What are the advantages of having a team of nurse practitioners and chiropractors help maintain the health of your spine after a car accident?
Benefits of Chiropractic and Nurse Practitioners for Motor Vehicle Collisions
One of the main causes of spinal injuries, such as whiplash, herniated discs, and soft tissue injury, which can cause severe pain and impair movement, is motor vehicle collisions (MVCs). For both short-term symptoms and long-term rehabilitation, these injuries frequently necessitate a multimodal therapy strategy. While nurse practitioners, as advanced practice registered nurses, conduct medical evaluations, write prescriptions, and oversee overall health management, chiropractors focus on musculoskeletal care, including spine adjustments and manual therapies. These professionals’ collaboration aims to provide a comprehensive, patient-centered strategy for spine health following MVC. (Kent, R., et al., 2023)
For those recuperating from auto accident injuries, a chiropractic and nurse practitioner team can offer thorough spinal health care with an emphasis on pain management and increased mobility.
A chiropractic and nurse practitioner team can offer a comprehensive approach to spinal health after a car accident by addressing pain, improving mobility, and facilitating faster recovery.
Chiropractors focus on spinal alignment and joint mobility.
Nurse practitioners provide broader medical oversight and patient education.
The team approach can lead to more effective and personalized care for individuals recovering from car accident injuries. (Riva, J. J., et al., 2010)
Key advantages of this collaborative approach
A chiropractor and nurse practitioner (NP) therapy team can combine their skills to provide comprehensive care for spine health following a motor vehicle collision (MVC) and address acute and long-term requirements.
Care that is multidisciplinary and holistic
Collaboration between chiropractors and NPs to address structural and systemic issues enhances treatment outcomes, particularly for spine injuries related to motor vehicle collisions (MVC), as well as for chronic headaches and neck discomfort. (Riva, J. J., et al., 2010)
Plans for Treatment That Are Unique to You
Chiropractors and NPs create personalized patient treatment plans, focusing on their specific injuries and overall health, including pre-existing conditions and medication needs. This approach enhances outcomes by tailoring care to the patient’s unique circumstances.
Managing Pain Without Relying Too Much on Drugs
By using non-invasive methods to alleviate pain, chiropractic therapy may help reduce the use of opioids. NPs can prescribe short-term pain relief and monitor side effects, ensuring safe use and reducing dependency risks. Natural pain management combined with medical supervision lessens dependence and side effects. (Prater, C., Tepe, M., & Battaglia, P. 2020)
Quicker Recuperation and Rehabilitation
As demonstrated in the treatment of auto accidents, chiropractic adjustments can lessen muscle spasms and restore joint function. By referring patients to physical therapy and tracking their progress, NPs can hasten recovery and reduce the likelihood of developing persistent back pain. This integrated therapy not only reduces chronic back pain and other long-term problems, but it also accelerates healing.
Help with Insurance and the Law
Chiropractic and medical providers must carefully record injuries and treatments for insurance claims or legal cases after an MVC to ensure just reimbursement and coverage for care.
Why It Works After MVC
Following a motor vehicle collision (MVC), a chiropractor and nurse practitioner team offers a patient-centered approach to spine health. This team enhances recovery, lowers chronic risks, and improves patient outcomes by fusing NP’s medical management with chiropractic knowledge. This method ensures rapid alleviation and long-term health, especially helpful for complex spine injuries due to MVC.
Injury, Chiropractic, and Functional Medicine Clinic
Dr. Jimenez, a nurse practitioner, uses medical knowledge and chiropractic care to treat various conditions. The clinic provides tailored care programs incorporating functional medicine, acupuncture, electroacupuncture, and sports medicine. The clinic focuses on strength, agility, and flexibility for treating chronic pain syndromes and injuries. Patients of all ages and abilities benefit from comprehensive care plans and in-person and virtual health coaching, ensuring tailored treatment and wellness outcomes.
Personal Injury Rehabilitation
References
Kent, R., Cormier, J., McMurry, T. L., Johan Ivarsson, B., Funk, J., Hartka, T., & Sochor, M. (2023). Spinal injury rates and specific causation in motor vehicle collisions. Accident; analysis and prevention, 186, 107047. https://doi.org/10.1016/j.aap.2023.107047
Riva, J. J., Muller, G. D., Hornich, A. A., Mior, S. A., Gupta, A., & Burnie, S. J. (2010). Chiropractors and collaborative care: An overview illustrated with a case report. The Journal of the Canadian Chiropractic Association, 54(3), 147–154.
Prater, C., Tepe, M., & Battaglia, P. (2020). Integrating a Multidisciplinary Pain Team and Chiropractic Care in a Community Health Center: An Observational Study of Managing Chronic Spinal Pain. Journal of primary care & community health, 11, 2150132720953680. https://doi.org/10.1177/2150132720953680
Explore effective pain management strategies after a car accident. Learn how to recover and manage your discomfort.
Introduction
Numerous bodily injuries are often the outcome of auto accidents. Among the most frequent, soft tissue injuries sustained in vehicle accidents may cause severe pain and suffering in many different parts of the body, making everyday living difficult and necessitating a methodical approach to pain treatment. Do you have any headaches that make you want to be in a dark, quiet place? Do you think your shoulders have a limited range of motion? Or if you have lower back and shoulder ache that radiates? With an emphasis on soft tissue injuries, their symptoms, and both surgical and non-surgical treatment options, this article provides suggestions for managing pain after an accident..
Understanding Soft Tissue Injuries
Soft tissue injuries damage muscles, tendons, ligaments, and fascia. Common examples include whiplash, sprains, strains, and contusions. These injuries frequently occur during automobile accidents due to sudden forces exerted on the body, such as rapid deceleration or impact. The mechanisms of soft tissue injuries can become an issue as they can affect a person’s functionality, especially if the area has overlapping risk profiles. (Arosarena & Eid, 2021)
Symptoms of Soft Tissue Injuries
Various symptoms of soft tissue injuries depend on where the injury is located and how severe it is, but often include:
Pain and Tenderness: Localized or diffuse pain that worsens with movement or pressure.
Swelling: Inflammation due to fluid buildup in the affected area.
Stiffness: Reduced range of motion in joints or muscles.
Bruising: Discoloration from damaged blood vessels beneath the skin.
Weakness: Reduced strength in the injured area, often noticeable in sprains or strains.
Neck or Back Pain: Common musculoskeletal pain associated with whiplash, where pain may radiate to the shoulders or arms due to a cracking sound within the cervical spine, causing pain to appear either hours or days. (Bannister et al., 2009)
Beyond the Surface: Understanding the Effects of Personal Injury- Video
Guidelines for Pain Management
Effective pain management after an automobile accident requires a comprehensive approach tailored to the individual’s injury severity, medical history, and response to treatment. The following guidelines provide a framework for managing pain associated with soft tissue injuries.
1. Initial Assessment & Diagnosis
Medical Evaluation: Individuals should seek immediate medical attention to assess the extent of injuries. A healthcare provider may use physical exams, imaging (e.g., X-rays, MRIs), or diagnostic tests to identify soft tissue damage.
Pain Assessment: Document pain levels using tools like the Visual Analog Scale (VAS) to guide treatment planning.
Monitor Symptoms: Track symptoms over time, as some injuries, like whiplash, may have delayed onset.
2. Non-Surgical Treatment Options
Non-surgical treatments are typically the first line of management for soft tissue injuries, aiming to reduce pain and inflammation and promote healing.
RICE
Rest: Limit activities that exacerbate pain to allow tissues to heal.
Ice: Apply cold packs every fifteen to twenty minutes every hour to reduce swelling and numbness in the affected area. (Hubbard & Denegar, 2004)
Compression: Use elastic bandages to minimize swelling, ensuring not to wrap too tightly.
Elevation: Elevating the injured area above the heart level can help reduce fluid buildup.
Evidence: RICE is widely recommended for acute soft tissue injuries to manage initial symptoms affecting the musculoskeletal system.
Medications
Over-the-Counter Pain Relievers: Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen or acetaminophen can temporarily help relieve pain and inflammation in soft tissues.
Muscle Relaxants: Prescribed for muscle spasms, particularly in whiplash cases.
Topical Analgesics: Creams or patches for localized pain relief.
Considerations: Long-term NSAID use should be monitored to avoid gastrointestinal or cardiovascular side effects.
Physical Therapy
Stretching and Strengthening: Guided exercises to restore mobility and strength.
Manual Therapy: Massage or myofascial release incorporates various techniques to reduce tension.
Modalities: Ultrasound, electrical stimulation, or heat therapy to enhance healing. (Papadopoulos & Mani, 2020)
Evidence: Physical therapy is effective for chronic whiplash and other soft tissue injuries, improving function and reducing pain.
Alternative Therapies
Acupuncture: May reduce pain by stimulating specific points in the body.
Chiropractic Care: Spinal adjustments to alleviate pain, particularly for neck and back injuries.
Massage Therapy: Helps promote relaxation and reduces muscle tension where the affected area needs attention.
Acupuncture and chiropractic care show promise for pain relief in soft tissue injuries through various results. Chiropractic care can incorporate soft tissue mobilization to increase internal rotation and improve range of motion by reducing musculoskeletal pain. (Jusdado-García & Cuesta-Barriuso, 2021)
Psychological Support
Cognitive Behavioral Therapy (CBT): Helps manage chronic pain by addressing emotional and psychological factors.
Mindfulness and Relaxation Techniques: Reduces stress-related pain amplification.
3. Surgical Treatment Options
Surgery is rarely required for soft tissue injuries; however, they are considered during severe cases or when conservative treatments fail.
Arthroscopic Surgery
They are used to repair or remove damaged tissue from torn ligaments or tendons (e.g., rotator cuff tears). They are minimally invasive, utilizing smaller incisions to reduce persistent pain or instability, creating a faster recovery.
Tendon or Ligament Repair
Open surgery to reattach or reconstruct severely torn tendons or ligaments is often followed by extensive rehabilitation to restore function.
Rarely used for severe contusions causing compartment syndrome, where pressure buildup threatens tissue viability.
Involves cutting the fascia to relieve pressure.
Risks: Infection, scarring, and prolonged recovery.
4. Rehabilitation & Long-Term Management
Gradual Return to Activity: Follow a structured rehabilitation plan to prevent re-injury.
Pain Monitoring: Regularly assess pain levels to adjust treatments as needed.
Lifestyle Modifications: Maintain a healthy weight, practice good posture, and avoid activities that strain the injured area.
Structured rehabilitation programs improve outcomes for soft tissue injuries by providing multimodal treatments that are customized for the individual. (Bussières et al., 2016)
Considerations & Precautions
Individualized Care: Treatment plans should account for age, overall health, and injury severity.
Avoid Overtreatment: Overuse of medications or unnecessary surgeries can lead to complications.
Follow-Up: Regular check-ups to monitor recovery and address persistent pain.
Legal and Insurance Aspects: Documents of injuries and treatments for insurance claims or legal proceedings should be related to the accident.
Conclusion
Following a car accident, pain treatment calls for a multimodal approach, especially for soft tissue injuries such sprains, strains, and whiplash. The combination of early medical examination, non-surgical therapies such as RICE, medication, physical therapy, and, in rare instances, surgical intervention may help people achieve successful pain relief and rehabilitation. The best results are ensured by seeking advice from medical experts and following evidence-based recommendations.
Injury Medical Chiropractic & Functional Medicine Clinic
We associate certified medical providers who understand the importance of assessing individuals with pain-like symptoms affecting their musculoskeletal system. When asking important questions to our associated medical providers, we advise patients to incorporate customized treatment plans for their pain correlated with musculoskeletal issues after being involved in an auto accident. Dr. Alex Jimenez, D.C., uses this information as an academic service. Disclaimer
Bannister, G., Amirfeyz, R., Kelley, S., & Gargan, M. (2009). Whiplash injury. The Journal of Bone and Joint Surgery. British volume, 91-B(7), 845-850. https://doi.org/10.1302/0301-620x.91b7.22639
Bussières, A. E., Stewart, G., Al-Zoubi, F., Decina, P., Descarreaux, M., Hayden, J., Hendrickson, B., Hincapié, C., Pagé, I., Passmore, S., Srbely, J., Stupar, M., Weisberg, J., & Ornelas, J. (2016). The Treatment of Neck Pain–Associated Disorders and Whiplash-Associated Disorders: A Clinical Practice Guideline. Journal of Manipulative and Physiological Therapeutics, 39(8), 523-564.e527. https://doi.org/10.1016/j.jmpt.2016.08.007
Jusdado-García, M., & Cuesta-Barriuso, R. (2021). Soft Tissue Mobilization and Stretching for Shoulder in CrossFitters: A Randomized Pilot Study. International Journal of Environmental Research and Public Health, 18(2), 575. https://doi.org/10.3390/ijerph18020575
Papadopoulos, E. S., & Mani, R. (2020). The Role of Ultrasound Therapy in the Management of Musculoskeletal Soft Tissue Pain. Int J Low Extrem Wounds, 19(4), 350-358. https://doi.org/10.1177/1534734620948343
Here, you can find expert advice on coping with spine and back pain, the aftermath of a car accident, and improving your quality of life.
Introduction
People who have been in an automobile accident, even a little one, may have physical injuries to their back, spine, and upper and lower limbs. Acute or persistent pain may be the consequence of injuries brought on by the abrupt forces involved in a collision. Does stiffness affect your shoulders, back, and neck? Do you have back discomfort that radiates down? Or have you been unable to do your everyday chores due to persistent headaches? Today, we’ll examine and comprehend the reasons behind back and spine discomfort, identify its symptoms, and investigate how people may heal and reclaim their quality of life with the aid of efficient therapies like chiropractic adjustments.
Spine & Back Pain Causes After a Car Accident
The spine and back are vulnerable during a car accident due to the rapid acceleration, deceleration, and twisting motions that occur. Common causes of pain include:
Whiplash and Soft Tissue Injuries: A person in a rear-end collision will experience a common injury known as whiplash. This musculoskeletal injury occurs when the head and neck are forcefully jerked forward and backward. (Stroke, 2023) This can strain or tear muscle tissue structures in the neck and upper back, leading to the development of pain and stiffness throughout the body.
Herniated Discs: The impact of a car collision can cause the spinal segments to compress or displace the intervertebral discs, causing them to bulge or rupture. This may irritate nearby nerves, compressing them, resulting in back pain-associated numbness or weakness within the upper and lower extremities. (Ge et al., 2019)
Spinal Misalignment: The sudden jolts and movements the body experiences after a car collision can misalign the spinal vertebrae, disrupting the spine’s natural curvature. This can lead to numerous pain-like symptoms, such as muscle spasms, restricted movement, and pain.
Fractures or Dislocations: In severe accidents, the spinal vertebrae may fracture or dislocate, causing intense pain and potential nerve damage. These injuries can negatively influence an individual’s social and financial situation when being treated. (Fakharian et al., 2017)
Facet Joint Injuries: The facet joints, which connect the vertebrae, can become sprained or damaged during a collision, leading to pain.
Symptoms of Spine & Back Pain
Depending on the collision’s severity, the spine and back can develop symptoms depending on the type of injury the person is experiencing. Common signs include:
Localized or Radiating Pain
Stiffness
Muscle Spasms
Numbness or Tingling
Headaches
Fatigue or Weakness
Delayed onset of symptoms is common, with pain or discomfort appearing hours or days after the accident. Seeking prompt medical evaluation is critical to prevent complications.
From Injury to Recovery with Chiropractic Care- Video
The Role Of Chiropractic Care in Treatment
Chiropractic care is a non-surgical treatment option focusing on restoring spinal alignment, improving mobility, and reducing pain within the musculoskeletal system. It is particularly effective for managing spine and back pain caused by car accidents. Key benefits of chiropractic care include:
Spinal Adjustments: Chiropractors use controlled, manual techniques to realign the spine, relieve pressure on the compressed nerves, and restore joint function. This can reduce pain, improve mobility, and restore the normal range of spinal movement. (Choi et al., 2015)
Soft Tissue Therapy: Chiropractors can incorporate massage or myofascial release techniques to help relax the tight muscles, reduce spasms, and promote healing in strained ligaments and tendons.
Pain Management: Since chiropractic care can alleviate pain without reliance on medications, which may have side effects. Chiropractic adjustments and therapies target the root cause of discomfort.
Rehabilitation Support: Chiropractors often provide exercises and stretches as part of the individual’s customized treatment plan to strengthen muscles and prevent future injuries.
Holistic Approach: Chiropractic care emphasizes overall wellness, addressing physical symptoms and lifestyle factors that impact the person’s recovery process.
Chiropractic care is effective for conditions like whiplash, which is associated with neck and lower back pain. Compared to standard medical care, it reduces pain and improves function. (Bryans et al., 2014)
Other Treatment Options
While chiropractic care is highly effective, a comprehensive treatment plan may include:
Physical Therapy: To restore strength and flexibility back to the body while reducing low back and neck pain. (Alrwaily et al., 2019)
Pain Management: Over-the-counter or prescription medications for short-term relief.
Medical Imaging: X-rays, MRIs, or CT scans to diagnose fractures or herniated discs.
Surgery: In rare cases, for severe injuries like spinal fractures or significant disc herniations.
When to Seek Care
Individuals involved in a car accident must have a prompt evaluation by a healthcare provider, such as a chiropractor or physician. Even if symptoms are mild, this is essential because if the injuries are untreated, they can cause overlapping risk profiles or long-term complications to the body. A chiropractor can assess spinal alignment, recommend a personalized treatment plan, and coordinate with other providers.
Conclusion
Following a vehicle accident, those who have back and spine pain may find that their everyday lives are significantly impacted, but recovery may be aided by prompt action and the right treatment. A safe and efficient method for controlling pain, regaining function, and averting chronic problems is chiropractic therapy. A chiropractor may help people recover from accidents by determining the root causes of pain-like symptoms and promoting general wellbeing.
Injury Medical Chiropractic & Personal Injury Clinic
We associate certified medical providers who understand the importance of assessing individuals with pain-like symptoms affecting their spines and backs. When asking important questions to our associated medical providers, we advise patients to incorporate customized treatment plans for their pain correlated with musculoskeletal issues. Dr. Alex Jimenez, D.C., uses this information as an academic service. Disclaimer
References
Alrwaily, M., Schneider, M., Sowa, G., Timko, M., Whitney, S. L., & Delitto, A. (2019). Stabilization exercises combined with neuromuscular electrical stimulation for patients with chronic low back pain: a randomized controlled trial. Braz J Phys Ther, 23(6), 506-515. https://doi.org/10.1016/j.bjpt.2018.10.003
Bryans, R., Decina, P., Descarreaux, M., Duranleau, M., Marcoux, H., Potter, B., Ruegg, R. P., Shaw, L., Watkin, R., & White, E. (2014). Evidence-based guidelines for the chiropractic treatment of adults with neck pain. J Manipulative Physiol Ther, 37(1), 42-63. https://doi.org/10.1016/j.jmpt.2013.08.010
Choi, J., Lee, S., & Jeon, C. (2015). Effects of flexion-distraction manipulation therapy on pain and disability in patients with lumbar spinal stenosis. J Phys Ther Sci, 27(6), 1937-1939. https://doi.org/10.1589/jpts.27.1937
Fakharian, E., Mohammadzadeh, M., Saberi, H. R., Fazel, M. R., Rejali, M., Akbari, H., Mirzadeh, A. S., & Mohammadzadeh, J. (2017). Spinal injury resulting from car accident: Focus to prevention. Asian J Neurosurg, 12(2), 180-184. https://doi.org/10.4103/1793-5482.152110
Ge, C. Y., Hao, D. J., Yan, L., Shan, L. Q., Zhao, Q. P., He, B. R., & Hui, H. (2019). Intradural Lumbar Disc Herniation: A Case Report and Literature Review. Clin Interv Aging, 14, 2295-2299. https://doi.org/10.2147/CIA.S228717
Can older people who exercise regularly lessen their risk of dementia and enhance their overall health?
Exercise and the Prevention of Dementia
Dementia, a term used to cover several conditions that impact memory and cognition, is currently the seventh leading cause of mortality worldwide. (World Health Organization, 2025) More than 10 million new cases of dementia are found around the world each year. (J.H. Yoon et al., 2023) Research investigating the relationship between exercise and insulin in the brain suggests that regular exercise may improve brain function and decrease the prevalence of dementia. Scientists have discovered that variables, such as.
Muscles must be exercised and mobilized. People who do not engage in physical activity have rigid muscles, which impede the effectiveness of insulin. The body’s sensitivity to insulin is improved by the contraction and relaxation of the muscles during movement. Dementia can be prevented by understanding how to decrease the body’s insulin resistance.
Physical Activity and Lower Risk
Over two weeks, researchers examined 21 older adults with prediabetes and found that exercise enhances cognitive performance by aiding the brain in insulin regulation. They conducted twelve supervised training sessions of moderate to extreme intensity. (Malin S. K. et al., 2025)
The results indicated that brain-derived extracellular vesicles containing insulin-related proteins had significantly increased.
These microscopic messengers are essential for brain maintenance and aid in neuronal communication.
Three serine/threonine-specific protein kinases known as AKT (protein kinase B, or PKB) are essential for several cellular functions, such as cell growth, survival, metabolism, and cell cycle control.
The protein affects the development and health of neuronal cells and is thought to play a significant role in insulin signaling.
The notion that exercise might help prevent dementia by potentially enhancing insulin signaling is important since poor insulin response can result in dementia.
Even while further research is needed, these findings prove that physical activity could be a cost-effective and easily accessible way to improve long-term brain health. To better understand how insulin affects brain activity, researchers will use MRIs and an insulin spray in the study’s next phase. To learn more about the effects of the insulin spray, they will compare the blood flow in the brain before and after it is administered.
Insulin and Exercise Are Essential for Brain Health
Insulin is a hormone that the pancreas makes. It controls blood sugar levels. But it’s just as vital for the health of the brain. Insulin binds to many receptors in the brain, which makes synaptic connections stronger and makes it easier for neurons to talk to each other. Both of these things help with memory and learning. (Gray, S. M., Meijer, R. I., & Barrett, E. J. 2014)
Type 2 diabetes, which impairs insulin transmission, increases the risk of cognitive impairment. (Yoon J.H. et al., 2023) Research has demonstrated that insulin resistance exacerbates tau tangles and amyloid-beta plaques, which are two critical characteristics of Alzheimer’s disease. (Hong, S., Han, K., & Park, C. Y. 2021) Increasing insulin sensitivity may slow down or even stop these changes in the brain. Working out, especially aerobic exercise, is good for the brain. According to earlier research, exercise can help people maintain or enhance their memory and brain function. (Rosenberg A. et al., 2020) Other ways to increase brain health include:
Maintaining social interaction
Challenging the mind
Getting a good night’s sleep
Controlling stress
A nutritious diet
Maintaining an active lifestyle
Controlling diabetes
Controlling blood pressure
To achieve the greatest possible effect, dementia prevention in the future will likely involve integrating lifestyle modifications, such as exercise, with medications. In individuals with diabetes or prediabetes, the risk of dementia is significantly reduced, and frequent exercise can assist in the preservation of optimal brain function.
Chiropractic and Functional Medicine Clinic
As a family nurse practitioner, Dr. Jimenez uses the latest medical expertise and chiropractic therapy to address many problems. Our clinic uses functional medicine, acupuncture, electro-acupuncture, and sports medicine to create individualized care plans that improve movement, encourage long-term health, and speed up the body’s natural healing process. We focus on strength, agility, and flexibility to help our patients thrive, regardless of age or health problems. At El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we want to help people with chronic pain syndromes and injuries. We focus on improving flexibility, mobility, and agility through programs suitable for people of all ages and abilities. We ensure that each patient gets personalized care and reaches their health objectives through detailed care plans and health coaching in person and online.
Is Movement Essential to Recovery?
References
World Health Organization. (2025). “Dementia.” World Health Organization. from https://www.who.int/news-room/fact sheets/detail/dementia#:~:text=Alzheimer%20disease%20is%20the%20most,60%E2%80%9370%25%20of%20cases.
Yoon, J. H., Hwang, J., Son, S. U., Choi, J., You, S. W., Park, H., Cha, S. Y., & Maeng, S. (2023). How Can Insulin Resistance Cause Alzheimer’s Disease?. International Journal of Molecular Sciences, 24(4), 3506. https://doi.org/10.3390/ijms24043506
Malin, S. K., Battillo, D. J., Beeri, M. S., Mustapic, M., Delgado-Peraza, F., & Kapogiannis, D. (2025). Two weeks of exercise alters neuronal extracellular vesicle insulin signaling proteins and pro-BDNF in older adults with prediabetes. Aging cell, 24(1), e14369. https://doi.org/10.1111/acel.14369
Gray, S. M., Meijer, R. I., & Barrett, E. J. (2014). Insulin regulates brain function, but how does it get there?. Diabetes, 63(12), 3992–3997. https://doi.org/10.2337/db14-0340
Hong, S., Han, K., & Park, C. Y. (2021). The insulin resistance by triglyceride glucose index and risk for dementia: population-based study. Alzheimer’s research & therapy, 13(1), 9. https://doi.org/10.1186/s13195-020-00758-4
Rosenberg, A., Mangialasche, F., Ngandu, T., Solomon, A., & Kivipelto, M. (2020). Multidomain Interventions to Prevent Cognitive Impairment, Alzheimer’s Disease, and Dementia: From FINGER to World-Wide FINGERS. The Journal of Prevention of Alzheimer’s disease, 7(1), 29–36. https://doi.org/10.14283/jpad.2019.41
Optimizing Recovery from Work-Related Back Injuries: The Interdisciplinary Approach of Dr. Alexander Jimenez, DC, APRN, FNP-BC
Introduction
Back injuries sustained at work are a leading cause of disability and lost productivity, affecting diverse professions such as truck drivers, construction workers, healthcare providers, and office employees. These injuries often result from improper lifting, repetitive motions, or prolonged sitting, leading to conditions like herniated discs, muscle strains, or chronic pain. For those injured, securing workers’ compensation benefits and accessing effective treatment are critical steps toward recovery. Dr. Alexander Jimenez, a dual-licensed chiropractor and nurse practitioner with over three decades of experience, specializes in treating work-related back injuries, particularly those from personal injury cases and auto accidents. His integrative approach, detailed on www.dralexjimenez.com and www.chiromed.com, combines chiropractic care, advanced medical interventions, and collaboration with trusted medical and legal professionals to deliver comprehensive care.
This article outlines the benefits of chiropractic care in managing work-related back injuries, the expanded treatment options enabled by Dr. Jimenez’s nurse practitioner licensure, and the interdisciplinary strategies that optimize recovery. It also highlights how Dr. Jimenez collaborates with legal providers to ensure patients receive the support needed to navigate workers’ compensation claims effectively.
The Burden of Work-Related Back Injuries
Work-related back injuries are prevalent across industries, with the Bureau of Labor Statistics reporting over 900,000 cases of nonfatal occupational injuries involving the back in 2020. High-risk occupations include:
Truck Drivers: Prolonged sitting and unloading heavy cargo increase spinal stress.
Construction Workers: Lifting, twisting, and repetitive motions contribute to injury.
Healthcare Workers: Patient handling and prolonged standing elevate risk.
Manual Laborers: Heavy lifting and improper techniques lead to strains.
Office Workers: Poor posture and sedentary behavior cause chronic pain.
These injuries often result from improper lifting, repetitive turning, twisting while lifting, or holding heavy objects overhead. Symptoms may include acute pain, limited mobility, or chronic conditions requiring long-term management. Workers’ compensation programs exist to cover medical expenses and lost wages, but the process can be complex, necessitating expert medical and legal guidance.
Benefits of Chiropractic Care for Work-Related Back Injuries
Chiropractic care is a cornerstone of non-invasive treatment for back injuries, focusing on restoring spinal alignment, reducing pain, and improving function. Dr. Jimenez leverages evidence-based chiropractic techniques to address work-related injuries, supported by randomized controlled trials (RCTs) and cohort studies.
Pain Reduction and Functional Improvement
Chiropractic adjustments, or spinal manipulations, realign the spine to alleviate pressure on nerves and muscles. A 2018 RCT published in The Spine Journal (Goertz et al.) found that chiropractic care combined with usual medical care significantly reduced pain and disability in patients with low back pain compared to medical care alone. Dr. Jimenez employs manual adjustments, flexion-distraction techniques, and soft tissue therapies to target specific injury sites, promoting natural healing.
Non-Invasive and Drug-Free Approach
Chiropractic care offers a drug-free alternative to pain management, reducing reliance on opioids, which is critical given the opioid crisis. A 2020 cohort study in Pain Medicine (Whedon et al.) demonstrated that patients receiving chiropractic care for low back pain had a lower likelihood of opioid prescriptions compared to those receiving only medical care. Dr. Jimenez integrates therapies like myofascial release and therapeutic exercises to manage pain without pharmacological interventions.
Prevention of Chronic Conditions
Early chiropractic intervention can prevent acute injuries from becoming chronic. A 2019 study in Journal of Manipulative and Physiological Therapeutics (Eklund et al.) showed that maintenance chiropractic care reduced the recurrence of low back pain episodes. Dr. Jimenez designs personalized treatment plans that include corrective exercises and ergonomic counseling to minimize re-injury risk.
Support for Workers’ Compensation Claims
Chiropractors play a vital role in documenting injuries for workers’ compensation claims. Dr. Jimenez provides detailed clinical notes and treatment plans, ensuring compliance with workers’ compensation requirements. His expertise in occupational health allows him to assess whether injuries are work-related, facilitating accurate reporting to employers and insurance carriers.
Expanded Scope of Practice: Nurse Practitioner Expertise
As a board-certified Family Nurse Practitioner (FNP-BC), Dr. Jimenez’s dual licensure enhances his ability to provide comprehensive care, particularly in personal injury and auto accident cases. Nurse practitioners (NPs) have an expanded scope of practice, allowing them to diagnose, treat, and prescribe medications, which complements chiropractic interventions.
Advanced Diagnostics and Treatment
NPs can order and interpret diagnostic imaging, such as X-rays, MRIs, and CT scans, to assess the extent of spinal injuries. A 2021 study in Journal of General Internal Medicine (Mafi et al.) highlighted the accuracy of NPs in managing musculoskeletal conditions through diagnostics and treatment planning. Dr. Jimenez uses these tools to develop precise treatment strategies, ensuring timely interventions for conditions like herniated discs or vertebral fractures.
Medication Management
In cases where pain or inflammation requires pharmacological support, Dr. Jimenez can prescribe medications like non-steroidal anti-inflammatory drugs (NSAIDs) or muscle relaxants. His NP training ensures judicious use of medications, aligning with evidence-based guidelines to avoid over-reliance. This is particularly beneficial in auto accident cases, where soft tissue injuries often require short-term pharmacological support alongside chiropractic care.
Coordination of Multidisciplinary Care
NPs are trained to coordinate care across specialties, making Dr. Jimenez uniquely positioned to oversee interdisciplinary treatment plans. For complex injuries, he collaborates with orthopedic surgeons, neurologists, and physical therapists to ensure holistic care. A 2020 RCT in BMJ Open (Côté et al.) demonstrated improved outcomes when NPs coordinated multidisciplinary care for back pain, reducing recovery time and costs.
Enhanced Patient Education
NPs emphasize patient education, empowering individuals to manage their recovery. Dr. Jimenez provides guidance on posture, lifting techniques, and lifestyle modifications, drawing on his NP training to address comorbidities like obesity or diabetes that may complicate recovery. This integrative approach aligns with the philosophies outlined on www.chiromed.com, emphasizing patient-centered care.
Interdisciplinary Treatment Strategies
Dr. Jimenez’s practices integrate chiropractic and NP services with interdisciplinary treatments tailored to work injury trauma and auto accident cases. These strategies address the physical, emotional, and legal challenges of recovery.
Comprehensive Treatment Modalities
Chiropractic Adjustments: Correct spinal misalignments to reduce pain and restore mobility.
Physical Therapy: Strengthen core muscles and improve flexibility through targeted exercises.
Hydrotherapy: Use water-based therapies to reduce inflammation and enhance circulation.
Spinal Injections: Administer corticosteroid injections for severe inflammation, guided by diagnostic imaging.
Rehabilitation Programs: Design long-term plans to restore function and prevent re-injury.
A 2017 cohort study in Spine (Blanchette et al.) found that multidisciplinary care combining chiropractic, physical therapy, and medical interventions resulted in faster return-to-work rates for back injury patients. Dr. Jimenez’s integrative approach mirrors these findings, ensuring patients receive tailored care.
Focus on Personal Injury and Auto Accidents
Personal injury cases, including auto accidents, often involve whiplash, soft tissue injuries, and spinal trauma. Dr. Jimenez’s dual expertise allows him to address these conditions comprehensively. For example, whiplash may require chiropractic adjustments to restore cervical alignment, physical therapy to strengthen neck muscles, and short-term NSAIDs to manage pain. His ability to order MRIs ensures accurate diagnosis of soft tissue damage, which is critical for workers’ compensation and insurance claims.
Collaboration with Medical Specialists
Dr. Jimenez collaborates with a network of trusted medical providers, including:
Orthopedic Surgeons: For surgical interventions like discectomy or spinal fusion.
Neurologists: To address nerve-related symptoms like radiculopathy.
Pain Management Specialists: For advanced pain relief techniques, such as epidural injections.
This collaborative model ensures seamless care, with Dr. Jimenez overseeing the treatment plan to maintain continuity. His practice websites emphasize this integrative philosophy, highlighting partnerships with specialists who share a commitment to patient outcomes.
Collaboration with Trusted Legal Providers
Navigating workers’ compensation and personal injury claims requires legal expertise, particularly when employers or insurance carriers dispute claims. Dr. Jimenez partners with trusted legal providers specializing in workers’ compensation and personal injury law to support his patients.
Role of Legal Providers
Legal providers assist with:
Claim Filing: Ensuring timely and accurate submission of workers’ compensation claims, adhering to state-specific statutes of limitations (e.g., one year in many states).
Dispute Resolution: Representing patients in disputes over injury causation or benefit denials.
Maximizing Benefits: Advocating for coverage of all necessary treatments, including chiropractic care, diagnostics, and rehabilitation.
Auto Accident Claims: Handling insurance negotiations and litigation for injuries sustained in work-related auto accidents.
Dr. Jimenez refers patients to attorneys who understand the medical complexities of back injuries, ensuring alignment between clinical documentation and legal arguments. This collaboration is critical in gray-area cases, such as injuries sustained at work-related events or while working from home.
Streamlined Communication
Dr. Jimenez maintains active communication with legal providers, sharing clinical notes and treatment plans to substantiate claims. Workers’ compensation is exempt from HIPAA privacy regulations for injury-related records, allowing seamless information exchange. This ensures legal providers have the evidence needed to advocate effectively, reducing delays in treatment or compensation.
Patient Advocacy
By connecting patients with reputable attorneys, Dr. Jimenez empowers them to focus on recovery without the stress of legal battles. His websites, www.dralexjimenez.com and www.chiromed.com, emphasize this patient-centered approach, highlighting resources for legal support alongside medical care.
Workers’ Compensation: Coverage and Process
Workers’ compensation is an employer-funded insurance program that covers medical expenses and lost wages for work-related injuries. Coverage typically includes:
Emergency department visits
Diagnostic testing (e.g., X-rays, MRIs)
Follow-up care with specialists
Surgical interventions
Rehabilitation and physical therapy
Dr. Jimenez ensures patients understand their rights under workers’ compensation, advising them to report injuries immediately to their employer’s human resources department. Prompt reporting strengthens claims and prevents disputes over injury causation.
Challenges and Solutions
Challenges in securing workers’ compensation include:
Gray-Area Injuries: Injuries at work-related events or while working remotely may be contested. Dr. Jimenez provides detailed documentation to clarify work-related causation.
Employer Pressure: Some employers may pressure workers to return before medical clearance. Dr. Jimenez collaborates with legal providers to protect patients’ rights.
Wage Replacement Issues: Workers reliant on overtime may face reduced compensation. Dr. Jimenez advises patients to consult attorneys to maximize benefits.
A 2019 study in Journal of Occupational and Environmental Medicine (Mueller et al.) found that early legal intervention improved outcomes in contested workers’ compensation cases, underscoring the value of Dr. Jimenez’s legal partnerships.
Maximizing Recovery: Patient-Centered Strategies
Dr. Jimenez’s integrative approach prioritizes patient compliance and transparency to optimize recovery. Key strategies include:
Adherence to Treatment Plans: Keeping appointments and following recommendations ensures consistent progress.
Open Communication: Patients are encouraged to report symptoms accurately, enabling adjustments to treatment plans.
Ergonomic Training: Guidance on posture, lifting, and workplace modifications reduces re-injury risk.
Holistic Care: Addressing comorbidities and mental health to support overall well-being.
His websites provide resources like exercise guides and ergonomic tips, reinforcing these strategies and empowering patients to take an active role in their recovery.
Conclusion
Work-related back injuries and auto accident trauma require a comprehensive, interdisciplinary approach to achieve optimal recovery. Dr. Alexander Jimenez, DC, APRN, FNP-BC, combines his expertise as a chiropractor and nurse practitioner to deliver evidence-based treatments, from spinal adjustments to advanced diagnostics and medication management. His collaboration with trusted medical and legal providers ensures patients receive holistic care and robust support through the workers’ compensation process. By integrating chiropractic care, medical interventions, and legal advocacy, Dr. Jimenez empowers patients to recover fully and return to work with confidence. Visit www.dralexjimenez.com and www.chiromed.com to learn more about his integrative approach and commitment to patient-centered care.
References
Goertz, C. M., et al. (2018). Effect of usual medical care plus chiropractic care vs usual medical care alone on pain and disability among US service members with low back pain: A comparative effectiveness clinical trial. The Spine Journal, 18(8), 1391–1399.
Whedon, J. M., et al. (2020). Association between chiropractic care and use of prescription opioids among patients with low back pain. Pain Medicine, 21(6), 1087–1095.
Eklund, A., et al. (2019). The Nordic maintenance care program: Effectiveness of chiropractic maintenance care versus symptom-guided treatment for recurrent and persistent low back pain. Journal of Manipulative and Physiological Therapeutics, 42(7), 477–487.
Mafi, J. N., et al. (2021). Nurse practitioners and physician assistants in primary care: A systematic review of scope of practice and patient outcomes. Journal of General Internal Medicine, 36(5), 1423–1432.
Côté, P., et al. (2020). Management of neck pain and associated disorders: A clinical practice guideline from the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. BMJ Open, 10(3), e035366.
Blanchette, M. A., et al. (2017). Effectiveness of multidisciplinary rehabilitation programs for work-related low back pain: A systematic review. Spine, 42(13), 1007–1016.
Mueller, K. L., et al. (2019). Impact of early legal representation on workers’ compensation claim outcomes. Journal of Occupational and Environmental Medicine, 61(4), 312–318.
What are the benefits of both a chiropractor and a nurse practitioner in cases of personal injury and car accidents?
Chiropractic and Nurse Practitioner On Auto Accidents
Following a car accident, both nurse practitioners and chiropractors are essential in treating injuries and accelerating healing. To treat musculoskeletal problems and restore mobility, chiropractors concentrate on manual therapies like adjustments and manipulations. In contrast, nurse practitioners offer comprehensive care that includes evaluations, diagnoses, treatment plans, and education, frequently working with specialists to maximize patient outcomes. (Physicians Group, LLC. 2024)
Chiropractors
Musculoskeletal injuries, such as neck and back discomfort, are frequently sustained in traffic accidents and are treated by chiropractors. Frequently, without the use of drugs, they employ manual methods to reduce pain and increase mobility. Their thorough documentation and professional opinions can also bolster personal injury lawsuits by demonstrating the severity of injuries. (Dies, S., & Strapp, J. W., 1992)
Identification and Management of Musculoskeletal Conditions
After an accident, chiropractors can detect and treat soft tissue injuries, muscle spasms, and spinal misalignments. (The Neck and Back Clinics, 2025)
Pain Management
Soft tissue mobilization and spinal adjustments are examples of manual therapies that can help lower inflammation and relieve pain.
Enhanced Mobility
Chiropractors can assist in restoring range of motion and enhancing general function by addressing joint and muscle limitations.
Holistic Medical Treatment
In order to prevent further injuries, chiropractors can offer advice on maintaining proper posture, ergonomics, and general well-being.
Cooperation with Other Medical Experts
To develop a thorough treatment plan for a patient, chiropractors might collaborate closely with doctors, physical therapists, and other professionals. (Physicians Group, LLC, 2024)
Nurse Practitioners
For injuries sustained in auto accidents, nurse practitioners can offer comprehensive care, including: (Integrity Spine & Orthopedics, 2024)
Evaluation and Diagnosis
Nurse practitioners are qualified to perform physical examinations, interpret test results, and diagnose illnesses such as concussions, soft tissue injuries, and whiplash.
Plans for Treatment
To meet the patient’s unique needs, they can create individualized treatment programs that include prescription drugs, physical therapy, and other therapies.
Education of Patients
To encourage healing and avoid problems, nurse practitioners can instruct patients on their injuries, the healing process, and self-care techniques.
Care Coordination
To guarantee a comprehensive approach to treatment, they can coordinate care with other professionals like neurologists, physical therapists, and surgeons.
Aftercare
Throughout the healing process, nurse practitioners can keep an eye on the patient’s progress, modify treatment plans as necessary, and offer continuous support.
Complex medical and legal requirements are frequently present in personal injury cases, especially those resulting from traffic accidents. With their different areas of expertise, chiropractors and nurse practitioners are essential to diagnosis, care, and record-keeping.
When it comes to personal injury claims, NPs and chiropractors both have special advantages. While NPs handle more general medical needs, such as writing prescriptions and organizing care, chiropractors concentrate on musculoskeletal problems and provide non-invasive treatments. As seen in places like the Accident Care and Treatment Center, where NPs and doctors oversee care in addition to chiropractic interventions, their cooperation can improve patient results. (Accident Care, 2025)
According to legal resources, the documentation of both experts is essential for insurance settlements and claims. Together, the thorough medical records of NPs regarding general health and the detailed reports of chiropractors on spinal injuries can make a strong case for compensation. In situations involving auto accidents, when patients would need both medical supervision and physical adaptations for a proper recovery, this synergy is especially noticeable. (Chiropractic Economics, 2023)
Injury Medical Chiropractic and Functional Medicine Clinic
Dr. Jimenez, a family practice nurse practitioner, combines advanced medical skills with chiropractic care to treat a variety of problems. Our clinic combines functional medicine, acupuncture, electro-acupuncture, and sports medicine to provide personalized care regimens for natural healing, mobility, and long-term wellness. By emphasizing flexibility, agility, and strength, we enable patients to thrive regardless of age or health challenges. El Paso Chiropractic Rehabilitation Clinic & Integrated Medicine Center specializes in treating injuries and chronic pain conditions. We focus on enhancing your ability through flexibility, mobility, and agility training that is adapted to all age groups and disabilities. We offer personalized care through in-person and virtual health coaching, as well as comprehensive care plans.
Don’t Ignore Your Post-Accident Pain
References
Physicians Group, LLC. (2024). The Role of Nurse Practitioners in Managing Auto Injuries. Physicians Group, LLC. https://physiciansgroupllc.com/the-role-of-nurse-practitioners-in-managing-auto-injuries/#:~:text=Nurse%20Practitioners%20are%20vital%20in,improved%20outcomes%20and%20patient%20satisfaction.
Dies, S., & Strapp, J. W. (1992). Chiropractic treatment of patients in motor vehicle accidents: a statistical analysis. The Journal of the Canadian Chiropractic Association, 36(3), 139–145.
The Neck and Back Clinics. (2025). Why Seeing a Chiropractor After a Car Accident Is Crucial for Long-Term Recovery. https://theneckandbackclinics.com/long-term-recovery/#:~:text=Reducing%20Inflammation%20and%20Pain,each%20patient%20for%20optimal%20recovery.
Integrity Spine & Orthopedics. (2024). The 9 Steps to Recovery After an Auto Accident. https://www.integrityspineortho.com/post/the-9-steps-to-recovery-after-an-auto-accident/#:~:text=CONTACT%20INTEGRITY%20SPINE%20AND%20ORTHOPEDICS%20AFTER%20A,concussions%2C%20soft%20tissue%20damage%20and%20spine%20damage.
Accident Care and Treatment Center, Inc. (2025). Comprehensive Therapies and Treatments in One Location. https://accidentcare.com/treatment/
Chiropractic Economics. (2023). Evidence-based chiropractic: the key to personal-injury cases. https://www.chiroeco.com/evidence-based-chiropractic-the-key-to-personal-injury-cases/
Find essential information on whiplash, including signs, prevention tips, and recovery strategies for optimal health.
Introduction
An abrupt impact, whether from a vehicle accident, sports injury, or fall, may cause symptoms that start off as a small shock and progress to crippling pain and functional impairment. Whiplash is one such ailment that often lacks recognition due to its intricacy. Although it is often linked to rear-end crashes, whiplash is a complex injury that, if ignored, may have long-term consequences for the musculoskeletal system and cervical spine. Have you had shoulder and neck stiffness before? Do you have persistent, chronic headaches? Or does it seem like your neck’s range of motion is limited? We’ll talk about whiplash’s frequent origins, symptoms, effects on the cervical spine and musculoskeletal system, and evidence-based therapy options to lessen the pain-like symptoms in today’s post.
What Is Whiplash?
Whiplash is a type of neck injury associated with a rapid back-and-forth head-and-neck motion, mimicking the crack of a whip, hence the name. This causes persistent physical complaints and disability, and complaints when left untreated. (Mayou & Radanov, 1996) Medically, it is categorized under cervical acceleration-deceleration (CAD) injuries. This abrupt motion can damage muscles, ligaments, intervertebral discs, and even the neural structures of the cervical spine.
Common Causes Of Whiplash
While motor vehicle accidents are the most recognized cause, many mechanisms can precipitate a whiplash injury:
Even minor collisions at speeds as low as 5–10 mph can produce enough force to cause whiplash symptoms in vulnerable individuals.
Symptoms of Whiplash
When individuals are experiencing whiplash, the symptoms can appear immediately or may be delayed for 24–72 hours post-injury. Additionally, whiplash injuries are considered soft tissue injuries to the neck with various clinical symptoms that vary in severity and may include: (Chen et al., 2009)
Neck pain and stiffness
Reduced range of motion
Shoulder and upper back pain
Headaches, especially originating at the base of the skull
Jaw pain or temporomandibular joint (TMJ) dysfunction
Dizziness or visual disturbances
Tingling or numbness sensations in the arms (cervical radiculopathy)
Fatigue and cognitive issues (“whiplash-associated disorders” or WAD)
How Whiplash Affects the Cervical Spine and Musculoskeletal System
Whiplash is more than just a soft tissue injury, as it impacts several interconnected systems:
1. Cervical Spine
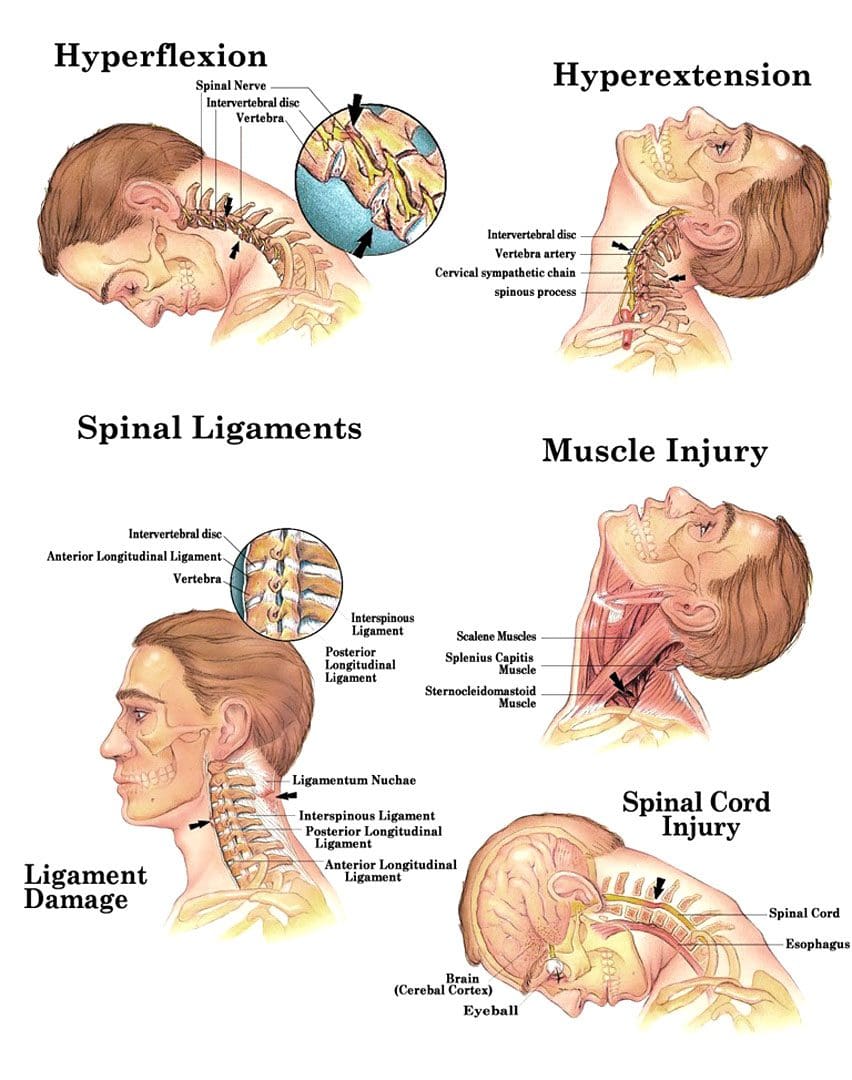
The rapid motion during a whiplash injury can lead to:
Cervical facet joint irritation
Intervertebral disc compression or herniation
Muscle strain or ligamentous sprain
Altered cervical lordosis, leading to chronic postural imbalances
This causes pain, stiffness, and tenderness in the neck area due to injuries within the bony, muscular, and ligamentous regions. (Alektoroff & Papanagiotou, 2021)
2. Musculoskeletal Dysfunction
Whiplash often initiates a cascade of biomechanical issues:
Myofascial pain syndromes, especially in the trapezius, levator scapulae, and sternocleidomastoid muscles
Compensatory thoracic or lumbar strain
Poor proprioception and neuromuscular control
Chronic trigger points and fibrotic tissue development
The longer these musculoskeletal imbalances persist, the more likely they will evolve into chronic pain syndromes and central sensitization.
Why Choose Chiropractic?-Video
Diagnosing Whiplash
Diagnosis is largely clinical, supported by a thorough history and physical exam. Imaging may be required to rule out more severe pathology:
X-rays: To rule out fractures or malalignment
MRI: For soft tissue or disc pathology
CT scans: If fracture or serious trauma is suspected
Functional assessments: Range of motion, palpation, neurologic evaluation
Evidence-Based Treatments for Whiplash
Treatment for whiplash should be multimodal and individualized, focusing on restoring function, reducing inflammation, and promoting healing. (Bussieres et al., 2016)
1. Chiropractic Care
Chiropractic adjustments can offer significant benefits in managing whiplash-associated disorders:
Myofascial release and soft tissue mobilization: Target muscle tension, trigger points, and fascial restrictions.
Postural retraining and ergonomic correction: Essential for long-term resolution.
Additionally, chiropractic patients experienced significant improvements in neck pain and function.
2. Physical Therapy
Individuals dealing with neck pain associated with whiplash can benefit from physical therapy to improve neck pain and disability. (Chrcanovic et al., 2022) Rehabilitative exercises are fundamental:
Neck range-of-motion drills
Isometric strengthening
Scapular stabilization and postural correction
Proprioceptive neuromuscular facilitation (PNF)
3. Functional Medicine Approach
From a functional medicine standpoint, addressing systemic inflammation, nutritional deficiencies, and stress response can enhance recovery:
Magnesium and B-complex supplementation for nerve healing
Sleep optimization and cortisol balance
4. Other Complementary Treatments
Acupuncture: Improves blood flow and pain modulation while alleviating pain and promoting relaxation. (Moon et al., 2014)
Gua Sha or cupping therapy: Relieves muscular tension
Dry needling: Effective for persistent trigger points
Manual lymphatic drainage: For patients experiencing edema or prolonged inflammation
Recovery and Prognosis
With consistent and proper treatment, many individuals recover within a few weeks. However, approximately 30–50% of individuals may develop chronic symptoms if not properly managed early on. Factors predicting prolonged recovery include:
High initial pain intensity
Poor coping mechanisms
History of prior neck injury
Psychosocial stressors
Early intervention using a holistic, integrative care model offers the best outcomes in preventing chronic whiplash-associated disorders.
Final Thoughts
Beyond the common “neck strain” classification, whiplash is a complicated neuromusculoskeletal injury that requires careful consideration by both patients and medical experts. Accurate diagnosis and successful treatment depend on an understanding of the complex effects on the cervical spine, neurology, and musculoskeletal function. Reducing symptoms and improving quality of life may be achieved by combining non-surgical treatments as part of a personalized treatment strategy.
Injury Medical & Personal Injury Clinic
We associate certified medical providers who understand the importance of assessing individuals with whiplash associated with their necks. When asking important questions to our associated medical providers, we advise patients to incorporate customized treatment plans for their pain associated with whiplash. Dr. Alex Jimenez, D.C., uses this information as an academic service. Disclaimer
References
Alektoroff, K., & Papanagiotou, P. (2021). [Whiplash injury of the cervical spine]. Radiologe, 61(8), 710-713. https://doi.org/10.1007/s00117-021-00877-5 (Schleudertrauma der Halswirbelsaule.)
Bussieres, A. E., Stewart, G., Al-Zoubi, F., Decina, P., Descarreaux, M., Hayden, J., Hendrickson, B., Hincapie, C., Page, I., Passmore, S., Srbely, J., Stupar, M., Weisberg, J., & Ornelas, J. (2016). The Treatment of Neck Pain-Associated Disorders and Whiplash-Associated Disorders: A Clinical Practice Guideline. J Manipulative Physiol Ther, 39(8), 523-564 e527. https://doi.org/10.1016/j.jmpt.2016.08.007
Chrcanovic, B., Larsson, J., Malmstrom, E. M., Westergren, H., & Haggman-Henrikson, B. (2022). Exercise therapy for whiplash-associated disorders: a systematic review and meta-analysis. Scand J Pain, 22(2), 232-261. https://doi.org/10.1515/sjpain-2021-0064
Moon, T. W., Posadzki, P., Choi, T. Y., Park, T. Y., Kim, H. J., Lee, M. S., & Ernst, E. (2014). Acupuncture for treating whiplash associated disorder: a systematic review of randomised clinical trials. Evid Based Complement Alternat Med, 2014, 870271. https://doi.org/10.1155/2014/870271
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine










 Common Causes Of Whiplash
Common Causes Of Whiplash





