For individuals dealing with newly formed or chronic lower back pain, can making daily walks a part of a weekly routine help relieve pain and discomfort symptoms and prevent strains and injuries?
Walking For Low Back Pain Relief
Walking is recommended to treat and prevent chronic or recurrent lower back pain. A study found that a personalized and progressive weekly walking program that builds up to 130 minutes of moderate intensity can significantly relieve severe lower back pain and prevent future flare-ups. (Pocovi N. C. et al., 2024) Walking is a cost-effective and easily accessible way to relieve lower back pain and prevent recurring or future injuries. It strengthens the back muscles, improves posture, and stabilizes the spine. (Suh JH, et al., 2019) Other benefits include improved overall physical health, posture, and circulation.
How Walking Helps
Walking for low back pain relief and general movement is better than not engaging in physical activities for individuals with recurrent lower back pain. Being sedentary can worsen back pain symptoms. (National Library of Medicine. 2019) Walking is second nature and is easy to incorporate into a weekly routine to help relieve back pain and improve overall health (Macquarie University, 2024)
Increases Spinal Flexibility
Walking and gentle movements increase the lower back’s functional range of motion, improve spinal flexibility, and reduce stiffness. (Smith J. A. et al., 2022)
Stabilizes Lumbar/Low Back Muscles
Walking builds muscle endurance and strength in the paraspinal muscles, increasing lumbar spinal stabilization. (Suh JH, et al., 2019)
Strengthens Core Muscles
Walking increases the body load and strengthens core muscles like the transversus abdominis, which lowers the risk of chronic lower back pain. (Lee J. S. and Kang S. J. 2016)
Improves Posture
Movement of the legs during walking enhances bodily awareness and helps correct posture.(Henry M. and Baudry S. 2019)
Increases Blood Circulation
Walking increases blood circulation to the muscles, supplying essential nutrients to spinal discs. It also reduces the frequency and severity of lower back muscle spasms. (Sitthipornvorakul E. et al., 2018)
Lubricates Spinal joints
Low-impact walking improves synovial fluid production and circulation, lubricating the lumbar spine’s facet joints and other joints that tend to get achy, such as the knees. (Zhang S. L. et al., 2013)
Relieves Inflammation
Walking helps reduce the presence of pro-inflammatory cytokines, like (IL-8 and TNF-alpha) associated with chronic lower back pain. (Slouma M. et al., 2023)
Promotes Weight Loss
Walking and a healthy diet can help individuals lose excess fat, which puts added strain on the lower back and correlates with lumbar intervertebral disc degeneration. (Wang M. et al., 2024)
Stress Relief
Regular walking can reduce mental stress associated with chronic lower back pain. (Choi S. et al., 2021)
Releases Endorphins
Moderate to vigorous physical activity, like walking at about 3 miles per hour for a half-hour daily, stimulates the release of endorphins, the body’s natural pain relievers. (Bruehl S. et al., 2020)
Walking Correctly
To get all the benefits of walking for low back pain relief, it is recommended to practice the following (Macquarie University, 2024)
Start slowly.
Gradually build intensity.
Stay consistent with the walking program.
Track progress to maintain motivation.
Healthcare Provider Consultation
Walking is a low-risk, low-impact activity well-tolerated by most individuals with nonspecific low back pain. (Pocovi N. C. et al., 2022) Because it doesn’t involve twisting or vigorous movements, it is considered a safe exercise for individuals with back pain symptoms (Gordon R. and Bloxham S. 2016). However, individuals experiencing severe lower back pain due to a traumatic injury or medical condition should consult a healthcare provider before starting a regular walking program.
Limit High Impact Activities
High-impact activities like running on hard surfaces or playing sports can exacerbate chronic lower back pain. If there is chronic lower back pain, it is recommended to limit activities that involve: (Al-Otaibi S. T. 2015)
Heavy lifting
Repetitive bending
Twisting motions
Injury Medical Chiropractic and Functional Medicine Clinic
Walking for low back pain relief. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Movement as Medicine
References
Pocovi, N. C., Lin, C. C., French, S. D., Graham, P. L., van Dongen, J. M., Latimer, J., Merom, D., Tiedemann, A., Maher, C. G., Clavisi, O., Tong, S. Y. K., & Hancock, M. J. (2024). Effectiveness and cost-effectiveness of an individualised, progressive walking and education intervention for the prevention of low back pain recurrence in Australia (WalkBack): a randomised controlled trial. Lancet (London, England), 404(10448), 134–144. https://doi.org/10.1016/S0140-6736(24)00755-4
Suh, J. H., Kim, H., Jung, G. P., Ko, J. Y., & Ryu, J. S. (2019). The effect of lumbar stabilization and walking exercises on chronic low back pain: A randomized controlled trial. Medicine, 98(26), e16173. https://doi.org/10.1097/MD.0000000000016173
National Library of Medicine., & InformedHealth.org [Internet]. Cologne, G. I. f. Q. a. E. i. H. C. I. (2022). Low back pain: Learn More – Why movement is so important for back pain. https://www.ncbi.nlm.nih.gov/books/NBK284944/
Macquarie University. (2024). Macquarie University. Walking to combat back pain: world-first study shows dramatic improvement. https://lighthouse.mq.edu.au/article/june-2024/walking-away-from-pain-world-first-study-shows-dramatic-improvement-in-lower-back-trouble
Smith, J. A., Stabbert, H., Bagwell, J. J., Teng, H. L., Wade, V., & Lee, S. P. (2022). Do people with low back pain walk differently? A systematic review and meta-analysis. Journal of sport and health science, 11(4), 450–465. https://doi.org/10.1016/j.jshs.2022.02.001
Suh, J. H., Kim, H., Jung, G. P., Ko, J. Y., & Ryu, J. S. (2019). The effect of lumbar stabilization and walking exercises on chronic low back pain: A randomized controlled trial. Medicine, 98(26), e16173. https://doi.org/10.1097/MD.0000000000016173
Lee, J. S., & Kang, S. J. (2016). The effects of strength exercise and walking on lumbar function, pain level, and body composition in chronic back pain patients. Journal of exercise rehabilitation, 12(5), 463–470. https://doi.org/10.12965/jer.1632650.325
Henry, M., & Baudry, S. (2019). Age-related changes in leg proprioception: implications for postural control. Journal of neurophysiology, 122(2), 525–538. https://doi.org/10.1152/jn.00067.2019
Sitthipornvorakul, E., Klinsophon, T., Sihawong, R., & Janwantanakul, P. (2018). The effects of walking intervention in patients with chronic low back pain: A meta-analysis of randomized controlled trials. Musculoskeletal science & practice, 34, 38–46. https://doi.org/10.1016/j.msksp.2017.12.003
Zhang, S. L., Liu, H. Q., Xu, X. Z., Zhi, J., Geng, J. J., & Chen, J. (2013). Effects of exercise therapy on knee joint function and synovial fluid cytokine levels in patients with knee osteoarthritis. Molecular medicine reports, 7(1), 183–186. https://doi.org/10.3892/mmr.2012.1168
Slouma, M., Kharrat, L., Tezegdenti, A., Metoui, L., Ghazouani, E., Dhahri, R., Gharsallah, I., & Louzir, B. (2023). Pro-inflammatory cytokines in patients with low back pain: A comparative study. Reumatologia clinica, 19(5), 244–248. https://doi.org/10.1016/j.reumae.2022.07.002
Wang, M., Yuan, H., Lei, F., Zhang, S., Jiang, L., Yan, J., & Feng, D. (2024). Abdominal Fat is a Reliable Indicator of Lumbar Intervertebral Disc Degeneration than Body Mass Index. World neurosurgery, 182, e171–e177. https://doi.org/10.1016/j.wneu.2023.11.066
Choi, S., Nah, S., Jang, H. D., Moon, J. E., & Han, S. (2021). Association between chronic low back pain and degree of stress: a nationwide cross-sectional study. Scientific reports, 11(1), 14549. https://doi.org/10.1038/s41598-021-94001-1
Bruehl, S., Burns, J. W., Koltyn, K., Gupta, R., Buvanendran, A., Edwards, D., Chont, M., Wu, Y. H., Qu’d, D., & Stone, A. (2020). Are endogenous opioid mechanisms involved in the effects of aerobic exercise training on chronic low back pain? A randomized controlled trial. Pain, 161(12), 2887–2897. https://doi.org/10.1097/j.pain.0000000000001969
Pocovi, N. C., de Campos, T. F., Christine Lin, C. W., Merom, D., Tiedemann, A., & Hancock, M. J. (2022). Walking, Cycling, and Swimming for Nonspecific Low Back Pain: A Systematic Review With Meta-analysis. The Journal of orthopaedic and sports physical therapy, 52(2), 85–99. https://doi.org/10.2519/jospt.2022.10612
Gordon, R., & Bloxham, S. (2016). A Systematic Review of the Effects of Exercise and Physical Activity on Non-Specific Chronic Low Back Pain. Healthcare (Basel, Switzerland), 4(2), 22. https://doi.org/10.3390/healthcare4020022
Al-Otaibi S. T. (2015). Prevention of occupational Back Pain. Journal of family & community medicine, 22(2), 73–77. https://doi.org/10.4103/2230-8229.155370
For many individuals, getting on the floor to do crunches or other exercises can be difficult due to medical conditions, age, and injuries. Can engaging in chair abdominal exercises at home, work, or anywhere a chair is available help strengthen the upper, lower, and oblique abdominal muscles?
Chair Abdominal Exercises
Chair abdominal exercises are essential for strengthening the core, maintaining healthy flexibility, mobility, posture, and injury prevention. Incorporating abdominal exercise into one’s day can be easy, regardless of schedule or fitness level. Various exercises are designed to be performed while seated, making them accessible to everyone, including those with mobility issues or new to exercise.
Benefits
Building and maintaining a solid core is essential for overall health, posture, and daily activities, especially as the body ages. A strong core maintains body balance and stability, prevents falls, protects individuals from back pain, and makes lifting, bending, and walking easier. It allows individuals to stay independent and active. The abdominal muscles are one part of the core, which includes muscles in the back, glutes, pelvic floor, and diaphragm. These are important for keeping the body upright and stable, protecting the spine and organs, and assisting with movements between the ribcage and pelvis. Adding abdominal exercise workouts to a fitness routine is one way to improve overall core strength and stability. Chair-based exercises are convenient and accessible as individuals don’t need specialized machines or equipment, just a sturdy chair and some space. (Frizziero A. et al., 2021)
Chair Workout
Chair abdominal exercises are ideal gentle exercises for older individuals who need to increase their strength and mobility. Because chairs provide stability and safety, these exercises focus on seated movements and are intended for those with limited mobility. Chair abdominal exercises can be adapted and modified to individual preferences and needs, preparing the body for more advanced standing exercises. They improve the ability to perform daily tasks and increase joint mobility, muscle strength, and coordination. To prevent injuries, each exercise session should begin with a warm-up and end with a cool-down.
A warm-up could be gentle seated marches, shoulder rolls, and deep breathing exercises.
A cool-down can include seated stretches, focusing on the back, neck, and legs to help the body recover and prevent stiffness.
It is recommended that patients talk to a healthcare provider first if they have limited mobility or chronic health issues. Here are some sample exercises.
Sitting Knee Lifts
Sit on the edge of the chair with your back straight.
Lift your knees toward your chest, engaging the upper abs.
Lower them slowly back down.
Repeat for 10 to 15 reps.
Beginners lift one knee at a time.
Lower it and repeat with the other leg.
Sitting Crunches
Sit on the edge of the chair.
Lean back slightly.
Place hands behind your head.
Crunch forward, bringing the chest toward your knees.
Return to the starting position.
Repeat for 10 to 15 reps.
Beginners can sit more on the chair and hold the seat for stability.
Reduce the range of motion when crunching the chest toward the knees.
Sitting Leg Lifts
Sit on the edge of the chair with the back straight.
Extend your legs in front of you and lift them together, engaging the lower abdominals.
Lower them back down slowly.
Repeat for 10 to 15 repetitions.
Beginners sit back on the chair and grip the sides.
Lift one leg and hold for a count before lowering.
Switch legs.
Sitting Scissor Kicks
Sit on the edge of the chair and lean back slightly.
Extend your legs in front.
Alternate lifting each leg up and down in a scissor motion.
Perform for 30 seconds to one minute.
Beginners tap one heel on the floor between lifts to reduce abdominal tension.
Sitting Side Crunches
Sit on the edge of the chair with the back straight.
Lift one knee toward the chest while bringing the opposite elbow toward the knee, engaging the obliques.
Alternate for 10 to 15 reps per side.
Beginners, keep your feet flat on the floor with your hands behind your head.
Gently bend to the side, return to the center, and bend to the other side.
Sitting Bicycle Crunches
Sit on the edge of the chair and lean back slightly.
Lift the feet off the ground.
Alternate bringing each knee toward the opposite elbow in a pedaling motion.
Perform for 30 seconds to one minute.
For beginners, keep the heel gently on the ground while you crunch on the opposite side.
For a challenge, slow the motion and hold each twist a few seconds longer to create more tension. (Krzysztofik M. et al., 2019)
Progress
For beginners, start with the easier versions and perform fewer repetitions and shorter durations if needed. Focus on maintaining proper posture and form. As the body gets stronger, increase the number of repetitions or extend the duration of each exercise. Once comfortable, try more challenging chair exercises. Chair abdominal exercises are a simple, effective way to strengthen the core, improve posture, and support overall health. Regularly doing these exercises as part of a well-rounded routine can build a solid core without special equipment. Remember to listen to the body and progress at your own pace to more challenging variations over time to keep building strength.
Injury Medical Chiropractic and Functional Medicine Clinic
Achieving and maintaining fitness requires consistent work and development. Retraining the body and maintaining its optimal health requires daily efforts through exercise. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Core Exercises and Back Pain
References
Frizziero, A., Pellizzon, G., Vittadini, F., Bigliardi, D., & Costantino, C. (2021). Efficacy of Core Stability in Non-Specific Chronic Low Back Pain. Journal of functional morphology and kinesiology, 6(2), 37. https://doi.org/10.3390/jfmk6020037
Krzysztofik, M., Wilk, M., Wojdała, G., & Gołaś, A. (2019). Maximizing Muscle Hypertrophy: A Systematic Review of Advanced Resistance Training Techniques and Methods. International journal of environmental research and public health, 16(24), 4897. https://doi.org/10.3390/ijerph16244897
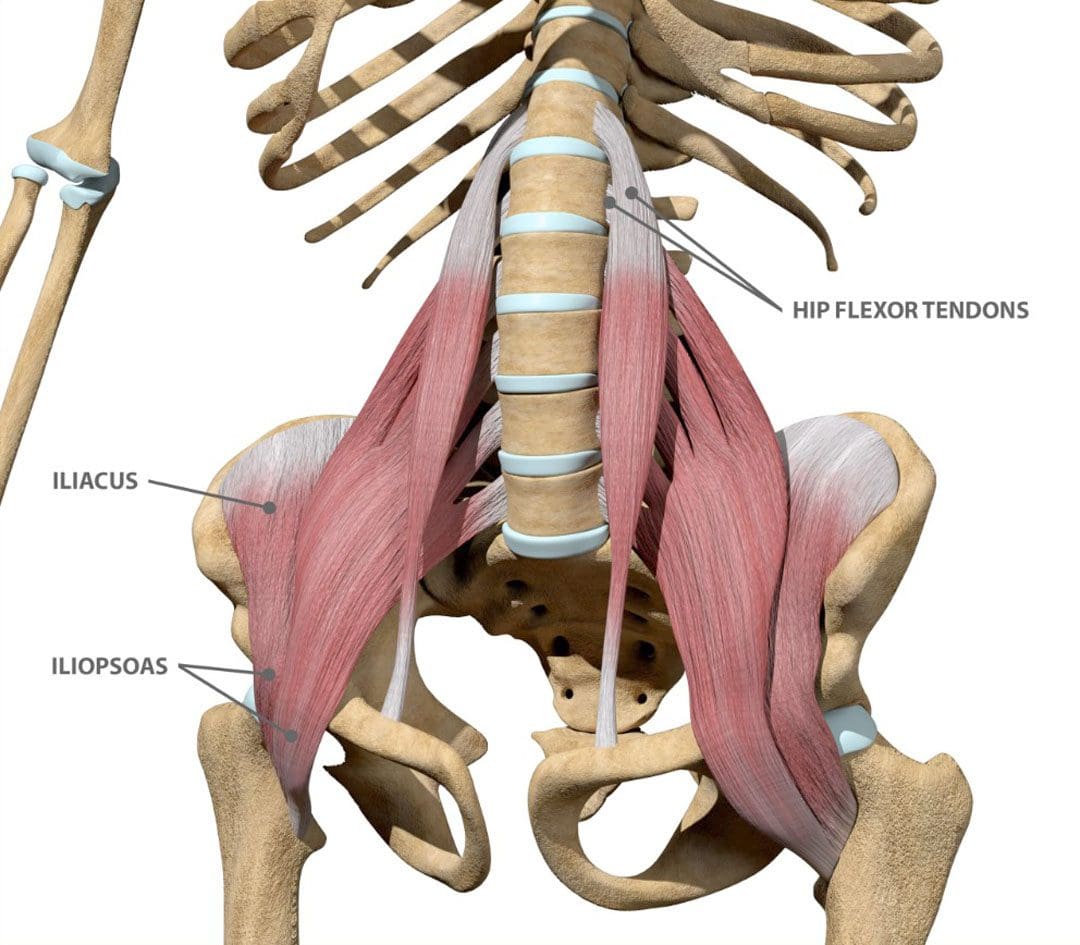
The iliacus muscle is a triangle-shaped muscle in the pelvic bone that flexes and rotates the thigh bone. It works with the other muscles in the hip and thigh to help bend, run, walk, sit, and maintain correct posture. Injuries and common medical conditions can affect its function, causing pain and stiffness. Can physical therapy help?
The Iliacus Muscle
The iliacus is one of the body’s most important hip flexor muscles. The iliacus and surrounding muscles work together to produce the stability and range of motion required for bending, dancing, sitting, and walking.
Anatomy
The iliacus muscle is part of a complex muscle system in the hip and pelvis. Two iliacus muscles on each side of the pelvic bone enable the thigh to flex and rotate. They are innervated by the femoral nerve, which provides movement and sensation to the lower limbs. (Bordoni B. and Varacallo M. 2023) The iliacus muscle sits on the wing-shaped ilium and fits into the curved surface of the ilium, called the iliac fossa. The top of the muscle is attached to the upper wings of the ilium or iliac crest. It extends past the hip joint, which connects to the upper thigh bone/femur at the lesser trochanter protrusion. The iliacus is part of a major trio of muscles called the iliopsoas, including the major psoas and minor psoas muscles. These muscles are also attached to the upper femur but extend upward, connecting to the lumbar/lower spine at several attachment points. The iliopsoas also interact with the quadratus lumborum muscle, the deepest muscle of the lower back that starts at the iliac crest and attaches to the lumbar spine at several points. The quadratus lumborum enables flexion and elevation of the spine, while the iliopsoas enable the flexion and rotation of the hip and thigh.
Functions
The iliacus muscle has many functions that include: (Physiopedia, 2024)
Flexing and rotating the femur.
Helps maintain proper body posture while standing and sitting.
Produces hip movement that enables walking, running, and climbing stairs.
Provides hip flexion – bringing the knee to the chest.
Enables the forward tilt of the pelvis and side-bending.
Conditions
Several conditions can affect the iliacus muscle, specifically from under and/or overuse injuries. These conditions, collectively known as Iliopsoas syndrome, are typically the result of overuse/repetitive strain or injuries. These include:
Iliopsoas tendinopathy – which affects tendons.
Iliopsoas bursitis – which affects cushioning sacs known as bursae.
Iliopsoas syndrome can affect anyone but is common in:
Individuals and athletes who repeatedly use movements that flex the hips.
Track-and-field athletes
Gymnasts
Dancers
Iliopsoas Bursitis
This is the inflammation of the cushioning sac or bursa under the iliacus muscle, which helps the muscle slide over the pelvic bone. Symptoms can range from mild discomfort to pain that radiates through parts of the leg and hips. Runners, skiers, and swimmers are commonly affected, and individuals who regularly have tight hips and individuals with different forms of arthritis can also be affected. Early treatment can prevent the symptoms from worsening. Mild cases can be treated with self-care and stretching to help relieve tightness, rest, ice application, and over-the-counter nonsteroidal anti-inflammatory drugs. In severe cases, treatment options that may be recommended include: (Physiopedia, 2024)
Physical therapy
Assistant walking devices to relieve pressure – for example, a cane.
Corticosteroid steroid injections
Prescription anti-inflammatory medications
Iliopsoas Tendinopathy
Another condition affecting the iliacus muscles is iliopsoas tendinopathy, sometimes called snapping hip syndrome, because individuals can hear an audible snapping sound (Davenport KL. 2019). The condition is often experienced by dancers who repeatedly flex and hyperextend their hips and can result in hip and groin pain that gets worse with kicking or rotation. Treatment of iliopsoas tendinopathy can include:
Retraining muscle imbalances with strengthening and stretching exercises.
If these fail to provide relief, corticosteroid injections may be used. A saline hydro dissection can relieve stress around the tendon by injecting fluids that cushion and release trapped tissues.
Tendon release surgery may be recommended when all other options have failed. The surgical release involves severing the tendon to reduce pain and improve the range of motion.
Rehabilitation
Core muscle strengthening is essential to the rehabilitation of iliacus muscle injuries. The iliopsoas is an integral component of the core group and can benefit from stretching and strengthening exercises (Yogateket, 2019)
Lunge stretches
Straight leg raises
Knee-to-chest stretches
Standing hip flexion with resistance bands
Certain yoga poses can also help and include variations on the bridge pose that encourage hip flexion. (Yoga International, 2024)
Injury Medical Chiropractic and Functional Medicine Clinic
Iliopsoas pain is often felt at the front of the hips, thigh, mid-back, and lower back. Chiropractic care can help with iliacus muscle injuries through:
Evaluation
A chiropractor can evaluate the condition and determine if the iliacus muscle is causing pain.
Treatment plan
A chiropractor can create a personalized treatment plan that may include exercise instructions, manipulation, and other therapies.
Rehabilitation
A chiropractor can create a rehabilitation program to expedite healing.
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Hip Labral Tear and Chiropractic Care
References
Bordoni, B., & Varacallo, M. (2024). Anatomy, Bony Pelvis, and Lower Limb, Iliopsoas Muscle. In StatPearls. https://www.ncbi.nlm.nih.gov/pubmed/30285403
Davenport KL. (2019). The professional dancer’s hip. Performing Arts Medicine, 77-87. https://doi.org/https://doi.org/10.1016/B978-0-323-58182-0.00009-2
Yogateket. Lizette Pompa. (2019). Essential yoga body parts. Hip flexor/psoas and yoga. Yogateket. https://www.yogateket.com/blog/hip-flexor-psoas-and-yoga
Incorrect manual handling and lifting is a leading cause of workplace injuries. Can health and safety training help reduce injuries and lost workdays?
Correct Manual Lifting Technique
Manually lifting objects using incorrect techniques can lead to acute back injuries, herniated discs, sciatica, and long-term issues like increased risk of reinjury, body misalignment, and chronic back pain. Individuals can prevent spinal disc compression and/or lower back muscle strain by learning to use correct manual lifting techniques. (CDC. The National Institute for Occupational Safety and Health (NIOSH). 2007)
Lifting Guide
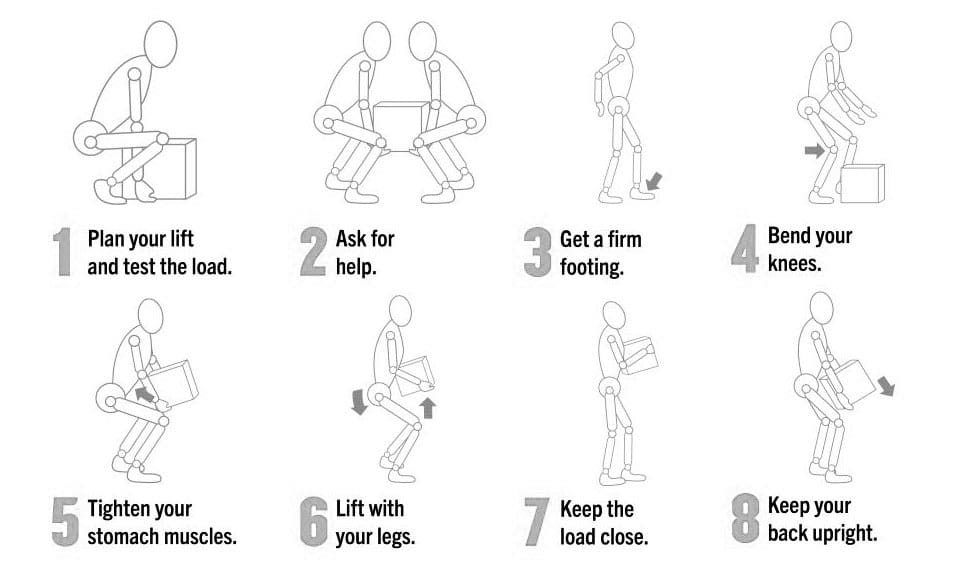
Individuals can protect their backs and prevent injury by following simple steps when lifting objects.
Support Base
Ensure there is a healthy support base from which to lift.
Keep feet shoulder-width apart with one foot slightly in front of the other.
Ask For Help
If coworkers or colleagues are available, ask for assistance.
If the load is too heavy, ask for help lifting and moving the object/s.
Use Mechanical Assistant Devices
Use hand trucks, dollies, or pushcarts whenever possible for uneven and heavy loads.
Squat To Lift Object
Bend at the hips and knees only, not the back.
Put one knee on the ground to ensure stability before lifting.
Check Posture
Looking straight ahead, maintain posture upright with the chest out, shoulders back, and lower back slightly arched.
Lift Slowly
Lift with the knees and hips only, gradually straightening the lower back.
Load Positioning
Once upright, hold the load close to the body around the stomach.
Move and Maintain Alertness
Always take small steps.
Maintain alertness as to where you are going.
Keep the shoulders square with the hips when changing directions to avoid twisting and losing or shifting balance.
Rest
If you are fatigued, set the load/object down and rest for a few minutes until you can fully engage in the task.
Squat To Set Object Down
Squat with the knees and hips and set the load down slowly.
Avoid quickly rising and jerking movements, and allow the legs, hips, and back muscles to reset.
Planning and Tips
Lifting anything heavy takes planning to prevent muscle spasms, back strain, and other musculoskeletal injuries. Considerations to keep in mind:
Make a Plan Before Lifting
Knowing what object/s are being lifted and where they are going will prevent individuals from making awkward movements while holding and carrying something heavy.
Set and clear a path.
If lifting something with another person, ensure both agree and understand the plan.
Lift Close to The Body
Individuals are stronger and more stable lifters if the object is held close to their body rather than at the end of their reach.
Make sure there is a firm hold on the object.
It is easier to maintain balance close to the body.
Maintain Feet Shoulder-Width Apart
Keep the feet about shoulder-width apart.
Having a solid base of support is important while lifting.
Placing the feet too close together will cause instability while placing them too far apart will hinder movement.
Take short steps.
Visualize The Motions Involved and Practice The Motions Before Lifting
Think about the motion before lifting.
Practice the lifting motion before lifting the object.
Focus on keeping the spine straight.
Raise and lower to the ground by bending the knees.
Avoid bending at the waist or hips.
Tighten the Stomach Muscles
Tightening the abdominal muscles will hold the back in a healthy lifting position and help prevent excessive force on the spine.
Lift With the Legs
The legs are stronger than the back muscles, so let the leg strength do the work.
Lower yourself to the ground by bending the knees, not the back.
Keep Eyes Up
Looking slightly upwards will help maintain a better spine position and help keep the back straight.
Avoid Twisting or Bending
Face in the direction you are walking.
Stop, take small steps, and continue walking if turning is required.
Back Belts
It has become common for many who work in jobs requiring manual lifting to wear back belts or support. However, research does not show that they decrease the risk of a lifting injury. (CDC and The National Institute for Occupational Safety and Health, 2023) Instead, it is recommended that the belt be thought of as a reminder of where the back muscles are positioned to keep the individual aligned, combined with the correct lifting techniques.
Injury Medical Chiropractic and Functional Medicine Clinic
Training the body and maintaining its optimal health for correct manual lifting techniques requires daily efforts through practice, conscious position corrections, and ergonomics. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Chiropractic Care For Injury Recovery
References
CDC. The National Institute for Occupational Safety and Health (NIOSH). (2007). Ergonomic Guidelines for Manual Material Handling. (No. 2007-131). Retrieved from https://www.cdc.gov/niosh/docs/2007-131/pdfs/2007-131.pdf
CDC. The National Institute for Occupational Safety and Health (NIOSH) (2023). Back Belts – Do They Prevent Injury? (No. 94-127). Retrieved from https://www.cdc.gov/niosh/docs/94-127/
How is fat turned into energy to be used as fuel for individuals working to improve their health and physical abilities?
Fat Into Energy Conversion
Fat is an essential component of a diet that fuels physical activity, work, exercise, etc. Its calorie density is the highest of all nutrients, and fat’s unlimited storage capacity makes it the body’s largest energy reserve. Fat is essential for longer, slower, lower-intensity endurance physical activities and exercises like walking and cycling.
What Is Fat?
Everything eaten is made up of:
Macronutrients
Protein
Carbohydrates
Fat
Micronutrients
Vitamins
Minerals
These are converted to energy, helping to fuel all bodily functions.
Dietary fat has been blamed for various health problems, but it is an essential nutrient for optimal health. The adipose tissue/stored fat provides cushion and insulation to internal organs, protects nerves, circulates vitamins A, D, E, and K through the body, and is the largest stored energy reserve. Stored body fat is different from dietary fat. Body fat is only stored when more calories are consumed than used from all foods, not just from dietary fats. There is an optimal level of body fat for health and regular physical and athletic activity.
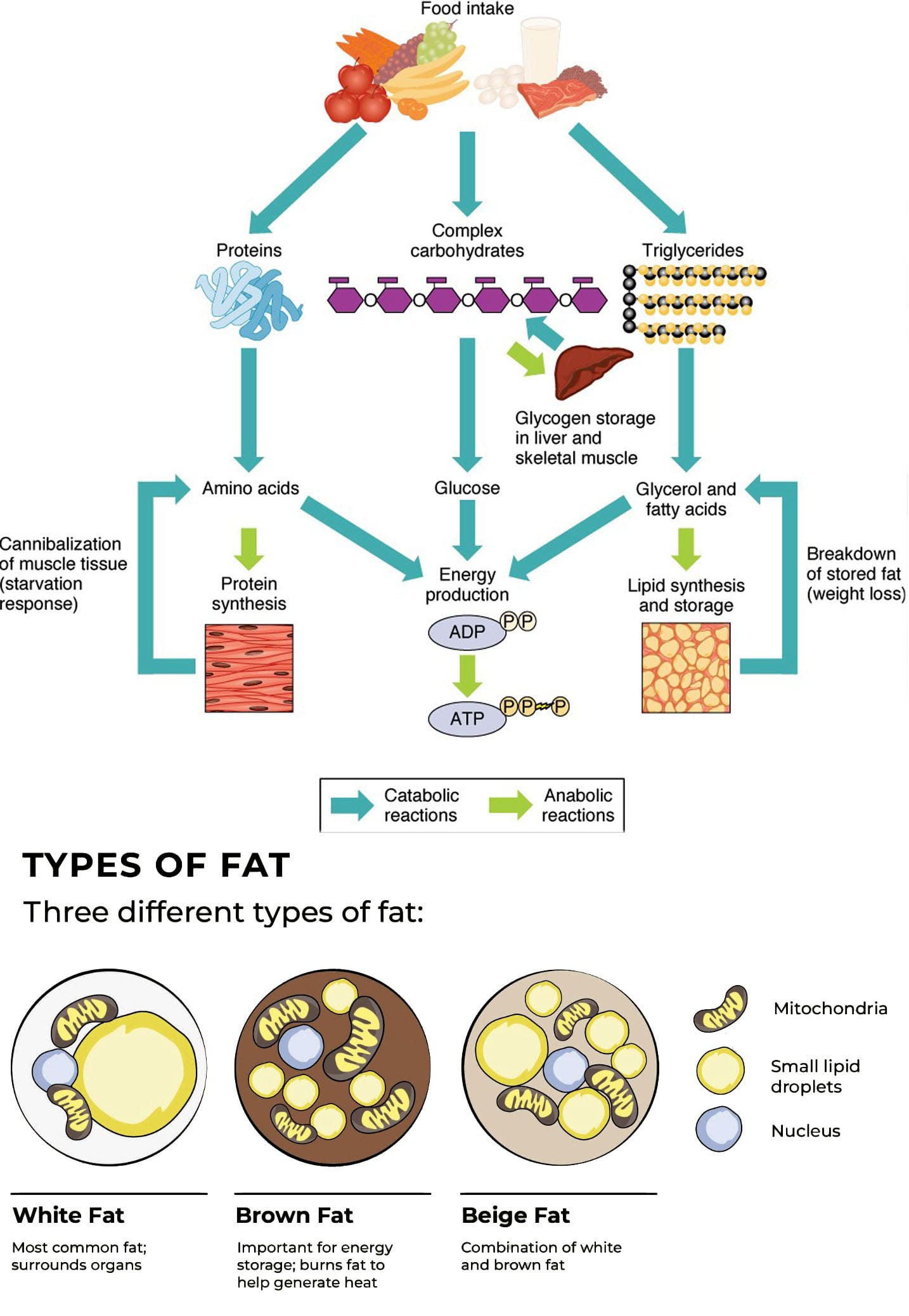
Types
Researchers and scientists are learning more and more about body fat/adipose tissue and its roles in the body. Two well-known types are white fat and brown fat.
White fat is responsible for energy storage and metabolic functions like insulin sensitivity.
White fat can transition to brown fat under certain cold temperatures. (Rabiee A. 2020)
Beige fat is another type that scientists are still learning about.
When Fat Is Burned
When fat is used as fuel, the fatty acids inside the fat cell are broken down and released into the system as water and carbon dioxide. (MacLean P. S. et al., 2015) The body uses the water for hydration, and the carbon dioxide is exhaled through the lungs. The remaining fat cell shrinks as it is depleted of its fatty acids. The fat into energy conversion also produces heat.
Fat for Fuel
Fat is the main fuel source for long-duration, low—to moderate-intensity physical activities and exercise like endurance sports. Even during high-intensity activities and training, where carbohydrates are the main fuel source, the body still needs fat to help access the stored carbohydrates or glycogen. Using fat to fuel activity includes three key components which include:
Digestion
Fat is slow to digest and convert into a usable form of energy.
The process can take up to six hours.
Transportation
After the body breaks down the fat, it needs time to transport it to the working muscles before it can be used as energy.
Conversion
Converting stored body fat into energy takes increased oxygen, requiring decreased physical activity and exercise intensity.
This is why timing when and how much fat is consumed is important for its full potential. Eating foods high in fat immediately before or during intense physical work activity or exercise is not recommended. First, the job, chore, or workout will be done before the fat can be used as energy. And second, it can cause uncomfortable gastrointestinal symptoms like nausea, vomiting, and diarrhea.
Fat Loss Optimization
For individuals trying to alter body fat composition, the most important thing is to adopt a safe and effective physical activity and exercise routine and to eat a balanced diet of nutrient-dense foods that provide adequate amounts of macronutrients, including dietary fat.
Macronutrient
Low-carbohydrate and high-fat diets, like the ketogenic and Paleo diets, all work on the same premise: Lower carbohydrate intake, high fat intake, and moderate to high protein intake lead to burning body fat as the primary fuel source while engaging in physical activity or exercising. There is some scientific evidence that long-term low-carb/high-fat diets are safe and may help improve metabolic risk factors for chronic disease. Some studies on these diets have shown them to be beneficial for performance in endurance sports, but several months of adaptation to a low-carb/high-fat diet are required for metabolic changes to occur. (Chang C. K., Borer K., and Lin P. J. 2017))
High-Intensity Interval Training
High-intensity interval training is an efficient way to convert fat to energy. In a study, overweight individuals were able to convert body fat to energy in half the time using HIIT vs. aerobic activity alone (Zhang H. et al., 2017). HIIT specifically converts visceral fat, typically white adipose tissue, often found in the midsection. (Mittal B. 2019) HIIT also helps increase muscle mass and resting metabolism. (Thyfault J. P. and Bergouignan A. 2020) However, any exercise regimen that helps increase muscle mass provides these beneficial effects.
Injury Medical Chiropractic and Functional Medicine Clinic
At Injury Medical Chiropractic and Functional Medicine Clinic, we focus on what works for you to relieve pain, restore function, prevent injury, and better the body. Through research methods and total wellness programs, individuals can condition themselves to excel in physical activity or sports through proper fitness and nutrition. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Integrative Medicine and Chiropractic Care
References
Richard, A. J., White, U., Elks, C. M., & Stephens, J. M. (2000). Adipose Tissue: Physiology to Metabolic Dysfunction. In K. R. Feingold, B. Anawalt, M. R. Blackman, A. Boyce, G. Chrousos, E. Corpas, W. W. de Herder, K. Dhatariya, K. Dungan, J. Hofland, S. Kalra, G. Kaltsas, N. Kapoor, C. Koch, P. Kopp, M. Korbonits, C. S. Kovacs, W. Kuohung, B. Laferrere, M. Levy, E. A. McGee, R. McLachlan, M. New, J. Purnell, R. Sahay, A. S. Shah, F. Singer, M. A. Sperling, C. A. Stratakis, D. L. Trence, & D. P. Wilson (Eds.), Endotext. https://www.ncbi.nlm.nih.gov/pubmed/32255578
Rabiee A. (2020). Beige Fat Maintenance; Toward a Sustained Metabolic Health. Frontiers in endocrinology, 11, 634. https://doi.org/10.3389/fendo.2020.00634
MacLean, P. S., Higgins, J. A., Giles, E. D., Sherk, V. D., & Jackman, M. R. (2015). The role for adipose tissue in weight regain after weight loss. Obesity reviews : an official journal of the International Association for the Study of Obesity, 16 Suppl 1(Suppl 1), 45–54. https://doi.org/10.1111/obr.12255
Chang, C. K., Borer, K., & Lin, P. J. (2017). Low-Carbohydrate-High-Fat Diet: Can it Help Exercise Performance?. Journal of human kinetics, 56, 81–92. https://doi.org/10.1515/hukin-2017-0025
Zhang, H., Tong, T. K., Qiu, W., Zhang, X., Zhou, S., Liu, Y., & He, Y. (2017). Comparable Effects of High-Intensity Interval Training and Prolonged Continuous Exercise Training on Abdominal Visceral Fat Reduction in Obese Young Women. Journal of diabetes research, 2017, 5071740. https://doi.org/10.1155/2017/5071740
Mittal B. (2019). Subcutaneous adipose tissue & visceral adipose tissue. The Indian journal of medical research, 149(5), 571–573. https://doi.org/10.4103/ijmr.IJMR_1910_18
Thyfault, J. P., & Bergouignan, A. (2020). Exercise and metabolic health: beyond skeletal muscle. Diabetologia, 63(8), 1464–1474. https://doi.org/10.1007/s00125-020-05177-6
Can correcting body misalignments and the elements of unhealthy posture help achieve a healthy posture?
Healthy Posture
Maintaining a healthy posture is more important than ever, as individuals from all walks of life realize how practicing awkward and unhealthy postures can wreak havoc on their bodies and quality of life. Unhealthy postures include rounding the upper and lower back, slouching, and forward head posture. Over time, these postures make daily activities more difficult or painful. Mobility, stability, and strengthening exercises can address unhealthy posture problems and issues, along with practicing correct sitting, standing, and resting postural habits to reinforce proper alignment daily. A chiropractic and physical therapy team can treat and train individuals to restore correct and healthy posture.
Body Alignment
Ideal posture involves correct body alignment or how the structural parts, such as the head, trunk, hips, knees, etc., relate to an individual’s form. Whether standing, sitting, lying down, or moving, body parts need to be balanced in relationship to each other to avoid unnecessary stress on the spine and musculoskeletal system. (Bone Health & Osteoporosis Foundation, 2024)
Posture Types
Posture is considered static when sitting or standing still and dynamic when moving. Both are categorized as active postures as they require the activation of stabilizing muscles to deal with gravity and maintain alignment. Lying down and remaining still is considered an inactive posture, as muscle involvement is minimal. However, both have the potential to be healthy or unhealthy.
Proper Body Alignment
An easy way to check proper alignment while standing is to stand against a wall with the base of the head, shoulder blades, and buttocks flush against the wall, with enough space for a hand wide enough to slide in between the wall and the small of the back. This exercise correctly lines up the head, shoulders, and hips to reduce or eliminate undue stress on the spine. Body balance is the foundation for active and inactive postures concerning workstations, industrial ergonomics, daily activities, and sports. (Mayo Clinic, 2023) Healthy alignment is a standard position in which all body joints are centered and balanced and the most mechanically efficient position for static or dynamic activities. Biomechanical efficiency (the ability to use the body’s muscles and joints to perform movements while minimizing energy use and maximizing output) enables the muscles surrounding the joints to work in balance and efficiently activate, which, in turn, helps reduce strain, tension, and injury. Balanced muscles also conserve energy, leading to better daily stamina.
Development of Imbalances
Individuals develop position and movement habits in joint positioning that have led to imbalanced muscles. When this is the case, some muscles can be chronically stretched, and others become chronically tight, all to hold the body up or move around, which can lead to postural conditions like upper crossed (Physiopedia, 2024) or lower crossed syndrome (Physiopedia, 2024) which often leads to pain and/or mobility issues.
Posture Assessment
The recommended way to determine if one’s posture is healthy or poor is by conducting a posture assessment. The examination looks at joint positions and gathers visual information about the planes into which parts of each joint move and the axes around which those movements occur (Singla D. and Veqar Z., 2014) (Debra Coglianese et al., 2006). In a posture assessment, body alignment is compared with the ideal standard, a plumb line, usually a string with a small weight attached to the bottom to help maintain straightness. The other end of the string is affixed to the ceiling to be used as an accurate reference for correct alignment. (Singla D. and Veqar Z. 2014) During a posture assessment, the patient stands next to the plumb line while the doctor or therapist compares the relative positions of the following areas:
Ears
Shoulder joint
Spine
Hip joint
Knee joint
Ankle joint
Feet
Any areas that don’t match the reference can indicate misalignments in one or several regions.
Making Corrections
Chiropractic care can help correct unhealthy posture by realigning the spine and strengthening the musculoskeletal system:
Spinal Adjustments
Chiropractors use their hands or instruments to apply controlled force to the spine to realign the vertebrae. This can help relieve pressure on muscles, ligaments, and nerves, which can improve posture.
Corrective Exercises
Chiropractors can create custom exercises to strengthen postural muscles and maintain proper alignment.
Massage Therapy
Chiropractors can use massage therapy to work on strained ligaments and soft tissue.
Guidance and Training
Chiropractors can teach patients how to move to encourage a neutral spine and provide strategies for maintaining healthy posture.
A posture corrector or brace can also help teach and engage the correct muscles to achieve proper alignment. However, it should not be relied on long-term because promoting and activating one’s stabilizing muscles is important rather than relying on a brace for prolonged periods.
Injury Medical Chiropractic and Functional Medicine Clinic
Achieving and maintaining proper posture requires consistent work and development. Retraining the body and maintaining its optimal health requires daily efforts through exercise, conscious position corrections, and ergonomics. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Upper Cross Syndrome
References
Bone Health & Osteoporosis Foundation. (2024). Proper body alignment. https://www.bonehealthandosteoporosis.org/patients/treatment/exercisesafe-movement/proper-body-alignment/
Mayo Clinic. (2023). Mayo Clinic Q and A: Proper posture and body alignment. https://newsnetwork.mayoclinic.org/discussion/mayo-clinic-q-and-a-proper-posture-and-body-alignment/
Singla, D., & Veqar, Z. (2014). Methods of postural assessment used for sports persons. Journal of clinical and diagnostic research: JCDR, 8(4), LE01–LE4. https://doi.org/10.7860/JCDR/2014/6836.4266
Coglianese, D. (2006). Muscles: Testing and Function With Posture and Pain, ed 5 (with Primal Anatomy CD-ROM). Physical Therapy, 86(2), 304-305. https://doi.org/https://doi.org/10.1093/ptj/86.2.304
An axillary nerve injury can cause pain, weakness, and shoulder mobility loss. Can physical therapy help restore and maintain shoulder joint flexibility?
Axillary Nerve
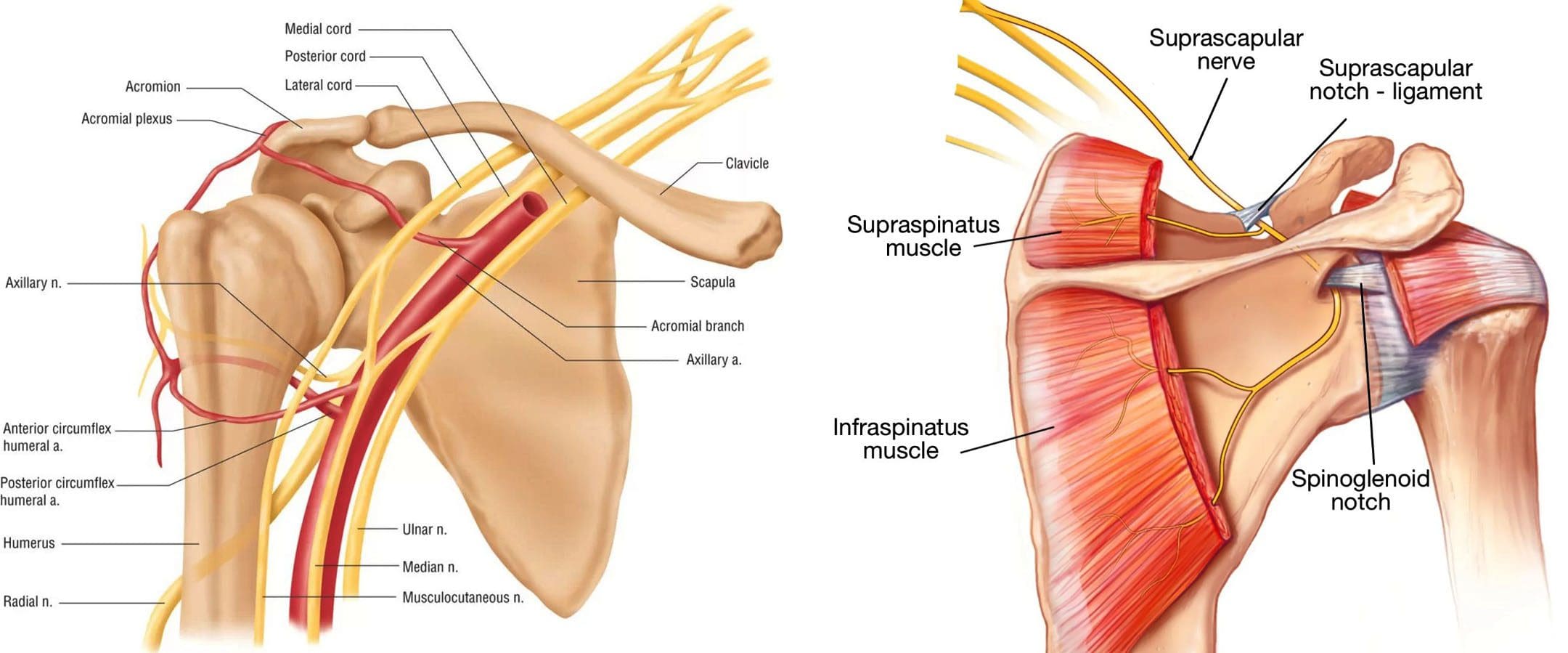
The axillary nerve, or the circumflex nerve, is a peripheral nerve that runs through the shoulder and supports movement and sensation in the upper limbs. It originates in the neck at the brachial plexus, a network of nerves that extends from the neck and upper torso to the shoulders and arms. Its primary purpose is to supply nerve function to the shoulder joint and three muscles in the arm and also innervates some skin in the region.
Anatomy
Except for the cranial nerves, all the body’s nerves branch off from the spinal cord, emerge from between vertebrae and continue to branch off as they travel to various muscles and other structures. The axillary nerve is named after the axilla, the medical name for the armpit. Individuals have two, one on each side. After leaving the spinal column, the axillary nerve runs behind the axillary artery and continues to the shoulder blade’s lower edge of the subscapularis muscle. It winds back and travels down the arm along the posterior humeral circumflex artery, which then passes through the quadrangular space (a small area of the shoulder blade just above the armpit where there is a gap in the muscles that allows nerves and blood vessels to pass through to the arm before it divides into terminal branches, which are:
Anterior Division
Supplies motor innervation to the deltoid’s anterior and middle heads, allowing the arm to abduct or move away from the body.
It winds around the neck of the humerus/funny bone, goes beneath the deltoid muscle, and then connects to the forward edge of the deltoid.
A few small cutaneous branches serve the skin in that area.
Posterior Division
Innervates the teres minor muscles and the lower part of the deltoid.
It enters the deep fascia and becomes the superior lateral cutaneous nerve.
It then wraps around the lower edge of the deltoid, connects to the skin over the lower two-thirds of the muscle, and covers the long head of the triceps brachii.
Articular Branch
Comes from the trunk of the axillary nerve and enters the glenohumeral joint, which is in the shoulder, below the subscapularis muscle.
Anatomical Variations
In a case report, healthcare providers noted an incidence of the nerve branching directly off the upper trunk of the brachial plexus rather than the posterior cord. (Subasinghe S. K. and Goonewardene S. 2016) In this case, it innervated the subscapularis muscle, latissimus dorsi, and the deltoid and teres minor muscles and also had a communicating branch to the posterior cord. Another case documented multiple abnormalities in the course of the axillary nerve in an individual with pain and severely limited shoulder mobility. (Pizzo R. A. et al., 2019) During reverse shoulder arthroplasty, the surgeon discovered that the axillary nerve ran beside the coracoid process instead of underneath and stayed close to the subscapularis muscle instead of traveling through the quadrangular space. The case noted earlier reports of axillary nerves not running through the quadrangular space. In those cases, the nerve pierced the subscapularis muscle or split into branches before reaching the quadrangular space.
Function
The axillary nerve functions as a motor nerve that controls movement and a sensory nerve that controls sensations like touch or temperature.
Motor
As a motor nerve, the axillary nerve innervates three muscles in the arm and includes:
Deltoid
Allows flexing of the shoulder joint and rotating the shoulder inward.
Long Head of the Triceps
It runs down the back of the outer arm, allowing straightening, pulling the upper arm toward the body, or extending it backward.
The radial nerve can also innervate this muscle.
Teres Minor
One of the rotator cuff muscles starts outside the shoulder and runs diagonally along the bottom edge of the shoulder blade.
It works with other muscles to allow for the external rotation of the shoulder joint.
Sensory
In its sensory role, the nerve carries information to the brain from the following:
Glenohumeral joint or the ball-and-socket joint in the shoulder.
The skin on the lower two-thirds of the deltoid muscle through the superior lateral cutaneous branch.
Injuries and Conditions
Problems with the axillary nerve can be caused by injuries anywhere along the arm and shoulder and by disease. Common injuries include:
Dislocations
Of the shoulder joint, which can cause axillary nerve palsy.
Fracture
Of the surgical neck of the humerus.
Compression
This stems from walking with crutches, also known as crutch palsy.
Direct Trauma
This can be from an impact sports, work, automobile accident, collision, or laceration.
Added Pressure
This can be from wearing a cast or splint.
Surgical Accidental Injury
An injury or damage can come from shoulder surgery, especially arthroscopic surgery on the inferior glenoid and capsule.
Quadrangular Space Syndrome
This is where the axillary nerve is compressed where it passes through that space, which is most common in athletes who perform frequent overhead motions)
Nerve Root Damage
Between the fifth and sixth cervical vertebrae, where the nerve emerges from the spinal cord, which can be caused by traction, compression, spinal disc prolapse, or a bulging disc.
Systemic Neurological Disorders
Example – multiple sclerosis
Erb’s Palsy
A condition often is the result of a birth injury called shoulder dystocia, in which a baby’s shoulder/s becomes stuck during childbirth.
Axillary Nerve Palsy
Damage can result in a type of peripheral neuropathy that can cause weakness in the deltoid and teres minor muscles.
This can result in losing the ability to lift the arm away from the body and weakness in various shoulder movements.
If the damage is severe enough, it can cause paralysis of the deltoid and other minor muscles, resulting in flat shoulder deformity, in which individuals cannot lay their shoulders flat when lying down.
Axillary nerve damage also can lead to a change, reduction, or loss of sensation in a small part of the arm just below the shoulder.
Nerve Injury Statistics
Three times more common in men than women.
It may be present in as many as 65% of shoulder injuries.
The risk of injury due to dislocation is significantly increased after age 50.
Tests
If a healthcare provider suspects a problem with axillary nerve function, they’ll test the shoulder’s range of motion and skin sensitivity. A difference in the range of motion between the shoulders can indicate a nerve injury. Individuals may be sent for electromyography and a nerve conduction study to verify nerve palsy. In some cases, an MRI and/or X-rays may be ordered, especially if the cause of possible nerve damage is unknown.
Rehabilitation
Depending on the severity and cause of the injury, non-surgical treatments may be recommended, with surgery as a last resort. Non-surgical treatment can include some combination of immobilization, rest, ice, physical therapy, and anti-inflammatory meds. Physical treatment typically lasts about six weeks and focuses on strengthening and stimulating the muscles to prevent joint stiffness, which can impair long-term function.
Surgery
If conservative treatments don’t work, surgery may be recommended, especially if several months have passed without improvement. Surgical outcomes are generally better if surgery is performed within six months of the injury, and regardless of the time frame, the prognosis is considered positive in about 90% of cases. Surgical procedures performed for axillary nerve dysfunction or injury include:
Neurolysis
This procedure involves targeted damage/degeneration of nerve fibers, interrupts the nerve signals, and eliminates pain while the damaged area heals.
Neurorrhaphy
This procedure stitches a severed nerve back together.
Nerve Grafting
Grafting involves transplanting a portion of another nerve, usually the sural nerve, to reconnect severed nerves.
This helps, especially when the damaged portion is too large to be repaired by neurorrhaphy.
It allows a pathway for signals and encourages the regrowth of nerve axons.
Neurotization or Nerve Transfer
Similar to grafting but used when the nerve is too damaged to heal.
This procedure involves transplanting a healthy but less important nerve, or a portion of a nerve, to replace the damaged one and restore function.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Shoulder Pain Chiropractic Treatment
References
Subasinghe, S. K., & Goonewardene, S. (2016). A Rare Variation of the Axillary Nerve Formed as Direct Branch of the Upper Trunk. Journal of clinical and diagnostic research : JCDR, 10(8), ND01–ND2. https://doi.org/10.7860/JCDR/2016/20048.8255
Pizzo, R. A., Lynch, J., Adams, D. M., Yoon, R. S., & Liporace, F. A. (2019). Unusual anatomic variant of the axillary nerve challenging the deltopectoral approach to the shoulder: a case report. Patient safety in surgery, 13, 9. https://doi.org/10.1186/s13037-019-0189-1
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine