As we age, staying active keeps us healthy,� our lives are lengthened and we feel great! Older individuals are discovering that exercise, sports and being physically fit does not mean having to do hardcore workouts and hard-to-maintain exercise/s and schedules.
Many of these individuals get their exercise from active pastimes like biking, Crossfit, and tennis. Others participate in less active recreational activities like walking, gardening or golf. Regardless of which activity they get into, they are all getting relaxation and fun while securing a healthy future.
Exercise helps us feel better because it improves our health.
Spending just a little time each day doing some type of physical activity, will bring these benefits:
Longer
Healthier life
Stronger bones
Reduced joint
Reduced muscle pain
Improved mobility
Improved balance
Lower risk of falls
Lower risk of serious injuries e.g. hip fractures
Slower loss of muscle mass
Fortunately, individuals are living longer but their quality of life means staying healthy and active to remain independent.
Staying active will lower the risk of many common diseases, relieve arthritis�pain and help you recover faster when illness hits.
Activity and Safety
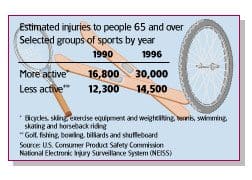
Keeping active means that it’s also important to be safe during these activities/exercises. With more older individuals participating in physical activities, there is an equal increase in sports-related injuries. This is true for bicyclists, skiers, weight lifters and those that use exercise machines.
A recent study by the U.S. Consumer Product Safety Commission (CPSC),� showed an estimated 53,000 people ages 65 and up were treated in U.S. emergency rooms for sports, physical activity-related injuries. Additional injuries were treated in doctor’s clinics/offices.
The increase comes from more older individuals engaging in active sports. However, most of these injuries were not severe but more importantly, they could’ve been prevented. An example was cyclists treated in emergency rooms for head injuries were not wearing helmets. Wearing a helmet reduces the risk of serious head injury up to 85 percent. Regular exercise along with doing it safely means you can enjoy yourself a lot more.
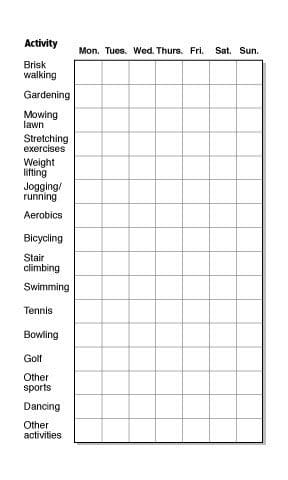
Activity log
Medium physical activity for 30 minutes a day is beneficial for everyone but especially those with chronic bone/joint conditions.
The 30 minutes of activity can be broken up into shorter periods of different activities, like 15 minutes of gardening and 15 minutes of stretching exercises. This can help not getting bored with a routine by mixing it up.
Activity log to keep track of the time you spend on each.
Injury Prevention Tips
When exercise/participating in an activity, doctors recommend following these tips:
Wear the proper safety gear for whichever activity/sport you choose.
Wear the right shoes for each sport/activity.
Warm-up before engaging in physical activity. This could be moderate walking at your normal pace with an emphasis on arm movements.
Exercise at least 30 minutes a day. Break the activities into shorter periods of 10 or 15 minutes throughout the day.
Follow the 10 percent rule, which means never increasing the program like walking/running distance or weight-lifting more than 10 percent a week.
Try not to do the same routine two days in a row.
Mix it up so as not to sprain/strain the same muscles and allow the other muscles to get a workout. So walk, swim, tennis or lift weights, as this keeps the exercise more interesting.
Read instructions carefully when working with exercise equipment, and if needed, ask a qualified professional to help you.
Check exercise equipment making sure it’s in proper working order.
If weight training interests you but you have never done it, make sure to get professional consultation before starting.
Stop exercising if there is severe pain or swelling and get checked by your doctor.
There are plenty of ways to enhance our lives as we age, and staying fit and active along with the proper diet are a few of the most important.
Our clinical focus and personal goals are to help your body heal itself naturally quickly and effectively.� At times, it may seem like a long path; nevertheless, with our commitment to you, it�s sure to be an�exciting journey. The�commitment to you in health is to, never lose�our deep connection to each one of our patients on this journey.
When your body is truly healthy, you will arrive at your optimal fitness level proper physiological fitness state. �We want to help you live a new and improved lifestyle. Over the last two decades, while researching and testing methods with thousands of patients, we have learned what works effectively at decreasing pain while increasing human vitality.
Lower Back Pain Chiropractic Treatment El Paso, TX
NCBI Resources
Aerobic exercise increases the blood flow to the body�s tissues, and people with high levels of cardiovascular fitness generally do better dealing with spinal problems. However, before anyone with a�spine condition or any medical condition�for that matter, starts a�wellness and fitness program, they should check with their primary caregiver, to clear the individual as�fit to exercise.
Back soreness, pain, and discomfort can make walking even moving a challenge, but through assistive devices, you can keep moving. If a spinal condition affects your ability to walk or if you have recently undergone surgery, a cane or walker can help maintain your independence.
Canes and walkers are designed in a simple fashion, but come with amazing benefits: They improve:
Balance
Prevent falls
Takes stress/pressure off the spine
There are all kinds and styles of assistive walking devices. Here are a few tips to help you select the best cane or walker.
Which To Get Cane or Walker
There are options when it comes to choosing but with so many options knowing which is the best for your condition can be challenging.
Talk with your health provider, which could be a primary physician, nurse, chiropractor, physical therapist, or other health care professionals familiar with your medical history and discuss which device would suit your condition and lifestyle the best.
Canes and walkers each have their pros and cons depending on the condition/s. Some considerations to think about when choosing between a cane and a walker:
What is the purpose of the device?
Canes are ideal for problems that occur on one side of the body like sciatica, which often affects one leg, and walkers are ideal for pain that occurs on both sides like weakness in both of the legs.
Which should I get to support my weight?
Canes can support up to 25 percent of your weight, and walkers can support up to 50 percent.
What is the amount of stability you need in the device?
Walkers have the most stability, but there are four-point canes that can also support proper balance and spine safety.
What amount of flexibility do you need in the device?
If you want perhaps the flexibility to go up and downstairs�a cane may be a better choice, as walkers should not be used on stairs.��
Considerations and Questions
Once you�ve decided on what type, then it’s time to decide which type to buy and make sure it is the correct model and style for you. A health care provider can help you find the right model that suits your needs, fits correctly and will educate and show you how to properly use it. Considerations to think about when buying a cane or walker.
Canes
Canes fall into three categories:
Standard: The simplest type of cane and comes with a comfortable T-shaped handle. This helps with balance, but these aren’t able to bear as much weight.
The Offset: A cane that can support more weight than a standard model comes with a flat grip for those with a weak grip and an upper shaft that can bend outward.
Multi-legged: Multiple-legged canes offer maximum stability, perfect for preventing slips, and falls. The only issue could be is that because of the multiple legs means it can be a little awkward at first. But once you get the hang of it
Questions for a Cane
What grip should I go with?
There�s no right or wrong grip. This all comes down to you and what feels the most comfortable as you move around. But, larger grips work better for those with joint problems, and the foam grip style or a type of memory foam that shapes to your hand seems to be the current trend.
What if the grip I chose is not the correct one?
If numbness, tingling, or pain begins to present in your hand/s when using the device or after, consult your doctor, chiropractor or physical therapist.
Where are Canes available?
Canes can be purchased at medical supply stores and pharmacies. But they can also be purchased online, which is extremely helpful if the model you want is not available at the store.
Where to learn how to properly use the cane?
Talk to your chiropractor, physical therapist or doctor who can give you tips and guidelines on how to use the device. They will also help make sure that the cane fits correctly.
Working with a health care professional to achieve the right fit can be highly beneficial. If the grip does not feel right, it’s not comfortable, or if it’s too long/short, the cane ends up doing more harm than good. A therapist/chiropractor will make sure everything is right.
Walkers
Walkers fall into three models:
Standard: These walkers have four legs with rubber ends and provide quality support and stability. But, because there are no wheels it needs to be picked up to move around.
Front-wheel walker: This type has two wheels in the front and two solid legs in the rear. This type does not need to be picked up and requires less effort.
Four-wheeled walkers: These move the easiest, but they can be difficult to get used to placing all your weight because of the easy rolling. Although they do have breaks and wheel adjustments to control the wheel speed, it can take some getting used to and training. Some models come with a seat.
Questions for a Walker
What grip should I go with?
Walker grips are usually made of hard plastic, non-slip rubber, or flexible memory foam. Again it�s all up to you to decide which is the most comfortable.
Preparing the home for a walker
Walkers can get snagged on rugs or bump into the furniture so it�s a good idea to set up your home and move the furniture/objects to help accommodate your movement.
Where can I purchase a walker?
Walkers are available at medical supply stores and pharmacies. They can also be purchased online.
How can I learn how to properly use my walker?
Using a walker can be a little uncomfortable at first. Movements that were easy, like sitting to standing might need to take some time to get the feel of it. But with time and practice, it will become second nature. Talk to your doctor or chiropractor/physical therapist about the right way to use your walker. They can help you develop a strategy and technique to improve mobility.
Spine Pain Won’t Slow You Down
Mobility assistive devices, like canes, and walkers can help you move around after an accident, spine surgery, or a chronic spine condition and allow you to maintain your freedom.
Our uplifting southwest community surrounded by its infinite beauty is a fantastic place to live and enjoy our families; it is, therefore, our mission to help each of our patients to live,�to�love,�to�matter�and�to�thrive�pain-free�in this beautiful special place.
Shoulder Pain Treatment El Paso, TX Chiropractor
NCBI Resources
As you move into your senior years, you may expect some discomfort and loss of mobility. Aging is hard on the body. But it is important to understand that there are things you can do to feel better. Regular exercise, a healthy diet, and�chiropractic care�can all make your senior years active and thriving.
As parents and grandparents, we first need to think about the activities that we will be doing throughout the day and consider how to protect ourselves and loved ones from falls and falling injury/s.
Around the House
Most accidents indeed happen at the house. Add that to the increasing number of people, both young and elder, that work from home. Consider the following tips.
Home
If possible, hire a professional to clean the gutters or get one of those gutter washers that you can use from the ground. Falls from the roof results in multiple injuries, and some are very serious.
Would you please not stand on a chair to change lights or clean those out-of-reach areas? Always use a reliable heavy-duty step ladder with anti-slip steps and handrails. Doctors from emergency rooms report that falls from chairs are a common case they treat.
Proper Lighting
Having the right lighting throughout the house is the best defense against tripping and falling. The stairways, hallways, and entrances are primary areas that should be adequately lit to see everything around you. The light switches should be easy to find and activate. Inexpensive nightlights should be placed anywhere you go at night, like the kitchen or bathroom. A small flashlight should also be kept nearby, possibly a keychain or next to the bed in case of an emergency or if the power goes out.
Kitchen
Falling on wood or tile kitchen floors can have a serious impact on the body. A wet slippery floor can be another cause for a fall, so clean up spills or fix a dripping refrigerator immediately. Using a no-slip floor wax rather than conventional floor wax will reduce accident probability. Keep a secondary heavy-duty step ladder with wide anti-slip steps and handrails for the kitchen.
Bathroom
The bathroom has the potential to be one of the most dangerous rooms. The slick hard floor floors from bath/shower water, along with the limited room to move around comfortably and metal towel rods, can make for a dangerous space to fall in. However, bathrooms can be made safe by the following:
Handrails/grabs can be placed along the walls and shower/bath, near the toilet and sink. Make sure that the proper height is measured.
Anti-slip bath/shower mats and anti-slip floormats can go a long way to help prevent falls. They provide traction and stability while standing and moving around.
There are some top assisted bath devices in various drug stores and home centers. They include shower seats and walk-in baths.
Raised toilet seats can be easily installed and shorten the distance needed to sit and, more importantly, get up comfortably from the toilet.
Elderly and physically challenged individuals could still need help. Make sure assistance is readily available. Elderly and physically challenged individuals could benefit by carrying an alarm or emergency contact system in case they fall or need help.
Stairways
The stairway is an area that can be another danger zone. One stairway danger is the use of canes, walkers, and walkers with wheels. These can easily get snagged on a step, or the wheels can slip and quickly travel down the stairs. Safety railing and step mats with traction nibs can help prevent slips and falls. Outdoor stairs should have non-slip tape to prevent falling.
Carpeting/Rugs
Carpeting and rugs are great for warmth, foot care, and decoration, but they can also pose a danger. Here are a few tips:
Throw rugs that are not properly anchored to the floor should be anchored or used in an area that will not pose a potential injury. These rugs can be bought with a rubber backing to prevent slippage. Stores carry non-slip backing that can be cut and used between the floor and the rug.
Carpeting needs to be smooth and not wrinkled, which can snag and cause tripping.
Bent corners should be removed and fixed to prevent unraveling or tacked down with non-slip tape.
Loose fibers need to be cut off.
Furniture
Individuals that don’t use an assisted device like a cane or walker could find navigating through the house difficult. Furniture should be arranged and organized for easy maneuverability. Electrical cords should be safely placed out of the walking path.These cords can be tacked to the floorboard, placed behind/under furniture, or stored in special cord tubes/runners. Small tables, floor lamps, and plants should not be in the walking path as well as this can cause an easy bump to fall scenario.�
Footwear
Footwear should be nice but also practical. Flat-soled shoes, high heels, not properly structured, or ill-fitting shoes can lead to slips and falls. Unsupported feet will not provide a solid foundation to help prevent a fall.
If there are foot issues, custom foot orthotics can really help stabilize balance, help the spine stay aligned, and bring relief from pain. Orthotics are designed to fit inside shoes to relieve pain from various foot conditions/issues. Non-slip and anti-slip soled shoes can also help prevent a slip and fall. With these types of shoes, care needs to be taken to avoid sticking to floor surfaces. This can contribute to stumbling and tripping. Don’t wear socks or hosiery on smooth tiled/wood floors; because there is no floor-foot traction, the potential for slipping increases.
When walking outside, if the sidewalk is slippery, walk on the grass or dirt area. Try walking in an area that does not show iciness or wetness. Cat litter or rock/sidewalk salt can provide foot traction.
Assistive Devices for Balance and Stability
If you feel unstable while walking, ask your doctor about an assisted device that includes canes and walkers. If using a cane, make sure the rubber grip tip is not worn down.
Conclusion
Here are a few tips that may help you to take a proactive approach to fall prevention. Depending on specific conditions and needs, you may want to talk to your doctor, chiropractor, physical therapist, or other health care professional. They will create a customized individual plan to help prevent falls and enjoy life.
Our clinical focus and personal goals are to help your body heal naturally, quickly, and effectively. At times, it may seem like a long path; nevertheless, with our commitment to you, it’s sure to be an exciting journey. The commitment to you in health is never to lose our deep connection to each one of our patients on this journey.
Plantar Fasciitis, Reduce Foot Pain with Custom Orthotics
NCBI Resources
Aging is hard on the body. As you move into your senior years, you may expect some discomfort and loss of mobility. But it is important to understand that there are things you can do to feel better. Regular exercise, a healthy diet, and chiropractic care can all make your senior years active and thriving.
As 2020 is off to a bustling start, New Year resolutions are in full swing! Most individuals want to make healthier choices throughout their year in 2020, whether that be exercising more, eating better, or just feeling energized. After the holidays hit, most people are left feeling fatigued,� suffering headaches, and overall discomfort.
A great way to stay on track with your goals is to keep track of them! The human body requires micronutrients and macronutrients to function. Micronutrients consist of essential vitamins and minerals. Macronutrients refer to protein, fat, and carbohydrates. Macronutrients all provide the body with energy. This energy is essential to properly repair cells as well as maintain metabolism, immunity, and growth.
Carbohydrates are the main energy system in the human body. These carbohydrates provide over 50% of the daily diet. However, not all carbohydrates are created equal. There are simple and complex carbohydrates. Simple carbohydrates are those found in glucose and fructose (examples: fruit, sugar, and milk). Complex carbohydrates are those that require the body to work a little harder to break down and contain glycogen. Glycogen is important to eat as it is a valuable source of fiber.
The main function of protein is to maintain and grow the body tissue. Proteins are made up of amino acids.� Amino acids are the stepping stones used for neurotransmitters, cell membranes, nucleic acids, and hormones. Protein is widely stored in the human body due to the large amount of muscle tissue the body is comprised of. Overall, there are amino acids that must be obtained through the diet to maintain optimal health. Some of these amino acids include lysine, threonine, and tryptophan.
Out of all the macronutrients, dietary fats require the least amount of grams per day. Similar to carbohydrates, there are two types of fat. Saturated and unsaturated. Saturated fats can be found in butter, where unsaturated fats mainly consist of nuts and avocados. A great supplement to take for healthy fats is Omega-3 and Omega-6, also known as fish oils. Fish oils also help improve cardiovascular health and help the Body generate specialized lipid mediators.
Although each individual requires protein, fat, and carbohydrates, the optimal amount of each depends on each person as well as their body composition. Tracking macronutrients has been shown to improve weight loss and reduce inflammation.
�Tracking macros or macronutrients coupled with exercise is a great way to see results. The macronutrients each person needs depends on their body type, their goals, and their lifestyle. Health coaches such as myself can help determine what an individual’s macronutrient intake should be for weight loss results. Personally, I use the Dr. J Today app, wrist band, and scale. This app allows patients to track their food, steps, water intake, and exercise as well as provides an informative digital library. The scale directly syncs to the app, allowing me to get instant access to the weight and body composition of the patient. This scale not only measures individuals but it also measures their lean body mass, water mass, BMI, and body fat. These resources allow us to gain optimal insight and make corrections that will actually make a difference. – Kenna Vaughn, Senior Health Coach
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Physical Activity to Prevent Back Pain and Weight Gain
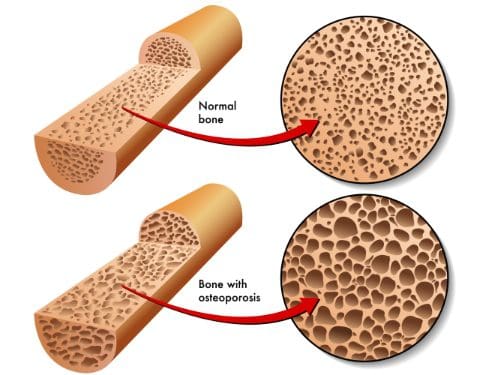
Osteoporosis
Regular physical activity will improve the body’s:
Balance
Reflexes
Coordination
This significantly reduces potential falls and injuries. Injuries from falling can be devastating for someone with osteoporosis.
Consult with your doctor before beginning any exercise program.
To help reverse bone loss, physical activity must fit the individual’s type and intensity. This will determine the appropriate exercises for your level of fitness as well as the risk of fracture.
As a way to begin walking is a great way to start a regular exercise therapy.
Walking improves bone strength because it distributes the body’s weight in a balanced manner over and over again. Bone responds best to the intensity of the walk and not the duration. Bones need to be consistently challenged as they respond by making more osteoblasts or the cellular material that fills the bone cavities. Adding these higher levels of resistance causes healthy stress to bones. This is what increases bone density.
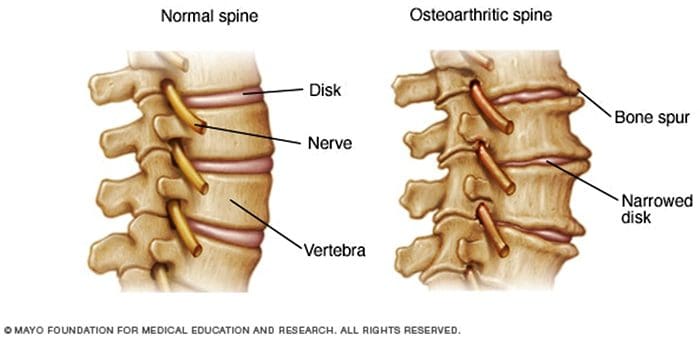
Osteoarthritis and rheumatoid arthritis are conditions that affect the flexibility of the spinal or facet joints. Flexibility, in this case, means the ability of joints to move through their normal range of motion. The amount of an individual’s range of motion is determined by how tight the muscles, tendons, and ligaments are. When muscles can stretch freely, this means the joint has better flexibility.
Low Back Pain & Possible Sciatica
To prevent low back and leg pain, the back, and hip muscles need to be flexible and strong. Individuals with poor flexibility and weak muscles in the back, pelvis, and thighs have a higher risk of increasing the curve of the lower back which can make the pelvis tilt too far forward.
Proper posture combined with flexible and strong muscles can help prevent nerve compression and pain.
Overall Health
Having healthy body composition means there needs to be more lean body mass i.e. muscle mass and less body fat. Strength training/CrossFit helps by raising the metabolic rate while lowering body fat. The increased muscle strength helps maintain correct posture and body mechanics in whatever you do.
Physical activity reduces the chance of injury while increasing physical performance like being able to climb stairs or carry groceries with much-added ease and confidence.
Exercise Suggestions
The benefits a regular exercise program offers are one of the keys to a healthier lifestyle. But take it in steps, see a health coach, physical therapist or chiropractor to help educate and guide you through an exercise treatment plan. Helpful tips:
It can take 6 to 8 weeks to see results so focus on short-term goals.
Work regular exercise into your schedule but keep important activities as a priority.
Friends and relatives can help give you support and join in the exercise.
You don’t have to do an entire workout. Instead, exercise for 10 minutes.
Consistency in physical activity is the goal. It’s not how long or hard the exercise is.
Keep a journal of your workouts and progress.
With the healthy changes made today, including diet choices and regular physical activity/exercise, your life will be one-hundred times better. This does not mean that you have to become an intense workout aficionado. Remember all that is needed is a reduction in weight of only 10%. This is what is needed to reduce the detrimental effects of being overweight.
Our clinical focus and personal goals are to help your body heal itself naturally quickly and effectively.� At times, it may seem like a long path; nevertheless, with our commitment to you, it�s sure to be an�exciting journey. The�commitment to you in health is to, never lose�our deep connection to each one of our patients on this journey.
When your body is truly healthy, you will arrive at your optimal fitness level proper physiological fitness state. �We want to help you live a new and improved lifestyle. Over the last two decades, while researching and testing methods with thousands of patients, we have learned what works effectively at decreasing pain while increasing human vitality.
*AMAZING* Custom Orthotics for Athletes | El Paso, Tx
NCBI Resources
It can be tempting to not exercise with a spinal condition. But remember that if there is no movement at all, you could make the pain worse.�Knowing what your body can handle and sticking to a workable schedule, these healthy steps will relieve you and help with your low back pain.
All individuals that participate in some form of sports or athletic training, professionals to weekend sports enthusiasts are at risk for back and neck injuries. Common injuries include strains, and sprains, pulls, and tears especially around the low back area. If left untreated these injuries can lead to chronic back pain or more severe conditions.
Although we can’t prevent all sports injuries, here are some sports tips to keep your spine healthy.
1.� Warm-Up and Stretch
Properly warming up with stretching exercises increases blood circulation and improves the flexibility of muscles and ligaments. This is not only for helping enhance athletic performance but prevents injuries by keeping the muscles/ligaments loose so if any type of collision, tear, or pull occurs the stretched muscles stay relaxed and do not tense up or contract, which helps reduce the severity of an injury. To stretch properly:
Stretch time on each part of the body is also 10-30 seconds
Stretch after the game to relieve sore or tight muscles
2. Use Proper Sport Equipment
All sports have a risk of injury. In general, the more contact there is the higher the risk of injury.
To reduce the risk of injury athletes should wear protective equipment that goes with their sport like neck rolls, shoulder, elbow and knee pads.
Well made and supportive shoes combined with custom orthotics are a must.
Other types of equipment include:
Helmet
Pads elbow, wrist, chest, knee, shins
Mouthpiece
Faceguard
Protective cup
Eye protection
3. Stay Hydrated
Injuries caused by heat occur as a result of�high temperatures, humidity and excessive/overdoing it. To avoid these serious injuries:
Drink plenty of water before, during, and after playing.
Try to avoid play or practice during extreme heat and humidity.
Wear lightweight clothing/uniform with maximum ability to allow sweat to evaporate.
Take plenty of breaks or periods of rest to allow the body to recover and recuperate.
4. Don’t Overwork/Overdo it
Repetitive Motion Disorders like tennis elbow, bursitis, and tendonitis, happen when movements e.g. swinging motions that go with the sport like tennis, bowling, golf, etc are repeated over and over and cause injury/damage to those parts of the body. To avoid overuse injury try:
Take plenty of breaks during practice and games. Do not power through it!
Use proper/correct form and techniques. If unsure then take lessons to make sure you are doing it correctly.
See a doctor if any pain or muscle fatigue, inflammation, swelling, or compression of nerve tissue present.
Cross-training can strengthen muscle groups and those areas that take the most force.
5. Stay Ready for Play with a Healthy Lifestyle
Besides sports, try to find ways to improve general health through a healthy lifestyle:
Get plenty of sleep, the body/mind needs to recover from all the activity.
Consult a doctor before beginning any new exercise program.
Staying fit, healthy and ready for play means preventing injuries from happening.� By being aware of how to prevent injuries with these basic tips, which feel free to take it further and raise the probability of avoiding back and all sports injuries.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
*BEST* Heel Spurs Treatment | El Paso, Tx (2020)
NCBI Resources
Extension sports like gymnastics, tennis, swimming, diving, football, volleyball, basketball, track and field, cricket have the most pronounced extension/rotation on the spine. With a normal extension of the lumbar spine (or backward bending), the facet joints begin to approximate each other and compress. This is a normal biomechanical movement. However, if the extension ranges are excessive, the procedures will impinge quite aggressively and damage to the cartilage surfaces within the facet joint can result.
You might not think it, but weight lifting and spine strengthening exercises can help reduce back pain. Remember the point of this type of weight lifting is not to build up the muscles like a bodybuilder but is to develop:
Core strength
Spine strength
Body strength
The muscles in the back keep the spine moving and functioning properly. When the spine or abdominal muscles are weak this creates a higher probability of a back strain or injury. Having strong, healthy spine muscles are important because they function in maintaining correct posture, which in some cases, causes chronic back pain because of poor posture.
If�only one part of the body is strengthened like the back is not enough. Therefore strengthening the rest of the body is a must. These include the body’s core and leg muscles. Total body strength will reduce back pain and can help perform regular activities, like lifting heavy objects much easier, with more confidence and with a lesser probability of injury.
Spine strengthening exercises benefits
Most important reasons are they:
Prevents future back injuries
Stabilizes the spine
Helps the spine move properly
Help maintain correct posture
Increases muscle tone
Teaches correct body mechanics
Helps build bone this is especially beneficial for those with osteoporosis or at risk of developing it
A personal trainer or sports chiropractor can help start a spine strengthening regimen. They will teach:
Simple
Specific
Strengthening
Weight lifting exercises.
A physical therapist can also develop a custom weight lifting/strength�exercise�program for optimal spine health and for reducing pain.
Most workout regimens incorporate a combination of weight lifting with actual weights/exercise machines and strengthening exercises/calisthenics with the body’s weight as the resistance for maintaining a healthy strong spine.
Here are a few weight lifting and back strengthening exercises that can help decrease and prevent back pain.
Talk to a doctor or chiropractor before beginning any exercise program. Remember to listen to your body and stop right away if there is something off.
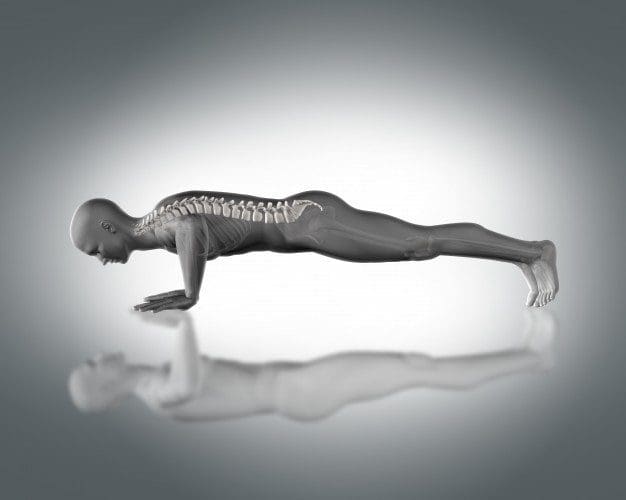
Push-ups
Push-ups help strengthen the:
Back
Chest
Arms
Core muscles
Your own body weight is the resistance.
To do this:
Position the body in a straight line from head to toe, the face looking down.
Hands should be wider than shoulder-distance apart. Walk the hands out so they are slightly higher than the shoulders
Keep the balance on toes and hands, with a straight back, lower the body to the floor by slowly bending the elbows until at a 90-degree angle.
Push up using arm upper back, and chest muscles.
Do 3 sets of 10 every day. As the strength increases do more reps.
Chest Flyes
Chest flies are excellent for building muscle in the:
Upper back
Chest
Dumbbells or a weight machine can be used for this exercise. To do this:
Lie on the floor with the knees bent and the feet flat on the ground.
Extend the arms out to either side of the body, and let them rest on the floor.
With a dumbbell in each hand, raise the dumbbells until they meet at the top at the same time, and keep a slight bend in the elbows.
Lower the hands to the ground, and repeat.
Do this exercise 15 times 3 times a week. With added strength add more reps.
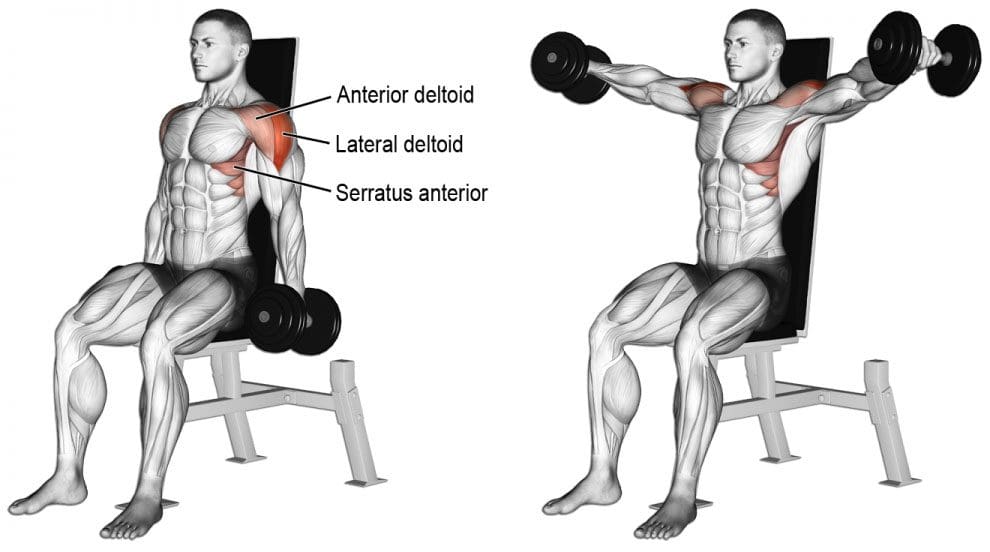
Lateral Raises
Lateral raises help strengthen the entire back. All that is needed is a set of dumbbells. To do this move:
Stand or sit with the feet equal hip-distance apart. Arms are at the side.
With a dumbbell in each hand and a slight bend in the elbows, raise the arms to the side until shoulder height. Keep the core engaged during the movement.
Once at shoulder height, slowly lower the dumbbells, and repeat.
Repeat this exercise 15 times 3 times a week. As strength increases add more reps.
These exercises should be performed slowly with a gradual build-up to more complex movements and adding more weight. Remember to breathe naturally. If you hold your breath during exercise, it can cause tension in the�muscles, which can worsen any pain or create new injuries.�Before adding weight or new spine strengthening exercises, talk to a doctor about exercising with back pain. They will let you know if there are certain movements or positions that should be avoided.
Weight lifting exercises done incorrectly can lead to more back pain and added injuries. If there is any pain while doing these exercises, stop and call a doctor, chiropractor or physical therapist right away.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
Back Pain Chiropractic Care | El Paso, Tx
NCBI Resources
It can be tempting to not exercise with a spinal condition. But remember that if there is no movement at all, you could make the pain worse. Knowing what your body can handle and sticking to a workable schedule, these healthy steps will relieve you and help with back pain.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine