Can incorporating electrical muscle stimulation help control pain, strengthen muscles, increase physical function, retrain lost movements, and/or manage inflammation for individuals experiencing neck and back pain?
Female doctor placing myostimulation physical therapy equipment on patient’s back
Electric Muscle Stimulation
Electrical muscle stimulation or E-stim is a physical therapy used to reactivate the muscles’ ability to contract. E-stim uses devices that transmit electrical impulses through the skin to target nerves and/or muscles. The most common forms include
Transcutaneous electric nerve stimulation, or TENS, is the most well-known type of electrical stimulation that offers devices that can be used at home or on the go.
Electrical muscle stimulation or EMS.
In physical therapy, E-stim stimulates muscles to contract, strengthening them and encouraging blood circulation.
Blood circulation can directly affect the condition of muscle tissue.
Electrical muscle stimulation is also used in spinal cord injury and other neuromuscular conditions. (Ho, C. H. et al., 2014)
E-stim
During treatment, electrodes are hooked to an electric stimulation machine and placed around the affected neck or back area.
The electrodes will be placed on the skin for most neck or back injuries.
The placement of the electrodes depends on the reason for treatment and the depth or superficiality of the electrical stimulation.
The electrodes are often placed near a motor point of a muscle to ensure the correct contraction.
The therapist will adjust the controls of the stimulation machine to achieve thorough muscle contraction with minimal discomfort.
Stimulation can last 5 – 15 minutes, depending on the treatment plan and injury severity.
Spinal Joint Stabilization
Activation of the muscles may help increase spinal joint stability, improving problems with spinal instability. (Ho, C. H. et al., 2014) Electric muscle stimulation is thought to enhance the exercise program a therapist prescribes to help maintain joint stability. Electrical stimulation may also help build muscle strength and endurance. (Veldman, M. P. et al., 2016) Muscle endurance is the repetitions a muscle can contract before it fatigues.
Healing and Pain Management
Electric muscle stimulation therapy can enhance tissue healing and help manage inflammation by reducing swelling and increasing circulation. It can reduce pain sensations by blocking nerve transmission at the spinal cord. (Johnson, M. I. et al., 2019) A healthcare professional may suggest a TENS or take-home electric stimulation unit to manage symptoms. (Johnson, M. I. et al., 2019)
Treatment
Interdisciplinary therapies tailored to an individual’s specific back or neck pain have been found to provide positive results. Exercise, yoga, short-term cognitive behavioral therapy, biofeedback, progressive relaxation, massage, manual therapy, and acupuncture are recommended for neck or back pain. (Chou, R. et al., 2018) Taking non-steroidal anti-inflammatory medications may also help. Electrical muscle stimulation could be an effective neck or back treatment.
Individuals unsure whether they need or would benefit from electrical should discuss symptoms and conditions with a primary physician, healthcare provider, or specialist to guide them in the right direction and determine the best treatment. Injury Medical Chiropractic and Functional Medicine Clinic focuses on what works for the patient and strives to better the body through researched methods and total wellness programs. Using an integrated approach, we treat injuries and chronic pain syndromes through personalized care plans that improve ability through flexibility, mobility, and agility programs personalized to the individual to relieve pain. If other treatment is needed, Dr. Jimenez has teamed up with the top surgeons, clinical specialists, medical researchers, and premier rehabilitation providers to provide the most effective treatments.
Thoracic Spine Pain
References
Ho, C. H., Triolo, R. J., Elias, A. L., Kilgore, K. L., DiMarco, A. F., Bogie, K., Vette, A. H., Audu, M. L., Kobetic, R., Chang, S. R., Chan, K. M., Dukelow, S., Bourbeau, D. J., Brose, S. W., Gustafson, K. J., Kiss, Z. H., & Mushahwar, V. K. (2014). Functional electrical stimulation and spinal cord injury. Physical medicine and rehabilitation clinics of North America, 25(3), 631–ix. https://doi.org/10.1016/j.pmr.2014.05.001
Veldman, M. P., Gondin, J., Place, N., & Maffiuletti, N. A. (2016). Effects of Neuromuscular Electrical Stimulation Training on Endurance Performance. Frontiers in physiology, 7, 544. https://doi.org/10.3389/fphys.2016.00544
Johnson, M. I., Jones, G., Paley, C. A., & Wittkopf, P. G. (2019). The clinical efficacy of transcutaneous electrical nerve stimulation (TENS) for acute and chronic pain: a protocol for a meta-analysis of randomised controlled trials (RCTs). BMJ open, 9(10), e029999. https://doi.org/10.1136/bmjopen-2019-029999
Chou, R., Côté, P., Randhawa, K., Torres, P., Yu, H., Nordin, M., Hurwitz, E. L., Haldeman, S., & Cedraschi, C. (2018). The Global Spine Care Initiative: applying evidence-based guidelines on the non-invasive management of back and neck pain to low- and middle-income communities. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 27(Suppl 6), 851–860. https://doi.org/10.1007/s00586-017-5433-8
For individuals who have exhausted all other treatment options for low back pain and nerve root compression, can laser spine surgery help alleviate nerve compression and provide long-lasting pain relief?
Laser Spine Surgery
Laser spine surgery is a minimally invasive surgical procedure that uses a laser to cut through and remove spinal structures that are compressing nerves and causing intense pain. The minimally invasive procedure often results in less pain, tissue damage, and faster recovery than more extensive surgeries.
How It Works
Minimally invasive procedures result in less scarring and damage to surrounding structures, often reducing pain symptoms and a shorter recovery time. (Stern, J. 2009) Small incisions are made to access spinal column structures. With open-back surgery, a large incision is made down the back to access the spine. The surgery differs from other surgeries in that a laser beam, rather than other surgical instruments, is used to cut structures in the spine. However, the initial incision through the skin is made with a surgical scalpel. Laser is an acronym for Light Amplification Stimulated by Emission of Radiation. A laser can generate intense heat to cut through soft tissues, especially those with a high water content, like spinal column discs. (Stern, J. 2009) For many spine surgeries, the laser cannot be used to cut through bone as it generates instant sparks that can damage surrounding structures. Rather, laser spine surgery is primarily used to perform a discectomy, which is a surgical technique that removes a portion of a bulging or herniated disc that is pushing against the surrounding nerve roots, causing nerve compression and sciatic pain. (Stern, J. 2009)
Surgical Risks
Laser spine surgery may help resolve the cause of nerve root compression, but there is an increased risk of damage to nearby structures. Associated risks include: (Brouwer, P. A. et al., 2015)
Infection
Bleeding
Blood clots
Remaining symptoms
Returning symptoms
Further nerve damage
Damage to the membrane around the spinal cord.
Need for additional surgery
A laser beam is not precise like other surgical tools and requires practiced mastery and control to avoid damage to the spinal cord and nerve roots. (Stern, J. 2009) Because lasers cannot cut through bone, other surgical instruments are often used around corners and at different angles because they are more efficient and allow greater accuracy. (Atlantic Brain and Spine, 2022)
Purpose
Laser spine surgery is performed to remove structures that are causing nerve root compression. Nerve root compression is associated with the following conditions (Cleveland Clinic. 2018)
Bulging discs
Herniated discs
Sciatica
Spinal stenosis
Spinal cord tumors
Nerve roots that are injured or damaged and constantly send chronic pain signals can be ablated with laser surgery, known as nerve ablation. The laser burns and destroys the nerve fibers. (Stern, J. 2009) Because laser spine surgery is limited in treating certain spinal disorders, most minimally invasive spine procedures do not use a laser. (Atlantic Brain and Spine. 2022)
Preparation
The surgical team will provide more detailed instructions on what to do in the days and hours before surgery. To promote optimal healing and a smooth recovery, it is recommended that the patient stay active, eat a healthy diet, and stop smoking prior to the operation. Individuals may need to stop taking certain medications to prevent excess bleeding or interaction with anesthesia during the operation. Inform the healthcare provider about all prescriptions, over-the-counter drugs, and supplements being taken.
Laser spine surgery is an outpatient procedure at a hospital or outpatient surgical center. The patient will likely go home on the same day of the operation. (Cleveland Clinic. 2018) Patients cannot drive to or from the hospital before or after their surgery, so arrange for family or friends to provide transportation. Minimizing stress and prioritizing healthy mental and emotional well-being is important to lowering inflammation and aiding recovery. The healthier the patient goes into surgery, the easier the recovery and rehabilitation will be.
Expectations
The surgery will be decided by the patient and healthcare provider and scheduled at a hospital or outpatient surgical center. Arrange for a friend or family member to drive to the surgery and home.
Before Surgery
The patient will be taken to a pre-operative room and asked to change into a gown.
The patient will undergo a brief physical examination and answer questions about medical history.
The patient lies on a hospital bed, and a nurse inserts an IV to deliver medication and fluids.
The surgical team will use the hospital bed to transport the patient in and out of the operating room.
The surgical team will assist the patient in getting onto the operating table, and the patient will be administered anesthesia.
The patient may receive general anesthesia, which will cause the patient to sleep for the surgery, or regional anesthesia, injected into the spine to numb the affected area. (Cleveland Clinic. 2018)
The surgical team will sterilize the skin where the incision will be made.
An antiseptic solution will be used to kill bacteria and prevent the risk of infection.
Once sanitized, the body will be covered with sterilized linens to keep the surgical site clean.
During Surgery
For a discectomy, the surgeon will make a small incision less than one inch in length with a scalpel along the spine to access the nerve roots.
A surgical tool called an endoscope is a camera inserted into the incision to view the spine. (Brouwer, P. A. et al., 2015)
Once the problematic disc portion causing the compression is located, the laser is inserted to cut through it.
The cut disc portion is removed, and the incision site is sutured.
After Surgery
After surgery, the patient is brought to a recovery room, where vital signs are monitored as the effects of the anesthesia wear off.
Once stabilized, the patient can usually go home one or two hours after the operation.
The surgeon will determine when the individual is clear to resume driving.
Recovery
Following a discectomy, the individual can return to work within a few days to a few weeks, depending on the severity, but it can take up to three months to return to normal activities. Length of recovery can range from two to four weeks or less to resume a sedentary job or eight to 12 weeks for a more physically demanding job that requires heavy lifting. (University of Wisconsin School of Medicine and Public Health, 2021) During the first two weeks, the patient will be given restrictions to facilitate the spine’s healing until it becomes more stable. Restrictions can include: (University of Wisconsin School of Medicine and Public Health, 2021)
No bending, twisting, or lifting.
No strenuous physical activity, including exercise, housework, yard work, and sex.
No alcohol in the initial stage of recovery or while taking narcotic pain medications.
No driving or operating a motor vehicle until discussed with the surgeon.
The healthcare provider may recommend physical therapy to relax, strengthen, and maintain musculoskeletal health. Physical therapy may be two to three times weekly for four to six weeks.
Process
Optimal recovery recommendations include:
Getting enough sleep, at least seven to eight hours.
Maintaining a positive attitude and learning how to cope and manage stress.
Maintaining body hydration.
Following the exercise program as prescribed by the physical therapist.
Practicing healthy posture with sitting, standing, walking, and sleeping.
Staying active and limiting the amount of time spent sitting. Try to get up and walk every one to two hours during the day to stay active and prevent blood clots. Gradually increase the amount of time or distance as recovery progresses.
Do not push to do too much too soon. Overexertion can increase pain and delay recovery.
Learning correct lifting techniques to utilize the core and leg muscles to prevent increased pressure on the spine.
Discuss treatment options for managing symptoms with a healthcare provider or specialist to determine if laser spine surgery is appropriate. Injury Medical Chiropractic and Functional Medicine Clinic care plans and clinical services are specialized and focused on injuries and the complete recovery process. Dr. Jimenez has teamed with the top surgeons, clinical specialists, medical researchers, therapists, trainers, and premiere rehabilitation providers. We focus on restoring normal body functions after trauma and soft tissue injuries using Specialized Chiropractic Protocols, Wellness Programs, Functional and integrative Nutrition, Agility and mobility Fitness Training, and Rehabilitation Systems for all ages. Our areas of practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
The Non-Surgical Approach
References
Stern, J. SpineLine. (2009). Lasers in Spine Surgery: A Review. Current Concepts, 17-23. https://www.spine.org/Portals/0/assets/downloads/KnowYourBack/LaserSurgery.pdf
Brouwer, P. A., Brand, R., van den Akker-van Marle, M. E., Jacobs, W. C., Schenk, B., van den Berg-Huijsmans, A. A., Koes, B. W., van Buchem, M. A., Arts, M. P., & Peul, W. C. (2015). Percutaneous laser disc decompression versus conventional microdiscectomy in sciatica: a randomized controlled trial. The spine journal : official journal of the North American Spine Society, 15(5), 857–865. https://doi.org/10.1016/j.spinee.2015.01.020
Atlantic Brain and Spine. (2022). The Truth About Laser Spine Surgery [2022 Update]. Atlantic Brain and Spine Blog. https://www.brainspinesurgery.com/blog/the-truth-about-laser-spine-surgery-2022-update?rq=Laser%20Spine%20Surgery
Cleveland Clinic. (2018). Can Laser Spine Surgery Fix Your Back Pain? https://health.clevelandclinic.org/can-laser-spine-surgery-fix-your-back-pain/
University of Wisconsin School of Medicine and Public Health. (2021). Home Care Instructions after Lumbar Laminectomy, Decompression or Discectomy Surgery. https://patient.uwhealth.org/healthfacts/4466
For individuals who suffer from migraine headaches, can incorporating physical therapy help decrease pain, improve mobility, and manage future attacks?
Migraine Physical Therapy
Cervicogenic migraine headaches can cause pain, limited motion, or confusing symptoms like dizziness or nausea. They may originate from the neck or cervical spine and be called cervicogenic headaches. A chiropractic physical therapy team can assess the spine and offer treatments that help improve mobility and decrease pain. Individuals may benefit from working with a migraine physical therapy team to perform treatments for specific conditions, quickly and safely relieving pain and returning to their previous level of activity.
Cervical Spine Anatomy
The neck is comprised of seven stacked cervical vertebrae. The cervical vertebrae protect the spinal cord and allow the neck to move through:
Flexion
Extension
Rotation
Side bending
The upper cervical vertebrae help support the skull. There are joints on either side of the cervical level. One connects to the back of the skull and allows motion. This suboccipital area is home to several muscles that support and move the head, with nerves that travel from the neck through the suboccipital area into the head. The nerves and muscles in this area may be a source of neck pain and/or headaches.
Symptoms
Sudden motions can trigger symptoms of cervicogenic migraine, or they may come on during sustained neck postures. (Page P. 2011) The symptoms are often dull and non-throbbing and may last several hours to days. Symptoms of cervicogenic migraine headache may include:
Pain on both sides of the back of the head.
Pain in the back of the head that radiates to one shoulder.
Pain on one side of the upper neck that radiates to the temple, forehead, or eye.
Pain in one side of the face or cheek.
Reduced range of motion in the neck.
Sensitivity to light or sound
Nausea
Dizziness or vertigo
Diagnosis
Tools a physician may use may include:
X-ray
MRI
CT scan
Physical examination includes neck range of motion and palpation of the neck and skull.
When first visiting a physical therapist, they will go through medical history and conditions, and questions will be asked about the onset of pain, symptom behavior, medications, and diagnostic studies. The therapist will also ask about previous treatments and review medical and surgical history. Components of the evaluation may include:
Palpation of the neck and skull
Measures of neck range of motion
Strength measurements
Postural assessment
Once the evaluation is completed, the therapist will work with the individual to develop a personalized treatment program and rehabilitation goals. Various treatments are available.
Exercise
Exercises to improve neck motion and decrease pressure on cervical nerves may be prescribed and may include. (Park, S. K. et al., 2017)
Cervical rotation
Cervical flexion
Cervical side bending
Cervical retraction
The therapist will train the individual to move slowly and steadily and avoid sudden or jerky movements.
Postural Correction
If forward head posture is present, the upper cervical spine and the suboccipital area could compress the nerves that travel up the back of the skull. Correcting posture may be an effective strategy for treatment and can include:
Performing targeted postural exercises.
Utilizing a supportive neck pillow for sleep.
Using a lumbar support when sitting.
Kinesiology taping may help increase tactile awareness of back and neck position and improve overall postural awareness.
Heat/Ice
Heat or ice may be applied to the neck and skull to help decrease pain and inflammation.
Heat can help relax tight muscles and improve circulation and may be used before performing neck stretches.
Massage
If tight muscles are limiting neck motion and causing head pain, a massage can help improve mobility.
A special technique called suboccipital release loosens the muscles that attach the skull to the neck for improved motion and decreased nerve irritation.
Manual and Mechanical Traction
Part of the migraine physical therapy plan may involve mechanical or manual traction to decompress the neck’s discs and joints, improve motion in the neck, and decrease pain.
Joint mobilizations may be used to improve neck motion and manage pain. (Paquin, J. P. 2021)
Electrical Stimulation
Electrical stimulation, like electro-acupuncture or transcutaneous neuromuscular electrical stimulation, may be used on the neck muscles to decrease pain and improve headache symptoms.
Therapy Duration
Most migraine physical therapy sessions for cervicogenic headaches last about four to six weeks. Individuals may experience relief within a few days of starting therapy, or symptoms may come and go in different phases for weeks. Some experience continued migraine headache pain for months after starting treatment and use techniques they learned to help control symptoms.
Injury Medical Chiropractic and Functional Medicine Clinic specializes in progressive therapies and functional rehabilitation procedures focused on restoring normal body functions after trauma and soft tissue injuries. We use Specialized Chiropractic Protocols, Wellness Programs, Functional and integrative Nutrition, Agility and mobility Fitness Training, and Rehabilitation Systems for all ages. Our natural programs use the body’s ability to achieve specific measured goals. We have teamed up with the city’s premier doctors, therapists, and trainers to provide high-quality treatments that empower our patients to maintain the healthiest way of living and live a functional life with more energy, a positive attitude, better sleep, and less pain.
Chiropractic Care For Migraines
References
Page P. (2011). Cervicogenic headaches: an evidence-led approach to clinical management. International journal of sports physical therapy, 6(3), 254–266.
Headache Classification Committee of the International Headache Society (IHS) (2013). The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia : an international journal of headache, 33(9), 629–808. https://doi.org/10.1177/0333102413485658
Rana M. V. (2013). Managing and treating headache of cervicogenic origin. The Medical clinics of North America, 97(2), 267–280. https://doi.org/10.1016/j.mcna.2012.11.003
Park, S. K., Yang, D. J., Kim, J. H., Kang, D. H., Park, S. H., & Yoon, J. H. (2017). Effects of cervical stretching and cranio-cervical flexion exercises on cervical muscle characteristics and posture of patients with cervicogenic headache. Journal of physical therapy science, 29(10), 1836–1840. https://doi.org/10.1589/jpts.29.1836
Paquin, J. P., Tousignant-Laflamme, Y., & Dumas, J. P. (2021). Effects of SNAG mobilization combined with a self-SNAG home-exercise for the treatment of cervicogenic headache: a pilot study. The Journal of manual & manipulative therapy, 29(4), 244–254. https://doi.org/10.1080/10669817.2020.1864960
For individuals experiencing shoulder and upper back pain, could periscapular bursitis be a possible cause?
Periscapular Bursitis
The scapula/shoulder blade is a bone that shifts position with upper body and shoulder movement. The scapula motion is critical to the normal function of the shoulder and the spine. When abnormal or sudden shoulder movements occur, inflammation and pain symptoms can develop. (Augustine H. Conduah et al., 2010)
Normal Scapula Function
The scapula is a triangular bone on the upper back outside the rib cage. Its outer or lateral side contains the shoulder joint socket /glenoid, while the rest of the bone serves as attachment points for the different shoulder and back muscles. The scapula shifts on the rib cage when moving the arm forward and back. This movement is called scapulothoracic motion and is critical to the normal function of the upper extremity and the shoulder joint. When the scapula does not glide in a coordinated motion, the function of the torso and shoulder joints can become stiff and painful. (J. E. Kuhn et al., 1998)
Scapular Bursa
A bursa is a fluid-filled sac that allows smooth, gliding motion between structures, body tissues, bones, and tendons. Bursae are found throughout the body, including those in front of the kneecap, outside the hip, and at the shoulder joint. When a bursa becomes inflamed and irritated, normal movements can become painful. There are bursae around the scapula in the upper back. Two of these bursa sacs are between the bones and the serratus anterior muscle that controls scapular movement on the chest wall. One bursa sac is located on the upper corner of the scapula, close to the spine at the base of the neck, and the other is at the bottom corner of the scapula, close to the mid-back. Either or both bursa sacs can be affected by periscapular bursitis. There are other bursae around the scapula and the surrounding tendons, but the two corner sacs tend to be the primary bursae that develop periscapular bursitis.
Inflammation
When these bursae become inflamed and irritated, swollen, and thickened, the condition known as bursitis results. When bursitis occurs near the scapula, muscle, and shoulder blade movements can lead to discomfort and pain. The most common symptoms of periscapular bursitis include:
An examination of the scapula may display abnormal movements of the shoulder blade. This can lead to winging, where the shoulder blade is not held correctly to the rib cage and protrudes abnormally. Individuals with winging of the scapula typically have abnormal shoulder joint mechanics because the shoulder’s positioning is altered.
Causes
The causes of periscapular bursitis can be varied. The most common is overuse syndrome, where a specific activity is causing irritation to the bursa. These can include:
Sports-related activities that result from repetitive use.
Work-related activities that result from repetitive use.
Traumatic injuries that cause inflammation or irritation to the bursa.
Some conditions can cause abnormal anatomy or bone protuberances, irritating the bursa. One condition is a benign bone growth known as an osteochondroma. (Antônio Marcelo Gonçalves de Souza and Rosalvo Zósimo Bispo Júnior 2014) These growths can project off the scapula, leading to irritation and inflammation.
Treatment
Treatment of periscapular bursitis begins with conservative therapies. Invasive treatments are rarely needed to correct the problem. Treatment can include:
Rest
The first step is to rest the irritated bursa and settle the inflammation.
This can take a few weeks and can be accomplished by modifying physical, sports, or work-related activities.
Ice
Ice is useful for reducing inflammation and controlling pain.
Knowing how to ice an injury properly can help manage the pain and swelling.
Physical Therapy
Physical therapy can alleviate the symptoms of inflammation through various exercises and stretches.
The therapy can improve scapular mechanics so the injury does not become ongoing and recurrent.
Abnormal movement of the scapula on the rib cage can not only lead to the development of bursitis, but if these abnormal mechanics are not addressed, the problem may recur.
Anti-Inflammatory Medications
Non-steroidal anti-inflammatory medications are used to control the inflammation in the short term. (Augustine H. Conduah et al., 2010)
The medications can help block the inflammatory response.
Before taking any medication, individuals should confirm with their healthcare provider that it is safe.
Cortisone Injections
Successful treatment with a cortisone shot is a sign that surgery will be more effective for individuals who may need surgery.
Cortisone injections can be very helpful in delivering a powerful anti-inflammatory dose directly to the site of inflammation. (Augustine H. Conduah et al., 2010)
Cortisone injections should be limited in terms of how many injections are offered to an individual, but in limited doses can be very helpful.
However, cortisone shots should only be performed once the diagnosis is confirmed.
Surgery
Surgery is seldom necessary but can be effective in individuals who are unable to find relief with conservative treatments.
Surgery is often used for individuals with abnormal scapular anatomy, like bone growths or tumors.
At Injury Medical Chiropractic and Functional Medicine Clinic, we treat injuries and chronic pain syndromes by improving an individual’s ability through flexibility, mobility, and agility programs tailored for all age groups and disabilities. Our chiropractor care plans and clinical services are specialized and focused on injuries and the complete recovery process. If other treatment is needed, individuals will be referred to a clinic or physician best suited to their injury, condition, and/or ailment.
Scapular Winging in Depth
References
Conduah, A. H., Baker, C. L., 3rd, & Baker, C. L., Jr (2010). Clinical management of scapulothoracic bursitis and the snapping scapula. Sports health, 2(2), 147–155. https://doi.org/10.1177/1941738109338359
Kuhn, J. E., Plancher, K. D., & Hawkins, R. J. (1998). Symptomatic scapulothoracic crepitus and bursitis. The Journal of the American Academy of Orthopaedic Surgeons, 6(5), 267–273. https://doi.org/10.5435/00124635-199809000-00001
de Souza, A. M., & Bispo Júnior, R. Z. (2014). Osteochondroma: ignore or investigate?. Revista brasileira de ortopedia, 49(6), 555–564. https://doi.org/10.1016/j.rboe.2013.10.002
For individuals experiencing or managing low back pain and/or sciatica, can lumbar traction therapy help provide consistent relief?
Lumbar Traction
Lumbar traction therapy for lower back pain and sciatica could be a treatment option to help restore mobility and flexibility and safely support an individual’s return to an optimal level of activity. It is often combined with targeted therapeutic exercise. (Yu-Hsuan Cheng, et al., 2020) The technique stretches the space between the vertebrae in the lower spine, relieving lower back pain.
Lumbar or low back traction helps to separate the spaces between the vertebrae.
Separating the bones restores circulation and helps relieve the pressure on pinched nerves like the sciatic nerve, decreasing pain and improving mobility.
Research
Researchers say lumbar traction with exercise did not improve individual outcomes compared to physical therapy exercises on their own (Anne Thackeray et al., 2016). The study examined 120 participants with back pain and nerve root impingement who were randomly selected to undergo lumbar traction with exercises or simple exercises for pain. Extension-based exercises focused on bending the spine backward. This movement is considered effective for individuals with back pain and pinched nerves. The results indicated that adding lumbar traction to physical therapy exercises did not offer significant benefits over extension-based exercise alone for back pain. (Anne Thackeray et al., 2016)
A 2022 study found that lumbar traction is helpful for individuals with lower back pain. The study investigated two different lumbar traction techniques and found that variable-force lumbar traction and high-force lumbar traction helped to relieve lower back pain. High-force lumbar traction was also found to reduce functional disability. (Zahra Masood et al., 2022) Another study found lumbar traction improves the range of motion in the straight leg raise test. The study examined different forces of traction on herniated discs. All the levels improved the individuals’ range of motion, but the one-half body-weight traction setting was associated with the most significant pain relief. (Anita Kumari et al., 2021)
Treatment
For individuals with only low back pain, exercise, and postural correction may be all that is needed to provide relief. Research confirms physical therapy exercises can help decrease pain and improve mobility (Anita Slomski 2020). Another study revealed the importance of centralizing sciatic symptoms during repetitive movements. Centralization is moving the pain back to the spine, which is a positive sign that the nerves and discs are healing and occurs during therapeutic exercise. (Hanne B. Albert et al., 2012) A chiropractor and physical therapy team can educate patients on preventing back pain episodes. Chiropractors and physical therapists are body movement experts who can show which exercises are best for your condition. Starting an exercise program that centralizes symptoms can help individuals return to their normal lifestyle quickly and safely. Consult a healthcare provider before starting any exercise program for back pain.
Movement Medicine: Chiropractic
References
Cheng, Y. H., Hsu, C. Y., & Lin, Y. N. (2020). The effect of mechanical traction on low back pain in patients with herniated intervertebral disks: a systemic review and meta-analysis. Clinical rehabilitation, 34(1), 13–22. https://doi.org/10.1177/0269215519872528
Thackeray, A., Fritz, J. M., Childs, J. D., & Brennan, G. P. (2016). The Effectiveness of Mechanical Traction Among Subgroups of Patients With Low Back Pain and Leg Pain: A Randomized Trial. The Journal of orthopaedic and sports physical therapy, 46(3), 144–154. https://doi.org/10.2519/jospt.2016.6238
Masood, Z., Khan, A. A., Ayyub, A., & Shakeel, R. (2022). Effect of lumbar traction on discogenic low back pain using variable forces. JPMA. The Journal of the Pakistan Medical Association, 72(3), 483–486. https://doi.org/10.47391/JPMA.453
Kumari, A., Quddus, N., Meena, P. R., Alghadir, A. H., & Khan, M. (2021). Effects of One-Fifth, One-Third, and One-Half of the Bodyweight Lumbar Traction on the Straight Leg Raise Test and Pain in Prolapsed Intervertebral Disc Patients: A Randomized Controlled Trial. BioMed research international, 2021, 2561502. https://doi.org/10.1155/2021/2561502
Slomski A. (2020). Early Physical Therapy Relieves Sciatica Disability and Pain. JAMA, 324(24), 2476. https://doi.org/10.1001/jama.2020.24673
Albert, H. B., Hauge, E., & Manniche, C. (2012). Centralization in patients with sciatica: are pain responses to repeated movement and positioning associated with outcome or types of disc lesions?. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 21(4), 630–636. https://doi.org/10.1007/s00586-011-2018-9
Can individuals with herniated discs find the relief they are looking for from traction therapy or decompression to provide pain relief?
Introduction
The spine allows the individual to be mobile and flexible without feeling pain and discomfort when a person is on the move. This is because the spine is part of the musculoskeletal system that consists of muscles, tendons, ligaments, the spinal cord, and spinal discs. These components surround the spine and have three regions to allow the upper and lower extremities to do their jobs. However, the spine also ages when the body starts to age naturally. Many movements or routine actions can cause the body to be stiff and, over time, can cause the spinal disc to herniate. When this happens, a herniated disc can lead to pain and discomfort in the extremities, thus making individuals deal with a reduced quality of life and pain in three spinal regions. Luckily, there are numerous treatments, like traction therapy and decompression, to alleviate the pain and discomfort associated with herniated discs. Today’s article looks at why herniated discs cause issues in the spine and the effects of how these two treatments can help reduce herniated discs. We talk with certified medical providers who consolidate our patients’ information to assess how a herniated disc in the spine may be the issue causing musculoskeletal pain. We also inform and guide patients on how integrating spinal decompression and traction therapy can help realign the spine and reduce disc herniation that is causing spinal issues. We encourage our patients to ask their associated medical providers intricate and important questions about incorporating non-surgical treatments as part of their routine to reduce pain and discomfort in their bodies. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
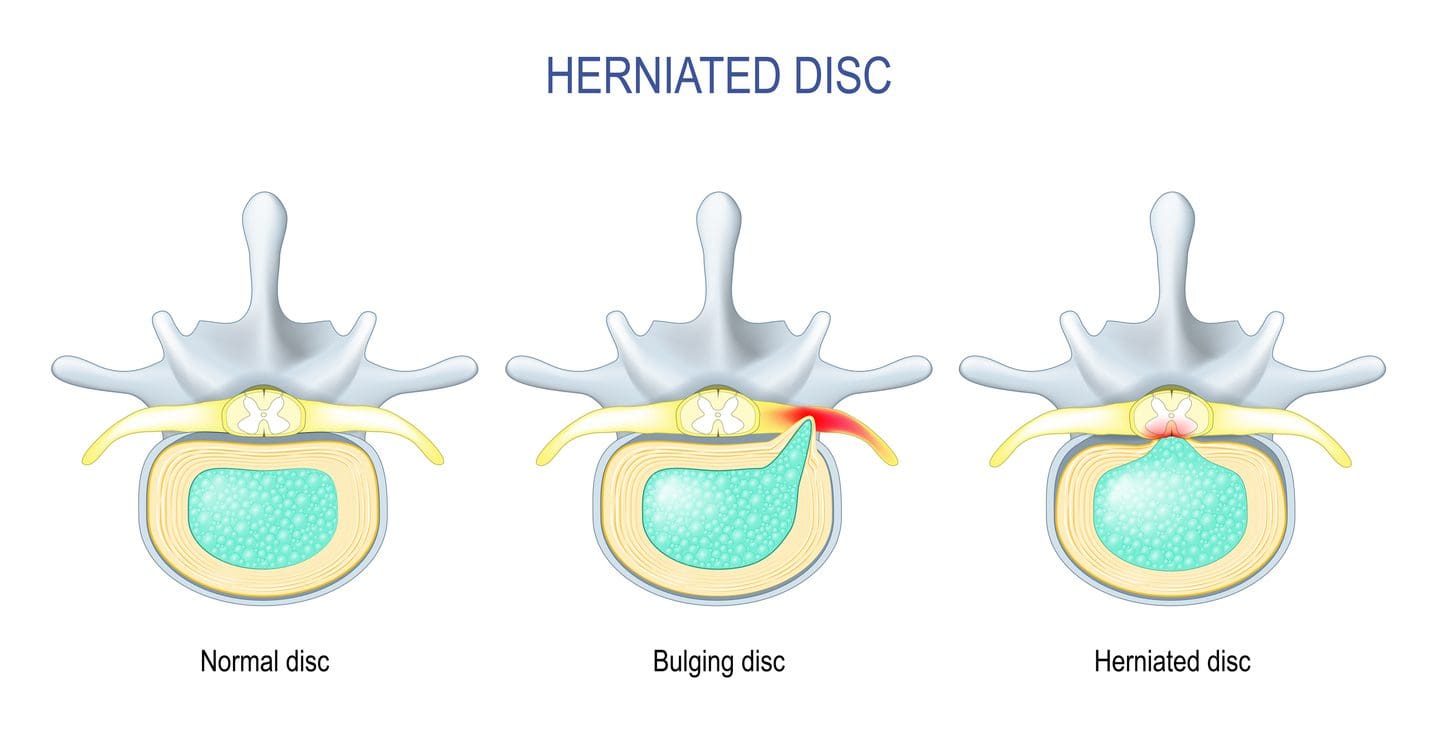
Why Herniated Discs Causes Issues In The Spine?
Have you been experiencing constant discomfort in your neck or back that doesn’t allow you to relax? Do you feel tingling sensations in your upper and lower extremities, making grasping objects or walking difficult? Or have you noticed that you are hunching over from your desk or standing and that stretching causes pain? As the spine keeps the body upright, its main components include the moveable vertebrae, the nerve root fibers, and spinal discs to help send neuron signals to the brain to allow movement, cushion the shocked forces on the spine, and be flexible. The spine allows the individual to perform various tasks without pain and discomfort through repetitive movements. However, when the body ages, it can lead to degenerative changes in the spine, causing the spinal disc to herniate over time. A herniated disc is a common degenerative musculoskeletal condition that causes the nucleus pulposus to break through any weak region of the annulus fibrosus and compress the surrounding nerve roots. (Ge et al., 2019) Other times, when repetitive motions start to cause a developing herniated disc, the inner portion of the disc can become desiccated and brittle. In contrast, the outer portion becomes more fibrotic and less elastic, causing the disc to shrink and be narrow. A herniated disc can affect young and old populations as they can have a multifactorial contribution that causes proinflammatory changes to the body. (Wu et al., 2020)
When many people are dealing with pain associated with a herniated disc, the disc itself goes through morphological change through the characterization of the disc being partial damage, which is then followed by the displacement and herniation of the inner disc portion in the vertebral canal to compress the spinal nerve roots. (Diaconu et al., 2021) This causes symptoms of pain, numbness, and weakness in the upper and lower body portions through nerve impingement. Hence why, many individuals are dealing with referred pain symptoms from their arms and legs that are radiating pain. When nerve compression associated with herniated discs starts to cause pain and discomfort, many individuals begin to seek out treatment to reduce the pain that the herniated disc is causing to provide relief for their bodies.
Spinal Decompression In Depth-Video
The Effects Of Traction Therapy In Reducing Herniated Disc
Many people who are suffering from pain that is being affected by herniated discs in their spines can seek out treatments like traction therapy to alleviate pain. Traction therapy is a non-surgical treatment that stretches and mobilizes the spine. Traction therapy can be mechanically or manually done by a pain specialist or with the help of mechanical devices. The effects of traction therapy can reduce the compression force on the spinal disc while reducing nerve root compression by expanding the disc height within the spine. (Wang et al., 2022) This allows the surrounding joints within the spine to be mobile and positively affect the spine. With traction therapy, intermittent or steady tension forces help stretch the spine, reduce pain, and improve functional outcomes. (Kuligowski et al., 2021)
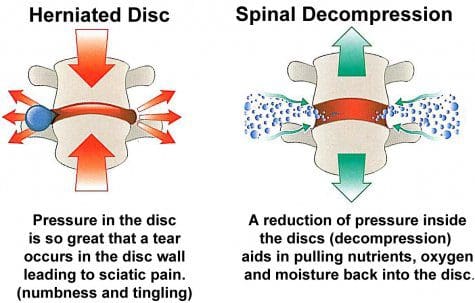
The Effects Of Spinal Decompression In Reducing Herniated Disc
Another form of non-surgical treatment is spinal decompression, a sophisticated version of traction that uses computerized technology to help apply controlled, gentle pulling forces to the spine. Spinal decompression does is that it can help decompress the spinal canal and help pull the herniated disc back to its original position while stabilizing the spine and keeping the vital bones and soft tissues safe. (Zhang et al., 2022) Additionally, spinal decompression can create negative pressure on the spine to allow the flow of nutritional fluids and blood oxygen back to the discs while creating an inverse relationship when tension pressure is introduced. (Ramos & Martin, 1994) Both spinal decompression and traction therapy can offer many therapeutic pathways to provide relief to many individuals dealing with herniated discs. Depending on how severe the herniated disc has caused issues to the person’s spine, many can rely on non-surgical treatments due to its customizable plan that is personalized to the person’s pain and can be combined with other therapies to strengthen the surrounding muscles. By doing so, many people can be pain-free over time while being mindful of their bodies.
References
Diaconu, G. S., Mihalache, C. G., Popescu, G., Man, G. M., Rusu, R. G., Toader, C., Ciucurel, C., Stocheci, C. M., Mitroi, G., & Georgescu, L. I. (2021). Clinical and pathological considerations in lumbar herniated disc associated with inflammatory lesions. Rom J Morphol Embryol, 62(4), 951-960. https://doi.org/10.47162/RJME.62.4.07
Ge, C. Y., Hao, D. J., Yan, L., Shan, L. Q., Zhao, Q. P., He, B. R., & Hui, H. (2019). Intradural Lumbar Disc Herniation: A Case Report and Literature Review. Clin Interv Aging, 14, 2295-2299. https://doi.org/10.2147/CIA.S228717
Kuligowski, T., Skrzek, A., & Cieslik, B. (2021). Manual Therapy in Cervical and Lumbar Radiculopathy: A Systematic Review of the Literature. Int J Environ Res Public Health, 18(11). https://doi.org/10.3390/ijerph18116176
Ramos, G., & Martin, W. (1994). Effects of vertebral axial decompression on intradiscal pressure. J Neurosurg, 81(3), 350-353. https://doi.org/10.3171/jns.1994.81.3.0350
Wang, W., Long, F., Wu, X., Li, S., & Lin, J. (2022). Clinical Efficacy of Mechanical Traction as Physical Therapy for Lumbar Disc Herniation: A Meta-Analysis. Comput Math Methods Med, 2022, 5670303. https://doi.org/10.1155/2022/5670303
Wu, P. H., Kim, H. S., & Jang, I. T. (2020). Intervertebral Disc Diseases PART 2: A Review of the Current Diagnostic and Treatment Strategies for Intervertebral Disc Disease. Int J Mol Sci, 21(6). https://doi.org/10.3390/ijms21062135
Zhang, Y., Wei, F. L., Liu, Z. X., Zhou, C. P., Du, M. R., Quan, J., & Wang, Y. P. (2022). Comparison of posterior decompression techniques and conventional laminectomy for lumbar spinal stenosis. Front Surg, 9, 997973. https://doi.org/10.3389/fsurg.2022.997973
For individuals experiencing lower back pain can understanding the anatomy and function of the multifidus muscle help in injury prevention and in the development of a highly effective treatment plan?
Multifidus Muscle
The multifidus muscles are long and narrow on either side of the spinal column, which helps stabilize the lower region of the spine or lumbar spine. (Maryse Fortin, Luciana Gazzi Macedo 2013) Sitting too much, practicing unhealthy postures, and lack of movement can progress to the multifidus muscle weakening or atrophy, which can lead to spinal instability, vertebral compression, and back pain. (Paul W. Hodges, Lieven Danneels 2019)
Anatomy
Known as the deep layer, it is the innermost layer of the three muscle layers of the back and controls the movement of the spine. The other two layers, known as the intrinsic and superficial, are responsible for the thoracic cage/rib cage and shoulder movement. (Anouk Agten et al., 2020) The multifidus has attachment points at:
The thoracic spine of the middle back.
The lumbar spine of the lower back.
The iliac spine – the base of the wing-shaped iliac bone of the pelvis.
Sacrum – series of bones at the base of the spine connected to the tailbone.
When standing or moving, the multifidus muscle works with the transversus abdominus and pelvic floor muscles to stabilize the lumbar spine. (Christine Lynders 2019)
Muscle Function
The main function is to stabilize the lower back, but it also helps extend the lower spine whenever reaching or stretching. (Jennifer Padwal et al., 2020) Because the muscle has numerous attachment points and is serviced by a specific branch of nerves known as the posterior rami, it allows each vertebra to work individually and more efficiently.
The multifidus muscle works with two other deep muscle groups to stabilize and move the spine. (Jeffrey J Hebert et al., 2015)
The rotatores muscle enables unilateral rotation, turning from side to side, and bilateral extension or bending backward and forward.
The semispinalis muscle above the multifidus allows extension and rotation of the head, neck, and upper back.
The multifidus muscle ensures spinal strength because it has more attachment points to the spine than the other layers, which reduces spinal flexibility and rotation but increases strength and stability. (Anouk Agten et al., 2020)
Lower Back Pain
A weak multifidus muscle destabilizes the spine and provides less support to the vertebra. This adds pressure on muscles and connective tissues between and adjacent to the spinal column, increasing the risk of lower back pain symptoms. (Paul W. Hodges, Lieven Danneels 2019) The loss of muscle strength and stability can cause atrophy or wasting away. This can cause compression and other back problems. (Paul W. Hodges et al., 2015) Back problems associated with multifidus muscle deterioration include (Paul W. Hodges, Lieven Danneels 2019)
Herniated discs – also bulging or slipped discs.
Nerve entrapment or compression pinched nerve.
Sciatica
Referred pain – nerve pain originating from the spine felt in other areas.
Osteoarthritis – wear-and-tear arthritis
Spinal osteophytes – bone spurs
Weak abdominal or pelvic floor muscles can compromise the core, increasing the risk of chronic lower back pain and injury.
Individuals are recommended to consult a physical therapist and chiropractor who can help develop the appropriate treatment, rehabilitation, and strengthening plan based on age, injury, underlying conditions, and physical abilities.
Can Core Exercises Help with Back Pain?
References
Fortin, M., & Macedo, L. G. (2013). Multifidus and paraspinal muscle group cross-sectional areas of patients with low back pain and control patients: a systematic review with a focus on blinding. Physical therapy, 93(7), 873–888. https://doi.org/10.2522/ptj.20120457
Hodges, P. W., & Danneels, L. (2019). Changes in Structure and Function of the Back Muscles in Low Back Pain: Different Time Points, Observations, and Mechanisms. The Journal of orthopaedic and sports physical therapy, 49(6), 464–476. https://doi.org/10.2519/jospt.2019.8827
Agten, A., Stevens, S., Verbrugghe, J., Eijnde, B. O., Timmermans, A., & Vandenabeele, F. (2020). The lumbar multifidus is characterised by larger type I muscle fibres compared to the erector spinae. Anatomy & cell biology, 53(2), 143–150. https://doi.org/10.5115/acb.20.009
Lynders C. (2019). The Critical Role of Development of the Transversus Abdominis in the Prevention and Treatment of Low Back Pain. HSS journal : the musculoskeletal journal of Hospital for Special Surgery, 15(3), 214–220. https://doi.org/10.1007/s11420-019-09717-8
Padwal, J., Berry, D. B., Hubbard, J. C., Zlomislic, V., Allen, R. T., Garfin, S. R., Ward, S. R., & Shahidi, B. (2020). Regional differences between superficial and deep lumbar multifidus in patients with chronic lumbar spine pathology. BMC musculoskeletal disorders, 21(1), 764. https://doi.org/10.1186/s12891-020-03791-4
Hebert, J. J., Koppenhaver, S. L., Teyhen, D. S., Walker, B. F., & Fritz, J. M. (2015). The evaluation of lumbar multifidus muscle function via palpation: reliability and validity of a new clinical test. The spine journal : official journal of the North American Spine Society, 15(6), 1196–1202. https://doi.org/10.1016/j.spinee.2013.08.056
Hodges, P. W., James, G., Blomster, L., Hall, L., Schmid, A., Shu, C., Little, C., & Melrose, J. (2015). Multifidus Muscle Changes After Back Injury Are Characterized by Structural Remodeling of Muscle, Adipose and Connective Tissue, but Not Muscle Atrophy: Molecular and Morphological Evidence. Spine, 40(14), 1057–1071. https://doi.org/10.1097/BRS.0000000000000972
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine