When it comes to chiropractic care, we believe in it, we�ve seen how great it works, and there are plenty of happy patients that can testify to its effectiveness.
However, there are some nay-sayers who believe that medical treatments are the only way to treat health care concerns and health conditions. While we do believe that medical treatments do indeed have their place, we also know for a fact that chiropractic offers far more benefits, provides faster results for many conditions including pain management, and provides farther reaching care that goes to the heart of the problem instead of just treating the symptoms.
If you�ve chosen to incorporate chiropractic care into your health plan, you�ve made a very wise decision. There are many benefits that chiropractic patients enjoy that those who choose a more medical-centric way do not. Here are three great advantages that chiropractic care will provide � and they�re big ones.
1. Chiropractic treats the root of the problem.
Modern medicine certainly has its place. It has helped many people. However, it tends to be rather short-sighted when dealing with many conditions.
Chiropractic, on the other hand, seeks to find the root of the problem, to address the reason the patient is having the problem and correct it.
For instance, if a patient came in with back pain, a medical doctor may prescribe painkillers and invasive treatments. Their goal is to stop the pain.
However, a chiropractor will try to find out why the patient�s back is hurting and address the cause while treating the pain without medications or invasive procedures.
2. Chiropractic is completely natural and noninvasive.
Chiropractic is entirely natural, using spinal adjustments and other techniques, combined with nutritional advice, lifestyle recommendations, and all-natural supplements.
�The others� are more reliant on medications that are often largely synthetic and have unpleasant, even dangerous side effects. Some medications are even addictive. Surgeries and other invasive procedures can leave you with difficulty in mobility and limited range of motion as you heal.
When you visit a chiropractor for your back pain, he or she will not only adjust your spine, they will also talk to you about your daily activities, habits, even how you sleep. They will make recommendations about things you can do to prevent the pain and strengthen your back. It may mean making some changes or doing some special exercises, but your treatment will be tailored specifically to you and your needs.
3. Chiropractic treats the body as a whole.
Medical treatments tend to treat what�s hurting right now but rarely look beyond that to see how the whole body is affected. What�s more, they don�t tend to look at what is causing the problem, treating the body in parts.
This is unnatural and not the best way to combat pain and many health conditions. It may work for a while, but eventually, issues in the body will manifest in other areas as well.
For instance, a problem with the hip may manifest as knee pain. The doctor treats the knee but does not address the hip (which is the cause of the problem). Eventually, the hip worsens, and the back, knee, and ankle become affected. The hips and other joints on the other side may also become affected as the body tries to compensate.
Chiropractic treats the body as a whole, not as parts. It finds the cause of the problem and addresses that while also treating the part that is in pain.
Chiropractic also looks at lifestyle, diet, habits, even relationships so see where you could have stressors or things that could be posing a risk to your health, making your condition worse or more difficult to treat.
*Auto Accident Injury* Treatment | El Paso, TX (2019)
Mr. Fred Foreman is a club basketball coach in El Paso, TX. When he first started the 6 Day Detox Kit,�Mr. Foreman had to change his diet and lifestyle habits.
Mr. Foreman discusses his experience with the 6 Day Detox Kit with Dr. Jimenez and expresses how much the nutritional program has helped improve his energy and performance, and overall health. Mr. Foreman recommends this kit to anyone that’s ready for a healthy change.
The sciatic nerve is the largest nerve in the human body and its main function is to connect the feet to the CNS. The painful symptoms associated with sciatic nerve pain, or sciatica, can tremendously affect a person’s quality of life.
Sciatica, or sciatic nerve pain, is caused by the compression of the sciatic nerve, which runs from the low back, down each leg, and into the feet.
Dr. Alex Jimenez focuses on the diagnosis, treatment, and prevention of a variety of health issues associated with the musculoskeletal and nervous systems.
Chiropractic care is an alternative option that utilizes spinal adjustments and manual manipulations to safely and effectively correct any spinal misalignments, or subluxations, which may be causing painful symptoms like sciatic nerve pain or sciatica. Dr. Jimenez is the non-surgical choice.
El Paso Back Clinic
We are blessed to present to you El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend us.
Dr. Alex Jimenez Discusses the Basics of Methylation Status and Activity
Methylation is the process of producing and/or developing a “one-carbon metabolism” from methyl, or CH3, groups. The main methyl donor group utilized for DNA methylation activity is known as s-adenosyl-L-methionine, or SAMe. Other methylation donors, such as MTHFR, COMT, and DNMT, will also use SAMe as their co-factor when regulating DNA methylation status.
According to healthcare professionals, DNA methylation occurs numerous times per second and it is in charge of a variety of bodily functions. Because methylation happens continuously throughout the human body, our overall health and wellness can determine whether we will be involved in healthy methylation activity or some sort of compromised methylation status.
Contents
DNA Methylation in the Human Body
DNA methylation is involved in a variety of fundamental processes throughout the body, such as cell division or DNA and RNA synthesis, early CNS development to address neural tube defects, epigenetic regulation of gene expression, immune cell differentiation, neurotransmitter biosynthesis and metabolism, such as that of dopamine, norepinephrine, epinephrine, and acetylcholine, histamine clearance, detoxification and hormone biotransformation, cellular energy metabolism, phospholipid synthesis, and myelination of peripheral nerves, among other processes.
The biochemical pathway chart above demonstrates the metabolism of methylation donors as well as their basic function, including that of MTHFR. Several methyl donors are also demonstrated to interchange reversibly while several methyl donors are only demonstrated to transfer into one-way pathways. Insufficient co-factors or vitamins and minerals associated with these can cause imbalances and deficiencies when regulating DNA methylation status. The methylation cycle works together methylation donors to recycle homocysteine into the by-product of that process. The compounds, such as the nutrients, minerals, and enzymes involved in this reaction also shown in the biochemical pathway above.
Basics of Methylation Status & Activity
Methylation can be affected by genetic as well as external and environmental factors. Our extended exposure to these otherwise harmful factors can even alter an individual’s epigenome. DNA methylation occurs at CpG regions through the utilization of DNMT enzymes associated with gene repression to become five different methylation groups.
A variety of DNMT’s are in charge of maintaining and regulating DNA methylation status and activity. DNMT1 is in change of controlling DNA methylation patterns. DNMT3A and DNMT3B are in charge of producing new methylation triggers and they’re also involved in genomic imprinting during embryonic development. Methylation begins to occur during the early perinatal period, where we inherit our parent’s methylation marks.
Understanding how DNA methylation status is influenced by our health and wellness is fundamental to promote methylation support. The utilization of supplements and/or medicine can help improve DNA methylation, however, there may be a risk of side-effects. Nutrition and lifestyle modifications are safe and effective options to help improve overall DNA methylation.
Promoting methylation support is an essential process towards maintaining overall health and wellness. DNA methylation is involved in a variety of bodily functions. Maintaining and regulating healthy methylation can help prevent a variety of health issues, as we will discuss in the next series of articles. The purpose of the following article is to introduce the basics of DNA methylation. It’s fundamental to understand how nutrition, lifestyle habits, supplements and even medicines, can improve DNA methylation as well as to promote overall health and wellness.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.Sea Green Smoothie
Servings: 1
Cook time: 5-10 minutes
� 1/2 cup cantaloupe, cubed
� 1/2 banana
� 1 handful of kale or spinach
� 1 handful of Swiss chard
� 1/4 avocado
� 2 teaspoons spirulina powder
� 1 cup water
� 3 or more ice cubes
Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie
Servings: 1
Cook time: 5-10 minutes
� 1/2 cup blueberries (fresh or frozen, preferably wild)
� 1 medium carrot, roughly chopped
� 1 tablespoon ground flaxseed or chia seed
� 1 tablespoons almonds
� Water (to desired consistency)
� Ice cubes (optional, may omit if using frozen blueberries)
Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice
Servings: 1
Cook time: 5-10 minutes
� 1 cup honeydew melons
� 3 cups spinach, rinsed
� 3 cups Swiss chard, rinsed
� 1 bunch cilantro (leaves and stems), rinsed
� 1-inch knob of ginger, rinsed, peeled and chopped
� 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped
Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice
Servings: 1
Cook time: 5-10 minutes
� 1 cup pineapple cubes
� 1 apple, sliced
� 1-inch knob of ginger, rinsed, peeled and chopped
� 3 cups kale, rinsed and roughly chopped or ripped
� 5 cups Swiss chard, rinsed and roughly chopped or ripped
Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice
Servings: 1
Cook time: 5-10 minutes
� 1 grapefruit, peeled and sliced
� 1 apple, washed and sliced
� 1 whole beet, and leaves if you have them, washed and sliced
� 1-inch knob of ginger, rinsed, peeled and chopped
Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie
Serving: 1
Cook time: 5 minutes
� 1 scoop protein powder
� 1 tablespoon ground flaxseed
� 1/2 banana
� 1 kiwi, peeled
� 1/2 teaspoon cinnamon
� Pinch of cardamom
� Non-dairy milk or water, enough to achieve desired consistency
Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many doctors and functional medicine practitioners can recommend nutritional advice and/or guidelines to help improve DNA methylation. Proper nutrition and lifestyle habits can ultimately help improve DNA methylation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download* All the above XYMOGEN policies remain strictly in force.
***
Our military members put their bodies through tremendous stress every day. Add to that minor to serious trauma and there is a strong case for chronic pain. This pain affects our veterans and soldiers on a daily basis, and interferes with their normal activities and impacts their ability to perform their regular jobs.
Too often, doctors dismiss the pain as �something you just have to live with� and write prescriptions for narcotics that impair and incapacitate the patient. There are better ways to manage a good bit of the chronic pain that members of the military live with each day. We’ll explore one way, mainly chiropractic, in today’s article.
Contents
Chronic Pain & Military Members
The regular demands of being a soldier, coupled with the stress that is prevalent, particularly among active duty military personnel, can create a perfect storm of sorts for chronic pain. When they are advised to tough it out or arrive at that option on their own, they usually do not get the medical attention they need. This can lead to exacerbation of the issue, compelling the soldier to seek treatment only when the pain is severe, or the condition is serious.
Single event trauma is all too common in this arena and plays a large part in the pain they experience, as does surgeries to correct injuries or trauma. However, the cumulative stress can have a detrimental effect on not just the condition and the pain, but the patient�s perception of the pain. In other words, it can cause them to experience the pain more acutely and have greater difficulty in managing it.
These issues are a part of the military and they aren�t likely to change. A chiropractor can help military personnel manage their pain, prevent injury, and regain flexibility and range of motion. It can be a solution that makes all the difference.
Alternative Treatments To Combat An Epidemic
Right now in the United States, opioid abuse has become an epidemic, yet doctors can rarely find viable alternatives that don�t have the dangerous and uncomfortable side effects � and that are not addictive. In truth, painkiller use is a growing problem with veterans and active military alike, mainly due to issues with substance abuse.
While their medications do relieve pain, the cost is just too great in many cases. Many people who take these pain pills report that they would live from pill to pill, their lives revolving around their next dose. That is why chiropractic is such an attractive option.
Chiropractic For PTSD
Post-traumatic stress disorder (PTSD) is a common condition among active military and veterans. Studies have found that complementary and alternative medicine (CAM) is very effective in treating PTSD.
Matter of fact, chiropractic care has received very high marks in this area. Typically, it involves combining chiropractic with some conventional approaches in an effort to bring relief to the patient.
Through specific spinal manipulations called vestibular rehabilitation treatment (VRT), the body is brought back into balance. This technique has been proven very effective among individuals who have brain injuries that are combat related. In one study, patients who received VRT for two weeks reported a significant decrease in PTSD symptoms, including depression and anxiety.
An Army report recommended the use of alternatives to pain drugs, including chiropractic care, massage, and acupuncture.
Chronic Pain & Chiropractic Care
Chiropractic care is a highly effective way to manage chronic pain and help speed healing from injuries. It is safe, non-invasive, and does not require any medication.
The chiropractor will use specific spinal adjustments and other techniques to bring the body back into alignment. A balanced body heals faster and experiences less pain.
The patient may also receive recommendations regarding lifestyle changes and dietary advice from their chiropractor which can help speed up the results and bring them to a place of less pain or no pain much faster.
Nutrition is a safe and effective way to promote methylation support without the side-effects of supplements and/or that of medicines. However, the foods you choose to eat can also tremendously affect your DNA methylation. The food quality and food packaging as well as how you make these dietary changes can determine your methylation status and activity. We will discuss these factors and their effects in detail below.
Contents
Food Quality
The quality of the foods you choose is fundamental to improve DNA methylation. Choosing high-quality foods, by way of instance, means choosing foods which contain an increased nutrient density, which is abundant in phytonutrients and antioxidants, and contains decreased amounts of toxins, such as pesticides, herbicides, fungicides, and heavy metals. Make sure to look for the terms below when purchasing foods:
Local-grown. Food which has not had to travel considerable distances before being sold generally has a much higher nutrient density.
Non-GMO. Genetically modified organisms, or GMOs, is a term which currently applies to a variety of foods, including commodity grains, such as soy, wheat, and corn. GMO crops are often preferred by some farmers due to their resistance to herbicides. As a result, GMO crops tend to have increased levels of herbicide toxins and/or foreign compounds which can cause cellular damage and other health issues.
Organic. Organic foods contain fewer pesticides, synthetic hormones, and are always non-GMO. The utilization of sewage water is prohibited for organically-grown crops, which tremendously reduces heavy metal health issues. Several organic food farmers also evaluate their soil and food products for heavy metal contamination.
Grass-fed/Pasture-raised. This term applies to graze animals, which are grain-fed in conventional commercial farming operations. Grass-fed/pasture-raised animals have better nutrient profiles, less pro-inflammatory fats, more anti-inflammatory fats, and less risk of heavy metal contamination due to other conventional animal feeds.
Wild caught. Fish which are wild caught also have better nutrient profiles. Generally, there are fewer toxins in wild-caught fish, however, make sure you�re choosing fish from clean waters or which has been evaluated for contaminants. The National Resources Defense Council has a good guide to sustainable and low-mercury seafood.
Cold pressed, unrefined, extra-virgin. These terms are currently applied to oils which are minimally processed and contain the highest amounts of phytonutrients. Avoiding these will prevent you from choosing oils which have been chemically processed with hexane, a solvent which can be found in highly- processed commercial oils.
Food Packaging
The food packaging you choose is also fundamental to improve DNA methylation because these can be a considerable source of toxins, which can also ultimately affect your overall health and wellness. Several simple lifestyle modifications can considerably reduce exposure to these toxins:
Minimize the utilization of plastic food and beverage containers. Preferred choices for containers include glass and stainless steel.
Never reheat food in plastic containers.
Minimize the utilization of canned food choices.
Avoid nonstick cookware. Preferred choices for containers include stainless steel, glass, and cast iron cookware.
Making Dietary Changes
The dietary changes you make can ultimately be fundamental to improve DNA methylation, although it can often be a difficult and sometimes overwhelming process. The key to making these dietary and lifestyle changes as easy and stress-free as possible is described below, including:
Utilizing leftovers for the next day�s meal or part of a meal, such as using leftover cooked salmon and broccoli from dinner as part of a large salad for lunch or for a snack the following day.
Cook extra food, such as chicken, green beans, saute?ed greens, and roasted mushrooms, which can be reheated for another meal.
Many foods freeze well and can be frozen in individual portions to easily combine, take “on the go”, or simply to save for another day.
Try to plan ahead so that you’re not caught in a situation where the only food available doesn’t fit your food plan. Keep suitable snacks on hand and bring meals with you to follow your regimen.
You may find it useful to invest in portable food containers which keep food cold/hot; choose stainless steel or glass containers.
If eating out, call restaurants ahead of time to discuss suitable menu choices. You�ll probably find that restaurants which cook foods from scratch with fresh/local ingredients are most suitable for you.
As previously discussed, improving DNA methylation is a fundamental process towards maintaining overall health and wellness. A balanced nutrition can help safely and effectively improve methylation support, however, choosing foods can also promote methylation support. The purpose of the following article is to easily demonstrate what foods to choose to improve DNA methylation. It’s fundamental to understand how the foods you choose can improve DNA methylation as well as to promote overall health and wellness.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.Sea Green Smoothie
Servings: 1
Cook time: 5-10 minutes
� 1/2 cup cantaloupe, cubed
� 1/2 banana
� 1 handful of kale or spinach
� 1 handful of Swiss chard
� 1/4 avocado
� 2 teaspoons spirulina powder
� 1 cup water
� 3 or more ice cubes
Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie
Servings: 1
Cook time: 5-10 minutes
� 1/2 cup blueberries (fresh or frozen, preferably wild)
� 1 medium carrot, roughly chopped
� 1 tablespoon ground flaxseed or chia seed
� 1 tablespoons almonds
� Water (to desired consistency)
� Ice cubes (optional, may omit if using frozen blueberries)
Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice
Servings: 1
Cook time: 5-10 minutes
� 1 cup honeydew melons
� 3 cups spinach, rinsed
� 3 cups Swiss chard, rinsed
� 1 bunch cilantro (leaves and stems), rinsed
� 1-inch knob of ginger, rinsed, peeled and chopped
� 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped
Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice
Servings: 1
Cook time: 5-10 minutes
� 1 cup pineapple cubes
� 1 apple, sliced
� 1-inch knob of ginger, rinsed, peeled and chopped
� 3 cups kale, rinsed and roughly chopped or ripped
� 5 cups Swiss chard, rinsed and roughly chopped or ripped
Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice
Servings: 1
Cook time: 5-10 minutes
� 1 grapefruit, peeled and sliced
� 1 apple, washed and sliced
� 1 whole beet, and leaves if you have them, washed and sliced
� 1-inch knob of ginger, rinsed, peeled and chopped
Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie
Serving: 1
Cook time: 5 minutes
� 1 scoop protein powder
� 1 tablespoon ground flaxseed
� 1/2 banana
� 1 kiwi, peeled
� 1/2 teaspoon cinnamon
� Pinch of cardamom
� Non-dairy milk or water, enough to achieve desired consistency
Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many doctors and functional medicine practitioners can recommend nutritional advice and/or guidelines to help improve DNA methylation. Proper nutrition and lifestyle habits can ultimately help improve DNA methylation. Understanding the role of methylation adaptogens can help promote methylation support. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download* All the above XYMOGEN policies remain strictly in force.
***
Dr. Alex Jimenez Discusses What Not to Eat to Improve DNA Methylation
Methylation is an important process which promotes a variety of bodily functions, including the production and regulation of hormones and neurotransmitters, the development of immune cells, and the management of the detoxification of exogenous substances as well as the clearance of histamine, among other essential processes. DNA methylation is also fundamental for cellular renewal to ultimately alter genetic expression.
By modifying your nutrition and lifestyle habits you can optimize your overall health and wellness. You can also improve this essential process by eating a variety of healthy foods. We’ve previously discussed what foods to eat to improve DNA methylation, in this article, we will discuss what foods not to eat to improve DNA methylation. Just like healthy foods can promote methylation support, unhealthy foods can tremendously affect methylation.
Contents
What Not to Eat for Methylation Support
The following article focuses on what not to eat to promote methylation support. Below, we will demonstrate what not to eat to improve DNA methylation including charred foods, added sugars, artificial sweeteners, hydrogenated fats, alcohol, and folic acid fortified foods. Our ultimate goal is to help you achieve optimal methylation support. By improving your DNA methylation, you can ultimately achieve overall health and wellness.
Charred Foods
Cooking at high temperatures to create a “seared” or “chargrilled” effect causes a chemical reaction known as the Maillard reaction. This process develops compounds, also known as heterocyclic amines, which have been considered to be pro-inflammatory, pro-oxidant, and damaging to cells.
Instead of eating charred foods, try eating slow-cooked or braised foods, where temperatures are lower and moisture is utilized throughout the cooking process. If you do eat grilled foods occasionally, utilizing marinades which contain garlic, rosemary, fruit pulp and other spices without sugar, can help prevent the development of harmful heterocyclic amines.
Added Sugars
Added sugars can tremendously affect our molecules, enzymes, and cellular structures. Eating too much sugar has been associated with almost all of the most common health issues, including heart disease, diabetes, Alzheimer�s disease, and cancer. Excess sugar consumption causes the human body to produce fat; where the excess sugar is then converted into triglycerides, or fat storage molecules, in the liver, which can cause fatty liver and an accumulation of fat deposits in various regions of the human body.
Added sugars can be hidden in a variety of foods. Even supplements, drugs and/or medications, can be sources of excess sugars. Reading the labels for nutrition facts in foods is a good way to start recognizing unwanted sources of sugars. Also, avoid eating high-sugar foods, such as fruit juices, carbonated beverages, confectionery, ice creams, and sweetened yogurts. Make sure to check condiments for hidden sugars. Choosing unprocessed, whole foods is the easiest way to avoid eating hidden added sugars.
Artificial Sweeteners
Artificial sweeteners are also not recommended if you want to improve your DNA methylation. Artificial sweeteners have been demonstrated to cause a physiological response where insulin develops and brain-reward signaling pathways are triggered. This can cause blood sugar imbalances and cravings. Both of these factors make it difficult to eat healthy foods.
Moreover, artificial sweeteners have been demonstrated to affect the brain and the nervous system. While artificial sweeteners require further research studies to determine their negative effects, caution is advised.
Artificial sweeteners which can help improve DNA methylation are stevia and the sugar alcohols erythritol and xylitol. It�s recommended to use these artificial sweeteners while you are weaning yourself off a high-sugar diet. Once you�ve limited sugar in your diet, you�ll find that your taste buds will naturally adapt to the sweetness in whole foods and even vegetables
Hydrogenated Fats
Hydrogenated fats are frequently produced when liquid oils are converted into solid fats. This process changes the molecular structure of the fat into one which is pro-inflammatory and harmful to cells. In the United States, the FDA has already ordered the removal of hydrogenated fats from the supply chain, however, the changes may take effect over a period of years.
To avoid choosing hydrogenated fats, be aware of any solid fats produced from oils which would normally be in a liquid state. On food labels, avoid the terms “hydrogenated” or “partially hydrogenated”, and look for labels that say “trans-fat free”. Utilizing minimally processed oils and butter, or ghee, and avoiding processed foods, is an easy way to avoid trans fats.
Alcohol
Alcohol can interfere with DNA methylation, negatively affecting our gene expression. For this reason, alcohol is not recommended if you want to improve your DNA methylation. If you do consume alcohol, make sure to keep it to a minimum. This means that both men and women should have no more than 1 to 2 alcoholic drinks per week. One alcoholic drink is approximately equivalent to 5 oz of wine, 12 oz of beer, or 1.5 oz of spirits.
Furthermore, it’s important to note that alcoholic beverages do not carry a food label, as other foods and drinks are required to do. Alcohol is not subject to the same regulations as other foods, therefore, it is much more difficult to determine whether one alcohol has higher sugar content than another. Grapes grown for wine are also frequently sprayed with pesticides; choosing organic varieties can ultimately help reduce your exposure.
Folic Acid Fortified Foods
Many grains are fortified with vitamins like folic acid or the synthetic form of folate. However, research studies have demonstrated that folic acid can restrict MTHFR activity and cause a variety of health issues. We recommend avoiding folic acid fortified foods and instead include sources of natural dietary folates, such as dark leafy greens, liver, and legumes, to help improve DNA methylation as well as overall health and wellness.
DNA methylation is a fundamental process in charge of a variety of essential bodily functions. A balanced nutrition can help safely and effectively improve methylation support, however, certain foods can also affect DNA methylation. The purpose of the following article is to easily demonstrate what not to eat to improve DNA methylation from a variety of different food groups. It’s essential to know what food groups to avoid to promote methylation support as well as to promote overall health and wellness. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many doctors and functional medicine practitioners can recommend nutritional advice and/or guidelines to help improve DNA methylation. Proper nutrition and lifestyle habits can ultimately help improve DNA methylation. Understanding the role of methylation adaptogens can help promote methylation support. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download* All the above XYMOGEN policies remain strictly in force.
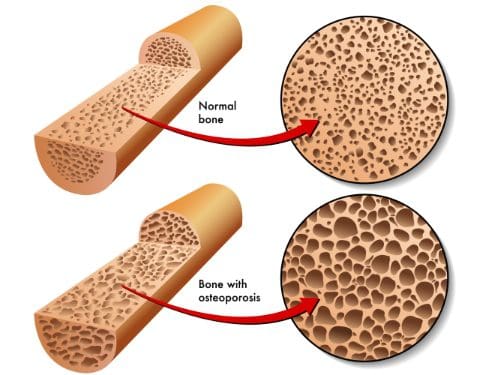
Osteopenia and osteoporosis, two very similar conditions, that are defined as decreased bone density, but osteopenia is far less. However, it is still a problem due to an increase of breaking a bone because of bone fragility.
Contents
Symptoms
Osteopenia usually doesn’t cause symptoms unless a bone is broken. However, some patients who present with osteopenia complain of dull back pain.
Symptoms associated with osteoporosis include the following:
Back pain, caused by a fractured or collapsed vertebra
Loss of height over time
A stooped posture
A bone fracture that occurs much more easily than expected
The causes and those at risk?
Women (primarily small-boned Caucasian and Asian) are most at risk for both conditions, primarily those who are age 65 or older as well as women who are postmenopausal. However, men can also be affected.
Anyone who meets any of the criteria for being at risk for either of the bone conditions should be evaluated. Often, catching the conditions early can make a significant difference in the effects that they have on the body and in some cases, can even be arrested so that they don�t progress.
Some of the common causes of both conditions include:
Lifestyle habits
Smoking
Insufficient calcium
Sedentary lifestyle
Excessive alcohol consumption
Vitamin D deficiency
Carbonated beverages
Medical Situations
Bulimia, anorexia, and other eating disorders
Estrogen deficiency in women
Certain hormone imbalances
Overactive thyroid
Certain treatments including radiation and chemotherapy
Low testosterone in men
Medications including anti-seizure, hydrocortisone, and steroids
Health issues
Tumors
Cystic fibrosis
Crohn�s disease
Digestive issues
It should also be noted that certain types of diets, particularly those that advocate extremely low fat, or no fat can also cause problems. Vitamin D is necessary for calcium absorption in the body, but vitamin D is a fat-soluble vitamin meaning the body requires some fat in order to make use of it. When there is inadequate fat, the vitamin cannot be absorbed and in turn, calcium cannot be absorbed.
A family history of osteopenia, osteoporosis, or low bone mass can increase a person risk by 50% to 85%.
A Diagnosis
Bone mineral density (BMD) tests are used to diagnose both osteopenia and osteoporosis by measuring the calcium levels in bone. This type of test can also provide an estimate of how much at risk a person is for bone fractures.
This test is painless and non-invasive. It is usually performed on the heel, shin bone, wrist, spine, finger, or hip.
Two common types of these tests are radiographs, a standard diagnostic tool for osteopenia, and Dual Energy X-ray Absorptiometry (DEXA). A DEXA scan is essentially a low energy x-ray so patients are not exposed to as much radiation as they would be if they had a regular x-ray. The results are attained by comparing the score (measurements were taken) to scans of individuals who do not have the condition.
Once the score is measured and compared, it is assessed using a chart that identifies the level or risk:
+1.0 to -1.0 – Normal bone density
-1.0 to -2.5 – Low bone density
-2.5 or higher – At risk for osteoporosis
What Treatments Is Available?
As with most conditions, prevention is the most effective treatment. If you have a family history or fall under any of the risk factors, there are things you can do to minimize the effects or prevent the conditions completely.
Your chiropractor can talk to you about lifestyle changes, exercise, and diet as well as supplements that you can take. Chiropractic adjustments can also be effective for many patients with osteopenia and osteoporosis as long as the chosen technique is a low force technique like Activator.
Many patients find these natural treatments preferable to any medications that may be prescribed. The most important thing you should do, though, is get a bone density test if you are in an at-risk category, are a woman who is postmenopausal or age 65 or older.
Dr. Alex Jimenez Discusses the Role of Methylation Adaptogens
When we support DNA methylation in the human body with high-dose supplements, such as folate and vitamin B12, essential nutrients in the production of methyl donor compounds, we are doing a lot to prevent methylation deficiencies. However, healthcare professionals suggest that we are not promoting methylation support by utilizing this approach.
Research studies evaluating the epigenome have demonstrated that both the increase and decrease of DNA methylation can cause health issues. DNA methylation imbalances can occur in different regions of the same gene. One area of the genome might be hypermethylated and turned off while another area of the genome might be hypomethylated and turned on.
Methylation imbalances in cancer cause tumor suppressor genes to become hypermethylated and turn off, allowing the tumor to continue to grow. Moreover, cancer-promoting oncogenes may also become hypomethylated and turn on, also allowing cancer to expand. A variety of methylation imbalances may be associated with several health issues. Even aging and especially accelerated aging can ultimately cause aberrant methylation.
What are Methylation Adaptogens?
Epigenetic methylation imbalances can occur due to numerous factors beyond the methylation cycle as well as vitamin B12 and folate intake. Other factors which can also affect DNA methylation include; toxin exposures, our microbiome and mitochondrial health, stress, lifestyle habits like exercise and physical activity as well as our diet and nutrition.
Improving your nutrition, diet, and lifestyle habits, with the goal of promoting methylation support, is a fundamental piece of maintaining overall health and wellness. It is also a safe and effective, alternative treatment option for methylation support. Research studies have demonstrated that specific foods appear to act as methylation adaptogens.
The term adaptogen, most commonly utilized in botanical medicine, refers to a plant-based chemical or substance which controls the biochemical pathways. Adrenal adaptogens, by way of instance, are also frequently used for stress and can support both underactive as well as overactive adrenal activity. Adaptogens are like a thermostat: when temperatures rise above the desired level, the thermostat turns off to drop temperatures. When temperatures drop below the desired level, the thermostat turns on to raise temperatures. Adaptogens are both gentle and powerfully effective.
Several natural compounds can also act as adaptogens in DNA methylation by both maintaining proper methylation status and regulating improper methylation activity. Furthermore, methylation adaptogens can help prevent abnormal DNA methylation which can cause a variety of health issues. Methylation is essential for our overall health and wellness.
Several methylation adaptogens include; anthocyanins, apigenin, betanin, biochanin A, caffeic acid, chlorogenic acid, coumaric acid, curcumin, daidzein, ellagic acid, EGCG, genistein, lycopene, myricetin, naringenin, quercetin, rosmarinic acid, and sulforaphane. These are plant compounds, known as bioactive phytonutrients, which are found directly in the foods we eat or should be eating. A diet which is rich in varied and colorful plant foods can supply the human body with plenty of these amazing molecules.
The following list of foods has been demonstrated to contain high amounts of methylation adaptogens. Include at least two servings of these every day for general methylation support, and more if you are taking a high dose methyl-donor supplement with folate/folic acid and vitamin B12. The foods below can help promote methylation support, including but not limited to:
Cruciferous vegetables (broccoli, cabbage, cauliflower, Brussels sprouts, bok choy, arugula, horseradish, kale, kohlrabi, watercress, rutabaga, radish, and turnip)
Berries
Ghee
Turmeric
Shiitake Mushrooms
Soy (fermented, traditional versions)
Rosemary
Green tea
Oolong tea
DNA methylation imbalances can cause a variety of health issues. Promoting methylation support with nutrition, lifestyle habits, and supplements is fundamental, however, understanding how these factors can help control DNA methylation is essential towards overall health and wellness. Many foods can provide what is known as methylation adaptogens. These can help safely and effectively promote methylation support, alongside exercise and physical activities, without experiencing the side-effects of supplementation.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many doctors and functional medicine practitioners can recommend nutritional advice and/or guidelines to help improve DNA methylation. Proper nutrition and lifestyle habits can ultimately help improve DNA methylation. Understanding the role of methylation adaptogens can help promote methylation support. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
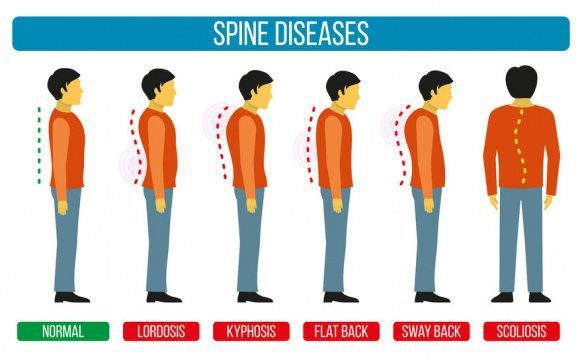
Sometimes there are abnormalities of the spine and it causes a misalignment of the natural curvatures or some curvatures may be exaggerated. These unnatural curvatures of the spine are characterized by three health conditions called lordosis, kyphosis, and scoliosis.
It is not intended to be naturally bent, twisted, or curved. The natural state of a healthy spine is somewhat straight with slight curves running front to back so that a side view would reveal them.
Viewing the spine from the back, you should see something completely different � a spine that runs straight down, top to bottom with no side to side curves. This doesn�t always happen though.
The spine is comprised of vertebrae, small bones that are stacked on top of each other with impact cushioning discs between each one. These bones act as joints, allowing the spine to bend and twist in a variety of ways.
They gently curve, sloping slightly inward at the small of the back, and again slightly at the neck. The pull of gravity, combined with body movement, can put a great deal of stress on the spine and these slight curves help absorb some of the impact.
Contents
Different conditions for different types of spinal curvatures
Each of these three spinal curvature disorders affects a certain area of the spine in a very specific way.
Hyper or Hypo Lordosis � This spinal curvature disorder affects the lower back, causing the spine to curve inwards or outwards significantly.
Hyper or Hypo Kyphosis � This spinal curvature disorder affects the upper back, causing the spine to bow, resulting in that area rounding or flattening abnormally.
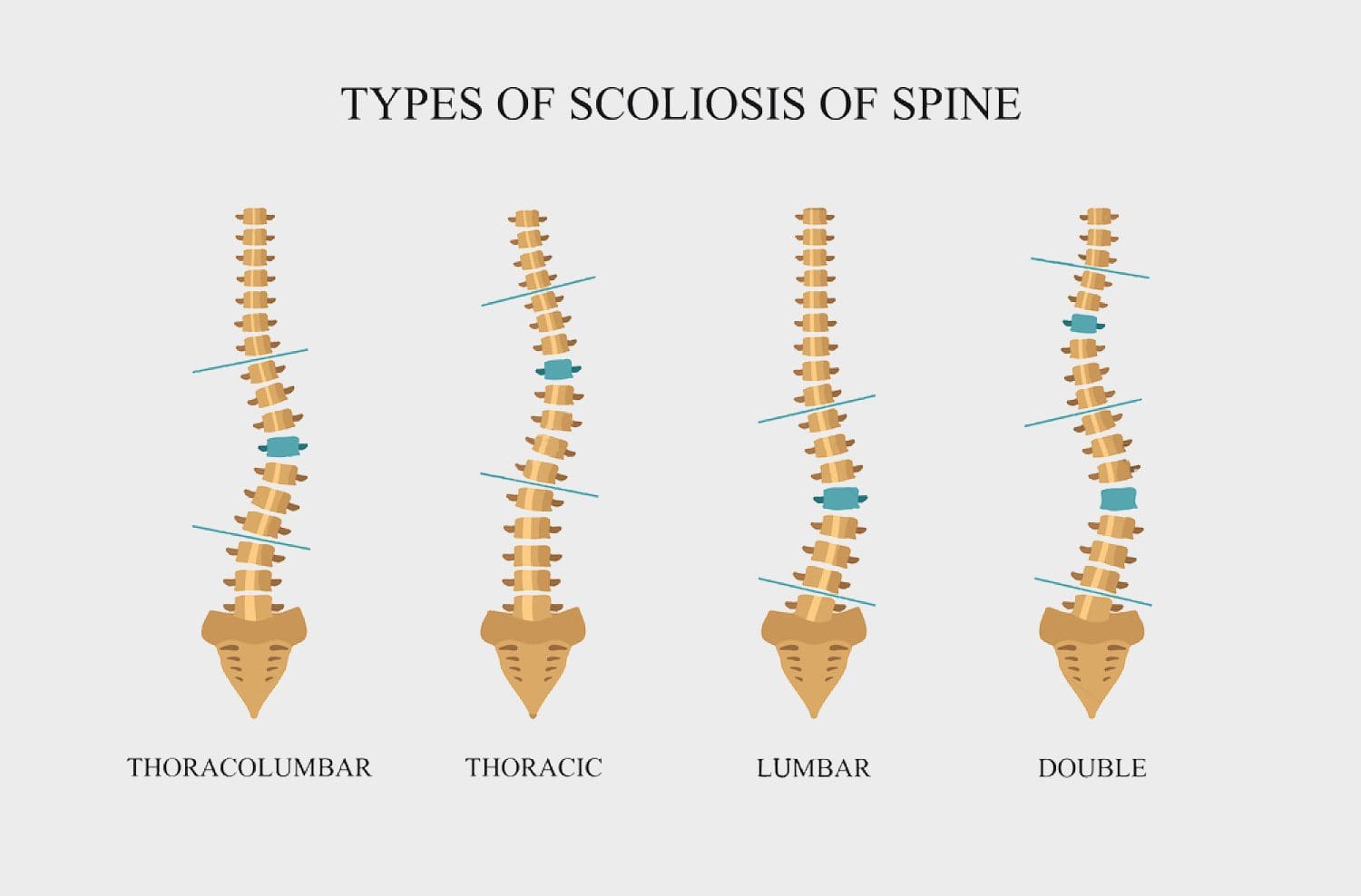
Scoliosis � This spinal curvature disorder can affect the entire spine, causing it to curve sideways, forming a C or S shape.
What are the symptoms?
Each type of curvature exhibits its own set of symptoms. While some symptoms may overlap, many are unique to the specific curvature disorder.
Lordosis
A �swayback� appearance where the buttocks stick out or are more pronounced.
Discomfort in the back, typically in the lumbar region
When lying on a hard surface on the back, the lower back area does not touch the surface, even when attempting to tuck the pelvis and straighten the lower back.
Difficulty with certain movements
Back pain
Kyphosis
A curve or hump to the upper back
Upper back pain and fatigue after sitting or standing for long periods (Scheuermann�s kyphosis)
Leg or back fatigue
The head bends far forward instead of being more upright
Scoliosis
Hips or waist are uneven
One shoulder blade is higher than the other
The person leans to one side
What are the causes?
Many different health issues can cause the spine to become misaligned or to form a spinal curvature. Each of the spinal conditions mentioned is affected by different conditions and situations.
Lordosis
Osteoporosis
Achondroplasia
Discitis
Obesity
Spondylolisthesis
Kyphosis
Kyphosis
Arthritis
Tumors on or in the spine
Congenital kyphosis (abnormal development of the vertebrae while the person is in utero)
Spina bifida
Scheuermann’s disease
Spine infections
Osteoporosis
Habitual slouching or poor posture
Scoliosis is still a bit of a mystery to doctors. They are not certain what exactly causes the most common form of scoliosis that is typically seen in children and adolescents. Some of the causes that they have pinpointed include:
There are screenings available for both children and adults to identify any spinal curvatures in their early stages through your chiropractor. Early detection of these disorders is crucial in identifying them before they become too serious.
Personalized Spine & *SCIATICA TREATMENT* | El Paso, TX (2019)
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine