April Hermosillo has achieved overall health and wellness by following proper nutrition and engaging in exercises/physical activities. As a regular fitness participant, April Hermosillo can experience low back pain which affects even her most basic tasks. April Hermosillo struggled with spine health issues and sciatica before receiving chiropractic care.
Dr. Alex Jimenez is a chiropractor in El Paso, TX who has helped April Hermosillo achieve pain relief so she can return to her everyday fitness routines. April Hermosillo describes how Dr. Jimenez has tremendously helped improve her overall symptoms. April Hermosillo highly recommends Dr. Alex Jimenez as the non-surgical choice for personalized spine and sciatica treatment and rehabilitation.
El Paso Back Clinic
We are blessed to present to you El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend us.
Fred Foreman is a basketball coach who depends on his overall health and wellness to be able to engage in his everyday responsibilities. As a result, coach Foreman started the 6 Day Detox Program from Xymogen, designed to help renew and enhance the human body’s cleansing and detoxification capabilities.
Fred Foreman discusses his experience with the 6 Day Detox Program, describing the benefits he developed as well as the effort he had to implement, to support his overall health and wellness through the detox. Fred Foreman feels a great sense of fulfillment with the 6 Day Detox Program and he encourages other people, who also wish to improve their well-being, to detox their body. Coach Foreman highly recommends the 6 Day Detox Program as an alternative treatment choice for overall health and wellness.
Injury Medical & Chiropractic Clinic
We are blessed to present to you El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend us.
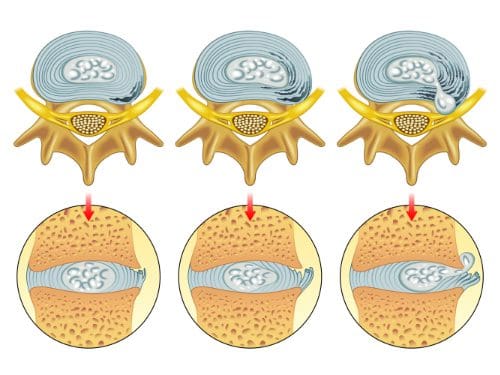
A herniated disc is a common spinal disc issue. The spine is a very intricate structure, and when one component fails to function correctly, it can affect the entire body, causing pain and loss of mobility.
Tiny bones, called vertebrae, are stacked on each other to form the spine. They are joined in such a way to facilitate movement, flexibility, and a wide range of motion. There are small, fluid-filled discs that rest between each vertebra, providing a cushion between the bones. When one of these discs becomes damaged, it can affect the surrounding nerves, causing pain and making movement difficult.
What is It?
A herniated disc is a common spinal condition that typically affects the cervical spine (neck region) or the lumbar spine (lower back), although it can occur in any part of the spine. Most often, a herniated disc happens at the L4 � L5 and the L5 � S1. This is because this portion of the spine, the lumbar region, bears the bulk of the body�s weight.
It is often referred to as a ruptured disc or slipped disc and occurs when the disc moves or slips out of place. It can also be the result of a disc that has a small tear and is leaking the jelly-like substance that is inside. This can put pressure on the surrounding nerves, causing pain and discomfort.
The first two stages are called incomplete herniations while the last two stages are called complete herniations.
Symptoms of a herniated disc may increase or worsen as the condition progresses although some patients do not experience any at all Typical symptoms include:
Pain in the affected area
Tingling
Numbness
Weakness
Leg or arm pain
Loss of reflex
Loss of mobility
Loss of flexibility
Decreased range of motion
What Causes It?
There are several causes. The most common are aging and degeneration, overuse, and normal wear and tear on the body.
A herniated disc resulting from an injury or trauma, such as a blow to the back, is less common, but it does happen. Because the back does bear most of the body�s weight, it can put a significant amount of pressure on the spine and discs. Over time, the discs may begin to weaken and a herniation can occur.
Injury or trauma that results in a herniation may include a car accident that involves sudden jerking, or incorrectly lifting heaving objects can put excessive pressure on the spine, causing it to herniate.
How is it Diagnosed?
A physical examination is usually the first step in diagnosing a herniated disc. The physician or chiropractor will examine the spine while the patient is standing, then while they are lying down. Depending on the severity and location of the herniation, they may note a decrease in spinal curvature.
Radicular pain will also be assessed, when the spine is unmoving, while in motion, and when pressure is applied. Other tests may also be administered. X-rays may also be taken, but an MRI is usually more accurate and provides greater detail.
What are the Treatments?
Medications may be recommended or prescribed, including NSAIDs, narcotics, muscle relaxers, and anticonvulsants. Some doctors may advise cortisone injections to reduce inflammation. Physical therapy may be recommended as a stand-alone treatment or in conjunctions with other treatments. Surgery for herniated discs is rare and usually reserved as a last resort option.
Chiropractic has been very effective in helping patients manage their pain and regain their mobility so they can return to their normal life. Therefore, it should be your first option for treatment before you go down the road with drugs or surgery.
Healthcare professionals can utilize a variety of clinical assessments to evaluate the methylation status of patients. However, there is no single assessment method or technique which can accurately demonstrate the complexity of methylation in the human body. Current assessments can help provide an understanding into methylation-related genetic polymorphisms, nutrient status, methylation-related neurotransmitters and neurotransmitter metabolites, amino acids, hormones and metabolites, oxidative stress, and detoxification load, all of which can also help provide the understanding of a patient’s methylation status.
Understanding Methylation Status
Some assessment methods and techniques, including measures to determine DNA methylation status, are generally limited to research studies and are not yet available to healthcare professionals. As DNA methylation status assessments become available, healthcare is necessary to understand data because conflicting outcome measures have been demonstrated in research studies based on a variety of methodologies while methylation is further evaluated. Moreover, although methods and techniques, as well as research studies, are quickly evolving, patterns of DNA methylation status in humans across cells, tissues, age, populations, environmental factors like nutrition and lifestyle modifications, and disease, are only just being characterized by healthcare professionals.
It is essential that we emphasize a variety of indicators and be mindful of the restrictions of our interpretations as well as their misunderstood factors. Plasma homocysteine, by way of instance, can decrease as methylation activity improves, however, it can also decrease when oxidative stress levels increase, independently of methylation activity improvements. But, as we�ve previously discussed, only a few SNPs have known, quantifiable changes in enzymatic function, and even then, their overall outcome measures on methylation are unknown. Healthcare professionals must depend on multiple clinical assessments to determine methylation health. In the following articles, we will discuss methylation status assessment options available to healthcare professionals.
Understanding Genetic Profiling
Genetic profiling can help provide some evidence of potential methylation status and risk of developing diseases. Several gene SNPs increase methylation activity, such as CBS, and several other gene SNPs may decrease methylation activity, such as MTHFR, BNMT, MTR, MTRR, and AHCY. However, understanding the overall outcome measures of gene SNPs is complicated to determine through polymorphisms and environmental factors. By way of instance, research studies have demonstrated that the MTHFR C677T polymorphism is associated with an increased risk of autism spectrum disorder, (with an odds ratio = 1.42, 95% CI 1.09-1.85), however, similar research studies have also demonstrated that this risk can decrease through periconceptional folate or folic acid intake.
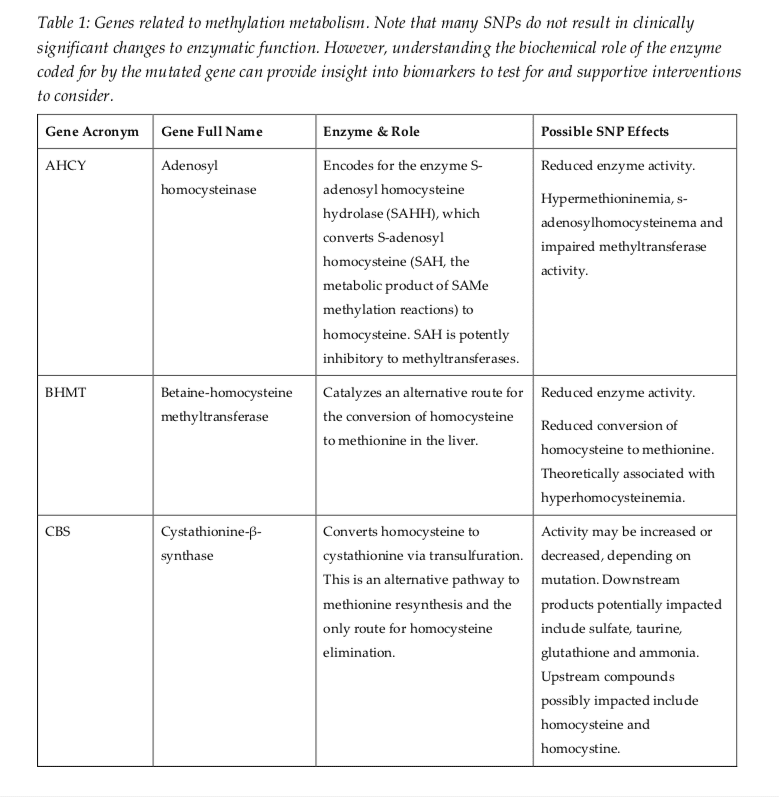
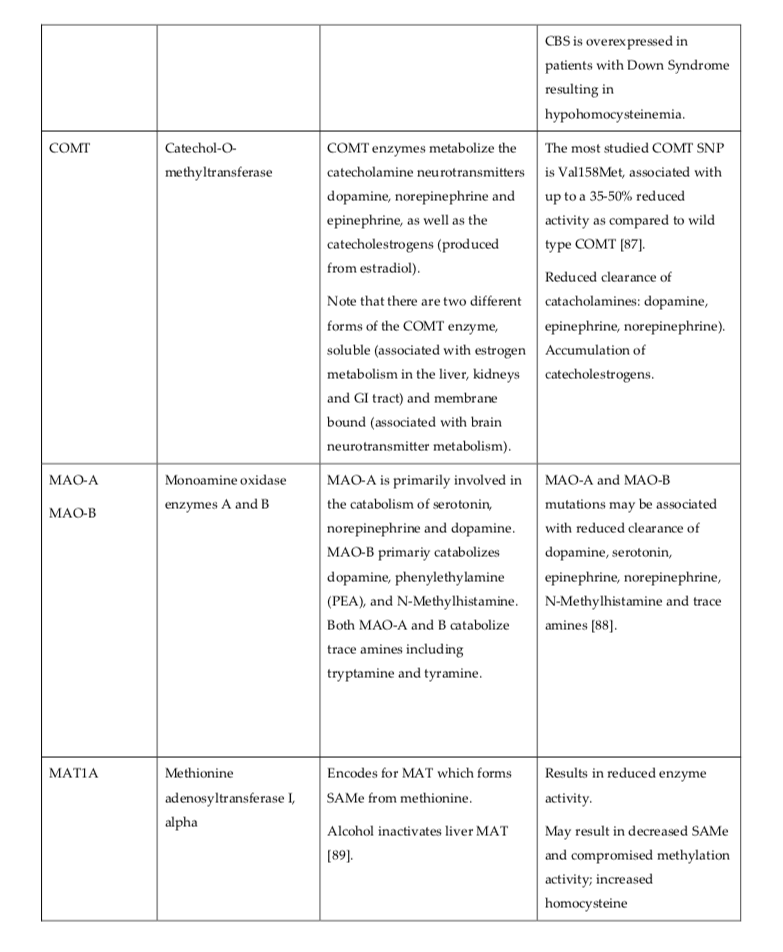
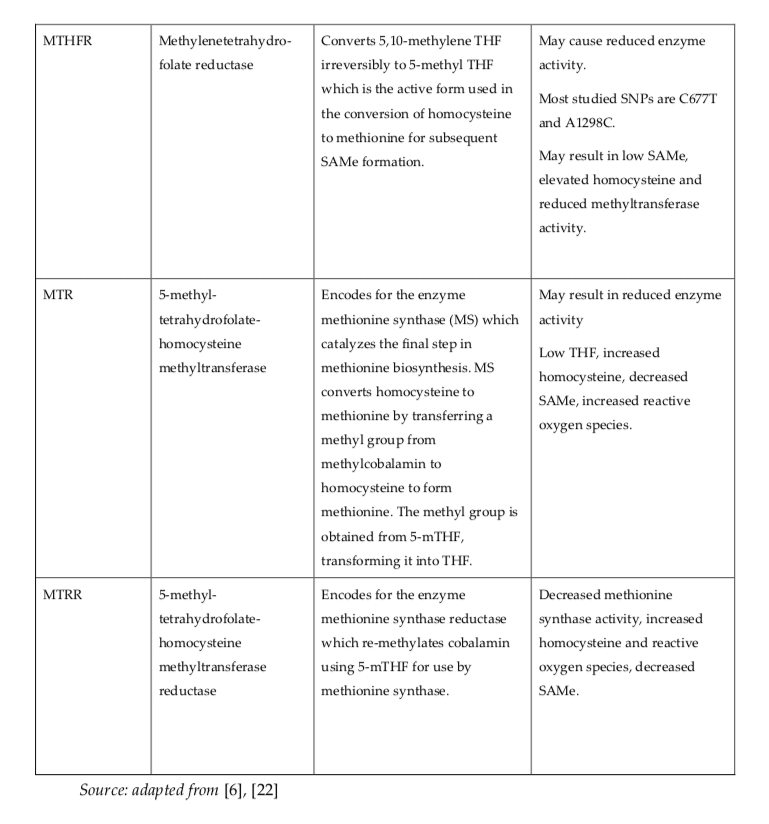
Furthermore, if a maternal MTHFR C677T polymorphism is combined with a CBS polymorphism, a lack of prenatal supplementation with B vitamins, and a fetal COMT polymorphism, the odds ratio for autism spectrum disorder can increase tremendously, (7.2, CI = 2.3�22.4; P=0.05). The risk of diseases associated with genotype is unfortunately rare because research studies on the combined outcome measures of gene SNPs are still very much in their early stages. In many circumstances, healthcare professionals will need to use careful clinical assessments to evaluate as well as to guide their treatments. The methylation-related genes presented in Table 1 below are frequently evaluated for SNPs. The outcome measures can help doctors understand patient methylation status.
A variety of methods and techniques are available to determine the methylation status of patients. However, the assessment of methylation status can still be challenging for many healthcare professionals. DNA methylation is characterized by the addition of a methyl group to DNA. Healthcare professionals must first understand the pros and cons of the variety of methods and techniques available to determine methylation status to allow them to make an informed choice when deciding which assessment will best suit their research study needs.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many doctors and functional medicine practitioners may recommend higher doses of methyl donors in several patients, however, further research studies are needed to determine the proper amount of methylation supplementation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Dr. Alex Jimenez Explains Why Methylation Can Go Wrong
As previously discussed, many healthcare professionals have demonstrated potential concerns associated with folic acid and methyl-folate supplementation. Some risks of folic acid or other folate derivative supplements, such as commonly used alternatives like 5-mTHF and folinic acid, have become widely recognized and they aren’t frequently discussed. These diseases are described below.
Several of these diseases can usually be treated with vitamin B12 supplementation, respectively, and although fundamental, these are not the main focus of the article. However, we will continue to discuss whether or not the side-effects of folic acid supplementation, or aberrant DNA methylation activity, are a result of methylation gone wrong. Epidemiological data suggests an inverse association between folate status and risk of health issues. Research studies have demonstrated that excessive methylation may be harmful.
Diseases Caused by Aberrant Methylation
Aberrant methylation caused by folic acid supplementation is not explained by UMFA or DHF. Therefore, healthcare professionals cannot rule out the possibility of excessive or aberrant methylation as a contributing and/or underlying factor for health issues.
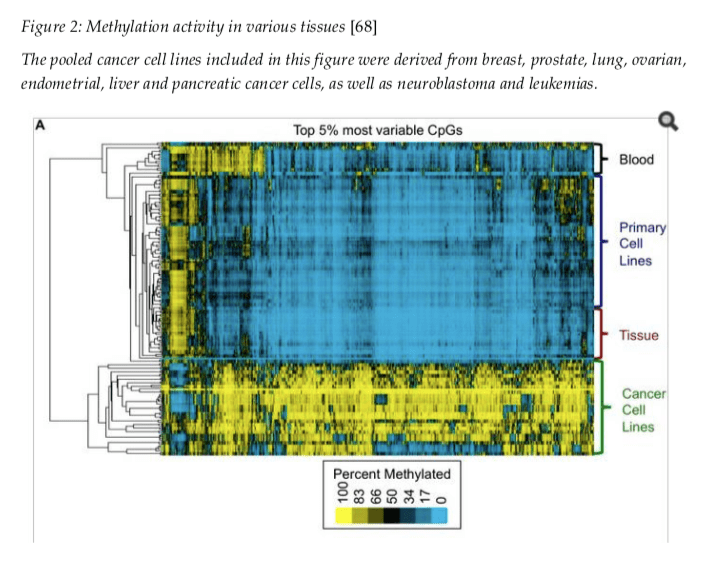
Cancer
Aberrant DNA methylation has been associated as a cause of a variety of cancers. Both loci-specific DNA hyper- and hypo-methylation has been demonstrated to occur in cancer cells, suggesting that both states can be distinguishing of tumorigenesis. Global DNA hypermethylation is also demonstrated in various cancer cells, as shown in Figure 2. The association between folic acid supplementation and colorectal cancer has been evaluated numerous times in research studies. A recent systematic review and meta-analysis demonstrated inconsistent and inconclusive evidence on the association between folic acid on colorectal cancer risk.
However, these research studies may oversee important details about the type, dose, and effect of supplementation as well as the folate, methylation, and disease status of the patient. By way of instance, specific DNA methylation in patients with stage II and III colon cancer has been considerably associated with the increased risk of developing future as well as predicting overall survival (hazard ratio 2.9, 95% CI 1.5-5.8, P=0.002) and disease-free survival (hazard ratio 4.0, 95% CI 1.6-10.2, P=0.003). In another research study, a randomized, controlled trial evaluating the potential benefits of 1 mg/d of folic acid supplementation for the prevention of colorectal adenomas, researchers found that folic acid failed to reduce the risk of the disease. As a matter of fact, researchers found that the risks of colorectal adenoma and noncolorectal cancers, especially prostate cancer, actually increased considerably.
Folic acid intake on breast cancer has also been evaluated in various research studies and is widely considered controversial. By way of instance, in one observational research study, dietary supplementation with folic acid greater or equal to 400 mcg/d was associated with a 20 percent increase in the risk of breast cancer compared with those reporting no supplement intake. In contrast, according to a 2014 Cochrane systematic review, food-sourced folate has protective properties against cancer. A recently published retrospective analysis gathered data from 367,993 women to demonstrate that higher food folate intake is associated with a lower risk of sex-hormone receptor-negative breast cancer in premenopausal women. However, further research studies are still required.
The connection between folate and cancer has also been tremendously analyzed. In a research study of women with breast cancer (n=204) compared with controls (n=408), participants with the highest tertile of plasma folate (median 17 nmol/L) had the highest risk of ER?(-) breast cancer (odds ratio 2.67, CI 1.44�4.92, P=0.001). Several researchers had previously shown an increased risk in breast cancer specifically when the MTHFR C667T polymorphism was combined with high plasma folate levels, which may be a potential concern because patients who are diagnosed with this polymorphism are among the most frequent to take supplemental folates.
In another case-control research study of approximately 300 participants, it appeared that increased levels of serum folate promoted the progression of existing benign tumors, or polyps, into colorectal cancer, however, it also prevented carcinogenesis in healthy controls, leading researchers to determine that serum folate can have dual roles in the onset and progression of cancer. Additionally, recent research studies demonstrate potential dysregulation of one-carbon metabolism in cancer cells, specifically methionine uptake transporters, while increasing the serine-glycine biosynthesis pathway. These outcome measures may potentially explain the harmful effects of folic acid, as well as that of other forms of folate, where there is a prior history of cancer in participants.
We can�t know from these research studies what folate derivative plays the biggest role in these outcome measures, because serum folate demonstrates various folate vitamers, however, we do know that serum folate is largely made up of 5-MTHF, about 86.7% percent, with UMFA typically making up a much smaller amount, about 4.0 percent. Whether the effect of the smaller amount of UMFA is enough to cause the progression of pre-cancerous lesions or whether increased levels of 5-MTHF are also implicated, healthcare professionals have to determine which intervention to choose to present the least risk to the patient’s overall health and wellness.
Autoimmunity
Systemic sclerosis is a misunderstood autoimmune health issue characterized by endothelial injury, immune abnormalities, and fibrosis. It is believed to develop from epigenetic dysfunction in immune cells which trigger immune cell activation and proliferation. Variations in several epigenetic mechanisms are involved in the pathogenesis of the disease. Hypermethylation of specific genes, Fli-1, KLF5, and BMPRII, can ultimately reduce their anti-fibrotic effects. Conversely, the overexpression of immune cells CD40L, CD70, and CD11a, are also involved and have been associated with hypomethylation of their corresponding genes, among other functions.
The pathogenesis of other autoimmune conditions may also be influenced through methylation. IgG4-related autoimmune pancreatitis, or AIP, and other autoimmune-like phenotypes are associated with MST1, a serine/threonine kinase, deficiency in humans, which leads to T-cell immunodeficiency and hypergammaglobulinemia with autoantibody production. IgG4-related AIP patients who also exhibit extrapancreatic lesions demonstrate a considerable increase in the methylation of MST1 and decreased protein development, suggesting that this gene is regulated through methylation and may be associated to the underlying disease. Aberrant methylation, both hypo- and hyper, have also been shown in rheumatoid arthritis and autoimmune thyroid diseases.
Allergy
We also found that researchers believe that environmental exposures which increased DNA methylation may also increase the risk for allergic disease by suppressing Th1 and T regulatory cell differentiation which would otherwise prevent the differentiation of allergy-promoting Th2 cells. In a research study of elderly men (n=704), minor increases, about 0.31 percent, in methylation at gene Alu repeat sequences have been considerably associated with prior sensitization to at least one allergen, raising the possibility that even small changes in epigenetic regulators might have considerable clinical effects. Hypermethylation at specific CpG sites is believed to be useful for differentiating clinically non-reactive and clinically reactive food-allergic phenotypes than serum IgE and skin prick testing.
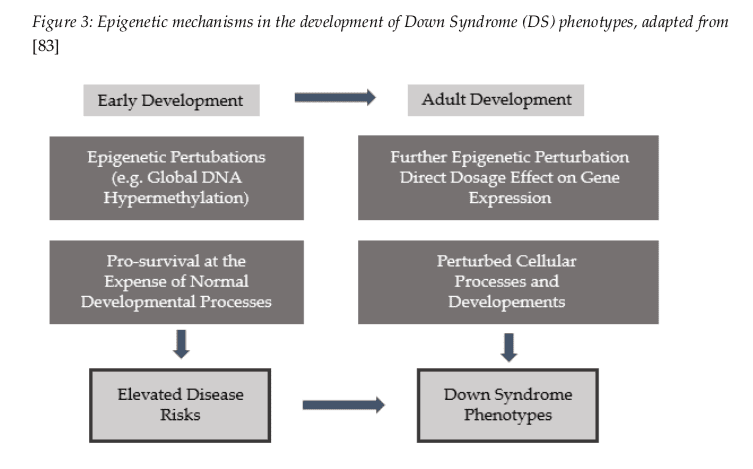
Down Syndrome
In Down Syndrome, early-life downregulation of the TET family genes involved in DNA demethylation and downregulation of REST transcription factor expression and subsequent methylation of REST-vacant sites, are believed to be potential pathways leading to the global DNA hypermethylation associated with Down Syndrome. More details can be found in Figure 3 below.
Reasons to be Cautious
While the effects of methylated folate or folic acid cannot be conclusively determined from the research studies discussed above, there are enough unknowns to justify potential concerns. Research studies are ongoing and it is not yet clear how aggressive 5- MTHF, or other methylation supplementation, affects well-being or the progression of diseases. Data suggest that we should be cautious and focus on supporting the body�s own health and wellness for methylation balance rather than attempting to override them.
Metabolic and DNA methylation are complex in their regulation of gene expression. Epigenomic regulation also depends on many environmental inputs, including both nutritional and lifestyle modifications, which make up methylation activity regulation. A safer way to support methylation activity, especially over the longer term, is through food-based nutrients as well as food and lifestyle practices which have been demonstrated to promote favorable methylation activity and epigenetic imprints in patients with these diseases.
DNA methylation is a fundamental epigenetic mechanism which regulates gene expression, cell energy production, detoxification, and many other functions. Unfortunately, some people may experience methylation health issues which can affect overall health and wellness. Many health professionals may help treat these methylation problems with supplementation, however, research studies have demonstrated that supplementation can sometimes cause methylation to go wrong. Aberrant methylation can cause a variety of diseases, including cancer, autoimmunity, allergy, and down syndrome.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many doctors and functional medicine practitioners may recommend higher doses of methyl donors in several patients, however, further research studies are needed to determine the proper amount of methylation supplementation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Dr. Alex Jimenez Explains Why Methylation Can Go Wrong
Many healthcare professionals have demonstrated several potential concerns associated with folic acid and methyl-folate supplementation. Several risks of folic acid or other folate derivative supplements, including commonly utilized alternatives such as 5-mTHF and folinic acid, have become widely recognized and they aren’t frequently discussed. These health issues are described below.
The increased intake of these supplements can mask a vitamin B12 deficiency. Vitamin B12 deficiencies are normally characterized by megaloblastic anemia, however, when folate levels are too high, cell division will continue to occur within the bone marrow and this will mask the anemia. Unaddressed vitamin B12 deficiencies can cause irreversible neurological damage and cognitive impairment.
Folate or folic acid supplements may also reduce the efficiency of certain anti-folate drugs and/or medications, such as methotrexate, anti-cancer, anti-malarial, and anti-bacterial medicines.
These health issues are generally treated with vitamin B12 supplementation, respectively, and although important, these are not the main focus of the article. However, we will discuss whether or not the side-effects of folic acid supplementation, or aberrant DNA methylation activity, are a result of methylation gone wrong. Epidemiological data suggests an inverse association between folate status and risk of disease. Research studies have demonstrated that excessive methylation factors may be harmful.
Health Issues Caused by Aberrant Methylation
Aberrant methylation caused by folic acid supplementation is not explained by UMFA or DHF. Therefore, healthcare professionals cannot rule out the possibility of excessive or aberrant methylation as a contributing and/or underlying factor for disease.
Immune Dysregulation and Dysfunction
Epigenetics has been demonstrated to play an essential role in the development of allergic diseases. By way of instance, epigenetic alterations, including DNA hyper- and hypomethylation, are associated with childhood IgE-mediated food allergies. Although not all research studies agree with the outcome measures regarding these specific mechanisms of action, there are several findings connecting the intake of methyl donors with the development of disease which prompt potential concerns for further investigation.
Several research studies have associated folic acid intake during pregnancy with an increased risk for developing allergic diseases in offspring. Increased levels of maternal folic acid supplementation, or more than 500 mcg/d as compared to less than 200 mcg/d, have been associated with an 85 percent increased risk for developing allergic eczema. In animals, maternal supplementation with a combination of folic acid, vitamin B12, choline, L-methionine, zinc, and betaine during pregnancy enhanced the development of many symptoms of allergic airway diseases, including airway hyperreactivity and higher concentrations of serum IgE.
Similar maternal supplementation with non-dietary methyl donors, including synthetic folic acid, has been demonstrated to increase offspring susceptibility to developing inflammatory bowel disease. Another research study, not of maternal intake, demonstrated that folic acid intake above 600 mcg/d, from either food and/or supplements, was associated with impaired natural killer cell activity.
Blood Sugar Dysregulation
Maternal folic acid supplementation at 500 mcg/d has also been associated with increased incidence of insulin resistance in children at 6 years of age, an effect apparently exacerbated by low maternal vitamin B12 status, according to research studies.
Prenatal Development Dysfunction
Increased folic acid intake is also associated with embryonic loss, growth delay, and increased risk of ventricular septal heart defects.
Comorbidity and Mortality in Diabetic Adults
In a retrospective research study of approximately 526 diabetic adults, increased levels of RBC folate were associated with an increased risk for developing cardiovascular and cerebrovascular disease. In addition, the ratio for dying within 15 years in those with high RBC folate was 2.10, or 95 percent CI = 1.37 � 3.20, compared with a baseline of those with low RBC folate.
If the association between increased methylation and disease are caused through alterations in methylation activity, the possibility exists that alternative forms of folate supplementation can also change methylation activity in ways that could cause the same risks.
Changes in folate have been demonstrated to affect DNA methylation. Many healthcare professionals turn to folate supplements in under-methylating patients to help �regulate� DNA methylation activity. Unfortunately, research studies regarding the effect of folate and methylation on the DNA �methylome� are conflicting and inconclusive. However, healthcare professionals should not ignore that increasing levels of folate and SAMe methyl donors might increase DNA methylation beyond healthy levels.
According to researchers, if there is too little methylation present, a gene that causes disease may be expressed. Conversely, if there is too much methylation present, a gene that prevents disease may be suppressed. If this is indeed true, we can only assume that when methylation goes wrong, our overall health and wellness can be affected. In part 2 of this article, Dr. Alex Jimenez explains how methylation can go wrong, specifically discussing cancer, autoimmune conditions, immune hypersensitivity and Down Syndrome.
DNA methylation is a fundamental epigenetic mechanism which regulates gene expression, cell energy production, detoxification, and many other functions. Unfortunately, some people may experience methylation health issues which can affect overall health and wellness. Many health professionals may help treat these methylation problems with supplementation, however, research studies have demonstrated that supplementation can sometimes cause methylation to go wrong. Aberrant methylation can cause a variety of health issues, including immune dysregulation and dysfunction, blood sugar dysregulation, and prenatal development dysfunction.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many doctors and functional medicine practitioners may recommend higher doses of methyl donors in several patients, however, further research studies are needed to determine the proper amount of methylation supplementation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Although high-dose methyl donor supplements can help patients with methylation deficits, some healthcare professionals may occasionally encounter patients with an intolerance to methylation donors. Patients with an intolerance to methyl donors can experience worsening symptoms as well as the appearance of neurological symptoms, regardless of their need for methylation support. Neurological symptoms may include, anxiety, depression, irritability, and brain fog, among other symptoms.
Intolerances to methyl donor supplements are not properly understood and further research studies are required to help determine the frequency and effects of these problems. It’s believed that the impaired metabolism of catecholamines through COMT and MAOA may play a role in the intolerance of methylation donors. Increased SAH is also believed to cause a variety of adverse effects.
Case 1.0: Methyl Donor Intolerance with COMT Polymorphism
A 31-year-old female diagnosed with a long-term panic disorder and a recent onset of agoraphobia demonstrated homozygous for COMT and MTHFR single nucleotide polymorphisms, or SNPs, through genetic testing. Vanilmandelic acid, or VMA, and homovanillate, or HVA, urinary organic acids were found to be between low and low-normal, respectively, indicating poor clearance of norepinephrine and epinephrine. These catecholamines are catabolized through COMT methylation, and their poor clearance may increase anxiety symptoms. Her homocysteine levels, on the other hand, were normal which demonstrated that either the MTHFR SNP was still functional enough to maintain SAMe levels, or that increased oxidative stress was confounding the normal homocysteine finding by increasing transsulfuration of homocysteine for glutathione formation.
High-dose methylated folate and betaine supplements were recommended, however, the patient immediately reported experiencing aggravated symptoms. This may have occurred due to the increased production of SAMe from the combined effects of the supplementation. SAMe levels in the brain regulate the rate of epinephrine biosynthesis from norepinephrine through methylation, therefore, increased SAMe availability could have triggered increased epinephrine synthesis. The decreased clearance due to the COMT SNP could have been the underlying cause for the increased symptomatology. Replacing methylated folate with unmethylated folic acid, and the discontinuation of betaine supplements resulted in significant symptom improvement, including the resolution of agoraphobia. Case adapted with permission from Lord & Bralley, 2012, Case Illustration 11.1 p. 594.
Folic Acid Supplement Risks
Furthermore, fortification and standard folic acid supplementation are believed to increase the risks of developing neural tube defects, particularly at levels above 400 mcg/d of dietary folate equivalent units, or DFEs. Folic acid is a purely synthetic compound which must first be converted to tetrahydrofolate, or THF, by being cycled twice through the enzyme dihydrofolate reductase, or DHFR, to be utilized in methylation. One cause of folic acid side-effects include elevated unmetabolized folic acid or UMFA.
Folic acid side-effects and restricted capacity of liver DHFR are believed to be the main problems in folic acid metabolism. One-time folic acid doses of 260 mcg or multiple folic acid doses of 100 mcg throughout the day have been demonstrated to cause detectable UMFA. People who regularly consume fortified foods, such as ready-to-eat cereals and fortified grains, are exposed to folic acid beyond the Tolerable Upper Limit of 1.0 mg/d, and with the utilization of multivitamin supplements, it may increase beyond that.
Folic acid from supplements is also much more easily absorbed than folate from foods. One DFE is equivalent to 1 mcg of dietary folate as compared to 0.6 mcg of folic acid from supplements taken with food or fortified foods. Therefore, 400 mcg of folic acid is equivalent to 667 mcg DFE. Research studies associate higher levels of folic acid intake with other side-effects. Dihydrofolate, or DHF, the intermediate metabolite in the conversion of folic acid to tetrahydrofolate and UMFA, can cause a variety of health issues.
DHF has been demonstrated to prevent thymidylate synthase and purine synthesis enzymes, which can affect DNA synthesis. DHF is also believed to restrict the production of the MTHFR enzyme, which can lead to a decrease in methionine synthesis and homocysteine clearance. A recent research study demonstrated that 5 mg/d of folic acid supplementation in infertile men demonstrated an unexpected reduction in sperm DNA methylation, similar to patients homozygous for the MTHFR C667T polymorphism.
Other research studies have also reported a connection between fortification and standard folic acid supplementation and colorectal cancer. According to the research studies, UMFA may actually metabolize through photo-catalysis into DNA-toxic products. A recent research study which evaluated the connection between UMFA and colorectal cancer diagnosis demonstrated a small positive association in men and individuals with the MTHFR C677T genotype, both heterozygous and homozygous.
However, the research studies demonstrated a small inverse association with women. Higher UMFA was also found to be associated with anemia in US seniors who consumed alcohol and reduced NK cell cytotoxicity in otherwise healthy postmenopausal women. Recent research studies looking at folate receptors in epithelial cancers demonstrated a high frequency of receptor FR-alpha which uptakes UMFA. It is believed that FR-alpha promotes tumor progression and reduces apoptosis through increased expression of anti-apoptotic protein Bcl-2. Folic acid exposure to tumor cells in-vitro was demonstrated to enhance the progress of this process.
Methylation is a biochemical process required for cell division, DNA and RNA synthesis, gene expression, histamine clearance, detoxification, and cellular energy metabolism, among other essential functions. As important as methylation, however, many people are diagnosed with methylation deficits, which can cause a variety of health issues. Healthcare professionals recommend high-dose methyl donors to help treat methylation deficits. But, are we supplementing too much? Some patients may have an intolerance to methylation donors and they may experience side-effects, such as worsening symptoms or neurological symptoms.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many doctors and functional medicine practitioners may recommend higher doses of methyl donors in several patients, however, further research studies are needed to determine the proper amount of methylation supplementation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Sciatica is a collection of symptoms characterized by pain, discomfort, tingling sensations, and numbness, in the low back. The painful symptoms of sciatica can affect a person’s quality of life. Edgar M. Reyes was unable to walk or engage in his regular physical activities, and he was diagnosed with sciatica.
Dr. Jimenez, a doctor of chiropractic in El Paso, TX, has tremendously helped Mr. Reyes find relief from his painful symptoms. He expresses how much Dr. Jimenez has helped him with his sciatic nerve pain, and he highly recommends Dr. Jimenez and his staff as the non-surgical choice for sciatica and low back pain.
El Paso Back Clinic
Professional worker carrying pipes and smiling.
We are blessed to present to you El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend us.
Flexibility is something that many people would like more of, but few know how to achieve it. You might find that improving your flexibility is easier than you think.
This is because flexibility training is often seen as difficult, painful, and time-consuming. It is also significantly underestimated. Why bother getting flexible if you aren�t an athlete or dancer? Why do regular people need to improve their flexibility? The answers to these questions may surprise you.
Why is flexibility important?
Flexibility is a critical component of keeping your body fit and healthy. Research shows that people who are more flexible are better able to reach their optimum fitness level.
It can also help to prevent injury and reduce your risk of conditions like arthritis and other chronic diseases. They also have a better range of motion and mobility as they age.
Muscles that are flexible have the potential to become stronger. This can help increase metabolism and improve fitness level.
A more flexible body can also carry out day to day activities easier and have less chance of injury. Blood flow is increased and circulation is improved which also helps to prevent chronic conditions like kidney disease and diabetes as well as heart disease.
Stretch for upper body flexibility
This upper body stretch also helps improve your posture. It is also great if you are primarily sedentary throughout the day, such as sitting at a desk for extended periods.
Stand or sit in a chair, back straight, chin level, feel slightly apart and knees soft.
Put your hands behind your head, elbows out, chin tucked.
Gently press your head forward to feel the stretch through your neck, shoulders, and upper back; hold for five seconds.
Tilt your head back so that your chin is pointing toward the ceiling.
Place the heels of your hands on your forehead and gently press to get a stretch through the front of the neck and the arms; hold for five seconds.
Bring your head to the start position, chin parallel to the floor, neck straight.
Put your right hand on the top of your head and gently press as if you are trying to touch your right ear to your right shoulder and feel the stretch along the left side of the neck and shoulder; hold for five seconds.
Put your left hand on the top of your head and gently press as if you are trying to touch your left ear to your left shoulder and feel the stretch along the right side of the neck and shoulder; hold for five seconds.
Raise your hands over your head and clasp your hands.
Stretch and lift your body, lengthening your spine.
Release your hands and bend to the right, using your right hand to grasp your left elbow and gently pull it to the right. Hold for five seconds.
Raise your hands over your head and clasp your hands. Stretch and lift your body, lengthening your spine.
Release your hands and bend to the left, using your left hand to grasp your right elbow and gently pull it to the left. Hold for five seconds.
Stretch for lower body flexibility
This is a great stretch for women who wear high heels or for cyclists and people who walk, run, or use an elliptical machine.
Sit on the floor with your legs straight in front of you, feet together, knees soft, and back straight.
Slowly bend your right knee and lean back if necessary, using your right arm as support behind you. Place your left hand under your left knee and flex your toes toward the ceiling, feeling the stretch through your calf. Hold for five seconds.
Stretch both legs out straight in front of you.
Slowly bend your left knee and lean back if necessary, using your left arm as support behind you. Place your right hand under your right knee and flex your toes toward the ceiling, feeling the stretch through your calf. Hold for five seconds.
Roll onto your back with your knees bent toward the ceiling and feet flat on the floor.
Gently bring your right knee to your chest, holding it with your hands to get a nice stretch. Hold for five minutes.
Return to the start position, on your back with your knees bent and feet flat on the floor.
Gently bring your left knee to your chest, holding it with your hands to get a nice stretch. Hold for five minutes.
Return to the start position, on your back with your knees bent and feet flat on the floor.
Stretch for flexibility in the back
This stretch is very good for low back pain.
Lie on your stomach keeping your legs straight, knees soft, and feet shoulder-width apart.
Place your hands under your shoulders, palms down on the floor and push your upper body up so that your back is curved with your lower body still on the floor. Tilt your head back for more stretch. Hold for 10 seconds.
Lower your upper body back to the mat and slowly roll over to your hands and knees.
Keep your knees shoulder width apart and your back straight.
While on your hands and knees, tuck your chin and round out your back, pushing it towards the ceiling, feel the stretch through your entire back. Hold for 10 seconds.
Return to the start position with your knees shoulder width apart and your back straight.
While on your hands and knees, lift your chin, stretching it upwards and drop your back so that your spine curves toward the floor. Hold for 10 seconds.
Return to the start position with your knees shoulder width apart and your back straight.
Folate deficiency and poor folate metabolism are associated with a variety of health issues, such as neural tube defects. Fortunately, the mandatory folic acid programs started by many developed countries over the last two decades have tremendously affected the prevalence of these health issues. The health benefits of utilizing folic acid supplements simply cannot be ignored.
Methylation deficits have also been associated with health issues like ADD/ADHD, allergies, addiction, anxiety, Alzheimer�s Disease, asthma, atherosclerosis, autism spectrum disorder, behavioral changes, bipolar disorder, chronic fatigue, chemical sensitivity, cleft palate, cancers, depression, diabetes, Downs syndrome, dementia, essential hypertension, fertility issues, fibromyalgia, insomnia, multiple sclerosis, neuropathy, Parkinson�s Disease, schizophrenia, and thyroid disease.
Methylation is an essential aspect of physiology. Healthcare professionals recognize that a person may develop methylation deficits in a variety of ways, including through nutrient deficiency, competition for methyl donor utilization, methylation inhibitors, genotype, and aging. Dr. Alex Jimenez, doctor of chiropractic, discusses how specific factors can eventually cause methylation deficits.
Nutrient Deficiency
Reduced levels of methyl donors caused by nutrient deficiency can ultimately affect both metabolic and DNA methylation activity in the human body. Many vital nutrients are involved in the process of methylation, which we will discuss in further detail below. However, the most frequently recognized nutrients which we can commonly be deficient in are folate and vitamin B12.
According to information from the National Health and Nutritional Examination Survey, or NHANES, the average dietary intake of food-fortified folic acid and natural food folates in adults range from 454 to 652 mcg DFE per day, of which 190 mcg/d is estimated to develop from folic acid fortification, compared with a target RDA of 400 mcg/d DFE. These average folate levels may increase the risk of developing nutrient deficiency in several people. These include women of childbearing age and non-Hispanic black women.
People have started to demonstrate low levels of dietary folate intake, ranging from 200-350 mcg/d DFE, when removing sources of fortified foods from their diet, such as gluten-containing grains and processed breakfast cereals. Although healthcare professionals recommend people avoid processed and refined foods, especially to prevent triggering food sensitivities, it’s fundamental to increase natural sources of folate to achieve optimal intake levels and promote overall health and wellness in the population.
The average intake for vitamin B12 is estimated to be at 3.4 mcg/d, higher than the recommended 2.4 mcg/d RDA for a majority of adults. However, healthcare professionals understand that specific population groups are at higher risk of developing methylation deficits associated with nutrient deficiency. As we age, people’s ability to produce the gastric hydrochloric acid and intrinsic factor necessary for vitamin B12 production can decrease. This can then lead to health issues which further limit gastric function.
Many patients that visit a doctor or functional medicine practitioner may also have conditions which can affect nutrient absorption and their functional status, including dysbiosis, small intestine bacterial overgrowth, altered transit time, Crohn�s disease, food allergies or sensitivities, and impaired thyroid function, among other health issues. These should be evaluated by the patient’s nutrient need.
While avoiding processed food-based diets is essential for optimal health and wellness, improperly-implemented whole-food diets can still have the potential to be imbalanced. Therefore, people should include foods that provide all of the necessary nutrients the human body required, including methylation nutrients. People should also check functional nutrient status through laboratory tests.
Competition for Methyl Donors
Methylation activity, such as high catecholamine turnover, histamine clearance, circulating estrogens, or detoxification, can decrease methyl donors. By way of instance, SAMe use for catecholamine biosynthesis and degradation increases during physiological and psychological stress, which can ultimately affect the availability of SAMe. In people who react to antigens, increased histamine activity can affect methyl donor levels.
L-Dopa drugs and/or medications are a common treatment in patients with Parkinson�s disease. L-Dopa metabolism occurs through COMT with SAMe as a cofactor to utilize its methyl group. Its use is associated with reduced plasma folate and elevated homocysteine. L-Dopa may affect the process of methylation which can remove heavy metals and other toxins that can be considered contributors to Parkinson’s disease, among other health issues.
Methylation Inhibitors
S-adenosyl homocysteine, or SAH, is a powerful competitive inhibitor of SAMe-dependent methyltransferases, including DNMT, which generally increases with hyperhomocysteinemia. The conversion of SAH to homocysteine is triggered by S-adenosyl homocysteine hydrolase, which is fully reversible and supports biosynthesis over hydrolysis. Therefore, an increased quantity of homocysteine can restrict the production of hydrolysis and promote the development of SAH, preventing SAMe-dependent methylation activity.
Genotype
Many enzymes and their corresponding genes play a role in methylation. However, many healthcare practitioners also include genotyping when evaluating their patients. Patients can order genetic profiling on their own and they are starting to bring that information to their doctors for evaluation. According to research studies, genotype can affect methylation status.
Frequency and Effects of MTHFR Polymorphisms
The most common MTHFR polymorphisms are C677T and A1298C. Some variations, such as the homozygote 677TT variants, can vary according to ethnicity and geography. Approximately 20 percent of these variations are reported in US Hispanics, Colombians and Amerindians in Brazil. While approximately 8 to 20 percent of these variations are reported in White populations in Europe, North America, and Australia. Approximately less than 2 percent of these variations are found in Black populations.
Meanwhile, the homozygote 1298CC variants can also vary according to ethnicity and geography. Approximately 7 to 12 percent of these variations are reported in White populations in North America and Europe. Approximately 4 to 5 percent of these variations are reported in Hispanics and approximately 1 to 4 percent of these variations are reported in Asians. Additional information is still required as to the dispersion of heterozygote genotypes, as well as that of compound genotypes, among population groups.
Moreover, variations in C667T polymorphisms may also be increasing. Research studies from Spain, by way of instance, demonstrated an increase of the C677T genotype in the post-folic acid-fortification era. Homozygous 667TT variants can have a 70 to 75 percent decrease in enzyme activity. Heterozygotes decrease 33 to 35 percent of enzyme activity. Homozygous 1298CC genotypes have a 39 percent decrease in enzyme activity, and heterozygotes have a 17 percent decrease in enzyme activity. Heterozygotes for both 667CT and 1298AC may also experience as much as a 52 percent decrease in enzyme activity, according to research studies.
Research studies have ultimately demonstrated that this change in enzyme activity can affect folate and homocysteine levels. A recent systematic review and meta-analysis reported a 16 percent decrease in erythrocyte folate levels for homozygous 677TT genotypes when compared with their wildtype 677CC counterparts and an 8 percent decrease for heterozygous 677CT genotypes. Red blood cell folate measurements include all the different folate vitamers, so we cannot exclude 5-mTHF, needed for homocysteine metabolism.
Aging
Aging can also affect DNA methylation, including global hypomethylation, with hypermethylation in normally unmethylated CpG areas, which may cause genomic instability. Maintaining proper methylation status through nutritional and lifestyle modifications are considered to be safe and effective, alternative treatment options that can help slow down the age-related decline in methylation.
DNA methylation is an epigenetic process which occurs when a methyl group triggers the function of genes and enzymes in DNA, ultimately impacting gene expression. Methyl groups can be directly delivered through dietary methyl donors, such as methionine, folate, betaine, and choline. However, low levels of methyl groups as well as methyl donors due to a variety of factors can cause methylation deficits. In this article, we discuss the causes for methylation deficits where we also provide smoothies and juices which can help promote methylation support.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications, there are several alternative treatment options you can try for yourself at home. As described above, however, supplementation for methylation support should be correctly determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support in a single serving. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many doctors and functional medicine practitioners may recommend higher doses of methyl donors in several patients, however, further research studies are needed to determine the proper amount of methylation supplementation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine