Everyone has dealt with acute or chronic pain at some point in their lives. The body’s response tells many of us where the pain is located and can leave the body sore as the immune system begins to heal the affected area. When disorders like autoimmune diseases start to attack the body for no reason, then that is when chronic issues and disorders begin to overlap in risk profiles on other various problems that affect both the muscles and organs. Autoimmune diseases like fibromyalgia can affect a person’s body; however, they could be associated with different issues affecting the body. Today’s article looks at fibromyalgia, how it affects the musculoskeletal system, and how chiropractic care helps manage fibromyalgia in the body. We refer patients to certified providers specializing in musculoskeletal treatments to help those with fibromyalgia. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Fibromyalgia?
Have you experienced excruciating pain that is spread all over your body? Do you have trouble sleeping and feel exhausted every day? Do you experience brain fog or other cognitive disturbances? Many of these issues are signs and conditions of fibromyalgia. Fibromyalgia is defined as a chronic condition that is characterized by widespread musculoskeletal pain. Symptoms like fatigue, cognitive disturbances, and multiple somatic symptoms often overlap and accompany this disorder. Around two to eight percent of the world population suffers from fibromyalgia, and it affects women more than men. Sadly though, fibromyalgia is a challenge to diagnose, and the pain can last several months to years. Some of the main symptoms that fibromyalgia does to the body include:
Muscle and joint stiffness
General sensitivity
Insomnia
Cognitive dysfunction
Mood disorders
Fibromyalgia could also potentially be associated with specific diseases like diabetes, lupus, rheumatic diseases, and musculoskeletal disorders.
How Does It Affect The Musculoskeletal System?
The musculoskeletal system in the body has three muscle groups: skeletal, cardiac, and smooth muscles that provide different functions correlating how the body moves. Individuals with fibromyalgia will experience amplified painful sensations affecting their brain and spinal cord to process pain and nonpainful signals potentially associated with musculoskeletal disorders. The neural structures from the brain become hyper-reactive to any soft tissues close to the spine, known as segmental facilitation. These changes that occur to the soft tissues are called trigger points, and if situated in the muscles, they are referred to as “myofascial” trigger points. Studies reveal that the pathophysiology of musculoskeletal dysfunction can be considered secondary to central abnormalities of pain modulation associated with fibromyalgia.
An Overview Of Fibromyalgia-Video
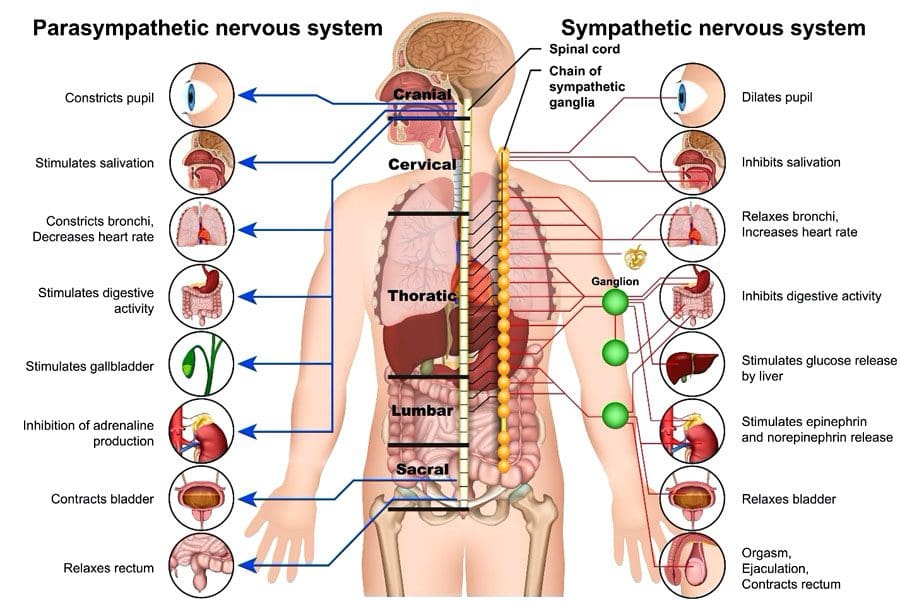
Have you been experiencing excruciating pain in different areas of your body? Have you been constantly tired throughout the entire day? Or has your mood been dampened all of a sudden? These are the signs that you have fibromyalgia, and the video above gives an overview of what fibromyalgia is. Fibromyalgia is defined as a chronic disorder that is difficult to diagnose. Studies reveal that fibromyalgia is possible to be described as a cognitive disorder that triggers painful amplifications and sensory nociceptors that become hypersensitive. So what does this mean, and how is the nervous system affected by fibromyalgia? The nervous system has the central and peripheral systems. The peripheral system has a component known as the autonomic nervous system that regulates involuntary bodily functions. The autonomic system consists of two subsystems: the sympathetic and parasympathetic systems. For individuals with fibromyalgia, the sympathetic nervous system, which provides the “fight or flight” response, is constantly active, causing the parasympathetic nervous system, which provides the “rest and digest” response, to be inactive in the body. The good news is that individuals with fibromyalgia and its associated symptoms can find relief through treatment.
Chiropractic Care & Fibromyalgia
Even though there hasn’t been a cure for fibromyalgia yet, treatments are available to manage and improve the symptoms associated with fibromyalgia with chiropractic care. Chiropractic care can help relieve fibromyalgia pain by carefully correcting spinal misalignments or subluxations through spinal adjustments and manual manipulations of the body. Studies reveal that the effectiveness of chiropractic care for fibromyalgia patients helps improve their range of motion to the cervical and lumbar areas of the spine. Chiropractic care can help improve their flexibility, decrease their pain levels, and have better sleep quality. People diagnosed with fibromyalgia need to understand that many options for pain management don’t rely on medicines. Chiropractic care is gentle and non-invasive. It can be helpful for individuals that want to take control of their circumstances and have chiropractic therapy as a vital part of managing their well-being.
Conclusion
Fibromyalgia is a chronic disorder that affects the musculoskeletal system by causing stiffness in the muscles and joints, general sensitivity, and other chronic issues associated with this disorder. Individuals with fibromyalgia will describe their pain as unbearable due to the nerves in the sympathetic system being hyperactive and tender to the touch. Fortunately, treatments like chiropractic care can help relieve fibromyalgia pain through spinal adjustments and manual manipulations. Chiropractic care for individuals with fibromyalgia can help improve their range of motion and flexibility and decrease their pain levels without using medicines. Incorporating chiropractic care as a treatment for fibromyalgia can be vital in managing a person’s well-being.
References
Bhargava, Juhi, and John A Hurley. “Fibromyalgia – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 1 May 2022, https://www.ncbi.nlm.nih.gov/books/NBK540974/.
Blunt, K L, et al. “The Effectiveness of Chiropractic Management of Fibromyalgia Patients: A Pilot Study.” Journal of Manipulative and Physiological Therapeutics, U.S. National Library of Medicine, 1997, https://pubmed.ncbi.nlm.nih.gov/9272472/.
Geel, S E. “The Fibromyalgia Syndrome: Musculoskeletal Pathophysiology.” Seminars in Arthritis and Rheumatism, U.S. National Library of Medicine, Apr. 1994, https://pubmed.ncbi.nlm.nih.gov/8036524/.
Maugars, Yves, et al. “Fibromyalgia and Associated Disorders: From Pain to Chronic Suffering, from Subjective Hypersensitivity to Hypersensitivity Syndrome.” Frontiers, Frontiers, 1 July 2021, https://www.frontiersin.org/articles/10.3389/fmed.2021.666914/full.
Siracusa, Rosalba, et al. “Fibromyalgia: Pathogenesis, Mechanisms, Diagnosis and Treatment Options Update.” International Journal of Molecular Sciences, MDPI, 9 Apr. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8068842/.
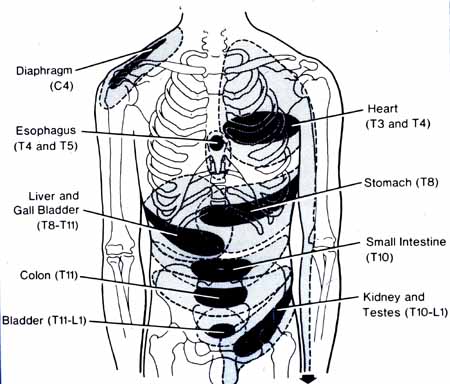
Experiencing low back pain and diarrhea can be a symptom of a viscerosomatic reflex,somatovisceral reflex, or a combination. A reflex is an involuntary response to nervous system stimulation. A doctor tapping below the knee causes the foot to kick forward is a basic example of a reflex. This is a somatovisceral or body organ reflex. Back pain could be from awkward posture, repetitive motions like bending or twisting, or injury that affects the spinal column. The effects could cause nerve compression and damage that can cause firing misinterpreted signals impacting/damaging internal organ function, causing pain and other symptoms.
However, the damage caused to the compressed/injured organ nerves can also cause back pain symptoms. This is a viscerosomatic or organ body reflex. One study found that a group of chiropractic patients dealing with low back pain also had increased bowel problems, even though there was no specific cause, link, or association between the two. Lower back pain and diarrhea may be completely unrelated, but if symptoms are recurring, there is an increased chance of an underlying medical issue.
Chiropractic Medicine
Chiropractic medicine is founded on the nervous system’s control of the body’s organ systems, whose impulse signals travel through the spinal cord. Body systems include the muscles, bones, and all organs. Any problems with the spine and/or nerve changes from normal wear and tear, injury, or infection can affect signal transmissions that can alter system functions. Altered nerve conduction can impact overall health and is referred to as reflex pathways in the nervous system. A somatovisceral reflex is where the musculoskeletal system causes altered nerve conduction creating organ system dysfunction and/or illness. Diarrhea brought on by back pain is an example.
Causes Of Back Pain and Diarrhea
Appendicitis
The appendix extends from the colon in the lower right abdomen. Appendicitis is inflammation of the appendix. The pain usually appears near the belly button and spreads to the right side of the stomach. Some individuals’ appendix extends behind the colon, which can also cause low back pain. Symptoms include:
Loss of appetite
Inability to relieve gas
Constipation
Abdominal pain – Moderate to severe
Diarrhea
Fever
Nausea
Vomiting
Appendicitis can be life-threatening and requires immediate treatment; if left untreated, the condition can worsen within hours, causing a rupture that can leak through the abdominal cavity.
Fecal impaction
Fecal impaction is stools that have become hard, dry, and stuck in the rectum and can cause abdominal and low back pressure and pain. It is commonly caused by chronic constipation, which can be associated with dehydration, lack of fiber, physical inactivity, medication side effects, or long-term use of laxatives. Taking laxatives for a long time can cause the intestines to shut off automatic evacuation of the bowels. Although the condition is common in older individuals, it can happen to individuals of any age who experience chronic constipation. Symptoms can include:
Bloating
Cramping
Bladder pressure
Bladder incontinence
Leakage or sudden diarrhea after long-term constipation.
Rectal bleeding
Enteropathic arthritis
Enteropathic arthritis is a chronic inflammatory arthritis associated with inflammatory bowel disease or IBD. Types include:
Ulcerative colitis
Crohn’s disease
Different arthritic diseases like ankylosing spondylitis and psoriatic arthritis can cause symptoms like diarrhea and abdominal pain or be associated with developing inflammatory bowel disease. Varying symptoms depend on the bowel disease and arthritis type and include:
Fatigue
Cramping
Joint pain
Joint stiffness
Loss of appetite
Bloody diarrhea
Pancreatic Cancer
The symptoms of pancreatic cancer vary depending on the type, location, and cancer stage. Pancreatic cancers in the early stages usually don’t cause signs or symptoms. Possible symptoms can include:
Chiropractic is ideal for addressing reflex issues. A doctor of chiropractic adjusts the spine to improve alignment, joint motion, and nerve energy transmission, improving nerve circulation/signal flow, which can help with unrelated health conditions. A chiropractor will locate any areas of spinal misalignment; once identified, a personalized treatment plan will return the correct alignment to the spine, enabling the nervous system to return to optimal function.
Sengupta, Jyoti N. “Visceral pain: the neurophysiological mechanism.” Handbook of experimental pharmacology,194 (2009): 31-74. doi:10.1007/978-3-540-79090-7_2
Walden, Anna L et al. “Bladder and bowel symptoms among adults presenting with low back pain to an academic chiropractic clinic: results of a preliminary study.” Journal of chiropractic medicine vol. 13,3 (2014): 178-87. doi:10.1016/j.jcm.2014.07.006
Wood, Jackie D. “Neuropathophysiology of functional gastrointestinal disorders.” World journal of gastroenterology vol. 13,9 (2007): 1313-32. doi:10.3748/wjg.v13.i9.1313
When the weather becomes hot, and everyone begins to plan fun activities to enjoy, one of the many activities that come to mind is hanging out in the pool. Swimming is an excellent way to combat the summer heat, but it can provide much more for the body. For athletes, it provides another form of cardio exercise to improve their quality performance when they are competing. While for individuals looking for an affordable exercise regimeor just some fun activity to do, swimming can become a form of therapy and be beneficial for them if they were previously injured. Today’s article looks at how swimming causes an impact on the musculoskeletal system, its beneficial properties to the heart, and how aqua therapy combined with chiropractic care helps optimize full-body health. We refer patients to certified providers specializing in musculoskeletal treatments and hydrotherapy to help those with musculoskeletal disorders. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Swimming & Its Impact On The Musculoskeletal System
Water exercises or swimming can benefit those looking for different cardio exercises to build muscle endurance or have a clear sense of mind. Swimming is fantastic for all body sizes, and when it is done correctly, it can be highly recognized as a form of rehabilitation and injury recovery known as aquatic therapy. Research studies reveal that aquatic treatments and exercises can significantly reduce pain in individuals that suffer from low back pain while increasing physical function. Some of the impacts that swimming/aquatic therapy provides on the musculoskeletal system include:
Builds muscle strength
Improves endurance
Stabilizes joints
Improves poor posture
Swimming/ hydrotherapy is an excellent low-impact exercise that is easy on the back and spine, especially for individuals suffering from low back pain or spinal misalignments. Studies reveal that the efficacy of aquatic activities helps strengthen the abdominals and legs and stretch the back while managing musculoskeletal issues.
When individuals suffer from back pain associated with chronic issues can become concerning for the vital organs that have a causal relationship with the muscle as they are affected as well. When spinal joints and muscles begin to suffer from abnormal weight increases, the muscles and ligaments become misaligned. Misalignment or subluxation is defined as spinal vertebrates that are out of place and cause pressure on the surrounding nerves exiting the spinal cord. These spinal issues then become a risk of developing musculoskeletal disorders in the body. Unlike many aerobic exercises like running or cycling that may be hard on the spine, swimming has little to no impact on the spinal structures. So when individuals begin to take up swimming, they realize that the water buoyancy helps support their body weight while relieving stress on all joints and decompressing the spine. This gives the individual a greater range of motion, while the water gives off a sense of purification as it helps the body relax. Hence, hydrotherapy helps relax people who suffer from obesity or muscle injuries associated with muscle and joint pain as the water provides gentle resistance while relaxing the muscles to promote longer exercise sessions.
The Benefits Of Swimming For The Heart
Swimming or any form of water aerobics is not only beneficial to the musculoskeletal system but can help improve cardiac function in the heart and even the lungs. Studies reveal that swimming is an effective option for maintaining and enhancing cardiovascular fitness. Some of the benefits swimming provides for the cardiovascular system include:
Lowers blood pressure
Improve circulation
Reduces heart rate
But how does swimming improve cardiovascular function in the body? Individuals submerge themselves underwater; they hold their breath until the air is needed. Being submerged underwater may help lung capacity while gaining control of how a person breathes. Breathing exercises associated with aqua therapy help promote stronger lungs and heart while increasing their capacity for blood and airflow to the heart and lungs. Say, for example, a person is having trouble breathing due to restrictive blood and air flow associated with cardiopulmonary issues, which potentially be involved in experiencing an asthma attack associated with obesity.
The Benefits Of Swimming-Video
Have you wanted to try a different form of cardio exercise? Have you been experiencing a limited range of motion in your arms, shoulders, back, and neck? Do you feel tightness across your chest? The video above gives an overview explanation of the health benefits of swimming. Swimming or aquatic therapy allows the individual experiencing chronic pain issues to do cardio activities without increasing or worsening pain, which is very therapeutic for the body. Many people are either training for an athletic event or finding a leisure activity that will benefit them in the long run. Swimming is considered an important factor in a person’s quality of life as it helps them become motivated to make small changes to better their health. Additionally, regular cardiovascular exercises/activities like swimming benefit pain reduction in a therapeutic sense. When individuals are trying to figure out and determine the proper training or therapy that can help alleviate their specific ailments, their goal is to see how those exercises should be done in a certain amount of time without causing fatigue or increased pain as the primary objective.
Aqua Therapy & Chiropractic Care
When looking for the proper exercise regime or treatment for pain issues, it can be challenging to see what works and doesn’t. For those with musculoskeletal disorders related to chronic issues, aqua therapy and chiropractic care go hand in hand in alleviating pain. Aqua therapy exercises can range from simple routines in shallow waters to high-tech equipment like underwater treadmills for muscle conditioning. Active water therapy exercises that are diverse in relieving musculoskeletal pain should be tailored to the person and the specific conditions that are ailing them.
But how does chiropractic care work hand in hand with aqua therapy? Well, chiropractic care and exercise have a casual relationship when it comes to treating musculoskeletal disorders. Many individuals do suffer from spinal misalignment, which becomes a risk of developing musculoskeletal issues that cause discomfort. Since many individuals associate chiropractic care with back issues, the reality shows that chiropractic care not only helps with back issues but various issues that affect the muscles, joints, and organs related to each other. An example would be an individual with low back problems who cannot do any activities for long periods while triggering gut issues. This is defined as somato-visceral pain where affected muscles associated with internal organs trigger pain. So for a chiropractor to adjust an individual dealing with back pain associated with gut or heart issues can slowly restore the person’s natural alignment by reducing the irritated nerve roots between the vertebrae and strengthening the surrounding muscles and tissues. Afterward, a chiropractor may recommend exercises like aquatic therapy to speed up the rehabilitation process, as studies reveal that physical activities are perceived to have a positive impact on health while being associated with perceived symptom reductions in musculoskeletal and injuries, as well as cardiovascular and blood conditions. Once a chiropractic regimen and exercise routine are in place, injury prevention kicks in, keeping the individual moving pain-free.
Conclusion
Whether it is having fun in the sun or finding a new exercise, swimming is not only for just playing but can be therapeutic for individuals dealing with chronic issues. Any aquatic exercise provides little to no impact on the body as it helps strengthen the musculoskeletal and cardiovascular systems with gentle force. Combined with chiropractic care, many individuals that are dealing with musculoskeletal issues associated with chronic organ issues will begin to become motivated to better themselves in the long run.
References
Ariyoshi, Mamoru, et al. “Efficacy of Aquatic Exercises for Patients with Low-Back Pain.” The Kurume Medical Journal, Kurume University School of Medicine, 11 Aug. 2009, https://www.jstage.jst.go.jp/article/kurumemedj1954/46/2/46_2_91/_article.
Lazar, Jason M, et al. “Swimming and the Heart.” International Journal of Cardiology, U.S. National Library of Medicine, 18 Apr. 2013, https://pubmed.ncbi.nlm.nih.gov/23602872/.
Massey, Heather, et al. “Perceived Impact of Outdoor Swimming on Health: Web-Based Survey.” Interactive Journal of Medical Research, JMIR Publications, 4 Jan. 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8767464/.
Shi, Zhongju, et al. “Aquatic Exercises in the Treatment of Low Back Pain: A Systematic Review of the Literature and Meta-Analysis of Eight Studies.” American Journal of Physical Medicine & Rehabilitation, U.S. National Library of Medicine, Feb. 2018, https://pubmed.ncbi.nlm.nih.gov/28759476/.
Everyone wants to be healthier at some point in their lives. Some individuals train to be athletes and must follow procedures to maintain their health. In comparison, others want to get healthier by eating the right food, exercising for at least 30 minutes to an hour, meditating or doing yoga to relieve stress, and maintaining a healthy weight. However, many environmental factors do affect the human body. They can alter how a person looks, weight, levels of physical activity, and how different foods affect the body’s metabolism. When environmental factors start to take hold of a person’s health, it can trigger unwanted issues that affect not only the muscles in the body but the associated internal organs that help provide the functionality to the body. Today’s article focuses on the musculoskeletal system, how different issues affect the musculoskeletal system and associate with other problems in the body, and various treatments to improve musculoskeletal health. We refer patients to certified providers specializing in musculoskeletal therapies that help those with musculoskeletal disorders. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
The Musculoskeletal System & Its Function
How does the musculoskeletal system play its role in the human body? The body is considered a complex being that consists of various organs, muscles, tissues, ligaments, and joints that help move a person from one place to another, resting while needed, and doing multiple activities in a casual relationship. Studies reveal that the musculoskeletal system is controlled by the central nervous system that interconnects the motor-sensory function for the body’s ability to move and rest.
The three main muscle groups that make up the musculoskeletal system are:
Skeletal muscle- Muscle tendons that are connected to the bones
Cardiac muscle- Muscles associated with the heart
Smooth muscle- Muscles that line with blood vessels and specific organs (ex. intestines)
Each muscle group provides different functions that correlate to how the body moves. Skeletal muscles make the legs and arms move. Cardiac muscles help the heart pump blood to the various muscles, organs, and tissues. Smooth muscles help specific organs (intestines, stomach, and urinary tract) digest, collect nutrients, and eliminate toxins in the body.
Issues That Affect The Musculoskeletal System
These factors are related to different issues that can not only disrupt the musculoskeletal system but can be an overlap of profiles affecting the cardiovascular system, spinal health, and gut system. The different factors that are associated with the musculoskeletal system are:
Obesity
Lack of physical activity
Poor Posture
Inflammation
Unhealthy Diet
How would various factors implicate musculoskeletal issues while triggering different bodily problems? Well, let’s use obesity as an example. Obesity is associated with issues like back and joint pain as studies reveal that these musculoskeletal issues make up pain and disability as a dominant source. A poor diet of processed foods high in fats and sugars can be associated with the risk of developing obesity.
Not only that, but obesity could potentially be involved in the thoracic spine and upper back pain due to the result of physical inactivity and poor dieting. The weight on the body can strain the muscles and ligaments in the back, causing the spinal vertebrae to become misaligned and pressure the nerves exiting the spinal cord. The misalignment of the vertebrae is called a subluxation. When a person is suffering from upper back pain, it can overlap with chest pain, which can be a concerning issue to vital organs like the heart, which potentially involved in the risk of cardiovascular disease. It is related to subluxation that may affect the heart contraction rate, rhythm, and power through the sympathetic efferent pathways originating from the thoracic region.
An Overview Of The Musculoskeletal System-Video
Are you experiencing pain in your upper back or chest? How about cardiac issues associated with shouldering and arming pain? Many of these issues are related to factors that affect the musculoskeletal system that might potentially be involved with chronic issues. The video above summarizes the musculoskeletal system’s role in the body. When environmental factors become a risk of developing musculoskeletal disorders that can potentially be involved in different bodily problems, studies reveal that musculoskeletal disorders associated with abnormal functions may cause a significant impact on regular performances. An example would be a person dealing with bad hip pain and cannot do any exercises triggering heart issues. This is defined as somato-visceral pain where the affected muscle is associated with an internal organ being a pain mediator.
Treatments For Improving Musculoskeletal System
In most treatments, many individuals utilize the following to improve not only the musculoskeletal system but other issues that affect the body:
Exercise
Healthy Diet
Stress Management Treatments
Chiropractic Therapy
No matter what affliction or health problem a person is dealing with, having the best treatment solution possible is a start on a person’s health and wellness journey. The first step is to have a precise diagnosis to the doctor while giving as much information as possible is critical. Providing them with a complete health history is an essential first step. After a manual examination of the issues causing them pain, the primary physician could refer the individual for chiropractic care to relieve issues affecting their musculoskeletal system.
Many people usually only associate chiropractic care with back problems. Still, the reality is that chiropractic therapy can be helpful for the musculoskeletal system and various issues related to the muscles and organs. A chiropractor can provide therapeutic stretches and recommend exercises to individuals to help them avoid the same problems later on. Many chiropractors offer recommendations and nutrition that individuals can utilize to help improve their condition. For the musculoskeletal system, a healthy diet may help achieve and maintain a healthy body weight while reducing the risk of chronic disease. Eating the right amount of healthy greens, fruits, beneficial carbs, and healthy fats can help reduce the risk of developing chronic issues in the body like cardiovascular diseases. However, if primary cardiac problems affect the body, it is best to seek medical attention as soon as possible.
Conclusion
The body is considered a complex being that consists of various organs, muscles, tissues, ligaments, and joints that provide various activities to the host. The musculoskeletal system has three muscle groups: skeletal, cardiac, and smooth muscles provide different functions that correlate to how the body moves. When various factors begin to cause issues to the musculoskeletal system, they can potentially be involved with pain issues that affect more than the body. Treatments like chiropractic care, a healthy diet, exercise, and stress management may be the stepping stones to alleviating various issues that are affecting the musculoskeletal system and a great start in achieving health and wellness.
References
Kennel, Peter J, et al. “Skeletal Muscle Changes in Chronic Cardiac Disease and Failure.” Comprehensive Physiology, U.S. National Library of Medicine, 20 Sept. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6752037/.
Malik, Khalid M, et al. “Musculoskeletal Disorders a Universal Source of Pain and Disability Misunderstood and Mismanaged: A Critical Analysis Based on the U.S. Model of Care.” Anesthesiology and Pain Medicine, Kowsar, 15 Dec. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6348332/.
Murphy, Andrew C, et al. “Structure, Function, and Control of the Human Musculoskeletal Network.” PLoS Biology, Public Library of Science, 18 Jan. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5773011/.
Stochkendahl, Mette J, et al. “Diagnosis and Treatment of Musculoskeletal Chest Pain: Design of a Multi-Purpose Trial.” BMC Musculoskeletal Disorders, BioMed Central, 31 Mar. 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2315652/.
The heart is a fantastic muscle in the body that allows hormones, oxygenated blood, and nutrients to travel and transport to all the muscles, tissues, and organs, providing functionality to the body. As one of the main components of the cardiovascular system, the heart works together with the lungs to help carry the deoxygenated blood to the pulmonary system to dispose of waste from the body. The human body needs the heart to stay healthy; however, factors like stress, obesity, autoimmune diseases, and unhealthy habits can affect the heart, causing cardiac issues associated with various body problems. Today’s article focuses on coronary heart disease, what are the risks associated with coronary heart disease, and ways to prevent coronary heart disease from progressively getting worse. We refer patients to certified providers specializing in cardiology treatments that help those with issues of coronary heart disease. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Coronary Heart Disease?
Have you been experiencing hypertension in your body or near your heart? How about unexplained chest pains that randomly showed up? Have you experienced pain running down your shoulders and arms? Many of these are signs that you could be experiencing coronary heart disease. Research studies have defined coronary heart disease as a common heart condition with plaque formation in the heart vessels that cuts off the supply of oxygenated blood to the heart and the rest of the body. As part of cardiovascular diseases, coronary heart disease can cause overlapping profile issues over time if it is not treated right away. Many disruptive factors can affect the heart muscle like:
Age and gender
Oxidative stress
Inflammation
Vascular immune dysfunction
Lack of physical activities
These disruptive factors can increase cardiovascular disease mortality that can affect the heart and be co-morbidities associated with different issues affecting the body. Studies reveal that the mechanisms of cardiac pain are associated with the chest and upper left arm pain. This is defined as referred pain where the sensory input from visceral organs mimics cardiac distress, and the corresponding muscles are affected. But how does this correlate to the heart muscle, and why does the chest experience pain? Visceral pain is a bit trickier to diagnose when cardiovascular disorders overlap the risk profiles associated with other issues affecting the body. For example, you could be experiencing pain in your chest and upper back, but your brain is telling you something is affecting your heart.
An Overview Of CAD-Video
Have you experienced shortness of breath? How about pain located in your chest or radiating from your shoulders and arms? Have you noticed inflammation occurring in your body? Many of these are signs and symptoms of you experiencing coronary artery disease in your body. The video above explains what coronary artery disease is and the risk factors associated with the progression of this common heart disease. Studies reveal that the risk factors can overlap in profiles that contribute to the development of coronary heart disease:
Environmental factors
Lifestyle habits
Diabetes mellitus
Obesity
Symptomatic angina
Smoking
When a person has these risk profiles overlapping different associated issues, their body becomes dysfunctional. Sometimes the symptoms affect other areas of the body, while the brain might be signaled that something is wrong with the heart. Since coronary artery disease progresses slowly over time, many individuals don’t experience the symptoms affecting their heart muscles.
Risk Issues Associated With CHD
Some of these symptoms that overlap in risk profiles may seem like heart issues but may refer to different problems affecting the body. This is defined as viscero-somatic pain, where the pain in the internal organs is associated with the corresponding muscles that share the same nerve. Chest pain associated with heart issues is a perfect example. Studies reveal that chest pains can become indistinguishable from angina, which may result from abnormalities in the thoracic viscera that overlap in profiles with heart issues. So what does it mean? It implies that sensory neurons from different visceral organs might mimic cardiac pain-causing risk-associated problems that affect the thoracic region of the spine triggering neck and upper back issues. Everything is connected as chest pains, dyspnea, and dyspepsia are intertwined with the thoracic anteriority becoming a mediator for cardiovascular diseases.
Ways To Prevent CHD
So let’s visualize a person going to their primary physician due to them experiencing heart issues associated with chest pains after the doctor goes through a manual examination on checking the individual’s heart and chest to see what problems are affecting the body. What does this implicates, and how do chest and back pains correlate with each other if there are heart issues? Studies reveal that the peripheral tissues in the body might be damaged from traumatic events that cause an inflammatory swelling in the cervical and thoracic region of the spine, causing muscle stiffness. Chiropractic care might be the answer to relieving pain and swelling triggering cervical and thoracic pain. Chiropractors use chiropractic adjustments to deliver a non-invasive, gentle treatment that reduces spinal misalignments to enhance the functionality of the musculoskeletal system. This will improve spinal health in the cervical and thoracic regions of the body by decreasing inflammatory swelling associated with heart issues. Chiropractic care, a healthy diet, and exercise also work hand in hand by positively impacting co-morbidities of coronary heart disease and other body problems like obesity to reduce cholesterol, help strengthen the weak muscles along the neck and upper back, and promote blood flow to the heart.
Conclusion
As part of the cardiovascular system, the heart supplies hormones, oxygenated blood, and nutrients throughout the entire body by ensuring that the muscles, tissues, and organs are functioning. When factors like stress, obesity, and unhealthy habits begin to affect the heart, it can develop cardiac issues like coronary heart disease associated with various body problems. Chest pains associated with heart issues that trigger neck and back pain in the body are known as viscero-somatic pain. Available treatments like chiropractic care and changing unhealthy habits work hand in hand to positively impact co-morbidities of coronary heart disease and reduce muscle stiffness along the neck and back muscles of the cervical and thoracic spine.
References
Börjesson, M. “Visceral Chest Pain in Unstable Angina Pectoris and Effects of Transcutaneous Electrical Nerve Stimulation. (TENS). A Review.” Herz, U.S. National Library of Medicine, Apr. 1999, https://pubmed.ncbi.nlm.nih.gov/10372297/.
Foreman, Robert D, et al. “Mechanisms of Cardiac Pain.” Comprehensive Physiology, U.S. National Library of Medicine, Apr. 2015, https://pubmed.ncbi.nlm.nih.gov/25880519/.
Malakar, Arup Kr, et al. “A Review on Coronary Artery Disease, Its Risk Factors, and Therapeutics.” Journal of Cellular Physiology, U.S. National Library of Medicine, Aug. 2019, https://pubmed.ncbi.nlm.nih.gov/30790284/.
Shahjehan, Rai Dilawar, and Beenish S Bhutta. “Coronary Artery Disease – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 9 Feb. 2022, https://www.ncbi.nlm.nih.gov/books/NBK564304/.
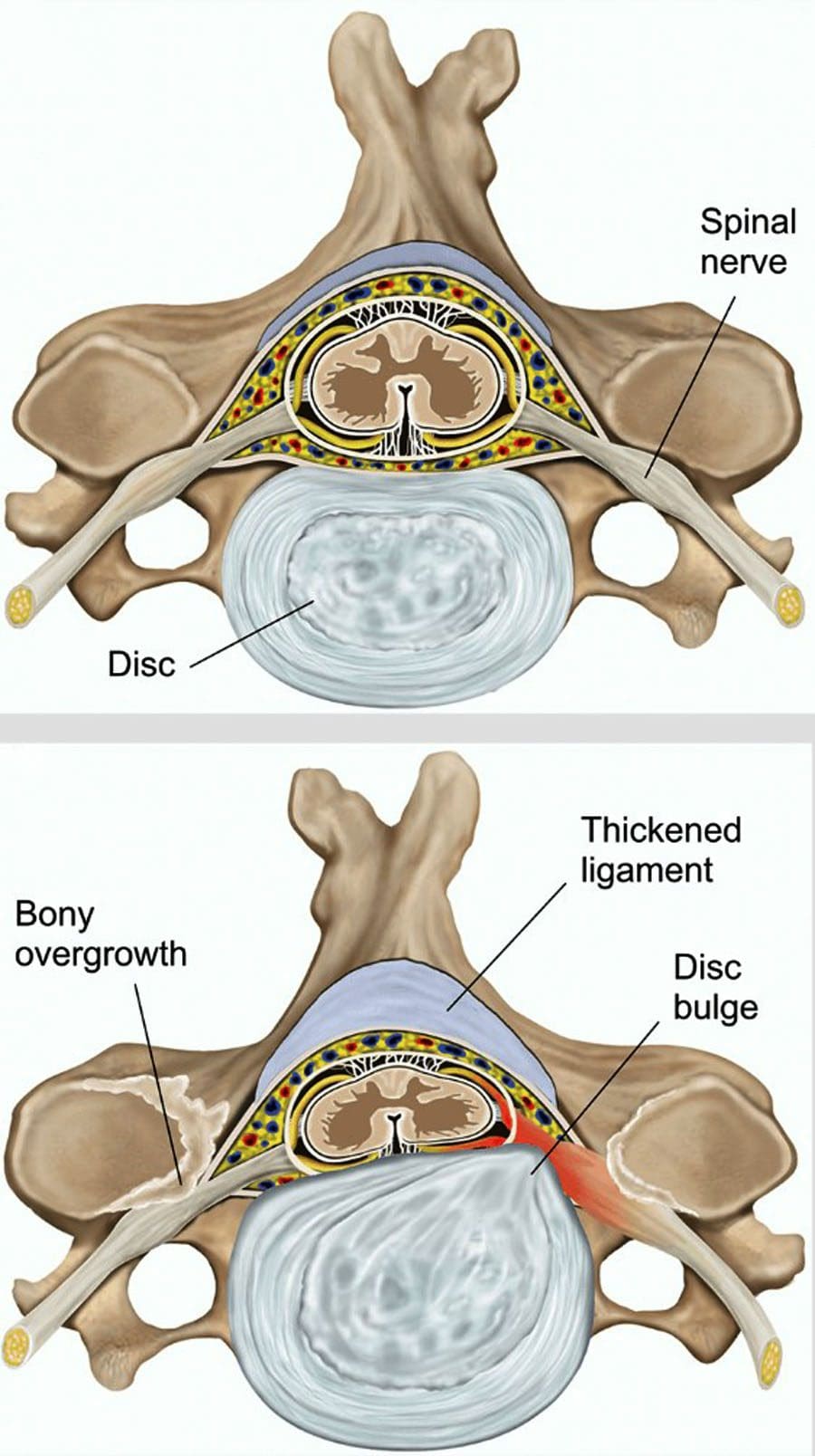
Cervical spinal stenosis is a condition that causes narrowing of the neck region of the spine. This narrowing can compress the nerves causing pain and discomfort. The symptoms are caused by the misalignment/subluxation of the neck, which is usually the c1 and c2 vertebrae. Misalignments can be caused by daily wear and tear; injuries and tumors can cause or worsen the condition. Cervical spinal stenosis is a severe condition that worsens as time progresses and can cause permanent damage and paralysis. Chiropractor recommendations and non-invasive techniques can alleviate the symptoms, along with therapeutic stretches and exercises, and diet is all part of a personalized treatment plan.
Stenosis Symptoms
The most common symptom is neck pain. Doctors recommend avoiding all activities that worsen the pain; however, chiropractors suggest remaining as active as possible to keep the muscles strong. This is because inactivity over time can lead to muscular deterioration around the neck. Other symptoms besides neck pain include:
Neck discomfort and pain
Headaches
Numbness, tingling in the shoulder, arm, hand
Difficulty maintaining balance
Walking problems
Chiropractor Recommendations
Pain Or Stiffness In The Neck Should Not Be Ignored
Pain or stiffness in the neck that worsens rapidly or does not ease up or go away after two weeks requires medical attention.
Ignoring or dismissing the pain or stiffness can worsen the condition.
Looking Down At A Phone Too Long
Looking down too long increases the strain on the neck.
Keeping the head forward for extended periods increases the chances of pinching/compressing nerves and causing radiculopathy.
Exercises That Roll The Neck Around
Exercises that roll or pull the neck are not advised as they can exacerbate the condition.
A chiropractor will recommend specific neck stretches and exercises on a case-by-case basis.
Heavy Bag, Purse, BackPack On One Shoulder
It is recommended to carry a backpack with both shoulders to distribute the weight evenly.
Over time, a backpack, bag, or purse on the same shoulder will disrupt the walk cycle and pull down on one side of the neck, exacerbating cervical spinal stenosis.
For bags and purses with one strap, it is recommended to alternate shoulders or use a crossbody strap.
Sleeping On The Stomach
Sleeping on the stomach means having to turn the neck to one side.
This stresses and aggravates cervical stenosis.
It is recommended to sleep on the side or back.
Treatment, Therapy, and Rehabilitation
Chiropractic is recommended for spinal stenosis because it corrects and re-aligns dislocated and herniated discs and decompresses the spine.
Treatment reduces pressure on the spinal cord and its joints and nerve networks.
Various techniques include physiotherapeutic massage, spinal adjustments, cervical traction, spinal decompression, and flexion-distraction, which will address stenosis symptoms, treat pain, reduce inflammation, numbness, and restore muscle function.
Non-Surgical Cervical Decompression
References
Clark, Aaron J et al. “Cervical spinal stenosis and sports-related cervical cord neurapraxia.” Neurosurgical focus vol. 31,5 (2011): E7. doi:10.3171/2011.7.FOCUS11173
Kukurin, George W. “The amelioration of symptoms in cervical spinal stenosis with spinal cord deformation through specific chiropractic manipulation: a case report with long-term follow-up.” Journal of manipulative and physiological therapeutics vol. 27,5 (2004): e7. doi:10.1016/j.jmpt.2004.04.009
Isaac Z. Evaluation of the patient with neck pain and cervical spine disorders. UpToDate. https://www.uptodate.com/contents/evaluation-of-the-patient-with-neck-pain-and-cervical-spine-disorders. Last updated May 2, 2016. Accessed February 25, 2018.
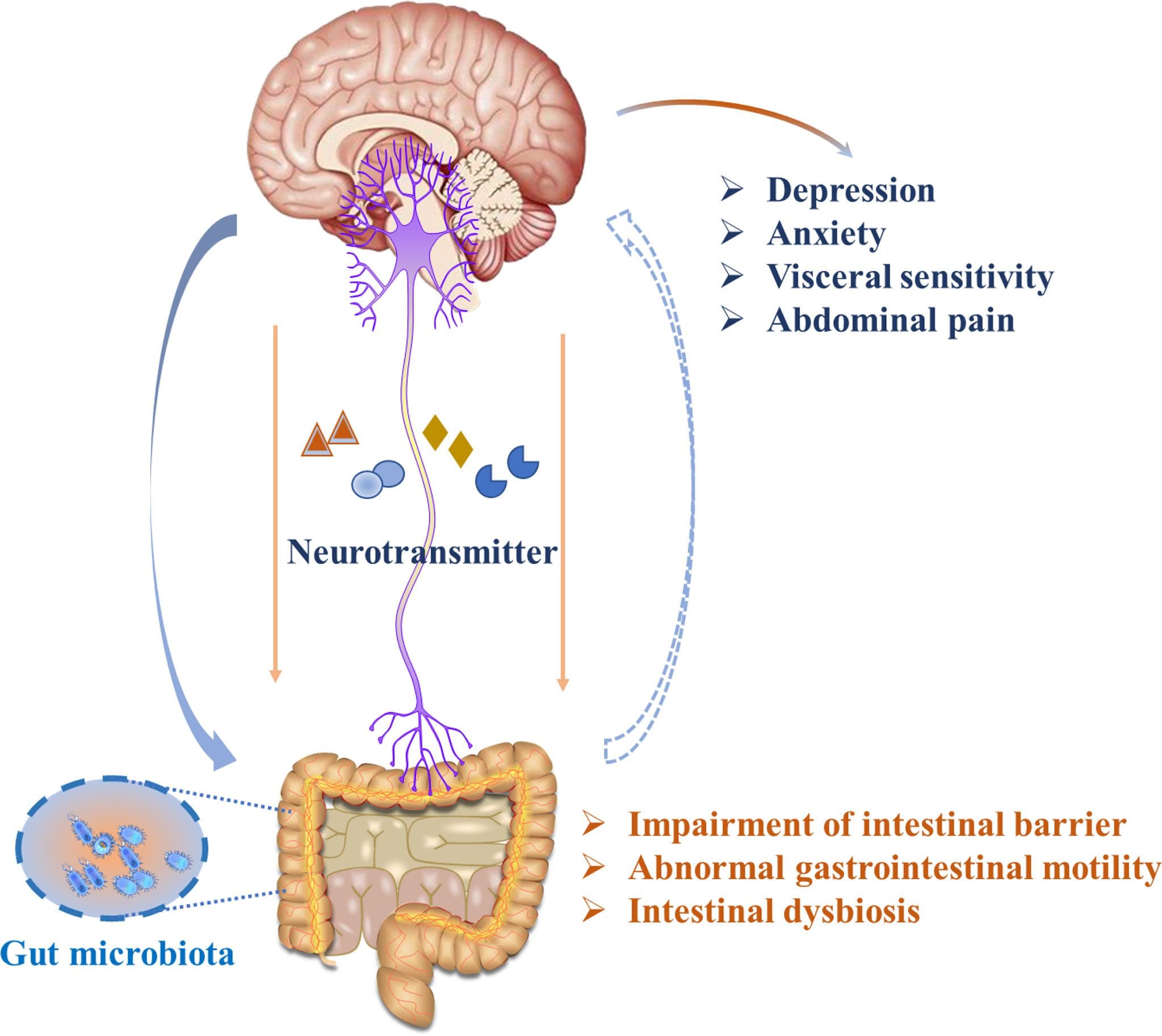
The gut-brain axis is fundamental to the body as it communicates bi-directional with the brain and the gut. Separately they provide different functions that are required of the body. The brain, part of the central nervous system, allows the neurons to travel to each overlapping nerve root while having a causal relationship with different muscles and organs connected to the spinal cord. While the gut, which is part of the gastrointestinal and digestive system, helps modulate the body’s homeostasis and regulates the immune system. The nerves, muscles, and organs correspond as the nerve pathways interconnect to the spinal cord. When injuries or traumatic events affect the body, it can lead the individual to suffer from pain affecting their body while increasing the risk associated within different locations. For example, chronic stress causing gut inflammation is associated with headaches or neck and back pain. Today’s article focuses on the gut-brain axis, what happens when chronic issues affect the gut-brain axis, and how somatovisceral pain affects the gut-brain axis. We refer patients to certified providers specializing in gastroenterology treatments that help those with issues that affect the gut-brain axis and overlapping problems impacting the body. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
How Does The Gut & Brain Work Together?
The way the gut and brain correlate together is quite remarkable. The gut allows food to be digested in the stomach to be bio-transformed into nutrients the body needs to function. While the brain sends neuron signals through the spinal cord, those signals help provide the sensory-motor functions to make the body move. Now, how do the brain and gut work together in the body? Well, studies reveal that the gut-brain axis correlates to the various systems like the autonomic nervous system, the HPA axis, and the nerves surrounding the gastrointestinal tract help the brain influence intestinal activity and regulate cognitive function. Each of these vital organs has a causal relationship where they:
Help with sleep regulation
Improve memory functionality
Helps coordinate physical and emotional well-being
Regulating inflammatory responses
When chronic issues affect the gut-brain axis, it can cause an overlap in risk profiles that rise in the body and not just in the brain or the gut. Studies reveal that issues that begin to affect the gut-brain axis can cause alteration within the bi-directional pathway and trigger other problems that correlate to the body.
Chronic Issues Affecting The Gut-Brain Axis
Have you been suffering from fatigue? How about reoccurring headaches that never seem to go away? Do digestive complaints like IBS, GERD, or gut inflammation affect more than your gut? These chronic issues can be various factors that impact the bi-directional connection of the gut-brain axis. Stress, gut inflammation, traumatic events, food allergens, autoimmunity, and metainflammation are some overlapping risk profiles associated with neck and back pain. Studies reveal that chronic stress in the brain can affect the gut’s composition and functionality by alternating intestinal permeability. When the gut microbiome is being affected, the harmful bacteria begin to overproduce and trigger the sympathetic branch of the nervous system to cause an imbalance of hormones to be released and be associated with stress-related muscle dysfunction in the body. So what does this implicates to the body? Let’s say, for example, that you have been experiencing pain in the cervical region of the spine, but your brain is telling the body that it is a headache. This is known as somato-visceral pain.
An Overview Of Somatosensory Tract-Video
Have you been suffering from cognitive and memory dysfunction? How about experiencing gastrointestinal issues that are affecting your gut? Or have you experienced any cramping, gnawing, or sharp pain that seems to be triggered by movement and appears in one area of the body? This is known as somato-visceral pain and is defined as soft tissues and muscles experiencing pain that can affect the internal organs. Somato-visceral pain is much easier to identify than viscero-somatic pain because visceral pain is caused by damaged internal organs associated with distress in different body locations. At the same time, somato-visceral pain is often associated with musculoskeletal pain. The video above explains the somatosensory tract that is in the body and how the body responds to the somatosensory system. The somatosensory system is located within the peripheral and central nervous systems. It is responsible for modulating the body’s sense of touch, vibration, temperature, and pain receptors that are located in the body. When traumatic events affect the somatic nerves, they can trigger changes in the gut-brain axis and cause alterations to the affected organs.
Somatovisceral Pain Affecting The Gut-Brain Axis
When dealing with chronic stress, the effects cause a dysfunctional gut-brain axis and cause issues affecting the two organs. Studies reveal that when chronic stress becomes an associated mediator for gut disturbances and dysregulation of the gut-brain axis, it can cause an overlap in risk profiles in the body. So what does this mean, and how is the body affected by somato-visceral pain? First, let’s look at what happens when the body is affected by chronic stress. When stress affects the gut and the brain, it can cause issues like IBS (irritable bowel syndrome) or headaches. Studies reveal that IBS is one of the most common gastrointestinal disorders that trigger visceral and somatic hypersensitivity on the sensory nerves. So the body experiencing sharp pain in the back or neck may be associated with IBS.
Now looking at headaches and their causes on the body, it is one example of somato-visceral pain. When a person is dealing with neck trauma due to an auto accident that causes whiplash can trigger cervicogenic headache. How do the two correlate with somato-visceral pain? Well, somato-visceral pain is when soft muscles and tissues are affected and can cause an impact on the internal organs. For cervicogenic headaches may trigger mechanical pain along the cervical spine to be aggravated by movement and be associated with musculoskeletal issues like rheumatoid arthritis, ankylosing spondylitis, or muscle strain on the upper cervical spine. Many individuals go to available treatments that can help them better understand the issue that is causing them to be in pain and how to alleviate them.
Conclusion
The gut-brain axis is fundamental in the body as it communicates bi-directional with the brain and the gut. These two organs help keep the body functioning as the brain provides neuron signals while the gut regulates homeostasis. The gut-brain axis helps the body by correlating with the various systems that help influence intestinal activity and control cognitive function. When traumatic factors affect the body’s soft tissues and muscles and trigger organ issues, this is known as somato-visceral pain. Somato-visceral pain is when the muscles are affecting the organs, and an example is cervical muscle strain associated with headaches. Providing much-needed information on available treatments can help many individuals when being examined by their physicians.
References
Appleton, Jeremy. “The Gut-Brain Axis: Influence of Microbiota on Mood and Mental Health.” Integrative Medicine (Encinitas, Calif.), InnoVision Health Media Inc., Aug. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6469458/.
Carabotti, Marilia, et al. “The Gut-Brain Axis: Interactions between Enteric Microbiota, Central and Enteric Nervous Systems.” Annals of Gastroenterology, Hellenic Society of Gastroenterology, 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4367209/.
Martin, Clair R, et al. “The Brain-Gut-Microbiome Axis.” Cellular and Molecular Gastroenterology and Hepatology, Elsevier, 12 Apr. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6047317/.
Suslov, Andrey V, et al. “The Neuroimmune Role of Intestinal Microbiota in the Pathogenesis of Cardiovascular Disease.” Journal of Clinical Medicine, MDPI, 6 May 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8124579/.
Yuan, Yao-Zong, et al. “Functional Brain Imaging in Irritable Bowel Syndrome with Rectal Balloon-Distention by Using Fmri.” World Journal of Gastroenterology, Baishideng Publishing Group Inc, June 2003, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4611816/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine