Excessive alcohol consumption: what is alcoholic peripheral neuropathy?
Contents
Alcoholic Peripheral Neuropathy
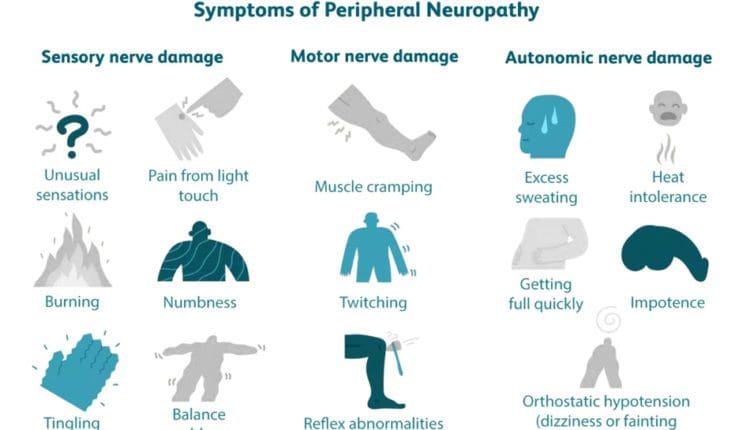
Alcoholic peripheral neuropathy (ALN) is a condition that damages the nerves in the body due to chronic alcohol consumption. It can cause sensory, motor, and autonomic dysfunction, which can lead to disability. This damage prevents the nerves from communicating information. Most symptoms generally start as mild but typically worsen over time as the neuropathy progresses. The most common symptoms are: (National Library of Medicine, 2023)
Numbness or tingling sensation in the extremities
Pain or a burning sensation in the extremities
Difficulty walking
Difficulty urinating
Difficulty talking or swallowing
Affected nerves include the peripheral and autonomic nerves, which help regulate internal body functions. Around 46% of chronic alcohol users will eventually develop the condition. (Julian T., Glascow N., Syeed R., & Zis P. 2019)
Causes
The exact cause of alcoholic neuropathy is unclear. But it is directly related to heavy and long-term alcohol consumption. (Julian T., Glascow N., Syeed R., & Zis P. 2019) It is believed overconsumption of alcohol can directly harm and hinder the nerves’ ability to communicate information. Unhealthy nutritional habits are often associated with it as well. Research shows that decreased thiamine/B vitamin plays a role, while others suggest an overall dietary deficiency may play a role. (Julian T., Glascow N., Syeed R., & Zis P. 2019) However, alcoholic neuropathy can also occur without the presence of malnutrition. (Julian T., Glascow N., Syeed R., & Zis P. 2019)
Neuropathy Development and Progression
Alcoholic peripheral neuropathy develops depending on many factors, including the amount of daily/nightly alcohol consumed, age and overall health, nutritional intake, and other individual factors. In most cases, the neuropathy takes several years or decades to develop, depending on the amount of alcohol consumed.
Pain or burning sensation in the arms, legs, or feet.
Symptoms that occur in the arms and legs typically affect both sides.
Cramps, aches, or weakness of the muscles.
Constipation or diarrhea.
Nausea and vomiting.
Difficulty urinating or incontinence.
Difficulty walking.
Difficulty talking or swallowing.
Heat intolerance.
Erection difficulties.
Most symptoms begin as mild and usually worsen over time as the neuropathy progresses. Alcoholic neuropathy affects individuals who consume excessive amounts of alcohol over a long time. (Julian T., Glascow N., Syeed R., & Zis P. 2019)
Healthcare providers will collect data involving past medical history and all current symptoms.
Physical Exam
This exam looks at other medical conditions contributing to symptoms, like diabetes or high blood pressure.
Neurological Exam
This is a noninvasive exam to determine the location and extent of neurological damage.
Healthcare providers may ask patients several questions and have them complete a series of small movements to check neurological function.
Blood and Urine Tests
These tests can detect diabetes, liver and kidney problems, infections, vitamin deficiencies, and other conditions that can cause neuropathic conditions.
Chronic alcohol use can also affect how the body stores and uses vitamins necessary for healthy nerve function. Vitamin levels that a healthcare provider may check include: (National Library of Medicine, 2023)
Vitamin A
Biotin
Folic acid
Niacin, or vitamin B3
Pyridoxine, or vitamin B6
Pantothenic acid
Liver Disease
Individuals with chronic liver disease often have neuropathy. The severity and stage are associated with a higher incidence of neuropathy. (Pasha MB, Ather MM, Tanveer MA, et al. 2019)
Treatment
Alcoholic neuropathy is not reversible, even when quitting drinking. However, individuals with the condition can make healthy changes to minimize symptoms and receive help for chronic alcohol use. The first step is stopping alcohol consumption. (Chopra K., & Tiwari V. 2012) Talk to a healthcare provider about what options are available. Treatment can include:
In-patient or outpatient rehab
Therapy
Medication
Social support from groups like Alcoholics Anonymous
A combination of treatments will likely be utilized. Other treatment options involve symptom management and preventing further injuries and may include:
Physical therapy
Keeping the head elevated while sleeping.
Orthopedic splints to maintain limb function and positioning.
Wearing compression stockings.
Adding vitamins and supplements.
Eating extra salt for those without hypertension
Medications to reduce pain and discomfort.
Intermittent catheterization or manual expression of urine for those with difficulty urinating.
Individuals with neuropathy may have reduced sensitivity in the arms and legs. If this occurs, additional steps need to be taken to prevent other injuries, that include (National Library of Medicine, 2023)
Wear special footwear to prevent foot injuries.
Checking feet daily for wounds.
Prevent burns by ensuring that bath and shower water is not too hot.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Peripheral Neuropathy Myths and Facts
References
National Library of Medicine. (2023). Alcoholic neuropathy. Retrieved from https://medlineplus.gov/ency/article/000714.htm
Julian, T., Glascow, N., Syeed, R., & Zis, P. (2019). Alcohol-related peripheral neuropathy: a systematic review and meta-analysis. Journal of Neurology, 266(12), 2907–2919. https://doi.org/10.1007/s00415-018-9123-1
National Institute of Neurological Disorders and Stroke. (2024). Peripheral neuropathy. Retrieved from https://www.ninds.nih.gov/health-information/disorders/peripheral-neuropathy
Pasha MB, A. M., Tanveer MA, et al. (2019). Frequency of peripheral neuropathy in chronic liver disease. Med Forum Monthly, 30(8), 23-26. https://medicalforummonthly.com/index.php/mfm/article/view/3761
Chopra, K., & Tiwari, V. (2012). Alcoholic neuropathy: possible mechanisms and future treatment possibilities. British journal of clinical pharmacology, 73(3), 348–362. https://doi.org/10.1111/j.1365-2125.2011.04111.x
For individuals with shoulder pain and problems, what are the stages of a frozen shoulder, how long do they last, and what can be done to relieve pain?
Contents
Frozen Shoulder Stages
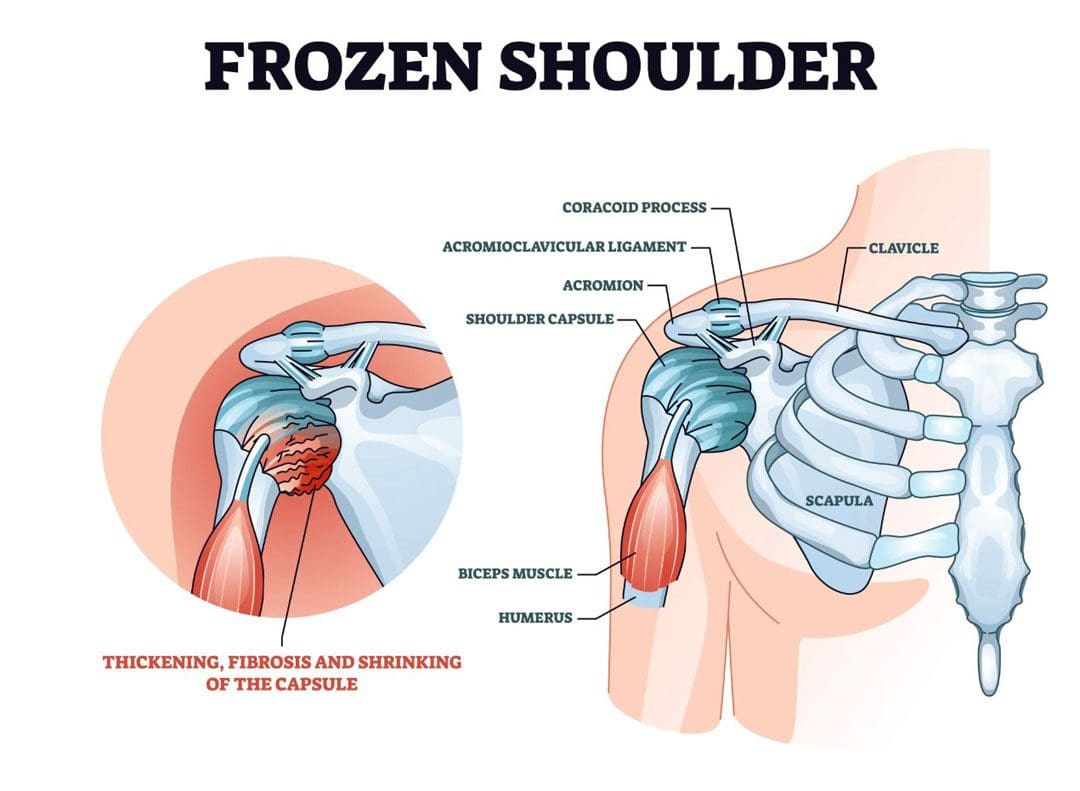
A frozen shoulder, also called adhesive capsulitis, is a very common cause of shoulder pain. It causes severe pain and limited mobility. The condition progresses through stages and can take up to two years to resolve completely. The stages of frozen shoulder include pre-freezing, freezing, freezing, and thawing.
Stage 1
Pre-Freezing – 1 month to 3 months
Pre-freezing describes the earliest stage of a frozen shoulder. This is when individuals first start to notice pain in their shoulder. (Soussahn, S. et al., 2024) Many in this stage will first experience the pain at night while changing sleeping positions. As the condition progresses, individuals may notice pain when they move their shoulders, especially when raising their arms or reaching behind them. Individuals may also find reduced mobility in that shoulder and may ache even when not using it. Because motion may be only slightly restricted in this stage, an early frozen shoulder can be mistaken for a rotator cuff problem. (Chan H. B. Y., Pua P. Y., & How C. H. 2017)
Root Cause
A frozen shoulder happens when there is inflammation in the tissue that surrounds the shoulder joint. Although the specific causes aren’t known, immobilization after an injury and other shoulder conditions, like bursitis, may play a role. (Johns Hopkins Medicine, 2025)
Stage 2
Freezing – 10 weeks to 8 months
The freezing stage is the most painful. The shoulder capsule becomes inflamed and can thicken and stiffen. As this happens, shoulder movements become increasingly difficult and painful. (Soussahn, S. et al., 2024)
Stage 3
Frozen – 4 months to 12 months
The third stage of a frozen shoulder is known as the frozen phase, where the shoulder is stiff. The examination finding confirming the frozen shoulder diagnosis is that neither the individual nor another person can move the shoulder. (UpToDate, 2024) With a rotator cuff issue, a patient cannot move their arm normally, but the healthcare provider can. This distinguishes between a frozen shoulder and a rotator cuff injury. The frozen stage is typically much less painful than freezing, but pain can result from simple activities. (Soussahn, S. et al., 2024) Rotation of the shoulder joint is limited, making activities like washing hair or reaching painful or difficult.
Stage 4
Thawing – 5 months to 2 years
In this phase, the shoulder joint capsule becomes thickened and stiff but gradually loosens with time. (Soussahn, S. et al., 2024) Stretching the shoulder capsule, even allowing for some discomfort, is important to ensure the shoulder joint’s mobility continues to recover. Not having the extreme pain associated with freezing the joint and seeing gradual gains in mobility make this stage tolerable.
Treatment
Frozen shoulder treatment starts with physical therapy and joint stretching. Anti-inflammatory medications, ice and heat application, and alternative therapies can all help manage the discomfort. A healthcare provider may also recommend a corticosteroid injection to reduce inflammation, relieve pain, and expedite improved mobility. Redler L. H. & Dennis E. R. 2019)
Surgery is seldom needed but is an option for treating a frozen shoulder. It is usually only considered if prolonged efforts at therapy have failed to improve symptoms. One of the problems is that surgery could worsen shoulder problems. (Le H. V., Lee S. J., Nazarian A., & Rodriguez E. K. 2017)
Prognosis
The timeline for recovery can be long, measured in months and possibly years. (Le H. V., Lee S. J., Nazarian A., & Rodriguez E. K. 2017) Expecting a quick recovery can cause more frustration. However, individuals can take steps to speed their recovery and reduce discomfort. Physical therapy can be beneficial, and a healthcare provider can suggest treatments to help alleviate pain while recovering. Over time, almost all patients will find complete relief and a normal or near-normal range of motion in their shoulder joints.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Motion Key To Healing
References
Soussahn, S., Hu, D., Durieux, J., Kosmas, C., & Faraji, N. (2024). Adhesive capsulitis: Utility of magnetic resonance imaging as a primary diagnostic tool and clinical management support. Current problems in diagnostic radiology, 53(4), 464–469. https://doi.org/10.1067/j.cpradiol.2024.03.005
Chan, H. B. Y., Pua, P. Y., & How, C. H. (2017). Physical therapy in the management of frozen shoulder. Singapore Medical Journal, 58(12), 685–689. https://doi.org/10.11622/smedj.2017107
UpToDate. (2024). Patient education: Frozen shoulder (beyond the basics). https://www.uptodate.com/contents/frozen-shoulder-beyond-the-basics
Redler, L. H., & Dennis, E. R. (2019). Treatment of Adhesive Capsulitis of the Shoulder. The Journal of the American Academy of Orthopaedic Surgeons, 27(12), e544–e554. https://doi.org/10.5435/JAAOS-D-17-00606
Le, H. V., Lee, S. J., Nazarian, A., & Rodriguez, E. K. (2017). Adhesive capsulitis of the shoulder: review of pathophysiology and current clinical treatments. Shoulder & elbow, 9(2), 75–84. https://doi.org/10.1177/1758573216676786
Can individuals incorporate nutritional snacks to consume before and after to have an effective workout and abundant energy?
Contents
How Can Exercise Help The Body?
When many people start thinking about their health and how to improve it, they usually begin exercising and eating healthier around the last week before the new year to jumpstart their health and wellness journey. These small changes can help the body tremendously as environmental factors like stress, physical inactivity, and various lifestyles can negatively impact the body, thus leading to stress and environmental factors. For individuals dealing with musculoskeletal disorders or autoimmune disorders, exercises and a healthy diet filled with nutritional foods can help mitigate pain-like symptoms and overlapping risk profiles. For individuals with low back pain, core stabilization exercises can help reduce pain and disability while improving core muscle activation to strengthen weak muscles. (Nayyab et al., 2021) As a non-surgical therapy, everyone can exercise for the body, which can help many people reduce any chronic diseases and issues they are dealing with. (Vina et al., 2012) At the same time, a person can exercise at any fitness level by incorporating the right amount of healthy snacks before and after a good workout. We associate with certified medical providers who inform our patients of the importance of having healthy snacks before and after working out to replenish the body and have energy throughout the day. While asking important questions to our associated medical providers, we advise patients to integrate small changes into their daily routine to restore energy through healthy snacking. Dr. Alex Jimenez, D.C., envisions this information as an academic service. Disclaimer.
Secrets of Optimal Wellness- Video
Pre- & Post Workout Benefits
When starting to work out, it is important to ensure that the body is properly fueled with the proper carbohydrates, proteins, and healthy fats that can be converted into energy to perform any exercise routines at full capacity. For athletic individuals, nutrition is closely connected with physical activity and the timing of when the body uses that energy. (Januszko & Lange, 2021) Hence, it is important for individuals starting to work out to consume enough energy through nutritional foods in a pre-workout environment. Pre-workout supplementation can help significantly improve greater changes in body composition and strength. (Cabre et al., 2022) Pre-workouts have benefited from increasing energy, enhancing strength and endurance, and reducing muscle fatigue through supplementation and healthy snacks that give people energy. Post-workouts can help with muscle recovery, and post-workout snacks can help maintain the body’s energy levels throughout the day.
Pre-Workout Snacks
Many dietary supplements for pre-workouts can help with health and performance improvement as they help increase muscle mass and strength while providing energy when exercising. (Brisebois et al., 2022) At the same time, incorporating carbohydrates can provide glycogen energy stored in the liver to provide muscle energy. (Henselmans et al., 2022) It is important to note that eating an hour before working out can give beneficial results. Some of the snacks many people can make and eat before working out include:
Chocolate milk with banana
Frozen grapes
Granola bar
Pretzels
Post Workout Snacks
It is important to restore and maintain that energy in the body when it comes to post-workout snacks after an intense workout. Many athletic and non-athletic individuals can incorporate nutritional carbohydrates and proteins to improve their physiological and biochemical adaptations to promote faster recovery and maintain the body’s hydration status. (Baroni et al., 2023) For instance, coconut water can be an alternative to sports drinks to replenish the body’s electrolytes. (O’Brien et al., 2023) Some of the post-workout snacks that are packed with protein and healthy carbs include:
Smoothies made with fruits, Greek yogurt, and protein powders
Chocolate milk with almonds
Crackers with string cheese
Cottage cheese
References
Baroni, L., Pelosi, E., Giampieri, F., & Battino, M. (2023). The VegPlate for Sports: A Plant-Based Food Guide for Athletes. Nutrients, 15(7). https://doi.org/10.3390/nu15071746
Brisebois, M., Kramer, S., Lindsay, K. G., Wu, C. T., & Kamla, J. (2022). Dietary practices and supplement use among CrossFit(R) participants. J Int Soc Sports Nutr, 19(1), 316-335. https://doi.org/10.1080/15502783.2022.2086016
Cabre, H. E., Gordon, A. N., Patterson, N. D., & Smith-Ryan, A. E. (2022). Evaluation of pre-workout and recovery formulations on body composition and performance after a 6-week high-intensity training program. Front Nutr, 9, 1016310. https://doi.org/10.3389/fnut.2022.1016310
Henselmans, M., Bjornsen, T., Hedderman, R., & Varvik, F. T. (2022). The Effect of Carbohydrate Intake on Strength and Resistance Training Performance: A Systematic Review. Nutrients, 14(4). https://doi.org/10.3390/nu14040856
Januszko, P., & Lange, E. (2021). Nutrition, supplementation and weight reduction in combat sports: a review. AIMS Public Health, 8(3), 485-498. https://doi.org/10.3934/publichealth.2021038
Nayyab, I., Ghous, M., Shakil Ur Rehman, S., & Yaqoob, I. (2021). The effects of an exercise programme for core muscle strengthening in patients with low back pain after Caesarian-section: A single blind randomized controlled trial. J Pak Med Assoc, 71(5), 1319-1325. https://doi.org/10.47391/JPMA.596
O’Brien, B. J., Bell, L. R., Hennessy, D., Denham, J., & Paton, C. D. (2023). Coconut Water: A Sports Drink Alternative? Sports (Basel), 11(9). https://doi.org/10.3390/sports11090183
Vina, J., Sanchis-Gomar, F., Martinez-Bello, V., & Gomez-Cabrera, M. C. (2012). Exercise acts as a drug; the pharmacological benefits of exercise. Br J Pharmacol, 167(1), 1-12. https://doi.org/10.1111/j.1476-5381.2012.01970.x
For individuals who have to be in one position for long periods, have poor postural alignment, and perform repetitive motions, what are myofascial pain syndrome spasm cycles?
Contents
Myofascial Pain Syndrome Spasm Cycles
Myofascial pain syndrome is a common condition that causes pain symptoms in a particular body area (Jafri M. S. 2014). A myofascial pain syndrome spasm cycle is a recurring pattern in which muscle tension and spasms in affected regions, caused by myofascial pain syndrome, lead to pain, triggering more muscle spasms. This creates a vicious cycle of discomfort and tightness that can be difficult to break without treatment; the pain perpetuates muscle spasms and vice versa.
Spasm Pain Cycle
Left untreated, myofascial pain is often experienced as a recurring cycle of spasm, pain, and spasm. (Kojidi M. M. et al., O2016) The exact cause of the spasm is not known. It may be related to excessive accumulation and release of acetylcholine, which causes sustained muscle contraction. (Nicol A, Crooks M, Hsu E, Ferrante M. 2018) Another theory is that repetitive small muscle trauma helps create a trigger point or knot in the muscle. (Thorne. 2021)
Active trigger points in muscles characterize myofascial pain syndrome. (Shah J. P. et al., 2015) These trigger points cause pain in the area where they are located and sometimes in other places, known as referred pain. Each muscle has a particular referral pattern of pain that goes from a trigger point in that muscle to another place in the body. (Shah J. P. et al., 2015) Medical providers and massage therapists trained in this area can identify trigger points by their pain patterns. With myofascial pain syndrome, muscles tense, and joint range of motion may decrease. (Jafri M. S. 2014)
Trigger Points
Myofascial pain syndrome is characterized by trigger points and sensitive knots within muscles that can cause referred pain when pressed, contributing to the spasm cycle.
Muscle Tension
A repeatedly tense or injured muscle can develop trigger points, which can lead tocle tightness and potential spasms.
Pain-Spasm-Pain Cycle
The pain from a trigger point can cause the muscle to further contract and spasm, leading to even more pain and perpetuating the cycle.
How Spasms and Pain Present
Myofascial pain is often caused by long periods of poor postural alignment, muscle injury, and repetitive motions. (Cleveland Clinic, 2023) For example, the upper body slumps forward when sitting at a desk workstation all day. The upper section of the trapezius muscle is located on the back of the neck and the top of the shoulder. The upper trapezius muscle works to raise the head. (Yoo W. G. 2015) The trapezius muscle now has to work more than it is used to. This overuse may cause microscopic muscle injury, leading to muscle spasms and pain. (Bron C., & Dommerholt J. D. 2012) (Nicol A, Crooks M, Hsu E, Ferrante M. 2018) Without treatment, the muscle spasms, pain, and microscopic muscle injury may persist or worsen, leading to trigger points and chronic pain. (Jafri M. S. 2014)
Causes
Repetitive Motions
Repeating the same movement, like typing on a computer, can trigger muscle tension and points.
Poor Posture
Maintaining incorrect posture for extended periods can strain muscles and contribute to trigger point development.
Muscle Injury
Past injuries can leave muscles susceptible to developing trigger points and pain cycles.
Stress
Psychological stress can lead to muscle tension and exacerbate existing trigger points.
Break the Cycle
Physical Therapy
A physical therapist can use stretching, massage, and trigger point therapy to release muscle tension and address trigger points.
Exercise
Regular exercise, including gentle stretching, can help improve muscle flexibility and reduce tension.
Heat Therapy
Applying heat to affected areas can help relax muscles and alleviate pain.
Ergonomics
Modifying work habits and posture to reduce strain on muscles.
Stress Management
Techniques like deep breathing and meditation can help reduce stress-related muscle tension.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Personal Injury Rehabilitation
References
Jafri M. S. (2014). Mechanisms of Myofascial Pain. International scholarly research notices, 2014, 523924. https://doi.org/10.1155/2014/523924
Kojidi, M. M., Okhovatian, F., Rahimi, A., Baghban, A. A., & Azimi, H. (2016). Comparison Between the Effects of Passive and Active Soft Tissue Therapies on Latent Trigger Points of Upper Trapezius Muscle in Women: Single-Blind, Randomized Clinical Trial. Journal of Chiropractic Medicine, 15(4), 235–242. https://doi.org/10.1016/j.jcm.2016.08.010
Nicol A, C. M., Hsu E, Ferrante M. (2018). Myofascial Pain Syndrome. Science Direct, 207-212. https://doi.org/https://doi.org/10.1016/B978-0-323-40196-8.00025-5
THORNE. (2021). Understanding Muscle Pain, Fascia, and Myofascial Release. https://www.thorne.com/take-5-daily/article/understand-muscle-pain-fascia-and-myofascial-release?srsltid=AfmBOop3Pp0wWEeiQEqpfPgAaTOpLvU7lOAGUv5VRYQdoH8OBcW4D_wk
Shah, J. P., Thaker, N., Heimur, J., Aredo, J. V., Sikdar, S., & Gerber, L. (2015). Myofascial Trigger Points Then and Now: A Historical and Scientific Perspective. PM & R: the journal of injury, function, and rehabilitation, 7(7), 746–761. https://doi.org/10.1016/j.pmrj.2015.01.024
Yoo W. G. (2015). Comparison of activation and change in the upper trapezius muscle during painful and non-painful computer work. Journal of Physical Therapy Science, 27(10), 3283–3284. https://doi.org/10.1589/jpts.27.3283
Bron, C., & Dommerholt, J. D. (2012). Etiology of myofascial trigger points. Current pain and headache reports, 16(5), 439–444. https://doi.org/10.1007/s11916-012-0289-4
Can individuals dealing with sciatica incorporate nonsurgical treatments to reduce thigh pain and restore mobility in the legs and hips?
Contents
The Tensor Fascia Latae
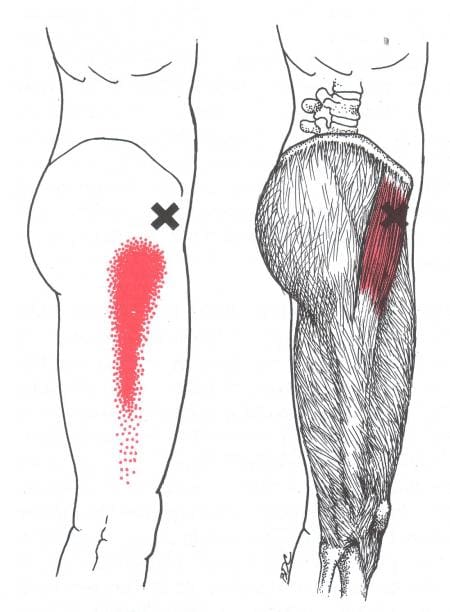
Do you feel stiffness or tightness in your legs, feet, and hips? Have you experienced walking crookedly when running errands? Or have you experienced radiating pain from your gluteal region down to your feet? The hips, thighs, and legs have numerous muscles, tissues, and ligaments surrounding the skeletal bone in the body’s lower extremities. These components allow the lower half of the body to stabilize the upper body’s weight and enable the individual to be mobile throughout the day. One muscle that works together is the tensor fasciae latae (TFL) muscle. The TFL muscle is part of the proximal anterolateral thigh between the deep fibers of the iliotibial (IT) band. It works with the gluteal muscles in various hip movements and assists with the knees. (Trammell et al., 2025) This muscle is poorly misunderstood as it helps with the hips and knee joint and pelvic stability. (Iyengar et al., 2022) At the same time, it has a casual relationship with the IT band.
The Iliotibial Band (ITB)
The iliotibial (IT) band is part of the lower extremities as it is a tough, fibrous fascial tissue that works together with the TFL muscle and has various functional roles that are dependent on posture and allows the individual to be mobile via walking, sprinting, and running. (Hutchinson et al., 2022) However, this muscle’s main function is knee flexion. When environmental factors affect the body, it can cause irritation and inflammation to the IT band, causing knee pain. (Martinez-Velez et al., 2020) When dealing with issues within their lower extremities, they affect the IT band, TFL muscle, and the thighs. Environmental factors can also affect the lower extremities as the surrounding muscles can aggravate the nerve roots, thus leading to sciatica pain. We associate with certified medical providers who inform our patients of how sciatica can negatively impact the lower extremities, especially the thighs. While asking important questions to our associated medical providers, we advise patients to integrate various non-invasive treatments to reduce sciatica and help regain mobility back to the lower body. Dr. Alex Jimenez, D.C., envisions this information as an academic service. Disclaimer.
Reclaim Your Mobility: Chiropractic Care For Sciatica Recovery-Video
Sciatica & Thigh Pain
When the general population hears about sciatica, it is a frequent diagnosis associated with low back pain, which causes discomfort within the lower extremities, especially in the thighs. Sciatica is a debilitating condition where the sciatic nerve is often compressed and irritated, causing pain. (Davis et al., 2025) Many influences cause sciatica to develop, and it can cause the individual to deal with a spinal imbalance, which correlates with walking incorrectly, causing the accessory muscles to work overtime and compressing the sciatic nerve, causing thigh pain. (Wang et al., 2022) With thigh pain correlating with sciatica, many symptoms can range from muscle weakness, absence of tendon reflexes to the knees, and sensory deficit. (Fairag et al., 2022) Luckily, treatments are available to reduce thigh pain associated with sciatica and regain mobility back to the lower extremities.
Treatments For Sciatica-Thigh Pain
When treating the lower extremities, especially when experiencing sciatica-thigh pain, many individuals with thigh pain associated with sciatica can incorporate non-invasive treatments to reduce the pain. Many athletic and non-athletic individuals can utilize PRICE (protection, rest, ice, compression, and elevation) to the affected muscles that can minimize the injuries causing pain. (Lempainen et al., 2022) This can help reduce the inflammatory effects causing issues to the thighs and lower extremities. Many non-surgical treatments like physio-exercise therapy, massages, stretching, and spinal stabilization therapies can improve core strength and posture and help with range of motion to relieve sciatica pain affecting the lower extremities. (Aguilar-Shea et al., 2022) Other non-surgical treatments like yoga, physical therapy, and chiropractic care can help improve joint and lower extremity motions, stretch and strengthen weak muscles surrounding the thighs, and relieve sciatic nerve pain. (Kim & Yim, 2020) When people start thinking about their bodies and how pain is affecting their quality of life, many can incorporate non-surgical treatments to reduce the pain associated with sciatica. Many people can make small positive changes in their routine by becoming more physically active, stretching more, eating healthier, and being more mindful of what they are doing, which can reduce the chances of sciatica returning and affecting the lower extremities. This can help them achieve a healthier, better life.
References
Aguilar-Shea, A. L., Gallardo-Mayo, C., Sanz-Gonzalez, R., & Paredes, I. (2022). Sciatica. Management for family physicians. J Family Med Prim Care, 11(8), 4174-4179. https://doi.org/10.4103/jfmpc.jfmpc_1061_21
Fairag, M., Kurdi, R., Alkathiry, A., Alghamdi, N., Alshehri, R., Alturkistany, F. O., Almutairi, A., Mansory, M., Alhamed, M., Alzahrani, A., & Alhazmi, A. (2022). Risk Factors, Prevention, and Primary and Secondary Management of Sciatica: An Updated Overview. Cureus, 14(11), e31405. https://doi.org/10.7759/cureus.31405
Hutchinson, L. A., Lichtwark, G. A., Willy, R. W., & Kelly, L. A. (2022). The Iliotibial Band: A Complex Structure with Versatile Functions. Sports Med, 52(5), 995-1008. https://doi.org/10.1007/s40279-021-01634-3
Iyengar, K. P., Azzopardi, C., Kiernan, G., & Botchu, R. (2022). Isolated pathologies of Tensor Fasciae Latae: Retrospective cohort analysis from a tertiary referral centre. J Clin Orthop Trauma, 29, 101870. https://doi.org/10.1016/j.jcot.2022.101870
Kim, B., & Yim, J. (2020). Core Stability and Hip Exercises Improve Physical Function and Activity in Patients with Non-Specific Low Back Pain: A Randomized Controlled Trial. Tohoku J Exp Med, 251(3), 193-206. https://doi.org/10.1620/tjem.251.193
Lempainen, L., Mecho, S., Valle, X., Mazzoni, S., Villalon, J., Freschi, M., Stefanini, L., Garcia-Romero-Perez, A., Burova, M., Pleshkov, P., Pruna, R., Pasta, G., & Kosola, J. (2022). Management of anterior thigh injuries in soccer players: practical guide. BMC Sports Sci Med Rehabil, 14(1), 41. https://doi.org/10.1186/s13102-022-00428-y
Can mustard be a low-calorie alternative to higher-fat condiments for individuals trying to reduce calorie intake?
Contents
Mustard
Prepared mustard is a common condiment used around the country. It is a low-calorie, highly flavored condiment that can replace more calorie-dense options. The familiar condiment combines mustard seeds with vinegar, salt, lemon, and other ingredients. There are also different varieties made from brown or black mustard seeds.
Health Benefits
Mustard is considered healthy because it contains antioxidants that provide various health benefits, including anti-cancer, antibacterial, antiviral, antifungal, anti-inflammatory, and wound-healing properties. (Mazumder A., Dwivedi A., & du Plessis J. 2016) Although not associated with significant health benefits, mustard is a low-calorie alternative to many higher-fat condiments, like mayonnaise. Different types of mustard seeds are used for health purposes. For example, some herbalists use white mustard seeds to clear the throat when mixed with honey (Ewing, Sarah, 1999). Antioxidants include isothiocyanates and sinigrin.
Isothiocyanates, the oil that gives mustard its pungent taste, have anti-cancer properties for breast, lung, GI tract, and prostate cancers.
However, the mechanism remains unclear, and more research is needed to determine the efficacy of mustard’s health benefits for cancer.
Isothiocyanates may also help manage diabetes and reduce unhealthy cholesterol, providing cardiovascular protection and neurological benefits that may help autistic individuals. More research is needed. (Palliyaguru D. et al., 2018)
Sinigrin is another antioxidant. Research shows this antioxidant has anti-cancer, antibacterial, antiviral, antifungal, anti-inflammatory, and wound-healing properties. (Mazumder A., Dwivedi A., & du Plessis J. 2016)
Nutrition
A single serving is usually about a teaspoon. A serving of prepared yellow and spicy mustard provides only about three calories. (U.S. Department of Agriculture, 2019) Its nutritional profile includes a rich supply of essential minerals, including calcium, iron, manganese, phosphorus, and zinc. It is also a good source of omega-3 fatty acids, tryptophan, phosphorus, iron, and protein. The seeds are also a very good source of selenium. Most calories come from carbohydrates, but because the calorie count is so low, these carbohydrates are not likely to significantly affect daily intake. Dijon mustard may provide more calories. A single serving of Dijon may contain up to 10 calories.
Preparation and Storage
Yellow mustard and Dijon are easy to find. Try course mustard varieties with distinct textures and seeds. Buy in small quantities, as mustard can lose flavor with time. Once opened, store in the refrigerator for up to one year. Mustard imparts a strong, spicy taste that pairs well with meat and seafood and can also be used to make salad dressings.
Side Effects
The U.S. Food and Drug Administration recognizes mustard as safe (GRAS). Eating too much can cause abdominal pain, diarrhea, and gut inflammation. However, mustard and mustard seed allergies are not uncommon. Symptoms may be mild or severe and generally appear shortly after consuming the product. Individuals may experience a rash or a tingly, itchy feeling in the mouth. Difficulty breathing is also possible. Other foods derived from the mustard plant, including leaves, seeds, flowers, sprouted seeds, oil, and foods that contain these, are likely to cause reactions in those with mustard allergies.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic focuses on and treats injuries and chronic pain syndromes through personalized care plans that improve ability through flexibility, mobility, and agility programs to relieve pain. Our providers use an integrated approach to create customized care plans for each patient and restore health and function to the body through nutrition and wellness, functional medicine, acupuncture, Electroacupuncture, and sports medicine protocols. If the individual needs other treatment, they will be referred to a clinic or physician best suited for them. Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, nutritionists, and health coaches to provide the most effective clinical treatments.
Enhancing Health Together
References
Mazumder, A., Dwivedi, A., & du Plessis, J. (2016). Sinigrin and Its Therapeutic Benefits. Molecules (Basel, Switzerland), 21(4), 416. https://doi.org/10.3390/molecules21040416
Ewing, Sarah. (1999). Black Mustard (Brassica nigra). https://opensiuc.lib.siu.edu/cgi/viewcontent.cgi?article=1421&context=ebl
Palliyaguru, D. L., Yuan, J. M., Kensler, T. W., & Fahey, J. W. (2018). Isothiocyanates: Translating the Power of Plants to People. Molecular nutrition & food research, 62(18), e1700965. https://doi.org/10.1002/mnfr.201700965
U.S. Department of Agriculture. (2019). Mustard, prepared, yellow. Retrieved from https://fdc.nal.usda.gov/food-details/326698/nutrients
Can individuals who sit for long hours daily prevent tight neck and shoulder muscles by improving their posture, regularly stretching, and massaging their trapezius muscles?
Contents
Trapezius Self Massage
The trapezius muscle is a triangle-shaped muscle in the upper back that starts at the base of the neck, spans the length of the upper shoulders, and extends into the middle back. This muscle’s main function is stabilizing and moving the scapula/shoulder blade. The trapezius also helps to move the head, neck, arms, shoulders, and torso, stabilizes the spine, and plays an important role in posture. Physical and mental stress can tighten the trapezius muscle, leading to neck and shoulder pain. Learning to perform a trapezius self-massage can ease tension and provide pain relief. (Domingo A. R. et al., 2017)
Anatomy
The trapezius consists of three parts in three different areas of the back. The bottom of the skull, across the shoulders, and down to the mid back. A trapezius self-massage focuses on the upper portion of the traps. This part is located at the top of the shoulders. To find the upper trapezius, cross one arm in front of your body so that you can place the palm on top of the other shoulder.
For a trapezius self-massage, you need to know that there are two areas where your upper traps start and where the muscle connects to a bone. The first point is on the bottom of the skull, close to the center of the back of the skull. Start there with your fingers and trace the muscle down the back of the neck to where the shoulders widen. If you get lost, You can walk your fingers up or down the muscle on either side to relocate its origin at the base of the skull, the vertebra at the base of your neck that sticks out. This is C-7, another of the upper trapezius’s origin sites. (University of Washington Department of Radiology, 2025)
Massage Technique
Massage oil is optional but can hydrate the skin during a massage. You can perform the trapezius self-massage using your hands.
Start at the Base of The Neck
Choose one shoulder to work at a time.
Raise the arm on the opposite side of your body.
Reach this arm across your body and fold it around your neck so that your fingers rest at the back base of your neck.
Apply a decent amount of pressure to the muscle while moving your fingers in a circular motion.
The action is similar to kneading dough.
Massage this area at the base of your neck for about 30 seconds to start.
If this part of your muscle is sore, you can massage it longer.
Slowly Work Out Towards The End of The Shoulder
Once you have spent about 30 seconds massaging the muscle at the base of the neck, work your way out toward the end of your shoulder.
In close increments, in your fingers across the trapezius muscle, spending at least 30 seconds at each point.
Follow the muscle until you reach the end of the shoulder.
Apply enough pressure, and use slow, rhythmic movements so that you feel relief.
If the pressure is not relieving or makes you wince, it’s too much.
Repeat as Needed
Repeat each side two to three times before switching to the other shoulder. After massaging, you may notice a certain trapezius area is particularly sore or tense. Zero in on those areas a little longer. Remember to relax throughout the trapezius self-massage. This is an opportunity to learn where tension is in your neck and shoulders and how to apply pressure to relieve it. This knowledge can also help you be mindful throughout your day, whether sitting, doing chores, or other physical activities. If you notice scrunching or slouching, massage the trapezius and remind yourself to keep your shoulders relaxed.
Benefits
Tension and tightness in the trapezius muscle are common, particularly among individuals who work in an office, do manual labor, or deal with a lot of stress. (Marker R. J. Campeau S., & Maluf K. S. 2017) Trapezius strains are a common overuse injury that is more likely to happen when the muscle is tight. (Salavati M. et al., 2017) The injury can cause unhealthy posture to avoid the pain. This poor posture will place more stress on the muscles, leading to a cycle of poor posture and chronic pain. A trapezius self-massage can benefit in many ways, including:
Improved blood circulation
Better quality of sleep
Improved posture
Improved range of motion
Decreased swelling
Faster recovery after workouts
Reduced risk of injury
Seeing a Healthcare Provider
Like any other muscle in the body, the trapezius can be injured and requires special treatment to recover. Sometimes, the neck or shoulder pain may not come from the trapezius muscle. Consider seeing a healthcare provider if you have pain in your neck or shoulder that doesn’t get better within a week or two, especially if it isn’t responding to at-home treatment. Regardless of how long you have been experiencing pain or stiffness, contact a healthcare provider if it prevents you from getting adequate sleep or interfering with daily activities. Reasons to see a healthcare provider immediately for neck or shoulder pain include: (Mount Sinai, 2025)
There is sudden pressure or pain in the left shoulder, which can sometimes signal a heart attack.
A fall or accident resulted in pain, swelling, or problems moving the neck or arm.
If there is shoulder pain, a fever, swelling, or redness.
The skin on the shoulder area appears discolored.
It’s important to take regular breaks to stretch and move your muscles. You can release tension in the trapezius by doing shoulder shrugs throughout the day and stretching regularly. When the trapezius feels tight or sore, give yourself a massage.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Whiplash Chiropractic Massage Therapy
References
Domingo, A. R., Diek, M., Goble, K. M., Maluf, K. S., Goble, D. J., & Baweja, H. S. (2017). Short-duration therapeutic massage reduces postural upper trapezius muscle activity. Neuroreport, 28(2), 108–110. https://doi.org/10.1097/WNR.0000000000000718
University of Washington Department of Radiology. (2025). Trapezius. https://rad.washington.edu/muscle-atlas/trapezius/
Marker, R. J., Campeau, S., & Maluf, K. S. (2017). Psychosocial stress alters the strength of reticulospinal input to the human upper trapezius. Journal of Neurophysiology, 117(1), 457–466. https://doi.org/10.1152/jn.00448.2016
Salavati, M., Akhbari, B., Ebrahimi Takamjani, I., Ezzati, K., & Haghighatkhah, H. (2017). Reliability of the Upper Trapezius Muscle and Fascia Thickness and Strain Ratio Measures by Ultrasonography and Sonoelastography in Participants With Myofascial Pain Syndrome. Journal of Chiropractic Medicine, 16(4), 316–323. https://doi.org/10.1016/j.jcm.2017.06.003
Mount Sinai. (2025). Shoulder pain. https://www.mountsinai.org/health-library/symptoms/shoulder-pain
Can individuals experiencing difficulty with functional mobility benefit from physical therapy to help them return to normal activities?
Contents
Outcome Measurement Tests
Outcome measurement tests assess the effects of a treatment plan on a patient. They can be used to determine a patient’s baseline function, monitor their progress, and evaluate the effectiveness of treatment. They also give the therapy team an effective way to measure mobility, flexibility, and range of motion.
The physical therapist may use other functional outcome measurements to help assess physical therapy progress.
They may measure your strength and range of motion.
Balance and posture may be evaluated.
Effective functional outcome measurement tests must meet certain criteria to be useful in a physical therapy clinic. First, they must be reliable, meaning the results must be consistent with each patient and within groups of patients. They must also be valid to measure exactly what they are intended to measure. An effective measurement test must also be easy to administer, so it must be practical and simple. Outcome measurement tests must also be purposeful. For example, a balance test must reflect a patient’s current function and be related to their balance ability.
Common Outcome Measurement Tests Used
Common functional outcome measurement tools that a physical therapist may use include:
The timed up-and-go or TUG test is a simple assessment used to evaluate a person’s mobility and balance by measuring how long it takes them to stand up from a chair, walk a short distance, turn around, walk back, and sit down again; it’s often used to identify potential fall risks in older adults, particularly those with mobility concerns, as a longer time to complete the task may indicate increased fall risk. (Centers for Disease Control and Prevention, 2017)
The Tinetti balance and gait evaluation, also known as the Performance-Oriented Mobility Assessment (POMA), is a clinical test used to assess balance and gait abilities, particularly in older adults. It evaluates stability during various standing and walking tests and provides a score that indicates a person’s fall risk potential.
The Berg Balance Scale (BBS) is a standardized test for adults that measures balance and the risk of falling. It’s widely used and can be performed in various settings.
The six-minute walk test (6MWT) is a medical assessment in which a person walks as far as they can in a designated area for exactly six minutes. This allows healthcare providers to evaluate their functional exercise capacity. It is particularly useful for assessing patients with lung or heart conditions where walking ability might be compromised. The distance covered during the six minutes is the key measurement used to interpret the test results. (Ferreira M. B. et al., 2022)
The functional reach test (FRT) is a clinical assessment that measures an individual’s dynamic balance by determining the maximum distance they can reach forward while standing in a fixed position. It assesses their risk of falling by evaluating how far they can extend their arm before losing stability. The FRT is often used to assess older adults or individuals with potential balance issues.
The Oswestry low back pain disability questionnaire is a self-administered questionnaire used to measure the level of disability a person experiences due to low back pain. It assesses how the pain impacts their daily activities in various aspects of life, such as personal care, work, and social life; a higher score indicates greater disability.
The functional independence measure (FIM) assesses a patient’s ability to perform daily activities independently. It also measures the patient’s disability level and how much assistance is needed.
Functional outcome measurement tests provide a starting point for developing physical therapy goals. For example, if the TUG test takes 19 seconds, individuals may aim for 10 seconds. A TUG score that falls at or over 10 seconds indicates reduced physical capacity (Kear B. M., Guck T. P., & McGaha A. L. 2017). This can be the motivation needed to reach physical therapy goals.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Understanding The Effects of Personal Injury
References
American Physical Therapy Association. (N.D.). Outcome Measures in Patient Care. https://www.apta.org/your-practice/outcomes-measurement
Centers for Disease Control and Prevention. (2017). Timed Up & Go Assessment. Retrieved from https://www.cdc.gov/steadi/media/pdfs/steadi-assessment-tug-508.pdf
Ferreira, M. B., Saraiva, F. A., Fonseca, T., Costa, R., Marinho, A., Oliveira, J. C., Carvalho, H. C., Rodrigues, P., & Ferreira, J. P. (2022). Clinical associations and prognostic implications of 6-minute walk test in rheumatoid arthritis. Scientific reports, 12(1), 18672. https://doi.org/10.1038/s41598-022-21547-z
Kear, B. M., Guck, T. P., & McGaha, A. L. (2017). Timed Up and Go (TUG) Test: Normative Reference Values for Ages 20 to 59 Years and Relationships With Physical and Mental Health Risk Factors. Journal of primary care & community health, 8(1), 9–13. https://doi.org/10.1177/2150131916659282
Can individuals managing facet arthropathy treat the condition with over-the-counter pain relievers, prescription muscle relaxers, exercise, and chiropractic spinal manipulation?
Contents
Facet Arthropathy
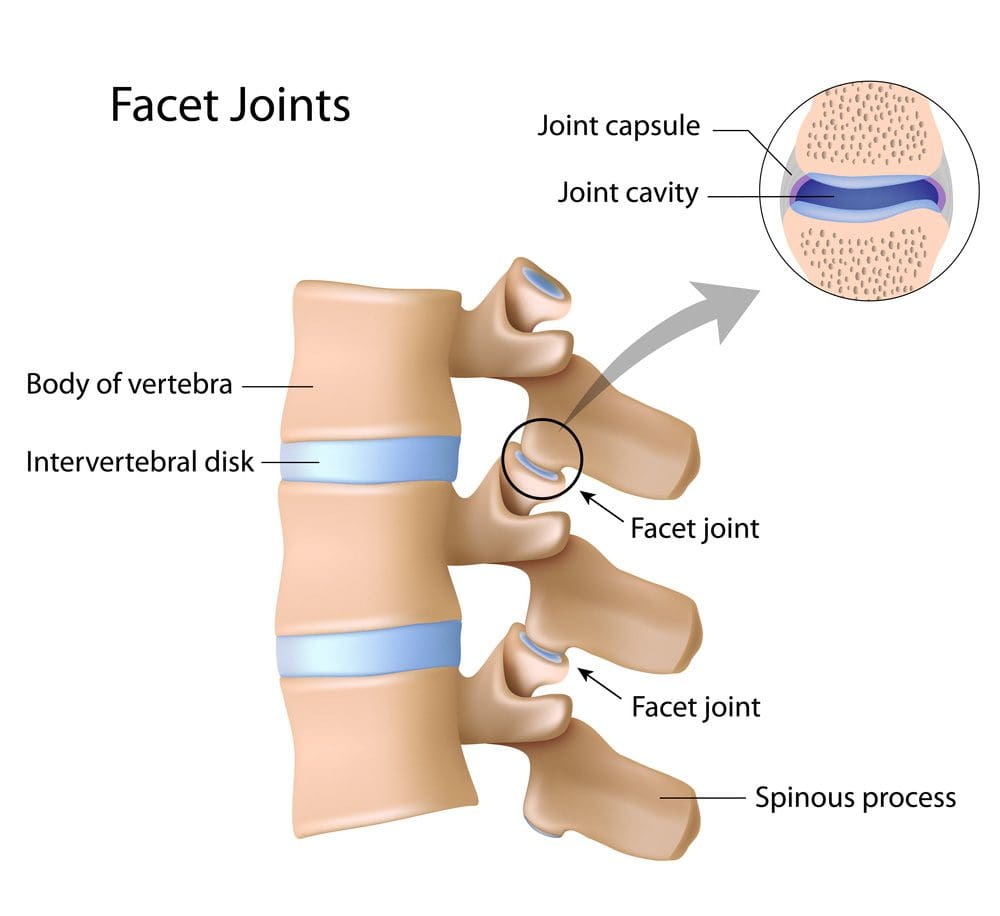
Facet arthropathy, or facet osteoarthritis, is arthritis that affects the facet joints in the spine. It causes pain and stiffness due to cartilage degeneration within these joints, often resulting from wear and tear associated with aging. Essentially, it occurs when the small joints in the back of the spine become arthritic and rub against each other painfully.
It affects the bony protrusions, called facet joints, that connect the spine’s bones.
Symptoms include neck and back pain that can worsen with standing, bending, or twisting.
Facet arthropathy is diagnosed using X-rays and other imaging studies.
Severe cases may require surgery.
Facet Joints
Twenty-four vertebrae form the spine, with two facet joints between each. Facet joints are small joints located at the back of each vertebra in the spine. They allow movement and stability, help maintain the alignment of the spinal bones/vertebrae, and limit excessive motion. The joints and the cushioning intervertebral disc form a three-joint complex between each vertebra.
The three-joint complex allows the spine to move, including bending, rotating, and extending.
Synovial fluid lubricates the joints so they can move.
The intervertebral disc provides flexibility and dissipates compressive loads.
The facet joints stabilize the spine by constraining rotation and bending.
Symptoms
Arthropathy refers to any disease affecting a joint, including arthritis. Osteoarthritis, also known as arthrosis, is a specific type of arthropathy. It is a non-inflammatory, degenerative arthritis. Pain is the main symptom that is typically worse in the morning when awakening, and in the evening, the pain can also get worse when twisting or bending backward. The symptoms can vary based on the part of the affected spine. Low back pain is the most common, a condition referred to as lumbar facet arthropathy because it affects the lumbar spine of the lower back. (Perolat R. et al., 2018) Common Symptoms include:
Muscle spasms or cramps.
Pain that may come in periodic flare-ups
Pain that worsens with standing or inactivity.
Dull pain on both sides of the spine.
Aching pain on both sides of the spine.
Pain in the lower back, buttocks, shoulders, or back of the skull
Radiating pain to the buttocks and legs.
Pain that improves with sitting, leaning forward, or changing positions.
Pins-and-needles sensations in the hands or feet.
Clicking sounds when moving the spine.
Catching sensations when moving the spine.
Muscle weakness.
Causes
Facet arthropathy causes progressive damage to the spine. Spinal osteoarthritis, aka spondylosis, is the most common cause, but it can also occur with a severe form of spinal arthritis known as ankylosing spondylitis. It is primarily due to age-related wear and tear, but injuries or repetitive stress on the spine can also cause it. Arthritis in the facet joints can develop due to:
Aging-related wear and tear
Disc problems
A previous back injury
Torn ligaments
Spinal fractures
Deterioration of facet joints can also cause bony overgrowths called osteophytes or bone spurs, which can cause radiating pain and restrict the spine’s range of motion.
Degeneration
The facet joints and intervertebral discs degenerate due to age-related wear and tear.
The cartilage in the facet joints can dry out, crack, and wear down.
The joint capsule and synovial membrane can inflame or tear, affecting synovial fluid production.
The loss of cartilage can lead to hypermobility, and the joint can stiffen over time.
Diagnosis
Imaging studies are important to the diagnosis. Several types confirm the diagnosis and also characterize the nature and severity of the condition:
X-rays provide a plain, black-and-white image of the spinal column.
CT scan composites multiple X-rays to create a three-dimensional image of the spinal column.
MRI uses magnetic and radio waves to generate images of soft tissues like ligaments and cartilage.
To confirm the diagnosis, a diagnostic block, which is a small amount of local anesthetic, is injected into a facet joint. The needle placement is directed either with an ultrasound or a CT scan. Facet arthroplasty is confirmed if the injection provides immediate relief (American Academy of Orthopaedic Surgeons, 2022). The healthcare provider will want to exclude other possible causes as part of the differential diagnosis. Conditions that mimic facet arthropathy include:
Herniated disc
Psoriatic arthritis
Reactive arthritis
Spinal gout
Spinal compression fracture
Treatment
The treatment varies depending on the location and severity of the condition. Generally, conservative treatments are used before more invasive procedures are considered.
Lifestyle Changes
Initially, a healthcare provider may recommend rest and avoiding aggravating movements, including any activity that involves bending or twisting.
Activities that take the weight off the facet joint, such as sitting, leaning forward, or changing positions, may help ease the pain.
Patients may also be advised to adjust their sleep positions to take the pressure off facet joints.
Options included curling up on your side or lying on your back with the knees supported with pillows.
Medications
If a diagnostic block is used, a patient may not need medications immediately. However, as the anesthetic starts to wear off, the patient may be prescribed over-the-counter or prescription pain relievers based on the severity of the pain. These can include:
Analgesics like Tylenol
Nonsteroidal anti-inflammatory drugs like Advil or Aleve
Muscle relaxants like Lloresal for acute back pain
Antidepressants like Cymbalta for chronic back pain
Physical Therapy
Physical therapy is a major part of the treatment of lower back pain. The treatment plan will include personalized exercises to strengthen the core muscles and avoid stress on the spine. Examples include:
Knee-to-chest stretches, hugging your knees for 30 to 60 seconds.
Walking 10 to 20 minutes per day.
Aquatic therapy to alleviate pressure on the spine.
Surgery
If conservative measures don’t work or provide sufficient relief, a healthcare provider may recommend specialist procedures or surgeries that include:
Lumbar intra-articular injections deliver an anesthetic or corticosteroid into the spine for longer-lasting pain relief.
Sinuvertebral nerve ablation destroys spinal nerves with a strong electrical current.
Extracorporeal shockwave therapy ESWT delivers low- or high-energy electrical pulses to help ease pain.
Spinal fusion surgery involves fusing two or more vertebrae to eliminate movement and pain in the facet joints.
Facet rhizotomy is a surgical procedure used to sever one of the nerves supplying the facet joint.
Stem cell regeneration is an experimental procedure in which stem cells are harvested and injected into damaged joints to restore function.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Facet Syndrome Pain Treatment
References
Perolat, R., Kastler, A., Nicot, B., Pellat, J. M., Tahon, F., Attye, A., Heck, O., Boubagra, K., Grand, S., & Krainik, A. (2018). Facet joint syndrome: from diagnosis to interventional management. Insights into imaging, 9(5), 773–789. https://doi.org/10.1007/s13244-018-0638-x
American Academy of Orthopaedic Surgeons. (2022). Spinal injections. https://orthoinfo.aaos.org/en/treatment/spinal-injections/
Should individuals wanting to engage in the exercise start with a warm-up and end with a cooldown to prepare the muscles for optimal performance and post-workout recovery?
Contents
Warming Up, Cooling Down
Warming up 5 to 10 minutes before exercise is beneficial for pumping blood to the muscles and preparing them for a run. Dynamic or active stretching and light aerobic activity are a few ways to warm up. This could be active stretching, such as walking lunges, brisk walking, or riding a stationary bike for a few minutes before running. However, individuals should avoid static stretches before running, as they can increase the risk of injury. The minimum length of time for an effective cooldown session is five minutes. Depending on the intensity of the workout, individuals may choose to extend that to 10 minutes.
Steps for a Running Warmup
Do five to 10 minutes of light aerobic exercise to loosen up muscles.
Walk briskly, march, jog slowly, or cycle on a stationary bike.
Don’t rush.
Perform dynamic stretches and movements during the warmup, including walking lunges, jumping jacks, or toe touches.
Begin the run with a slow jog and gradually increase speed.
Slow down if you run out of breath.
This is part of knowing how fast you should run; starting too fast is a common mistake.
Pay attention to posture and form.
Ensure you are using the best technique before speeding up.
Warm Up Benefits
When warming up, the blood vessels dilate. The increased blood flow primes the muscles with oxygen and prepares them to perform at their best. Blood flow also increases the temperature in the muscles for enhanced flexibility. Allowing the heart rate to increase gradually is beneficial, instead of going full max heart output by jumping full speed into the running. (The American Heart Association, 2024)
Properly Cooling Down
At the end of the run:
Cool down by walking or slowly jogging for five to 10 minutes.
Breathing and heart rate should gradually return to normal.
Drink water or an electrolyte-infused drink to rehydrate the body.
Benefits of a Cooldown
The cool-down keeps blood flowing throughout the body at a consistent level. Stopping immediately can cause light-headedness because heart rate and blood pressure can drop rapidly. Winding down slowly allows heart rate and blood pressure to fall gradually. The cooldown is also a good mental transition from the intensity and accomplishing the workout.
Before or After Stretching
Stretching evidence shows it doesn’t have the benefits once thought. Static stretching before, during, or after exercise has not been shown to prevent injury or delayed onset muscle soreness. (Herbert R. D., de Noronha M., & Kamper S. J. 2011) Stretching cold muscles is not recommended. However, there is some evidence that dynamic or active stretching after a warmup can benefit performance. Active stretching is done with exercises that take the muscles through their full range of motion and mimic the actions that will be done during the workout. (Van Hooren B., & Peake J. M. 2018)
Stretching After Running
Standard stretching includes the hamstring stretch, quad stretch, calf stretch, low lunge stretch, IT band stretch, butterfly stretch, hip and backstretch, arms and abs stretch, and triceps stretch. Tips for proper stretching:
Don’t Bounce
Avoid bouncing, as this mimics pulling a rubber band back and forth. You want the muscle to stay stretched.
Hold the stretch for 15 to 30 seconds.
Don’t Stretch Through Pain
Don’t stretch beyond the point where tightness is felt in the muscle.
Do not push through muscle resistance.
Never stretch to the point of pain.
Stretch Whole Body
Don’t just stretch the areas with tightness and/or soreness.
Stretch the whole body equally to prevent injury.
Don’t Hold Your Breath
Take deep breaths during the stretch.
Stay relaxed and breathe in and out slowly.
If starting a new fitness routine, consult your healthcare provider to determine the optimal running warmups and stretching exercises.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
The Science of Motion
References
The American Heart Association. (2024). Warm up, cool down. https://www.heart.org/en/healthy-living/fitness/fitness-basics/warm-up-cool-down
Herbert, R. D., de Noronha, M., & Kamper, S. J. (2011). Stretching to prevent or reduce muscle soreness after exercise. The Cochrane database of systematic reviews, (7), CD004577. https://doi.org/10.1002/14651858.CD004577.pub3
Van Hooren, B., & Peake, J. M. (2018). Do We Need a Cool-Down After Exercise? A Narrative Review of the Psychophysiological Effects and the Effects on Performance, Injuries and the Long-Term Adaptive Response. Sports medicine (Auckland, N.Z.), 48(7), 1575–1595. https://doi.org/10.1007/s40279-018-0916-2
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine