El Paso, TX. Dr. Alex Jimenez answers the question what is epigenetics, dietetics? And simplifies the science behind this new method in health care.
Dietetics is a field of science that studies how food and nutrition affect human health. Dietetics strongly emphasizes public health and education for all about the importance of healthy dietary choices.
Dietitian nutritionists present nutrition combined with science to help individuals improve their health. Nutrition and dietetic technicians also work with dietitian nutritionists to provide general nutrition education. Both groups are nationally credentialed and are an essential part of health care and foodservice management.
Professional Dietitian Nutritionists tend to focus on specific populations, or movements, which include:
Design individual nutritional plans to address specific health issues:
Unhealthy weight
Diabetes
Hypertension
Develop facility-wide nutrition programs:
Health care
Educational
Correctional Institutions
Increase public awareness of proper nutritional habits
Improve the accuracy and comprehension of food labels
Ensure the safety of the food supply
Research changes in diet:
Example: Reduce salt intake affects health
Result: Reduces blood pressure
Work with food manufacturers to improve nutritional quality of prepared foods
Food Information Council (2005), more than two-thirds of Americans surveyed expressed a favorable opinion toward the idea of using genetic information to develop personalized nutrition recommendations.
International Food Information Council. 2005 Consumer Attitudes toward Functional Foods/Foods for Health Executive Summary. July 2006. http://www.ific.org/ research/upload/2005funcfoodsresearch.pdf. Accessed September 2, 2007
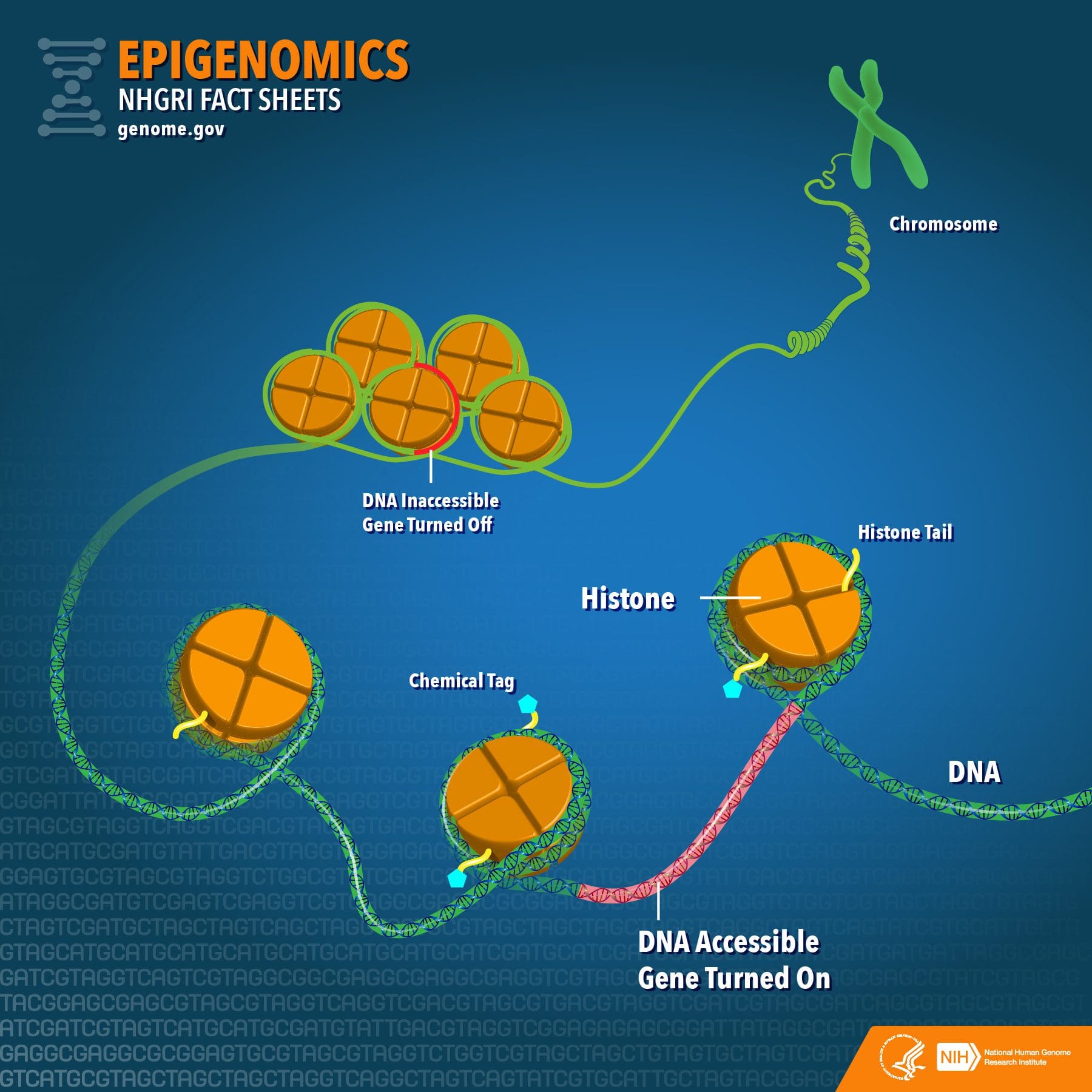
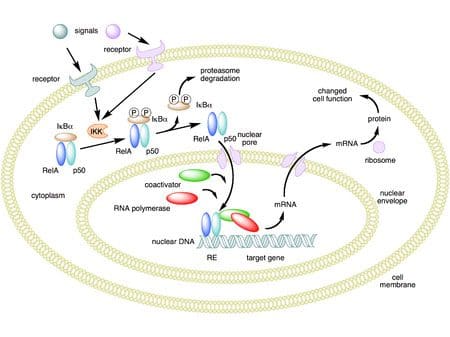
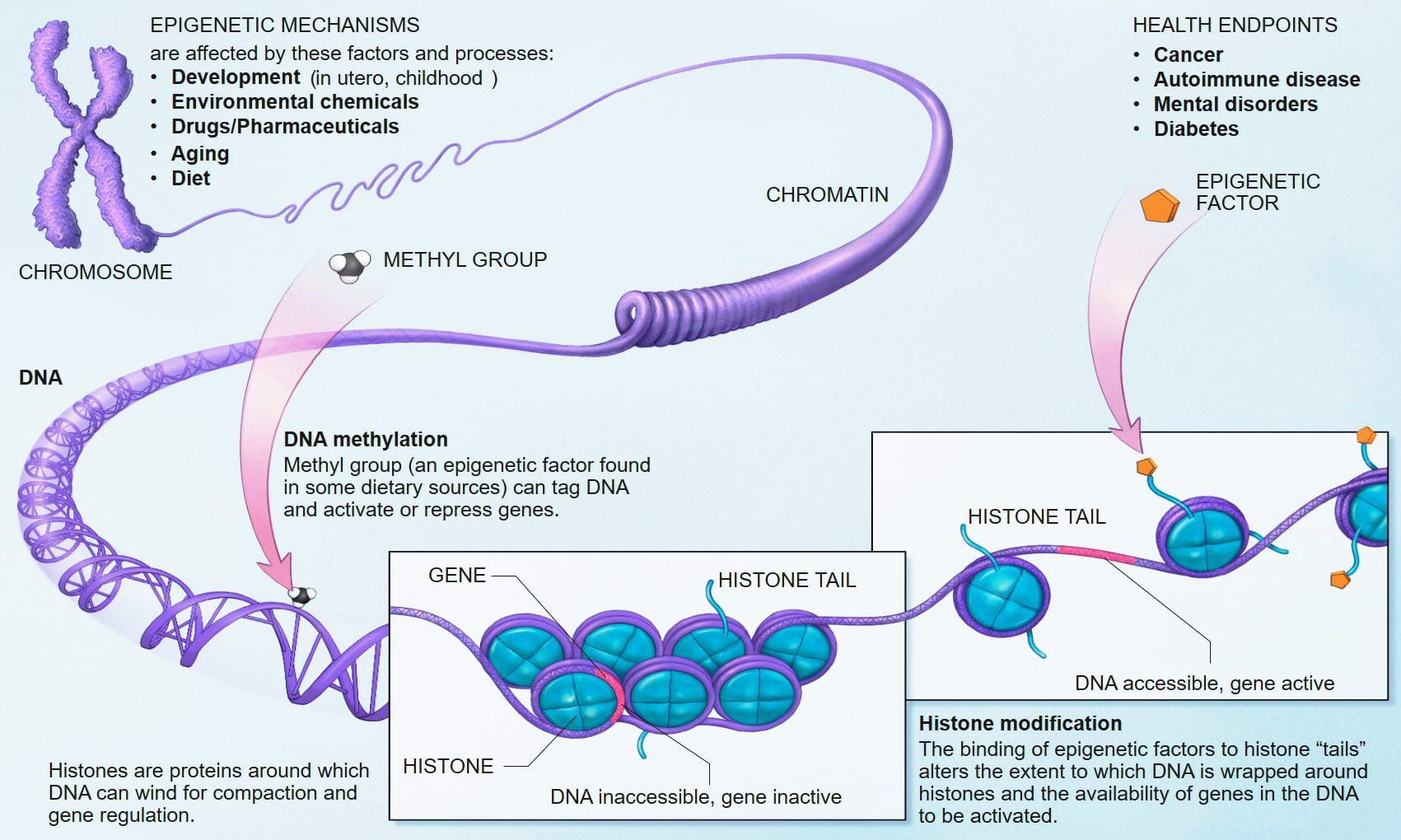
Our epigenome provides an extra layer of instructions that influence gene activity. This is an extra layer of instructions that affect whether or not various genes are turned on or off, and ultimately affect cellular function and metabolism.
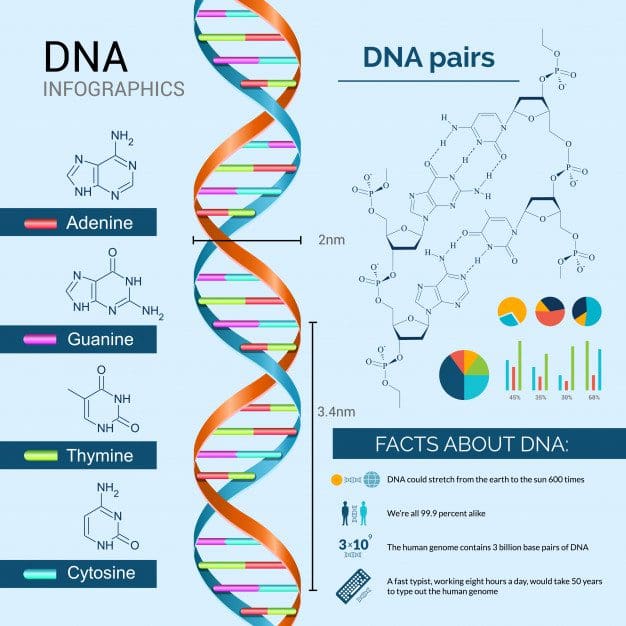
These are typically abbreviated as A, G, T, and C.
The Sequence or Order of These Bases Is What Drives Our Life Instructions
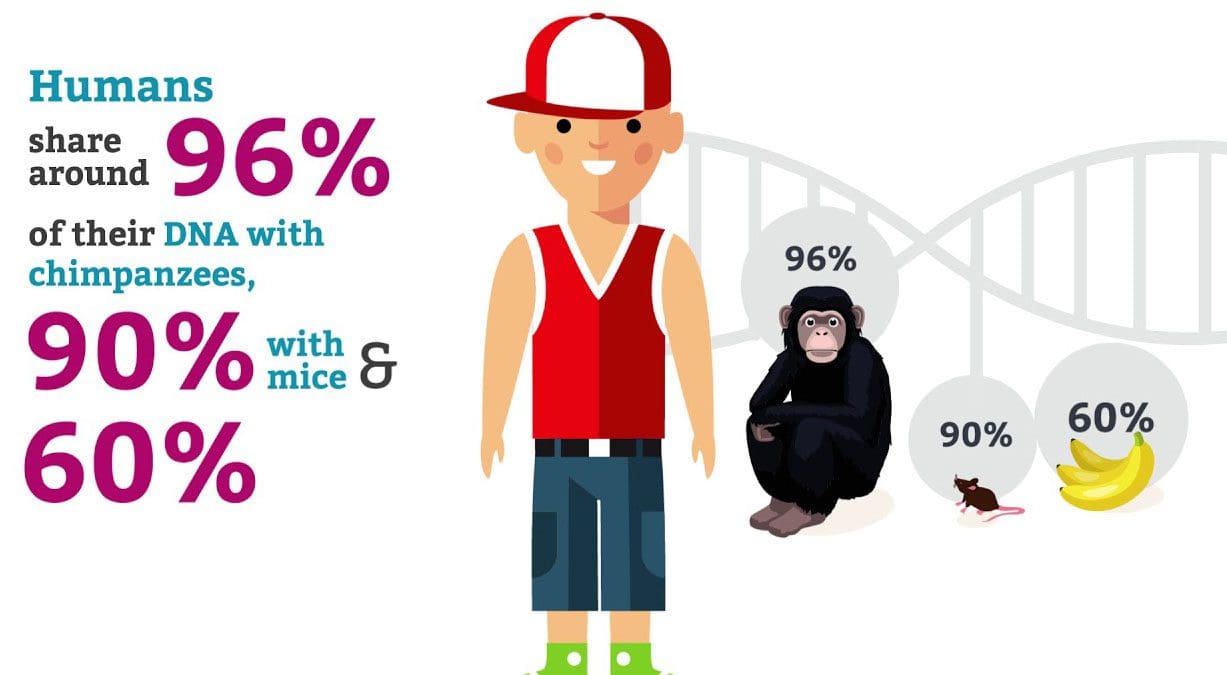
The human DNA sequence is somewhat similar to a chimpanzee. However, only a fraction of different sequences is what makes us human.
Inside The 3 Billion Bases are About 20,000 Genes
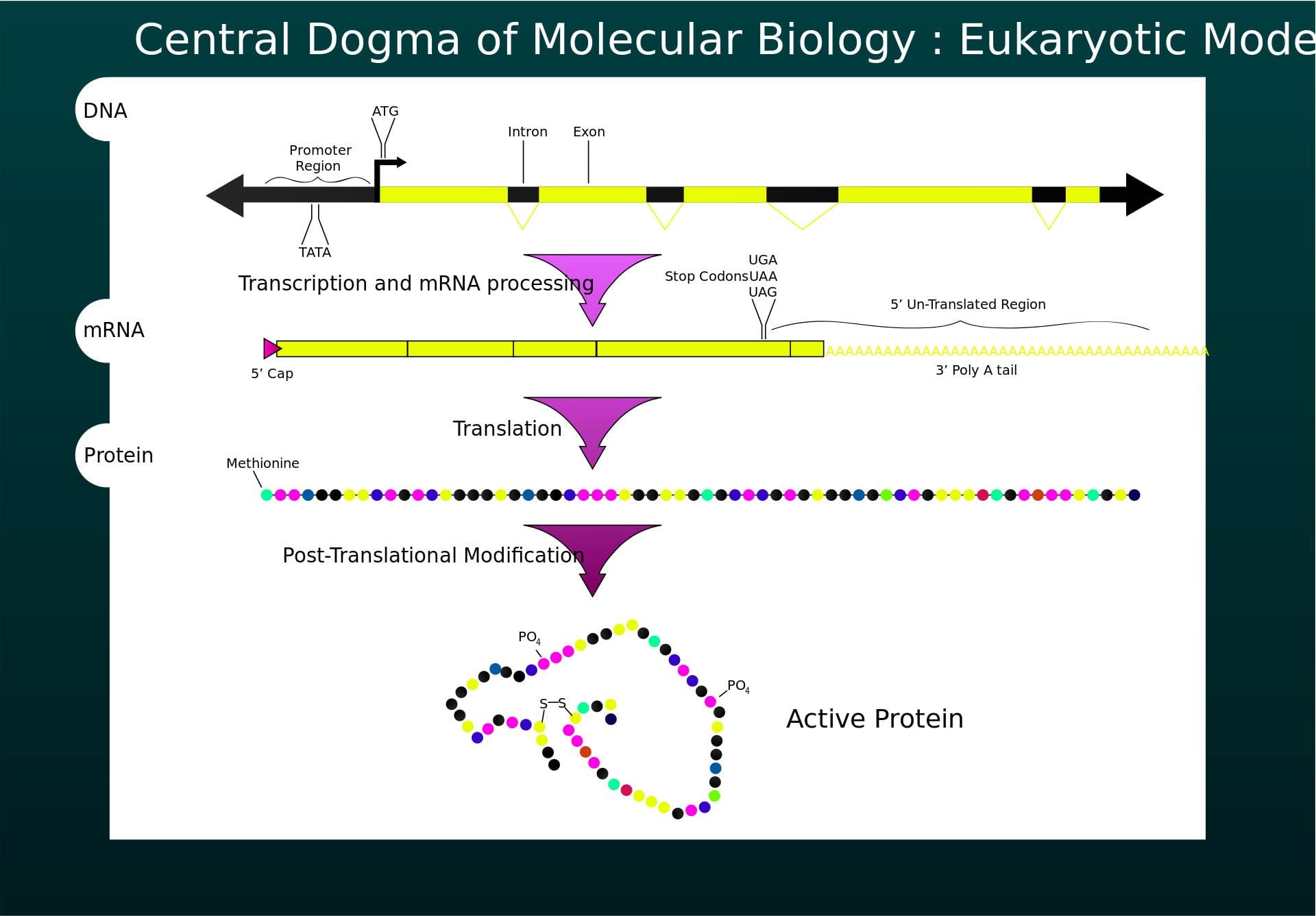
Genes are a specific set of sequences/instructions on how to make proteins, (complex molecules that trigger biological actions for carrying out life functions).
The DNA gives the instructions for various essential proteins to be produced inside the cell.
Epigenetics is what controls our genes: Epigenetics determine a cell�s specialization (e.g., skin cells, blood cells, hair cells, liver cells, etc.) as a fetus develops through gene expression (active) or silent (dormant).
Nurture: Environmental stimuli can cause genes to turn on or off.
They AreEverywhere
What We Eat
Where We Live
Who We Interact With
Sleep
Exercise
Age
All of these can cause chemical alterations around the genes that can turn them on or off over time.
In certain diseases, e.g., cancer or Alzheimer�s, certain genes will switch to the opposite state. This means they turn away from being in a normal/healthy state into an unhealthy state.
They Are What Makes Us Unique
Expedition 45/46 commander and retired astronaut Scott Kelly (right), along with his twin brother, retired astronaut Mark Kelly (left), speak to media.
This is why some of us have:
Blonde hair
Dark skin
Dislike certain foods
More social than others
The different combinations of genes that get turned on or off is what makes each one of us.
There are even indications that some epigenetic changes are inherited.
It Is Reversible
With 20,000 genes, the results of different combinations being turned on or off are enormous.
Imagine if we could map every single cause and effect of the different combinations
Reverse the gene�s state to keep healthy genes while eliminating unhealthy genes
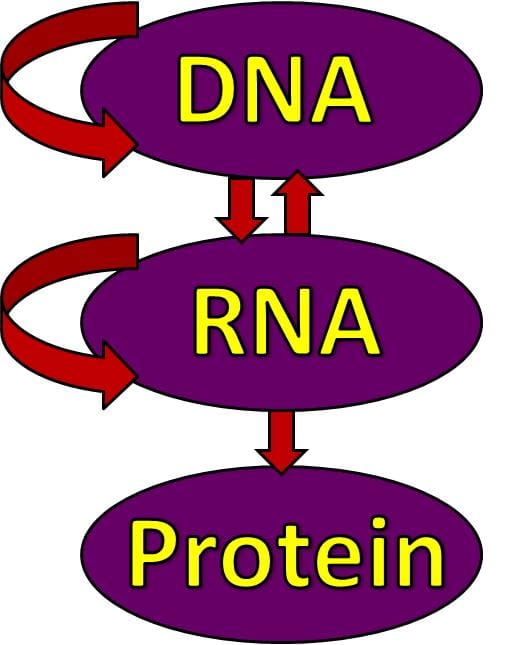
DNA is the script, the instructions for the actors
The cells are the actors
The literal DNA sequence are all the words
Certain blocks of words are key instructions for events to happen, these are the genes
The Epigenetic concept is like movie directing
Different directors can shoot the same script
However, each director makes choices in regard to:
Adjustments with actors/scenes/dialogue
What to keep/remove
These choices are going to alter the movie, hence alter the DNA
Therefore, one director’s movie will be different than another director’s even though they shot the same script.
In other words, the same exact DNA sequence for a particular gene may give rise to different outcomes, depending on its epigenotype and, unlike the genetic code, which Gosden and Feinberg liken to �indelible ink,� the epigenetic code can be altered �like a code written in pencil in the margins�
Gosden RG, Feinberg AP. Genetics and epigenetics�Nature�s pen-and-pencil set. N Engl J Med. 2007;356:731-733.
Can methylation donors help promote a balanced methylation support?
Many doctors and functional medicine practitioners generally recommend higher doses of methyl donors, such as 5-methyltetrahydrofolate, or 5-MTHF, and methylcobalamin, in several patients. By way of instance, people with genetic polymorphisms and people with out-of-range methylation-related biomarkers, such as in hyperhomocysteinemia, may often develop health issues which may affect the function of specific enzymes, such as methylenetetrahydrofolate reductase, or MTHFR, among others.
Nutrient deficiencies associated with methyl donors are a prevalent finding in laboratory evaluations, and depending on your population, these may be closely associated with vitamin B12 deficiency-related neuropathy, which is relatively common. Many doctors and functional medicine practitioners also understand the importance of methylation support to help improve hereditary or environmental epigenetic health issues. Improving methylation status and avoiding the pathways of disease and dysfunction associated with potential nutritional deficits in methylation activity is the goal of many healthcare professionals.
However, as with any other biochemical process, methylation activity occurs through the balance of homeodynamics, or the dynamic form of homeostasis. An imbalance in these biochemical processes can ultimately lead to dysfunction and disease. Therefore, although we can be confident that making sure we have enough methyl donors available for use in the human body is essential, we have to question whether �pushing� reaction rates utilizing supraphysiological doses are safe and effective. Instead of forcing reaction rates, perhaps the goal of healthcare professionals should ultimately be to allow the human body to function correctly.
Methylation Supplementation
Numerous health issues associated with long-term, high-dose supplementation for methylation donors include:
According to research studies, the effects of these genetic alterations remains unclear. In comparison to the altered function of MTHFR C677T and A1298C single nucleotide polymorphisms, or SNPs, which have been moderately evaluated, the diagnosis of other SNPs can demonstrate the overall function of these specific enzymes. The effect of these SNPs on methylation activity depends on enzymes working together in the circumstance of a person’s internal and external environment. These outcome measures have been demonstrated in a variety of genome research studies. As a result, researchers are unable to determine the effects which these alterations, including that of MTHFR C677T, can develop on a patient’s overall methylation status.
The correct supplementation dose for methylation donors remains mostly unknown, as it may vary tremendously between patients. No research studies have currently demonstrated what the correct dosage or duration of methyl-donor supplementation is required to balance biochemical and epigenetic methylation status. Various side effects of high-dose 5-methyltetrahydrofolate, or 5-MTHF, supplementation have been demonstrated in clinical practice, including anxiety and worsening of symptoms.
Hypermethylation may be detrimental to an individual’s overall health and wellness. The following series of articles contain many examples of region-specific DNA hypermethylation health issues, including immune dysfunction, Downs Syndrome, and cancer. Both DNA hyper- and hypomethylation can develop due to deficiencies in methylation donors. Folic acid has been associated with increased immune hypersensitivity and cancer. The bottom line is that we don�t understand what effect long-term, high-dose methylation donors and supplementation can have on DNA methylation support. Further research studies are still required to show this effect.
Methylation is a biochemical process which involves the conversion of methylation activity for the function of a variety of processes in the human body. Methylation imbalances, however, can cause a variety of health issues. Methylation donors are a form of supplementation for methylation support. But, research studies have demonstrated that supplementation for methylation support may not be right for everyone. The best way to improve methylation is through proper nutrition, physical activity, and exercise, among other dietary and lifestyle modifications. The nutritional guidelines below can help safely and effectively improve methylation support, promoting overall health and wellness.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Nutrition for Methylation Support
Methylation status can often depend on a patient’s dietary and lifestyle factors. Dietary and lifestyle factors, including physical activity and exercise, stress, sleep, medicines, and toxin exposure, plays a role in methylation. Single interventions with high-dose nutrient supplementation may lack long-term effectiveness or these may not achieve the desired methylation support.
Dietary and lifestyle modifications are safe and effective, alternative treatment options for most individuals with methylation imbalances. This may be fundamental for certain vulnerable individuals, such as patients with active cancers. Aging is also known to be associated with decreased methylation activity, therefore, the Methylation Diet and Lifestyle, or MDL, program can be utilized as an anti-aging tool. Methylation status diagnosis and treatment is essential during preconception, pregnancy and the postnatal period.
The MDL program and supplementation can help promote overall health and wellness. A dietary and lifestyle treatment approach can also be utilized as a follow-up plan for people who need high-dose nutraceutical support. A variety of foods can promote methylation support. Dietary and lifestyle modifications have also been demonstrated to considerably improve methylation activity.
In the following articles, we will discuss dietary and lifestyle factors which can help support methylation. We will also discuss the basic biochemistry of methylation, the roles of methylation in the human body, how to evaluate methylation status, and the risks and benefits of methyl donor supplementation as well as the health issues associated with too little or too much methylation activity.
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications, there are several alternative treatment options you can try for yourself at home. As described above, however, supplementation for methylation support should be correctly determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support in a single serving. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
alanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many doctors and functional medicine practitioners may recommend higher doses of methyl donors in several patients, however, further research studies are needed to determine the proper amount of methylation supplementation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Some people find it easier to engage in certain healthy activities during different times of the year. For instance, they may enjoy the fresh produce of summer or going for a run during the cooler days of fall. However, there are some things you can do to stay healthy regardless of the season. These are some good habits you can cultivate and develop for good health, rain or shine, cool weather or warm. By incorporating these four practices into your daily routine, you are very likely to see much less of your doctor and enjoy your life a whole lot more.
See a Chiropractor Regularly
Visiting a chiropractor regularly will keep your body balanced and your spine aligned. Chiropractic care has several significant benefits including decreased pain, faster healing from injuries, increased mobility, and better flexibility.
What makes it even more preferable is that chiropractic takes a whole-body approach to health issues. This means that when you have a problem such as pain or a medical condition, your chiropractor will work to get to the root of it and treat the condition where it starts while traditional medicine typically focuses on symptoms. Chiropractic care is non-invasive and drug-free, a truly natural approach to health care.
Maintain a Balanced Diet
A healthy diet is the cornerstone of good health. You should maintain a diet that includes lean meats, fresh fruits and vegetables, and whole grains. The key is choosing fresh, seasonal foods that are local to your area. Foods grown in their season have certain vitamins and minerals that the body needs for the time of year in which they are ripe and ready.
It is also worth noting that several small studies have found that animal protein can exacerbate pain, specifically osteoarthritis. It does not mean you should stop eating meat altogether because certain types of meat offer significant health benefits. Salmon is a good example. It is loaded with heart-healthy Omega 3 Fatty Acids � which, incidentally, also help to reduce inflammation in the body.
Find an Exercise Routing that Works
If you want to be able to move, then you have to start moving. Exercise is crucial for maintaining a healthy lifestyle. The problem is, many people believe that the only way they can exercise is by joining the gym or going for a run which has to be done in good weather. This isn�t so.
There are plenty of things you can do indoors, even in small spaces or while on vacation, to get some exercise. If you have problems with mobility, walking is an excellent option, but even gardening is great.
Also, women over 40 should do weight-bearing exercises several times a week to ward off osteoporosis. Furthermore, exercise is a great complement to chiropractic. It helps to keep your body flexible and increases your range of motion. Three to five times a week for 20 to 30 minutes is all you need.
Get Good Sleep
Good sleep is one of the most underrated keys to good health. When you sleep, it gives your brain and body an opportunity to refresh and heal. The discs in your spine are rehydrated, your body relaxes, and you less susceptible to stress when you are well rested.
On average, adults need anywhere from seven to nine hours of sleep a night in order to reap the full benefits. Take time to set up your bedroom for good rest: a comfortable mattress, a good pillow (they can wear out so change them regularly), a cool, dark, quiet room, and a relaxing environment that may include white noise or lavender scent. Make your bedroom as comfortable and sleep-inducing as possible.
Good health practices don�t have to be complicated or difficult. Start with small steps and let those behaviors become habits. Good health habits will help you have a long, full life.
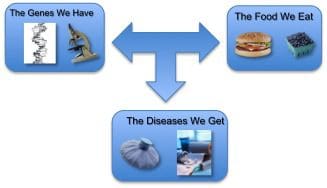
Nutrigenomics examines Relationships Between What We Eat
The risk/response to diseases
Genes and gene expression
Biomarkers
Uses A Variety of Tools In Identifying Disease Risk
Food diaries record nutrient input
Biomarkers: Example metabolite or hormone levels are examined to understand the body�s response
Genomic essays to identify relevant gene variations
Clinical data:
Age
Weight
Sex
BMI for monitoring the health impact of food
Applied to a Wide Range of Conditions
Risk of developing metabolic syndrome based on genetic variants and controlled by diet and lifestyle
Links between gut microbiota, obesity, and mental health
Correlation between specific nutrient intake and diseases
Example: Coffee and cardiac irregularities
Personalized Interventions
Identify, and provide supplements to a woman who metabolizes folate poorly in order to reduce neural tube defects in pregnancy.
Recommending a low fat diet versus low carbohydrate diet as the best way to lose excess weight.
As technology advances along with medical breakthroughs, there is not a day without there being a new cure or treatment to learn about. The trend is currently focused on the field of genetics and genomics, which consists of having personalized nutrition.
In the past recommending nutritional plans was population based. The only difference was between age, sex and pregnancy.
There is mounting evidence that nutrition throughout one’s life course modifies the epigenome.
There has been an increase in studies, which have reported associations between gene polymorphisms, nutrition, and disease risk.
Epigenetics
Epigenetic processes affect how the body uses nutrients.
The field of epigenetics explains unaccounted for variations in disease risk that is linked to the understanding of the interaction between nutrition and the genome.
A personalized nutrition dietary recommendation has the potential to decrease nutrition-related diseases.
There are still practical and economic challenges associated with this strategy.
Major epigenetic processes are DNA methylation, histone modification and noncoding RNAs.
This suggests the possibility that epigenotypes or (stable pattern of gene expression outside the actual base pair sequence of DNA) associated with disease risk can be changed.
Effects of Nutrients
The nature of an epigenetic change that is induced by specific nutrient/s intervention depends on the animal species, sex, genotype, and target gene, as well as, the timing of exposure and direction of the nutritional change.
There is also the possibility that epigenetic marks present at birth may act as predictors for future disease risk and pave the way to improve an individual’s health.
Terminology
Genes: Instructions written in our DNA sequence for making proteins that carry out all our biological functions.
Not all DNA is made up of genes; some are only used for spacing like the way the letters on a keyboard are arranged, so the buttons are easier to get to. Some are instructions for the instructions, like a content page that shows what to look for before beginning a chapter in a book.
Genetics: Study of gene inheritance how they vary from person to person and are passed on.
Genome: Is the collective term for all of our genes.
Genomics: A field of genetics that looks and analyzes the sequence of the genome.
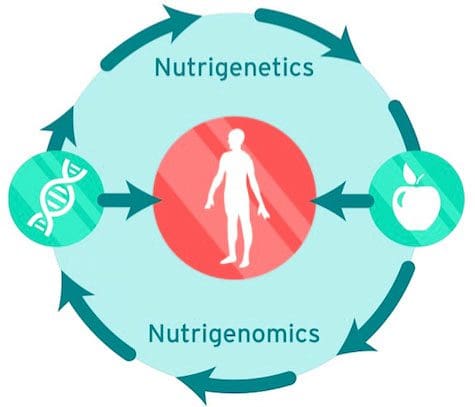
Nutrigenetics: Is concerned with how our genetic variations affect the way we respond to nutrients.
Epigenetics: The modification to the expression of genes, not involving changes in the genetic code itself (mainly via histones and methylation), that occurs in response to environmental factors. This results in genes being switched �on� or �off.�
Nutritional Genomics goal is to prevent the onset and development of chronic diseases. This is done by targeting dietary recommendations based on an individual�s genetic profile. Discoveries being made in the field, demonstrate that individuals are benefitting from adhering to different nutritional guidelines. However, this also depends on their genotype.
Knowing an individual’s genetic code helps better understand the intricacies and complexities of a case and aids in guiding recommendations in line with an individual’s genetic requirements.
However, even knowing someone�s SNP does not tell if a gene is on or off. This is where functional testing and case history come into play. Therefore, genomic testing is just a portion of the bigger picture.
Epigenetics is still a new science with the availability of new tools continually emerging. The field is rapidly progressing, and the findings reflect these advances in understanding and analyzing technologies.
And while trying to wrap your head around all of this can be daunting, don’t worry, it takes a few reps before it starts to make sense. And because of this, one of Dr. Jimenez’ goals is to simplify as much as possible. The program, terminology, and diet. And one way is going to be through SMOOTHIES! Putting it all into one easy drink will make it easier for everyone.
The American Heart Association and American Stroke Association advocate that many of the effects of diet on cardiovascular disease (CVD) risk and the outcomes are mediated by changes in gene expression. This means that the utilization of global transcriptional profiling is an important tool in nutrigenomics, and therefore cannot be denied that nutrigenomics is being taken seriously by those in the field of medical research.
What is systems medicine and how is it integrated into our overall health and wellness?
Systems medicine is an interdisciplinary field of study which evaluates the systems of the human body as part of a whole, including biochemical, physiological, and environmental interactions. And, with the outlining of the human genome back in 2001, Systems Medicine became widely recognized.
Humans are estimated to have between 20,000 and 25,000 genes although this number could drop further as genome sequence quality and gene finding methods improve over time. While the code for our lives seems smaller than what we expected, tremendous consideration is now being paid to the regulatory aspects of the genome and research studies on the heritable epigenome are gaining momentum. Methylation, a cornerstone epigenetic and metabolic process, now yields more than 85,000 hits on a PubMed search.
With the readily available access to genetic testing, many patients now have a greater understanding of their genes, most often concerning their single nucleotide polymorphisms, or SNPs, associated with methylation. It truly is a wildly exciting time to be practicing Functional Medicine, the clinical application of systems medicine. Several hypotheses have been developed on the phenotypic expression of single nucleotide variations. A heterozygous mutation in MTHFR A1298C SNP, by way of instance, can make it difficult for people to detoxify efficiently. Genetic testing and metabolic biomarkers can help demonstrate “lesions” in methylation.
What is Methylation Support?
Methylation is fundamental towards a variety of bodily functions, including detoxification, neurotransmitter production, and epigenetic regulation. Researchers have seen the impact that improving methylation can have on fortifying folic acid and reducing neural tube defects. The Methylation Diet and Lifestyle, or MDL, program was created with the purpose of embracing both the importance of healthy methylation balance as well as recognizing the limitations in our current understanding of methylation.
Methylation imbalances, such as hypermethylation and hypomethylation, in the gene promoter regions are associated with many health issues, from allergies and aging to neurodegenerative diseases and cancer. The regulation of the epigenome is a highly complex process. And, further research studies are still required to determine the effect of high-dose, long-term methylation interventions.
Furthermore, healthcare professionals need to consider whether high-dose, long-term methylation interventions are the right treatment approach for patients with these health issues. Numerous research studies have demonstrated reasonable concerns about supplementation. There are also patients who are unable to take methyl donor supplementation due to poor epinephrine clearance and other biogenic amines or detoxification activity. Understanding whether this treatment approach may be an appropriate methylation intervention, however, suggests that other, alternative treatment options may be required for overall health and wellness.
Food-based folates, by way of instance, have only been demonstrated to have protective effects on methylation. A variety of phytochemicals, not closely associated with methylation, seem to effectively modulate global epigenetic and biochemical methylation activity. And, decreasing methyl donor depletion by reducing toxic exposures, nourishing the microbiome, and increasing the stress response is safe and efficient. Nutrition can ultimately help eliminate the “lesions” in methylation for balanced bodily functions.
Methylation is a simple biochemical process which affects a variety of bodily functions, including DNA production, detoxification, and cellular energy, among many other fundamental processes. However, approximately 60 percent of people in the United States have a genetic mutation which tremendously affects methylation. When methylation isn’t working efficiently, it can affect the production of a variety of important molecules, including glutathione, coenzyme Q10, and melatonin, among many other fundamental substances. Understanding the importance of methylation support is important towards our overall health and wellness, and there are several ways you and your doctor can promote better methylation support.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
The Methylation Diet and Lifestyle Program
The Methylation Diet and Lifestyle program wouldn’t have been created if it wasn’t for the years of discussions on current research studies and patient treatment approaches. The following article serves as a guide to help people how to evaluate their methylation status and understand the current methylation health issues, and how to incorporate an MDL program into your protocols as well as the potential concerns from supplementation. Nutritional guidelines and lifestyle modifications can help improve methylation.
However, how can we determine when we should utilize the MDL? This treatment approach ultimately offers the methylation support patients might need, especially for those who cannot tolerate supplementation. It is also a safe and effective long-term strategy for a majority of patients who have utilized a short-term course of higher-dose methyl donors. The full MDL program also supports detoxification, microbiome and hormone balance, stress reduction, and it can be modified to incorporate other programs which are also generally recommended, such as elimination diets, grain and lectin-free plans, low FODMAP diets and traditional gut restoration programs. Highly restricted plans, such as the ketogenic diet used for epilepsy, can incorporate aspects of the MDL with additional nutraceutical support. Any dietary program can work with the Methylation Diet and lifestyle program for overall health and wellness.
Smoothies and Juices for Life
While many healthcare professionals can recommend the nutritional guidelines and lifestyle modifications described above, there are several remedies you can try for yourself at home. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support in a single serving. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
The scope of our information is limited to chiropractic, spinal health issues, and functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Louie Martinez depends on his wellness to be able to perform daily physical activities. And thanks to Dr. Jimenez, a chiropractor. Louie Martinez has found pain relief for a variety of health issues. Chiropractic care is a safe and alternative treatment option that focuses on the diagnosis, treatment, and prevention of a variety of injuries and/or conditions associated with the musculoskeletal and nervous systems. Louie Martinez describes how Dr. Alex Jimenez has restored his quality of life. Louie Martinez is grateful for the chiropractic care Dr. Alex Jimenez has provided for him, and he highly recommends him as the non-surgical choice for a variety of health issues, including back pain and sports injuries.
Best Chiropractic
We are blessed to present to you El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend us.
Individuals with diabetes have a 35 percent risk of developing neck pain and back pain, according to a recent research study. The researchers conducted eight research studies on separate occasions which revealed that individuals with diabetes have a higher chance of developing neck pain and back pain. According to the researchers, chronic pain is common in people with diabetes.
Approximately 80 percent of the population will experience some type of back pain throughout their lifetime and nearly half of that number will also suffer from neck pain, according to researchers. Meanwhile, diabetes has become an increasingly common health issue. About 382 million individuals have been diagnosed with type 2 diabetes, according to the World Health Organization.
Despite the outcome measures, it seems there’s still inadequate evidence in the research study to establish a causal connection between diabetes and chronic pain,” stated Manuela Ferreira, Ph.D., the research study’s senior author and associate professor in the university’s Institute of Bone and Joint Research. “The evidence requires further evaluation of this institution,” he explained.
“Type 2 diabetes and chronic back pain both have a strong connection with lack of physical activity or exercise and obesity. Thus, a logical development of the research study may be required to evaluate these outcome measures in further detail,” he explained. “Our evaluation adds to the proof that weight management and physical activity or exercise play essential roles in health and wellness.”
The research study also demonstrated that diabetes drugs and/or medications might also influence chronic pain, possibly via its effect on blood sugar levels. However, this connection also requires further research studies. Additionally, the research study advocated that health professionals should consider screening for diabetes in patients looking for chronic pain relief, such as back pain or neck pain.
Chronic pain affects many individuals with diabetes. The most common type of chronic pain frequently reported by patients with diabetes include neck pain, back pain, and neuropathic pain in the hands and feet. Chronic pain can affect an individual’s daily physical activities. According to researchers, individuals with diabetes have a higher risk of developing chronic pain, or painful symptoms which persist for more than six months.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
The scope of our information is limited to chiropractic, spinal health issues, and functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
More and more people are choosing chiropractic care for their pack pain and other issues. In fact, they are leaving their traditional medical practices with their pills and surgeries, and opting for the all-natural, non-invasive practice of chiropractic. So why this seemingly sudden exodus over to chiropractic care? It seems that there are several potential reasons.
The American College of Physicians recommends chiropractic for low back pain.
The American College of Physicians published its updated guidelines in 2017, recommending chiropractic and other non-drug treatments, as a first line treatment for chronic and acute lower back pain. Among the treatments listed was spinal manipulation which was �strongly recommended.� It is very effective when combined with exercises like Pilates, yoga, and tai chi.
Studies show chiropractic to be effective for low back pain.
A study published in the April 2017 issue of the Journal of the American Medical Association cited spinal manipulation therapy to be helpful in treating low back pain. The researchers reviewed and analyzed a number of randomized clinical trials that focused on spinal manipulation as a treatment for low back pain. The results were consistent with each, showing that chiropractic treatment, specifically spinal manipulation, was effective in helping low back pain patients with improving function while minimizing pain during treatment courses of up to six weeks.
95% of people who used chiropractic in the past would do it again.
In the 2016 Gallup-Palmer College of Chiropractic Annual Report, 95% of people who have used chiropractic in the past say that it is an effective treatment. What�s more, 97% of people who used a chiropractor in the previous year said that if they had back or neck pain they would seek chiropractic treatment again. More than half of adults who have never seen a chiropractor said they would seek chiropractic treatment if they developed neck or back pain.
In a consumer survey chiropractic was rated higher than all other treatments for back pain.
A Consumer Reports survey published in July 2011 ranked chiropractic higher than Pilates, yoga, and even medications for relieving back pain, osteoarthritis, and neck pain. Many chiropractic patients like the whole-body approach that includes lifestyle recommendations, dietary advice, and supplements for treating pain, immobility, and range of motion issues. Many of the respondents said they opted for the natural treatments like chiropractic in order to avoid the harmful and undesirable side effects of prescription medication.
People are concerned about the opioid epidemic.
With the Centers for Disease Control (CDC) declaring prescription drug (specifically opioid) abuse an epidemic, people are searching for safer, non-drug options. It is startlingly easy for a person to get addicted to pain medication, even while under a doctor�s care. Because of this, natural treatments are becoming more and more popular to people who want to avoid that potential for addiction or who are at a higher risk for becoming addicted.
With spinal fusion surgery on the rise, patients with back pain are seeking less invasive options.
Spinal fusion surgery has been on a steep rise, increasing by 500% in recent years. Many patients are choosing to seek out natural treatments like chiropractic in order to avoid a surgery this drastic. It also helps that chiropractic looks at the whole person and the patient may get advice on lifestyle habits they need to change, dietary adjustments, and exercises that they can do at home.
Alessio Nencioni, Irene Caffa, Salvatore Cortellino and Valter D. Longo
Abstract | The vulnerability of cancer cells to nutrient deprivation and their dependency on specific metabolites are emerging hallmarks of cancer. Fasting or fasting-mimicking diets (FMDs) lead to wide alterations in growth factors and in metabolite levels, generating environments that can reduce the capability of cancer cells to adapt and survive and thus improving the effects of cancer therapies. In addition, fasting or FMDs increase resistance to chemotherapy in normal but not cancer cells and promote regeneration in normal tissues, which could help prevent detrimental and potentially life-threatening side effects of treatments. While fasting is hardly tolerated by patients, both animal and clinical studies show that cycles of low-calorie FMDs are feasible and overall safe. Several clinical trials evaluating the effect of fasting or FMDs on treatment-emergent adverse events and on efficacy outcomes are ongoing. We propose that the combination of FMDs with chemotherapy, immunotherapy or other treatments represents a potentially promising strategy to increase treatment efficacy, prevent resistance acquisition and reduce side effects.
Dietary and lifestyle-related factors are key determinants of the risk of developing cancer, with certain cancers being more dependent on dietary habits than others1�9 . Consistent with this notion, obesity is estimated to account for 14% to 20% of all cancer-related mortality in the United States7 , leading to guidelines on nutrition and physical activity for reducing the risk of developing cancer6 . In addition, given the emerging propensity of cancer cells, but not of normal tissues, to disobey anti-growth signals (owing to oncogenic mutations)10 and their inability to properly adapt to fasting conditions11,12, there is growing interest in the possibility that certain calorie-limited diets could also become an integral part of cancer prevention and, perhaps, of cancer treatment as a means to increase efficacy and tolerability of anticancer agents11�13.
Even though in the past decade we have witnessed unprecedented changes and remarkable advances in cancer treatment14,15, there remains a crucial need for more effective and, possibly, curative approaches for tumours but also, and just as importantly, for strategies to reduce the side effects of cancer treatments15,16. The issue of treatment-emergent adverse events (TEAEs) is one of the key hurdles in medical oncology15,16. In fact, many patients with cancer experience acute and/or longterm side effects of cancer treatments, which may require hospitalization and aggressive treatments (such as antibiotics, haematopoietic growth factors and blood transfusions) and profoundly affect their quality of life (for example, chemotherapyinduced peripheral neuropathy)16. Thus, effective toxicity-mitigating strategies are warranted and anticipated to have major medical, societal and economic impact15,16.
Fasting forces healthy cells to enter a slow division and highly protected mode that protects them against toxic insults derived from anticancer drugs while sensitizing different types of cancer cells to these therapeutics11,12,17. This discovery implies that a single dietary intervention could potentially help address different and equally important aspects of cancer therapy.
In this Opinion article, we discuss the biological rationale for using fasting or fasting-mimicking diets (FMDs) to blunt TEAEs but also to prevent and treat cancer. We also illustrate the caveats of this experimental approach18,19 and the published and ongoing clinical studies in which fasting or FMDs have been applied to patients with cancer.
Systemic & Cellular Fasting Response
Fasting leads to changes in the activity of many metabolic pathways associated with the switch into a mode able to generate energy and metabolites using carbon sources released primarily from adipose tissue and in part from muscle. The changes in the levels of circulating hormones and metabolites translate into a reduction in cell division and metabolic activity of normal cells and ultimately protect them from chemotherapeutic insults11,12. Cancer cells, by disobeying the anti-growth orders dictated by these starvation conditions, can have the opposite response of normal cells and therefore become sensitized to chemotherapy and other cancer therapies.
Systemic Response To Fasting
The response to fasting is orchestrated in part by the circulating levels of glucose, insulin, glucagon, growth hormone (GH), IGF1, glucocorticoids and adrenaline. During an initial post-absorptive phase, which typically lasts 6�24hours, insulin levels start to fall, and glucagon levels rise, promoting the breakdown of liver glycogen stores (which are exhausted after approximately 24hours) and the consequent release of glucose for energy.
Glucagon and low levels of insulin also stimulate the breakdown of triglycerides (which are mostly stored in adipose tissue) into glycerol and free fatty acids. During fasting, most tissues utilize fatty acids for energy, while the brain relies on glucose and on ketone bodies produced by hepatocytes (ketone bodies can be produced from acetyl-CoA generated from fatty acid ?-oxidation or from ketogenic amino acids). In the ketogenic phase of fasting, ketone bodies reach concentrations in the millimolar range, typically starting after 2�3 days from the beginning of the fast. Together with fat-derived glycerol and amino acids, ketone bodies fuel gluconeogenesis, which maintains glucose levels at a concentration of approximately 4mM (70mg per dl), which is mostly utilized by the brain.
Glucocorticoids and adrenaline also contribute to direct the metabolic adaptations to fasting, helping maintain blood sugar levels and stimulating lipolysis20,21. Notably, although fasting can at least temporarily increase GH levels (to increase gluconeogenesis and lipolysis and to decrease peripheral glucose uptake), fasting reduces IGF1 levels. In addition, under fasting conditions, IGF1 biological activity is restrained in part by an increase in the levels of insulin-like growth factor binding protein 1 (IGFBP1), which binds to circulating IGF1 and prevents its interaction with the corresponding cell surface receptor22.
Finally, fasting decreases the levels of circulating leptin, a hormone predominantly made by adipocytes that inhibits hunger, while increasing the levels of adiponectin, which increases fatty acid breakdown23,24. Thus, in conclusion, the hallmarks of the mammalian systemic response to fasting are low levels of glucose and insulin, high levels of glucagon and ketone bodies, low levels of IGF1 and leptin and high levels of adiponectin.
Cellular Response To Fasting
The response of healthy cells to fasting is evolutionarily conserved and confers cell protection, and at least in model organisms, has been shown to increase lifespan and healthspan12,22,25�31. The IGF1 signalling cascade is a key signalling pathway involved in mediating the effects of fasting at the cellular level. Under normal nutrition, protein consumption and increased levels of amino acids increase IGF1 levels and stimulate AKT and mTOR activity, thereby boosting protein synthesis. Vice versa, during fasting, IGF1 levels and downstream signalling decrease, reducing AKT-mediated inhibition of mammalian FOXO transcription factors and allowing these transcription factors to transactivate genes, leading to the activation of enzymes such as haem oxygenase 1 (HO1), superoxide dismutase (SOD) and catalase with antioxidant activities and protective effects32�34. High glucose levels stimulate protein kinase A (PKA) signalling, which negatively regulates the master energy sensor AMP-activated protein kinase (AMPK)35, which, in turn, prevents the expression of the stress resistance transcription factor early growth response protein 1 (EGR1) (Msn2 and/or Msn4 in yeast)26,36.
Fasting and the resulting glucose restriction inhibit PKA activity, increase AMPK activity and activate EGR1 and thereby achieve cell-protective effects, including those in the myocardium22,25,26. Lastly, fasting and FMDs (see below for their composition) also have the ability to promote regenerative effects (Box 1) by molecular mechanisms, some of which have been implicated in cancer, such as increased autophagy or induction of sirtuin activity22,37�49.
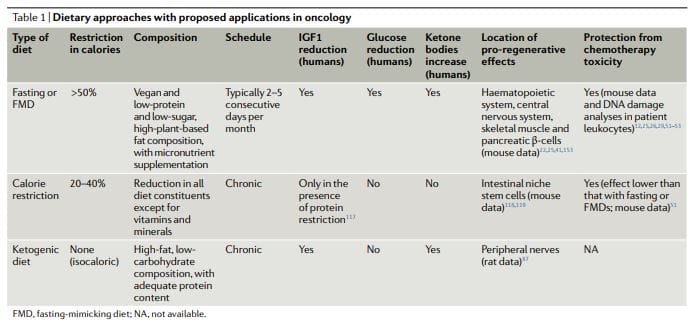
Dietary Approaches In Cancer FMDs
The dietary approaches based on fasting that have been investigated more extensively in oncology, both preclinically and clinically, include water fasting (abstinence from all food and drinks except for water) and FMDs11,12,17,25,26,50�60 (Table 1). Preliminary clinical data indicate that a fast of at least 48hours may be required to achieve clinically meaningful effects in oncology, such as preventing chemotherapy-induced DNA damage to healthy tissues and helping to maintain patient quality of life during chemotherapy52,53,61.
However, most patients refuse or have difficulties completing water fasting, and the potential risks of the extended calorie and micronutrient deficiency associated with it are difficult to justify. FMDs are medically designed dietary regimes very low in calories (that is, typically between 300 and 1,100kcal per day), sugars and proteins that recreate many of the effects of water-only fasting but with better patient compliance and reduced nutritional risk22,61,62. During an FMD, patients typically receive unrestricted amounts of water, small, standardized portions of vegetable broths, soups, juices, nut bars, and herbal teas, as well as supplements of micronutrients. In a clinical study of 3 monthly cycles of a 5-day FMD in generally healthy subjects, the diet was well tolerated and reduced trunk and total body fat, blood pressure and IGF1 levels62. In previous and ongoing oncological clinical trials, fasting or FMDs have typically been administered every 3�4 weeks, for example, in combination with chemotherapy regimens, and their duration has ranged between 1 and 5 days52,53,58,61,63�68. Importantly, no serious adverse events (level G3 or above, according to Common Terminology Criteria for Adverse Events) were reported in this studies52,53,58,61.
Ketogenic Diets
Ketogenic diets (KDs) are dietary regimens that have normal calorie, high-fat and low-carbohydrate content69,70. In a classical KD, the ratio between the weight of fat and the combined weight of carbohydrate and protein is 4:1. Of note, FMDs are also ketogenic because they have high-fat content and have the ability to induce substantial elevations (?0.5mmol per litre) in the levels of circulating ketone bodies. In humans, a KD can also reduce IGF1 and insulin levels (by more than 20% from baseline values), although these effects are affected by the levels and types of carbohydrates and protein in the diet71. KDs can reduce blood glucose levels, but they normally remain within the normal range (that is,>4.4mmol per litre)71.
Notably, KDs may be effective for preventing the increase in glucose and insulin that typically occurs in response to PI3K inhibitors, which was proposed to limit their efficacy72. Traditionally, KDs have been used for treating refractory epilepsy, mainly in children69. In mouse models, KDs induce anticancer effects, particularly in glioblastoma70,72�86. Clinical studies indicate that KDs probably have no substantial therapeutic activity when used as single agents in patients with cancer and suggest that potential benefits of these diets should be sought in combination with other approaches, such as chemotherapy, radiotherapy, antiangiogenic treatments, PI3K inhibitors and FMDs72,73.
KDs were reported to have neuroprotective effects in peripheral nerves and in the hippocampus87,88. However, it remains to be established whether KDs also have proregenerative effects similar to fasting or FMDs (Box 1) and whether KDs also can be used to protect living mammals from the toxicity of chemotherapy. Notably, the regenerative effects of fasting or FMDs appear to be maximized by the switch from the starvation-response mode, which involves the breakdown of cellular components and the death of many cells, and the re-feeding period, in which cells and tissues undergo reconstruction22. Because KDs do not force entry into a starvation mode, do not promote a major breakdown of intracellular components and tissues and do not include a refeeding period, they are unlikely to cause the type of coordinated regeneration observed during the FMD refeeding.
Calorie Restriction
While chronic calorie restriction (CR) and diets deficient in specific amino acids are very different from periodic fasting, they share with fasting and FMDs a more or less selective restriction in nutrients, and they have anticancer effects81,89�112. CR typically involves a chronic 20�30% reduction in energy intake from the standard calorie intake that would allow an individual to maintain a normal weight113,114. It is very effective in reducing cardiovascular risk factors and cancer incidence in model organisms, including primates108,109,114.
However, CR can cause side effects, such as changes in physical appearance, increased cold sensitivity, reduced strength, menstrual irregularities, infertility, loss of libido, osteoporosis, slower wound healing, food obsession, irritability, and depression. In patients with cancer, there are substantial concerns that it may exacerbate malnutrition and that it will unavoidably cause excessive loss of lean body mass18,113�116. CR reduces fasting blood glucose levels, though they remain within the normal range114. In humans, chronic CR does not affect IGF1 levels unless a moderate protein restriction is also implemented117.
Studies show that by reducing mTORC1 signaling in Paneth cells, CR augments their stem cell function and that it also protects reserve intestinal stem cells from DNA damage118,119, but it is unknown whether pro-regenerative effects in other organs are also elicited by CR. Thus, the available data suggest that fasting and FMDs create a metabolic, regenerative and protective profile that is distinct and probably more potent than that elicited by a KD or CR.
Fasting & FMDs In Therapy: Effects on hormone and metabolite levels
Many of the changes in the levels of circulating hormones and metabolites that are typically observed in response to fasting have the capability to exert antitumour effects (that is, reduced levels of glucose, IGF1, insulin and leptin and increased levels of adiponectin)23,120,121 and/or to afford protection of healthy tissues from side effects (that is, reduced levels of IGF1 and glucose). Because ketone bodies can inhibit histone deacetylases (HDACs), the fasting-induced increase of ketone bodies may help slow tumor growth and promote differentiation through epigenetic mechanisms122.
However, the ketone body acetoacetate has been shown to accelerate, instead of reduce, the growth of certain tumors, such as melanomas with mutated BRAF123. Those changes for which there is the strongest evidence for a role in the beneficial effects of fasting and FMDs against cancer are the reductions in the levels of IGF1 and glucose. At the molecular level, fasting or an FMD reduces intracellular signaling cascades including IGF1R�AKT�mTOR�S6K and cAMP�PKA signaling, increases autophagy, helps normal cells withstand stress and promotes anticancer immunity25,29,56,124
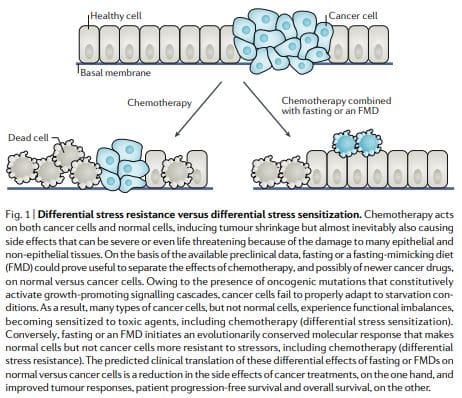
Some yeast oncogene orthologues, such as Ras and Sch9 (functional orthologue of mammalian S6K), are able to decrease stress resistance in model organisms27,28. In addition, mutations that activate IGF1R, RAS, PI3KCA or AKT, or that inactivate PTEN, are present in the majority of human cancers10. Together, this led to the hypothesis that starvation would cause opposite effects in cancer versus normal cells in terms of their ability to withstand cell stressors, including chemotherapeutics. In other words, starvation can lead to a differential stress resistance (DSR) between normal and cancer cells.
According to the DSR hypothesis, normal cells respond to starvation by downregulating proliferation associated and ribosome biogenesis and/or assembly genes, which forces cells to enter a self-maintenance mode and shields them from the damage caused by chemotherapy, radiotherapy and other toxic agents. By contrast, in cancer cells, this self-maintenance mode is prevented through oncogenic changes, which cause constitutive inhibition of stress response pathways12 (Fig. 1). Consistent with the DSR model, short-term starvation or the deletion of proto-oncogene homologues (that is, Sch9 or both Sch9 and Ras2) increased protection of Saccharomyces cerevisiae against oxidative stress or chemotherapy drugs by up to 100-fold as compared with yeast cells expressing the constitutively active oncogene homologue Ras2val19.
Similar results were obtained in mammalian cells: exposure to low-glucose media protected primary mouse glia cells against toxicity from hydrogen peroxide or cyclophosphamide (a prooxidant chemotherapeutic) but did not protect mouse, rat and human glioma and neuroblastoma cancer cell lines. Consistent with these observations, a 2-day fasting effectively increased the survival of mice treated with high-dose etoposide compared with non-fasted mice and increased the survival of neuroblastoma allograftbearing mice compared with non-fasted tumor-bearing mice12.
Subsequent studies found that reduced IGF1 signaling in response to fasting protects primary glia and neurons, but not glioma and neuroblastoma cells, from cyclophosphamide and from pro-oxidative compounds and protects mouse embryonic fibroblasts from doxorubicin29. Liver IGF1-deficient (LID) mice, transgenic animals with a conditional liver Igf1 gene deletion that exhibit a 70�80% reduction in circulating IGF1 levels (levels similar to those achieved by a 72-hour fast in mice)29,125, were protected against three out of four chemotherapy drugs tested, including doxorubicin.
Histology studies showed signs of doxorubicin-induced cardiac myopathy in only doxorubicin-treated control mice but not in LID mice. In experiments with melanoma-bearing animals treated with doxorubicin, no difference in terms of disease progression between control and LID mice was observed, indicating that cancer cells were not protected from chemotherapy by reduced IGF1 levels. Yet, again, tumour-bearing LID mice exhibited a remarkable survival advantage compared with the control animals owing to their ability to withstand doxorubicin toxicity29. Thus, overall, these results confirmed that IGF1 downregulation is a key mechanism by which fasting increases chemotherapy tolerability.
Both dexamethasone and mTOR inhibitors are widely used in cancer treatment, either because of their efficacy as anti-emetics and anti-allergics (that is, corticosteroids) or for their antitumour properties (that is, corticosteroids and mTOR inhibitors). However, one of their main and frequently dose-limiting side effects is hyperglycaemia. Consistent with the notion that increased glucose�cAMP� PKA signalling reduces resistance to toxicity of chemotherapeutic drugs12,26,126, both dexamethasone and rapamycin increase toxicity of doxorubicin in mouse cardiomyocytes and mice26. Interestingly it was possible to reverse such toxicity by reducing circulating glucose levels through either fasting or insulin injections26.
These interventions reduce PKA activity while increasing AMPK activity and thereby activating EGR1, indicating that cAMP� PKA signalling mediates the fasting-induced DSR via EGR1 (ref. 26). EGR1 also promotes the expression of cardioprotective peptides, such as the atrial natriuretic peptide (ANP) and the B-type natriuretic peptide (BNP) in heart tissue, which contributes to the resistance to doxorubicin. Furthermore, fasting and/or FMD might protect mice from doxorubicin-induced cardiomyopathy by boosting autophagy, which may promote cellular health by reducing reactive oxygen species (ROS) production through the elimination of dysfunctional mitochondria and by removal of toxic aggregates.
In addition to reducing chemotherapyinduced toxicity in cells and increasing survival of chemotherapy-treated mice, cycles of fasting induce bone marrow regeneration and prevent the immunosuppression caused by cyclophosphamide in a PKA-related and IGF1-related manner25. Thus, compelling preclinical results indicate the potential of fasting and FMDs to increase chemotherapy tolerability and to avoid major side effects. Because initial clinical data lend further support to this potential, these preclinical studies build a strong rationale for evaluating FMDs in randomized clinical trials with TEAEs as a primary end point.
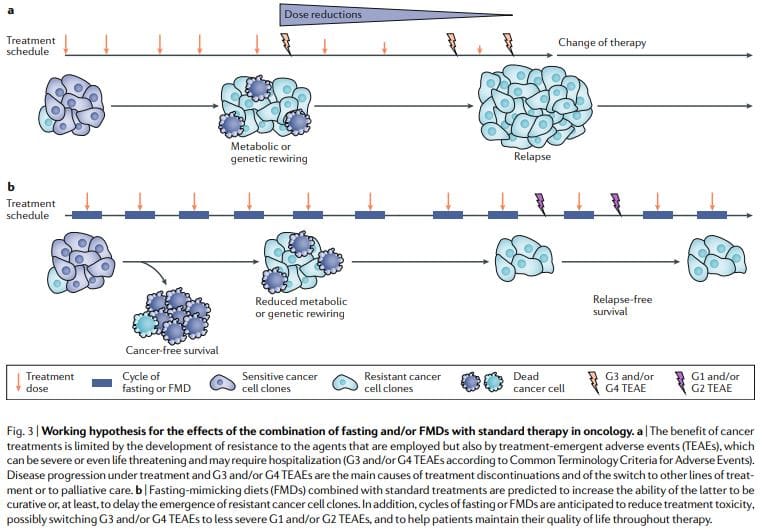
Differential Stress Sensitization: Increasing The Death of Cancer Cells
If used alone, most dietary interventions, including fasting and FMDs, have limited effects against cancer progression. According to the differential stress sensitization (DSS) hypothesis, the combination of fasting or FMDs with a second treatment is much more promising11,12. This hypothesis predicts that, while cancer cells are able to adapt to limited oxygen and nutrient concentrations, many types of cancer cells are not able to execute changes that would allow survival in the nutrient-deficient and toxic environment generated by the combination of fasting and chemotherapy, for example. Early experiments in breast cancer, melanoma and glioma cells found a paradoxical increase in the expression of proliferation-associated genes or of ribosome biogenesis and assembly genes in response to fasting11,12. Such changes were accompanied by unexpected AKT and S6K activation, a propensity to generate ROS and DNA damage and a sensitization to DNA-damaging drugs (via DSS)11.
We consider such an inappropriate response of cancer cells to the altered conditions including the reduction in IGF1 and glucose levels caused by fasting or FMDs as a key mechanism underlying the antitumour properties of these dietary interventions and their potential usefulness for separating the effects of anticancer treatments on normal versus malignant cells11,12 (Fig. 1). In line with the DSS hypothesis, periodic cycles of fasting or of FMDs are sufficient to slow the growth of many types of tumour cells, ranging from solid tumour cell lines to lymphoid leukaemia cells, in the mouse and, most importantly, to sensitize cancer cells to chemotherapeutics, radiotherapy and tyrosine kinase inhibitors (TKIs)11,17,22,25,50,54�57,59,60,124,127,128.
By reducing glucose availability and increasing fatty acid ?-oxidation, fasting or FMDs can also promote a switch from aerobic glycolysis (Warburg effect) to mitochondrial oxidative phosphorylation in cancer cells, which is necessary for sustaining cancer cell growth in the most nutrient-poor environment50 (Fig. 2). This switch leads to increased ROS production11 as a result of increased mitochondrial respiratory activity and may also involve a reduction in cellular redox potential owing to decreased glutathione synthesis from glycolysis and the pentose phosphate pathway50. The combined effect of ROS augmentation and reduced antioxidant protection boosts oxidative stress in cancer cells and amplifies the activity of chemotherapeutics. Notably, because a high glycolytic activity demonstrated by high-lactate production is predictive of aggressiveness and metastatic propensity in several types of cancer129, the anti-Warburg effects of fasting or FMD have the potential to be particularly effective against aggressive and metastatic cancers.
Apart from a change in metabolism, fasting or FMDs elicit other changes that can promote DSS in pancreatic cancer cells. Fasting increases the expression levels of equilibrative nucleoside transporter 1 (ENT1), the transporter of gemcitabine across the plasma membrane, leading to improved activity of this drug128. In breast cancer cells, fasting causes SUMO2-mediated and/or SUMO3-mediated modification of REV1, a DNA polymerase and a p53-binding protein127. This modification reduces the ability of REV1 to inhibit p53, leading to increased p53-mediated transcription of pro-apoptotic genes and, ultimately, to cancer cell demise (Fig. 2). Fasting also increases the ability of commonly administered TKIs to stop cancer cell growth and/or death by strengthening MAPK signalling inhibition and, thereby, blocking E2F transcription factor-dependent gene expression but also by reducing glucose uptake17,54.
Finally, fasting can upregulate the leptin receptor and its downstream signalling through the protein PR/SET domain 1 (PRDM1) and thereby inhibit the initiation and reverse the progression of B cell and T cell acute lymphoblastic leukaemia (ALL), but not of acute myeloid leukaemia (AML)55. Interestingly, an independent study demonstrated that B cell precursors exhibit a state of chronic restriction in glucose and energy supplies imposed by the transcription factors PAX5 and IKZF1 (ref. 130). Mutations in the genes encoding these two proteins, which are present in more than 80% of the cases of pre-B cell ALL, were shown to increase glucose uptake and ATP levels. However, reconstituting PAX5 and IKZF1 in preB-ALL cells led to an energy crisis and cell demise. Taken together with the previous study, this work indicates that ALL may be sensitive to the nutrient and energy restriction imposed by fasting, possibly representing a good clinical candidate for testing the efficacy of fasting or FMD.
Notably, it is likely that many cancer cell types, including AML29, can acquire resistance by circumventing the metabolic changes imposed by fasting or FMDs, a possibility that is further increased by the metabolic heterogeneity that characterizes many cancers129. Thus, a major goal for the near future will be to identify the types of cancer that are most susceptible to these dietary regimens by means of biomarkers. On the other hand, when combined with standard therapies, fasting or FMDs have rarely resulted in the acquisition of resistance in cancer mouse models, and resistance to fasting combined with chemotherapy is also uncommon in studies in vitro, underlining the importance of identifying therapies that, when combined with FMDs, result in potent toxic effects against cancer cells with minimal toxicity to normal cells and tissues11,17,50,55�57,59,124.
Antitumour Immunity Enhancement by Fasting or FMD
Recent data suggest that fasting or FMDs by themselves, and to a greater extent when combined with chemotherapy, trigger the expansion of lymphoid progenitors and promote tumour immune attack via different mechanisms25,56,60,124. An FMD reduced the expression of HO1, a protein that confers protection against oxidative damage and apoptosis, in cancer cells in vivo but upregulated HO1 expression in normal cells124,131. HO1 downregulation in cancer cells mediates FMD-induced chemosensitization by increasing CD8+ tumour-infiltrating lymphocyte-dependent cytotoxicity, which may be facilitated by the downregulation of regulatory T cells124 (Fig. 2). Another study, which confirmed the ability of fasting or FMDs and CR mimetics to improve anticancer immunosurveillance, implies that the anticancer effects of fasting or FMDs may apply to autophagy competent, but not autophagy-deficient, cancers56. Finally, a recent study of alternate-day fasting for 2 weeks in a mouse colon cancer model showed that, by activating autophagy in cancer cells, fasting downregulates CD73 expression and consequently decreases the production of immunosuppressive adenosine by cancer cells60. Ultimately, CD73 downregulation via fasting was shown to prevent macrophage shift to an M2 immunosuppressive phenotype (Fig. 2). On the basis of these studies, it is appealing to speculate that FMDs could be particularly useful instead of or in combination with immune checkpoint inhibitors132, cancer vaccines or other drugs that prompt antitumour immunity, including some conventional chemotherapeutics133.
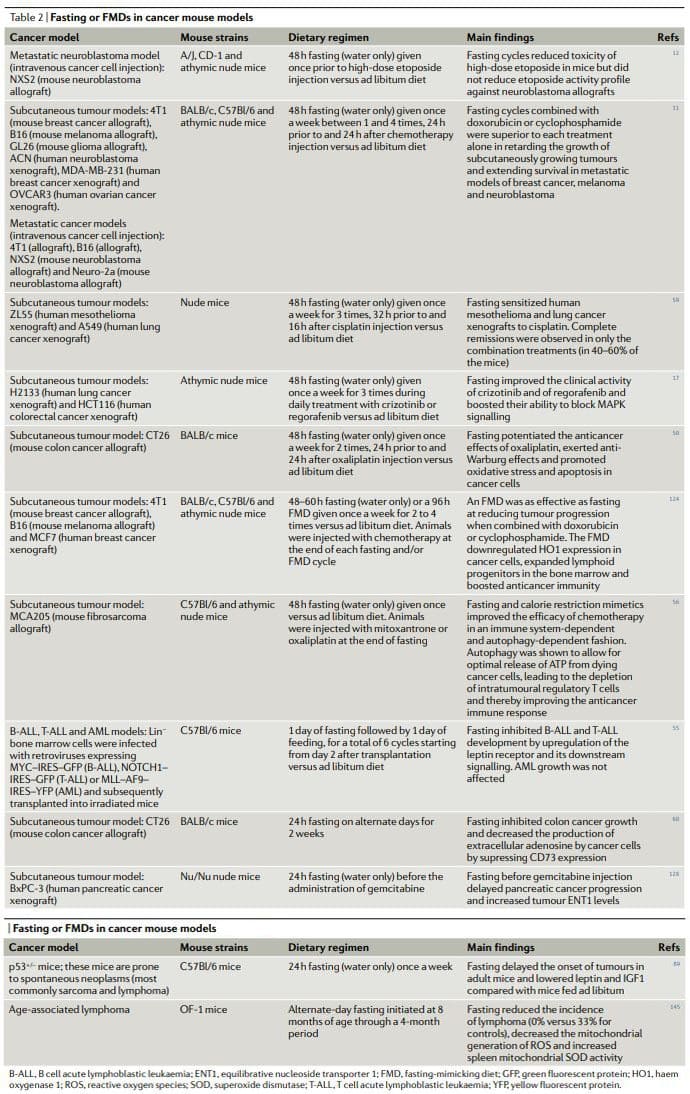
Anticancer Diets in Mouse Models
Overall, the results of preclinical studies of fasting or FMDs in animal cancer models, including models for metastatic cancer (Table 2), show that periodic fasting or FMDs achieve pleiotropic anticancer effects and potentiate the activity of chemotherapeutics and TKIs while exerting protective and regenerative effects in multiple organs22,25. Achieving the same effects without fasting and/or FMDs would require first the identification and then the use of multiple effective, expensive and frequently toxic drugs and would probably be without the advantage of inducing healthy cell protection. It is noteworthy that in at least two studies fasting combined with chemotherapy proved to be the only intervention capable of achieving either complete tumour regressions or long-term survival in a consistent fraction of the treated animals11,59
Chronic KDs also show a tumour growth-delaying effect when used as a monotherapy, particularly in brain cancer mouse models77,78,80�82,84,134. Gliomas in mice maintained on a chronic KD have reduced expression of the hypoxia marker carbonic anhydrase 9 and of hypoxia-inducible factor 1?, decreased nuclear factor-?B activation and reduced vascular marker expression (that is, vascular endothelial growth factor receptor 2, matrix metalloproteinase 2 and vimentin)86. In an intracranial mouse model of glioma, mice fed a KD exhibited increased tumour-reactive innate and adaptive immune responses that were primarily mediated by CD8+ T cells79. KDs were shown to improve the activity of carboplatin, cyclophosphamide and radiotherapy in glioma, lung cancer and neuroblastoma mouse models73�75,135. In addition, a recent study shows that a KD could be very useful in combination with PI3K inhibitors72. By blocking insulin signalling, these agents promote glycogen breakdown in the liver and prevent glucose uptake in the skeletal muscle, which leads to transient hyperglycaemia and to a compensatory insulin release from the pancreas (a phenomenon known as �insulin feedback�). In turn, this raise in insulin levels, which can be protracted, particularly in patients with insulin resistance, reactivates PI3K�mTOR signalling in tumours, thus strongly limiting the benefit of PI3K inhibitors. A KD was shown to be very effective at preventing insulin feedback in response to these drugs and to strongly improve their anticancer activity in the mouse. Finally, according to a study in a murine tumour-induced cachexia model (MAC16 tumours), KDs could help prevent the loss of fat and non-fat body mass in patients with cancer85.
CR reduced tumorigenesis in genetic mouse cancer models, mouse models with spontaneous tumorigenesis and carcinogen induced cancer mouse models, as well as in monkeys91,92,97,98,101,102,104�106,108,109,136�138. By contrast, a study found that CR from middle age actually increases the incidence of plasma cell neoplasms in C57Bl/6 mice139. However, in the same study, CR also extended maximum lifespan by approximately 15%, and the observed increase in cancer incidence was attributed to the increased longevity of mice undergoing CR, the age at which tumour-bearing mice undergoing CR died and the percentage of tumour-bearing mice undergoing CR that died. Thus, the authors concluded that CR probably retards promotion and/or progression of existing lymphoid cancers. A meta-analysis comparing chronic CR with intermittent CR in terms of their ability to prevent cancer in rodents concluded that intermittent CR is more effective in genetically engineered mouse models, but it is less effective in chemically induced rat models90. CR was shown to slow tumour growth and/or to extend mouse survival in various cancer mouse models, including ovarian and pancreatic cancer140,94 and neuroblastoma81.
Importantly, CR improved the activity of anticancer treatment in several cancer models, including the activity of an antiIGF1R antibody (ganitumab) against prostate cancer141, cyclophosphamide against neuroblastoma cells135 and autophagy inhibition in xenografts of HRAS-G12Vtransformed immortal baby mouse kidney epithelial cells100. However, CR or a KD in combination with anticancer therapies seems to be less effective than fasting. A mouse study found that, in contrast to fasting alone, CR alone was not able to reduce the growth of subcutaneously growing GL26 mouse gliomas and that, again, in contrast to short-term fasting, CR did not increase cisplatin activity against subcutaneous 4T1 breast tumours51. In the same study, fasting also proved substantially more effective than CR and a KD at increasing the tolerability of doxorubicin51. Although fasting or an FMD, CR and a KD likely act on and modulate overlapping signalling pathways, fasting or an FMD probably affects such mechanisms in a more drastic fashion during an intense acute phase of a maximum duration of a few days.
The phase of refeeding could then favour the recovery of homeostasis of the whole organism but also activate and invigorate mechanisms that can promote the recognition and removal of the tumour and regenerate the healthy cells. CR and a KD are chronic interventions that are able to only moderately repress nutrient-sensing pathway, possibly without reaching certain thresholds necessary to improve the effects of anticancer drugs, while imposing a major burden and often a progressive weight loss. CR and a KD as chronic dietary regimens in patients with cancer are difficult to implement and likely bear health risks. CR would likely lead to severe loss of lean body mass and the reduction of steroid hormones and possibly immune function142. Chronic KDs are also associated with similar although less severe side effects143. Thus, periodic fasting and FMD cycles lasting less than 5 days applied together with standard therapies have a high potential to improve cancer treatment while reducing its side effects. Notably, it will be important to study the effect of the combination of periodic FMDs, chronic KDs and standard therapies, particularly for the treatment of aggressive cancers such as glioma.
Fasting and FMDs in Cancer Prevention
Epidemiological studies and studies in animals, including monkeys108,109,144, and humans lend support to the notion that chronic CR and periodic fasting and/or an FMD could have cancer-preventive effects in humans. Nevertheless, CR can hardly be implemented in the general population owing to issues of compliance and to possible side effects115. Thus, while evidence-based recommendations of foods to prefer (or to avoid) as well as lifestyle recommendations to reduce cancer risk are becoming established6,8,9,15, the goal now is to identify and, possibly, standardize well tolerated, periodic dietary regimens with low or no side effects and evaluate their cancer-preventive efficacy in clinical studies.
As discussed earlier, FMD cycles cause downregulation of IGF1 and glucose and upregulation of IGFBP1 and ketone bodies, which are changes similar to those caused by fasting itself and are biomarkers of the fasting response22. When C57Bl/6 mice (which spontaneously develop tumours, primarily lymphomas, as they age) were fed such an FMD for 4 days twice a month starting at middle age and an ad libitum diet in the period between FMD cycles, the incidence of neoplasms was reduced from approximately 70% in mice on the control diet to approximately 40% in mice in the FMD group (an overall 43% reduction)22. In addition, the FMD postponed by over 3 months the occurrence of neoplasm related deaths, and the number of animals with multiple abnormal lesions was more than threefold higher in the control group than in the FMD mice, indicating that many tumours in the FMD mice were less aggressive or benign.
A previous study of alternate-day fasting, which was performed in middle-aged mice for a total of 4 months, also found that fasting reduced the incidence of lymphoma, bringing it from 33% (for control mice) to 0% (in fasted animals)145, although because of the short duration of the study it is unknown whether this fasting regimen prevented or simply delayed the tumour onset. Furthermore, alternate-day fasting imposes 15 days per month of complete water-only fasting, whereas in the FMD experiment described above mice were placed on a diet that provided a limited amount of food for only 8 days per month. In humans, 3 cycles of a 5-day FMD once a month were shown to reduce abdominal obesity and markers of inflammation as well as IGF1 and glucose levels in subjects with elevated levels of these markers62, indicating that periodic use of an FMD could potentially have preventive effects for obesity-related or inflammation-related, but also other, cancers in humans, as it has been shown for mice22.
Therefore, the promising results of preclinical studies combined with the clinical data on the effect of an FMD on risk factors for ageing-associated diseases, including cancer62, lend support to future randomized studies of FMDs as a possibly effective tool to prevent cancer, as well as other ageing-associated chronic conditions, in humans.
Clinical Applicability in Oncology
Four feasibility studies of fasting and FMDs in patients undergoing chemotherapy have been published as of today52,53,58,61. In a case series of 10 patients diagnosed with various types of cancer, including breast, prostate, ovarian, uterus, lung and oesophageal cancer, who voluntarily fasted for up to 140hours before and/or up to 56hours following chemotherapy, no major side effects caused by fasting itself other than hunger and lightheadedness were reported58. Those patients (six) who underwent chemotherapy with and without fasting reported a significant reduction in fatigue, weakness and gastrointestinal adverse events while fasting. In addition, in those patients in which cancer progression could be assessed, fasting did not prevent chemotherapy-induced reductions in tumour volume or in tumour markers. In another study, 13 women with HER2 (also known as ERBB2) negative, stage II/III breast cancer receiving neo-adjuvant taxotere, adriamycin and cyclophosphamide (TAC) chemotherapy were randomized to fast (water only) 24hours before and after beginning chemotherapy or to nutrition according to standard guidelines52.
Short-term fasting was well tolerated and reduced the drop in mean erythrocyte and thrombocyte counts 7 days after chemotherapy. Interestingly, in this study, the levels of ?-H2AX (a marker of DNA damage) were increased 30minutes after chemotherapy in leukocytes from non-fasted patients but not in patients who had fasted. In a dose escalation of fasting in patients undergoing platinum-based chemotherapy, 20 patients (who were primarily treated for either urothelial, ovarian or breast cancer) were randomized to fast for 24, 48 or 72hours (divided as 48hours before chemotherapy and 24hours after chemotherapy)53. Feasibility criteria (defined as three or more out of six subjects in each cohort consuming?200kcal per day during the fast period without excess toxicity) were met. Fasting-related toxicities were always grade 2 or below, the most common being fatigue, headache and dizziness. As in the previous study, reduced DNA damage (as detected by comet assay) in leukocytes from subjects who fasted for at least 48hours (as compared with subjects who fasted for only 24hours) could also be detected in this small trial. In addition, a nonsignificant trend towards less grade 3 or grade 4 neutropenia in patients who fasted for 48 and 72hours versus those who fasted for only 24hours was also documented.
Very recently, a randomized crossover clinical trial was conducted assessing the effects of an FMD on quality of life and side effects of chemotherapy in a total of 34 patients with breast or ovarian cancer61. The FMD consisted of a daily caloric intake of<400kcal, primarily by juices and broths, starting 36�48hours before the beginning of chemotherapy and lasting until 24hours after the end of chemotherapy. In this study, the FMD prevented the chemotherapy induced reduction in quality of life and it also reduced fatigue. Again, no serious adverse events of the FMD were reported. Several other clinical trials of FMDs in combination with chemotherapy or with other types of active treatments are currently ongoing at US and European hospitals, primarily in patients who are diagnosed with breast or prostate cancer63,65�68. These are either one-arm clinical studies to assess FMD safety and feasibility or randomized clinical studies focusing either on the effect of the FMD on the toxicity of chemotherapy or on the quality of life of patients during chemotherapy itself. Altogether, these studies have now enrolled over 300 patients, and their first results are expected to become available in 2019.
Challenges in The Clinic
The study of periodic fasting or of FMDs in oncology is not devoid of concerns, particularly in relation to the possibility that this type of dietary regimen could precipitate malnutrition, sarcopenia, and cachexia in predisposed or frail patients (for example, patients who develop anorexia as a consequence of chemotherapy)18,19. However, no instances of severe (above grade 3) weight loss or of malnutrition were reported in the clinical studies of fasting in combination with chemotherapy published as of now, and those patients who did experience a weight loss during fasting typically recovered their weight before the subsequent cycle without detectable harm. Nevertheless, we recommend that periodic anorexia and nutritional status assessments using gold-standard approaches18,19,146�150 should be an integral part of these studies and that any ensuing nutritional impairment in patients undergoing fasting and/or FMDs is rapidly corrected.
Conclusions
Periodic fasting or FMDs consistently show powerful anticancer effects in mouse cancer models including the ability to potentiate chemoradiotherapy and TKIs and to trigger anticancer immunity. FMD cycles are more feasible than chronic dietary regimens because they allow patients to consume food regularly during the FMD, maintain a normal diet between cycles and do not result in severe weight loss and possibly detrimental effects on the immune and endocrine systems. Notably, as standalone therapies, periodic fasting or FMD cycles would probably show limited efficacy against established tumors. In fact, in mice, fasting or FMDs affect the progression of a number of cancers similarly to chemotherapy, but alone, they rarely match the effect obtained in combination with cancer drugs which can result in cancer-free survival11,59. Thus, we propose that it is the combination of periodic FMD cycles with standard treatments that holds the highest potential to promote cancer-free survival in patients, as suggested by the mouse models11,59 (Fig. 3).
This combination may be particularly potent for several reasons: first, cancer drugs and other therapies can be effective, but a portion of patients do not respond because cancer cells adopt alternative metabolic strategies leading to survival. These alternative metabolic modes are much more difficult to sustain under fasting or FMD conditions because of the deficiencies or changes in glucose, certain amino acids, hormones, and growth factors, as well as in other unknown pathways leading to cell death. Second, fasting or FMDs can prevent or reduce resistance acquisition. Third, fasting or FMDs protect normal cells and organs from the side effects caused by a wide variety of cancer drugs. On the basis of preclinical and clinical evidence of feasibility, safety and efficacy (at reducing IGF1, visceral fat and cardiovascular risk factors), FMDs also appear as a viable dietary approach to be studied in cancer prevention. An important future challenge will be to identify those tumours that are the best candidates to benefit from fasting or FMDs. Even in cancer types that are apparently less responsive to fasting or FMDs, it may still be possible to identify the mechanisms of resistance and to intervene with drugs able to revert that resistance. Conversely, more caution should be adopted with other types of diets, especially if high in calories, as they could lead to exacerbated and not inhibited growth of certain cancers. For example, the KD increases growth of a melanoma model with mutated BRAF in mice123, and it was also reported to accelerate disease progression in a mouse AML model72.
Furthermore, it is essential to apply FMDs with an understanding of the mechanisms of action, since their potency if applied incorrectly could generate negative effects. For example, when rats were fasted and treated with a potent carcinogen before refeeding, this resulted in the growth of aberrant foci in liver, colon and rectum when compared with non-fasted rats151,152. Although the mechanisms involved in this effect are not understood, and these foci may have not resulted in tumours, these studies suggest that a minimum period of 24�48hours between the chemotherapy treatment and the return to the normal diet is important to avoid combining the regrowth signals present during the refeeding after fasting with high levels of toxic drugs such as chemotherapy. The clinical studies of fasting or FMD in patients undergoing chemotherapy support its feasibility and overall safety52,53,58,61. In a small-size randomized trial that enrolled 34 patients, an FMD helped patients maintain their quality of life during chemotherapy and reduced fatigue61. In addition, preliminary data suggest the potential of fasting or FMDs to reduce chemotherapy induced DNA damage in healthy cells in patients52,53.
Ongoing clinical studies of FMDs in patients with cancer63,65�68 will provide more solid answers as to whether prescribing periodic FMDs in combination with conventional anticancer agents helps improve tolerability and activity of the latter. It is important to consider that FMDs will not be effective in reducing the side effects of cancer treatments in all patients and neither will they work to improve the efficacy of all therapies, but they have great potential to do so at least for a portion and possibly for a major portion of patients and drugs. Frail or malnourished patients or patients at risk of malnutrition should not be enrolled in clinical studies of fasting or FMDs, and patient nutritional status and anorexia should be carefully monitored throughout clinical trials. An appropriate intake of proteins, essential fatty acids, vitamins and minerals combined, where possible, with light and/or moderate physical activity aimed at increasing muscle mass should be applied between fasting or FMD cycles in order for the patients to maintain a healthy lean body mass18,19. This multimodal dietary approach will maximize the benefits of fasting or FMDs while at the same time protecting patients from malnutrition.
Although oral devices, such as splints and bite guards, are the most prevalent treatments for facial pain associated with temporomandibular disorders, or TMD, patients have found that these remedies are frequently less effective than self-care techniques, such as jaw exercises or warm compresses, according to a new research study published by researchers at the New York University (NYU) College of Dentistry in New York City.
The research study, published in the journal Clinical Oral Investigations, demonstrates that self-care techniques should primarily be utilized to help treat muscle-related temporomandibular disorders or TMD.
TMD, occasionally known as TMJ after the temporomandibular joint, is a collection of prevalent painful conditions which develop in the jaw joint and its surrounding muscles. Myofascial temporomandibular disorder, or mTMD, is a muscular condition which affects over 10 percent of women. Individuals with TMD often suffer from other chronic pain conditions. Research studies found that 7 to 18 percent of people with TMD also experience fibromyalgia, a condition characterized by widespread pain.
Treatments for TMD and Fibromyalgia
Dentists and patients utilize an assortment of treatments to help manage facial pain, such as oral devices like splints and bite guards, pain medicines, including nonsteroidal anti-inflammatory drugs, and self-care methods like jaw exercises and hot compresses.
Oral devices are a prevalent first-line treatment for TMD, regardless of research study outcome measures regarding their advantages, stated Vivian Santiago, Ph.D., MPH, research study scientist at the Department of Oral and Maxillofacial Pathology, Radiology, and Medicine at NYU College of Dentistry, and the research study’s leading author.
“While oral splints have been discovered to have some benefits, they have yet to be found to be as successful for patients who have widespread pain when treating mTMD,” she explained.
In this research study, the researchers evaluated what non-medication remedies women with mTMD utilized to handle their pain as well as how successful patients perceived these remedies. The researchers interviewed a total of 125 women including 26 women who had fibromyalgia and mTMD, so as to find out whether treatment differed for patients.
The most frequent treatments reported were oral devices (utilized by 59 percent of participants), physical therapy (utilized by 54 percent of participants), and at-home jaw exercises (utilized by 34 percent of participants). The least frequent treatments reported were acupuncture (utilized by 20 percent), chiropractic care (utilized by 18 percent), trigger point injections (utilized by 14 percent), yoga (utilized by 7 percent), and meditation (utilized by 6 percent). Participants frequently used more than one treatment.
Participants reported the most improvement in their pain from well-known self-care techniques, such as jaw exercises, yoga, meditation, massage, and warm compresses, with over 84 percent reporting that these techniques helped reduce painful symptoms. Only 64 percent of participants who used the oral devices reported that they helped improve their pain. About 11 percent of women who used oral devices stated that these made their pain worse, an area which warrants further research studies.
Oral devices failed to outperform self-care techniques in improving facial pain, according to Karen Raphael, Ph.D., professor at the Department of Oral and Maxillofacial Pathology, Radiology, and Medicine at NYU College of Dentistry, and the research study’s co-author.
“Our outcome measures encourage utilizing self-care techniques as the first line of treatment for mTMD before contemplating more costly interventions,” stated Raphael.
The researchers didn’t find substantial differences between the amount of remedies reported by women with and without fibromyalgia. While the use of alternative treatment options for mTMD was reported among women with fibromyalgia, further research studies are still required. Pain relief tended to be greater through the use of self-care techniques in women with and without fibromyalgia.
“While fibromyalgia is diagnosed by a healthcare professional, such as a rheumatologist, TMD is typically diagnosed and treated by a dentist,” said Santiago. “Our research study demonstrates that dentists must ask patients with facial pain if they also have widespread chronic pain because this might provide more information to help plan their treatment.”
Fibromyalgia is a health issue characterized by widespread chronic pain accompanied by fatigue, sleep, memory and mood problems. Fibromyalgia has been associated with a variety of other health issues, such as TMD and/or TMJ. Individuals with this painful disorder may often struggle to engage in their everyday physical activities. As a qualified and experienced chiropractor, I’ve helped treat numerous patients with fibromyalgia. It’s important for patients to know that they are not alone when it comes to treating their painful symptoms. Chiropractic care is an alternative treatment option which can help treat a variety of health issues, including fibromyalgia.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
The scope of our information is limited to chiropractic, spinal health issues, and functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine