Tennis is a sport that can be enjoyed by individuals of all ages and provides optimal physical activity and cardiovascular exercise. Although it can be leisurely, it does require being light on the feet with quick, starting, stopping, turning, and twisting movements for those new to playing tennis. If back pain is present, playing can be difficult. One study showed almost 40% of tennis players missed one or more tournaments because of low back pain/problems. A 2016 study found that tennis players with low back pain have difficulty moving their muscles with ease.
Know and Understand the Risks
Playing tennis has its risks when it comes to back pain. What can bring on or worsen back pain are the repetitive motions, like swinging, serving, volleying, and the uneven force placed on the body. This force is the power and momentum that is used for certain swings like serving and forehands. What happens is it does not evenly distribute through the body, increasing the potential to cause strains and sprains. For example, the serving motion repeatedly puts a hyperextension force through the spine. The result is overuse injuries.
Preparation
No one wants to injure their back for those new to tennis and those who have been playing for years. This is where off-court conditioning comes in and preventive measures. This includes:
Don’t play for too long when starting or multiple days in a row
Gradually increase the frequency and intensity
Focus on the fundamental skills rather than trying to blast the ball like the pros.
Trying to smash the ball too soon can result in a rotator cuff injury.
Stay Aware of Your Body
Playing tennis can cause an individual to become distracted; however, it’s crucial to be mindful of the body and what’s going on.
Pay attention to the heat.
Humidity
Proper rest between games
Hydration to prevent muscle cramping
Stretching before and after playing
Warming up and cooling down
Take a break and stretch out if pain symptoms present.
Never play through the pain that could result in worsening or creating new injuries.
Pay attention to proper form.
Apply modifications to prevent and avoid worsened back pain. This could be serving more simply or hitting around a stroke that generates pain symptoms.
Cooling Down
After a match, rehydrate the body and cool down. This could be a little walking around the court, if possible getting in a pool or water splash park, and let the musculoskeletal system recover. Do some spinal exercises afterward, like yoga poses. Applying anti-inflammatory creams or gels can help keep the muscles loose and promote circulation. Anti-inflammatory foods can help with pain and inflammation.
Spinal Conditions
There are individuals with spinal conditions that should not play tennis. These include:
Acute disc herniation
Active bone injury/s – fractures and stress fractures
Spinal instability – spondylolisthesis
Post-spine surgery
A spinal condition involving nerves and/or the spinal cord
Consult a doctor before adding tennis to a physical regimen. Tennis is an aerobic activity that has several benefits. It keeps the body physically active for mental and physical wellness. The hormones released can help mitigate musculoskeletal pain and negative emotions like depression and anxiety that can come from experiencing back pain.
Body Composition
Magnesium
Magnesium supports a healthy immune system. It helps maintain:
Aids muscle relaxation after exercise/physical activity
Magnesium is essential in several biochemical reactions; a slight deficiency can increase cardiovascular disease risk. Deficiency can also lead to an increased risk of insulin resistance. Magnesium-rich foods are also high fiber foods. Dietary fiber helps with:
Digestion
Helps control weight
Reduces cholesterol
Stabilizes blood sugar
Recommended sources of Magnesium include:
Green vegetables – spinach, swiss chard, and turnip greens
Nuts – almonds and cashews
Seeds
Legumes
Cocoa
References
Clinics in Sports Medicine. (April 1988) “Low back pain in the competitive tennis player.” https://europepmc.org/article/med/2968850
Journal of Science and Medicine in Sport. (April 2016) “Trunk muscle activation, fatigue and low back pain in tennis players” https://www.sciencedirect.com/science/article/abs/pii/S1440244015000845
Jahnen-Dechent, Wilhelm, and Markus Ketteler. “Magnesium basics.” Clinical kidney journal vol. 5,Suppl 1 (2012): i3-i14. doi:10.1093/ndtplus/sfr163
Katz, David L et al. “Cocoa and chocolate in human health and disease.” Antioxidants & redox signaling vol. 15,10 (2011): 2779-811. doi:10.1089/ars.2010.3697
Wang, Jinsong, et al. “Dietary magnesium intake improves insulin resistance among non-diabetic individuals with metabolic syndrome participating in a dietary trial.” Nutrients vol. 5,10 3910-9. 27 Sep. 2013, doi:10.3390/nu5103910
Stretching out for everyday wear and tear. The body was designed for movement, mobility, and physicality. When discomfort, aches, and pain present in the neck, shoulders, back, and joints, it is often from a decrease of natural body movement. Many think that sitting still and resting is the best solution to alleviate the pain. While it is important to rest, it is the type of rest that helps the body. Sitting still with no movement is not recommended. The muscles, ligaments, and tendons need to flex and stretch out to help reduce pain and prevent injury. Safe, chiropractic-approved stretches can increase mobility and fluidity, helping the body stay flexible and loose.
Stretching Out For Everyday Wear and Tear Is Important
Whether experiencing pain or are getting ready for the day, there are many reasons why stretching is important. One, stretching is essential to optimal joint health. When muscles surrounding the joints become tight/tense, this significantly reduces mobility in the joint. Regular stretching lengthens the muscles, relaxing the joints to move without discomfort/awkwardness. Stretching optimizes blood circulation to flow smoothly through the body. Routine stretching helps reduce stress and improves energy. Other benefits include:
Post-workout/exercise/physical activity soreness and pain relief
Improves athletic performance
Prevents injury/s
Helps heal existing injuries
Improves posture
Stretching Safe at Home
Chiropractors often recommend stretches for patients to follow to help improve their progress between appointments. If persistent pain is presenting, consult with a qualified chiropractic doctor before performing any stretches. If done incorrectly, they can exacerbate pain and cause further damage. No matter an individual’s lifestyle, the wear and tear of everyday life can cause tightness, inflammation, or generalized pain. Developing a regular stretching routine can address any tense, tight, sore areas that will help keep the body pain-free.
Tailbone Stretch
Most individuals feel tailbone pain from sitting for long periods of time. Reasons for tailbone pain can result from:
Falling backward
Sitting in the wrong position
Childbirth
Hypermobility
All can injure the tailbone and/or the surrounding muscles and tissue.
Tailbone stretching improves movement and flexibility in these muscles and tissue, maintaining the tailbone’s health. One recommended stretch is the piriformis cross leg stretch.
Lie flat on the back.
Bring both knees toward the hips.
Rest the right ankle across the left knee.
Wrap both hands around the left thigh
Pull toward the chest.
Hold for 20-30 seconds.
Slowly bring down both legs and return to the starting position.
Repeat on the other side.
Wrist and Hand Stretch
For those that are constantly writing, typing, or lifting regularly, wrist and hand pain can begin to present. Stretches for the hands and wrists can:
Increase flexibility
Alleviate pain
Reduce the risk of injury
The prayer stretch for the wrists and hands is specifically designed to strengthen the muscles and tendons in the wrists.
Standing with the back straight and feet shoulder-width apart.
Place hands together in a prayer position.
Hands in front of the face.
Pressing both palms together, slowly spread the elbows apart.
Begin to lower the hands to waist height
Stop once the hands become level with the belly button or when the stretch is felt.
Hold the position for 10-30 seconds.
Return to the original position.
Repeat as needed.
Knee Stretch
When tightness or soreness presents in the knee, stretching the hamstrings can help. The hamstrings go through a great deal of wear and tear, supporting the hips and knees, maintaining mobility and flexibility.
Standing with the back straight.
Step forward with the left foot.
Flex the left foot and keep the right foot flat.
Loosen the hips and bend the right knee.
As the right leg is bent, keep the left leg completely straight with the heel pressing into the ground.
If maintaining balance is difficult, use a wall for support.
Hold the position for 10-15 seconds.
Return to starting position.
Repeat on the other side.
Body Composition Health
The Gut’s Hormones
When a meal enters the stomach and intestines, it triggers the digestive tract to release hormones that create the full feeling. These are the gut’s hormones, with each having a specific set of actions and effects. Examples include PYY, GLP-1, and GIP. Gut hormones are essential because they signal the body to slow down or stop eating. Therefore, the size of a meal influences the number of gut hormones that get released. The body releases larger quantities of gut hormones in response to meals with a higher caloric density. This is because larger meals usually contain more calories. This is one reason the body feels more satisfied after a large meal. Smaller meals are less satisfying, which means an individual will want to eat again after the meal.
After eating comes the digestion and absorption of macronutrients. This is known as the postprandial state. The body is in storage mode during the postprandial state. Even though the metabolic rate increases after a meal, the contents of that meal get broken down and stored for fuel. Four hours after a meal, the body goes back to its baseline state, which primarily burns through the stored fuel. Eating frequent, small meals throughout the day means the body spends more of the day in the postprandial storage state.
References
Bandy, WD et al. “The effect of time and frequency of static stretching on flexibility of the hamstring muscles.” Physical therapy vol. 77,10 (1997): 1090-6. doi:10.1093/ptj/77.10.1090
Freitas, SR et al. “Stretching Effects: High-intensity & Moderate-duration vs. Low-intensity & Long-duration.” International journal of sports medicine vol. 37,3 (2016): 239-44. doi:10.1055/s-0035-1548946
Hotta, Kazuki et al. “Daily muscle stretching enhance blood flow, endothelial function, capillarity, vascular volume and connectivity in aged skeletal muscle.” The Journal of physiology vol. 596,10 (2018): 1903-1917. doi:10.1113/JP275459
le Roux, C W et al. “Attenuated peptide YY release in obese subjects is associated with reduced satiety.” Endocrinology vol. 147,1 (2006): 3-8. doi:10.1210/en.2005-0972
Maintaining the body’s musculoskeletal system and keeping it strong can be done through chiropractic and by managing general overall health. This system includes the:
Bones
Muscles
Tendons
Ligaments
Soft tissues
These all work together to support the body’s weight and allow for movement.Injuries, disease, and aging can cause stiffness, pain, and other issues with mobility, function that can lead to various conditions and/or disease.
The musculoskeletal system
The skeleton provides the framework for the muscles and other soft tissues. Working together, they support the body’s weight, help to maintain proper posture and the ability for movement. Various disorders and conditions can lead to problems with the musculoskeletal system. This includes:
Focusing on overall health and maintaining it will keep the system in top form. This is done by:
Eating a healthy balanced diet
Maintaining a healthy weight
Regular physical activity/exercise
Chiropractic support will take the body to optimal health levels.
How does the system work?
The nervous system is the body’s central command center. It controls voluntary muscle movements. Voluntary muscles are controlled intentionally. Large muscle groups are utilized to do activities like lifting a large object. Smaller groups are used for movements, like pressing a button. Movement/motion occurs when:
The nervous system which includes the brain and nerves, transmits a signal to activate the skeletal/voluntary muscles.
The muscle fibers contract/tense in response to the signal.
When the muscle activates, it pulls on the tendon.
Tendons attach muscles to bones.
The tendon pulls the bone, generating movement.
For the muscle to relax, the nervous system sends another signal.
This signal triggers the muscle/s to relax/deactivate.
The relaxed muscle releases tension
The bone is moved to a resting position.
System Parts
The musculoskeletal system functions to help stand, sit, walk, run and move in general. The adult body has 206 bones and more than 600 muscles. These are connected by ligaments, tendons, and soft tissues. The parts of the system are:
Bones
Bones support the body, protect organs and tissues, store calcium, fat and produce blood cells.
A bone’s outside shell encapsulates a spongy center.
Bones provide structure and form to the body.
They work with the muscles, tendons, ligaments, and other connective tissues to help with movement.
Cartilage
This is a type of connective tissue.
Cartilage provides cushion to the bones inside the joints, along the spine, and ribcage.
It is firm and rubbery.
It protects bones from rubbing against each other.
It is also found in the nose, ears, pelvis, and lungs.
Joints
Bones come together and form joints.
Some have a large range of motion, for example, the ball-and-socket shoulder joint.
Others, like the knee, allow bones to move back and forth but do not rotate.
Muscles
Every muscle is made of thousands of fibers.
The muscles allow the body to move, sit upright, and remain still.
Some muscles help with running, dancing, and lifting.
Others are for writing, fastening something, talking, and swallowing.
Ligaments
Ligaments are made of tough collagen fibers
They connect the bones and provide stability to the joints.
Tendons
Tendons connect the muscles to the bones.
They are made of fibrous tissue and collagen
They are tough but not as stretchable.
Conditions and disorders
Various conditions can cause problems with the musculoskeletal system. They can affect the way an individual moves. The most common causes of inflammation, pain, and mobility issues are:
Aging
With the natural aging process, bones lose density.
Less-dense bones can lead to osteoporosis and bone fractures/broken bones.
As the body ages, muscles lose their mass, and cartilage starts to wear down.
This can lead to pain, stiffness, and decreased range of motion.
After an injury, an individual might not heal as quickly.
Arthritis
Pain, inflammation, and joint stiffness are the result of arthritis.
Older individuals are more likely to develop osteoarthritis. This is from the cartilage inside the joints breaking down. However, the condition can affect individuals of all ages.
Other types of arthritis also cause pain and inflammation. This includes:
Rheumatoid arthritis
Ankylosing spondylitis
Gout
Back problems
Back pain and muscle spasms can result from muscle strains or injuries, for example, a herniated disc.
Some conditions like spinal stenosis and scoliosis can cause structural problems in the back.
This can lead to pain and limited mobility.
Cancer
Different types of cancer affect the musculoskeletal system, for example, bone cancer.
Congenital abnormalities can affect the body’s structure, function, and appearance. For example, clubfoot is a common musculoskeletal condition that babies can be born with. It causes stiffness and reduces the range of motion.
Disease
A wide range of diseases can affect bones, muscles, and connective tissues functionality.
For example, osteonecrosiscauses the bones to deteriorate and the cells to die.
Other disorders, like fibrous dysplasia and brittle bone disease, cause the bones to fracture/break easily.
All types of injuries can affect bones, muscles, cartilage, and connective tissues.
Injuries can occur from repetitive overuse. Examples include:
Carpal tunnel syndrome, Bursitis, and Tendinitis
Sprains
Muscle tears
Broken bones
Injuries to the tendons, ligaments and other soft tissues can lead to chronic conditions.
Maintaining musculoskeletal health
Recommended ways of maintaining a healthy musculoskeletal system are to keep the bones and muscles healthy by getting:
Regular physical activity and exercise
This includes weight-bearing exercises combined with cardiovascular activities. Strengthening the muscles will support the joints and protect/prevent damage.
Proper sleep
This is so the bones and muscles can recover and rebuild.
Maintain a healthy weight
Added weight places pressure on the bones and joints.
This causes various health problems.
If there is added weight, it is recommended to consult a health coach and nutritionist about a personalized weight-loss plan.
They can help make healthy food choices that will make for strong bones and include anti-inflammation foods.
Quit tobacco use
Smoking decreases blood flow in the body.
The bones, muscles, and soft tissues need proper blood circulation to maintain health.
Regular chiropractic adjustments
Adjustments will help maintain the body’s balance and alignment.
This, along with recommended stretches and exercises, will take the body to optimal health.
Healthy Body Composition
Bodyweight Squat
This is one of the best strength exercises for building general functional low body strength. The muscle groups that get worked include the:
Quadriceps
Hamstrings
Glutes
Deep abdominals
Hip abductors
Hip rotators
Squats work almost every muscle in the legs. This also builds core strength to help with everyday movements like pushing, pulling, and lifting. There is no need to load added weight on the back to benefit from this exercise. Using the body’s weight is a perfect workout. This can be done with several variations once strength is built up. The objective is to focus on strict form for maximum effectiveness.
The feet should be shoulder-width apart.
Bend at the hips
Don’t let the knees go past the toes.
Lower the body until the thighs are parallel to the floor
References
American Chiropractic Association. Back Pain Facts and Statistics. Accessed 1/5/2021.
Centers for Disease Control and Prevention. Arthritis. Accessed 1/5/2021.
Centers for Disease Control and Prevention. Arthritis-Related Statistics. Accessed 1/5/2021.
Centers for Disease Control and Prevention. Work-Related Musculoskeletal Disorders & Ergonomics. Accessed 1/5/2021.
Merck Manuals. Effects of Aging on the Musculoskeletal System. Accessed 1/5/2021.
National Institute of Arthritis and Musculoskeletal and Skin Diseases. Healthy Muscles Matter. Accessed 1/5/2021.
Although it is not officially summer, the past few weeks sure feels like it. Especially for those with joint discomfort and pain. As the body ages, individuals may notice their joints have some mobility/flexibility issues in the summer heat. Again, the heat and humidity are the culprits. The hotter it is, the more the body is susceptible to inflammation and swelling. The more prone an individual’s body is to swelling, the more pain can present. Barometric pressure can also have some form of impact on joint health. The pressure changes can cause the joints to become more sensitive. When the pressure changes, individuals often speak of their joints feeling tighter combined with stiffness, leading to a cycle of swelling and pain.
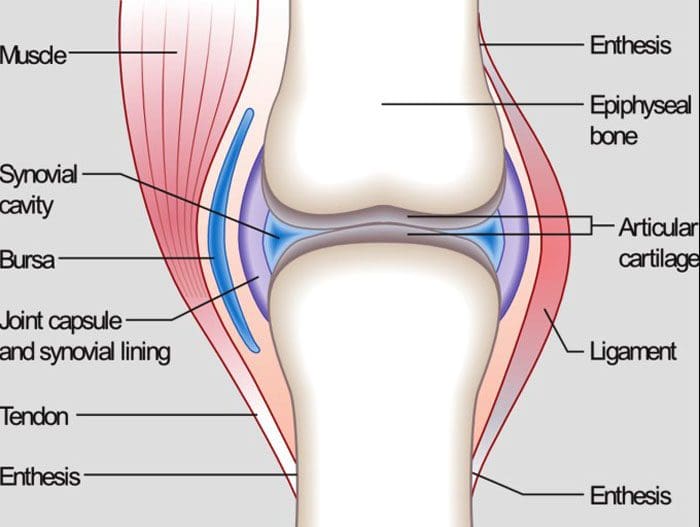
Joint Anatomy
Whether it’s the hip, knee, elbow, or hand, all of the body’s joints have fluid in them. It is a gel-like substance known as synovial fluid. This is what lubricates the joints and keeps them functioning smoothly. However, the temperature and humidity levels can change the thickness of the fluid in the joints. This means that the synovial fluid can become inflamed with the weather changes. This is a symptom when the joints begin to feel like they cannot move and/or are becoming stiff. Joint inflammation can become more common and chronic as the body gets older.
Weather and the joints
The summer heat and humidity can affect the joint because:
The tendons, ligaments, and muscles expand in this type of weather
The heat can restrict individuals from moving around. Non-use stiffens the joints
Joints that have worn down cartilage could have exposed nerves that are reacting to the temperature changes
Humidity causes the body to lose water by sweating. This can reduce the fluid around the joints leading to stiffness, immobility, and pain.
However, not everyone has joint problems in the summer heat. Many have joint issues when it’s cold, damp, or raining. Other’s are at their best in cool, dry weather. It depends on an individual’s body and how their joints react when the temperature changes.
Maintaining joint health for the summer heat
When joint discomfort or pain presents in the summer, there are a few easy ways to gain relief.
Properly Hydrate the Body
Water and sports drinks maintain the fluid levels in the body, specifically, it keeps the joints moving. One way to hydrate the body can be achieved by eating healthy fruits and vegetables. Water-rich fruits and vegetables include:
Watermelon
Oranges
Strawberries
Tomatoes
Cucumbers
Spinach
Celery
Over-The-Counter pain ointments and creams
Arthritis and anti-inflammatory creams/ointments can ease joint pain by allowing more blood circulation in the affected areas.
Dressing for the heat
Wear loose, natural fiber, breathable clothing that allows the body to move freely while maintaining a cool temperature.
Relax in the air conditioning
Get into the air conditioning. The cool air can help reduce joint inflammation.
Get in the Water
Swimming or just wading through doing some light exercise in the water cools the body’s core. In addition, the buoyancy of the water relieves pressure on the joints.
Body Composition Testing
Body Water
The body is made up of as much as 2/3’s water. Even though much of the body is made up of water, the percentage of body composition changes based on functional needs. Essential functions of water include:
Water is the building block to almost every cell in the body
It regulates the body’s temperature through sweating and respiration
Carbohydrates and proteins for energy are transported via the water in the blood
Water assists in the removal of metabolic waste through urination
It is part of the shock-absorbing system that protects the brain and spinal cord
Water is part of the saliva and fluid that lubricates the joints
The amount of water in the body depends on various factors. This includes:
Age
Gender
Physical activity
It is referred to as Total Body Water or TBW.
TBW is constantly changing with gains and losses of fluid in healthy adults. The body can detect irregularities and compensate for losses and/or gains to make sure that the systems are balanced.
The information herein is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. In addition, we provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Morton, Darren, and Robin Callister. “Exercise-related transient abdominal pain (ETAP).” Sports medicine (Auckland, N.Z.) vol. 45,1 (2015): 23-35. doi:10.1007/s40279-014-0245-z
Peeler, Jason et al. “Managing Knee Osteoarthritis: The Effects of Body Weight Supported Physical Activity on Joint Pain, Function, and Thigh Muscle Strength.” Clinical journal of sports medicine: official journal of the Canadian Academy of Sports Medicine vol. 25,6 (2015): 518-23. doi:10.1097/JSM.0000000000000173
Quick, D C. “Joint pain and weather. A critical review of the literature.” Minnesota medicine vol. 80,3 (1997): 25-9.
Timmermans, Erik J et al. “The Influence of Weather Conditions on Joint Pain in Older People with Osteoarthritis: Results from the European Project on OSteoArthritis.” The Journal of rheumatology vol. 42,10 (2015): 1885-92. doi:10.3899/jrheum.141594
There are different types of muscle from a biological perspective, however, there is no such thing as lean muscle. Lean suggests the absence of body fat. But the fact is that all muscle is lean muscle. It is important to build muscle mass as the body ages, however, it is more important to build lean body mass. Here is the difference.
Lean Body Mass
Lean Body Mass is the total weight of an individual’s body minus all the weight from the fat mass.
Lean Body Mass (LBM) = Total Weight – Fat Mass
Lean Body Mass includes the weight of the:
Skin
Body Water
Bones
Organs
Muscle Mass
Because Lean Body Mass consists of various components, any change in the weight of these areas is recorded as changes in lean body mass. However, the weight of the body’s organs will not change. Bone density does decrease with time and age, but will not significantly affect the weight of lean body mass. With lean body mass, 2 areas of focus include:
Body water
Muscle mass
Lean Muscle
Sometimes, individuals use the term lean muscle referring to the shape of the muscles. However, both types of muscle are lean and fat-free.
The difference between muscle mass and lean muscle
The strict definition of muscle mass is the weight of the muscles of the body. When individuals say they are gaining muscle mass, they typically mean that the muscles look and feel bigger.
Lean muscle masson the other hand is a term often used when someone is referring to the weight of the muscles, not factoring in the amount of fat that could be present within a muscle.
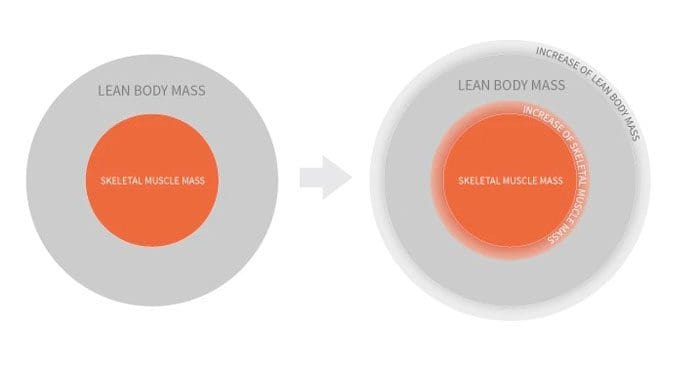
Combining Lean Gains
Increases in Skeletal Muscle Mass are also an increase in Lean Body Mass. What tends to happen is individuals combine them as lean mass gains or lean gains. However, an increase in Lean Body Mass does not always increase muscle.
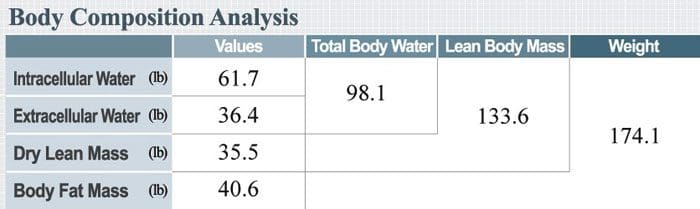
This is because body water makes up a significant portion of an individual’s Lean Body Mass. For example, a body composition analysis of a 174-pound male.
98.1 Total Body Water + 35.5 Dry Lean Mass = 133.6 Lean Body Mass
Water makes up more than 55% of total body weight
This is normal for healthy adult males
Lean Body Mass consists of three components, two of which are water.
Everything else grouped together makes up the individual’s Dry Lean Mass.
This includes bone minerals, protein content, etc.
Muscle gains contribute to Lean Body Mass gains, but so does water. The difference is that water levels can fluctuate throughout the day depending on:
Hydration levels
Diet
Physical activity
The muscle tissue itself contains a significant amount of water. Muscle tissue is comprised of up to 79% water. Research has shown that resistance training increases intracellular water in both men and women. This creates an issue when looking at lean gains.
Lean Mass gains can happen quickly, and the increases are mostly body water
Measuring Lean Body Mass and Muscle Mass
What not to do
Don’t try to use a scale to calculate changes in Skeletal Muscle Mass. A popular method used is to estimate muscle gain from the number on the scale and applying fitness websites/magazine tips. The problem with this technique is that estimating progress has many factors that can influence an increase in body weight. These include:
It is the difference between total body weight and body fat weight. However, these calculations are more for helping physicians determine the appropriate amount of prescription medication/s or if an individual will be undergoing anesthesia and not a computation of overall body composition.
Paying Attention to Weight Loss
Paying attention to weight loss is an inaccurate reflection of lean body mass, muscle mass, or lean mass.
Weight loss, or gain, does not reflect overall health and body composition.
Resistance training/weightlifting workouts combined with added protein will generate a muscle mass percentage increase
Skeletal Muscle Mass is connected with Lean Body Mass
Everyone’s body composition is different, making the proportion of an individual’s skeletal muscle mass to Lean Body Mass unique.
Lean Mass or Lean body mass is the safest term to use to describe gains.
Which Is More Important?
When it comes to tracking muscle gain or fat loss, it all comes down to what tools are being used to measure progress.
If working with just a weight scale, an individual will only know their weight increases or decreases.
This is difficult to see the difference in weight gain from water, muscle, or body fat.
For individuals that want accurate measuring of their muscle gain and assessing their health, then body composition analysis is the key.
Body Composition Difference
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP*, CIFM*, CTG*
email: [email protected]
phone: 915-850-0900
Licensed in Texas & New Mexico
References
Galán-Rioja, Miguel Ángel et al. “Effects of Body Weight vs. Lean Body Mass on Wingate Anaerobic Test Performance in Endurance Athletes.” International journal of sports medicine vol. 41,8 (2020): 545-551. doi:10.1055/a-1114-6206
Köstek, Osman et al. “Changes in skeletal muscle area and lean body mass during pazopanib vs sunitinib therapy for metastatic renal cancer.” Cancer chemotherapy and pharmacology vol. 83,4 (2019): 735-742. doi:10.1007/s00280-019-03779-5
Ribeiro, Alex S et al. “Resistance training promotes an increase in intracellular hydration in men and women.” European journal of sports science vol. 14,6 (2014): 578-85. doi:10.1080/17461391.2014.880192
Ten Haaf, Dominique S M et al. “Protein supplementation improves lean body mass in physically active older adults: a randomized placebo-controlled trial.” Journal of cachexia, sarcopenia and muscle vol. 10,2 (2019): 298-310. doi:10.1002/jcsm.12394
Here are a few recommended stretches and exercises for relieving herniated disc symptoms. The vertebrae are the small bones that make up the spine. They have cushion discs between each one. These are the intervertebral discs and are the body’s shock absorbers. The discs can be thought of as small balloons that are filled with an elastic gel-type material. There are twenty-three of these cushions.
Functioning as the body’s shock absorbers transferring various forces, weight, and stress from vertebra to vertebra, so that no one is overburdened taking on all the impact the body goes through. But like any machine, the discs can wear down over time, and sustain injury. When this happens the cushioning gel can leak out and press on the nerve roots emerging from the spine. This type of injury is a herniated disc.
Herniated Disc Treatment
A herniated disc can lose its height because of fluid and water loss.
This loss affects the bone structures bringing them closer together affecting the ligaments that connect each segment. The ligaments become loose and do not provide the same stability. Ligaments cannot be strengthened with exercise making it more important to strengthen the muscles around the spine to make up for this stability loss. Depending on the severity of the injury, the displaced disc can cause pressure to build upon the nerves, resulting in pain and other discomforts. This comes from the loss of the disc’s cushion causing the vertebrae to rub against each other. Stretches and exercises designed for herniated discs can work in conjunction with conservative treatment to relieve the pain and discomfort.
Stretches and Exercises for Pain Relief
Consult a medical spine specialist/chiropractor before beginning a stretch and exercise regimen. This is because the herniation can become worse or additional injury/s can occur without proper instruction. Once the injury and clinical considerations have been addressed, gentle stretches and exercises can help reduce the pain and other symptoms. Strengthening the back and hamstring muscles reduces pressure on the spinal column helping to prevent pain and promotes healing by:
Increasing blood flow to the spine
Building strength to support the spinal muscles
Decreases stress on the spine
Helps relieve the pain
Improves abnormal postures and awkward body positions
Equipment is not necessary but there are few items that can help the process.
A herniated disc in the neck is usually caused by a forward head posture and a swayback or excessive curvature of the spine.
Isometric hold
Sit straight
Relax the shoulders
Place one hand on the forehead
Push head into the hand without moving the head
Hold for 5 to 15 seconds.
Repeat 15 times
Chin tuck
Lie on your back on a flat surface
Place arms at sides
Tuck the chin in and down toward the chest until a stretch is felt
Hold for 5 to 10 seconds
Repeat 15 to 20 times
Lumbar/Low Back Stretches and Exercises
Back flexion stretch
This stretch extends the back muscles to relieve low back pain.
Lie flat on your back
Pull the knees toward the chest and wrap your arms around the knees
Lift head straight up off the floor until there is a stretch across the mid and low back
Hold for 10 seconds
Repeat 5 to 10 times
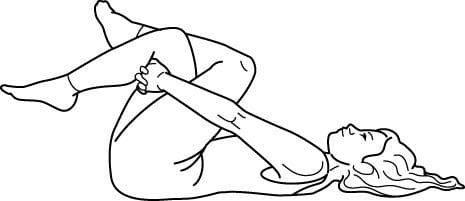
Piriformis stretch
This stretches the small muscle in the buttocks helping to relieve low back pain and helps with sciatica.
Lie flat on your back on the floor or yoga mat
Bend the knees
Plant feet on the floor
Pick up one leg and rest the ankle on the other leg’s bent knee
Reach one arm through the leg and use both hands to grasp the bent leg
Pull the leg toward the chest until there is a stretch in the buttock
Hold for 30 seconds
Repeat on the other leg
Prone extension stretch
This stretch helps reposition the disc back to its proper position, expediting the healing process. Start slowly and if pain presents, stop immediately.
Lie face down on the floor or yoga mat
Place the forearms on the floor next to the body
The elbows should be at a 45- degree angle
Slowly prop the body up, being sure to keep the hips on the floor
Keep pressing upward until the elbows are at a 90-degree angle
Hold the position for 10-15 seconds
Return to starting position
Repeat the stretch 10 times
Gradually increase the upward position hold time until it can be maintained for 30 seconds
Performing these stretches and exercises or similar types will help with herniated injury recovery and prevent worsening or creating new injuries.
Body Composition
Benefits of yoga
Yoga benefits mental and physical health. Yoga helps improve individual physical health. Specific poses can help:
Improve balance
Flexibility
Build/Tone muscle
Prevent injury
Improve sense of well-being
Yoga stretches the muscles while relieving physical and emotional stress. Practicing yoga regularly can prevent obesity, and reduce the risk of developing metabolic syndrome. Yoga can help decrease leptin which is a hormone that helps control appetite. This is important for individuals going through chronic stress who are twice as likely to develop metabolic syndrome.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP*, CIFM*, CTG*
email: [email protected]
phone: 915-850-0900
Licensed in Texas & New Mexico
References
Court C, Mansour E, Bouthors C. Thoracic disc herniation: Surgical treatment, Orthopaedics & Traumatology: Surgery & Research, 104(1)S31-@40, 2018, https://www.sciencedirect.com/science/article/pii/S1877056817303419.
At home or a gym, working out with cardio exercise equipment can be a highly beneficial treatment for back discomfort, soreness, and pain. However, when checking out all the cardio machines it is recommended to use those that will help with back pain and not worsen or cause further injury. The same goes for purchasing cardio equipment to use at home. Research has found that exercise training could be highly effective in the treatment of back pain. A study on pain found that the endorphins generated from aerobic exercise help to lessen low back pain. The North American Spine Society announced evidence-based recommendations for the treatment of back pain, and one of the top recommendations was aerobic exercise. Individuals can always go outside to:
Walk
Hike
Run
Bike ride
But mixing it up with cardio equipment can have its own benefits for different reasons. It could be too hot, raining, sometimes individuals prefer a set workout program to reach calorie or distance goals, and it could be easier on the spine. Working out at home or at a gym, cardiovascular machines can help bring relief for back pain.
Cardiovascular Exercise Back Pain Treatment
Cardiovascular exercise is highly recommended for everyone. For individuals dealing with back pain, exercise combined with conservative therapy is usually part of a treatment plan. This includes:
Physical therapy
Chiropractic care
Health coaching
Diet
Aerobic exercise regimen
With an exercise program, experts recommend starting with moderate-intensity aerobic exercise. Moderate intensity workouts are meant to get an individual’s heart and blood pumping, sweating a little, and slightly deep breathing. These types of exercise include:
Power walking outside
Power walking on a treadmill
Stationary biking
As long as the physical activity gets the heart rate up, these exercises have been shown to decrease back pain, relieve stress, and elevate mood. 20 minutes of moderate-intensity exercise three to five times a week for six weeks is what is recommended. This will help the back become healthier, feel better, and is recommended by the American Heart Association.
Exercise Not For All Spine Conditions
However, not all spinal conditions benefit from regular exercising. Getting an evaluation from a doctor, spine specialist, or chiropractor is recommended for injuries, severe and/or persistent back pain before starting a cardiovascular exercise program. This could be a spinal fracture, or spinal condition that requires bracing, or intense physical therapy/rehabilitation. Individuals that do not exercise regularly or have a medical or heart condition/s definitely need to get a doctor’s clearance before beginning a cardiovascular workout regimen.
Top Cardiovascular Exercises and Equipment
Once a doctor clears the individual for aerobic exercise there is no cardio equipment that is off-limits. Elliptical machines and stationary bikes are the most well-tolerated by individuals with back problems/conditions. Because they are low impact. However, if it is tolerable using a jogging treadmill is beneficial as well. Listen to the body. If a workout on a treadmill causes back pain that is not just workout soreness, stop with that machine and try different cardiovascular equipment that is more low impact. Do not ignore back pain. If pain is continuous and exercising is not helping, stop and see a doctor, or chiropractor to evaluate and analyze the situation. Then they can adjust the exercise part of the treatment plan according to the presenting symptoms.
Body Composition
Concurrent Training
Concurrent training is the combination of aerobic and resistance exercises during the same workout session. Aerobic and resistance exercise impacts the body in different ways. The type of aerobic training determines how it interacts with resistance exercise. The order of the types of exercises like aerobic and resistance workouts can make a difference. Having an understanding of a few specifics about concurrent training will help to make decisions about an exercise program.
Aerobic/interval and resistance training does not seem to interfere with the others’ adaptations
However, gaining strength could be lowered by adding running to a resistance program
Whereas bicycling does not have the same effect.
Cycling and the ergonomics that go with it are similar to traditional lower-body resistance exercises. The muscle contractions that come with running result in muscle damage, while the contractions in cycling also cause muscle damage, it is not to the same extent. Pairing the exercise programs correctly is key, such as a running program in combination with an upper-body lifting exercise can be beneficial. While running and doing leg presses every day could interfere with each other and could cause injuries. Or if doing both aerobic and resistance exercises in the same session, or on the same day, consider the order of the exercises, depending on what the goal is.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP*, CIFM*, CTG*
email: [email protected]
phone: 915-850-0900
Licensed in Texas & New Mexico
References
British Journal of Sports Medicine. (November 2020) “Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis” https://bjsm.bmj.com/content/54/21/1279
Pain. (December 2020) “Are endogenous opioid mechanisms involved in the effects of aerobic exercise training on chronic low back pain? A randomized controlled trial” https://journals.lww.com/pain/Citation/2020/12000/Are_endogenous_opioid_mechanisms_involved_in_the.23.aspx
North American Spine Society. (2020) “Evidence-Based Clinical Guidelines for Multidisciplinary Spine Care” https://www.spine.org/Portals/0/assets/downloads/ResearchClinicalCare/Guidelines/LowBackPain.pdf
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine