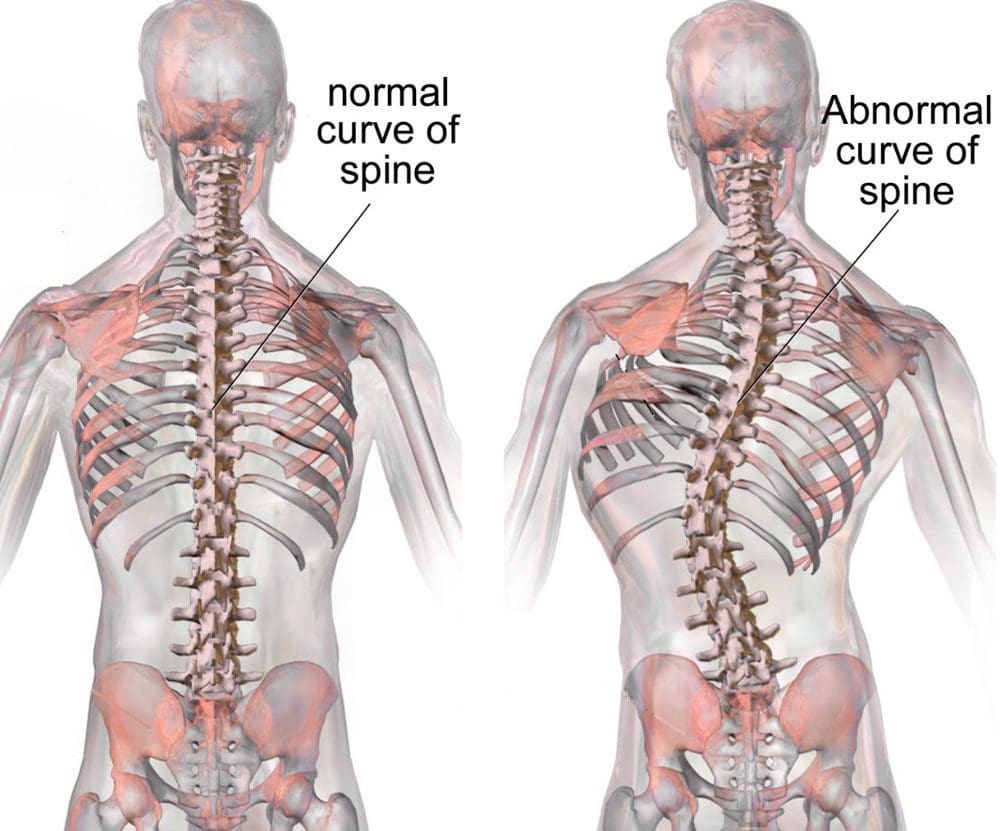
Idiopathic scoliosis means that no cause congenital or neuromuscular that created the spinal deformation has been identified. However, idiopathic scoliosis is the most common type, affecting 2% to 3% of individuals. Individuals diagnosed with an idiopathic disease or condition can be frustrated with more questions than answers, but it can still be treated in adults and kids.
Idiopathic Scoliosis
Congenital Scoliosis
Congenital scoliosis is an abnormal curvature of the spine related to which the patient was born.
Usually, a failure of formation or segmentation during normal development leads to the spinal condition.
Neuromuscular Scoliosis
Individuals with neuromuscular scoliosis are usually born with neurological disorders that contribute to muscular unevenness, often resulting in the development of the condition.
For example, individuals with cerebral palsy are born with muscular unevenness that can contribute to scoliosis development.
Who Is Affected
Anyone can develop scoliosis, but children and adults are divided into separate categories.
Children
Children with this condition are divided into three subcategories:
Adolescents are from 11 onward or when starting puberty, to the point where the skeleton fully matures.
Adults
Idiopathic scoliosis in adults results from undiagnosed or untreated scoliosis in childhood that gradually progressed.
Causes
Research has found a genetic predisposition to developing scoliosis, as it has been found to run in families. Genetic testing has been designed to help determine the risk of developing progressive scoliosis. Theories have been presented about abnormalities that affect the nervous system. These include:
Dysfunctions of the brain stem or equilibrium have been frequently identified in individuals with idiopathic scoliosis.
Other theories suggest skeletal growth abnormalities or hormonal/metabolic dysfunction may contribute to the condition.
However, determining its exact cause remains unknown.
Signs and Symptoms
Here are some things to look out for.
The body leans to one side.
There is an unevenness of the ribcage or hips.
Uneven shoulders.
Shoulder blades may protrude or stick out.
The head is not positioned directly above the pelvis.
Diagnosis
Idiopathic scoliosis curves tend to follow predictable patterns.
Magnetic resonance images/MRIs of the spine can show evidence of any significant abnormalities. If no other related condition is present to suggest different causes, then the idiopathic scoliosis diagnosis can be made.
Treatment
Treatment depends on the individual’s age and the degree of curvature in the spine.
In many cases, adolescent or juvenile idiopathic scoliosis patients that have a mild curve can be treated with a brace.
Adults could need surgical intervention, such as a fusion surgery where rods and screws are added to realign the spine and relieve the pressure on the nerves.
Chiropractor
References
Burnei, G et al. “Congenital scoliosis: an up-to-date.” Journal of medicine and life vol. 8,3 (2015): 388-97.
Clément, Jean-Luc, et al. “Relationship between thoracic hypokyphosis, lumbar lordosis and sagittal pelvic parameters in adolescent idiopathic scoliosis.” The European spine journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society vol. 22,11 (2013): 2414-20. doi:10.1007/s00586-013-2852-z
Giampietro, Philip F et al. “Congenital and idiopathic scoliosis: clinical and genetic aspects.” Clinical medicine & research vol. 1,2 (2003): 125-36. doi:10.3121/cmr.1.2.125
“Scoliosis – Symptoms, Diagnosis and Treatment.” https://www.aans.org/Patients/Neurosurgical-Conditions-and-Treatments/Scoliosis
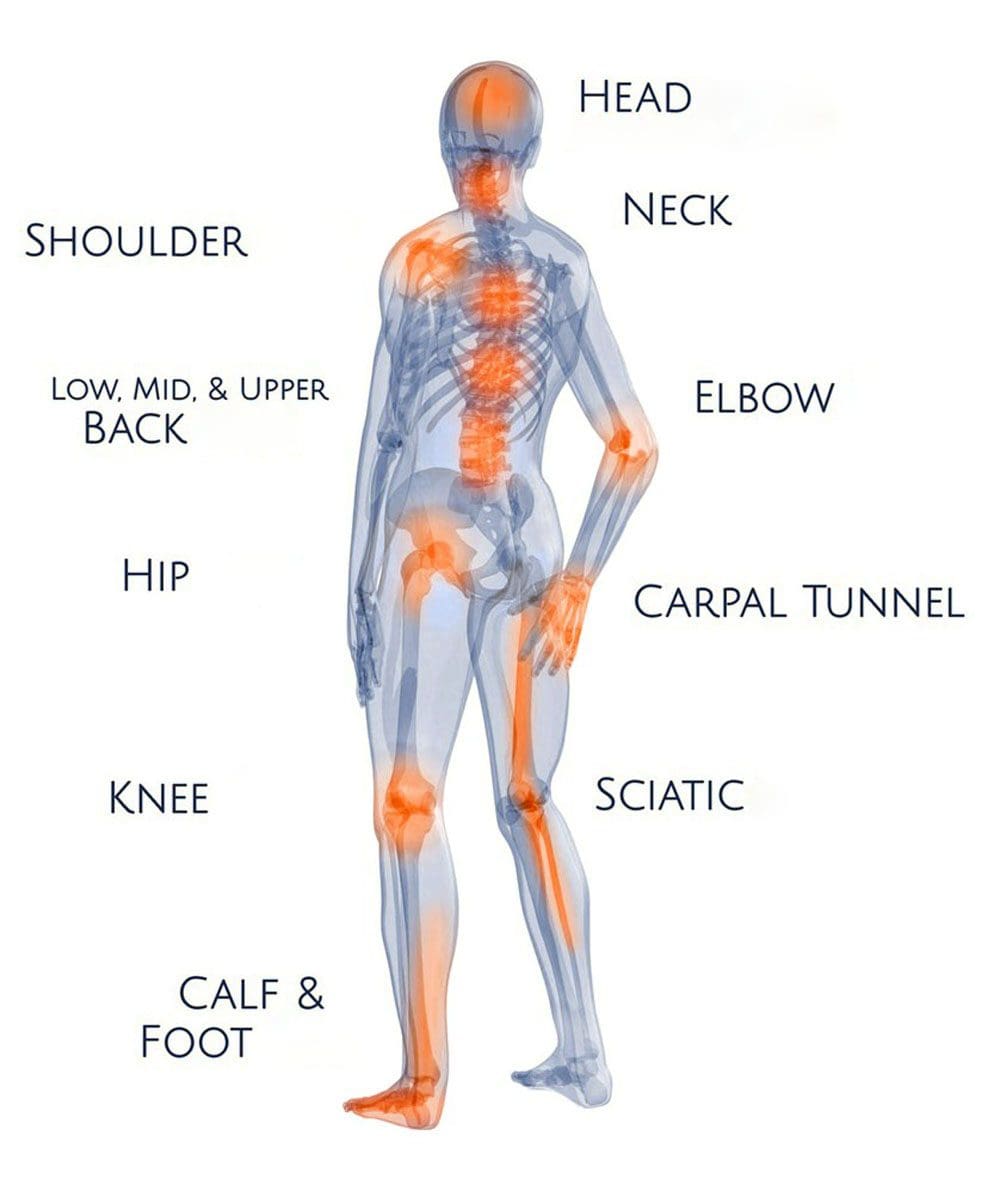
Pinched Nerves and Muscle Spasms: A pinched or compressed nerve can occur in various body regions, from the wrist to the foot. When a nerve is compressed, a pins and needles feeling can present until the pressure is relieved, or there can be no sensation symptoms, but other symptoms like muscle spasms, especially in the arm or leg, can appear. Individuals will feel a repetitive fluttering or twitching when the arm or leg is not in motion. A pinched nerve could be the cause of spasms in the back or extremities. Injury Medical Chiropractic and Functional Medicine Clinic can help if symptoms are not stopping or worsening.
Pinched Nerves and Muscle Spasms
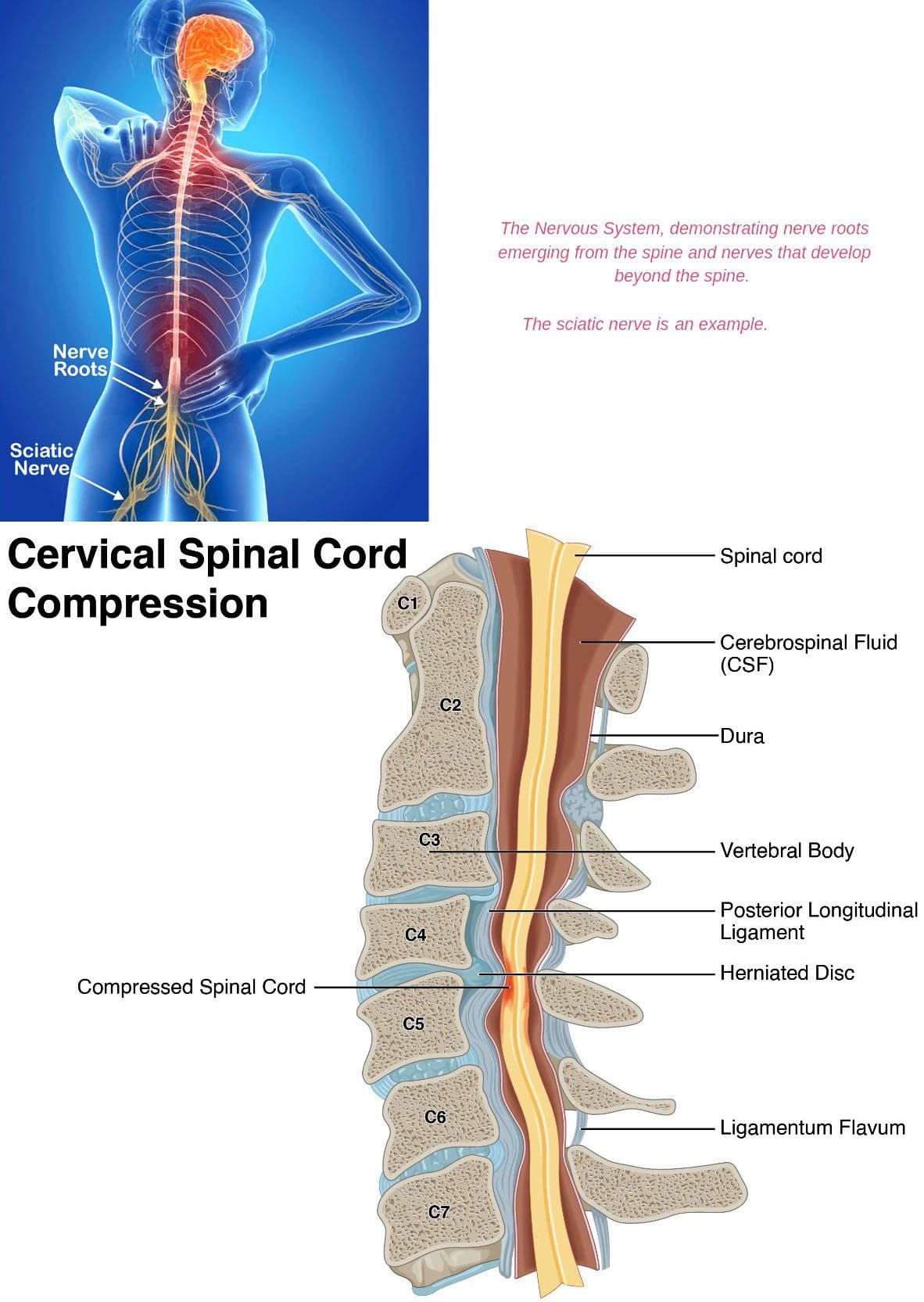
When multiple symptoms appear, individuals may not realize they are connected. Individuals may think aches, pains, and spasms are normal aging processes. Pinched nerves occur when there is an impingement on any one of the numerous nerves of the spine. Impingements can be caused by:
Repetitive motion injuries
Disc degeneration
Herniated/ruptured discs
Bone spurs
Arthritis
Trauma injury
The pain symptoms from the spasm can be quick, sharp, or pulsating and throbbing. The muscles respond by tightening or spasming as the nerve sends interrupted/incomplete signals. In addition to muscle spasms, a pinched nerve can contribute to other symptoms, including the following.
Tingling
Numbness
Pins and needles sensation
Reduced range of motion
Muscle weakness
Signs a Pinched Nerve Might Be Causing Spasms
Sudden shooting pain that radiates down the leg or arm.
Weak muscles
Muscle atrophy – shrinking or deteriorating.
Chronic tingling in the extremities.
A burning sensation in a specific area; this could but is not necessarily the source of the pinched nerve.
Electrical shock-type pain accompanies the spasms.
If a pinched nerve is left untreated and continues to generate symptoms, it can affect daily life and lead to uncomfortable long-term issues. Severe nerve compression combined with inflammation can cause damage to nearby soft tissues and muscles, leading to chronic conditions. When the nerves are damaged, it can be harder to control the muscles making certain motions uncomfortable or difficult to move certain body parts.
Chiropractic Care
Chiropractic care, massage, and decompression therapy will relieve pinched nerves and muscle spasms and restore neuromusculoskeletal system function. The body will be realigned, and patients will be trained on stretching exercises, muscle strengthening, posture training, and nutritional support to optimize the body’s natural healing abilities to repair the damaged nerves.
Low Back Pain
References
Bustamante, S, and P G Houlton. “Swelling of the leg, deep venous thrombosis, and the piriformis syndrome.” Pain research & management vol. 6,4 (2001): 200-3. doi:10.1155/2001/104091
Chu, Eric Chun-Pu, and Robert J Trager. “Thoracic Schwannoma as an Unusual Cause of Sciatic Pain in the Chiropractic Office: A Case Report.” The American journal of case reports vol. 23 e938448. 16 Nov. 2022, doi:10.12659/AJCR.938448
Coletti, Roger H. “The ischemic model of chronic muscle spasm and pain.” European journal of translational myology vol. 32,1 10323. 18 Jan. 2022, doi:10.4081/ejtm.2022.10323
Hirayama, Jiro, et al. “Relationship between low-back pain, muscle spasm and pressure pain thresholds in patients with lumbar disc herniation.” The European spine journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society vol. 15,1 (2006): 41-7. doi:10.1007/s00586-004-0813-2
Kennedy, John G, and Donald E Baxter. “Nerve disorders in dancers.” Clinics in sports medicine vol. 27,2 (2008): 329-34. doi:10.1016/j.csm.2008.01.001
Waddell, Roger K. “Chiropractic care for a patient with spasmodic dysphonia associated with cervical spine trauma.” Journal of chiropractic medicine vol. 4,1 (2005): 19-24. doi:10.1016/S0899-3467(07)60108-6
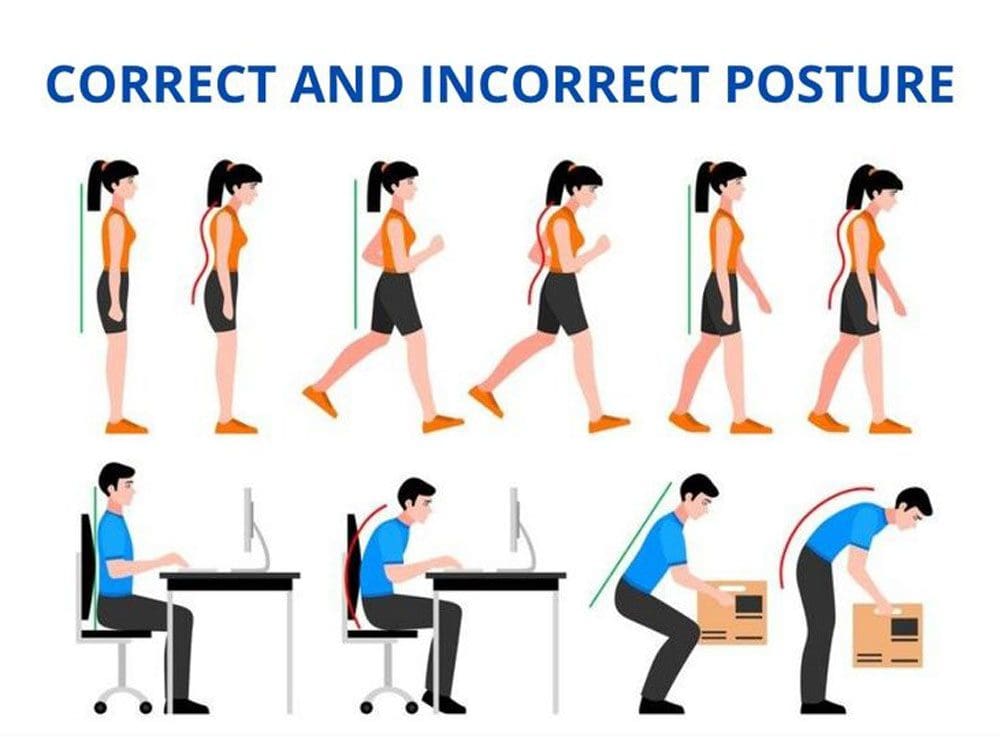
Healthy Posture Guidelines: Posture is how an individual holds their body. Healthy posture is when minimal stress is applied to the joints. Maintaining and holding your body correctly can prevent pain, injuries, and other health problems. Faulty postures and musculoskeletal imbalances often precipitate painful conditions in the spine and extremities. However, unhealthy postures do not always present with discomfort and pain symptoms that can go unnoticed for years. This leads to chronic stress and advanced wear of the joints. Injury Medical Chiropractic and Functional Medicine Clinic can realign the spine, relieve symptoms, and restore flexibility, mobility, and function.
Healthy Posture Guidelines
There are two types of posture:
Dynamic Posture
This posture is when the body moves, like walking, running, or bending to pick up something.
Static Posture
This posture is when the body is not moving, like sitting, standing, or sleeping.
Both are important, and the key is the spine’s position. The spine has three natural curves: neck, mid, and low back. Correct posture maintains the curves with the head above the shoulders, and the top of the shoulder should be over the hips.
Unhealthy Positioning
Postural faults include:
Forward head positioning
Rounded shoulders
Loss of the normal lordosis curve in the lower back.
Early warning signs of postural problems may include:
The inability to sit or stand for a prolonged period.
Stiffness when getting up from a chair after sitting.
Feeling of physical exhaustion at the end of the day.
Muscle imbalances.
Loss of normal flexibility.
Symptoms of discomfort.
Affected Health
Unhealthy posture can affect overall health and includes:
Misaligned musculoskeletal system.
Decreased flexibility.
Neck, shoulder, and back pain.
The advanced wearing down of the spine making it more fragile and susceptible to injury.
Affected joint movement.
Affected balance.
Increased risk of falling.
Digestion problems.
Potential breathing problems.
Improvements
Be mindful of your posture during everyday activities, like walking, watching tv, washing dishes, etc.
Maintain Physical Activity
Certain exercises like yoga, tai chi, and other classes focusing on body awareness can help develop healthy posture habits.
Exercises that strengthen the core muscles around the back, abdomen, and pelvis.
Maintain Healthy Weight
Extra weight can weaken the abdominal muscles, cause problems for the pelvis and spine, and contribute to back pain.
Wear Comfortable Shoes
High heels, for example, can throw off the body’s balance and force unhealthy walking movements.
This puts added stress on the muscles and affects posture.
Proper Height
Make sure workstations are at a comfortable height, whether sitting in front of a computer, making dinner, or eating.
Chiropractic Care
Chiropractors and physical massage therapists specialize in evaluating and treating musculoskeletal dysfunction and identifying and screening for postural dysfunction. Healthy posture can have an immediate effect on health that include:
Proper alignment of bones and joints.
Reduced wear on the muscles and joints.
Reduced stress on ligaments.
Decreased risk of back injury.
Increased energy.
Improved digestion.
A chiropractic team will massage and relax the muscles reducing tension, adjust and realign the spine, increase joint movement, and ease the individual into a healthy posture. The team will also provide careful rehabilitation exercises and nutritional recommendations to maintain a healthy posture.
Custom Foot Orthotics
References
Carini, Francesco, et al. “posture and posturology, anatomical and physiological profiles: overview and current state of the art.”Acta bio-medica : Atenei Parmensis vol. 88,1 11-16. 28 Apr. 2017, doi:10.23750/abm.v88i1.5309
Creze, Maud, et al. “posture-related stiffness mapping of paraspinal muscles.”Journal of anatomy vol. 234,6 (2019): 787-799. doi:10.1111/joa.12978
Korakakis, Vasileios, et al. “physiotherapist perceptions of optimal sitting and standing posture.”Musculoskeletal science & practice vol. 39 (2019): 24-31. doi:10.1016/j.msksp.2018.11.004
Skiing sports require balance, strength, endurance, and muscle power. It is recommended to start training for ski season about eight to twelve weeks before heading to the slopes. However, any amount of training is better than no training; as long as you stay consistent and focus on exercises that enhance skiing or snowboarding, even a few weeks of fitness training can make a difference. A ski conditioning workout can help you ski better, stay out longer, prevent injuries, and have more fun.
Skiing
Before beginning any training plan, check with your doctor or a certified training professional. The recommended strategy is a cardio and strength workout routine that trains and strengthens the lower-body muscles, including the quads, hamstrings, and glutes. This will improve mobility and balance to help control the skis better and support body parts like the knees, which are more prone to skiing injuries.
General Overview of Training
Increase Muscle Power
Strengthen the quads, glutes, hamstrings, and hips.
Posture and Balance
Train the core and the muscles around the hips, which helps provide stability.
Increase Endurance
Condition the body to handle vigorous conditions.
Increase Cardiovascular Function
Cardiovascular activities include running, biking, or interval training to strengthen the lungs and heart.
Training Schedule
Starting
With skiing, you’ll need a combination of cardio and strength training and enhanced aerobic fitness for the higher altitude.
Individuals are encouraged to start around six to eight weeks before ski season because it takes around that amount of time to experience the benefits.
The muscles need time to recover and repair themselves between sessions.
As aforementioned, you can still exercise even if you have missed the training window.
Pick an enjoyable activity: jogging, biking, and high-intensity interval training/HITT.
The goal should be 30 minutes of cardio activity 2-3 times a week to prepare the heart and lungs for downhill runs.
Recommended workouts for getting into ski shape:
Elliptical trainer – The elliptical trainer is highly recommended for ski training, as it mimics the same upper-body and lower-body movements used in Nordic skiing.
This could be a short session on a treadmill, jumping jacks, or a quick jog.
Guidelines as you progress through the workout:
Inhale during initial exertion, and exhale as you return to the starting position.
Maintain breathing patterns during faster exercises.
Rest at the end of each exercise.
Walking Lunge with Rotation Exercise
This exercise works the glutes, quads, hamstrings, and abdominals and improves core rotation.
Stand with your feet slightly apart.
Step one foot forward into a lunge.
As you step forward, rotate your body to the side in the direction of your lead knee.
Arms should be at chest height, slightly elevated from the sides.
Drive up and through your forward leg to take the next lunge.
Repeat ten times on each side for a total of 20.
Tips and modifications:
If you don’t have enough space, you can stay in one spot and alternate lunging.
Make it easier by keeping the back leg straight.
Make sure that your knees do not go inward.
Stay in a straight line with your foot and hip.
Lateral Ski Jump Exercise
This power exercise prepares for the explosive ski movements and energy bursts needed to control the descent.
Stand with your feet hip-width apart and knees slightly bent, balancing on one leg.
Jump to the side, landing on the other leg.
Think about landing softly with your knee slightly bent.
Jump to the other side, landing softly on the other leg.
Swing the arms sideways across your body like a speed skater.
Repeat 15 on each side.
Tips and modifications:
Make smaller jumps to the side
Move slower
Touch your toe to the ground instead of keeping it off the floor.
Chop Exercise
This exercise will strengthen the core to initiate turns using the core rather than the arms or shoulders and help prevent lower back pain.
Use a resistance band that you can secure slightly above the shoulders.
Stand sideways to where the band is anchored.
Position yourself so that you can reach up evenly with your shoulder to grab the free end of the band with both hands.
Your knees should be slightly bent.
Pull the band down across your body while turning your body.
Think about the trunk doing most of the work for this exercise, not the arms and shoulders.
Keep your arms as straight as you can as you pull the band down
The arms should act as guides, with the obliques and back muscles generating the pulling and rotating power.
Do this 15 times, then repeat facing the other way.
Rest for 90 seconds before moving on to the next exercise.
Tips and modifications:
Adjust the band resistance level by shortening it to increase resistance or lengthening it to ease resistance.
The goal is to feel tired at the end of the reps but not so exhausted that you struggle to finish.
Hip Roll Exercise
This exercise strengthens the muscles of the hips, including the glutes, to help prevent knee pain. There’s a direct relationship between hip strength and knee control. When hip strength is weak, the knees tend to shift inward.
Stand on your left leg.
Lean your body forward at the hips, keeping the back straight.
Lift your right leg back behind you, slightly off the ground.
Rotate or roll your hip away from your standing foot.
Maintain the body in a straight line as you roll your hips back.
Repeat 10-15 times on each side.
Tips and modifications:
If balancing is difficult, hold on to the back of a chair or keep your toes on the ground.
Whether you’re going alpine or Nordic skiing, these are just a few exercises designed to help all types and levels of recreational skiers and snowboarders. Always check with your doctor before starting any exercise routine, and it is recommended to consult a ski instructor or personal trainer for more comprehensive and intense workouts.
Ski Team Workout
References
Laskowski, E R. “Snow skiing.” Physical medicine and rehabilitation clinics of North America vol. 10,1 (1999): 189-211.
Nagle, Kyle B. “Cross-Country Skiing Injuries and Training Methods.” Current sports medicine reports vol. 14,6 (2015): 442-7. doi:10.1249/JSR.0000000000000205
Steadman, J R et al. “Training for Alpine skiing.” Clinical orthopedics and related research,216 (1987): 34-8.
Therell, Terese, et al. “Effects of Core Strength Training on Skiing Economy in Elite Junior Cross-Country Skiers.” Research quarterly for exercise and sport vol. 93,3 (2022): 608-614. doi:10.1080/02701367.2021.1887441
Ankylosing spondylitis, or AS, is a type of inflammatory arthritis that usually impacts the spine, causing back stiffness and pain, pain in the hips, and decreased range of motion. Brain fog can also be a symptom of AS and other chronic inflammatory conditions. Brain fog can affect memory, concentration, decision-making, learning, and problem-solving. Injury Medical Chiropractic and Functional Medicine Clinic can educate on the causes of ankylosing spondylitis brain fog and how to reduce its effects.
Brain Fog
Experts do not fully understand how conditions like AS cause brain fog and how it affects the brain and central nervous system. However, they believe brain fog is linked to chronic inflammation and pain associated with the condition, along with certain factors.
Chronic Inflammation
Inflammation occurs when the body’s immune system attacks healthy cells.
This triggers the release of inflammation-causing cytokines.
Cytokines can interfere with normal brain function.
Ankylosing Spondylitis Chronic Pain
Chronic pain can cause fatigue and unhealthy sleep quality.
Fatigue and poor sleep can worsen chronic pain, leading to intense fatigue and extreme sleep issues, becoming a vicious cycle.
Corticosteroids
Doctors typically treat ankylosing spondylitis with corticosteroids.
Individuals with cardiovascular risk factors have an increased risk of brain fog from the medications.
Depression
Individuals with AS can present symptoms of depression, which has been linked to cognitive impairment.
Depression can contribute to the development of brain fog.
Cornelson, Stacey M et al. “Chiropractic Care in the Management of Inactive Ankylosing Spondylitis: A Case Series.” Journal of chiropractic medicine vol. 16,4 (2017): 300-307. doi:10.1016/j.jcm.2017.10.002
Creaky Joints. (September 17, 2018) “You can ease inflammatory arthritis brain fog with these 12 tips for a sharper mind.” https://creakyjoints.org/living-with-arthritis/arthritis-brain-fog/
Vitturi, Bruno Kusznir et al. “Cognitive Impairment in Patients with Ankylosing Spondylitis.” The Canadian journal of neurological sciences. Le journal canadien des sciences neurologiques vol. 47,2 (2020): 219-225. doi:10.1017/cjn.2020.14
Zhang, Jun-Ming, and Jianxiong An. “Cytokines, inflammation, and pain.” International anesthesiology clinics vol. 45,2 (2007): 27-37. doi:10.1097/AIA.0b013e318034194e
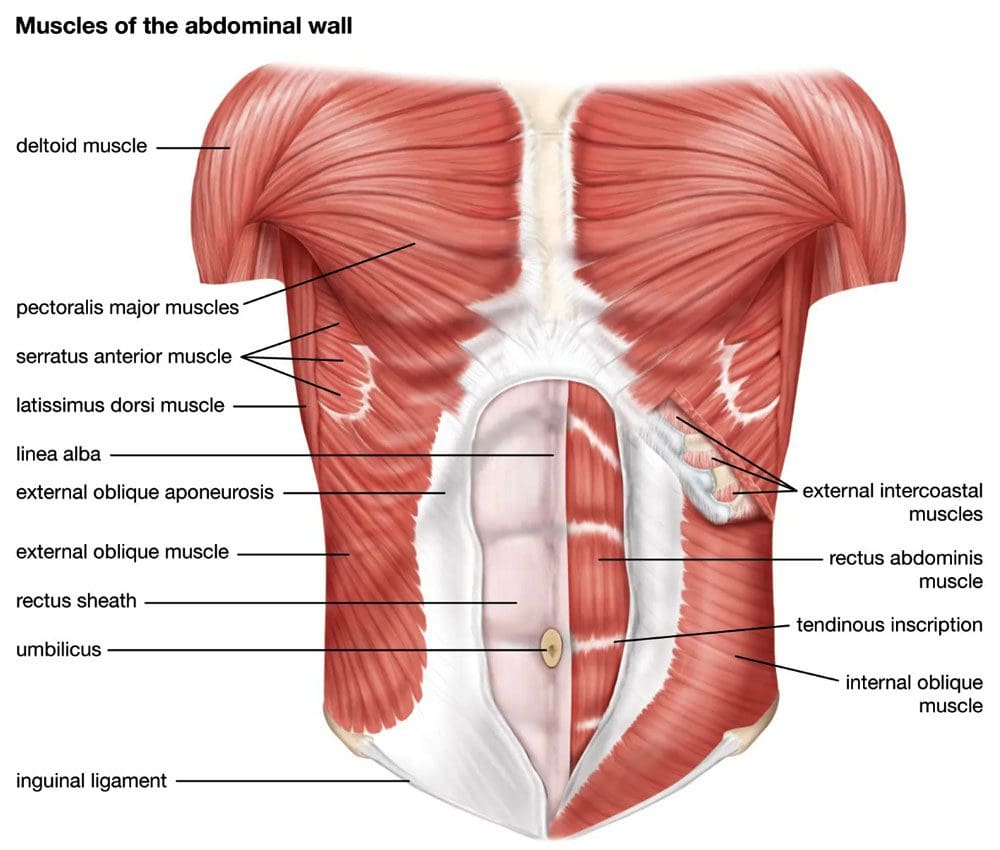
The 0blique muscles support and aid in side-to-side movement, helping maintain back strength and healthy posture. There are two oblique muscle sets, the internal and external obliques. Maintaining a strong core is one recommended way to protect the body and spine. However, many forget to train and strengthen all of the oblique muscles. Individuals tend to focus on the superficial core muscle, or rectus abdominis, and not enough or any attention goes to the lateral stabilizers or the internal and external obliques. Chiropractic and functional medicine can restore musculoskeletal flexibility, mobility, and function.
Oblique Muscles
The external obliques make up a large part of the trunk area. There are two external obliques on either side of the body, located on the lateral sides of the abdominal region. These muscles have an essential role in daily movements.
External
External obliques help with trunk rotation and support spine rotation.
They assist with pulling the chest down to compress the abdominal cavity.
They help with bending from side to side.
Any strain or injury to these muscles can lead to abdominal, hip, and back issues.
Maximizing external oblique strength is important to maintain a strong core.
Internal
The internal oblique is a muscle deep within the lateral side of the abdomen.
The internal oblique muscle is one of the main stabilizers and functions to flex the trunk and compress the chest.
Its positioning makes it invisible, but it still has an essential role in body movement.
This muscle can function bilaterally, meaning both sides can operate at the same time.
These muscles provide spinal and posture support.
Strain or injury in this area can cause posture problems and abdominal, hip, and back issues.
Rotation and Mobility
The internal and external obliques are the primary rotators of the spine and provide thoracic spine mobility.
The internal obliques work with the external obliques and the rectus abdominis for lateral spine flexion of the quadratus lumborum and lumbar paraspinals.
They attach to the diaphragm, transverse abdominis, and thoracolumbar fascia, contributing to core stabilization.
A quadratus lumborum muscle spasm can result from muscle inhibition in the obliques.
Inhibition
If the internal obliques are inhibited, compensation can cause an alteration in the sequence patterns of the posterior oblique subsystem.
When this system is not functioning correctly, individuals usually complain of discomfort in the hips and shoulders.
A common sign of oblique inhibition is individuals holding their breath during basic movement patterns to gain stability, indicating dysfunction in the intrinsic stabilization subsystem.
Simple movements include walking gait, single-leg stance, flexion, extension, etc.
If you are experiencing waistline, hip, and low back stiffness or tightness and pain, consult our professional chiropractic team. We’re ready to help!
Oblique Anatomy and Movement
References
Calais-Germain, Blandine, and Stephen Anderson. Anatomy of Movement. Seattle: Eastland, 1993.
Cook G. Movement: Functional Movement Systems: Screening, Assessment, and Corrective Strategies. Aptos, CA: On Target Publications, 2010.
Elphinston J. Stability, Sport and Performance Movement: Practical Biomechanics and Systematic Training for Movement Efficacy and Injury Prevention. Lotus Publishing, 2013.
Huxel Bliven, Kellie C, and Barton E Anderson. “Core stability training for injury prevention.” Sports health vol. 5,6 (2013): 514-22. doi:10.1177/1941738113481200
Myers TW. Anatomy Trains: Myofascial Meridians for Manual and Movement Therapists. Edinburgh: Churchill Livingstone, 2001.
Neumann DA. Kinesiology of the Musculoskeletal System: Foundations for Physical Rehabilitation. St. Louis: Mosby, 2002.
Starrett K, Cordoza G. Becoming a Supple Leopard: The Ultimate Guide to Resolving Pain, Preventing Injury, and Optimizing Athletic Performance. Las Vegas: Victory Belt Pub., 2013.
Weinstock D. NeuroKinetic Therapy: An Innovative Approach to Manual Muscle Testing. Berkeley, CA: North Atlantic, 2010.
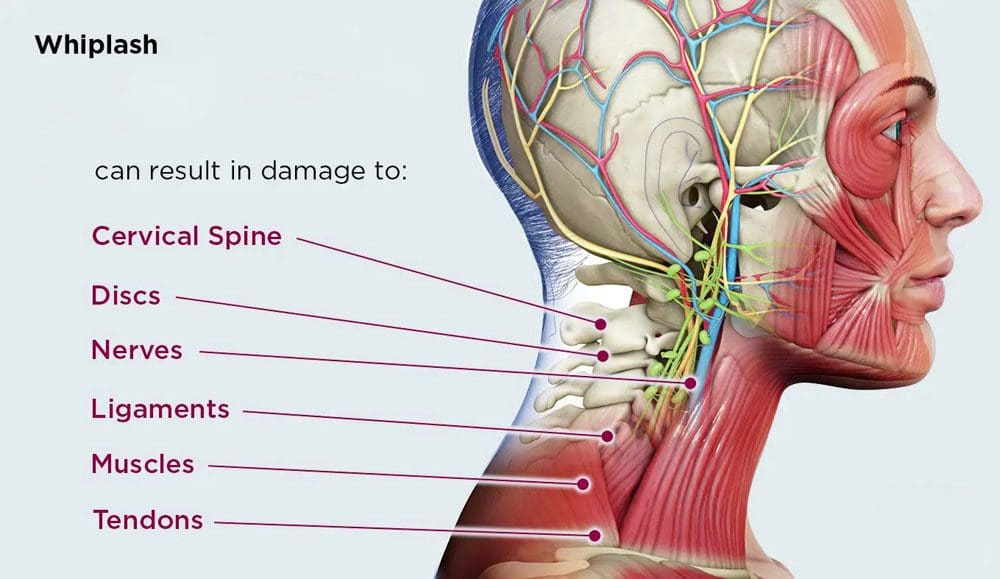
Whiplash-associated disorders, or WAD, describe injuries sustained from sudden acceleration/deceleration movements. It is a common outcome after a motor vehicle collision but can also be caused by sports injuries, falls, or assaults. Whiplash refers to the mechanism of the injury, while WAD refers to the presence of symptoms like pain, stiffness, muscle spasm, and headaches. A WAD prognosis is unpredictable, with some cases remaining acute with a full recovery, while others progress to chronic conditions with long-term symptoms and disability. Early intervention recommendations include rest, chiropractic care and physical rehabilitation, massaging and stretching exercises, and an anti-inflammatory diet.
Whiplash Associated Disorders
Cervical hyperextension injuries happen to drivers and passengers of moving, slow-moving (less than 14 miles per hour), and stationary vehicles when struck from behind.
The individual’s body is thrown forward, but the head does not follow the body and instead whips forward, resulting in hyperflexion or extreme forward movement of the neck.
The chin limits forward flexion, but the momentum can be sufficient to cause cervical distraction and neurological injuries.
When the head and neck have reached maximum flexion, the neck snaps back, resulting in hyperextension or extreme backward movement of the neck.
Pathology
Most WADs are considered soft tissue-based injuries with no fractures.
Stages
The injury goes through stages:
Stage 1
The upper and lower spine experiences flexion in stage one.
Stage 2
The spine takes on an S-shape while extending and eventually straightens, causing lordosis.
Stage 3
The entire spine is hyperextending with an intense force that causes the facet joint capsules to compress.
Symptoms
Whiplash-associated disorders can be classified through grades by the severity of symptoms, including neck pain, stiffness, occipital headache, cervical, thoracic, and lumbar back pain, upper-limb pain, and paraesthesia.
Grade 0
No complaints or physical symptoms.
Grade 1
Neck complaints but no physical symptoms.
Grade 2
Neck complaints and musculoskeletal symptoms.
Grade 3
Neck complaints and neurological symptoms.
Grade 4
Neck complaints and fracture and/or dislocation.
Most cervical fractures occur predominantly at C2 or C6, or C7.
A chiropractor will identify areas of restricted joint motion, muscle tension, muscle spasm, intervertebral disc injury, and ligament injury.
They will analyze posture, and spinal alignment, check for tenderness, tightness, and how well the spinal joints move.
This will allow the chiropractic physical therapy team to understand the injured body mechanics and how the spine is operating to make a thorough diagnosis.
The doctor will order imaging tests like an x-ray or an MRI to evaluate any degenerative changes that may have existed before the whiplash injury.
Once the injury has been accurately diagnosed, the chiropractor will design a personalized treatment plan.
Spinal Adjustments
Spinal manipulation is applied to areas of the spine that are out of alignment to realign the spine and activate the healing process.
Flexion-distraction technique is a gentle technique that uses slower, less intense pushing motions on the discs used to treat disc herniations that often occur after a whiplash injury.
Instrument-assisted manipulation utilizes special instruments to apply various forces or massage settings to the area.
Targeted spinal manipulation targets specific areas to rework, release, and rebuild the structures.
Massage Therapy stimulates the affected muscles to relax them from their tense state.
A treatment plan may utilize:
Instrument-assisted therapy
Trigger point therapy
Resistance-based stretches to rehabilitate soft tissue damage.
Our chiropractic team is ready to help you feel your best so you can return to normal activities and get on with your life.
Ritchie, C., Ehrlich, C. & Sterling, M. Living with ongoing whiplash-associated disorders: a qualitative study of individual perceptions and experiences. BMC Musculoskelet Disord 18, 531 (2017). https://doi.org/10.1186/s12891-017-1882-9
Sterling, Michele. “Whiplash-associated disorder: musculoskeletal pain and related clinical findings.” The Journal of manual & manipulative therapy vol. 19,4 (2011): 194-200. doi:10.1179/106698111X13129729551949
Wong, Jessica J et al. “Are manual therapies, passive physical modalities, or acupuncture effective for the management of patients with whiplash-associated disorders or neck pain and associated disorders? An update of the Bone and Joint Decade Task Force on Neck Pain and Its Associated Disorders by the OPTIMa collaboration.” The spine journal: official Journal of the North American Spine Society vol. 16,12 (2016): 1598-1630. doi:10.1016/j.spinee.2015.08.024
Woodward, M N et al. “Chiropractic treatment of chronic ‘whiplash’ injuries.” Injury vol. 27,9 (1996): 643-5. doi:10.1016/s0020-1383(96)00096-4
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine



 Healthy Posture Guidelines
Healthy Posture Guidelines


 Brain Fog
Brain Fog
 Oblique Muscles
Oblique Muscles