How do healthcare professionals in a chiropractic clinic provide a clinical approach to preventing medical errors for individuals in pain?
Introduction
Medical errors resulted in 44,000–98,000 hospitalized American deaths annually, and many more caused catastrophic injuries. (Kohn et al., 2000) This was more than the number of people who died annually from AIDS, breast cancer, and auto accidents at the time. According to later research, the actual number of deaths may be closer to 400,000, placing medical errors as the third most common cause of death in the US. Frequently, these mistakes are not the product of medical professionals who are inherently bad; rather, they are the outcome of systemic issues with the health care system, such as inconsistent provider practice patterns, disjointed insurance networks, underutilization or absence of safety protocols, and uncoordinated care. Today’s article looks at the clinical approach to preventing a medical error in a clinical setting. We discuss associated medical providers specializing in various pretreatments to aid individuals suffering from chronic issues. We also guide our patients by allowing them to ask their associated medical providers very important and intricate questions. Dr. Alex Jimenez, DC, only utilizes this information as an educational service. Disclaimer
Defining Medical Errors
Determining what medical error is the most crucial step in any conversation about preventing medical errors. You might assume this is a very easy chore, but that is only until you delve into the vast array of terminology utilized. Many terms are used synonymously (sometimes mistakenly) since some terminology is interchangeable, and occasionally, the meaning of a term depends on the specialty being discussed.
Even though the healthcare sector stated that patient safety and eliminating or reducing medical errors were priorities, Grober and Bohnen noted as recently as 2005 that they had fallen short in one crucial area: determining the definition of “perhaps the most fundamental question… What is a medical error? A medical error is a failure to complete a planned action in a medical setting. (Grober & Bohnen, 2005) However, none of the terms that one would often identify expressly with a medical error—patients, healthcare, or any other element—are mentioned in this description. Despite this, the definition offers a solid framework for further development. As you can see, that specific definition consists of two parts:
An execution error: A failure to complete a planned action as intended.
A planning error: is a technique that, even with perfect execution, does not produce the desired results.
The concepts of faults of execution and planning errors are insufficient if we are to define a medical error adequately. These may occur anywhere, not only at a medical establishment. The component of medical management must be added. This brings up the idea of unfavorable occurrences, known as adverse events. The most common definition of an adverse event is unintentional harm to patients brought about by medical therapy rather than their underlying disease. This definition has gained international acceptance in one way or another. For example, in Australia, the term incidents are defined as in which harm resulted in a person receiving health care. These consist of infections, injury-causing falls, and issues with prescription drugs and medical equipment. Certain unfavorable occurrences might be avoidable.
Common Types of Medical Errors
The only issue with this notion is that not all negative things happen accidentally or intentionally. Because the patient may ultimately benefit, an expected but tolerated adverse event may occur. During chemotherapy, nausea and hair loss are two examples. In this instance, refusing the recommended treatment would be the only sensible approach to prevent the unpleasant consequence. We thus arrive at the concept of preventable and non-preventable adverse occurrences as we further refine our definition. It isn’t easy to categorize a choice to tolerate one impact when it is determined that a favorable effect will occur simultaneously. But purpose alone isn’t necessarily an excuse. (Patient Safety Network, 2016, para.3) Another example of a planned mistake would be a right foot amputation due to a tumor on the left hand, which would be accepting a known and predicted unfavorable event in the hopes of a beneficial consequence where none has ever arisen before. There is no evidence to support the anticipation of a positive outcome.
Medical errors that cause harm to the patient are typically the focus of our research. Nonetheless, medical mistakes can and do occur when a patient is not harmed. The occurrence of near misses could provide invaluable data when planning how to reduce medical errors in a healthcare facility. Still, the frequency of these events compared to the frequency clinicians report them needs to be investigated. Near misses are medical errors that could have caused harm but did not to the patient, even if the patient is doing well. (Martinez et al., 2017) Why would you acknowledge something that could potentially result in legal action? Consider the scenario where a nurse, for whatever reason, had just been looking at photographs of different medications and was about to provide a medication. Maybe something lingers in her memory, and she decides that’s not how a specific medication looks. Upon checking, she found that the incorrect medicines had been administered. After checking all the paperwork, she fixes the mistake and gives the patient the right prescription. Would it be possible to avoid an error in the future if the administration record included photographs of the proper medication? It is easy to forget that there was a mistake and a chance for harm. That fact remains true regardless of whether we were fortunate enough to find it in time or suffer any negative consequences.
Errors of Outcomes & Process
We need complete data to develop solutions that improve patient safety and decrease medical errors. At the very least, when the patient is in a medical facility, everything that can be done to prevent harm and put them in danger should be reported. Many doctors have determined that using the phrases errors and adverse events was more comprehensive and suitable after reviewing mistakes and adverse events in health care and discussing their strengths and weaknesses in 2003. This combined definition would increase data gathering, including mistakes, close calls, near misses, andactive and latent errors. Additionally, the term adverse events includes terms that usually imply patient harm, such as medical injury and iatrogenic injury. The only thing that remains is determining whether a review board is a suitable body to handle the separation of preventable and non-preventable adverse events.
A sentinel event is an occurrence where reporting to the Joint Commission is required. The Joint Commission states that a sentinel event is an unexpected occurrence involving a serious physical or psychological injury. (“Sentinel Events,” 2004, p.35) There isn’t a choice, as it needs to be documented. Most healthcare facilities, however, do keep their records outlining sentinel incidents and what to do in the event of one to guarantee that the Joint Commission standards are met. This is one of those situations when it’s better to be safe than sorry. Since “serious” is a relative concept, there may be some wriggle room when defending a coworker or an employer. On the other hand, reporting a sentinel event incorrectly is better than failing to report a sentinel event. Failing to disclose can have serious consequences, including career termination.
When considering medical errors, people frequently make the mistake of focusing just on prescription errors. Medication errors are undoubtedly frequent and involve many of the same procedural flaws as other medical errors. Breakdowns in communication, mistakes made during prescription or dispensing, and many other things are possible. But we would be gravely misjudging the issue if we assumed that drug errors are the only cause of harm to a patient. One major challenge in classifying the different medical errors is determining whether to classify the error based on the procedure involved or the consequence. It is acceptable to examine those classifications here, given numerous attempts have been made to develop working definitions that incorporate both the process and the outcome, many of which are based on Lucian Leape’s work from the 1990s.
Enhance Your Lifestyle Today- Video
Analyzing & Preventing Medical Errors
Operative and nonoperative were the two main categories of adverse events that Leape and his colleagues distinguished in this study. (Leape et al., 1991) Operative problems included wound infections, surgical failures, non-technical issues, late complications, and technical difficulties. Nonoperative: headings such as medication-related, misdiagnosed, mistreated, procedure-related, fall, fracture, postpartum, anesthesia-related, neonatal, and a catch-all heading of the system were included under this category of adverse occurrences. Leape also classified errors by pointing out the point of process breakdown. He also categorized these into five headings, which include:
System
Performance
Drug Treatment
Diagnostic
Preventative
Many process faults fall under more than one topic, yet they all help to pinpoint the exact cause of the issue. If more than one physician was engaged in determining the precise areas that need improvement, then additional questioning might be required.
Technically, a medical error can be made by any staff member at a hospital. It is not limited to medical professionals like physicians and nurses. An administrator may unlatch a door, or a cleaning crew member could leave a chemical within a child’s grasp. What matters more than the identity of the perpetrator of the mistake is the reason behind it. What before it? And how can we make sure that doesn’t occur again? After gathering all the above data and much more, it’s time to figure out how to prevent similar errors. As for sentinel events, the Joint Commission has mandated since 1997 that all of these incidents undergo a procedure called Root Cause Analysis (RCA). However, using this procedure for incidents that need to be reported to outside parties would need to be corrected.
What Is A Root Cause Analysis?
RCAs “captured the details as well as the big picture perspective.” They make evaluating systems easier, analyzing whether remedial action is necessary, and tracking trends. (Williams, 2001) What precisely is an RCA, though? By examining the events that led to the error, an RCA can focus on events and processes rather than reviewing or placing blame on specific people. (AHRQ,2017) This is why it is so crucial. An RCA frequently makes use of a tool called the Five Whys. This is the process of continuously asking yourself “why” after you believe you have determined the cause of an issue.
The reason it’s called the “five whys” is because, while five is an excellent starting point, you should always question why until you identify the underlying cause of the problem. Asking why repeatedly could reveal many process faults at different stages, but you should keep asking why about every aspect of the issue until you run out of other things that could be adjusted to provide a desirable result. However, different tools besides this one can be utilized in a root cause investigation. Numerous others exist. RCAs must be multidisciplinary and consistent and involve all parties involved in the error to avoid misunderstandings or inaccurate reporting of occurrences.
Conclusion
Medical errors in healthcare institutions are frequent and mostly unreported events that seriously threaten patients’ health. Up to a quarter of a million individuals are thought to pass away each year as a result of medical blunders. These statistics are unacceptable in a time when patient safety is supposedly the top priority, but not much is being done to alter practices. If medical errors are accurately defined and the root cause of the problem is found without assigning blame to specific staff members, this is unnecessary. Essential changes can be made when fundamental causes of system or process faults are correctly identified. A consistent, multidisciplinary approach to root cause analysis that uses frameworks like the five whys to delve down until all issues and defects are revealed is a helpful tool. Although it is now necessary for the wake of sentinel events, the Root Cause Analysis may and should be applied to all mistake causes, including near misses.
Kohn, L. T., Corrigan, J., Donaldson, M. S., & Institute of Medicine (U.S.). Committee on Quality of Health Care in America. (2000). To err is human : building a safer health system. National Academy Press. books.nap.edu/books/0309068371/html/index.html
Leape, L. L., Brennan, T. A., Laird, N., Lawthers, A. G., Localio, A. R., Barnes, B. A., Hebert, L., Newhouse, J. P., Weiler, P. C., & Hiatt, H. (1991). The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N Engl J Med, 324(6), 377-384. doi.org/10.1056/NEJM199102073240605
Martinez, W., Lehmann, L. S., Hu, Y. Y., Desai, S. P., & Shapiro, J. (2017). Processes for Identifying and Reviewing Adverse Events and Near Misses at an Academic Medical Center. Jt Comm J Qual Patient Saf, 43(1), 5-15. doi.org/10.1016/j.jcjq.2016.11.001
Can understanding the body’s hinge joints and how they operate help with mobility and flexibility problems and manage conditions for individuals with difficulty fully bending or extending their fingers, toes, elbows, ankles, or knees?
Hinge Joints
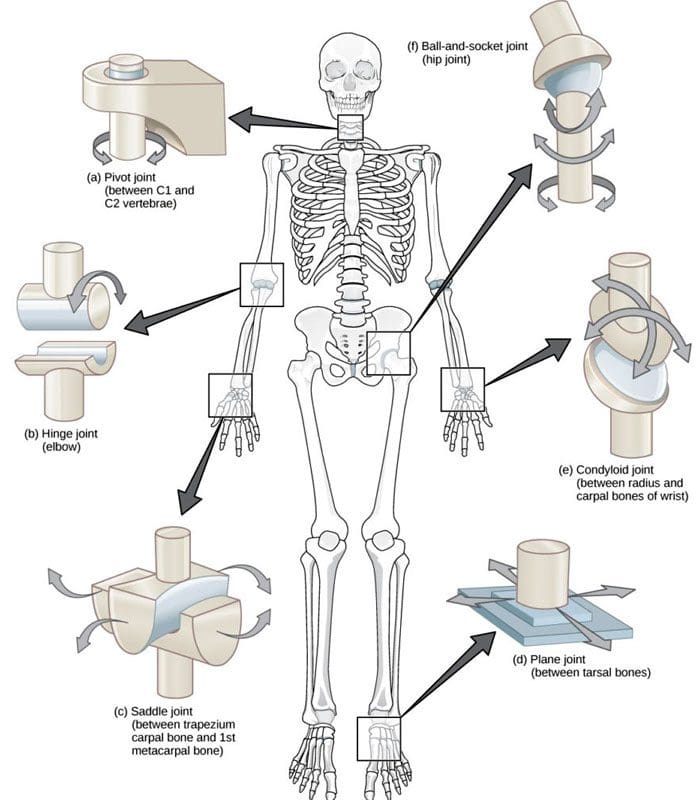
A joint forms where one bone connects to another, allowing motion. Different types of joints differ in structure and movement depending on their location. These include hinge, ball and socket, planar, pivot, saddle, and ellipsoid joints. (Boundless. General Biology, N.D.) Hinge joints are synovial joints that move through one plane of motion: flexion and extension. Hinge joints are found in the fingers, elbows, knees, ankles, and toes and control movement for various functions. Injuries, osteoarthritis, and autoimmune conditions can affect hinge joints. Rest, medication, ice, and physical therapy can help alleviate pain, improve strength and range of motion, and help manage conditions.
Anatomy
A joint is formed by the joining of two or more bones. The human body has three main classifications of joints, categorized by the degree to which they can move. These include: (Boundless. General Biology, N.D.)
Synarthroses
These are fixed, immovable joints.
Formed by two or more bones.
Amphiarthroses
Also known as cartilaginous joints.
A fibrocartilage disc separates the bones that form the joints.
These movable joints allow for a slight degree of movement.
Diarthroses
Also known as synovial joints.
These are the most common freely mobile joints that allow movement in multiple directions.
The bones that form the joints are lined with articular cartilage and enclosed in a joint capsule filled with synovial fluid that allows for smooth motion.
Synovial joints are classified into different types depending on differences in structure and the number of motion planes they allow. A hinge joint is a synovial joint that allows movement in one plane of motion, similar to a door hinge that moves forward and backward. Within the joint, the end of one bone is typically convex/pointed outward, with the other concave/rounded inward to allow the ends to fit smoothly. Because hinge joints only move through one plane of movement, they tend to be more stable than other synovial joints. (Boundless. General Biology, N.D.) Hinge joints include:
The finger and toe joints – allow the fingers and toes to bend and extend.
The elbow joint – allows the elbow to bend and extend.
The knee joint – allows the knee to bend and extend.
The talocrural joint of the ankle – allows the ankle to move up/dorsiflexion and down/plantarflexion.
Hinge joints allow the limbs, fingers, and toes to extend away and bend toward the body. This movement is essential for activities of daily living, such as showering, getting dressed, eating, walking, standing up, and sitting down.
Conditions
Osteoarthritis and inflammatory forms of arthritis can affect any joint (Arthritis Foundation. N.D.) Autoimmune inflammatory forms of arthritis, including rheumatoid and psoriatic arthritis, can cause the body to attack its own joints. These commonly affect the knees and fingers, resulting in swelling, stiffness, and pain. (Kamata, M., Tada, Y. 2020) Gout is an inflammatory form of arthritis that develops from elevated levels of uric acid in the blood and most commonly affects the hinge joint of the big toe. Other conditions that affect hinge joints include:
Injuries to the cartilage within the joints or ligaments that stabilize the outside of the joints.
Ligament sprains or tears can result from jammed fingers or toes, rolled ankles, twisting injuries, and direct impact on the knee.
These injuries can also affect the meniscus, the tough cartilage within the knee joint that helps cushion and absorb shock.
Rehabilitation
Conditions that affect hinge joints often cause inflammation and swelling, resulting in pain and limited mobility.
After an injury or during an inflammatory condition flare-up, limiting active movement and resting the affected joint can reduce increased stress and pain.
Applying ice can decrease inflammation and swelling.
Once the pain and swelling start to subside, physical and/or occupational therapy can help rehabilitate the affected areas.
A therapist will provide stretches and exercises to help improve the joint range of motion and strengthen the supporting muscles.
For individuals experiencing hinge joint pain from an autoimmune condition, biologic medications to decrease the body’s autoimmune activity are administered through infusions delivered every several weeks or months. (Kamata, M., Tada, Y. 2020)
Cortisone injections may also be used to decrease inflammation.
At Injury Medical Chiropractic and Functional Medicine Clinic, we passionately focus on treating patients’ injuries and chronic pain syndromes and improving ability through flexibility, mobility, and agility programs tailored to the individual. Our providers use an integrated approach to create personalized care plans that include Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine protocols. Our goal is to relieve pain naturally by restoring health and function to the body. If the individual needs other treatment, they will be referred to a clinic or physician best suited for them. Dr. Jimenez has teamed up with the top surgeons, clinical specialists, medical researchers, and premier rehabilitation providers to provide the most effective clinical treatments.
Kamata, M., & Tada, Y. (2020). Efficacy and Safety of Biologics for Psoriasis and Psoriatic Arthritis and Their Impact on Comorbidities: A Literature Review. International journal of molecular sciences, 21(5), 1690. doi.org/10.3390/ijms21051690
For individuals dealing with sciatica, can non-surgical treatments like chiropractic care and acupuncture reduce pain and restore function?
Introduction
The human body is a complex machine that allows the host to be mobile and stable when resting. With various muscle groups in the upper and lower body portions, the surrounding muscles, tendons, nerves, and ligaments serve a purpose for the body as they all have specific jobs in keeping the host functional. However, many individuals have developed various habits that cause strenuous activities that cause repetitive motions to their muscles and nerves and affect their musculoskeletal system. One of the nerves that many individuals have been dealing with pain is the sciatic nerve, which causes many issues in the lower body extremities and, when not treated right away, leads to pain and disability. Luckily, many individuals have sought non-surgical treatments to reduce sciatica and restore body function to the individual. Today’s article focuses on understanding sciatica and how non-surgical therapies like chiropractic care and acupuncture can help reduce the sciatic pain-like effects that are causing overlapping risk profiles in the lower body extremities. We discuss with certified medical providers who consolidate with our patients’ information to assess how sciatica is often correlated with environmental factors that cause dysfunction in the body. We also inform and guide patients on how various non-surgical treatments can help reduce sciatica and its correlating symptoms. We also encourage our patients to ask their associated medical providers many intricate and important questions about incorporating various non-surgical therapies as part of their daily routine to reduce the chances and effects of sciatica from returning. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
Understanding Sciatica
Do you often feel radiating pain that travels down one or both legs when sitting down for a long period? How often have you experienced tingling sensations that cause you to shake your leg to reduce the effect? Or have you noticed that stretching your legs causes temporary relief? While these overlapping pain symptoms can affect the lower extremities, many individuals may think it is low back pain, but in actuality, it is sciatica. Sciatica is a common musculoskeletal condition that affects many people worldwide by causing pain to the sciatic nerve and radiating down to the legs. The sciatic nerve is pivotal in providing direct and indirect motor function to the leg muscles. (Davis et al., 2024) When the sciatic nerve is compressed, many people state that the pain can vary in intensity, accompanied by symptoms like tingling, numbness, and muscle weakness that can affect a person’s ability to walk and function.
However, some of the root causes that lead to the development of sciatica can play into the factor that causes the pain in the lower extremities. Several inherent and environmental factors are often associated with sciatica, causing lumbar nerve root compression on the sciatic nerve. Factors like poor health status, physical stress, and occupational work are correlated with the development of sciatica and can impact a person’s routine. (Gimenez-Campos et al., 2022) Additionally, some of the root causes of sciatica can include musculoskeletal conditions like herniated discs, bone spurs, or spinal stenosis, which can correlate with these inherent and environmental factors that can reduce many individuals’ motility and life quality. (Zhou et al., 2021) This causes many individuals to seek out treatments to relieve sciatica pain and its correlating symptoms. While the pain caused by sciatica can vary, many individuals often seek non-surgical treatments to alleviate their discomfort and pain from sciatica. This allows them to incorporate effective solutions to managing sciatica.
Beyond Adjustments: Chiropractic & Integrative Healthcare- Video
Chiropractic Care For Sciatica
When it comes to seeking non-surgical treatments to reduce sciatica, non-surgical treatments can reduce the pain-like effects while helping restore body function and mobility. At the same time, non-surgical treatments are customized to the individual’s pain and can be incorporated into a person’s routine. Some non-surgical treatments like chiropractic care are excellent in reducing sciatica and its associated pain symptoms. Chiropractic care is a form of non-surgical therapy that focuses on restoring the body’s spinal movement while improving body function. Chiropractic care utilizes mechanical and manual techniques for sciatica to realign the spine and help the body heal naturally without surgery or medication. Chiropractic care can help decrease intradiscal pressure, increase intervertebral disc space height, and improve the range of motion in the lower extremities. (Gudavalli et al., 2016) When dealing with sciatica, chiropractic care can alleviate the unnecessary pressure on the sciatic nerve and help reduce the risk of reoccurrence through consecutive treatments.
The Effects of Chiropractic Care For Sciatica
Some of the effects of chiropractic care for reducing sciatica can provide insight to the person as chiropractors work with associated medical providers to devise a personalized plan to relieve the pain-like symptoms. Many people who utilize chiropractic care to reduce the effects of sciatica can incorporate physical therapy to strengthen the weak muscles that surround the lower back, stretch to improve flexibility and be more mindful of what factors are causing sciatic pain in their lower extremities. Chiropractic care may guide many people on proper poster ergonomics, and various exercises to reduce the chances of sciatica returning while offering positive effects to the lower body.
Acupuncture For Sciatica
Another form of non-surgical treatment that can help reduce the pain-like effects of sciatica is acupuncture. As a key component in traditional Chinese medicine, acupuncture therapy involves professionals placing thin, solid needles at specific points on the body. When it comes to reducing sciatica, acupuncture therapy can exert analgesic effects on the body’s acupoints, regulate the microglia, and modulate certain receptors along the pain pathway to the nervous system. (Zhang et al., 2023) Acupuncture therapy focuses on restoring the body’s natural energy flow or Qi to promote healing.
The Effects of Acupuncture For Sciatica
Regarding the effects of acupuncture therapy on reducing sciatica, acupuncture therapy can help reduce the pain signals that sciatica produces by changing the brain signal and rerouting the corresponding motor or sensory disturbance of the affected area. (Yu et al., 2022) Additionally, acupuncture therapy can help provide pain relief by releasing endorphins, the body’s natural pain reliever, to the specific acupoint that correlates with the sciatic nerve, reducing inflammation around the sciatic nerve, thus alleviating pressure and pain and helping improve nerve function. Both chiropractic care and acupuncture offer valuable non-surgical treatment options that can provide aid in the healing process and reduce pain caused by sciatica. When many people are dealing with sciatica and looking for numerous solutions to reduce the pain-like effects, these two non-surgical treatments can help many people address the underlying causes of sciatica, enhance the body’s natural healing process, and help provide significant relief from the pain.
Gimenez-Campos, M. S., Pimenta-Fermisson-Ramos, P., Diaz-Cambronero, J. I., Carbonell-Sanchis, R., Lopez-Briz, E., & Ruiz-Garcia, V. (2022). A systematic review and meta-analysis of the effectiveness and adverse events of gabapentin and pregabalin for sciatica pain. Aten Primaria, 54(1), 102144. doi.org/10.1016/j.aprim.2021.102144
Gudavalli, M. R., Olding, K., Joachim, G., & Cox, J. M. (2016). Chiropractic Distraction Spinal Manipulation on Postsurgical Continued Low Back and Radicular Pain Patients: A Retrospective Case Series. J Chiropr Med, 15(2), 121-128. doi.org/10.1016/j.jcm.2016.04.004
Yu, F. T., Liu, C. Z., Ni, G. X., Cai, G. W., Liu, Z. S., Zhou, X. Q., Ma, C. Y., Meng, X. L., Tu, J. F., Li, H. W., Yang, J. W., Yan, S. Y., Fu, H. Y., Xu, W. T., Li, J., Xiang, H. C., Sun, T. H., Zhang, B., Li, M. H., . . . Wang, L. Q. (2022). Acupuncture for chronic sciatica: protocol for a multicenter randomised controlled trial. BMJ Open, 12(5), e054566. doi.org/10.1136/bmjopen-2021-054566
Zhang, Z., Hu, T., Huang, P., Yang, M., Huang, Z., Xia, Y., Zhang, X., Zhang, X., & Ni, G. (2023). The efficacy and safety of acupuncture therapy for sciatica: A systematic review and meta-analysis of randomized controlled trails. Front Neurosci, 17, 1097830. doi.org/10.3389/fnins.2023.1097830
Zhou, J., Mi, J., Peng, Y., Han, H., & Liu, Z. (2021). Causal Associations of Obesity With the Intervertebral Degeneration, Low Back Pain, and Sciatica: A Two-Sample Mendelian Randomization Study. Front Endocrinol (Lausanne), 12, 740200. doi.org/10.3389/fendo.2021.740200
For individuals who suffer from migraine headaches, can incorporating physical therapy help decrease pain, improve mobility, and manage future attacks?
Migraine Physical Therapy
Cervicogenic migraine headaches can cause pain, limited motion, or confusing symptoms like dizziness or nausea. They may originate from the neck or cervical spine and be called cervicogenic headaches. A chiropractic physical therapy team can assess the spine and offer treatments that help improve mobility and decrease pain. Individuals may benefit from working with a migraine physical therapy team to perform treatments for specific conditions, quickly and safely relieving pain and returning to their previous level of activity.
Cervical Spine Anatomy
The neck is comprised of seven stacked cervical vertebrae. The cervical vertebrae protect the spinal cord and allow the neck to move through:
Flexion
Extension
Rotation
Side bending
The upper cervical vertebrae help support the skull. There are joints on either side of the cervical level. One connects to the back of the skull and allows motion. This suboccipital area is home to several muscles that support and move the head, with nerves that travel from the neck through the suboccipital area into the head. The nerves and muscles in this area may be a source of neck pain and/or headaches.
Symptoms
Sudden motions can trigger symptoms of cervicogenic migraine, or they may come on during sustained neck postures. (Page P. 2011) The symptoms are often dull and non-throbbing and may last several hours to days. Symptoms of cervicogenic migraine headache may include:
Pain on both sides of the back of the head.
Pain in the back of the head that radiates to one shoulder.
Pain on one side of the upper neck that radiates to the temple, forehead, or eye.
Pain in one side of the face or cheek.
Reduced range of motion in the neck.
Sensitivity to light or sound
Nausea
Dizziness or vertigo
Diagnosis
Tools a physician may use may include:
X-ray
MRI
CT scan
Physical examination includes neck range of motion and palpation of the neck and skull.
When first visiting a physical therapist, they will go through medical history and conditions, and questions will be asked about the onset of pain, symptom behavior, medications, and diagnostic studies. The therapist will also ask about previous treatments and review medical and surgical history. Components of the evaluation may include:
Palpation of the neck and skull
Measures of neck range of motion
Strength measurements
Postural assessment
Once the evaluation is completed, the therapist will work with the individual to develop a personalized treatment program and rehabilitation goals. Various treatments are available.
Exercise
Exercises to improve neck motion and decrease pressure on cervical nerves may be prescribed and may include. (Park, S. K. et al., 2017)
Cervical rotation
Cervical flexion
Cervical side bending
Cervical retraction
The therapist will train the individual to move slowly and steadily and avoid sudden or jerky movements.
Postural Correction
If forward head posture is present, the upper cervical spine and the suboccipital area could compress the nerves that travel up the back of the skull. Correcting posture may be an effective strategy for treatment and can include:
Performing targeted postural exercises.
Utilizing a supportive neck pillow for sleep.
Using a lumbar support when sitting.
Kinesiology taping may help increase tactile awareness of back and neck position and improve overall postural awareness.
Heat/Ice
Heat or ice may be applied to the neck and skull to help decrease pain and inflammation.
Heat can help relax tight muscles and improve circulation and may be used before performing neck stretches.
Massage
If tight muscles are limiting neck motion and causing head pain, a massage can help improve mobility.
A special technique called suboccipital release loosens the muscles that attach the skull to the neck for improved motion and decreased nerve irritation.
Manual and Mechanical Traction
Part of the migraine physical therapy plan may involve mechanical or manual traction to decompress the neck’s discs and joints, improve motion in the neck, and decrease pain.
Joint mobilizations may be used to improve neck motion and manage pain. (Paquin, J. P. 2021)
Electrical Stimulation
Electrical stimulation, like electro-acupuncture or transcutaneous neuromuscular electrical stimulation, may be used on the neck muscles to decrease pain and improve headache symptoms.
Therapy Duration
Most migraine physical therapy sessions for cervicogenic headaches last about four to six weeks. Individuals may experience relief within a few days of starting therapy, or symptoms may come and go in different phases for weeks. Some experience continued migraine headache pain for months after starting treatment and use techniques they learned to help control symptoms.
Injury Medical Chiropractic and Functional Medicine Clinic specializes in progressive therapies and functional rehabilitation procedures focused on restoring normal body functions after trauma and soft tissue injuries. We use Specialized Chiropractic Protocols, Wellness Programs, Functional and integrative Nutrition, Agility and mobility Fitness Training, and Rehabilitation Systems for all ages. Our natural programs use the body’s ability to achieve specific measured goals. We have teamed up with the city’s premier doctors, therapists, and trainers to provide high-quality treatments that empower our patients to maintain the healthiest way of living and live a functional life with more energy, a positive attitude, better sleep, and less pain.
Chiropractic Care For Migraines
References
Page P. (2011). Cervicogenic headaches: an evidence-led approach to clinical management. International journal of sports physical therapy, 6(3), 254–266.
Headache Classification Committee of the International Headache Society (IHS) (2013). The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia : an international journal of headache, 33(9), 629–808. doi.org/10.1177/0333102413485658
Rana M. V. (2013). Managing and treating headache of cervicogenic origin. The Medical clinics of North America, 97(2), 267–280. doi.org/10.1016/j.mcna.2012.11.003
Park, S. K., Yang, D. J., Kim, J. H., Kang, D. H., Park, S. H., & Yoon, J. H. (2017). Effects of cervical stretching and cranio-cervical flexion exercises on cervical muscle characteristics and posture of patients with cervicogenic headache. Journal of physical therapy science, 29(10), 1836–1840. doi.org/10.1589/jpts.29.1836
Paquin, J. P., Tousignant-Laflamme, Y., & Dumas, J. P. (2021). Effects of SNAG mobilization combined with a self-SNAG home-exercise for the treatment of cervicogenic headache: a pilot study. The Journal of manual & manipulative therapy, 29(4), 244–254. doi.org/10.1080/10669817.2020.1864960
Certain neurological disorders can cause acute episodes of peripheral neuropathy, and for individuals diagnosed with chronic peripheral neuropathy, can physical therapy help improve the ability to move around safely along with medications, procedures, and lifestyle adjustments to help control and manage symptoms?
Peripheral Neuropathy Treatments
Peripheral neuropathy treatment includes symptomatic therapies and medical management to help prevent worsening nerve damage.
For acute types of peripheral neuropathy, medical interventions and therapies can treat the underlying process, improving the condition.
For chronic types of peripheral neuropathy, medical interventions and lifestyle factors can help to prevent the condition’s progression.
Chronic peripheral neuropathy treatment focuses on controlling the pain symptoms and protecting areas of diminished sensation from damage or infection.
Self-Care and Lifestyle Adjustments
For individuals who have been diagnosed with peripheral neuropathy or are at risk of developing the condition, lifestyle factors play a significant role in managing symptoms and preventing nerve damage from worsening and can even prevent the condition from developing. (Jonathan Enders et al., 2023)
Pain Management
Individuals can try these self-care therapies and see if and which help reduce their discomfort and then develop a routine that they can work off of. Self-care for pain symptoms include:
Placing a warm heating pad on painful areas.
Placing a cooling pad (not ice) on painful areas.
Covering the area or leaving it uncovered, depending on comfort levels.
Wear loose-fitting clothes, socks, shoes, and/or gloves not made with material that can cause irritation.
Avoid using lotions or soaps that can cause irritation.
Use soothing creams or lotions.
Keeping the painful areas clean.
Injuries Prevention
Diminished sensation is one of the most common effects that can lead to problems like stumbling, difficulty getting around, and injuries. Preventing and regularly checking for injuries can help avoid complications like infected wounds. (Nadja Klafke et al., 2023) Lifestyle adjustments to manage and prevent injuries include:
Wear well-padded shoes and socks.
Inspect feet, toes, fingers, and hands regularly to look for cuts or bruises that may not have been felt.
Clean and cover cuts to avoid infections.
Use extra caution with sharp utensils like cooking and work or gardening tools.
Disease Management
Lifestyle factors can help prevent disease progression and are closely correlated with the risks and underlying causes. To help prevent peripheral neuropathy or its progression can be done by: (Jonathan Enders et al., 2023)
Maintain healthy glucose levels if you have diabetes.
Avoid alcohol for any peripheral neuropathy.
Maintain a well-balanced diet, which can include vitamin supplements, especially for vegetarians or vegans.
Over-the-Counter Therapies
A few over-the-counter therapies can help with painful symptoms and can be taken as needed. Over-the-counter pain therapies include: (Michael Überall et al., 2022)
Topical lidocaine spray, patch, or creams.
Capsaicin creams or patches.
Topical Icy Hot
Non-steroidal anti-inflammatory medications – Advil/ibuprofen or Aleve/naproxen
Tylenol/acetaminophen
These treatments can help relieve painful symptoms of peripheral neuropathy, but they do not help improve diminished sensation, weakness, or coordination problems. (Jonathan Enders et al., 2023)
Prescription Therapies
Prescription therapies for treating peripheral neuropathy include pain medications and anti-inflammatories. Chronic types of peripheral neuropathy include:
Alcoholic neuropathy
Diabetic neuropathy
Chemotherapy-induced neuropathy
The prescription treatments for chronic types differ from the treatments for acute types of peripheral neuropathy.
Pain Management
Prescription treatments can help manage the pain and discomfort. Medications include (Michael Überall et al., 2022)
Sometimes, a prescription strength supplement or vitamin B12 given through injection can help prevent progression when peripheral neuropathy is associated with a severe vitamin deficiency. Prescription treatment can help treat the underlying process in some types of acute peripheral neuropathy. Treatment for acute peripheral neuropathy, such as Miller-Fisher syndrome or Guillain-Barré syndrome, can include:
Corticosteroids
Immunoglobulins – immune system proteins
Plasmapheresis is a procedure that removes the liquid portion of blood, returning the blood cells, which modifies the overactivity of the immune system. (Sanja Horvat et al., 2022)
Researchers believe there is an association between these conditions and inflammatory nerve damage, and modifying the immune system is beneficial for treating symptoms and the underlying disease.
Surgery
In some cases, surgical procedures can benefit individuals who have certain types of peripheral neuropathy. When another condition is exacerbating the symptoms or process of peripheral neuropathy, surgery may help relieve symptoms and prevent disease progression. This has proved effective when nerve entrapment or vascular insufficiency are factors. (Wenqiang Yang et al., 2016)
Complementary and Alternative Medicine
Some complementary and alternative approaches can help individuals cope with the pain and discomfort. These treatments can serve as an ongoing option for those who have chronic peripheral neuropathy. Options can include: (Nadja Klafke et al., 2023)
Acupuncture involves the placement of needles in specific areas of the body to help reduce pain symptoms.
Acupressure involves applying pressure on specific areas of the body to help reduce pain symptoms.
Massage therapy can help relax muscle tension.
Meditation and relaxation therapies can help manage symptoms.
Physical therapy can also serve as an important component of living with chronic peripheral neuropathy and recovering from acute peripheral neuropathy.
Physical therapy can help strengthen weak muscles, improve coordination, and learn how to adapt to sensory and motor changes to get around safely.
Individuals considering complementary or alternative treatment are encouraged to speak with their primary healthcare provider to determine whether it is safe for their condition. Injury Medical Chiropractic and Functional Medicine Clinic will work with the individual’s healthcare provider and/or specialists to develop an optimal health and wellness treatment solution to provide pain relief and improve quality of life.
Peripheral Neuropathy: A Successful Recovery Story
References
Enders, J., Elliott, D., & Wright, D. E. (2023). Emerging Nonpharmacologic Interventions to Treat Diabetic Peripheral Neuropathy. Antioxidants & redox signaling, 38(13-15), 989–1000. doi.org/10.1089/ars.2022.0158
Klafke, N., Bossert, J., Kröger, B., Neuberger, P., Heyder, U., Layer, M., Winkler, M., Idler, C., Kaschdailewitsch, E., Heine, R., John, H., Zielke, T., Schmeling, B., Joy, S., Mertens, I., Babadag-Savas, B., Kohler, S., Mahler, C., Witt, C. M., Steinmann, D., … Stolz, R. (2023). Prevention and Treatment of Chemotherapy-Induced Peripheral Neuropathy (CIPN) with Non-Pharmacological Interventions: Clinical Recommendations from a Systematic Scoping Review and an Expert Consensus Process. Medical sciences (Basel, Switzerland), 11(1), 15. doi.org/10.3390/medsci11010015
Überall, M., Bösl, I., Hollanders, E., Sabatschus, I., & Eerdekens, M. (2022). Painful diabetic peripheral neuropathy: real-world comparison between topical treatment with lidocaine 700 mg medicated plaster and oral treatments. BMJ open diabetes research & care, 10(6), e003062. doi.org/10.1136/bmjdrc-2022-003062
Horvat, S., Staffhorst, B., & Cobben, J. M. G. (2022). Intravenous Lidocaine for Treatment of Chronic Pain: A Retrospective Cohort Study. Journal of pain research, 15, 3459–3467. doi.org/10.2147/JPR.S379208
Yang, W., Guo, Z., Yu, Y., Xu, J., & Zhang, L. (2016). Pain Relief and Health-Related Quality-of-Life Improvement After Microsurgical Decompression of Entrapped Peripheral Nerves in Patients With Painful Diabetic Peripheral Neuropathy. The Journal of foot and ankle surgery: official publication of the American College of Foot and Ankle Surgeons, 55(6), 1185–1189. doi.org/10.1053/j.jfas.2016.07.004
For individuals dealing with eczema, can incorporating acupuncture into a treatment plan help manage and reduce symptoms?
Acupuncture for Eczema
Eczema is a chronic skin disorder that causes intense itching, dry skin, and rashes. Common treatment options for eczema include:
Moisturizers
Topical steroids
Prescription medications
Some research suggests that acupuncture may also help individuals with eczema. In recent years, researchers have looked at acupuncture as a possible treatment option and found that it can reduce symptoms.
Acupuncture
Acupuncture involves inserting thin metallic needles in specific acupoints in the body. It is believed that by stimulating specific points, the body’s central nervous system activates and releases certain chemicals designed to enable healing. Ailments that are treated using acupuncture include: (Johns Hopkins Medicine. 2024)
Headaches
Back pain
Nausea
Asthma
Osteoarthritis
Fibromyalgia
Treatment
Studies have found that acupuncture could be a treatment option depending on the severity of the condition and the intensity of the itching sensations. (Ruimin Jiao et al., 2020) The needles are placed at various points associated with relieving the condition. These points include: (Zhiwen Zeng et al., 2021)
LI4
Located at the base of the thumb and index finger.
It has been shown to help reduce inflammation and irritation.
LI11
This point is located within the elbow to reduce itchiness and dryness.
LV3
Located on the top of the foot, this point reduces stress on the nervous system.
SP6
The SP6 is on the lower calf above the ankle and can help reduce inflammation, redness, and skin irritation.
SP10
This point is located adjacent to the knee and reduces itchiness and inflammation.
ST36
This point is located below the knee on the back of the leg and is used to improve overall well-being.
Eczema flare-ups are also linked to stress and anxiety. Acupuncture has been shown to reduce anxiety and stress, which can also help relieve eczema symptoms (Beate Wild et al., 2020).
Acupuncture helps repair skin barrier damage or the outer part of the skin designed to protect the body. (Rezan Akpinar, Saliha Karatay, 2018)
Individuals with eczema tend to have a weakened skin barrier; this benefit can also improve symptoms. (National Eczema Association. 2023)
Individuals with eczema often have an overactive immune system contributing to the disorder.
According to research, acupuncture can also help in regulating the immune system. (Zhiwen Zeng et al., 2021)
Risks
Acupuncture is generally considered safe, but there are some risks to be aware of. These risks include: (Ruimin Jiao et al., 2020)
Swelling where the needles are inserted.
Red spots on the skin.
Increased itchiness.
A rash known as erythema – occurs when small blood vessels are injured.
Most studies on acupuncture for eczema show positive results that prove it can aid in relieving symptoms. (SeHyun Kang et al., 2018) (Ruimin Jiao et al., 2020) However, individuals should talk to their healthcare provider to see if it’s a safe option.
Jiao, R., Yang, Z., Wang, Y., Zhou, J., Zeng, Y., & Liu, Z. (2020). The effectiveness and safety of acupuncture for patients with atopic eczema: a systematic review and meta-analysis. Acupuncture in medicine : journal of the British Medical Acupuncture Society, 38(1), 3–14. doi.org/10.1177/0964528419871058
Zeng, Z., Li, M., Zeng, Y., Zhang, J., Zhao, Y., Lin, Y., Qiu, R., Zhang, D. S., & Shang, H. C. (2021). Potential Acupoint Prescriptions and Outcome Reporting for Acupuncture in Atopic Eczema: A Scoping Review. Evidence-based complementary and alternative medicine : eCAM, 2021, 9994824. doi.org/10.1155/2021/9994824
Wild, B., Brenner, J., Joos, S., Samstag, Y., Buckert, M., & Valentini, J. (2020). Acupuncture in persons with an increased stress level-Results from a randomized-controlled pilot trial. PloS one, 15(7), e0236004. doi.org/10.1371/journal.pone.0236004
Akpinar R, Karatay S. (2018). Positive Effects of Acupuncture on Atopic Dermatitis. International Journal of Allergy Medications 4:030. doi.org/10.23937/2572-3308.1510030
Kang, S., Kim, Y. K., Yeom, M., Lee, H., Jang, H., Park, H. J., & Kim, K. (2018). Acupuncture improves symptoms in patients with mild-to-moderate atopic dermatitis: A randomized, sham-controlled preliminary trial. Complementary therapies in medicine, 41, 90–98. doi.org/10.1016/j.ctim.2018.08.013
Can individuals with joint hypermobility find relief through nonsurgical treatments in reducing pain and restoring body mobility?
Introduction
When a person moves their body, the surrounding muscles, joints, and ligaments are incorporated into various tasks that allow them to stretch and be flexible without pain or discomfort. Many repetitive motions enable the individual to continue their routine. However, when the joints, muscles, and ligaments are stretched farther than normal in the upper and lower extremities without pain, it is known as joint hypermobility. This connective tissue disorder can correlate with other symptoms that affect the body and cause many people to seek treatment to manage joint hypermobility symptoms. In today’s article, we will look at joint hypermobility and how various non-surgical treatments can help reduce pain caused by joint hypermobility and restore body mobility. We talk with certified medical providers who consolidate our patients’ information to assess how their pain may be associated with joint hypermobility. We also inform and guide patients on how integrating various non-surgical treatments can help improve joint function while managing the associated symptoms. We encourage our patients to ask their associated medical providers intricate and insightful questions about incorporating non-surgical therapies as part of their routine to reduce pain and discomfort from joint hypermobility. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
What Is Joint Hypermobility?
Do you often feel your joints locked up in your hands, wrists, knees, and elbows? Do you experience pain and fatigue in your joints when your body feels constantly tired? Or when you stretch your extremities, do they extend farther than usual to feel the relief? Many of these various scenarios are often correlated with individuals experiencing joint hypermobility. Joint hypermobility is an inherited disorder with autosomal dominant patterns that characterize joint hyperlaxity and musculoskeletal pain within the body extremities. (Carbonell-Bobadilla et al., 2020) This connective tissue condition is often related to the flexibility of the connected tissues like ligaments and tendons in the body. An example would be if a person’s thumb is touching their inner forearm without feeling pain or discomfort, they have joint hypermobility. Additionally, many individuals dealing with joint hypermobility will often have a difficult diagnosis as they will develop skin and tissue fragility over time, causing musculoskeletal complications. (Tofts et al., 2023)
When individuals deal with joint hypermobility over time, many often have symptomatic joint hypermobility. They will present with musculoskeletal and systemic symptoms that lead to displaying skeletal deformities, tissue and skin fragility, and structural differences in the body’s system. (Nicholson et al., 2022) Some of the symptoms that joint hypermobility are shown in a diagnosis include:
Muscle pain and joint stiffness
Clicking joints
Fatigue
Digestive issues
Balance issues
Luckily, there are various treatments that many people can use to help restrengthen the surrounding muscles around the joints and reduce the correlating symptoms caused by joint hypermobility.
Movement As Medicine-Video
Nonsurgical Treatments For Joint Hypermobility
When dealing with joint hypermobility, many individuals need to seek treatments to reduce the correlating pain-like symptoms of joint hypermobility and help relieve the body’s extremities while restoring mobility. Some excellent treatments for joint hypermobility are non-surgical therapies that are non-invasive, gentle on the joints and muscles, and cost-effective. Various non-surgical treatments can be customized for the individual depending on how severe their joint hypermobility and comorbidities affect the person’s body. Non-surgical treatments can relieve the body from joint hypermobility by treating the causes of the pain through reduction and maximizing functional capacity and restoring a person’s quality of life. (Atwell et al., 2021) The three non-surgical treatments that are excellent for reducing pain from joint hypermobility and helping strengthen the surrounding muscles are below.
Chiropractic Care
Chiropractic care utilizes spinal manipulation and helps restore joint mobility in the body to reduce the effects of joint hypermobility by stabilizing the affected joints from the hypermobile extremities. (Boudreau et al., 2020) Chiropractors incorporate mechanical and manual manipulation and various techniques to help many individuals improve their posture by being more mindful of their bodies and work with multiple other therapies to emphasize controlled movements. With other comorbidities associated with joint hypermobility, like back and neck pain, chiropractic care can reduce these comorbidity symptoms and allow the individual to regain their quality of life.
Acupuncture
Another non-surgical treatment that many individuals can incorporate to reduce joint hypermobility and its comorbidities is acupuncture. Acupuncture utilizes small, thin, solid needles that acupuncturists use to block pain receptors and restore the body’s energy flow. When many individuals are dealing with joint hypermobility, their extremities in the legs, hands, and feet are in pain over time, which can cause the body to be unstable. What acupuncture does is help reduce the pain caused by joint hypermobility associated with the extremities and restore balance and functionality to the body (Luan et al., 2023). This means that if a person is dealing with stiffness and muscle pain from joint hypermobility, acupuncture can help rewire the pain by placing the needles in the body’s acupoints to provide relief.
Physical Therapy
Physical therapy is the last non-surgical treatment many people can incorporate into their daily routine. Physical therapy can help manage joint hypermobility that are tailored to help strengthen weak muscles that are surrounding the affected joints, improving a person’s stability and helping reduce the risk of dislocation. Additionally, many individuals can use low-impact exercise to ensure optimal motor control when doing regular exercises without putting excessive strain on the joints. (Russek et al., 2022)
By incorporating these three non-surgical treatments as part of a customized treatment for joint hypermobility, many individuals will begin to feel a difference in their balance. They will not experience joint pain by being more mindful of the body and incorporating small changes in their routine. Even though living with joint hypermobility can be a challenge for many individuals, by integrating and utilizing the right combination of non-surgical treatments, many can begin to lead active and fulfilling lives.
References
Atwell, K., Michael, W., Dubey, J., James, S., Martonffy, A., Anderson, S., Rudin, N., & Schrager, S. (2021). Diagnosis and Management of Hypermobility Spectrum Disorders in Primary Care. J Am Board Fam Med, 34(4), 838-848. doi.org/10.3122/jabfm.2021.04.200374
Boudreau, P. A., Steiman, I., & Mior, S. (2020). Clinical management of benign joint hypermobility syndrome: a case series. J Can Chiropr Assoc, 64(1), 43-54. www.ncbi.nlm.nih.gov/pubmed/32476667
Carbonell-Bobadilla, N., Rodriguez-Alvarez, A. A., Rojas-Garcia, G., Barragan-Garfias, J. A., Orrantia-Vertiz, M., & Rodriguez-Romo, R. (2020). [Joint hypermobility syndrome]. Acta Ortop Mex, 34(6), 441-449. www.ncbi.nlm.nih.gov/pubmed/34020527 (Sindrome de hipermovilidad articular.)
Luan, L., Zhu, M., Adams, R., Witchalls, J., Pranata, A., & Han, J. (2023). Effects of acupuncture or similar needling therapy on pain, proprioception, balance, and self-reported function in individuals with chronic ankle instability: A systematic review and meta-analysis. Complement Ther Med, 77, 102983. doi.org/10.1016/j.ctim.2023.102983
Nicholson, L. L., Simmonds, J., Pacey, V., De Wandele, I., Rombaut, L., Williams, C. M., & Chan, C. (2022). International Perspectives on Joint Hypermobility: A Synthesis of Current Science to Guide Clinical and Research Directions. J Clin Rheumatol, 28(6), 314-320. doi.org/10.1097/RHU.0000000000001864
Russek, L. N., Block, N. P., Byrne, E., Chalela, S., Chan, C., Comerford, M., Frost, N., Hennessey, S., McCarthy, A., Nicholson, L. L., Parry, J., Simmonds, J., Stott, P. J., Thomas, L., Treleaven, J., Wagner, W., & Hakim, A. (2022). Presentation and physical therapy management of upper cervical instability in patients with symptomatic generalized joint hypermobility: International expert consensus recommendations. Front Med (Lausanne), 9, 1072764. doi.org/10.3389/fmed.2022.1072764
Tofts, L. J., Simmonds, J., Schwartz, S. B., Richheimer, R. M., O’Connor, C., Elias, E., Engelbert, R., Cleary, K., Tinkle, B. T., Kline, A. D., Hakim, A. J., van Rossum, M. A. J., & Pacey, V. (2023). Pediatric joint hypermobility: a diagnostic framework and narrative review. Orphanet J Rare Dis, 18(1), 104. doi.org/10.1186/s13023-023-02717-2
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine