Can individuals with low back pain find nonsurgical solutions to restore lumbar mobility and stability to the lower limbs?
Introduction
As one of the top three common problems that many young and older adults experience at some point in their lives, low back pain can have a huge impact on their routine. Back pain can often be due to normal factors like lifting heavy objects, being in a reclined position, or being physically inactive. Other times, it can be due to traumatic injuries, musculoskeletal disorders, or physical injuries. When many people are dealing with low back pain, many will often take over-the-counter medication to reduce the pain-like symptoms that they are experiencing. However, that is only a temporary solution, as the pain does come back through repetitive motions that can lead to a life of disability. To that point, many individuals, especially working adults, will have to call off work to get their lower back pain treated. This causes a socio-economic burden for many, and it can be miserable. Today’s article will examine what causes back pain and how various nonsurgical tips and tricks can reduce low back pain. We speak with certified medical providers who incorporate our patients’ information to provide multiple nonsurgical solutions to ease low back pain in many individuals. We also inform our patients of tips and tricks to reduce common back pain symptoms causing lumbar issues. We encourage our patients to ask intricated and educational questions to our associated medical providers about the pain-like symptoms they are experiencing correlating with the lower back. Dr. Alex Jimenez, D.C., utilizes this information as an academic service. Disclaimer.
What Causes Back Pain?
Do you feel constant aches or pains in your lower back after a long workday? Do you feel stiffness in your lower back muscles that hurts when stretched? Or are you in constant pain that you are unable to function throughout the entire day? Many of these scenarios that people are experiencing are correlated with low back pain. Since the back in the musculoskeletal system is a complicated structure consisting of bones, joints, ligaments, and muscles, it can succumb to various injuries, sprains, and aches, leading to lower back pain. Many individuals dealing with back pain are non-specific and can affect the state of the lumbar spinal discs. When many individuals have various physical activities, they will have disc abnormalities and low back pain. (Jensen et al., 1994) At the same time, many individuals will notice that a series of sequelae develop various pain-like symptoms that are taken into account and cause functional loss associated with acute or chronic lower back pain that can affect the lower limbs. (Hoy et al., 2014) Some of the other causes of low back pain can be musculoskeletal symptoms that can lead to a life of disability. (Malik et al., 2018) More often than not, many individuals dealing with lower back pain do recover; however, after a while, reoccurrence of lower back pain is common when the same repetitive motions are being performed and when people who had lower back pain in previous encounters will deal with chronic pain and disability. (Hartvigsen et al., 2018) Luckily, numerous treatments can help reduce the pain, like the effects of low back pain, help restore mobility to the lumbar spine, and stabilize the lower limbs.
Diabetic Back Pain Explained- Video
Have you been experiencing muscle stiffness and aches in your lower back that are affecting your lower limbs? Did you lift a heavy object that caused you to strain your back muscles and make it difficult to work? Or were you bending over to pick up an object or tie your shoes so your back muscles are aching? When many individuals are dealing with low back pain from these various scenarios, it can lead to a life of disability and misery when not treated right away. Since low back pain is a pervasive musculoskeletal disorder, many individuals have different diagnoses, which can make it difficult to treat. (Deyo et al., 1990) However, there are numerous ways that many people dealing with low back pain can find the relief they deserve. Many people will often seek various treatments that can reduce low back pain and help them regain their spinal mobility so they can get back to their daily routine. The video above explains how back pain can be associated with autoimmune disorders like diabetes and how various treatments can help reduce pain-like symptoms.
Nonsurgical Tips & Tricks To Reduce Low Back Pain
When it comes to reducing and treating low back pain, many individuals will begin to seek treatment to reduce their low back pain. Many will often go to nonsurgical treatments since they are cost-effective and can be combined with other therapies to relieve musculoskeletal pain. Nonsurgical treatments can range from spinal decompression and chiropractic care to spinal manipulation. (Chou et al., 2017) When many people are finding relief for their lower back pain, some tips and tricks that many people can do to prevent it from flaring up include:
Maintaining a healthy weight and diet
Slowly incorporating exercises
Avoid prolonging activity
Stretch
Sleep on a medium-firm mattress
Continue nonsurgical treatments to reduce the chances of low back pain returning
Maintain good posture
With these tips and tricks, many individuals will begin to notice their lower back pain reducing and promote healthy lifestyle choices.
References
Chou, R., Deyo, R., Friedly, J., Skelly, A., Hashimoto, R., Weimer, M., Fu, R., Dana, T., Kraegel, P., Griffin, J., Grusing, S., & Brodt, E. D. (2017). Nonpharmacologic Therapies for Low Back Pain: A Systematic Review for an American College of Physicians Clinical Practice Guideline. Ann Intern Med, 166(7), 493-505. https://doi.org/10.7326/M16-2459
Hartvigsen, J., Hancock, M. J., Kongsted, A., Louw, Q., Ferreira, M. L., Genevay, S., Hoy, D., Karppinen, J., Pransky, G., Sieper, J., Smeets, R. J., Underwood, M., & Lancet Low Back Pain Series Working, G. (2018). What low back pain is and why we need to pay attention. Lancet, 391(10137), 2356-2367. https://doi.org/10.1016/S0140-6736(18)30480-X
Hoy, D., March, L., Brooks, P., Blyth, F., Woolf, A., Bain, C., Williams, G., Smith, E., Vos, T., Barendregt, J., Murray, C., Burstein, R., & Buchbinder, R. (2014). The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis, 73(6), 968-974. https://doi.org/10.1136/annrheumdis-2013-204428
Jensen, M. C., Brant-Zawadzki, M. N., Obuchowski, N., Modic, M. T., Malkasian, D., & Ross, J. S. (1994). Magnetic Resonance Imaging of the Lumbar Spine in People without Back Pain. New England Journal of Medicine, 331(2), 69-73. https://doi.org/10.1056/nejm199407143310201
Malik, K. M., Beckerly, R., & Imani, F. (2018). Musculoskeletal Disorders a Universal Source of Pain and Disability Misunderstood and Mismanaged: A Critical Analysis Based on the U.S. Model of Care. Anesth Pain Med, 8(6), e85532. https://doi.org/10.5812/aapm.85532
For individuals trying to build muscle but are not seeing results, can knowing factors like what foods to eat, how to work out, and genetics help achieve meaningful muscle gains?
Muscle Growth Nutritional Mistakes
Muscle growth is an important element of overall fitness and health. Individuals can make nutritional mistakes like not eating enough protein or carbohydrates and not properly hydrating themselves which can prevent them from gaining muscle. Factors that contribute to muscle building, include:
Nutrition
Genetics
Training
Individuals who want to increase muscle mass more efficiently can rework these issues to maintain consistency and commitment to exercise and nutrition. Benefits include:
Building muscle helps strengthen bones
Improves balance
Decreases the risk of cardiovascular disease and diabetes.
Experts point out some common mistakes that can hinder muscle growth, like not eating enough protein, not consuming enough calories, overtraining, or practicing improper form and technique. As everybody is different there is no one-size-fits-all approach to building muscle or hypertrophy. These include:
Genetics
An individual’s genes contribute to how easy or difficult it can be to build muscle.
Some individuals have a higher proportion of fast-twitch muscle fibers, which increases growth potential.
The natural distribution of muscle and body fat also varies and can affect the rate and location of muscle growth.
There are also differences in individual recovery capabilities that can influence the frequency and intensity of training sessions.
Nutrition
Nutrition matters when trying to build muscle. Individuals need to eat enough protein for muscle repair and growth.
Individuals may need to consume more calories than they burn to create energy stores.
At the same time, individuals need to consume enough carbohydrates and healthy fats to fuel workouts and recovery.
Training
Gaining muscle requires regular resistance or strength training exercises.
These exercises cause micro tears in muscle fibers, which then repair and grow back stronger and larger.
Effective resistance training includes – consistency, intensity, recovery, and progressive overload.
Progressive overload means gradually increasing the weight, frequency, or number of repetitions in an exercise routine to challenge the muscles.
Muscle Strength for Healthy Aging
Research shows that performing exercises that build muscle mass can slow age-related cognitive decline and decrease the risk of neurodegenerative diseases like Alzheimer’s disease and dementia. (Joseph Michael Northey, et al., 2018)
Muscle-building exercise can also improve heart health and lower the risk of cardiovascular diseases. (Johns Hopkins Medicine. 2023)
Nutritional Mistakes
When trying to gain muscle, challenges can affect progress. Some of the most common mistakes that can delay or set back muscle growth and recommendations include.
Not Enough Protein
Eating protein like lean meats, dairy products, and seafood, is crucial for muscle repair and growth.
Not consuming enough protein makes the body unable to grow muscles, and you’ll see suboptimal improvements.
Get enough protein from various sources like beef, lamb, chicken, turkey, fish, eggs, dairy, legumes, and plant-based proteins.
However, there is a limit to how much protein the body can use effectively at one time for muscle protein synthesis.
It is recommended to distribute protein intake evenly throughout the day, aiming for about 20 to 30 grams of high-quality protein in each meal.
If the body is in a caloric deficit, the ability to grow muscle is limited.
Insufficient calorie intake can create energy deficits, making the body use muscle for energy instead of growing.
To fix this, individuals need to consume more calories than calories burned.
It can be helpful to track calorie intake with an application to make adjustments as needed.
Individuals having trouble increasing their calorie intake or there are questions about what the body needs, consult with a registered dietitian or nutritionist.
Not Enough Carbs
Carbohydrates are the body’s main energy source during high-intensity workouts.
Not consuming enough can lead to decreased performance and slower recovery.
Recommendations include consuming a variety of whole grains and minimally processed carbohydrates, such as brown rice, potatoes, sweet potatoes, oats, and quinoa.
For individuals doing regular, moderate-to-intense training, carbohydrate recommendations can range from 3 to 7 grams per kilogram of body weight per day.
For individuals doing endurance or intense frequency training routines may need to increase this range.
Not Hydrating Enough
Water is necessary for all bodily functions, including muscle contraction and repair.
For individuals who are not sure how much water they need? Recommendations include using half of an individual’s body weight as a starting point to figure out how many ounces to drink per day.
For example, individuals who weigh 140 pounds can set a baseline hydration goal of 70 ounces of water/8 cups per day which can be adjusted according to activities.
Water Intake Recommendations
The recommended total fluid intake from food and drink varies by age and sex. The general recommendations are around:
11.5 cups per day for women
15.5 cups for adult men
For just water, women need around 9 cups of fluid per day, and men need around 13 cups to replace fluids that are lost throughout the day.
However, the exact amount of water needed to stay properly hydrated also depends on an individual’s activity level and overall health. (Academy of Nutrition and Dietetics. 2022)
To prevent dehydration, sip water consistently throughout the day, especially before, during, and after workouts.
Foods with a high water content like certain fruits can help achieve daily hydration goals.
Not Enough Healthy Fats
Not consuming enough healthy fats can cause the body to not be able to produce enough hormones that support muscle growth.
Relying on supplements instead of getting nutrients from whole foods can also lead to nutritional deficiencies and imbalances.
Recommendations are to add more healthy fats, like avocados, nuts, seeds, fatty fish, and olive oil.
Forgetting Post-Workout Nutrition
After working out, the body is ready to absorb nutrients and start the process of muscle repair and growth.
The body needs nutrients to activate the recovery post-exercise
When the body lacks nutrition after a workout it can slow muscle growth and cause fatigue.
Recommendations are to pack a balance of protein and carbohydrates to refuel right after a workout.
Training Mistakes
Undertraining or performing low-intensity workouts can also slow down muscle growth.
Individuals who are not overloading their muscles – for example, using weights that are too light – will not break them down so they can grow bigger and stronger.
A lack of microdamage means muscle growth will be slower.
Muscle overload also requires rest.
Recommendations are to take at least one day of rest per week and avoid strength training in the same muscle group two days in a row.
When creating a lifting plan, be sure to include compound exercises like squats, deadlifts, and bench presses.
These exercises work with multiple muscle groups and are recommended for building strength and muscle.
A training routine should include a variety of compound movements, like lunges, split squats, leg presses, pull-downs, upright rows, and push-ups.
If unsure of which compound exercises to include, consult a personal trainer, physical therapist, or sports chiropractor.
Northey, J. M., Cherbuin, N., Pumpa, K. L., Smee, D. J., & Rattray, B. (2018). Exercise interventions for cognitive function in adults older than 50: a systematic review with meta-analysis. British journal of sports medicine, 52(3), 154–160. https://doi.org/10.1136/bjsports-2016-096587
Can healthcare providers help many individuals with lumbar disc degeneration find relief through spinal decompression treatments?
Introduction
Many individuals often do everyday motions that can allow the spine to bend, twist, and turn in various ways without feeling pain and discomfort. However, as the body ages, so does the spine, as the spinal discs begin the natural process of degeneration. Since the spinal discs in the spinal column absorb the vertical pressure weight, it stabilizes the upper and lower extremities and provides motion. To that point, when many individuals suffer from various injuries or environmental factors that cause the spinal disc to be compressed, it can lead to low back issues that cause pain and discomfort when a person is doing an activity. Since low back pain is one of the three most common problems that many people worldwide have dealt with, it can become a socio-economic issue that can lead to a life of disability and misery. Low back pain is often correlated with disc degeneration, and the surrounding ligaments and muscle tissues can affect the upper and lower extremities. This causes referred pain to the different musculoskeletal groups, causing many people to seek treatment that can not only be affordable but also effective in reducing the pain. Today’s article looks at the anatomy of the lumbar disc, how disc degeneration affects the lumbar spine, and how spinal decompression can reduce lumbar disc degeneration from causing more pain to the lower back. We speak with certified medical providers who incorporate our patients’ information to provide numerous treatment plans to ease the pain-like symptoms associated with lumbar disc degeneration causing low back pain. We also inform our patients that there are non-surgical options to reduce these pain-like issues correlated with disc degeneration and restore lumbar mobility to the body. We encourage our patients to ask intricated and educational questions to our associated medical providers about the pain-like symptoms they are experiencing correlating with the lower back. Dr. Alex Jimenez, D.C., utilizes this information as an academic service. Disclaimer.
The Anatomy Of The Lumbar Disc
Do you feel tension or stiffness in your lower back after waking up in the morning? Do you feel sudden or gradual pain from bending down to lift a heavy object that is affecting your lower back? Or do you feel the pain in one location or another in your back that is causing you pain and discomfort in your lumbar spinal region? Many of these pain-like issues are often correlated with disc degeneration combined with low back pain. The spinal disc’s anatomy comprises three elements that work together in a specific pattern to resist forces placed in the lumbar spine. (Martin et al., 2002) Since the lumbar spine is the thickest portion of the back, the spinal disc supports the upper body’s weight while stabilizing the lower body. However, the spinal disc will shrink over time when the body ages. Since degeneration is a natural process, many individuals will begin to feel less mobile, which can cause many issues within the lumbar spine.
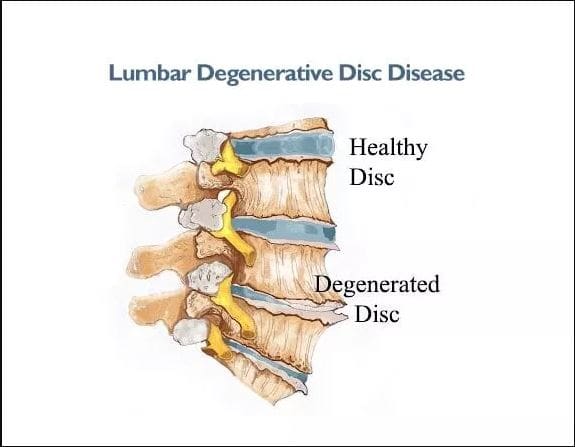
How Disc Degeneration Affects The Lumbar Spine
When disc degeneration occurs in the lumbar spine, the spinal disc begins to decrease in volume, and the nutrients that hydrate the disc start to deplete and become compressed. When disc degeneration affects the lumbar spine, the nerve roots from the central system are affected. They can be associated with any particular group of pathological conditions that may irritate the surrounding nerves and produce pain-like symptoms. (Bogduk, 1976) To that point, this causes referred pain in the lower limbs and radiating pain in the lower back. At the same time, glycosphingolipid antibodies are activated in the immune system, causing inflammatory effects. (Brisby et al., 2002) When people are dealing with low back pain associated with disc degeneration, many people will feel their lower back lock up, causing limited mobility and stiffness. At the same time, the surrounding muscle and soft tissues are overstretched and tightened. The spinal disc will also affect the nerve fibers surrounding the spine, leading to nociceptive lower back pain. (Coppes et al., 1997) However, many individuals can find available treatments to reduce low back pain associated with disc degeneration.
An Overview Of Spinal Decompression- Video
Spinal Decompression Can Reduce Lumbar Disc Degeneration
Many individuals can seek out non-surgical treatments to reduce low back pain associated with disc degeneration as it is cost-effective and, through consecutive treatments, can start feeling better. Some non-surgical treatments like spinal decompression can help rehydrate the spinal disc through gentle traction and promote natural healing. Spinal decompression can be manual or mechanical, using negative pressure to increase disc height. (Vanti et al., 2021) This allows many individuals to feel the relief they deserve and feel better over time. Spinal decompression can reduce disc degeneration, stabilize the lumbar spine, and help regain spinal mobility back to the lower portions. (Daniel, 2007) When many individuals begin to take care of their bodies and reduce the chances of low back pain from returning to cause more issues to the back.
Brisby, H., Balague, F., Schafer, D., Sheikhzadeh, A., Lekman, A., Nordin, M., Rydevik, B., & Fredman, P. (2002). Glycosphingolipid antibodies in serum in patients with sciatica. Spine (Phila Pa 1976), 27(4), 380-386. https://doi.org/10.1097/00007632-200202150-00011
Coppes, M. H., Marani, E., Thomeer, R. T., & Groen, G. J. (1997). Innervation of “painful” lumbar discs. Spine (Phila Pa 1976), 22(20), 2342-2349; discussion 2349-2350. https://doi.org/10.1097/00007632-199710150-00005
Daniel, D. M. (2007). Non-surgical spinal decompression therapy: does the scientific literature support efficacy claims made in the advertising media? Chiropr Osteopat, 15, 7. https://doi.org/10.1186/1746-1340-15-7
Martin, M. D., Boxell, C. M., & Malone, D. G. (2002). Pathophysiology of lumbar disc degeneration: a review of the literature. Neurosurg Focus, 13(2), E1. https://doi.org/10.3171/foc.2002.13.2.2
Vanti, C., Turone, L., Panizzolo, A., Guccione, A. A., Bertozzi, L., & Pillastrini, P. (2021). Vertical traction for lumbar radiculopathy: a systematic review. Arch Physiother, 11(1), 7. https://doi.org/10.1186/s40945-021-00102-5
For individuals dealing with chronic sciatica, when pain and other symptoms significantly impact daily activities and the ability to walk, can a musculoskeletal healthcare provider help relieve and manage symptoms through a multidisciplinary treatment plan?
Chronic Sciatica
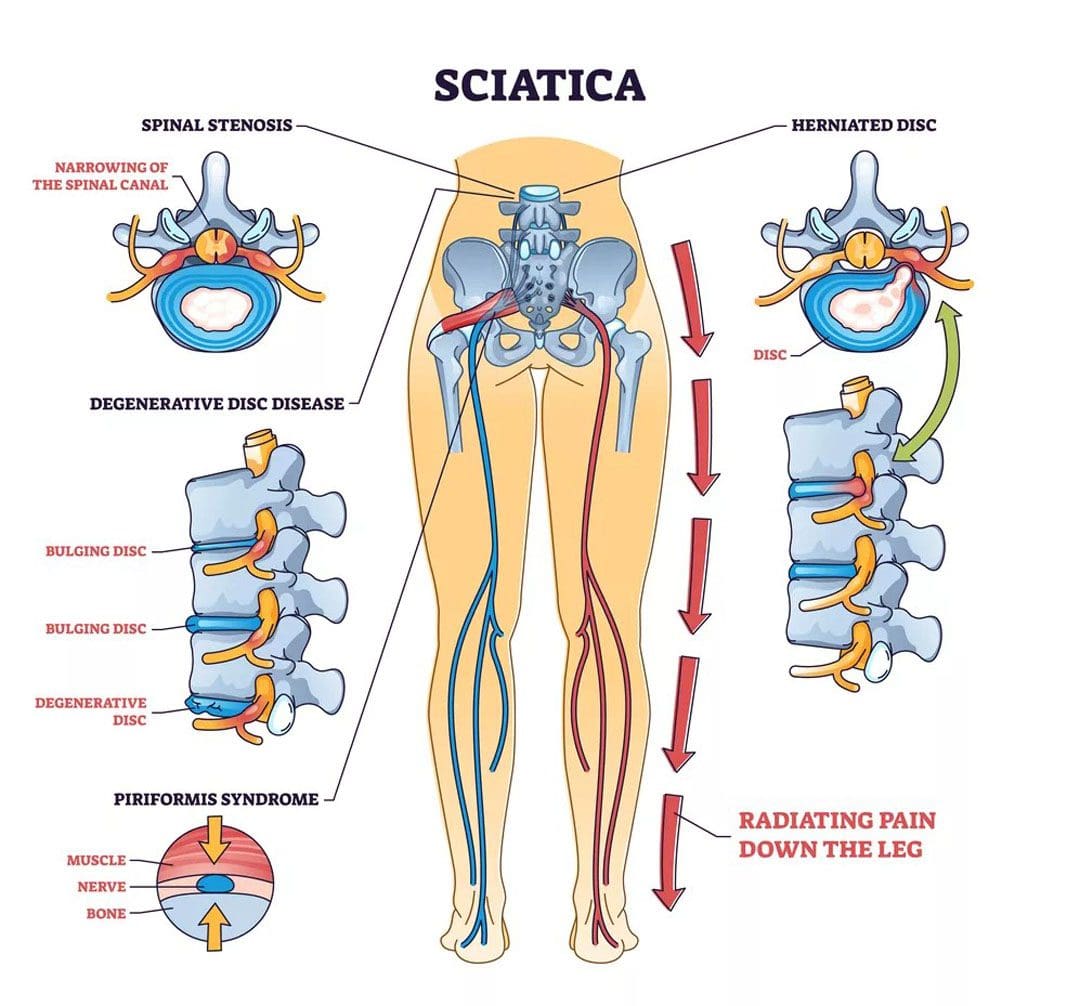
Sciatica is a common condition that results from compression of the sciatic nerve in the lower back or leg. Chronic sciatica occurs when symptoms last for 12 months or longer.
Advanced Sciatica Symptoms
Advanced or chronic sciatica usually produces pain that radiates or travels down the back of the leg. Long-term sciatic nerve compression can result in:
Leg pain
Numbness
Tingling
Electrical or burning sensations
Weakness
Weakness
Instability of the legs, which can impact the ability to walk.
Severe nerve compression can progress to leg paralysis if the nerve is significantly damaged from chronic compression. (Antonio L Aguilar-Shea, et al., 2022)
Sciatica can progress to nerve damage of the smaller nerves and travel into the legs and feet. Nerve damage/neuropathy can result in pain, tingling, and loss of sensation. (Jacob Wycher Bosma, et al., 2014)
Disabling Sciatica Treatment Options
When sciatica becomes disabling, affecting an individual’s ability to walk, more involved treatment is needed to bring relief. Many cases of chronic and disabling sciatica are caused by problems with the lumbar spine. Compression of the nerve roots that form the sciatic nerve can occur from bulging or herniated discs or spinal stenosis. If symptoms of sciatica persist beyond 12 months with little or no relief from physical therapy, non-surgical mechanical decompression, stretches and exercises, or pain management techniques, surgical procedures may be needed. (Lucy Dove, et al., 2023)
Lumbar decompression surgery encompasses several procedures to create more space in the lumbar spine and relieve nerve compression. Lumbar decompression surgery can include: (Mayfield Clinic. 2021)
Discectomy
This procedure removes a portion of a damaged disc between vertebrae to alleviate root compression from a bulging or herniated disc.
Laminectomy
This procedure removes the lamina, a portion of the vertebrae causing nerve compression, especially if there is a bone spur due to arthritic and degenerative changes in the spine.
Foraminotomy
This procedure widens the foramina, the openings in the vertebrae where the nerve roots exit to relieve compression.
Spinal Fusion
This procedure takes two or more vertebrae fusing them together with metal rods and screws for stabilization.
The procedure can be performed if:
An entire disc is removed.
Multiple laminectomies were performed.
One vertebra has slipped forward over another.
Daily Relief Management for Advanced Sciatica
Achieving relief from advanced sciatica symptoms at home can include regularly practicing methods like taking a hot bath or shower massage, and applying a heating pad to the lower back or glutes to relax tight muscles to help release the tightness surrounding the sciatic nerve.
Corrective or therapeutic exercises like sciatic nerve glides can help reduce tension along the nerve while low-back exercises that move the spine into forward or backward bending can reduce compression. (Witold Golonka, et al., 2021)
Medications like nonsteroidal anti-inflammatory drugs/NSAIDs, muscle relaxants, or nerve-pain medications may be recommended. (Antonio L Aguilar-Shea, et al., 2022)
Advanced sciatica may not be as responsive to conservative treatment methods, as the injury has set in and the nerve and surrounding tissues have become significantly restricted.
Sciatica symptoms lasting longer than 12 months require more involved treatment like injections or surgery to address symptoms effectively. (Antonio L Aguilar-Shea, et al., 2022)
Healing Chronic Sciatica
If the underlying cause can be effectively treated then chronic sciatica can be healed. Chronic sciatica often results from spinal conditions like herniated discs or lumbar spinal stenosis. These conditions narrow the space around the nerve roots that exit from the spinal cord and merge to form the sciatica nerve. Surgery is performed to open the space in the spine. (Mayfield Clinic. 2021) Sometimes sciatica is brought on by less common causes like a tumor or a spinal infection. In these cases, symptoms will not resolve until the underlying cause is addressed. Tumors may need to be surgically removed while infections require aggressive antibiotics to prevent spreading to other regions of the body. (Hospital for Special Surgery. 2023)
Pain Specialist Treatment Plan Development
Ongoing pain, numbness, tingling, and weakness are all symptoms that should be addressed with a healthcare provider. A pain specialist can help create a treatment plan that involves: (Hospital for Special Surgery. 2023)
Aguilar-Shea, A. L., Gallardo-Mayo, C., Sanz-González, R., & Paredes, I. (2022). Sciatica. Management for family physicians. Journal of family medicine and primary care, 11(8), 4174–4179. https://doi.org/10.4103/jfmpc.jfmpc_1061_21
Bosma, J. W., Wijntjes, J., Hilgevoord, T. A., & Veenstra, J. (2014). Severe isolated sciatic neuropathy due to a modified lotus position. World journal of clinical cases, 2(2), 39–41. https://doi.org/10.12998/wjcc.v2.i2.39
Dove, L., Jones, G., Kelsey, L. A., Cairns, M. C., & Schmid, A. B. (2023). How effective are physiotherapy interventions in treating people with sciatica? A systematic review and meta-analysis. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 32(2), 517–533. https://doi.org/10.1007/s00586-022-07356-y
Golonka, W., Raschka, C., Harandi, V. M., Domokos, B., Alfredson, H., Alfen, F. M., & Spang, C. (2021). Isolated Lumbar Extension Resistance Exercise in Limited Range of Motion for Patients with Lumbar Radiculopathy and Disk Herniation-Clinical Outcome and Influencing Factors. Journal of clinical medicine, 10(11), 2430. https://doi.org/10.3390/jcm10112430
For individuals dealing with chronic pain conditions can having a better understanding of pain management specialists help in developing effective multidisciplinary treatment plans?
Pain Management Specialists
Pain management is a growing medical specialty that takes a multi-disciplinary approach to treating all types of pain. It is a branch of medicine that applies scientifically proven techniques and methods to relieve, reduce, and manage pain symptoms and sensations. Pain management specialists evaluate, rehabilitate, and treat a spectrum of conditions, including neuropathic pain, sciatica, postoperative pain, chronic pain conditions, and more. Many primary healthcare providers refer their patients to pain management specialists if pain symptoms are ongoing or significant in their manifestation.
Specialists
Healthcare providers specializing in pain management recognize the complex nature of pain and approach the problem from all directions. Treatment at a pain clinic is patient-centric but depends on the clinic’s available resources. Currently, there are no set standards for the types of disciplines needed, another reason treatment options vary from clinic to clinic. Experts say that a facility should offer patients:
A coordinating practitioner specializing in pain management and consulting specialists on the patient’s behalf.
Other specialties represented in pain management are anesthesiology, neurosurgery, and internal medicine. A coordinating healthcare provider may refer an individual for services from:
A healthcare provider should have completed additional training and credentialing in pain medicine and be an MD with board certification in at least one of the following (American Board of Medical Specialties. 2023)
Anesthesiology
Physical rehabilitation
Psychiatry
Neurology
A pain management physician should also have their practice limited to the specialty they hold the certification.
Management Goals
The field of pain management treats all types of pain as a disease. Chronic, such as headaches; acute, from surgery, and more. This allows for applying science and the latest medical advances to pain relief. There are now many modalities, including:
Medication
Interventional pain management techniques – nerve blocks, spinal cord stimulators, and similar treatments.
Physical therapy
Alternative medicine
The objective is to minimize and make symptoms manageable.
Individuals determined that surgery does not benefit their condition.
A better understanding of pain syndromes by communities and insurance companies and increased pain studies will help increase insurance coverage for treatments and technology to improve interventional outcomes.
Nalamachu S. (2013). An overview of pain management: the clinical efficacy and value of treatment. The American journal of managed care, 19(14 Suppl), s261–s266.
American Society of Interventional Pain Physicians. (2023). Pain Physician.
For individuals watching their food intake during the Thanksgiving holiday, can knowing the nutritional value of turkey help maintain diet health?
Nutrition and Benefits
Minimally processed turkey can be a beneficial source of protein, vitamins, and minerals. However, processed turkey can be high in sugar, unhealthy fats, and sodium.
Sarcopenia, or muscle wasting, commonly leads to frailty in elderly individuals.
Getting enough protein at every meal is essential for older adults to maintain muscle mass and physical mobility.
Turkey can help meet guidelines suggesting lean meat consumption 4-5 times a week to maintain muscle health with aging. (Anna Maria Martone, et al., 2017)
Reduces Diverticulitis Flare-Ups
Diverticulitis is inflammation of the colon. Dietary factors that influence the risk of diverticulitis include:
Fiber intake – lowers risk.
Processed red meat intake – raises risk.
Intake of red meat with higher total fat – raises risk.
Researchers studied 253 men with diverticulitis and determined that replacing one serving of red meat with a serving of poultry or fish reduces the risk of diverticulitis by 20%. (Yin Cao et al., 2018)
The study’s limitations are that the meat intake was recorded in men only, the intake was self-reported, and the amount consumed at each eating episode was not recorded.
It may be a helpful substitution for anyone at risk for diverticulitis.
Turkey is a lean alternative to other low-sodium meats, especially if the skin is removed and cooked fresh.
Turkey is also high in the amino acid arginine.
Arginine can help keep arteries open and relaxed as a precursor to nitric oxide. (Patrick J. Skerrett, 2012)
Allergies
Meat allergies can happen at any age. A turkey allergy is possible and may be associated with allergies to other types of poultry and red meat. Symptoms can include: (American College of Allergy, Asthma & Immunology. 2019)
Martone, A. M., Marzetti, E., Calvani, R., Picca, A., Tosato, M., Santoro, L., Di Giorgio, A., Nesci, A., Sisto, A., Santoliquido, A., & Landi, F. (2017). Exercise and Protein Intake: A Synergistic Approach against Sarcopenia. BioMed research international, 2017, 2672435. https://doi.org/10.1155/2017/2672435
Cao, Y., Strate, L. L., Keeley, B. R., Tam, I., Wu, K., Giovannucci, E. L., & Chan, A. T. (2018). Meat intake and risk of diverticulitis among men. Gut, 67(3), 466–472. https://doi.org/10.1136/gutjnl-2016-313082
For individuals with back pain, how can health practitioners incorporate non-surgical solutions to reduce spinal pain?
Introduction
The spine is one of the most important structures in the human body, providing host mobility and stability when vertical pressure is pressing on the spinal structure. The spine is surrounded by various muscles, ligaments, and tissues that help support the upper and lower body portions and extremities. When normal factors like heaving lifting, improper stances, obesity, or pre-existing conditions start to affect the body, it can cause the spinal structure to potentially cause unwanted issues that lead to back, neck, and shoulder pain. When experiencing these three common body pains often correlate with other associated symptoms that can affect the other extremities. When this happens, many individuals begin to miss out on work or daily activities that can cause them to be miserable, and they even try to look for various solutions to reduce the pain they are experiencing. Today’s article looks at one of the common body pains like back pain and how it can cause numerous issues that affect a person’s ability to function, and how non-surgical solutions can not only reduce the pain-like effects but also provide the necessary relief that many people deserve in their health and wellness journey. We speak with certified medical providers who incorporate our patients’ information to provide numerous treatment plans to ease the pain-like symptoms associated with spinal issues causing back pain. We also inform our patients that there are non-surgical options to reduce these pain-like issues and restore spinal mobility to the body. We encourage our patients to ask intricated and educational questions to our associated medical providers about the pain-like symptoms they are experiencing correlating with the lower back. Dr. Alex Jimenez, D.C., utilizes this information as an academic service. Disclaimer.
Back Pain Affecting The Spine
Do you often experience radiating pain in your lower back that causes symptoms of numbness or tingling sensations down to your legs and feet? Do you feel muscle stiffness in the morning while getting up, only to slowly disappear throughout the day? Or do you feel symptoms of muscle aches and pain when carrying a heavy object from one location to another? Many individuals, more often than not, have dealt with back pain associated with various factors. With back pain being in the top three common problems in the workforce, many individuals have dealt with the common problem in multiple ways. From improper heavy lifting to excessive sitting at a desk, back pain can cause musculoskeletal issues that many are trying to find relief. Low back pain can either be acute or chronic, depending on the severity. It can lead to mobility impairment within the thoracic, lumbar, and sacroiliac spinal regions, causing referred pain to the lower extremities. It can lead to a life of impairment without any symptoms or signs of serious medical or psychological conditions associated with environmental factors. (Delitto et al., 2012) Back pain is also associated with spinal conditions like inflammation, asymmetric loading, and muscle strain, which can cause the spinal structures to be compressed, thus causing disc herniations. (Zemková & Zapletalová, 2021)
Additionally, back pain is a multifactorial musculoskeletal condition that causes many individuals to be in a socio-economic situation that can decrease their quality of life. Many examples of back pain are correlated with altered motor control within the spinal erector muscles that causes impaired proprioception in the spine. (Fagundes Loss et al., 2020) When this happens to many individuals, they often experience a hindrance of lumbar stability, body balance, posture, and postural control. At the same time, when many working individuals are having severe back pain associated with everyday factors, the amount of pain they are in can change the threshold of the mechanoreceptors that are transmitting the pain signals through the spinal cord. To this point, back pain can affect the neuromuscular response and affect normal musculoskeletal functionality. Fortunately, numerous treatments can help reduce back pain and provide relief to spinal pain that is affecting many individuals.
The Role Of Chiropractic Care- Video
How many times a day do you experience back pain associated with stiffness, general aches, or pains that are affecting your ability to work? Do you notice you hunching more when moving from one location to another? Or do you feel aches and pain in your back after stretching in the morning? Many individuals dealing with these common environmental factors are closely associated with back pain. Back pain is in the top three most common problems many individuals have experienced at some point in their lives. More often than not, many people have dealt with back pain by using home remedies to reduce the pain-like effects. However, research studies reveal that when many individuals start to ignore the pain, it can lead them to a life of disability and cause numerous amounts of distress if not treated right away. (Parker et al., 2015) Hence, non-surgical treatments can not only reduce the pain associated with back pain but also help restore spinal mobility. Non-surgical treatments like chiropractic care incorporate spinal manipulation, which can positively affect the spine. (Koes et al., 1996) What chiropractic care does is that it includes mechanical and manual manipulation techniques to stretch out tight muscles and reduce trigger points from reforming. The video above shows how chiropractic care can positively affect the individual while being part of a health and wellness journey to reducing back pain.
Non-Surgical Spinal Decompression For Back Pain
Just like chiropractic care, spinal decompression is another non-surgical treatment that uses traction to gently pull and stretch the spine to alleviate compressed spinal discs associated with back pain and help stretch out tight muscles. When many people start to incorporate spinal decompression as part of their routine, they will notice that spinal decompression can reduce intradiscal pressure within the negative range. (Ramos, 2004) What this does is that when the spinal discs are being pulled by gentle traction, all the fluids and nutrients that were not hydrating the disc flow back and help kickstart the body’s natural healing process. When many people begin to utilize spinal decompression for their back pain, they will notice a huge reduction in their pain after a few consecutive sessions. (Crisp et al., 1955) When many people start to combine other various non-surgical therapies with spinal decompression, they will be able to regain their spinal mobility while being more mindful of what environmental factors are affecting their spine and not repeat the issue to allow back pain to return.
References
Crisp, E. J., Cyriax, J. H., & Christie, B. G. (1955). Discussion on the treatment of backache by traction. Proc R Soc Med, 48(10), 805-814. https://www.ncbi.nlm.nih.gov/pubmed/13266831
Delitto, A., George, S. Z., Van Dillen, L., Whitman, J. M., Sowa, G., Shekelle, P., Denninger, T. R., & Godges, J. J. (2012). Low Back Pain. Journal of Orthopaedic & Sports Physical Therapy, 42(4), A1-A57. https://doi.org/10.2519/jospt.2012.42.4.a1
Fagundes Loss, J., de Souza da Silva, L., Ferreira Miranda, I., Groisman, S., Santiago Wagner Neto, E., Souza, C., & Tarrago Candotti, C. (2020). Immediate effects of a lumbar spine manipulation on pain sensitivity and postural control in individuals with nonspecific low back pain: a randomized controlled trial. Chiropr Man Therap, 28(1), 25. https://doi.org/10.1186/s12998-020-00316-7
Koes, B. W., Assendelft, W. J., van der Heijden, G. J., & Bouter, L. M. (1996). Spinal manipulation for low back pain. An updated systematic review of randomized clinical trials. Spine (Phila Pa 1976), 21(24), 2860-2871; discussion 2872-2863. https://doi.org/10.1097/00007632-199612150-00013
Parker, S. L., Mendenhall, S. K., Godil, S. S., Sivasubramanian, P., Cahill, K., Ziewacz, J., & McGirt, M. J. (2015). Incidence of Low Back Pain After Lumbar Discectomy for Herniated Disc and Its Effect on Patient-reported Outcomes. Clin Orthop Relat Res, 473(6), 1988-1999. https://doi.org/10.1007/s11999-015-4193-1
Ramos, G. (2004). Efficacy of vertebral axial decompression on chronic low back pain: study of dosage regimen. Neurol Res, 26(3), 320-324. https://doi.org/10.1179/016164104225014030
Zemková, E., & Zapletalová, L. (2021). Back Problems: Pros and Cons of Core Strengthening Exercises as a Part of Athlete Training. International Journal of Environmental Research and Public Health, 18(10), 5400. https://doi.org/10.3390/ijerph18105400
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine