Can individuals receive a full night’s rest by recognizing sleep disturbances to only get proper muscle function and improve their health?
Contents
What Causes Sleep Disturbances?
As many people are in a constant state of motion and trying to complete their tasks, they will feel extremely exhausted and tempted to take a quick nap on their bed. However, a short nap can sometimes turn longer and thus affect a person’s sleep schedule. At the same time, when the body is ready to go to sleep, sometimes the mind is wide awake, causing people to become more tired throughout the day. These types of sleep disturbances can not only affect the person but also affect the body as well. In today’s article, we will be looking at what causes sleep disturbances, how improper sleep affects the muscles in the body, and how to incorporate various ways to reduce sleep disturbances. We discuss with certified medical providers who inform our patients how various sleep disturbances can affect the individual and the body. While asking informed questions to our associated medical providers, we advise patients to include various techniques to reduce sleep disturbances that can impact the musculoskeletal system. Dr. Alex Jimenez, D.C., encompasses this information as an academic service. Disclaimer.
How often do you feel general aches and pains in your upper and lower extremities that make you sluggish? Do you experience constant headaches that make it difficult to get out of bed? Or do you feel stiffness in your neck, shoulder, and back in the morning that goes away throughout the day? When it comes to the correlation between what causes sleep disturbance to the body, it can vary from person to person, depending on the situation. Let’s say a person is dealing with a stressful situation that causes them to be unable to get a good night’s rest; that would be known as a sleep disturbance. Sleep disturbances, by definition, are causes that can impact a person’s fundamental aspects of their sleep hygiene. (Cormier, 1990) Understandably, everyone is trying to practice good sleep hygiene; however, when environmental factors cause overlapping risk profiles to develop into sleep disturbances, they can affect the body. These can range from cognitive disorders to musculoskeletal conditions and chronic conditions.
How Does Improper Sleep Affect The Muscles & Body?
When classifying sleep disorders that can cause improper sleep in the body, four major categories can be the issue. They are:
Disorders that initiate and maintain sleep
Excessive somnolence disorders
Sleep-wake schedule disorders
Various dysfunctions are associated with sleep (Weitzman, 1981)
These four categories can cause many people to develop improper sleeping habits that can affect their bodies and muscles. Symptoms like fatigue correlate with poor sleep quality and can increase muscle pain intensity. At the same time, many individuals dealing with fatigue can experience muscle pain intensity associated with comorbidities that can make a person feel miserable. (Boggero et al., 2022) Environmental factors affecting the musculoskeletal system can correlate with metabolic disorders and thus affect sleep. Additionally, improper sleep and disturbances have been interplayed with metabolic disorders that can increase the risk of obesity, hypertension, insulin resistance and cause many people to have improper sleeping habits and, which, in turn, affects their musculoskeletal system. (Wei et al., 2022) Some of the effects of improper sleep that can affect muscle include:
Muscle weakness
Instability
Muscle pain
Discomfort
However, when people start to decide to try to improve their sleep schedule and reduce sleep disturbances, many people start to look for ways to get a full night’s rest.
Chronic Pain Chiropractic Care- Video
Ways To Reduce Sleep Disturbances
When trying to improve sleep quality while reducing disturbances, many people start to find ways to incorporate proper sleeping habits. Since sleep’s ultimate goal is to help individuals maintain and improve physical and mental health, many can achieve long-term sleep improvement through appropriate sleep hygiene and modifications. (Baranwal et al., 2023) Some of the ways many people can reduce sleep disturbances are the following:
Exercise
Sleeping on the right mattress
Establish a bedtime routine
Limit electronic screen time
Reduce eating and drinking caffeinated drinks before bed
Incorporating these small changes allows the individual to have proper sleeping habits and reduce overlapping risk profiles affecting the body and musculoskeletal function.
Finding The Right Mattress
Everyone knows that finding the best mattress is important for a good night’s rest. It is also important for people to find the right mattress to stay asleep and reduce musculoskeletal conditions. When it comes to finding the right mattress, it is important to ensure that the mattress’s firmness plays a huge role in improving a person’s sleep quality and reducing pain and disability for people dealing with sleep disorders associated with musculoskeletal conditions. (Caggiari et al., 2021) This allows the individual to have few sleep disturbances and helps them have that full 8 hours of sleep.
Reduce Screen Time
The next way to reduce sleep disturbances is by reducing screen time to prevent it from affecting sleep habits. Since many people are more technologically advanced, it is hard not to doom scroll at night. When many people are on their phones in bed, it can lead to sleep onset latency and cause issues like daytime tiredness. (Brautsch et al., 2023) The best way to reduce tiredness and sleep issues at night is by allowing 30 minutes to digitally disconnect and place any electronic away from the bed to ensure that the 8 hours of sleep is met. This, in turn, allows the brain to turn off and disassociate from anything digital or social media. When it comes to incorporating proper sleep habits, making small changes in a person’s routine can become beneficial in the long run as not only the body can relax but also the muscles.
References
Baranwal, N., Yu, P. K., & Siegel, N. S. (2023). Sleep physiology, pathophysiology, and sleep hygiene. Prog Cardiovasc Dis, 77, 59-69. https://doi.org/10.1016/j.pcad.2023.02.005
Boggero, I. A., Pickerill, H. M., & King, C. D. (2022). Fatigue in Adults with Chronic Arthralgia/Myalgia in the Temporomandibular Region: Associations with Poor Sleep Quality, Depression, Pain Intensity, and Future Pain Interference. J Oral Facial Pain Headache, 36(2), 155-163. https://doi.org/10.11607/ofph.2944
Brautsch, L. A., Lund, L., Andersen, M. M., Jennum, P. J., Folker, A. P., & Andersen, S. (2023). Digital media use and sleep in late adolescence and young adulthood: A systematic review. Sleep Med Rev, 68, 101742. https://doi.org/10.1016/j.smrv.2022.101742
Caggiari, G., Talesa, G. R., Toro, G., Jannelli, E., Monteleone, G., & Puddu, L. (2021). What type of mattress should be chosen to avoid back pain and improve sleep quality? Review of the literature. J Orthop Traumatol, 22(1), 51. https://doi.org/10.1186/s10195-021-00616-5
Cormier, R. E. (1990). Sleep Disturbances. In H. K. Walker, W. D. Hall, & J. W. Hurst (Eds.), Clinical Methods: The History, Physical, and Laboratory Examinations (3rd ed.). https://www.ncbi.nlm.nih.gov/pubmed/21250242
Wei, Z., Chen, Y., & Upender, R. P. (2022). Sleep Disturbance and Metabolic Dysfunction: The Roles of Adipokines. International Journal of Molecular Sciences, 23(3), 1706. https://doi.org/10.3390/ijms23031706
Getting a good night’s sleep can be difficult for individuals suffering from arthritis. Can finding a mattress that fits an individual’s needs help relieve aches and pains and provide restful sleep?
Contents
Mattress For Arthritis
Quality sleep can be difficult for those managing arthritis. Joint pain, stiffness, and tenderness can make falling and staying asleep feel impossible. A mattress for arthritis should be firm, provide comfortable support, and relieve joint pressure. (Sleep Foundation, 2024)
How Mattresses Affect Arthritis?
Not adequate support or cushioning can exacerbate arthritis pain and stiffness.
Individuals not sleeping well at night can experience significant physical and mental fatigue, increase the risk of injury, and perceive a higher level of pain.
Zoned mattresses provide targeted pressure relief to areas of arthritis pain, like the neck and lower back.
Mattresses that don’t support the body are more likely to disrupt sleep and exacerbate nighttime and daytime pain symptoms.
The body needs time to recover and repair during sleep, so the right mattress for arthritis will allow sound rest throughout the night.
A joint-supporting mattress can alleviate pain and stiffness.
What to Look For Mattress Types
Mattresses fall into three basic categories.
Foam or Latex
These mattresses are often recommended for individuals with chronic pain because they conform to the body and alleviate pressure points without being too firm that they aggravate existing injuries or inflammation.
Not all foam is the same; some mattresses are too soft to support someone with arthritis.
Latex is a more reliable material for support and durability, but it’s also more expensive than memory foam.
Innerspring
Innerspring mattresses are often long-lasting and provide firm support.
However, they are not recommended for individuals with arthritis because they can be hard on joints and pressure points.
The innerspring system doesn’t mold or conform to the body, so getting and staying comfortable can be difficult, if not impossible.
They’re not as heat-retaining as foam mattresses so that hot sleepers may prefer them.
Hybrid
A hybrid mattress typically consists of individually wrapped springs topped with one or more layers of memory foam.
Hybrid mattresses are often recommended for arthritis patients because they meet the expert-recommended balance between support and cushioning.
Firmness Levels
Mattress firmness is rated on a scale of 1 to 10, with firmer mattresses scoring higher, often 6 or 7 and above. However, no one firmness rating works for all individuals with arthritis. Finding the right firmness for arthritis symptoms is highly individualized. For some, a super firm sleep surface can aggravate symptoms. In determining what firmness number is needed, consider weight. For example, a person weighing 400 pounds will have a different experience on a soft mattress than a person weighing 150 pounds. Typically, larger bodies need a firmer mattress to avoid sinking too far into the mattress’s core. Petite individuals may be perfectly supported on a mattress rated 5 or 6 for firmness, but taller or heavier individuals should look for a mattress rated seven or eight.
Support and Pressure Relief
Individuals will want to look for a mattress that targets specific areas for relieving aches and pains, such as the shoulders, hips, and lower back. Foam helps relieve pressure points in the body without feeling too soft, which is helpful when managing joint pain. There is debate over whether latex or memory foam is better for relieving sensitive pressure points. A Journal of Chiropractic Medicine study suggests that latex foam may outperform traditional memory foam as it reduces body pressure and evenly distributes weight along pressure points. (Low F. Z. et al., 2017)
Motion Transfer
Motion transfer refers to a mattress’s ability to isolate body movement. It’s helpful to consider how much you and your partner are affected by each other’s movement throughout the night. This may not be necessary for individuals who don’t sleep with a partner. So, if you or a partner disrupt sleep throughout the night, a mattress with better motion absorption is recommended.
Sleep Position Can Affect Arthritis and Joint Pain
Mattress manufacturers often design mattresses to accommodate back, side, or stomach sleepers, as different sleeping positions usually require different types of support. One study suggests that sleeping-related pain can be reduced in those with lower back pain when they choose the right sleeping surface for their preferred sleep position. (Jacobson B. H. et al., 2010) Therefore, purchasing a mattress for the preferred position is important.
Durability
A mattress’s expected lifespan depends on the materials it’s made from. A mattress that immediately loses some of its features and benefits won’t last very long. This is why it is recommended to know how long the trial period is for the mattress and keep track of its performance. Count on at least six to seven years, but latex and hybrid mattresses can last longer.
Trial Period
Considering the trial period on the mattress is important when buying online. Determining if it’s right for your body can take a little while as it takes a while to break in a new mattress, so look for a longer trial period to see and feel if it is the right choice. (Mattress Firm, 2023) Most online mattress retailers offer at least a 100-day trial period, while some offer 365 days to send it back. However long the trial period, looking into the terms and conditions of any return policy is recommended. A company can say you can return it if it doesn’t meet expectations; however, restrictions or exclusions may apply to your purchase.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Fighting Inflammation Naturally
References
Sleep Foundation. Noyed D. (2024). How to Choose a Mattress. https://www.sleepfoundation.org/mattress-information/how-to-choose-a-mattress
Low, F. Z., Chua, M. C., Lim, P. Y., & Yeow, C. H. (2017). Effects of Mattress Material on Body Pressure Profiles in Different Sleeping Postures. Journal of Chiropractic Medicine, 16(1), 1–9. https://doi.org/10.1016/j.jcm.2016.09.002
Jacobson, B. H., Boolani, A., Dunklee, G., Shepardson, A., & Acharya, H. (2010). Effect of prescribed sleep surfaces on back pain and sleep quality in patients diagnosed with low back and shoulder pain. Applied ergonomics, 42(1), 91–97. https://doi.org/10.1016/j.apergo.2010.05.004
Mattress Firm. (2023). Breaking In a New Mattress: Tips for a Comfortable Night’s Sleep. Mattress Firm Blog. https://www.mattressfirm.com/blog/sleep-tips/break-in-a-new-mattress
Can individuals dealing with scoliosis incorporate various exercises and stretches to improve their posture and reduce pain?
Contents
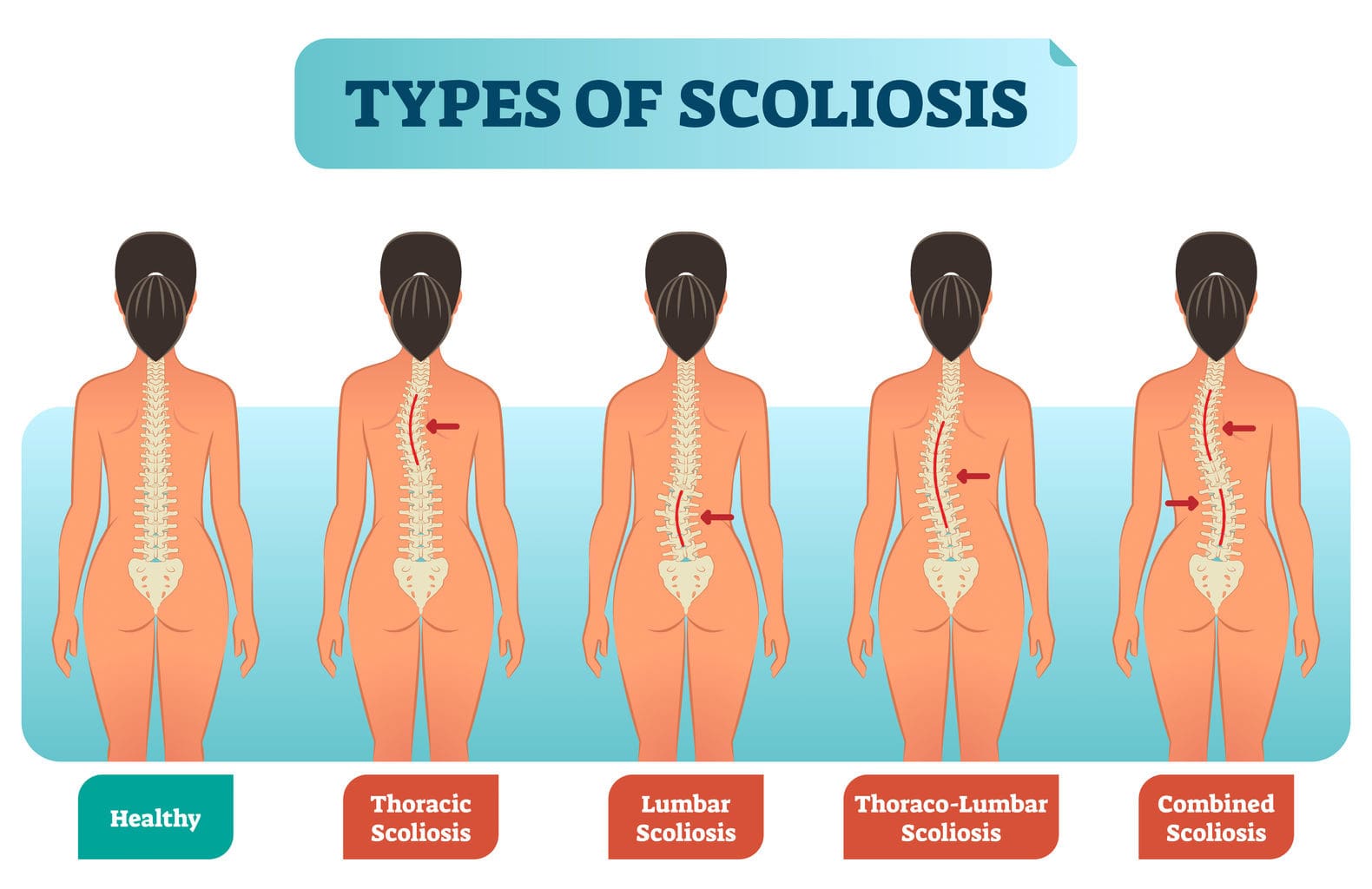
What Is Scoliosis?
More often than anything, many people have tried to maintain proper posture to prevent musculoskeletal and spinal conditions from forming. However, it can be difficult to maintain an appropriate posture when strenuous environmental factors come into play. This can range from being in a hunched position to developing spinal conditions that can affect the curvature of the spine. One of the most well-known spinal conditions many people can develop through numerous risk factors is spinal scoliosis. Spinal scoliosis is often defined as a curvature deviation in the normal vertical spinal line. (Janicki & Alman, 2007) This causes the spine to develop an S or C curve in the thoracic or lumbar portion of the spine, leading to overlapping risk profiles in the body and causing pain-like symptoms that can make a person feel miserable. Today’s article looks at scoliosis, how it affects the body, and how various exercises can help manage scoliosis. We discuss with certified medical providers who inform our patients how non-surgical treatments, like various exercises, help manage symptoms associated with scoliosis. While asking informed questions to our associated medical providers, we advise patients to include various exercises and pain management techniques to reduce pain-like symptoms correlating with scoliosis. Dr. Alex Jimenez, D.C., encompasses this information as an academic service. Disclaimer.
How Does It Affect The Body?
Since scoliosis is a spinal deformity condition that affects the spine, it can happen at any age and is categorized into four group forms:
Congenital (Presented by birth)
Neuromuscular (Resulted from cerebral palsy or muscular dystrophy)
Idiopathic (The common spinal condition)
Degenerative (Adult-onset scoliosis)
Within these four groups of scoliosis, some of the pain-like symptoms can vary depending on the size of the curve and how far the progression leads to overlapping risk profiles in the thoracic and lumbar spine portions. (Aebi, 2005) Some of the symptoms that are associated with scoliosis are back pain. Many individuals with scoliosis, especially adolescent individuals, have back pain associated with adolescent idiopathic scoliosis due to increasing age, injuries, and how severe the spine is curved. (Achar & Yamanaka, 2020) Additional symptoms that many individuals experience with scoliosis that can affect their bodies have specific features that cause pain. Individuals with scoliosis often have increasing asymmetrical pain when standing for prolonged periods and residing at rest, thus mimicking sciatica pain. (Zaina et al., 2023) This is because pain is one of the biomarkers for scoliosis. When pain starts to affect the body, issues like muscle dysfunction, concave disc pressure, asymmetrical facet joint strains, and a high BMI (body mass index) become the main mechanical parameters in the body. They are assessed by doctors when being examined. (Ilharreborde et al., 2023) When individuals are being assessed by their doctors to manage scoliosis, non-surgical treatments can help manage the pain-like symptoms and restore joint stability and mobility to the body.
Movement Medicine: Chiropractic Care- Video
Various Exercises For Managing Scoliosis
When many individuals dealing with scoliosis go in for non-surgical treatments, they will be assessed and evaluated by pain specialists to determine what the next steps for treatment can be provided for them. For scoliosis, non-surgical treatments like chiropractic care can be provided to reduce the musculoskeletal conditions associated with scoliosis. Chiropractors utilize mechanical and manual spinal manipulation of the spine. They can set the vertebra back in place while restoring the spinal joint with optimal motion, improving the range of motion, and allowing the body to function properly. (Milne et al., 2022) At the same time, chiropractors can recommend various exercises and stretches to help manage symptoms associated with scoliosis as part of their treatment plan. Incorporating various exercises can help rectify spinal deformity, help the different muscle groups become stronger, and allow the individual to work a bit on managing scoliosis symptoms. Below are some of the various exercises and stretches to manage scoliosis.
Practicing Good Posture
Practicing good posture can benefit many individuals with scoliosis, especially young ones. Many people realize that maintaining good posture can help reduce muscle pain and tension in the back. It allows many people to realign their bodies and retrain them to stand with good posture naturally. Maintaining good posture, whether standing or seated, can allow doctors to scan the body for any tension signs. For those with scoliosis, it can gradually strengthen the weak core muscles in their bodies.
Abdominal Presses
Abdominal presses allow the individual to maintain neutral spinal alignment while strengthening the abdominal core muscles. To do this:
Individuals must lie on their backs on a yoga mat, keeping their backs in a neutral, tension-free position with bent knees.
They raise both feet and thighs off the mat to form a 90-degree angle with their knees above the hips. *They can support themselves with a chair or wall.
Next, individuals can use their hands to push and pull the knees with their abdominal muscles.
When doing this static exercise, make sure that they hold for three full breaths in two sets of ten and relax in between.
Bird-Dog
Bird-dog is a yoga move that can help stretch tight and weak muscles in the back and allow the body to balance itself. To do this:
Individuals can be on their hands and knees with a neutral spine position on a yoga mat, ensuring their hands are under their shoulders and their knees are under their hips.
With controlled breathing, extend one arm straight out while extending the opposite leg back.
Maintain the position for five to thirty seconds, andslowly return to the neutral spine.
Repeat the motion with the opposite for 10 to 15 reps.
Incorporating these exercises can help manage pain-like symptoms associated with scoliosis, help many individuals strengthen their weak muscles, and help improve their posture on their health and wellness journey.
Ilharreborde, B., Simon, A. L., Shadi, M., & Kotwicki, T. (2023). Is scoliosis a source of pain? J Child Orthop, 17(6), 527-534. https://doi.org/10.1177/18632521231215861
Janicki, J. A., & Alman, B. (2007). Scoliosis: Review of diagnosis and treatment. Paediatr Child Health, 12(9), 771-776. https://doi.org/10.1093/pch/12.9.771
Milne, N., Longeri, L., Patel, A., Pool, J., Olson, K., Basson, A., & Gross, A. R. (2022). Spinal manipulation and mobilisation in the treatment of infants, children, and adolescents: a systematic scoping review. BMC Pediatr, 22(1), 721. https://doi.org/10.1186/s12887-022-03781-6
Zaina, F., Marchese, R., Donzelli, S., Cordani, C., Pulici, C., McAviney, J., & Negrini, S. (2023). Current Knowledge on the Different Characteristics of Back Pain in Adults with and without Scoliosis: A Systematic Review. J Clin Med, 12(16). https://doi.org/10.3390/jcm12165182
Could learning to apply healthy sleep hygiene habits help improve sleep and overall health for individuals with sleeping difficulties?
Contents
Primary Insomnia
Insomnia affects most adults at some point in their lives. Primary insomnia is a fairly common condition characterized by difficulty sleeping, and sometimes, it can resolve without treatment. A diagnosis of primary insomnia means that there is no need to worry that a medical or psychological issue is causing sleep problems. Secondary insomnia is the result of medication side effects or medical or psychological issues. However, individuals may need a diagnostic evaluation, including blood tests or an overnight sleep study, to determine an underlying cause for persistent insomnia. Managing lifestyle habits is usually effective for the relief of primary insomnia. If that doesn’t work, medical treatment may be recommended.
Symptoms
Primary insomnia means not getting enough sleep. Individuals with primary insomnia average six hours of sleep per night (Flynn-Evans E. E. et al., 2017). They often toss and turn or get out of bed frequently. Typically, primary insomnia makes it hard to fall asleep and/or stay asleep. Individuals can wake up easily by triggers like noises or even without triggers. Sleep deprivation can lead to several health problems when awake. Symptoms of insomnia fatigue include: (Salisbury-Afshar E. 2018)
Trouble waking up in the morning
Constant yawning
Feeling tired and sleepy throughout the day
Lack of energy for physical activity
Lack of motivation
Hunger
Difficulty concentrating
Irritability
Headaches
Hypersomnia or falling asleep during the day
Sensitivity to noise or lights when awake
Bouts of hyperactivity
Jumpiness
Being easily alarmed or frightened
Individuals can experience these symptoms for a few days in a row and resolve the day after a restful night of sleep or after a nap. There are times when fatigue can help with falling asleep, which helps to resolve insomnia.
Complications
Individuals can develop severe anxiety and distress about the fact that they are not getting enough sleep. This anxiety is usually more severe before going to bed or in the middle of the night, but the worry can continue during the day as well. Persistent insomnia and chronic lack of sleep can lead to depression and predispose the mind and body to health complications. (Sun, Q., & Tan, L. 2019) Insufficient sleep is associated with lowered immune system function, obesity, and heart disease. (Hung C. M. et al., 2018)
Causes
The conundrum of primary insomnia is that it does not have an identifiable cause, but certain risk factors predispose individuals to have primary insomnia. The condition persists throughout a person’s life, often worsening or improving for months or years. Primary insomnia can be more common among those who have family members with insomnia. Research has found that, while primary insomnia isn’t caused by psychiatric issues, tending to stress or a worry-prone personality might be predisposing factors. (Hung C. M. et al., 2018)
Circadian Rhythm
Research has found that primary insomnia is associated with circadian rhythm irregularities. It can result from individuals falling into deeper sleep phases earlier than those who don’t have the condition (Flynn-Evans E. E. et al., 2017). However, it can be challenging to know whether early deep sleep is a cause or an effect of primary insomnia. This is because sleep deprivation can also lead to abrupt or rapid onset of deep sleep.
Diagnosis
Getting enough sleep is a common concern throughout life. Diagnosing primary insomnia involves various steps. One of the main components of identifying insomnia is determining whether the individual needs more sleep than they are getting. For individuals who are unable to get the proper amount of sleep, the second aspect of primary insomnia diagnosis is focused on finding the reason for their lack of sleep. Diagnostic tests measure insomnia and its effects and include:
Sleep Study
A polysomnogram is an overnight sleep study measuring brain activity, muscle activity, and breathing.
The polysomnogram is expected to show decreased sleep and normal breathing patterns if it is primary insomnia. (Sun, Q., & Tan, L. 2019)
Pittsburgh Sleep Quality Index
The PSQI is a questionnaire that includes a self-assessment of sleep.
It helps identify sleep patterns and issues like using the bathroom frequently at night.
Multiple Sleep Latency Test
An MSLT is a daytime nap study in which participants are monitored to determine how fast they fall asleep.
The test results are a reflection of your sleep deprivation.
These studies help assess whether an individual is not getting enough sleep and what type of sleep interruption is experienced. Other tests might include screening questionnaires or other assessments of emotional issues like depression and anxiety. Sometimes, individuals are aware of these problems but may dismiss symptoms of depression and anxiety, and they instead manifest as insomnia.
Individuals might need to have tests to determine whether any of these underlying issues are contributing to their insomnia. Individual medical symptoms and physical examination would guide the diagnostic testing.
Sleep Hygiene Habits
Individuals can start making small lifestyle adjustments to help regulate their sleep. The key is to avoid things that prevent falling asleep when you want to. Healthy habits include:
Avoid caffeine in the afternoon or evening.
Avoid alcohol.
Avoid napping during the day.
Don’t turn on a phone, computer, or television screen in the bedroom before bed.
Staying away from bright lights for several hours before sleep.
Scheduling tasks so you feel caught up before going to sleep.
Getting enough to eat so you aren’t hungry before going to bed.
Not eating so much that you feel bloated before going to bed.
Doing some light exercise several hours before going to bed.
Medical Treatment
If lifestyle habits don’t help alleviate insomnia, talk to a healthcare provider about medical therapy. Some notice a benefit from treatment with non-prescription-based strategies like counseling, cognitive behavioral therapy for insomnia (CBT-I), or acupuncture. These approaches can have a longer-lasting effect without the risk of side effects. (Salisbury-Afshar E. 2018) A healthcare provider might recommend melatonin or may prescribe medication such as antidepressants, antihistamines, or benzodiazepines.
Injury Medical Chiropractic and Functional Medicine Clinic
Navigating insomnia can be challenging, but understanding the treatment process can significantly help the individual. A healthcare provider can determine the most effective treatment strategies. This can include physical therapy, rest, health coaching, and medication. Overcoming these limitations is possible. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Building a Stronger Body
References
Flynn-Evans, E. E., Shekleton, J. A., Miller, B., Epstein, L. J., Kirsch, D., Brogna, L. A., Burke, L. M., Bremer, E., Murray, J. M., Gehrman, P., Rajaratnam, S. M. W., & Lockley, S. W. (2017). Circadian Phase and Phase Angle Disorders in Primary Insomnia. Sleep, 40(12), 10.1093/sleep/zsx163. https://doi.org/10.1093/sleep/zsx163
Salisbury-Afshar E. (2018). Management of Insomnia Disorder in Adults. American Family Physician, 98(5), 319–322.
Sun, Q., & Tan, L. (2019). Comparing primary insomnia to the insomnia occurring in major depression and general anxiety disorder. Psychiatry Research, 282, 112514. https://doi.org/10.1016/j.psychres.2019.112514
Hung, C. M., Li, Y. C., Chen, H. J., Lu, K., Liang, C. L., Liliang, P. C., Tsai, Y. D., & Wang, K. W. (2018). Risk of dementia in patients with primary insomnia: a nationwide population-based case-control study. BMC psychiatry, 18(1), 38. https://doi.org/10.1186/s12888-018-1623-0
Guo, H. M., Liu, M., Xiang, Y. T., Zhao, J., Ungvari, G. S., Correll, C. U., Ng, C. H., Chiu, H. F., & Duan, Z. P. (2017). Insomnia in Adults With Chronic Hepatitis B, Liver Failure, and Cirrhosis: A Case-Control Study. Perspectives in psychiatric care, 53(1), 67–72. https://doi.org/10.1111/ppc.12138
Can incorporating natural probiotic foods help improve many people’s gut health and restore functionality to their bodies?
Contents
Introduction
Many people trying a healthier lifestyle will start incorporating more nutritious options to ensure the body and the gut get the necessary nutrients. When it comes to gut health, many people will begin to notice how they have more energy and will also start to see how different foods can affect their health. The gastrointestinal system plays a huge role in many people’s health and wellness and is associated with many environmental factors that can impact the body. When that happens, many people can incorporate probiotics to help with gut health. In today’s article, we will dive into how gut health impacts the body, how probiotics improve gut health, and how people can incorporate probiotic-rich foods into their diet. We discuss with certified medical providers who inform our patients how incorporating probiotics can help improve gut health. While asking informed questions to our associated medical providers, we advise patients to include foods rich in probiotics to reduce overlapping risk profiles affecting the gut. Dr. Alex Jimenez, D.C., encompasses this information as an academic service. Disclaimer.
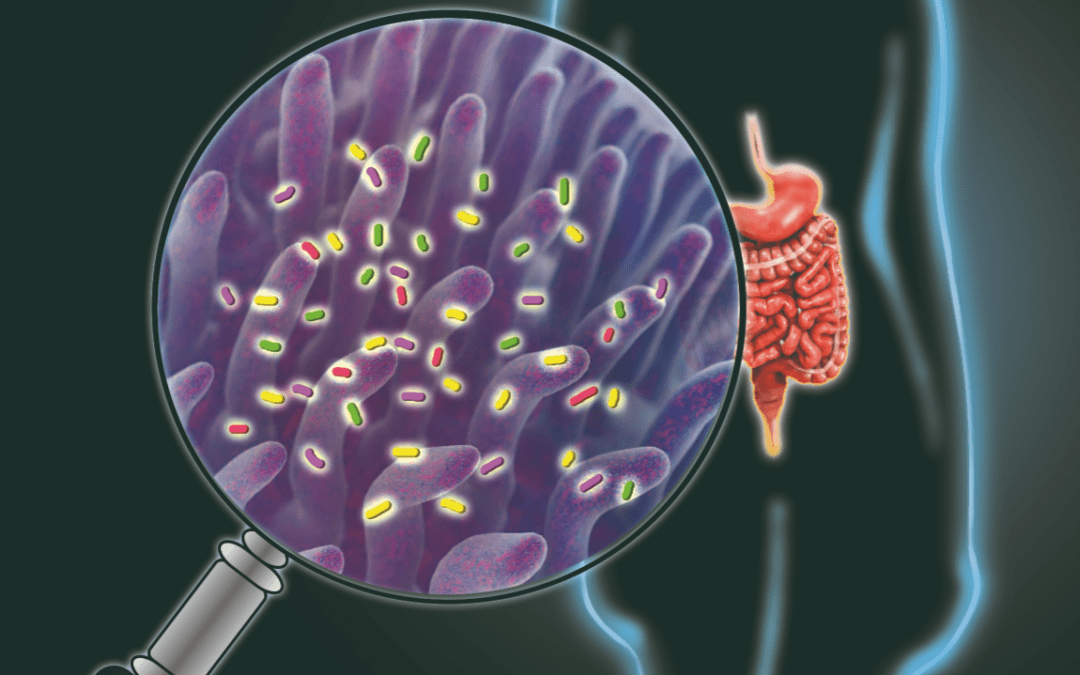
How Gut Health Impacts The Body
Do you feel sluggish and full constantly after a heavy meal? Do you notice red imperfections in your skin after eating a certain food item? Or have you experienced constant cold and flu symptoms impacting your daily routine? Many do not realize that the overlapping risk profile scenarios affecting their bodies correlate with the gut system. The gut system is the second brain in the human body and can also be impacted by pathogens and environmental factors. The gastrointestinal (GI) tract is home to abundant microorganisms that form an intricate and mutual relationship that benefits the body. (Thursby & Juge, 2017) Inside the GI tract, numerous bacteria help with food digestion and transport the nutrients to different body areas. When the gut system deals with alterations in its microbial communities, it can negatively impact the functional structures of the gut’s composition and function. (Yoon & Yoon, 2018)
This means that when bad bacteria are abundant in the gut system, it can cause the body to be dysfunctional and, over time, can develop chronic issues like inflammation and gut dysbiosis. Environmental factors like stress, poor dieting, and physical inactivity can impact the gut. They can be potentially harmful through these abnormal chances, causing the bad bacteria to overflow the good bacteria, allowing the immune system to attack the gut system. (Zhang et al., 2015) When this happens, many people start to feel symptoms of pain and discomfort in their bodies and start looking for ways to reduce these pain-like symptoms while improving their gut health.
Balance Body & Metabolism- Video
How Probiotics Improve Gut Health
When it comes to reducing pain-like symptoms in the body, it is also important to improve gut health. One way to improve gut health is by incorporating probiotics into a healthy diet. Probiotics have beneficial organisms that can provide helpful properties by stimulating the growth and activities of good bacteria in the gut. (Li et al., 2021) Probiotics can help line the gut while boosting the immune system, allowing the GI tract to absorb the nutrients a person eats. At the same time, different strains of probiotics can impact the gut barrier, the immune system, and cognitive function in the body. (Wieers et al., 2019) Additionally, many people can incorporate probiotic-rich foods into their diet.
Probiotic-Rich Foods To Try
There are some benefits when it comes to incorporating probiotic-rich foods into a diet, as probiotics play a role in hosting innate and adaptive immune responses, which occur mainly on the surface of the intestinal barrier. (Mazziotta et al., 2023) Some of the benefits of consuming probiotic-rich foods include:
Restoring the natural balance of gut bacteria
Strengthening immune system
Reduces cholesterol levels
Heals Leaky gut
Some the foods like kefir, yogurt, sauerkraut, miso, and kimchi are great examples of probiotic-rich foods as they can be incorporated into any healthy diet and can help produce a higher abundance of health-promoting bacteria to increase gut microbiome diversity and enhance a person’s activity levels. (Jager et al., 2019) When people start incorporating probiotics into their health and wellness journey, they will notice that their energy levels are maintained during their daily activities and that their gut health is optimal. As stated earlier, the gut is known as the second brain in the body, so when pathogens and environmental factors start to cause issues to the gut, the body feels it. But if probiotics are introduced to the gut, the gut and body are happy.
References
Jager, R., Mohr, A. E., Carpenter, K. C., Kerksick, C. M., Purpura, M., Moussa, A., Townsend, J. R., Lamprecht, M., West, N. P., Black, K., Gleeson, M., Pyne, D. B., Wells, S. D., Arent, S. M., Smith-Ryan, A. E., Kreider, R. B., Campbell, B. I., Bannock, L., Scheiman, J.,…Antonio, J. (2019). International Society of Sports Nutrition Position Stand: Probiotics. J Int Soc Sports Nutr, 16(1), 62. https://doi.org/10.1186/s12970-019-0329-0
Li, H. Y., Zhou, D. D., Gan, R. Y., Huang, S. Y., Zhao, C. N., Shang, A., Xu, X. Y., & Li, H. B. (2021). Effects and Mechanisms of Probiotics, Prebiotics, Synbiotics, and Postbiotics on Metabolic Diseases Targeting Gut Microbiota: A Narrative Review. Nutrients, 13(9). https://doi.org/10.3390/nu13093211
Mazziotta, C., Tognon, M., Martini, F., Torreggiani, E., & Rotondo, J. C. (2023). Probiotics Mechanism of Action on Immune Cells and Beneficial Effects on Human Health. Cells, 12(1). https://doi.org/10.3390/cells12010184
Thursby, E., & Juge, N. (2017). Introduction to the human gut microbiota. Biochem J, 474(11), 1823-1836. https://doi.org/10.1042/BCJ20160510
Wieers, G., Belkhir, L., Enaud, R., Leclercq, S., Philippart de Foy, J. M., Dequenne, I., de Timary, P., & Cani, P. D. (2019). How Probiotics Affect the Microbiota. Front Cell Infect Microbiol, 9, 454. https://doi.org/10.3389/fcimb.2019.00454
Zhang, Y. J., Li, S., Gan, R. Y., Zhou, T., Xu, D. P., & Li, H. B. (2015). Impacts of gut bacteria on human health and diseases. Int J Mol Sci, 16(4), 7493-7519. https://doi.org/10.3390/ijms16047493
Experiencing a whiplash injury can be disorienting and painful. Can recognizing the signs of more serious complications, seeking timely medical intervention, and following a structured whiplash rehabilitation plan help individuals find relief and restore function and quality of life?
Contents
Whiplash Rehabilitation
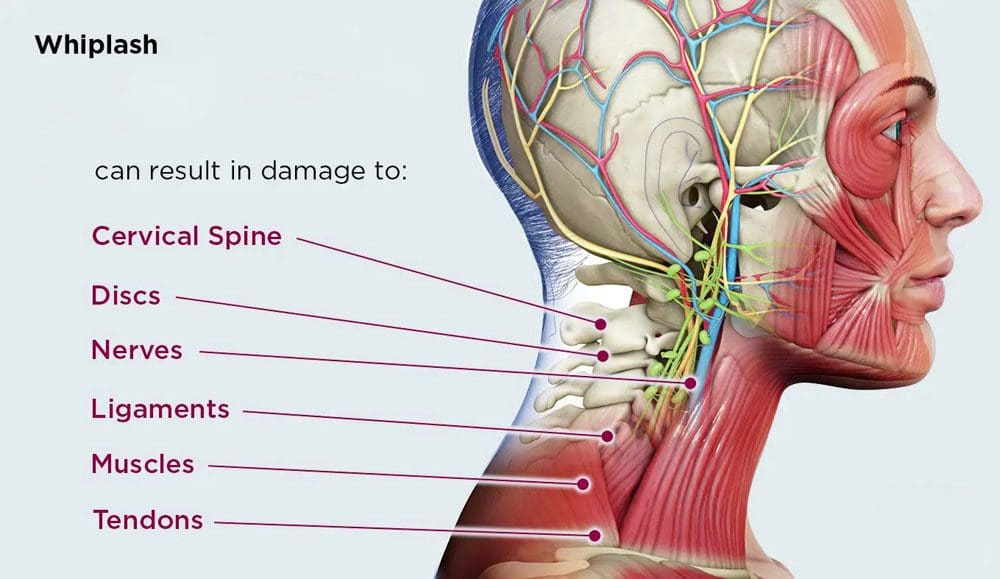
For individuals who have recently been in an automobile accident, once the initial neck pain and stiffness have passed, it’s crucial to recognize potential delayed symptoms, such as nerve damage. While many recover quickly, some may experience prolonged symptoms requiring more aggressive treatment and management.
Neck Injury
Whiplash injuries result from sudden, forceful whipping back and forth of the head, commonly occurring in rear-end vehicle collisions, and are one of the most common neck injuries. Other potential causes include: (Johns Hopkins Medicine, 2024)
Following a healthcare provider’s recommendations regarding medication use, including dosage and duration, is critical to managing symptoms while effectively minimizing potential side effects.
Rehabilitation Steps
To determine the appropriate treatment whiplash rehabilitation plan, a healthcare provider will assess how much the pain affects daily life, including mental health and the ability to do regular activities (American Academy of Physical Medicine and Rehabilitation, 2024). X-rays or other imaging tests will be done to determine how serious the damage to the neck or spine is. Resting and icing the injured area are recommended to relieve inflammation. A provider may recommend slowly increasing neck movements several times daily and continuing with normal daily activities, as exercise will help maintain flexibility. Not moving the neck may prolong pain, stiffness, and healing. Physical therapy may be recommended if symptoms continue for over one or two weeks. (American Academy of Physical Medicine and Rehabilitation, 2024)
Symptoms last longer than the healthcare provider estimated
Other symptoms develop, like weakness, numbness, or a sensation of pins and needles.
Long-Term Injury Side Effects
Individuals in whiplash rehabilitation usually recover in a few weeks to months, but some may have longer-lasting pain as the injury can cause nerve damage. (Fundaun J. et al., 2022) Discuss any new or worsening symptoms with a healthcare provider for guidance. (Johns Hopkins Medicine, 2024)
Over-the-counter pain relievers, such as acetaminophen or NSAIDs.
Muscle relaxants for tightness and tension.
Prescription pain medications.
If pain becomes chronic, antidepressants such as serotonin and norepinephrine reuptake inhibitors may be prescribed. These medications can help manage pain and improve sleep quality. (Ferreira G. E. et al., 2023) For severe inflammation and pain, corticosteroid injections directly into the affected area can provide relief. Healthcare providers administer these injections, offering long-lasting effects. (Harvard Health Publishing, 2015)
Injury Medical Chiropractic and Functional Medicine Clinic
Navigating a whiplash injury can be challenging, but understanding the whiplash rehabilitation process can significantly aid in recovery. A healthcare provider can determine the most effective treatment strategies. It is important to talk with a healthcare provider to determine the cause and extent of the injury to provide individualized patient education regarding treatment. This can include physical therapy, rest, health coaching, medication, and surgery, which may be recommended in certain cases. Overcoming these limitations is possible. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
American Academy of Physical Medicine and Rehabilitation. (2024). Cervical whiplash. https://www.aapmr.org/about-physiatry/conditions-treatments/musculoskeletal-medicine/cervical-whiplash
Rush University Medical Center. (2014). 5 facts about whiplash. https://www.rush.edu/news/5-facts-about-whiplash
National Library of Medicine. MedlinePlus. (2024). Whiplash. Retrieved from https://medlineplus.gov/ency/imagepages/9853.htm
National Health Service NHS. (2023). Whiplash. https://www.nhs.uk/conditions/whiplash/
University of Rochester Medical Center. (2024). Whiplash injury. https://www.urmc.rochester.edu/encyclopedia/content.aspx?contenttypeid=85&contentid=p01388
National Library of Medicine. MedlinePlus. (2020). Pregabalin. Retrieved from https://medlineplus.gov/druginfo/meds/a605045.html
Fundaun, J., Kolski, M., Baskozos, G., Dilley, A., Sterling, M., & Schmid, A. B. (2022). Nerve pathology and neuropathic pain after whiplash injury: a systematic review and meta-analysis. Pain, 163(7), e789–e811. https://doi.org/10.1097/j.pain.0000000000002509
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2023). Back pain: diagnosis, treatment, and steps to take. Retrieved from https://www.niams.nih.gov/health-topics/back-pain/diagnosis-treatment-and-steps-to-take
Ferreira, G. E., Abdel-Shaheed, C., Underwood, M., Finnerup, N. B., Day, R. O., McLachlan, A., Eldabe, S., Zadro, J. R., & Maher, C. G. (2023). Efficacy, safety, and tolerability of antidepressants for pain in adults: overview of systematic reviews. BMJ (Clinical research ed.), 380, e072415. https://doi.org/10.1136/bmj-2022-072415
Harvard Health Publishing. (2015). New recommendations aim to improve safety of pain-relieving spinal steroid injections. Harvard Health Publishing
Harvard Medical School. https://www.health.harvard.edu/blog/new-recommendations-aim-to-improve-safety-of-pain-relieving-spinal-steroid-injections-201505077991
Individuals dealing with fibromyalgia can find natural remedies to reduce the pain-like symptoms and provide relief to their bodies?
Contents
Introduction
When it comes to the immune system in the human body, it is the number one defender in healing the body naturally from chronic illness or injuries to which the host has succumbed. When the body is dealing with unwanted pathogens, the immune system sends out inflammatory cytokines to attach to the affected area, allowing the healing process to take effect. However, when environmental factors or pathogens develop inside the body over time, the immune system can become confused and begin to attack healthy cells; when this happens, the body can develop autoimmune diseases. This causes chronic issues and overlapping risk profiles to develop and cause the body to succumb to pain and discomfort. Autoimmune diseases like fibromyalgia can affect the various muscles in the body and cause a person to be in tremendous amounts of pain. Luckily, there are different natural remedies to dampen the pain-like effects of fibromyalgia. In today’s article, we are looking at the impact of fibromyalgia on the body and how various natural remedies can help reduce fibromyalgia flare-ups. We discuss with certified medical providers who inform our patients how fibromyalgia can affect the body and be correlated with pain-like symptoms. While asking informed questions to our associated medical providers, we advise patients to incorporate various natural remedies to reduce the chances of fibromyalgia causing more issues in the body. Dr. Alex Jimenez, D.C., encompasses this information as an academic service. Disclaimer.
How Fibromyalgia Affects The Body
Have you been dealing with pain and discomfort in different areas of your body? Do you feel exhausted throughout the day despite having a good night’s rest? Or have you been dealing with constant migraines that you would rather stay in bed all day? Many pain-like scenarios are associated with musculoskeletal conditions that can affect the entire body through painful sensations. However, musculoskeletal conditions have a casual relationship with not only environmental factors but also with autoimmune diseases like fibromyalgia. Now, fibromyalgia is characterized by chronic and widespread musculoskeletal pain and can be associated with hypersensitivity processing to pain in the brain. (Siracusa et al., 2021) This is because many factors like genetics, environmental, hormonal, neural, and immunological are all associated with fibromyalgia and can cause the neuron signals to be haywire and hypersensitive to the body. (Garcia Rodriguez & Abud Mendoza, 2020) When that happens, the body begins to experience musculoskeletal pain-like symptoms like muscle-joint stiffness and fatigue that can cause the vagus nerve to be in a constant hyperactive state in the body.
Additionally, since fibromyalgia is an autoimmune disease, the role of the immune system and inflammation also come into play as the body produces altered levels of pro-inflammatory cytokines to dysregulate neuro-sensitizing molecules and affect the small nerve fibers in the body (Clauw et al., 2024). Unfortunately, when doctors diagnose fibromyalgia, comorbidities can cause overlapping risk profiles in the body. Fortunately, there are numerous treatments and natural remedies available to reduce and manage pain-like symptoms associated with fibromyalgia.
Fibromyalgia: Food Choices & Neutraceutical Options- Video
Natural Remedies To Reduce Fibromyalgia
When it comes to finding numerous ways to reduce the pain-like effects of fibromyalgia, many people seek out over-the-counter medicine to reduce the musculoskeletal pain associated with fibromyalgia, which can provide temporary relief. Luckily, there are natural remedies that can improve overall fibromyalgia symptoms that can improve the global functioning of the body, pain reduction, psychological relief, and brain activity. (Assavarittirong et al., 2022) Many natural remedies for fibromyalgia include:
Incorporating vitamins and supplements
Making small changes in diet and lifestyle
Utilizing non-surgical treatments
Supplements
When it comes to reducing fibromyalgia flare-ups, many people wonder where to start on their health and wellness journey. The best way to start making small changes to their health and reducing fibromyalgia flare-ups is by incorporating vitamins and supplements. Vitamins and supplements can help the body by incorporating the necessary nutrients that the body needs to provide energy and function to the muscles, tissues, bones, and vital organs. When it comes to incorporating various vitamins and supplements to reduce fibromyalgia symptoms, many people have started incorporating vitamin D to boost the immune system and reduce muscle impairment in tissue structure and function. (Lombardo et al., 2022) This is because when individuals are dealing with fibromyalgia flare-ups, they experience extreme muscle pain, and it spreads throughout the entire body. At the same time, many people can also incorporate magnesium as part of the regime to reduce fibromyalgia. When people start to integrate magnesium, they will experience reduced symptoms of muscle pain, fatigue, anxiety, and improved sleep difficulties. (Boulis et al., 2021) By incorporating vitamins and supplements into individuals with fibromyalgia, they will begin to notice over time that the symptoms associated with fibromyalgia are reduced.
Diet & Lifestyle Changes
Another way for individuals dealing with fibromyalgia is by incorporating a diet that has anti-inflammatory properties and lifestyle changes that can be customized for the person’s treatment plan. When it comes to the diet portion of reducing fibromyalgia, many wonder how to start. Since a healthy diet is crucial for a natural treatment to reduce fibromyalgia, the main goal is to reduce the inflammatory effects associated with fibromyalgia. When people start incorporating fruits and vegetables that have been shown not only to reduce oxidative stress but also to reduce the inflammatory markers caused by fibromyalgia. (Lowry et al., 2020) While incorporating a healthy diet containing anti-inflammatory foods, exercising and utilizing non-surgical treatments also play a crucial role in managing fibromyalgia. When it comes to exercising can be a multimodal treatment as it can help create a physiological response that decreases the sympathetic activity and shifts the parasympathetic activity that relaxes the muscular and nervous system, thus reducing the stress levels of individuals with fibromyalgia. (Metyas et al., 2024) This allows people to manage their symptoms and make small changes in their health and well-being. At the same time, they can incorporate non-surgical treatments like chiropractic care and acupuncture to realign the body and reduce symptoms of stiffness and pain correlated with fibromyalgia. By doing so and managing their fibromyalgia symptoms, many people can begin taking back their health and wellness with these natural remedies for their fibromyalgia.
References
Assavarittirong, C., Samborski, W., & Grygiel-Gorniak, B. (2022). Oxidative Stress in Fibromyalgia: From Pathology to Treatment. Oxid Med Cell Longev, 2022, 1582432. https://doi.org/10.1155/2022/1582432
Boulis, M., Boulis, M., & Clauw, D. (2021). Magnesium and Fibromyalgia: A Literature Review. J Prim Care Community Health, 12, 21501327211038433. https://doi.org/10.1177/21501327211038433
Clauw, D., Sarzi-Puttini, P., Pellegrino, G., & Shoenfeld, Y. (2024). Is fibromyalgia an autoimmune disorder? Autoimmun Rev, 23(1), 103424. https://doi.org/10.1016/j.autrev.2023.103424
Garcia Rodriguez, D. F., & Abud Mendoza, C. (2020). Physiopathology of fibromyalgia. Reumatol Clin (Engl Ed), 16(3), 191-194. https://doi.org/10.1016/j.reuma.2020.02.003 (Fisiopatologia de la fibromialgia.)
Lombardo, M., Feraco, A., Ottaviani, M., Rizzo, G., Camajani, E., Caprio, M., & Armani, A. (2022). The Efficacy of Vitamin D Supplementation in the Treatment of Fibromyalgia Syndrome and Chronic Musculoskeletal Pain. Nutrients, 14(15). https://doi.org/10.3390/nu14153010
Lowry, E., Marley, J., McVeigh, J. G., McSorley, E., Allsopp, P., & Kerr, D. (2020). Dietary Interventions in the Management of Fibromyalgia: A Systematic Review and Best-Evidence Synthesis. Nutrients, 12(9). https://doi.org/10.3390/nu12092664
Metyas, C., Aung, T. T., Cheung, J., Joseph, M., Ballester, A. M., & Metyas, S. (2024). Diet and Lifestyle Modifications for Fibromyalgia. Curr Rheumatol Rev, 20(4), 405-413. https://doi.org/10.2174/0115733971274700231226075717
Siracusa, R., Paola, R. D., Cuzzocrea, S., & Impellizzeri, D. (2021). Fibromyalgia: Pathogenesis, Mechanisms, Diagnosis and Treatment Options Update. Int J Mol Sci, 22(8). https://doi.org/10.3390/ijms22083891
For individuals who are looking for a whipped cream substitute for a dairy-free alternative, what are the options to choose from?
Contents
Whipped Cream Substitute
Individuals may want to use a whipping cream substitute if they have a dairy allergy, prefer a plant-based lifestyle, or are choosing low-fat foods. Whipping cream is made from milk and contains the same proteins found in milk and other dairy products that individuals with a dairy allergy may react to. However, heavy whipping and whipped cream contain small amounts of lactose and are safe for those with lactose intolerance. (University of Virginia, 2022) Because of this, individuals do not need to seek a whipping cream substitute if they are lactose intolerant. Fortunately, there are several dairy-free options and whipping cream alternatives.
Nutrition
The nutrition information for one tablespoon or 15 grams of light whipping cream. (USDA, FoodData Central, 2018)
Whipping and whipped cream are both high in calories due to their high fat content. Dairy fat and heart health have been issues; however, recent research suggests that dairy fat intake is associated with lower cardiovascular disease risk. (Trieu K. et al., 2021)
Substitutes
Coconut Milk
The nutritional value of coconut milk is similar to that of whipping cream. Coconut milk is a vegan and dairy-free alternative to whipped cream. It contains just the right amount of fat for whipping. To make perfect peaks with canned coconut milk, chill the can overnight and beat with a hand or stand mixer until soft and fluffy. Sifted powdered sugar and stevia make the best sweeteners because they will not weigh them down. The coconut milk adds coconut flavor. One tablespoon or 15 grams of coconut milk has 30 calories, 0.3 grams of protein, 3.2 grams of fat, and 0.4 grams of carbohydrates. (USDA, FoodData Central, 2018)
Silken Tofu Pureed with Soy Milk
Another vegan and dairy-free whipping cream substitute is made with silken tofu, soy milk, sugar, and vanilla extract. Because tofu is high in protein and low fat, this alternative is lower in fat than dairy whipping cream but is higher in carbohydrates. To make:
Combine 1 pound of silken tofu, one tablespoon of vanilla extract, and 1/4 cup of sugar in a blender or food processor until smooth.
While the machine is running, gradually add the soy milk until it becomes light and fluffy.
Refrigerate until ready to serve.
Powdered Milk, Vanilla Extract, and Lemon Juice
Combine 1/2 cup cold water, two tablespoons lemon juice, and one teaspoon vanilla extract in a large bowl.
Sprinkle 1/2 cup non-fat powdered milk over the water and beat with an electric mixer or beater for 4 minutes or until stiff.
Then beat in 1/4 cup granulated sugar until it dissolves and the mixture is smooth.
Chill for at least 30 minutes before using.
Powdered milk is dairy, so it is not ideal for plant-based diets or people with dairy allergies.
Evaporated Milk and Lemon Juice
Combine a can of chilled evaporated milk with one teaspoon of lemon juice.
Beat with an electric mixer until smooth and creamy.
Egg Whites, Sugar, and Bananas
Whip two large ripe bananas with two egg whites and three teaspoons of sugar until fluffy.
Be careful not to overbeat.
Flour, Cornstarch, and Milk
A low-fat, low-carb cream. To make:
One cup of almond, rice, low-fat or nonfat dairy milk, and two tablespoons of cornstarch.
Combine with a whisk.
Continue whisking and add one tablespoon of flour until the mixture is smooth.
This preparation is a solid whipping cream substitute for a thickener in recipes.
You may have to experiment to find what works for the recipe and taste, but here are a few options.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a personalized treatment plan. Our providers use an integrated approach to create customized care plans for each patient and restore health and function to the body. Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, nutritionists, and health coaches to provide the most effective clinical treatments.
Chiropractic and Integrative Healthcare
References
University of Virginia. (2022). Lactose Content of Common Dairy Foods. https://med.virginia.edu/ginutrition/wp-content/uploads/sites/199/2022/04/Lactose_Content_of_Common_Foods-4-2022.pdf
Trieu, K., Bhat, S., Dai, Z., Leander, K., Gigante, B., Qian, F., Korat, A. V. A., Sun, Q., Pan, X. F., Laguzzi, F., Cederholm, T., de Faire, U., Hellénius, M. L., Wu, J. H. Y., Risérus, U., & Marklund, M. (2021). Biomarkers of dairy fat intake, incident cardiovascular disease, and all-cause mortality: A cohort study, systematic review, and meta-analysis. PLoS medicine, 18(9), e1003763. https://doi.org/10.1371/journal.pmed.1003763
USDA, FoodData Central. (2018). Nuts, coconut milk, canned (liquid expressed from grated meat and water). Retrieved from https://fdc.nal.usda.gov/food-details/170172/nutrients
Can modified workouts and/or having a personal trainer design an alternate fitness routine while in injury recovery help injured individuals and athletes maintain fitness?
Contents
Maintain Fitness During Injury Recovery
Individuals with personal, work, or sports injuries must take time off to rest, recover, and rebuild. However, there are ways to maintain fitness and endurance levels while unable to engage in full workouts and exercise.
Fitness Base
Injured individuals and athletes will lose a certain amount of fitness during recovery. After all, the body is injured and needs to focus most of its attention on healing to get back to normal. Deconditioning is a fact of life when the body stops exercising, but there are ways to stay active to maintain a fitness base. Individuals can modify or scale back exercise. Before exercising after an injury, get a doctor’s approval. Then, follow their recommendations. (Garber C. E. et al., 2011)
Even if one body part or joint is immobilized, cross-training principles can help individuals discover new ways to stay fit while rehabilitating. The key is to have the right attitude and remain active within tolerance levels until the injury is healed. Trying new things may take some creativity and flexibility, but most find training through injury is possible and not difficult. Here are ways to continue working out while recovering.
Lower Back Injury Workout
Talk with a doctor or sports doctor to understand exercise limitations before modifying workouts. Walking, swimming, or recumbent cycling are generally safe for individuals with a lower back injury. These workouts can help maintain cardiovascular fitness. An example of a modified workout may consist of the following:
Warm up before exercising.
Perform the workout on Monday, Wednesday, and Friday.
Perform each exercise for 30 to 60 seconds with 15 seconds of rest between exercises.
Complete the entire circuit three to four times.
Complete 30 to 60 minutes of non-weight-bearing cardiovascular exercises on Tuesday, Thursday, and Saturday.
Chest Press
Lat Pulldown
Overhead Press
Leg Extension
Wall Sit
Shoulder and Elbow Injury Workout
Shoulder or other upper body injuries often make it possible to continue traditional cardiovascular exercise because the lower body can be fully exercised. Walking, stair climbing, stationary cycling like an under-desk bike, and the elliptical trainer all work. Circuit training routines will maintain strength and power in the non-injured muscles and joints. The following example routine can be done four to five times weekly.
Warm-up.
Perform each exercise for 30 to 60 seconds, allowing 15 seconds of rest between exercises.
Complete the entire routine three to four times.
Stationary cycling for two minutes at a moderate pace and two at a higher intensity.
Leg Press
Elliptical trainer for two minutes at a moderate pace and two at a higher intensity.
Ab Crunches
Walking Lunges
Low Back Extensions
Treadmill walking for two minutes at a moderate pace and two at a higher intensity or incline.
Wall sits
Ankle and Foot Injury Workout
If the doctor approves, individuals can use a rowing machine or a stationary bike with one leg or swim a few laps. As a doctor or physical therapist recommends, individuals may also need an ankle brace or other support. A sports doctor or personal trainer can help recommend other non-weight-bearing cardiovascular exercises for 30 to 60 minutes three times weekly. Here is a sample workout to try:
Warm-up.
Perform the workout on Monday, Wednesday, and Friday.
Perform each exercise for 30 to 60 seconds with 15 seconds rest between exercises.
Complete the workout three to four times.
Leg Extensions
Chest Press
Lat Pulldown
Overhead Press
Seated Cable Rows
Incline Push-Up
Bicycle Crunches
Hanging Leg Raise
Leg and Knee Injury Workout
Leg and knee injuries can be limiting, as most endurance exercise requires flexion and knee joint extension. One-legged cycling or using an upper-body ergometer/handcycle are options. Swimming may be possible if the individual uses a pull buoy to keep them from kicking or using their legs. Here are two circuit workout examples:
Circuit 1
Warm-up.
Perform this on Monday, Wednesday, and Friday.
Perform each exercise for 30 to 60 seconds with 15 seconds of rest between exercises.
Complete the workout three to four times.
Pull-Up or Assisted Pull-Up
Chest Press
Lat Pulldown
Overhead Press
Circuit 2
Warm-up.
Perform the workout on Tuesday, Thursday, and Saturday.
Perform each exercise for 30 to 60 seconds with 15 seconds of rest between exercises.
Complete the workout three to four times.
Seated Russian Twist
Ab Crunch
V-Sit ab exercise
Injury Medical Chiropractic and Functional Medicine Clinic
Individuals may need significant rest time to heal properly, so consult a doctor on the balance of rest and training. Doing the exercises prescribed by the physical therapist during rehabilitation is important. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Treating Ankle Sprains
References
Garber, C. E., Blissmer, B., Deschenes, M. R., Franklin, B. A., Lamonte, M. J., Lee, I. M., Nieman, D. C., Swain, D. P., & American College of Sports Medicine (2011). American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Medicine and science in sports and exercise, 43(7), 1334–1359. https://doi.org/10.1249/MSS.0b013e318213fefb
Is applying ice the best option for individuals who experience an acute back strain injury?
Contents
Temperature Treatment
Ice temperature treatment, also known as cryotherapy or cold therapy, is a treatment that uses freezing temperatures to reduce pain and swelling. It can be applied in a variety of ways, including:
Ice packs:
Ice massage
Coolant sprays
Whirlpools
Ice baths
Ice is usually recommended for acute injuries and is a common and simple way to treat pain and swelling. Individuals can buy freezable gel packs or make their own with ice cubes in a plastic bag or towel. Heat therapy tends to be used more with chronic issues involving muscle spasms to increase blood circulation.
How Ice Relieves Pain and Reduces Inflammation
Ice temperature treatment works by:
Narrowing blood vessels slows blood circulation to the injured area and soft tissues and reduces swelling.
Reduced blood flow also helps control excessive swelling.
Ice has a short-term analgesic-numbing effect. The coldness numbs nerve endings, relieving pain symptoms.
Relieving the pain allows the muscles to relax.
Controlling blood circulation helps control pain by reducing the flow of irritating chemicals that can inundate the injury site. These chemicals are a natural and the correct response to inflammation, but the ice keeps them in check to help control pain.
After a Back Injury
For a back strain injury, ice and anti-inflammatory medication like NSAIDs are the first line of treatment during the inflammatory phase, which usually lasts 24 to 72 hours. Because heat can increase inflammation by increasing blood circulation, it is not recommended as an initial treatment. After the first few days, most doctors and pain specialists recommend using ice or heat, depending on the individual’s preference. While researchers continue to investigate the best ways to treat acute injuries, most doctors still recommend ice as the first line of defense for back injuries.
A review of studies evaluated 20 different treatment categories to learn about their safety and effectiveness. (McIntosh G. & Hall H. 2011) Treatments included over-the-counter pain medications, acupuncture, McKenzie exercises, other back exercises, and temperature treatments. Regarding temperature treatment, the review found moderate evidence that using a heat wrap 5 days after the injury could help relieve pain. However, there was not enough evidence to support the effectiveness of any of the temperature treatments, necessitating more research. (McIntosh G. & Hall H. 2011)
Physical Therapy and Activity
The review found that prolonged rest should be avoided, and gentle exercise and a progressive return to physical activity should be encouraged to achieve the best outcomes for pain relief and restoring function. Staying active significantly reduces time off from work and chronic disability for up to 1 year compared to traditional medical treatment. (McIntosh G. & Hall H. 2011) Research also found that introducing physical therapy early on could expedite recovery. Mobility work, targeted exercises, and strengthening exercises have been shown to relieve pain, reduce injury recurrence, and improve overall function. More research supports physical activity and exercise as effective treatment options for acute lower back strains. However, further research regarding temperature treatments is required. (French S. D. et al., 2006) (See Q. Y. et al., 2021)
Injury Medical Chiropractic and Functional Medicine Clinic
It is important to talk with a healthcare provider to determine the cause and extent of the injury to provide individualized patient education regarding treatment. This can include physical therapy, rest, health coaching, medication, and surgery, which may be recommended in certain cases. Overcoming these limitations is possible. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Beyond the Surface: Understanding the Effects of Personal Injury
References
McIntosh, G., & Hall, H. (2011). Low back pain (acute). BMJ clinical evidence, 2011, 1102.
French, S. D., Cameron, M., Walker, B. F., Reggars, J. W., & Esterman, A. J. (2006). A Cochrane review of superficial heat or cold for low back pain. Spine, 31(9), 998–1006. https://doi.org/10.1097/01.brs.0000214881.10814.64
See, Q. Y., Tan, J. B., & Kumar, D. S. (2021). Acute low back pain: diagnosis and management. Singapore Medical Journal, 62(6), 271–275. https://doi.org/10.11622/smedj.2021086
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine