Spinal Hygiene Explained: Daily Habits to Keep Your Spine Strong and Pain-Free
A woman performs spinal hygiene exercises on a fitness ball at home, strengthening her back muscles.
Spinal hygiene is the practice of caring for your spine every day to keep it strong, flexible, and healthy. Just like brushing your teeth helps prevent cavities, spinal hygiene helps avoid back problems and keeps your body moving well. The spine supports your whole body, protects the nervous system, and lets you bend, twist, and stand tall. Good habits can make a big difference in how you feel now and as you get older.
What Spinal Hygiene Means
Spinal hygiene includes simple daily actions to protect the spine’s natural shape and movement. The spine has gentle curves that help absorb shock and allow smooth motion. When these curves stay balanced, and the spine moves freely, you feel better overall.
Proper posture: Sit and stand with your shoulders back, head aligned over your spine, and pelvis in a neutral position to avoid extra strain.
Regular movement and exercise: Stay active with walking, swimming, or stretching to keep joints loose and muscles strong.
Proper body mechanics: Lift things by bending your knees, keeping objects close to your body, and avoiding twists to prevent injury.
Core strength: Build muscles around your midsection for better support and stability.
Hydration and nutrition: Drink plenty of water to keep spinal discs cushioned, and eat foods rich in calcium, vitamin D, magnesium, and omega-3 fatty acids to support bone and tissue health.
Stress management: Use deep breathing, meditation, or yoga to reduce tension that tightens back muscles.
These steps help maintain the spine’s integrity and prevent issues like stiffness or pain (Spinenpain.org, n.d.; Lifemovesmt.com, n.d.).
Neglecting spinal hygiene can lead to problems over time. Poor habits can cause muscle imbalances, joint wear, reduced motion, and conditions such as herniated discs or chronic back pain. This can affect your nervous system, since the spine houses nerves that control body functions. When the spine is out of alignment, it may press on nerves, leading to pain, weakness, or other issues (Servinglifedallas.com, n.d.; Drmmalone.com, n.d.).
Benefits of Good Spinal Hygiene
Taking care of your spine brings many advantages. It reduces the chance of back pain, improves how easily you move, and supports better posture. A healthy spine also helps the nervous system function smoothly, boosting energy, coordination, and overall well-being. Regular care can slow age-related changes, lower injury risk, and help you stay active longer.
Prevents muscle tightness and joint problems
Improves blood flow and nutrient delivery to spinal tissues
Enhances balance and reduces fall risk
Supports better sleep and less daily discomfort
Studies and experts note that these habits promote long-term health and vitality (Illinoisspinalcare.com, n.d.; Spinehealth.org, n.d.).
How Chiropractic Care Fits In
Chiropractic care plays a key role in spinal hygiene. Chiropractors use gentle adjustments to fix misalignments, called subluxations, that can stress the spine and nerves. These adjustments restore proper movement, reduce pain, and improve function. Regular chiropractic visits act as preventive maintenance, catching small issues before they grow.
Many people combine chiropractic with other habits for the best results. Adjustments improve alignment, while daily posture and exercise help maintain gains. This approach helps address common complaints such as neck or low back pain and supports recovery from injuries (Illinoisspinalcare.com, n.d.; Eastportlandchiropractor.com, n.d.).
The Power of Integrative Care with Chiropractors and Nurse Practitioners
An integrative approach brings together diverse experts to achieve stronger results. Chiropractors focus on the spine’s structure, alignment, and movement through adjustments and rehab. Nurse practitioners (NPs), especially those with advanced training, address broader health needs such as nutrition, stress management, hormone balance, and lifestyle changes.
This team effort addresses both the physical spine and daily habits that affect it. For example, a chiropractor might correct alignment after an injury, while an NP guides on anti-inflammatory foods or stress reduction to aid healing. Together, they create personalized plans that work better than one alone, especially for complex pain, chronic issues, or recovery from accidents.
Dr. Alexander Jimenez, DC, APRN, FNP-BC, stands out in this field. As a Doctor of Chiropractic and board-certified Family Nurse Practitioner, he combines spinal adjustments, decompression therapy, and functional medicine. His practice emphasizes root-cause care, using nutrition, lifestyle tweaks, and advanced diagnostics for musculoskeletal problems, personal injuries, and overall wellness. Clinical observations from his work show that integrative methods restore mobility, reduce pain, and improve quality of life by treating the whole person—not just symptoms (Dralexjimenez.com, n.d.; A4m.com, n.d.).
Simple Ways to Start Spinal Hygiene Today
You can begin with easy changes that fit into daily life.
Posture checks: Set reminders to sit tall and take breaks from sitting every 30 minutes.
Daily stretches: Try cat-cow pose, child’s pose, or seated twists for 5-10 minutes.
Safe lifting: Always bend at the knees and use your legs.
Stay hydrated: Drink water throughout the day to keep your discs healthy.
Eat spine-friendly foods: Include leafy greens, fish, nuts, and dairy or alternatives for key nutrients.
Move often: Walk or do low-impact activity for at least 30 minutes most days.
Manage stress: Practice deep breathing or short meditation sessions.
Adding regular chiropractic check-ups can help monitor and maintain progress (Lifemovesmt.com, n.d.; Newlifefamilychiropractic.net, n.d.).
Final Thoughts
Spinal hygiene is a smart, everyday way to protect one of your body’s most important parts. By focusing on posture, movement, nutrition, and professional care when needed, you support a strong spine, healthy nerves, and a better quality of life. Small habits add up to big benefits, helping you stay active and pain-free for years.
A physiotherapist works on a patient’s foot as part of their neuropathy treatment in the clinic
A Local, Integrative Approach from El Paso Back Clinic
Peripheral neuropathy is a common concern for many people in El Paso. Questions usually center on why symptoms are happening, how diabetes and spine health are connected, and what can be done beyond medication. At El Paso Back Clinic, care focuses on non-invasive, whole-person strategies that improve nerve function, movement, and daily quality of life.
This article answers the most common local questions in clear language and explains how integrative chiropractic care—coordinated with nurse practitioner (NP) oversight—addresses neuropathy by treating both symptoms and root causes. Clinical insights reflect the experience of Dr. Alexander Jimenez, DC, APRN, FNP-BC.
What Is Peripheral Neuropathy?
Peripheral neuropathy happens when nerves outside the brain and spinal cord are damaged or irritated. These nerves help you feel sensation, move muscles, and regulate automatic body functions like sweating and digestion. When nerve signals are disrupted, symptoms can feel burning, sharp, numb, or electric (West Texas Pain Institute, n.d.; Frontier Neurology, n.d.).
Most Common Neuropathy Symptoms We See in El Paso
People in El Paso often describe similar patterns:
Burning or throbbing pain (especially at night)
Tingling or “pins and needles”
Numbness in the feet or hands
Electric or shooting pain
Muscle weakness or cramping
Balance problems or frequent trips
Sensitivity to touch
In more advanced cases, symptoms can involve digestion, bladder control, or sweating (Frontier Neurology, n.d.).
Why Neuropathy Is So Common in This Region
A major driver locally is diabetes and prediabetes. High blood sugar can injure small blood vessels that feed nerves, leading to poor nerve signaling over time.
Other contributors include:
Spine and posture problems that stress nerve roots
Vitamin deficiencies (especially B vitamins)
Circulation issues
Prior injuries or repetitive strain
Certain medications or alcohol overuse
Inflammatory or autoimmune conditions
Many patients have multiple contributing factors, which is why a full evaluation is important (Medicos Family Clinic, n.d.; West Texas Pain Institute, 2023).
How Diabetic Neuropathy Affects Daily Life
Diabetic neuropathy often begins in the feet and slowly progresses upward. Common concerns include:
Burning feet at night
Loss of protective sensation
Higher risk of cuts, sores, and ulcers
Changes in walking or posture
Increased fall risk
Early integrative care can slow progression and reduce complications (El Paso Feet, n.d.; iVascular Center, n.d.).
How Neuropathy Is Evaluated at El Paso Back Clinic
Diagnosis is not based solely on symptoms. A complete assessment looks at the whole person.
Evaluation commonly includes:
Detailed health and symptom history
Review of blood sugar control and medications
Neurological and sensory testing
Posture and movement analysis
Spinal and joint evaluation
Imaging when nerve compression is suspected
Dr. Jimenez emphasizes that neuropathy symptoms often overlap with spinal nerve irritation or biomechanical stress, making dual-scope evaluation especially valuable (Jimenez, n.d.-a; Nonsurgical Spine Center, n.d.).
Can Neuropathy Improve Without Surgery?
For many people, yes. Most patients want conservative options before considering surgery or long-term medication use.
Non-surgical strategies may include:
Chiropractic care
Targeted exercise and physical therapy
Lifestyle and nutrition guidance
Laser therapy
Nerve stimulation techniques
Footwear and balance support
Stress and sleep optimization
Combining approaches is often more effective than relying on just one method (P3 Physical Therapy, n.d.; El Paso Feet, n.d.).
How Chiropractic Care Supports Nerve Health
Chiropractic care focuses on restoring healthy movement in the spine and joints, thereby reducing stress on nerves.
At El Paso Back Clinic, care may include:
Gentle spinal adjustments
Joint mobilization
Postural correction
Nerve decompression strategies
Soft tissue techniques
Guided movement and mobility work
Clinical observations show that improving spinal mechanics can enhance nerve signaling and reduce irritation—especially when neuropathy overlaps with back or neck problems (Jimenez, n.d.-b; El Paso Back Clinic, n.d.).
The Role of Nurse Practitioners in Neuropathy Care
Nurse practitioners (NPs) are essential for addressing medical and metabolic contributors to nerve damage.
NP-guided support may involve:
Lab testing and result interpretation
Diabetes and metabolic management
Identifying vitamin or nutrient deficiencies
Reviewing medication side effects
Monitoring nerve-related complications
Dr. Jimenez’s dual licensure allows structural findings and medical factors to be evaluated together, helping patients understand why symptoms are happening—not just where they hurt (Jimenez, n.d.-c).
Why an Integrative Approach Works Best
Neuropathy rarely has a single cause. Integrative care addresses multiple systems at once.
Benefits include:
More accurate diagnosis
Personalized care plans
Reduced dependence on pain medications
Improved balance, strength, and confidence
Better long-term nerve health
This approach is especially helpful for people with diabetes, chronic back pain, or long-standing symptoms (HealthCoach Clinic, n.d.; Pain and Wellness Institute, n.d.).
Physical Therapy and Movement for Nerve Recovery
Physical therapy complements chiropractic care by retraining safe movement and improving circulation.
Physical therapy may help by:
Strengthening supportive muscles
Improving balance and coordination
Reducing fall risk
Teaching nerve-friendly movement patterns
When coordinated with chiropractic and NP care, recovery is often faster and more sustainable (P3 Physical Therapy, n.d.).
Lifestyle Habits That Matter for Neuropathy
Daily habits can either protect or irritate nerves.
Helpful habits include:
Keeping blood sugar stable
Wearing supportive footwear
Limiting alcohol and avoiding smoking
Staying physically active
Managing stress
Prioritizing sleep
Small, consistent changes can reduce flare-ups and improve comfort over time (Modern Pain Houston, n.d.; Dr. Dennis Harris, n.d.).
Emotional and Community Support
Living with nerve pain can affect mood and sleep. Support makes a difference.
Education and coaching
Stress-management strategies
Peer or virtual support groups
Family involvement in care plans
Support resources help patients feel informed and empowered (Foundation for Peripheral Neuropathy, n.d.).
When to Seek Professional Help
Consider an evaluation if you notice:
Persistent tingling or numbness
Burning or electric pain
Muscle weakness
Balance problems or frequent falls
Foot wounds that heal slowly
Early care can help prevent progression and complications (West Texas Pain Institute, n.d.; Frontier Neurology, n.d.).
The El Paso Back Clinic Difference
At El Paso Back Clinic, neuropathy care is centered on conservative, patient-focused solutions. By combining chiropractic care with nurse practitioner oversight and lifestyle strategies, patients receive practical, non-invasive options designed to improve nerve function and daily life.
Healthy Mexican Food in El Paso: Wellness Choices at El Paso Back Clinic®
Mexican food brings fresh, bold flavors to life in El Paso, Texas. At El Paso Back Clinic®, the premier wellness chiropractic care clinic, we see how good nutrition supports recovery, reduces inflammation, and boosts overall health. Led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, our team combines chiropractic adjustments with nutrition guidance to help patients heal from injuries and live pain-free.
In a city rich with Mexican culture, choosing healthier versions of classic dishes fits perfectly into a holistic wellness plan. Focus on grilled proteins, plenty of vegetables, and fresh ingredients to enjoy tasty meals that aid healing and mobility.
Shrimp Ceviche Recipe – Meals by Molly: Seafood Recipes
Chicken Tortilla Soup: Broth-based with lean chicken, veggies, and avocado.
Burrito Bowls: Brown rice, beans, grilled protein, and fresh salsa.
Soft Tacos: Corn tortillas with fish, chicken, or beans plus extra veggies.
These dishes use natural ingredients like beans for gut health, avocado for good fats, and fresh salsas for vitamins (Havranek, n.d.; Isabel Eats, n.d.).
Key fresh ingredients that support wellness include:
Beans (black or pinto) for fiber and protein.
Avocado for healthy fats that fight inflammation.
Nopalitos (cactus) and calabacitas (zucchini) for low-calorie nutrients.
Pico de gallo with tomatoes, onions, and chilies.
Lean proteins like grilled chicken, shrimp, or fish.
These elements help reduce swelling and support recovery, especially when paired with care at El Paso Back Clinic® (Gran Luchito, n.d.).
El Paso offers excellent spots for healthy Mexican options. Many places let you customize for wellness:
Sabrosa La Vida for fresh meals.
Verde Salad Co. for build-your-own bowls.
Timo’s Restaurant for lean, veggie-focused plates.
Look for restaurants that grill proteins and use fresh prep. These choices make it easy to eat well while enjoying local flavors.
At El Paso Back Clinic®, we focus on holistic wellness. Dr. Alexander Jimenez uses integrative chiropractic care and nurse practitioner expertise to treat the whole person. Spinal adjustments improve alignment and nerve function, while nutrition advice targets inflammation and healing.
Dr. Jimenez often recommends anti-inflammatory foods like fresh veggies, lean proteins, and healthy fats found in healthier Mexican dishes. This helps patients recover faster from back pain, injuries, or chronic issues (Jimenez, n.d.a; Jimenez, n.d.b).
Our clinic offers:
Personalized chiropractic adjustments.
Nutrition plans to reduce inflammation.
Functional medicine for root-cause healing.
Rehab to build strength and mobility.
Combining these with smart food choices yields better long-term wellness outcomes (Cleveland Clinic, n.d.).
Here are simple tips to make healthy Mexican eating part of your routine:
Start with ceviche or salsa instead of chips.
Fill half your plate with veggies.
Choose water or herbal tea over sugary drinks.
Try home cooking with local fresh ingredients.
In El Paso’s dry climate, staying hydrated helps too.
Healthy Mexican food supports the body in powerful ways. At El Paso Back Clinic®, we help patients use nutrition and chiropractic care together for pain relief, better mobility, and vibrant health. Dr. Jimenez and the team are here to guide you toward feeling your best.
Contact us today to start your personalized wellness journey.
Innovations in Sciatica Treatment in 2026: A Shift Toward Targeted, Minimally Invasive, and Integrative Care
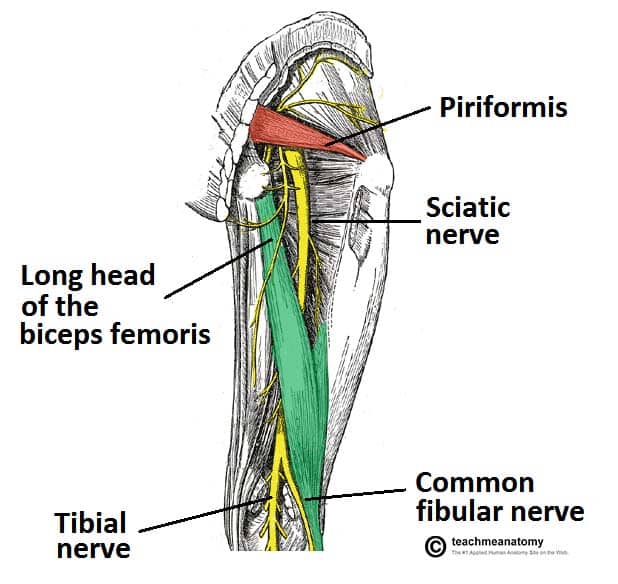
Sciatica is one of the most common causes of chronic lower back and leg pain. It occurs when the sciatic nerve—the longest nerve in the body—is irritated or compressed, often due to disc herniation, spinal degeneration, inflammation, or biomechanical imbalance. For years, treatment options focused mainly on pain medications, steroid injections, or surgery when symptoms became severe.
In 2026, sciatica care has entered a new phase. Treatment is no longer just about “blocking pain.” Instead, the focus is on precision diagnosis, nerve healing, inflammation reduction, and functional recovery, with fewer complications and faster healing times. These advances also emphasize integrated, interdisciplinary care, combining chiropractic treatment with the diagnostic and clinical oversight of nurse practitioners (NPs).
This article explains the most important innovations shaping sciatica treatment in 2026, using easy-to-understand language while staying grounded in current clinical research and real-world outcomes.
Understanding Sciatica: Why Better Solutions Were Needed
Sciatica is not a single disease. It is a symptom caused by pressure or irritation along the sciatic nerve, usually beginning in the lower spine and traveling into the buttock and leg. Pain can feel sharp, burning, electric, or aching and may include numbness or weakness.
Common contributors include:
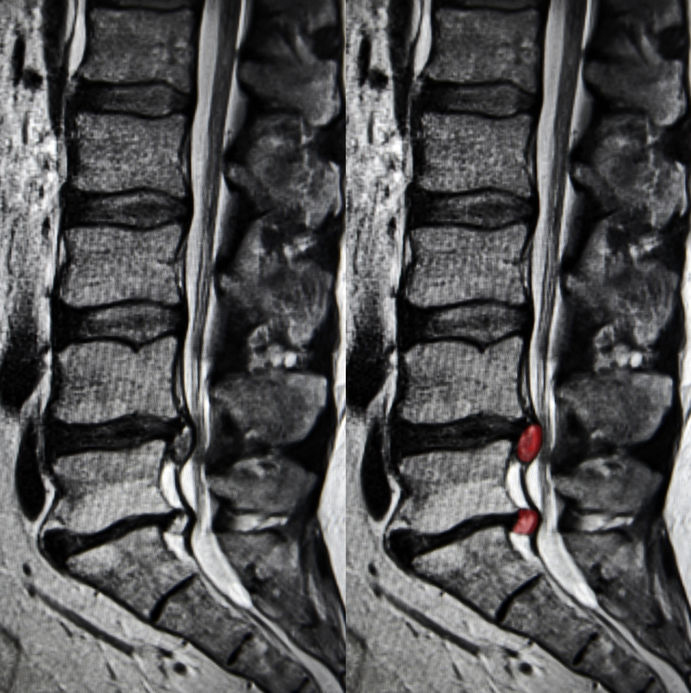
Herniated or bulging lumbar discs
Spinal stenosis
Degenerative disc disease
Muscle imbalance or pelvic instability
Inflammation around nerve roots
Traditional treatments often relied on:
Long-term anti-inflammatory or pain medications
Opioids for severe cases
Epidural steroid injections
Surgery as a last resort
While these approaches helped some patients, they did not always address the underlying cause, and many carried risks such as dependency, complications, or prolonged recovery (Stanford Health Care, n.d.).
What Has Changed in 2026?
By 2026, sciatica treatment emphasizes early, targeted, and minimally invasive care. Research and clinical experience now show that addressing nerve irritation early and restoring healthy movement patterns can prevent chronic pain and disability (BioSpace, 2025).
Key changes include:
Improved imaging and diagnostics
Precision-guided nerve procedures
Regenerative medicine options
Advanced neuromodulation technologies
Integrated chiropractic and NP-led care models
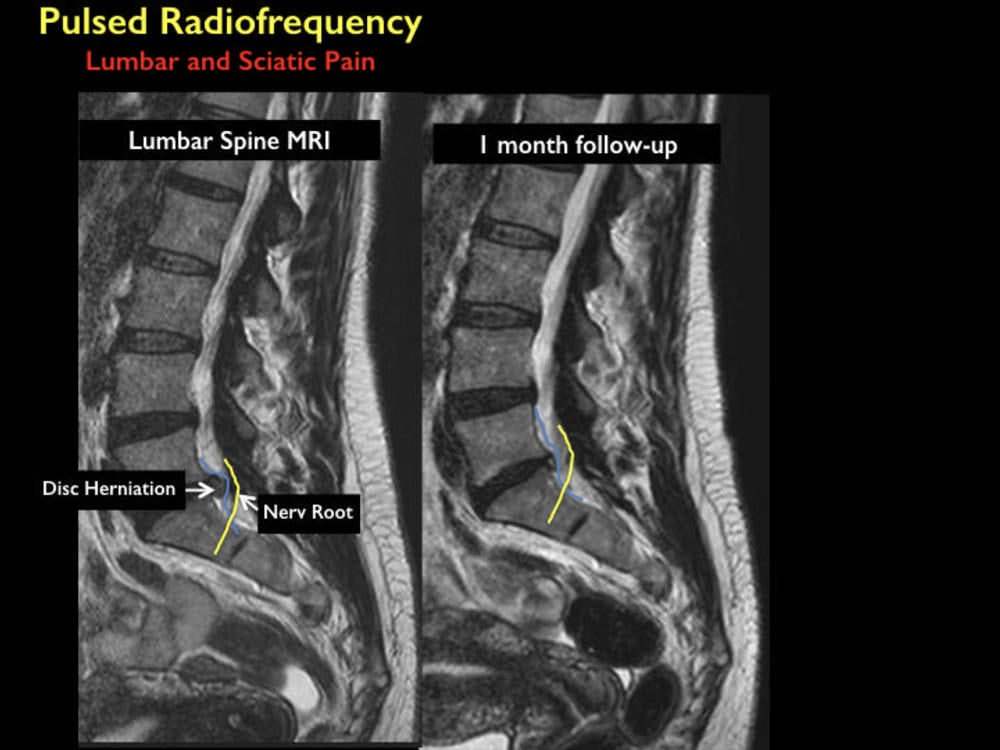
Advanced Diagnostic Imaging: Seeing the True Source of Pain
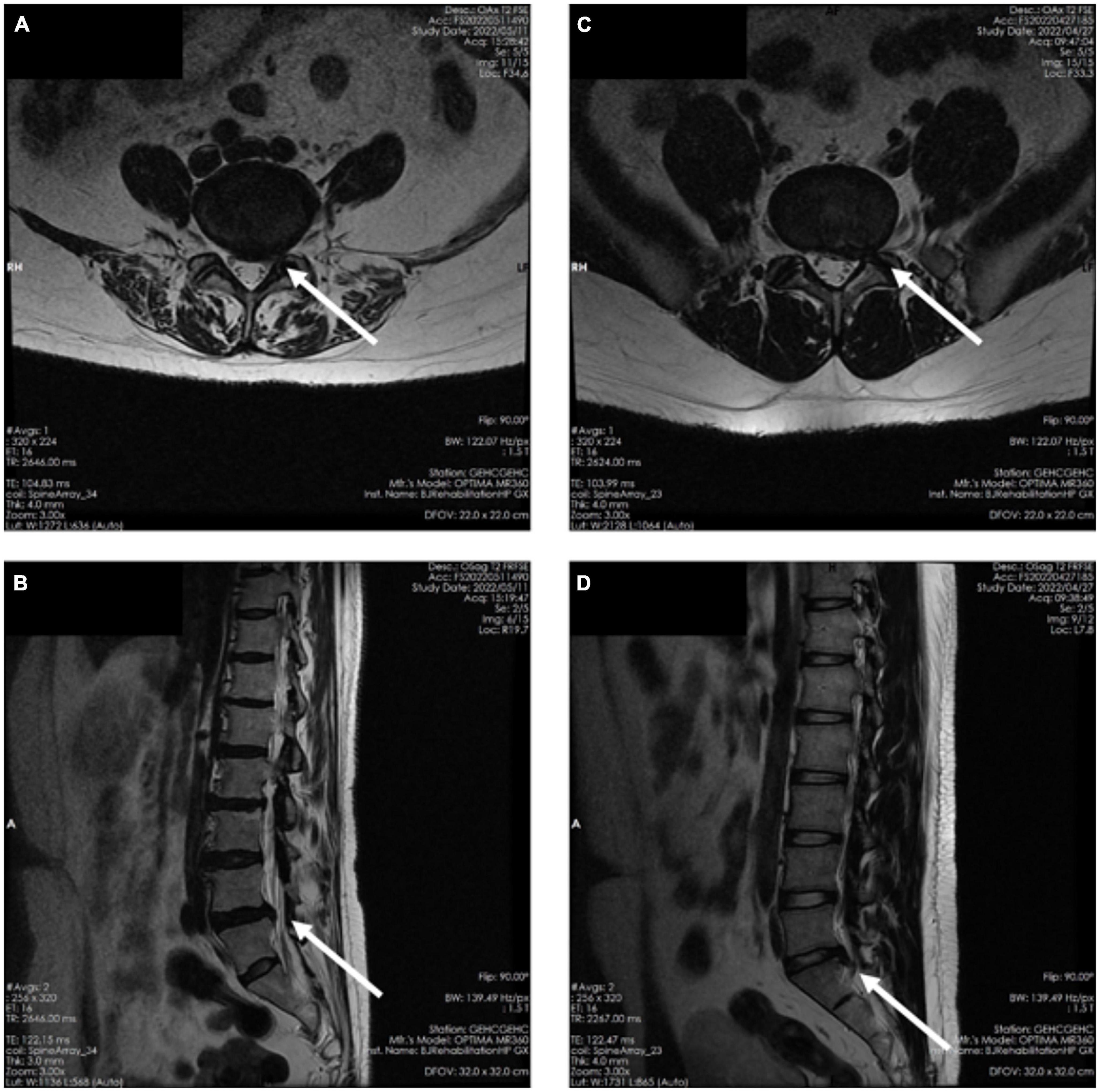
One of the biggest improvements in sciatica care is high-resolution MRI technology. Modern imaging allows clinicians to:
Identify the exact nerve root involvement
Distinguish disc-related pain from muscular or inflammatory causes
Detect subtle nerve inflammation missed in earlier imaging methods
Enhanced MRI protocols now guide treatment decisions more accurately, reducing unnecessary procedures and improving outcomes (Stanford Health Care, n.d.).
Nurse practitioners play a critical role here by:
Ordering and interpreting imaging
Correlating findings with physical symptoms
Coordinating referrals and follow-up care
Minimally Invasive Pain Procedures: Precision Without Surgery
Improved Nerve Blocks
Modern nerve blocks are no longer “blind injections.” In 2026, they are image-guided and highly targeted, delivering medication exactly where inflammation and irritation occur.
Benefits include:
Faster pain relief
Reduced medication dosage
Improved diagnostic clarity
Lower complication risk
Nerve blocks are now often used as diagnostic tools to help clinicians determine whether pain is mechanical, inflammatory, or neuropathic in origin (Apollo Spine & Pain, 2026a).
Radiofrequency Ablation (RFA)
Radiofrequency ablation uses controlled heat to disrupt pain signals traveling through irritated nerves. Newer RFA systems are more precise and selective than earlier versions.
Key advantages:
Long-lasting pain relief
Minimal tissue damage
Short recovery time
Reduced reliance on medications
RFA is especially helpful for chronic sciatica that does not respond to conservative care (Apollo Spine & Pain, 2026b).
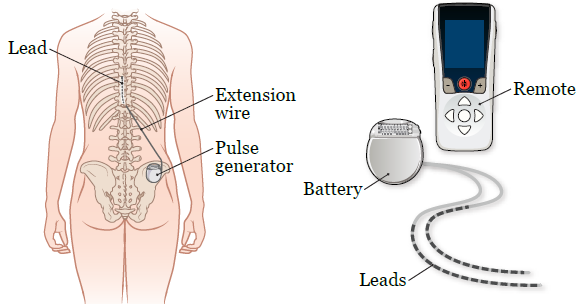
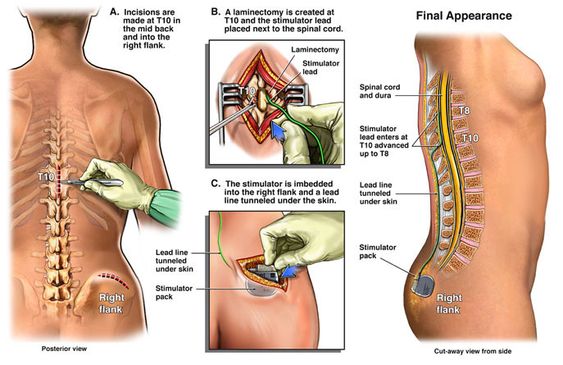
Spinal Cord Stimulation: Rewiring Pain Perception
Spinal cord stimulation (SCS) has evolved significantly. New devices are smaller, smarter, and more adaptive. They deliver gentle electrical signals that change how the brain interprets pain signals from the sciatic nerve.
Modern SCS systems offer:
Personalized stimulation patterns
Adjustable settings via external controllers
Reduced side effects compared to older models
SCS is now used earlier in care for select patients, helping many avoid surgery altogether (Pain and Spine Specialists, n.d.).
Regenerative Medicine: Supporting Nerve Healing
Platelet-Rich Plasma (PRP)
PRP therapy uses a patient’s own blood components to promote healing and reduce inflammation. In sciatica care, PRP is increasingly used around:
Inflamed nerve roots
Degenerative disc structures
Surrounding soft tissues
Research suggests PRP may:
Reduce inflammation
Support tissue repair
Improve long-term outcomes
While still evolving, regenerative therapies are driving growth in the global sciatica treatment market (Grand View Research, n.d.; PMC, 2024).
Therapeutic Exercise Innovations: Movement as Medicine
Nerve Flossing and Targeted Rehab
Exercise therapy in 2026 is more specific and personalized. One standout approach is nerve flossing, which involves controlled movements designed to improve nerve mobility and reduce irritation.
Benefits include:
Improved nerve glide
Reduced stiffness
Decreased pain during daily activities
Programs are now customized using imaging findings and functional testing, ensuring exercises match the patient’s specific condition (Goodman Campbell, 2026).
Chiropractic Care: A Drug-Free Foundation
Chiropractic care remains central to non-surgical sciatica treatment. Modern chiropractic approaches focus on restoring spinal alignment, reducing nerve compression, and improving movement patterns.
Common techniques include:
Spinal adjustments
Flexion-distraction therapy
Soft tissue mobilization
Low-level laser therapy
Research continues to associate chiropractic care with reduced opioid use and improved pain outcomes (ReachMD, 2024; UH Hospitals, 2025).
Integrated Care: Chiropractors and Nurse Practitioners Working Together
One of the most important shifts in 2026 is the collaborative care model. Instead of isolated treatment, patients benefit from coordinated care involving chiropractors and nurse practitioners.
This model allows for:
Accurate diagnosis and imaging oversight
Conservative, drug-free pain management
Monitoring of neurological symptoms
Reduced opioid exposure
Clinical observations from Dr. Alexander Jimenez, DC, APRN, FNP-BC, highlight that patients receiving coordinated chiropractic and NP care often experience:
Faster recovery
Better functional improvement
Fewer invasive interventions
Greater long-term pain control
His integrative approach emphasizes treating the cause of nerve irritation, not just the symptoms (Jimenez, n.d.).
Why These Innovations Matter
Together, these advances represent a major shift in sciatica care:
From surgery-first to conservative-first
From symptom masking to root-cause resolution
From isolated care to interdisciplinary teamwork
Patients now have more options, fewer risks, and better long-term outcomes.
Conclusion: The Future of Sciatica Care Is Personalized and Precise
By 2026, sciatica treatment has become more effective, safer, and patient-centered. Innovations in diagnostics, minimally invasive procedures, regenerative medicine, and integrative chiropractic-NP–NP care are reducing the need for surgery and long-term medication use.
The focus is no longer just pain relief—it is nerve health, mobility restoration, and sustainable recovery. As research and technology continue to evolve, patients suffering from sciatica can expect even more targeted, evidence-based solutions in the years ahead.
Common Sports Injuries in El Paso and How El Paso Back Clinic Supports Full Recovery
Sports and physical activity are part of everyday life in El Paso. From running and weight training to football, soccer, and basketball, people of all ages stay active year-round. While this active lifestyle is healthy, it also leads to a high number of sports-related musculoskeletal injuries—especially when combined with the region’s heat, rough ground, and uneven terrain.
At El Paso Back Clinic, sports injury care focuses on restoring spinal alignment, joint mobility, muscle balance, and overall movement quality. When chiropractic care is combined with nurse practitioner (NP) support, athletes receive complete, coordinated care that promotes healing, performance, and long-term injury prevention.
Clinical observations from Dr. Alexander Jimenez, DC, APRN, FNP-BC, show that athletes recover more efficiently when spine health, joint mechanics, muscle function, and medical oversight are addressed together rather than separately.
Why Sports Injuries Are So Common in El Paso
El Paso presents unique physical challenges for athletes and active individuals. The environment itself can increase stress on the musculoskeletal system.
Common contributing factors include:
High temperatures, which increase fatigue and dehydration
Hard and uneven surfaces, stressing feet, ankles, knees, and hips
Year-round activity, limiting rest and recovery
High-impact sports, such as football and basketball
Repetitive movement patterns, common in running and training
When the spine and joints are not moving properly, the body compensates. Over time, these compensations increase injury risk and slow healing (NIAMS, n.d.).
Common Sports-Related Musculoskeletal Injuries Seen in El Paso
Sprains and Strains
Sprains and strains are among the most frequently treated injuries at El Paso Back Clinic.
Sprains affect ligaments
Strains affect muscles or tendons
Common areas include:
Ankles
Knees
Hamstrings
Lower back
These injuries often occur during quick movements, twisting, jumping, or improper warm-ups (Orthospine Centers, n.d.).
Knee Injuries (ACL, Meniscus, Runner’s and Jumper’s Knee)
Knee injuries are especially common in sports that involve cutting, jumping, or sudden stops.
Typical knee problems include:
ACL tears
Meniscus tears
Patellar tendonitis (jumper’s knee)
Runner’s knee
Misalignment in the spine, hips, or feet can increase stress on the knee joint, making chiropractic care an important part of recovery (Spectrum Therapy Consultants, n.d.).
Tendonitis and Overuse Injuries
Tendonitis develops when tendons are repeatedly stressed without enough recovery.
Common forms include:
Tennis elbow
Golfer’s elbow
Achilles tendonitis
Patellar tendonitis
These injuries often worsen slowly and are common in athletes who push through pain (Woodlands Sports Medicine, n.d.).
Shin Splints and Stress Fractures
Lower-leg injuries are common in runners and field athletes.
These include:
Shin splints
Foot stress fractures
Tibial stress injuries
Hard surfaces, worn footwear, and poor biomechanics increase the risk of these injuries (CTX Foot & Ankle, n.d.).
Hip Labral Tears
Hip labral tears affect the cartilage that stabilizes the hip joint.
Common symptoms include:
Deep hip or groin pain
Clicking or locking sensations
Reduced range of motion
These injuries are common among athletes who frequently twist, pivot, or sprint (Texas Spine Clinic, n.d.).
Rotator Cuff and Shoulder Injuries
Shoulder injuries often occur in athletes who lift, throw, or absorb contact.
Common issues include:
Rotator cuff strains or tears
Shoulder impingement
Joint instability
Shoulder pain is often linked to spinal and postural imbalances that chiropractic care addresses (Marque Medical, n.d.).
Lower Back Pain and Sciatica
Lower back pain is one of the most common complaints among athletes.
Contributing factors include:
Muscle strain
Core weakness
Poor posture
Spinal joint restrictions
When spinal alignment is compromised, nerve irritation such as sciatica may occur (Marque Medical, n.d.).
How Chiropractic Care at El Paso Back Clinic Helps Sports Injuries
Chiropractic care at El Paso Back Clinic focuses on restoring proper motion to the spine and joints. This allows the nervous system, muscles, and joints to work together efficiently.
Improving alignment reduces stress on injured tissues and supports natural healing (Vista Hills Chiropractic, n.d.).
Benefits of Chiropractic Care for Athletes
Athletes receiving chiropractic care often experience:
Reduced pain and stiffness
Improved joint mobility
Better balance and coordination
Faster recovery times
Lower risk of repeat injuries
Clinical experience shows that addressing spinal alignment early improves outcomes across many sports injuries (Jimenez, n.d.).
The Role of Nurse Practitioners in Integrated Sports Injury Care
Nurse practitioners (NPs) play an important role in sports injury management by providing medical oversight and coordination of care.
NPs may assist by:
Performing initial evaluations
Ordering diagnostic imaging (X-ray, MRI)
Managing pain and inflammation
Coordinating physical therapy
Monitoring healing progress
This medical support ensures injuries are accurately diagnosed and treated safely (NIAMS, n.d.).
Functional and Preventive Approach to Recovery
NPs often use a functional approach that looks beyond the injured area.
This includes evaluating:
Movement patterns
Training load
Nutrition and hydration
Sleep and recovery habits
Inflammation levels
Addressing these factors helps athletes heal fully and return stronger.
Coordinated Care: Chiropractic, NP, and Rehabilitation
One of the strengths of El Paso Back Clinic is coordinated care. Chiropractic care and NP oversight work together with rehabilitation to create a clear recovery plan.
A coordinated plan may include:
Chiropractic adjustments for alignment
Rehabilitation exercises for strength and stability
Medical monitoring for healing progress
Gradual return-to-sport planning
This team-based approach improves outcomes and reduces setbacks (Southwest Chiropractors, n.d.).
PRP Therapy and Advanced Recovery Options
For certain injuries, platelet-rich plasma (PRP) therapy may be recommended.
PRP may support healing for:
Tendon injuries
Ligament sprains
Knee injuries
Early osteoarthritis
NPs evaluate whether PRP is appropriate and coordinate care alongside chiropractic treatment and rehabilitation (Desert Institute of Sports Medicine, n.d.).
Clinical Example: Knee Injury Recovery at El Paso Back Clinic
Based on clinical observations from Dr. Jimenez, a typical knee injury recovery plan may include:
NP evaluation to diagnose the injury
Imaging to assess ligament or cartilage damage
Chiropractic care to improve spinal, hip, and knee alignment
Rehabilitation exercises to restore strength and stability
PRP therapy, when appropriate
Performance monitoring to prevent re-injury
This integrated approach supports long-term joint health and athletic performance.
Preventing Future Sports Injuries
Prevention is a major focus at El Paso Back Clinic.
Key strategies include:
Proper warm-ups and mobility work
Strengthening core and stabilizing muscles
Maintaining hydration in hot conditions
Correcting posture and movement patterns
Allowing adequate recovery time
Chiropractic and NP care help identify small problems before they become serious injuries (Texas Children’s Hospital, n.d.).
Long-Term Benefits of Integrated Sports Injury Care
Athletes who receive integrated care often experience:
Faster recovery
Fewer recurring injuries
Improved flexibility and strength
Better overall performance
Greater confidence in movement
Treating the spine, joints, muscles, and nervous system together leads to a more complete recovery.
Conclusion
Sports injuries are common in El Paso due to the climate, terrain, and high levels of physical activity. Injuries such as sprains, strains, knee injuries, tendonitis, back pain, and stress fractures can limit performance if not treated properly.
At El Paso Back Clinic, chiropractic care restores alignment and mobility, while nurse practitioners provide diagnostics, medical oversight, and coordinated treatment options. Together, this approach supports full recovery, injury prevention, and long-term performance.
Clinical experience from Dr. Alexander Jimenez shows that athletes recover best when care focuses on the whole musculoskeletal system—not just the painful area.
Relieve Lower Back and Hip Pain with Squats, Core Exercises, and Chiropractic Care at El Paso Back Clinic®
Many people in El Paso suffer from lower back pain and hip discomfort due to daily activities, work demands, injuries, or long-term issues. These problems often stem from muscle strains, poor posture, tight hips or glutes, and weak supporting muscles. At El Paso Back Clinic® in El Paso, TX, we specialize in helping patients overcome these challenges through personalized chiropractic care, rehabilitation, and safe exercises.
Squats and core exercises, performed correctly, strengthen the muscles that support the spine, improve alignment, and enhance hip mobility. This reduces stress on the back during movement. They are effective for chronic low back pain, mild sciatica, and general aches from weak muscles. Proper form is essential—sharp pain, numbness, or weakness means you should seek professional evaluation first.
Strong Core + Chiropractic for Lower Back and Hip Pain Relief
The lower back and hips are closely connected through shared muscles, joints, and nerves. Tight hips or glutes can tug on the back, leading to strain. Weak core muscles cause spinal instability and poor posture, leading to chronic pain.
Muscle imbalances force the back to overcompensate in everyday tasks.
Reduced hip mobility leads to excessive forward leaning, stressing the lower back.
Problems in ankle or upper back mobility contribute further.
These factors can result in lumbar instability or pain radiating from the hips to the back.
How Squats Benefit Lower Back and Hip Conditions
Squats strengthen the legs, glutes, and core. With proper technique, they relieve pressure from the lower back.
Proper squats maintain a neutral spine and engaged core, providing stability and minimizing lumbar strain. Activating core and hip muscles during squats supports the spine, preventing excessive arching or rounding.
Squats also increase hip mobility. Tight hip flexors are a common cause of back pain during deeper squats. Improved flexibility allows the hips to function better, sparing the back from overload.
Builds glutes and legs for stronger spinal support.
Enhances blood flow and reduces inflammation in the area.
Aids mild pain that improves with gentle activity.
Research supports that the correct form reduces risks associated with squats.
Core Exercises: A Key to Back and Hip Relief
Core exercises focus on deep muscles in the abdomen, back, and pelvis, acting as a natural spinal brace.
Strong core muscles enhance posture and balance, easing the load on spinal discs and preventing persistent pain from inadequate support. Studies show core stability exercises effectively reduce non-specific low back pain and improve function.
Core training also supports hip pain by stabilizing the pelvis, which is beneficial for conditions like arthritis or glute tightness.
Planks and bird-dogs develop endurance in stabilizing muscles.
Pelvic tilts and bridges safely activate deep muscles.
Standing core activities help relieve pain from prolonged sitting.
Evidence indicates that core exercises often outperform general workouts in reducing pain.
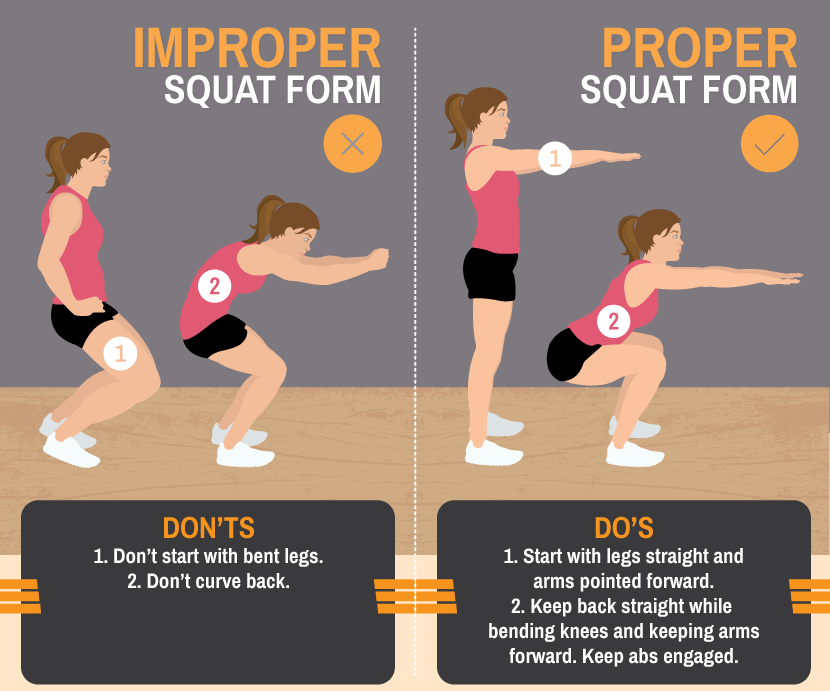
Mastering Proper Form for Safe Squats and Core Work
Incorrect squat form is a leading cause of lower back pain. Frequent mistakes include back rounding, knee collapse, or excessive weight.
Safe squat guidelines:
Position feet shoulder-width apart, toes slightly turned out.
Engage your core as if bracing for impact.
Hinge at the hips, keep the chest high, and descend until the thighs are parallel to the ground.
Drive up through heels, maintaining a neutral spine.
For core exercises, prioritize controlled movement. Hold planks straight with tight abs—avoid dipping or arching.
Begin with bodyweight versions and always warm up to boost circulation and lower injury risk.
Pain during squats typically indicates a weak core, tight hips, or mobility deficits. Address these with targeted stretches and progressive loading.
When Exercises Are Helpful and When to Get Professional Care
Squats and core exercises support:
Chronic low back pain from muscle weakness.
Mild sciatica by decreasing nerve pressure.
Hip tightness referring pain to the back.
Posture-related daily discomfort.
They foster long-term resilience and prevent compensatory back strain. Halt immediately if experiencing severe pain, numbness, weakness, or loss of balance—these may indicate serious conditions such as a disc herniation.
Consult a provider before beginning, especially if you have pre-existing injuries.
Integrative Care at El Paso Back Clinic®
At El Paso Back Clinic®, Dr. Alexander Jimenez, DC, APRN, FNP-BC, leads a team that delivers comprehensive, integrative chiropractic and wellness care for lower back and hip pain. Our approach combines squats and core exercises with chiropractic adjustments, spinal decompression, physical therapy, functional medicine, and rehabilitation programs.
Chiropractic adjustments correct misalignments and joint dysfunctions. A reinforced core helps maintain these corrections by enhancing spinal stability.
Dr. Jimenez creates tailored plans that address root causes through evidence-based protocols, drawing on over 30 years of experience in complex injuries, sciatica, and chronic pain. This multidisciplinary method often yields superior, sustained results compared to isolated treatments.
Visit our main location at 11860 Vista Del Sol, Suite 128, El Paso, TX 79936, or call (915) 850-0900 to schedule your consultation.
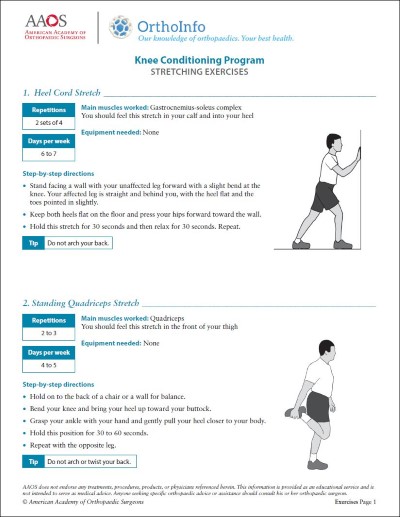
Beginner Exercises to Try Under Guidance
Start with these fundamentals, supervised by our team:
Bodyweight Squats: 3 sets of 10-15 repetitions, emphasizing technique.
Glute Bridges: Lie on your back, and elevate your hips by engaging your glutes.
Bird-Dog: On hands and knees, extend opposite arm and leg while bracing core.
Planks: Maintain position for 20-30 seconds, gradually increasing duration.
Pelvic Tilts: On the back, press the lower back into the floor via a pelvic tilt.
Incorporate 2-3 sessions weekly. Include hip mobility work and advance gradually.
Regain Comfort and Mobility Today
At El Paso Back Clinic®, squats and core exercises form integral components of our rehabilitation strategies for lower back and hip pain. They fortify stabilizing muscles, correct alignment, and promote mobility to manage strains, poor posture, instability, and tightness.
Combined with expert chiropractic and integrative care under Dr. Alexander Jimenez, they deliver lasting strength and relief.
Reach out to El Paso Back Clinic® today. Our team will assess your needs and develop a customized plan for optimal recovery.
Make Your Health Goals Stick in 2026: How El Paso Back Clinic’s Integrative Team Supports Real Change
The patient uses a weight machine for injury rehabilitation under the supervision of a doctor of chiropractic and a nurse practitioner.
Most people don’t fail at New Year’s goals because they “don’t want it enough.” They fail because life gets busy, pain flares up, energy crashes, and stress piles on. When your body hurts or feels stiff, even simple plans—like walking more, lifting weights, or sleeping better—can feel harder than they should.
At El Paso Back Clinic, the goal is to make health changes easier to achieve and maintain through a team-based, integrative approach. That means bringing together the strengths of chiropractic care (movement, structure, mobility, and recovery) with the strengths of nurse practitioner care and wellness coaching (nutrition, sleep, stress, and whole-body support). The clinic describes this as a blend of injury care, wellness strategies, mobility programs, and integrated medicine designed to improve function and quality of life. El Paso Back Clinic® • 915-850-0900+2El Paso Back Clinic® • 915-850-0900+2
This kind of care supports common goals like:
increasing fitness and mobility
managing pain so you can stay active
improving energy and sleep
lowering stress and improving your stress response
“Integrative care” means your plan isn’t built around only one angle. Instead, it connects the pieces that usually get separated:
How you move
How you recover
How you eat
How you sleep
How you manage stress
How do you build habits that fit your real life
El Paso Back Clinic describes integrative chiropractic benefits as going beyond traditional adjustments by combining care approaches that support overall wellness and function. El Paso Back Clinic® • 915-850-0900
Why this matters for resolutions
Many resolutions are difficult to maintain because the plans ignore the real barriers. For example:
You want to exercise more—but your back pain spikes.
You want to lose weight—but your sleep is poor and your stress is high.
You want more energy—but your nutrition is inconsistent, and you’re not recovering.
An integrative plan helps because it aims to reduce the friction that makes healthy habits feel impossible.
The Team Approach: Chiropractor + Nurse Practitioner Mindset
Many clinics talk about how chiropractic care supports goals such as mobility, stress reduction, better sleep, and improved performance. gotcore.net+2Freedom Chiropractic+2 At El Paso Back Clinic, that support is often strongest when chiropractic care is paired with whole-person planning.
The chiropractor’s lane: move better with less strain
Chiropractic care commonly focuses on:
joint motion and spinal mechanics
posture and movement habits
mobility and flexibility
recovery support when you start working out again
helping reduce strain patterns that keep pain looping
The descriptions of services at El Paso Back Clinic emphasize spine-focused care and the restoration of function for back and musculoskeletal concerns. El Paso Back Clinic® • 915-850-0900+1
The NP/wellness lane: build a plan that supports your body from the inside out
A nurse practitioner and wellness-minded team approach can support:
nutrition planning that fits your schedule
sleep improvement routines
stress management strategies
health screening and medical risk review when appropriate
coaching that makes change more realistic to sustain
This matches the habit-focused guidance many health organizations recommend: set realistic goals, build routines, and avoid extreme “all at once” changes. Prism Health North Texas
Dr. Alexander Jimenez’s clinical observations (El Paso context)
Dr. Alexander Jimenez (DC, APRN, FNP-BC) frequently describes a dual-scope approach that connects biomechanics (how you move) with broader health planning (nutrition, functional assessments, and recovery strategies). His published clinic content also highlights the use of assessments and, when needed, imaging and integrated care planning to support recovery and function. LinkedIn+3El Paso, TX Doctor Of Chiropractic+3El Paso, TX Doctor Of Chiropractic+3
Why Resolutions Often Fail (And How an Integrative Plan Fixes That)
Here are common “resolution killers” and what a coordinated plan can do differently:
Pain blocks movement → Address mobility limits and movement mechanics so activity feels doable. National Spine & Pain Centers+1
Low energy → Improve sleep, nutrition consistency, and recovery structure. gotcore.net+1
Stress overload → Add stress skills and routines that calm the system and support follow-through. NIH News in Health+1
No accountability → Regular check-ins and plan adjustments keep you from quitting after a setback. drmmalone.com+1
A key idea in habit-based care is that early wins create a “positive feedback loop”—you feel better, so it becomes easier to keep going. drmmalone.com
1) Increase Fitness and Mobility (Without Getting Injured)
If your goal is to work out more, the priority is often moving well enough to train consistently.
Many chiropractic resources emphasize mobility, flexibility, and injury prevention as people increase activity at the start of the year. 5280 Balanced Health Center+2Freedom Chiropractic+2 El Paso Back Clinic also emphasizes flexibility, mobility, and agility programs to improve ability and quality of life. El Paso Back Clinic® • 915-850-0900
A simple evidence-based target
For general health, adults are commonly advised to aim for 150 minutes of moderate activity per week, plus 2 days of muscle-strengthening activities. CDC+1 That can be split into smaller chunks—like 30 minutes, 5 days a week.
What the integrative plan can look like
Assess mobility limits (hips, spine, shoulders) and address movement friction
Build a realistic weekly schedule
Progress intensity slowly, so you don’t crash or flare
Easy “start small” movement ideas:
10–20 minute walk after meals
2 strength sessions per week (basic full-body)
5-minute mobility routine daily
Progression rules that keep people consistent:
Add time before you add intensity
Keep at least 1–2 recovery days weekly
Measure consistency, not perfection
2) Manage Pain So You Can Stay Active
Pain goals often work better when you focus on function—not “zero pain tomorrow.” A pain-focused plan might aim to reduce flare-ups and increase what you can do safely. National Spine & Pain Centers
El Paso Back Clinic positions its care around helping people with frustrating injuries and chronic pain syndromes improve mobility and function. El Paso Back Clinic® • 915-850-0900
Practical pain goals that tend to stick
“Walk 20 minutes, 4 days/week without a flare.”
“Lift twice/week with pain staying under a 3–4/10.”
NP-style wellness support can focus on sleep, stress, consistency in nutrition, and pacing habits that support recovery. Prism Health North Texas+1
Helpful pacing ideas (simple but powerful):
Use shorter workouts more often
Stop just before your “flare threshold”
Build capacity gradually rather than “weekend warrior” bursts
3) Boost Energy the Smart Way
Energy is not just “motivation.” If you’re tired, your plan needs better recovery.
Many chiropractic sources link better sleep and reduced tension with feeling more capable and consistent over time. gotcore.net+1 El Paso Back Clinic also describes a wellness-focused approach aimed at improving energy, sleep, and overall function. El Paso Back Clinic® • 915-850-0900
It’s common to hear people say they want to “boost immunity.” A safe and practical way to think about this is:
You can support overall wellness by improving sleep, physical activity, and stress management—foundations that matter for health.
Regular physical activity is widely recommended for health. CDC
Mindfulness-based approaches have evidence supporting their effectiveness for stress, sleep, and pain management. NIH News in Health
So instead of chasing extreme detoxes or perfect diets, an integrative plan often focuses on steady basics:
sleep routine
movement most days
nutrition consistency
stress skills
That’s the kind of “quiet consistency” that makes resolutions last.
5) Lower Stress and Improve Stress Response
Stress shows up in the body: tight shoulders, headaches, jaw tension, shallow breathing, gut tension, and poor sleep.
Mindfulness-based treatments have evidence supporting reduced anxiety/depression symptoms and improved sleep, and may help people cope with pain. NIH News in Health Many chiropractic sources also connect care with stress reduction and better sleep as part of overall wellness. gotcore.net+1
Pick one main goal (fitness OR pain, energy, OR stress)
Add two support habits
Track consistency weekly
Adjust every 2–4 weeks
Examples of “support habits”:
protein at breakfast
20-minute walk 4x/week
5 minutes of mobility daily
bedtime routine 5 nights/week
A Simple 4-Week Plan (El Paso Back Clinic Style: Practical, Not Perfect)
This is a general example you can personalize with your provider team.
Week 1: Reduce friction
Identify mobility limits and pain triggers
Set one realistic activity goal
Begin a simple nutrition and sleep routine
Week 2: Build consistency
Add a second strength or mobility day
Keep intensity moderate
Track sleep and energy patterns
Week 3: Progress carefully
Increase walking time or training volume slightly
Add a stress routine you can repeat
Adjust the plan based on how your body responds
Week 4: Lock in your system
Keep what’s working
Simplify what isn’t
Create a “busy week version,” so you don’t fall off
This approach fits the clinic’s overall theme of improving function through mobility, recovery, and whole-person planning. El Paso Back Clinic® • 915-850-0900+1
When to Get Checked Right Away
If you have severe or unusual symptoms, don’t “push through.” Seek urgent medical care for red flags like:
chest pain, severe shortness of breath, fainting
sudden weakness, facial droop, confusion
loss of bowel/bladder control
fever with severe spine pain
major trauma with worsening symptoms
Bottom Line: Your Best Results Come From a Whole Plan
At El Paso Back Clinic, an integrative model supports real-life resolutions by combining:
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine







:max_bytes(150000):strip_icc()/281448-grilled-chicken-fajitas-mfs-4-6c901272e8e34755bf0c5a535c8cb9fa.jpg)