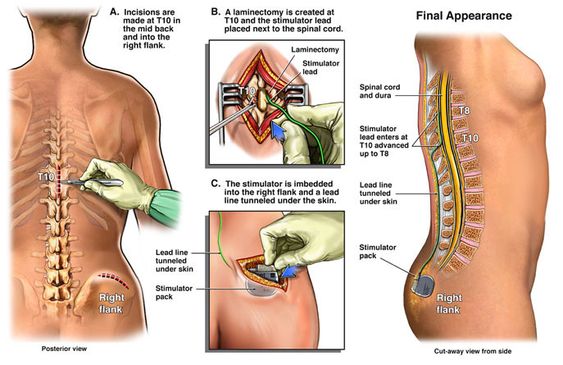
Spinal Cord Stimulation: Rewiring Pain Perception
Spinal cord stimulation (SCS) has evolved significantly. New devices are smaller, smarter, and more adaptive. They deliver gentle electrical signals that change how the brain interprets pain signals from the sciatic nerve.
Modern SCS systems offer:
Personalized stimulation patterns
Adjustable settings via external controllers
Reduced side effects compared to older models
SCS is now used earlier in care for select patients, helping many avoid surgery altogether (Pain and Spine Specialists, n.d.).
Regenerative Medicine: Supporting Nerve Healing
Platelet-Rich Plasma (PRP)
PRP therapy uses a patient’s own blood components to promote healing and reduce inflammation. In sciatica care, PRP is increasingly used around:
Inflamed nerve roots
Degenerative disc structures
Surrounding soft tissues
Research suggests PRP may:
Reduce inflammation
Support tissue repair
Improve long-term outcomes
While still evolving, regenerative therapies are driving growth in the global sciatica treatment market (Grand View Research, n.d.; PMC, 2024).
Therapeutic Exercise Innovations: Movement as Medicine
Nerve Flossing and Targeted Rehab
Exercise therapy in 2026 is more specific and personalized. One standout approach is nerve flossing, which involves controlled movements designed to improve nerve mobility and reduce irritation.
Benefits include:
Improved nerve glide
Reduced stiffness
Decreased pain during daily activities
Programs are now customized using imaging findings and functional testing, ensuring exercises match the patient’s specific condition (Goodman Campbell, 2026).
Chiropractic Care: A Drug-Free Foundation
Chiropractic care remains central to non-surgical sciatica treatment. Modern chiropractic approaches focus on restoring spinal alignment, reducing nerve compression, and improving movement patterns.
Common techniques include:
Spinal adjustments
Flexion-distraction therapy
Soft tissue mobilization
Low-level laser therapy
Research continues to associate chiropractic care with reduced opioid use and improved pain outcomes (ReachMD, 2024; UH Hospitals, 2025).
Integrated Care: Chiropractors and Nurse Practitioners Working Together
One of the most important shifts in 2026 is the collaborative care model. Instead of isolated treatment, patients benefit from coordinated care involving chiropractors and nurse practitioners.
This model allows for:
Accurate diagnosis and imaging oversight
Conservative, drug-free pain management
Monitoring of neurological symptoms
Reduced opioid exposure
Clinical observations from Dr. Alexander Jimenez, DC, APRN, FNP-BC, highlight that patients receiving coordinated chiropractic and NP care often experience:
Faster recovery
Better functional improvement
Fewer invasive interventions
Greater long-term pain control
His integrative approach emphasizes treating the cause of nerve irritation, not just the symptoms (Jimenez, n.d.).
Why These Innovations Matter
Together, these advances represent a major shift in sciatica care:
From surgery-first to conservative-first
From symptom masking to root-cause resolution
From isolated care to interdisciplinary teamwork
Patients now have more options, fewer risks, and better long-term outcomes.
Conclusion: The Future of Sciatica Care Is Personalized and Precise
By 2026, sciatica treatment has become more effective, safer, and patient-centered. Innovations in diagnostics, minimally invasive procedures, regenerative medicine, and integrative chiropractic-NP–NP care are reducing the need for surgery and long-term medication use.
The focus is no longer just pain relief—it is nerve health, mobility restoration, and sustainable recovery. As research and technology continue to evolve, patients suffering from sciatica can expect even more targeted, evidence-based solutions in the years ahead.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine