The body incorporates different muscles that have specific jobs to help mobilize the skeletal joints while providing function to the arms, neck, legs, and back. Many individuals use their muscles for everyday uses like lifting and carrying objects, moving from one place to another, and protecting vital organs from damage. To that point, issues like traumatic events, injuries, and environmental factors can affect the body and cause damage to the muscles. When the muscles are affected by these factors, tiny knots can form along the taut muscle band that can cause painful symptoms that affect specific areas in the body. One of the muscles affected by pain is the trapezius muscle, known as the “coat hanger” muscle, which can be associated with chronic symptoms of myofascial pain syndrome. Today’s article examines the trapezius muscle, how myofascial pain affects the trapezius muscle, and how to manage myofascial trapezius pain. We refer patients to certified providers specializing in musculoskeletal treatments to aid individuals suffering from trapezius muscle pain associated with myofascial pain. We also guide our patients by referring them to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Jimenez DC provides this information as an educational service only. Disclaimer
What Is The Trapezius Muscle?
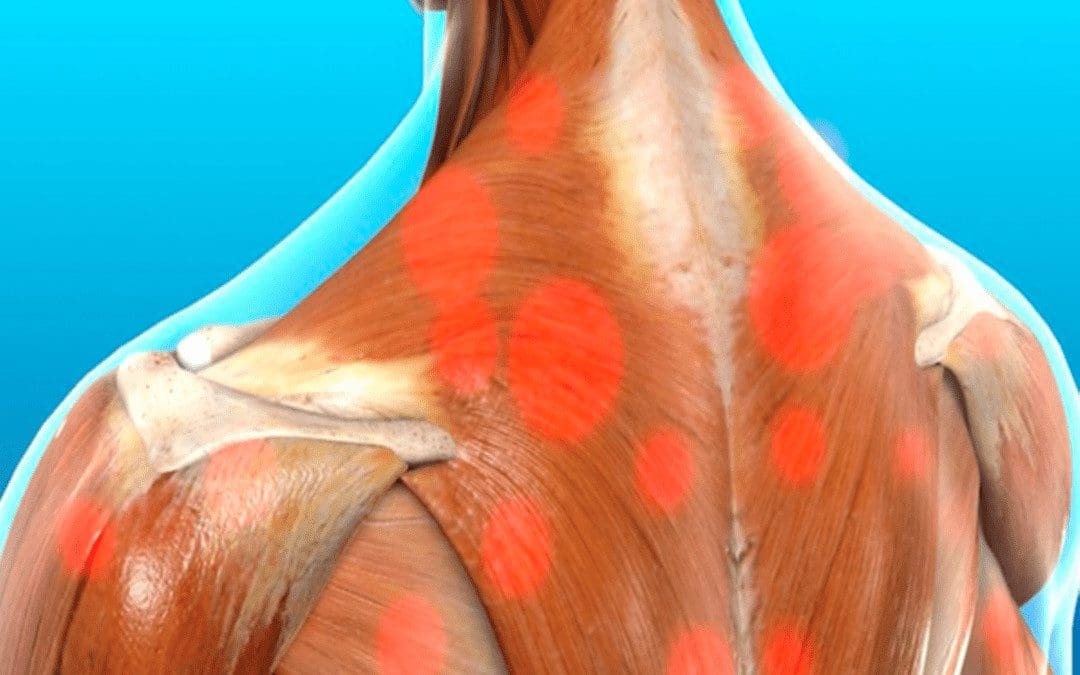
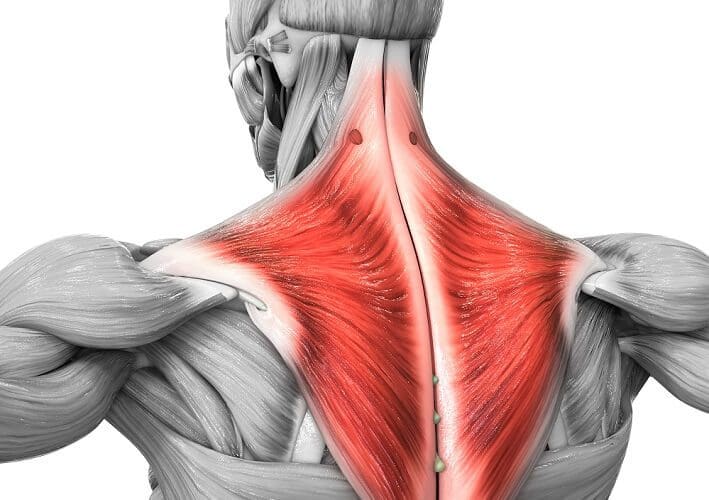
Have you experienced pain in your neck, shoulders, or mid-upper back? Do you feel headaches occurring near your temples? What about tenderness in certain areas of your body? Some of these symptoms may appear in your trapezius muscles. The trapezius muscle is located across the back that looks like a simple trapezoid with upper, middle, and lower muscle fibers that have different functions for the upper-middle back, shoulders, and neck. While the entire trapezius muscle helps rotates, elevate, and retract the scapula while extending the head and neck, and turning the chin by itself. At the same time, the entire muscle can help with assisting the extension of the cervical and thoracic spine.
Upper Trapezius muscles: allow the shoulders to rise, bend the head and neck, and help support the weight of the upper extremities of the body, including the arms.
Middle Trapezius muscles: assist with flexion and abduction of the arms around the shoulders at a nearly full range.
Lower Trapezius muscles: Helps retract the scapula while rotating the glenoid fossa upwards by decompressing the vertebral borders of the scapula. These fibers help assist the flexion and abduction of the arms.
When traumatic forces or injuries affect the trapezius muscles, painful symptoms begin to affect the muscles, causing them to be tender to the touch and affecting different areas in the body.
How Does Myofascial Pain Affect The Trapezius Muscle?
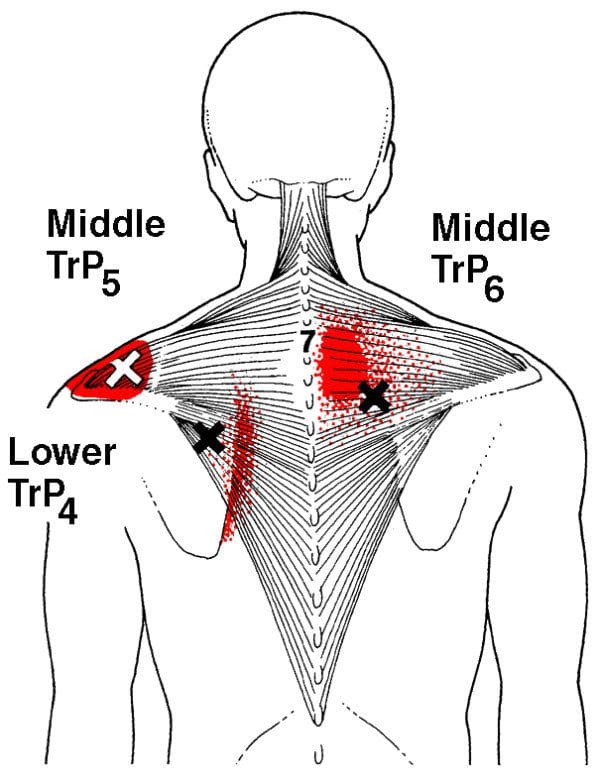
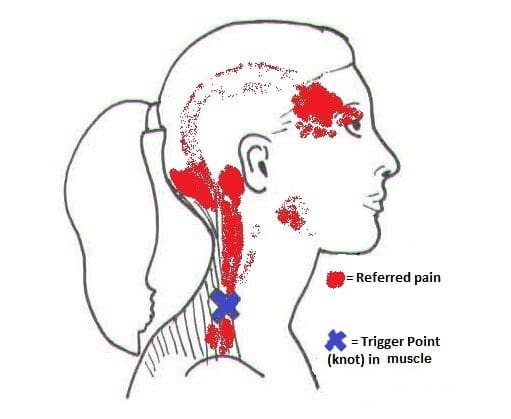
When traumatic forces or injuries affect the trapezius muscles, certain parts of the shoulders, neck, and upper-mid back will experience pain-related symptoms. When people experience headaches and shoulder and neck pain in their bodies while feeling tenderness in their trapezius muscles, this is known as referred pain associated with myofascial pain. Myofascial pain is when tiny knots along the taut muscle bands begin to make the muscle area tender to the touch. Individuals who suffer from myofascial pain in their trapezius muscles might experience hyperirritable spots that inflict pain and motor dysfunction. Studies reveal that individuals who work in food services may have symptoms of shoulder pain associated with myofascial pain due to repetitive motions on the upper trapezius muscles affecting their upper bodies. Myofascial trigger pain is a bit challenging to diagnose since the pain can be in different locations and mimic various ailments in the body. To that point, when the trapezius muscles are affected by trigger pain may potentially be involved with cervical myofascial pain. Cervical myofascial pain is a disorder that causes pain from muscle overuse or trauma in the neck. When the pain affects the neck muscles, it can travel down to the trapezius muscles causing tenderness and sensitivity in the affected muscle area. Stress, postural mechanics, or repetitive movements can develop myofascial pain syndrome and affect the surrounding muscles.
Trapezius Trigger Points- Video
Have you felt sore around your shoulders, neck, and upper-mid back? What about muscle tenderness in certain areas of your body? Do you feel tension along your neck or near the temples of your head? If you have been dealing with any of these symptoms, then you might be experiencing myofascial trapezius pain. The video above explains how trigger points from traumatic events can affect the trapezius muscle and cause referred pain that overlaps other conditions that may affect the body. Studies reveal that trigger points in the head and neck muscles of many suffering individuals have tension-type headaches. Tension-type headaches are one of the symptoms associated with myofascial trapezius pain. Some of the other symptoms related to myofascial pain affecting the trapezius muscle include:
Deep aching pain
Stiffness
Muscle spasms
Tightness around the shoulder and neck
Tenderness along the shoulders, neck, and upper back
Occipital headaches
How To Manage Myofascial Trapezius Pain
When many individuals suffer from myofascial trapezius pain, many would go to their primary doctor and explain to them that they are experiencing tension headaches constantly. Since myofascial pain is associated with the trapezius muscle is a bit complex and challenging for doctors to diagnose since every person’s pain is different. Many doctors will refer their patients to associated specialists like physical therapists, massage therapists, or chiropractors to determine where the pain is located along the trapezius muscle. Different treatments can help alleviate stiff muscles, and studies reveal that spinal manipulative therapy can help manage chronic pain from myofascial origins. Spinal subluxations or misalignment could potentially involve the corresponding spinal nerve root causing antinociceptive effects to the tender muscle, thus causing pain to the trapezius muscle. Utilizing various treatments to treat myofascial trapezius pain can provide individuals with beneficial relief from their pain along with managing their associated symptoms.
Conclusion
The trapezius muscle is a large superficial trapezoid-shaped muscle located in the back. The upper, middle, and lower muscle fibers have different functions in the head, neck, shoulders, and arms. The trapezius muscle also helps with assisting the extension of the cervical and thoracic spine. When traumatic events or injuries affect the trapezius muscle, it can be developed over time to create trigger points along the taut muscle band of the trapezius muscle and cause referred pain to the upper extremities of the body. Luckily various treatments can help manage the associated pain symptoms from myofascial trapezius pain and can help many individuals get back on their health and wellness journey.
References
Fernández-de-Las-Peñas, César, et al. “Myofascial Trigger Points and Their Relationship to Headache Clinical Parameters in Chronic Tension-Type Headache.” Headache, U.S. National Library of Medicine, Sept. 2006, https://pubmed.ncbi.nlm.nih.gov/16942471/.
Hwang, Ui-Jae, et al. “Predictors of Upper Trapezius Pain with Myofascial Trigger Points in Food Service Workers: The Strobe Study.” Medicine, Wolters Kluwer Health, June 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5500039.
Laframboise, Michelle A, et al. “Effect of Two Consecutive Spinal Manipulations in a Single Session on Myofascial Pain Pressure Sensitivity: A Randomized Controlled Trial.” The Journal of the Canadian Chiropractic Association, Canadian Chiropractic Association, June 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4915475/.
Ourieff, Jared, et al. “Anatomy, Back, Trapezius – StatPearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 26 July 2021, https://www.ncbi.nlm.nih.gov/books/NBK518994/.
Touma, Jeffrey, et al. “Cervical Myofascial Pain – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 4 July 2022, https://www.ncbi.nlm.nih.gov/books/NBK507825/.
The neck ensures that the head is upright in the body while providing mobility to rotate, bend, and tilt in various directions. The neck is part of the cervical spine and provides sensory-motor functions from the nerve pathways spread out along the shoulders and upper back. When traumatic events or injuries affect the cervical spine and cause pain to the neck over time, however, if not treated, it can lead to problematic symptoms associated with muscle pain. Neck pain can lead to muscle stiffness and cause myofascial trigger pain associated with referred pain along the rest of the upper body. Today’s article looks at the effects of neck pain, how it is associated with myofascial trigger pain, and ways to manage neck pain associated with myofascial trigger pain. We refer patients to certified providers specializing in musculoskeletal treatments to aid individuals suffering from neck pain associated with myofascial trigger pain. We also guide our patients by referring them to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Jimenez DC provides this information as an educational service only. Disclaimer
The Effects Of Neck Pain
Have you been feeling muscle stiffness around your neck and shoulders? Do you experience random headaches that affect your day? What about feeling tingling sensations along your arms and hands? These symptoms are associated with neck pain and can affect many individuals if not treated over time. Many people who suffer from neck pain will feel muscle stiffness that affects not only the sides of the neck but around the shoulders and their upper back. Studies reveal that neck pain is a multifactorial musculoskeletal disorder that affects the worldwide population and can become a chronic problem. Risk factors associated with the contributing development of neck pain include:
Stress
Poor posture
Anxiety
Sleep position
Neuromusculoskeletal disorders
Auto accidents
Traumatic events
Many of these risk factors associated with neck pain can cause pain symptoms and cause pain in different locations of the body, making diagnosing the pain source problematic for doctors.
Neck Pain Associated With Myofascial Trigger Pain
Since neck pain is common for many individuals, one of the symptoms associated with muscle stiffness and tenderness is myofascial trigger pain overlapping neck pain. Studies reveal that the formation of trigger points is caused when various physical activities begin to yield repetitive stress or cause micro-tears in the definite muscle groups that can cause tension within the muscle fibers. To that point, knots in the taut band of the muscles become hypersensitive and produce referred pain, tenderness, motor dysfunction, and autonomic phenomena. When the neck suffers from a traumatic event that affects the spine, over time can create trigger points or myofascial pain. It is difficult to diagnose where the pain is located in the body because myofascial trigger pain often mimics other pain conditions. It can confuse many individuals as they think they are suffering from one pain, but it’s a different pain that affects their body. Other studies reveal that individuals with myofascial pain syndrome associated with neck pain have a tender point within the tight muscular band, causing local discomfort. To that point, myofascial pain can cause referral pain in remote areas like cervical spine disorders like herniation can often be confused with myofascial pain when there is referral pain in the upper extremities of the body. Some of the symptoms associated with myofascial trigger pain that affects the neck include:
Deep, aching pain
Headaches
Muscle tenderness in the neck or shoulders
Tingling sensation or numbness down the arms and hands
Muscle stiffness
Neck Pain & Trigger Points- Video
Are you experiencing numbness that is running down your shoulders to your hands? What about muscle stiffness along the sides of the neck or shoulders? Or do headaches seem to pop out of nowhere and affect your day? You could risk suffering from neck pain associated with myofascial trigger pain. The video above explains how neck pain is associated with trigger points and how to trigger pain can be primary or secondary to neck pain. Studies reveal that myofascial pain syndrome is a common muscular pain disorder that is misunderstood and involves referred pain to form minor, tender trigger points within the muscles. To that point, myofascial pain associated with neck pain may be consistent with specific patterns of pain associated with each trigger point, contributing factors like emotional, postural, and behavioral factors that cause tension in the neck and frequently related symptoms from various conditions make diagnosing difficult. Since myofascial trigger points are complex and mimic other conditions that affect a different body part, many believe that different ailments affect their body than the actual ailment itself. Thankfully there are ways to manage neck pain associated with myofascial trigger pain and relieve muscle pain.
Ways To Manage Neck Pain Associated With Myofascial Trigger Pain
Since myofascial trigger pain associated with the neck can be a bit complex and challenging to diagnose, many doctors will refer patients to a physical therapist, a chiropractor, or another spine specialist to examine the trigger points causing neck pain. Various treatments can range from home remedies to severe muscle injections, depending on how severe the injuries are since everyone’s pain is different. Some of the available treatments that can reduce and manage myofascial neck pain include:
Exercising (helps stretch and strengthen neck and upper back muscles)
Massage (helps loosen stiff muscles in the neck and shoulders)
Heat therapy (helps relax and increase blood flow to the affected area)
Chiropractic care (uses spinal manipulation to prevent further pain issues from happening)
Acupuncture (helps to relax the trigger point and relieve pain)
Incorporating these various treatments can provide beneficial relief to those suffering from myofascial neck pain and help manage the symptoms associated with the body.
Conclusion
The neck provides mobility to the head as it can rotate, bend, and tilt in various directions while providing sensory-motor functions to the shoulders and upper back from the nerve roots in the cervical spine. When traumatic forces impact the neck, myofascial trigger pain can lead to neck pain. Myofascial trigger pain associated with neck pain is where tiny knots in the affected neck muscles become tender and stiff, which causes referred pain to different locations in the body. Myofascial neck pain is challenging to diagnose but manageable to treat with various treatments and techniques that can release the knots from the affected muscle and prevent future symptoms from happening. This allows many individuals to feel relief from their neck pain and continue their wellness journey.
References
Alghadir, Ahmad H, et al. “Efficacy of Combination Therapies on Neck Pain and Muscle Tenderness in Male Patients with Upper Trapezius Active Myofascial Trigger Points.” BioMed Research International, Hindawi, 10 Mar. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7085833/.
Ezzati, Kamran, et al. “Prevalence of Cervical Myofascial Pain Syndrome and Its Correlation with the Severity of Pain and Disability in Patients with Chronic Non-Specific Neck Pain.” The Archives of Bone and Joint Surgery, Mashhad University of Medical Sciences, Mar. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8121028/.
Fricton, J R, et al. “Myofascial Pain Syndrome of the Head and Neck: A Review of Clinical Characteristics of 164 Patients.” Oral Surgery, Oral Medicine, and Oral Pathology, U.S. National Library of Medicine, Dec. 1985, https://pubmed.ncbi.nlm.nih.gov/3865133/.
Kazeminasab, Somaye, et al. “Neck Pain: Global Epidemiology, Trends and Risk Factors.” BMC Musculoskeletal Disorders, BioMed Central, 3 Jan. 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8725362/.
The neck has two functions that allow the body to make sure that it holds the head up. The motor functions enable the neck to be mobile with the head as it can turn, twist and rotate without any discomfort or pain affecting it. For the sensory functions, the neck can feel when it has been stretched or adjusted or feel pain when it is injured. These two functions ensure that the neck is working correctly, but when injuries or unwanted events occur and affect the neck, it can cause unwanted problems. Neck injuries have a wide range of painful symptoms that can affect the spine’s head, neck, and cervical region. Today’s article will focus on myelopathy neck pain, its causes and symptoms, and how decompression therapy can help alleviate myelopathy neck pain for many individuals. Referring patients to qualified and skilled providers who specialize in spinal decompression therapy. We guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is essential for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
What Is Myelopathy Pain?
Have you been experiencing upper back or neck pain? Do you feel a tingling sensation running from your neck down to your hands? Or have you experienced difficulty in simple tasks like writing or putting on clothes? Experiencing these symptoms might show that you are suffering from myelopathy pain in the neck and cervical area of the spine. Research studies have defined myelopathy pain as when the neck suffers from a traumatic injury that causes severe compression on the spinal cord in the cervical area. The spinal cord in the spine has nerve roots that are branched out in the cervical region and allow the signals to be transported from the brain to the rest of the body. When traumatic injuries cause an impact on the spine, the blunt force will compress the spinal cord causing unwanted symptoms that affects either the cervical or lumbar portions of the spine. When the spinal cord becomes compressed, it can cause issues to the cervical part of the spine’s sensory and motor neck functions.
The Symptoms & Causes
When a person is suffering from myelopathy pain in the cervical regions of their spine, research studies have shown that the symptoms that myelopathy pain causes are motor dysfunction, where a person is having difficulty doing ordinary activities like getting ready for the day. Other symptoms that cervical myelopathy can cause to the neck are sensory dysfunctions, where the arms and hands feel numb to the touch. This tingling sensation gives off a pins and needles feeling to the body, and it can become uncomfortable for many individuals experiencing this sensation. This could be due to the cervical nerves and the spinal cord nerves being in pain. Additional research has mentioned that cervical myelopathy is caused when osteoarthritic changes in the spinal column that causes the spinal canal to be reduced. Myelopathy cervical pain can also be caused by cervical herniation in the neck, where the spinal discs aggravate the nerve roots. Other causes for the development of myelopathy are:
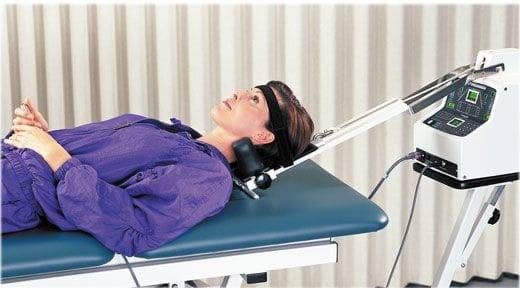
Feeling a tingling sensation running down from your shoulders to your hands? How about muscle stiffness from your neck turning it side to side? Is it difficult to do simple tasks like brushing your hair or buttoning up a shirt? Perhaps you are experiencing cervical myelopathy in the neck that is causing these symptoms, and decompression/traction treatments could be the relief you need. The video above shows how to assemble the Chatanooga decompression machine for cervical decompression/traction treatments. This treatment allows the individual to lay their head on the traction table and be secured. The device enables moderate pulling to release the pinched nerves from causing more pain to the neck and upper half of the body. Cervical decompression/traction can also help with neck and spinal issues like cervical herniation, radicular pain, and muscle stiffness. Cervical decompression/traction therapy has many beneficial factors in a person’s wellness treatment. This link will explainhow cervical decompression offers impressive relief for many people who suffer from neck pain and cervical myelopathy.
How Decompression Therapy Helps Alleviate Myelopathy Neck Pain
With myelopathy, neck pain causing not only neck pain but also upper body pain that hinders a person’s ability to do simple tasks. Research studies have shown that decompression surgery can help alleviate myelopathy neck pain by restoring the neurological motor function back in the spinal cord and providing relief to the cervical nerve roots. Other research studies have found that decompression treatments for myelopathy neck pain can help improve neck functionality, reduce neck disability, and even help restore a person’s quality of life by bringing back their motor function for the upper extremities that are associated with the neck.
Conclusion
Overall, having myelopathy neck pain can cause a person to lose their motor and sensory functions in their upper body. The factors like herniation, spinal spondylolysis, and spinal injuries are some of the causes of the development of myelopathy. It can make a person deal with constant neck pain without finding relief. Decompression treatments help many suffering individuals dealing with myelopathy neck pain by relieving the tension from the cervical nerve root that is causing the pain signals in the cervical area. By reducing the inflamed cervical nerve, people can feel the relief they desire when incorporating decompression treatments into their wellness journey.
References
Cheung, W Y, et al. “Neurological Recovery after Surgical Decompression in Patients with Cervical Spondylotic Myelopathy – a Prospective Study.” International Orthopaedics, Springer-Verlag, Apr. 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2269013/.
Donnally, Chester J, et al. “Cervical Myelopathy.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 6 Mar. 2022, https://www.ncbi.nlm.nih.gov/books/NBK482312/.
Fehlings;Wilson JR;Kopjar B;Yoon ST;Arnold PM;Massicotte EM;Vaccaro AR;Brodke DS;Shaffrey CI;Smith JS;Woodard EJ;Banco RJ;Chapman JR;Janssen ME;Bono CM;Sasso RC;Dekutoski MB;Gokaslan ZL;, Michael G. “Efficacy and Safety of Surgical Decompression in Patients with Cervical Spondylotic Myelopathy: Results of the Aospine North America Prospective Multi-Center Study.” The Journal of Bone and Joint Surgery. American Volume, U.S. National Library of Medicine, 18 Sept. 2013, https://pubmed.ncbi.nlm.nih.gov/24048552/.
Medical Professionals, Cleveland Clinic. “Myelopathy: Symptoms, Causes and Treatments.” Cleveland Clinic, 2 Oct. 2021, https://my.clevelandclinic.org/health/diseases/21966-myelopathy.
Milligan, James, et al. “Degenerative Cervical Myelopathy: Diagnosis and Management in Primary Care.” Canadian Family Physician Medecin De Famille Canadien, College of Family Physicians of Canada, Sept. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6741789/.
The neck allows the head to turn up, down, left, right, and side to side while supporting it. The neck is also part of the cervical spine as ligaments, muscles, and spinal discs surround it. However, just like the lower back, the neck is sustainable to suffer from neck-related injuries or pulled muscles that can cause many individuals to suffer from neck pain. Luckily there are ways to treat neck pain like gentle stretches, chiropractic adjustments, massages, and decompression therapy. Today’s article will discuss the cervical nerves, what happens to the neck when these nerves are pinched, and how cervical decompression therapy can help alleviate the pinched cervical nerves from the neck. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
The Cervical Nerves
The cervical nerve’s function is to conduct information on the motor and sensory skills that the neck is allowed to do. Since the neck’s primary function is to keep the head upright, research studies have found that the cervical regions of the spinal cord are where the cervical nerves lie. The cervical nerves branched out all over the neck muscles as the central nervous system allows the neuron signals to send the information to the cervical nerves. These nerve functions help control the head, neck, shoulders, and upper limbs to move in any direction without feeling pain. However, just like the lower back, the neck can also suffer from injuries, pulled muscles, or chronic conditions that can cause a person to be in pain.
What Happens When The Cervical Nerves Are Pinched?
Have you ever felt your back, neck, arms, or legs stiff? How about the sensations of feeling tingles on your shoulders, lower back, or even your arms? This might be due to pinched nerves if you suffer from these conditions. When the neck suffers from an injury or the muscles have become tense, this is due to a pinched cervical nerve. Research studies have found that a pinched nerve in the cervical area of the spine is mostly a compressed nerve due to a herniated disc. This causes pressure on the cervical nerve roots and causes radiating pain from the neck to the shoulders and down to the arms.
The cervical nerves send out radiating pain signals to the upper body and neck due to being compressed, causing the individual to be miserable. Other research studies have found that when the cervical nerve roots are being pinched, it can cause a condition known as cervical radiculopathy. This causes symptoms of pain, sensory and motor deficits, and even diminishes reflexes from the neck to the arms. When this happens to the neck, it can cause many problems for the individual. Research studies have stated that mechanical and degenerative factors are presented for many suffering from chronic neck pain. In contrast, those suffering from cervical spondylosis complain about neck stiffness, degenerative changes, and neurological complications to the body and neck.
Treating Pinched Nerves With Decompression Therapy-Video
Has your neck been feeling stiff lately? Does it hurt when you are turning your head from side to side? You could be experiencing a pinched nerve in the cervical area of the spine, and decompression therapy could be the answer. Cervical decompression allows a person to lay on a motorized traction table, and the machine gently pulls on the cervical spine and takes the pressure off the cervical nerve root. When the cervical decompression machine gently pulls the cervical spine, it allows the necessary nutrients to rehydrate the herniated disc and reduce the pain that the neck muscles were suffering from, causing them to relax. In case you want to learn more about cervical decompression therapy, this link will explain its benefits and how it can alleviate pinched cervical nerves.
As stated earlier, many treatments can help many dealing with neck pain and compressed cervical pinch nerves. One of these treatments is cervical traction decompression therapy, and it can help alleviate not only neck pain but also reduce it. Research studies have found that many individuals suffering from cervical radiculopathy utilize cervical traction to increase the intervertebral disc gap while also relieving the pressure off the cervical root. This allows the neck muscles to relax and pull the herniated cervical disc back to the spine. When people utilize cervical decompression to alleviate their neck pain, they can feel relief after a few sessions.
Conclusion
Overall, cervical decompression therapy allows the individual to feel relief through gentle stretching on the cervical spinal discs and takes the pressure off the cervical roots. When the cervical roots are compressed, it causes a wide variety of symptoms that causes problems from the neck down to the arms. Some of these symptoms can even affect a person’s quality of life and make them miserable if not treated right away. Utilizing decompression therapy and other non-surgical treatments allows the person to be pain-free and continue their wellness journey.
References
Binder, Allan I. “Cervical Spondylosis and Neck Pain.” BMJ (Clinical Research Ed.), BMJ Publishing Group Ltd., 10 Mar. 2007, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1819511/.
Iyer, Sravisht, and Han Jo Kim. “Cervical Radiculopathy.” Current Reviews in Musculoskeletal Medicine, Springer US, Sept. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4958381/.
Khan, Rehan Ramzan, et al. “A Randomized Controlled Trial of Intermittent Cervical Traction in Sitting vs. Supine Position for the Management of Cervical Radiculopathy.” Pakistan Journal of Medical Sciences, Professional Medical Publications, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5768820/.
Waxenbaum, Joshua A, et al. “Anatomy, Head and Neck, Cervical Nerves.” StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 26 July 2021, https://www.ncbi.nlm.nih.gov/books/NBK538136/.
Do you ever get that stiff feeling just by turning your head, or do your shoulders start to feel tense after a stressful day at work? How about feeling a headache coming on for no apparent reason? This is due to neck pain, and many factors can cause a person to have neck pain. Even though neck pain can be a nuisance to many individuals, there are therapeutic ways to alleviate neck pain: one of them is cervical decompression therapy. This article will look at what neck pain is, its symptoms, and how decompression therapy can help alleviate neck pain for many individuals. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is Neck Pain?
As part of the cervical spine, the neck supports the head while surrounding and protecting the spinal cord and allows a wide range of motion. Research studies have found that the neck has a coordinated network of nerves, bones, joints, and muscles that have an essential job but have several problems that can cause pain. Neck pain is a common complaint among many individuals, as the neck muscles are strained for long periods due to poor posture. Other research studies have found any injuries or conditions affecting the neck, causing a restricted range of motion. This can be scary for many individuals due to being hunched over by looking at their phones, being on the computer, even minor things like reading a book or suffering from an auto accident, and having rheumatoid arthritis can affect the neck.
The Symptoms For Dealing With Neck Pain
Pain can come in two types of forms, which are acute and chronic. Acute pain can become a dull, mild ache that can last from a few hours to a few days, depending on where the person is injured. Chronic pain, however, can become a nuisance as it can send constant radiating pain that can cause a hindrance to any part of the body. As research has shown, the pain can vary for neck pain as it can become mild and uncomfortable to excruciating, where excess movement can make it worst. Some of the most common neck pain symptoms usually involve:
Even though neck pain can become a nuisance for many individuals, there are ways to alleviate the symptoms of neck pain and provide relief.
Cervical Decompression Therapy-Video
Research studies have found that manipulation, stretching, and strengthening of the neck muscle can reduce the chronic pain symptoms that it has caused. The video above shows what cervical decompression does for many individuals suffering from cervical pain and neck pain. Cervical decompression therapy lets individuals lay their heads on the traction table and are strapped in. The traction machine gently stretches the cervical spine to release the compressed spinal disc. Cervical decompression therapy allows the compressed spinal nerve roots to be alleviated from the cervical spine. It will enable the beneficial oxygen to come back into the spinal disc and increase the disc height for the neck. If you want to learn more about spinal decompression therapy, this link will explain the benefits of spinal decompression and how it can alleviate low back pain symptoms.
How Can Decompression Therapy Help With Neck Pain
As stated earlier in the article, feeling stiffness when turning your head, feeling the tension in the shoulders, and having headaches pop up out of nowhere is scary when you don’t know how they happened. When these symptoms start to turn into chronic issues, it can be hard to find relief to get rid of the pain. Luckily there is a solution for alleviating neck pain, and cervical decompression therapy could help get rid of the pain. Cervical decompression therapy allows individuals to lay their heads on the traction table and be strapped in, causing the traction machine to stretch the neck to alleviate the painful symptoms gently. Research studies have found that cervical decompression therapy can relieve tension headaches and improve the range of motion. This will cause the spinal disc to be stretched and alleviate symptoms caused by cervical herniated discs. Combined with light stretching, cervical decompression therapy can also improve cervical disc herniation symptoms. Research shows that this combination of treatments promotes neuromuscular tissue edema and inflammatory absorption from the cervical herniated disc. This will allow the restoration of the curvature of the cervical vertebrae and reduce disc pressure by improving it.
Conclusion
Having any neck pain is a nuisance, and if it is not treated right away, it can become an issue over time. Neck pain can cause stiffness to the neck muscles and disrupt the range of motion, making it unbearable for the individual to turn their heads from left to right and up and down. Luckily treatments like cervical decompression therapy allow individuals to feel relief from neck pain. Cervical decompression therapy provides traction to the individual by stretching the neck ligament gently to release the compressed cervical spinal discs and will enable the reduction of pain that is causing discomfort to the neck. When this happens, many individuals suffering from neck pain will feel instant relief and an improvement in their range of motion from their necks.
References
Binder, Allan I. “Neck Pain.” BMJ Clinical Evidence, BMJ Publishing Group, 4 Aug. 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2907992/.
Landers, Merrill R, et al. “Anterior Cervical Decompression and Fusion on Neck Range of Motion, Pain, and Function: A Prospective Analysis.” The Spine Journal: Official Journal of the North American Spine Society, U.S. National Library of Medicine, Nov. 2013, https://pubmed.ncbi.nlm.nih.gov/24041918/.
Staff, Mayo Clinic. “Neck Pain.” Mayo Clinic, Mayo Foundation for Medical Education and Research, 31 July 2020, https://www.mayoclinic.org/diseases-conditions/neck-pain/symptoms-causes/syc-20375581.
Xu, Qing, et al. “Nonsurgical Spinal Decompression System Traction Combined with Electroacupuncture in the Treatment of Multi-Segmental Cervical Disc Herniation: A Case Report.” Medicine, Lippincott Williams & Wilkins, 21 Jan. 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8772752/.
Rheumatoid arthritis, or RA, is a chronic health issue which affects approximately 1 percent of the population in the United States. RA is an autoimmune disorder that causes the inflammation and degeneration of the synovial tissue, specific cells and tissue which form the lining of the joints within the human body. Rheumatoid arthritis may and generally does affect every joint in the body, especially as people get older. RA commonly develops in the joints of the hands and feet, severely restricting an individual’s ability to move, however, those with significant disease in the spine are at risk of damage like paraplegia. Rheumatoid arthritis of the spine is frequent in three areas, causing different clinical problems.
The first is basilar invagination, also referred to as cranial settling or superior migration of the odontoid, a health issue where degeneration from rheumatoid arthritis at the base of the skull causes the it to “settle” into the spinal column, causing the compression or impingement of the spinal cord between the skull and the 1st cervical nerves. The second health issue, and also the most frequent, is atlanto-axial instability. A synovitis and erosion of the ligaments and joints connecting the 1st (atlas) and the 2nd (axis) cervical vertebrae causes instability of the joint, which may ultimately result in dislocation and spinal cord compression. In addition, a pannus, or localized mass/swelling of rheumatoid synovial tissue, can also form in this region, causing further spinal cord compression. The third health issues is a subaxial subluxation which causes the degeneration of the cervical vertebrae (C3-C7) and often results in other problems like spinal stenosis.
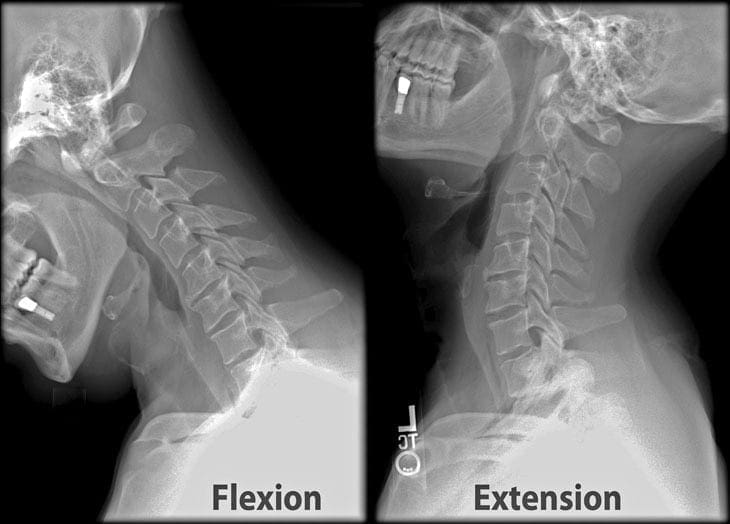
Imaging studies are crucial to properly diagnose patients with rheumatoid arthritis of the cervical spine. X-rays will demonstrate the alignment of the spine, and if there is obvious cranial settling or instability. It can also be difficult to demonstrate the anatomy at the bottom of the skull, therefore, computed tomography scanning, or CT scan, with an injection of dye within the thecal sac is arranged. Magnetic resonance imaging, or MRI, is beneficial to assess the severity of nerve compression or spinal cord injury, and allows visualization of structures, including the nerves, muscles, and soft tissues. Flexion/extension x-rays of the cervical spine are usually obtained to evaluate for signs of ligamentous instability. These imaging studies entails a plain lateral x-ray being taken with the patient bending forward and the other lateral x-ray being taken with the individual extending the neck backwards.�The scope of our information is limited to chiropractic, spinal injuries, and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain and Auto Injury
Whiplash is one of the most common causes of neck pain after an automobile accident. A whiplash-associated disorder occurs when a person’s head and neck moves abruptly back-and-forth, in any direction, due to the force of an impact. Although whiplash most commonly occurs following a rear-end car crash, it can also result from sports injuries. During an auto accident, the sudden motion of the human body can cause the muscles, ligaments, and other soft tissues of the neck to extend beyond their natural range of motion, causing damage or injury to the complex structures surrounding the cervical spine. While whiplash-associated disorders are considered to be relatively mild health issues, these can cause long-term pain and discomfort if left untreated. Diagnosis is essential.
While computed tomography scanning, or CT scans, of the cervical spine are frequently utilized to help diagnose neck injuries, simple radiographs are still commonly performed for patients who have experienced minor cervical spine injuries with moderate neck pain, such as those who have suffered a slip-and-fall accident. Imaging diagnostic assessments may reveal underlying injuries and/or aggravated conditions to be more severe than the nature of the trauma. The purpose of the article is to demonstrate the significance of cervical spine radiographs in the trauma patient.�
Abstract
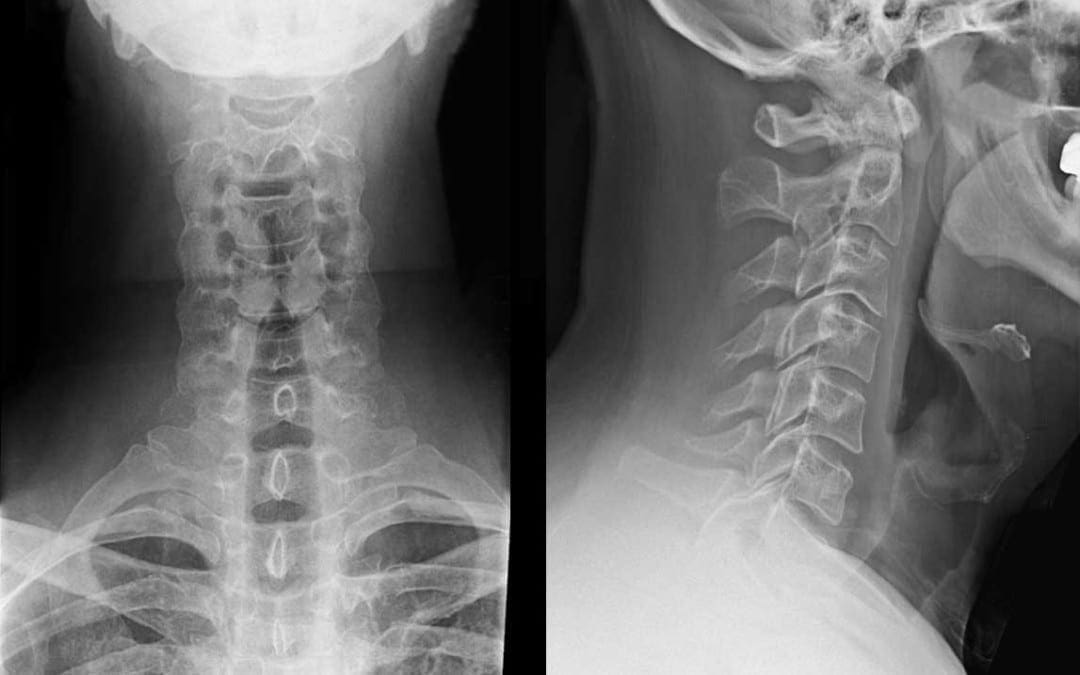
Significant cervical spine injury is very unlikely in a case of trauma if the patient has normal mental status (including no drug or alcohol use) and no neck pain, no tenderness on neck palpation, no neurologic signs or symptoms referable to the neck (such as numbness or weakness in the extremities), no other distracting injury and no history of loss of consciousness. Views required to radiographically exclude a cervical spine fracture include a posteroanterior view, a lateral view and an odontoid view. The lateral view must include all seven cervical vertebrae as well as the C7-T1 interspace, allowing visualization of the alignment of C7 and T1. The most common reason for a missed cervical spine injury is a cervical spine radiographic series that is technically inadequate. The �SCIWORA� syndrome (spinal cord injury without radiographic abnormality) is common in children. Once an injury to the spinal cord is diagnosed, methylprednisolone should be administered as soon as possible in an attempt to limit neurologic injury.
Radiographs continue to be used as a first-line imaging diagnostic assessment modality in the evaluation of patients with suspected cervical spine injuries. The aim of cervical spine radiographs is to confirm the presence of a health issue in the complex structures of the neck and define its extent, particularly with respect to instability. Multiple views may generally be necessary to provide optimal visualization.
Dr. Alex Jimenez D.C., C.C.S.T.
Introduction
Although cervical spine radiographs are almost routine in many emergency departments, not all trauma patients with a significant injury must have radiographs, even if they arrive at the emergency department on a backboard and wearing a cervical collar. This article reviews the proper use of cervical spine radiographs in the trauma patient.
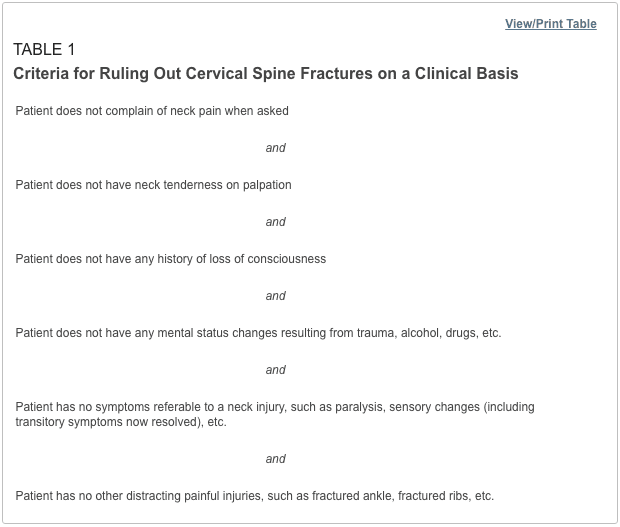
Low-risk criteria have been defined that can be used to exclude cervical spine fractures, based on the patient’s history and physical examination.1�6 Patients who meet these criteria (Table 1) do not require radiographs to rule out cervical fractures. However, the criteria apply only to adults and to patients without mental status changes, including drug or alcohol intoxication. Although studies suggest that these criteria may also be used in the management of verbal children,7�9 caution is in order, since the study series are small, and the ability of children to complain about pain or sensory changes is variable. An 18-year-old patient can give a more reliable history than a five-year-old child.
Some concern has been expressed about case reports suggesting that �occult� cervical spine fractures will be missed if asymptomatic trauma patients do not undergo radiography of the cervical spine.10 On review, however, most of the reported cases did not meet the low-risk criteria in Table 1. Attention to these criteria can substantially reduce the use of cervical spine radiographs.
Cervical Spine Series and Computed Tomography
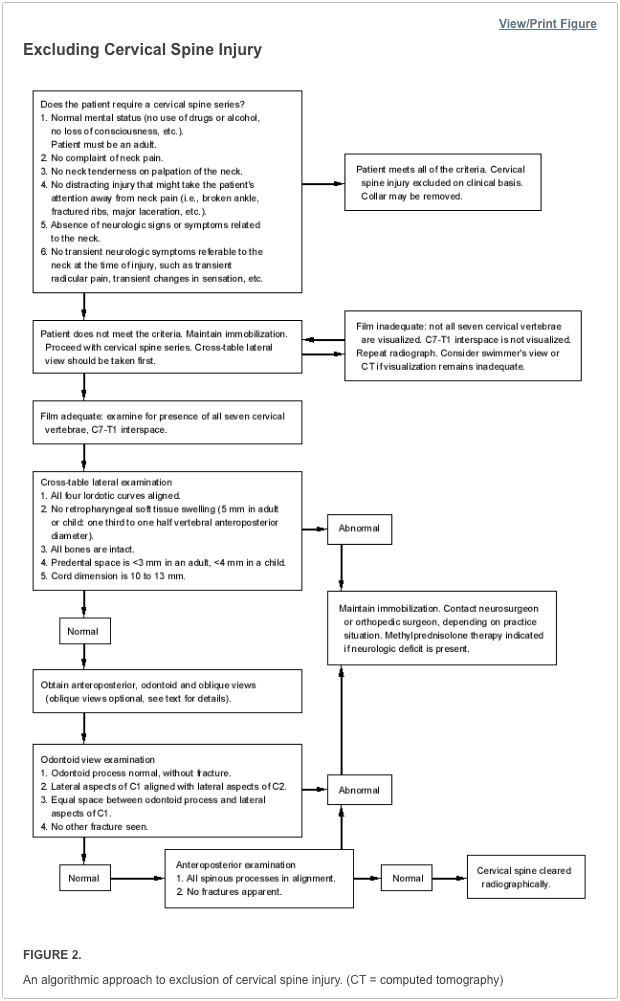
Once the decision is made to proceed with a radiographic evaluation, the proper views must be obtained. The single portable cross-table lateral radiograph, which is sometimes obtained in the trauma room, should be abandoned. This view is insufficient to exclude a cervical spine fracture and frequently must be repeated in the radiographic department.11,12 The patient’s neck should remain immobilized until a full cervical spine series can be obtained in the radiographic department. Initial films may be taken through the cervical collar, which is generally radiolucent. An adequate cervical spine series includes three views: a true lateral view, which must include all seven cervical vertebrae as well as the C7-T1 junction, an anteroposterior view and an open-mouth odontoid view.13
If no arm injury is present, traction on the arms may facilitate visualization of all seven cervical vertebrae on the lateral film. If all seven vertebrae and the C7-T1 junction are not visible, a swimmer’s view, taken with one arm extended over the head, may allow adequate visualization of the cervical spine. Any film series that does not include these three views and that does not visualize all seven cervical vertebrae and the junction of C7-T1 is inadequate. The patient should be maintained in cervical immobilization, and plain films should be repeated or computed tomographic (CT) scans obtained until all vertebrae are clearly visible. The importance of obtaining all of these views and visualizing all of the vertebrae cannot be overemphasized. While some missed cervical fractures, subluxations and dislocations are the result of film misinterpretation, the most frequent cause of overlooked injury is an inadequate film series.14,15
In addition to the views listed above, some authors suggest adding two lateral oblique views.16,17 Others would obtain these views only if there is a question of a fracture on the other three films or if the films are inadequate because the cervicothoracic junction is not visualized.18 The decision to take oblique views is best made by the clinician and the radiologist who will be reviewing the films.
Besides identifying fractures, plain radiographs can also be useful in identifying ligamentous injuries. These injuries frequently present as a malalignment of the cervical vertebrae on lateral views. Unfortunately, not all ligamentous injuries are obvious. If there is a question of ligamentous injury (focal neck pain and minimal malalignment of the lateral cervical x-ray [meeting the criteria in Table 2]) and the cervical films show no evidence of instability or fracture, flexion-extension views should be obtained.17,19 These radiographs should only be obtained in conscious patients who are able to cooperate. Only active motion should be allowed, with the patient limiting the motion of the neck based on the occurrence of pain. Under no circumstance should cervical spine flexion and extension be forced, since force may result in cord injury.
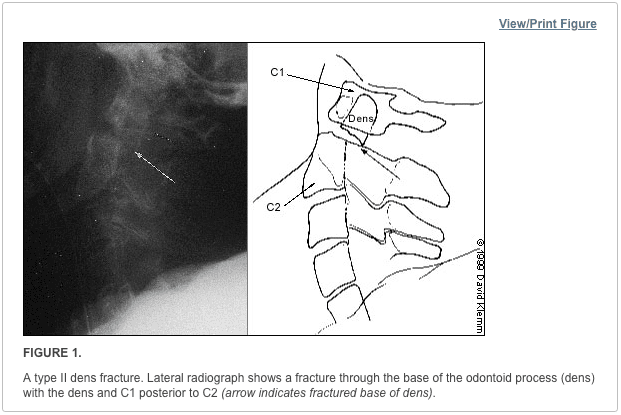
Although they may be considered adequate to rule out a fracture, cervical spine radiographs have limitations. Up to 20 percent11,20,21 of fractures are missed on plain radiographs. If there is any question of an abnormality on the plain radiograph or if the patient has neck pain that seems to be disproportionate to the findings on plain films, a CT scan of the area in question should be obtained. The CT is excellent for identifying fractures, but its ability to show ligamentous injuries is limited.22 Occasionally, plain film tomography may be in order if there is a concern about a type II dens fracture (Figure 1).
While some studies have used magnetic resonance imaging (MRI) as an adjunct to plain films and CT scanning,23,24 the lack of wide availability and the relatively prolonged time required for MRI scanning limits its usefulness in the acute setting. Another constraint is that resuscitation equipment with metal parts may not be able to function properly within the magnetic field generated by the MRI.
Cervical Spine Radiography
Figure 2 summarizes the approach to reading cervical spine radiographs.
Lateral View
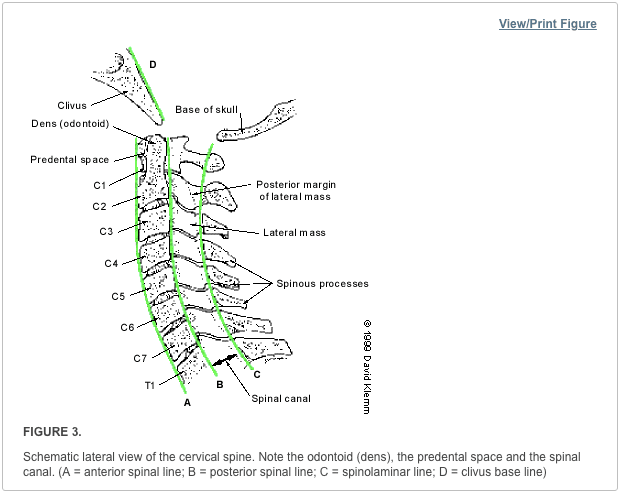
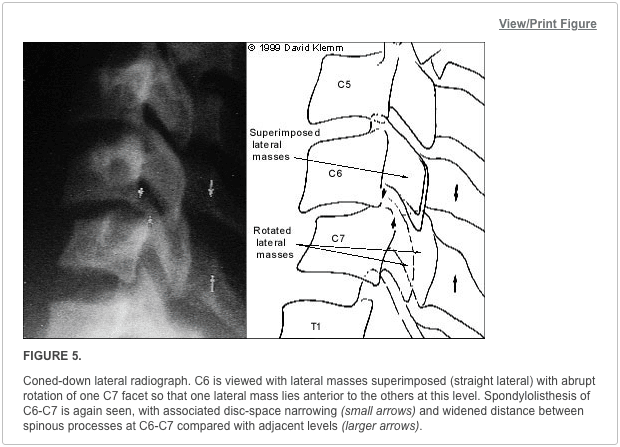
Alignment of the vertebrae on the lateral film is the first aspect to note (Figure 3). The anterior margin of the vertebral bodies, the posterior margin of the vertebral bodies, the spinolaminar line and the tips of the spinous processes (C2-C7) should all be aligned. Any malalignment (Figures 4 and 5) should be considered evidence of ligamentous injury or occult fracture, and cervical spine immobilization should be maintained until a definitive diagnosis is made.
Confusion can sometimes result from pseudosubluxation, a physiologic misalignment that is due to ligamentous laxity, which can occur at the C2-C3 level and, less commonly, at the C3-C4 level. While pseudosubluxation usually occurs in children, it also may occur in adults. If the degree of subluxation is within the normal limits listed in Table 2 and the neck is not tender at that level, flexion-extension views may clarify the situation. Pseudosubluxation should disappear with an extension view. However, flexion-extension views should not be obtained until the entire cervical spine is otherwise cleared radiographically.
After ensuring that the alignment is correct, the spinous processes are examined to be sure that there is no widening of the space between them. If widening is present, a ligamentous injury or fracture should be considered. In addition, if angulation is more than 11 degrees at any level of the cervical spine, a ligamentous injury or fracture should be assumed. The spinal canal (Figure 2) should be more than 13 mm wide on the lateral view. Anything less than this suggests that spinal cord compromise may be impending.
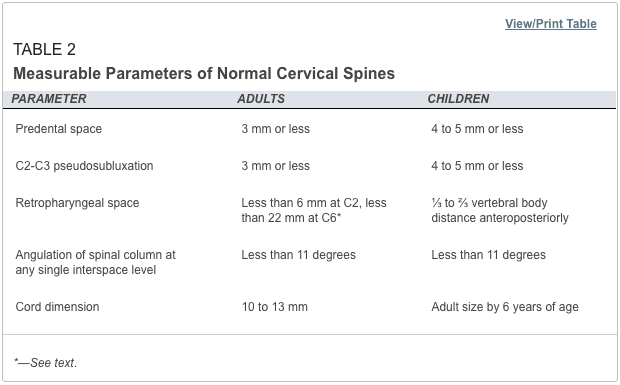
Next, the predental space�the space between the odontoid process and the anterior portion of the ring of C1 (Figure 2)�is examined. This space should be less than 3 mm in adults and less than 4 mm in children (Table 2). An increase in this space is presumptive evidence of a fracture of C1 or of the odontoid process, although it may also represent ligamentous injury at this level. If a fracture is not found on plain radiographs, a CT scan should be obtained for further investigation. The bony structures of the neck should be examined, with particular attention to the vertebral bodies and spinous processes.
The retropharyngeal space (Figure 2) is now examined. The classic advice is that an enlarged retropharyngeal space (Table 2) indicates a spinous fracture. However, the normal and abnormal ranges overlap significantly.25 Retropharyngeal soft tissue swelling (more than 6 mm at C2, more than 22 mm at C6) is highly specific for a fracture but is not very sensitive.26 Soft tissue swelling in symptomatic patients should be considered an indication for further radiographic evaluation. Finally, the craniocervical relationship is checked.
Odontoid View
The dens is next examined for fractures. Artifacts may give the appearance of a fracture (either longitudinal or horizontal) through the dens. These artifacts are often radiographic lines caused by the teeth overlying the dens. However, fractures of the dens are unlikely to be longitudinally oriented. If there is any question of a fracture, the view should be repeated to try to get the teeth out of the field. If it is not possible to exclude a fracture of the dens, thin-section CT scans or plain film tomography is indicated.
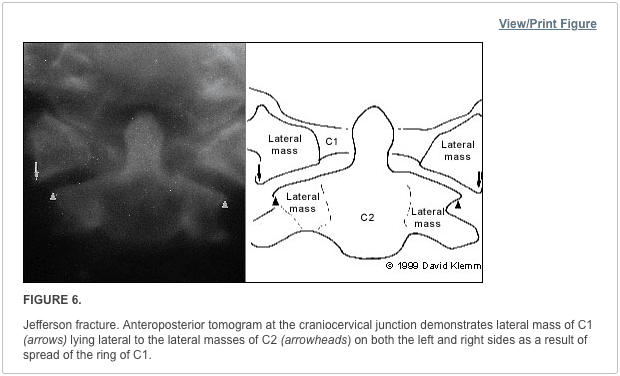
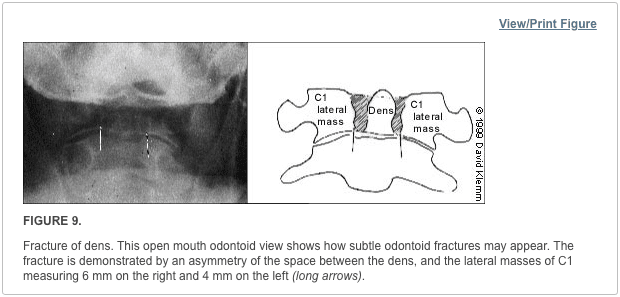
Next, the lateral aspects of C1 are examined. These aspects should be symmetric, with an equal amount of space on each side of the dens. Any asymmetry is suggestive of a fracture. Finally, the lateral aspects of C1 should line up with the lateral aspects of C2. If they do not line up, there may be a fracture of C1. Figure 6 demonstrates asymmetry in the space between the dens and C1, as well as displacement of the lateral aspects of C1 laterally.
Anteroposterior View
The height of the cervical spines should be approximately equal on the anteroposterior view. The spinous processes should be in midline and in good alignment. If one of the spinous processes is off to one side, a facet dislocation may be present.
Common Cervical Abnormalities
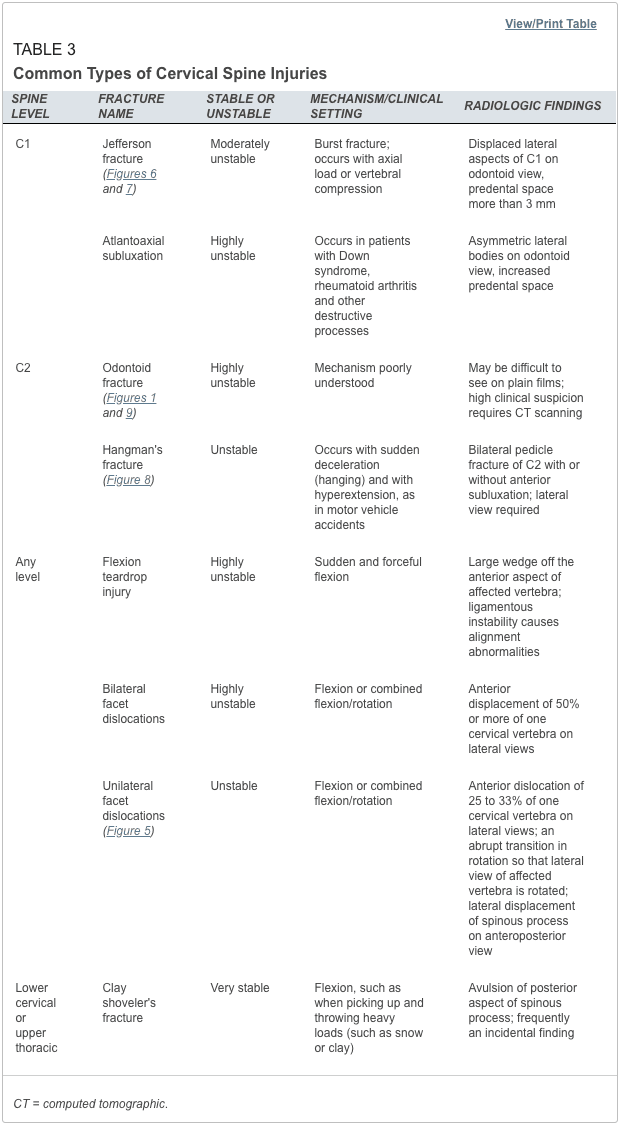
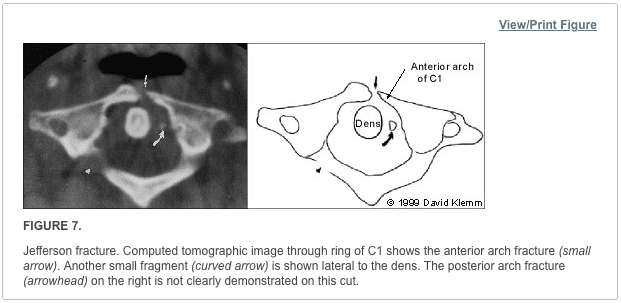
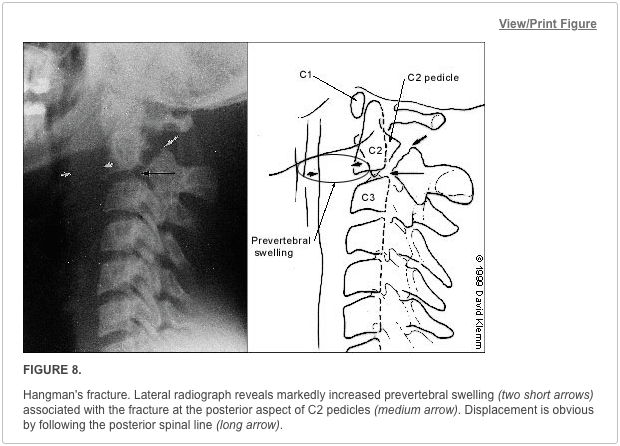
The most common types of cervical abnormalities and their radiographic findings are listed in Table 3. Except for the clay shoveler’s fracture, they should be assumed to be unstable and warrant continued immobilization until definitive therapy can be arranged. Any patient found to have one spinal fracture should have an entire spine series, including views of the cervical spine, the thoracic spine and the lumbosacral spine. The incidence of noncontiguous spine fractures ranges up to 17 percent.27,28 Figures 7 through 9 demonstrate aspects of common cervical spine fractures.
Initial Treatment of Cervical Spine and Cord
If a cervical fracture or dislocation is found, orthopedic or neurosurgical consultation should be obtained immediately. Any patient with a spinal cord injury should begin therapy with methylprednisolone within the first eight hours after the injury, with continued administration for up to 24 hours. Patients should receive methylprednisolone in a dosage of 30 mg per kg given intravenously over one hour. Over the next 23 hours, intravenous methylprednisolone in a dosage of 5.4 mg per kg per hour should be administered. This therapy has been shown to improve outcomes and minimize cord injury,29 although it is not without its problems. The incidence of pneumonia is increased in patients treated with high dosages of methylprednisolone.30
�Sciwora� Syndrome: Unique in Children
A special situation involving children deserves mention. In children, it is not uncommon for a spinal cord injury to show no radiographic abnormalities. This situation has been named �SCIWORA� (spinal cord injury without radiographic abnormality) syndrome. SCIWORA syndrome occurs when the elastic ligaments of a child’s neck stretch during trauma. As a result, the spinal cord also undergoes stretching, leading to neuronal injury or, in some cases, complete severing of the cord.31 This situation may account for up to 70 percent of spinal cord injuries in children and is most common in children younger than eight years. Paralysis may be present on the patient’s arrival in the emergency department. However, up to 30 percent of patients have a delayed onset of neurologic abnormalities, which may not occur until up to four or five days after the injury. In patients with delayed symptoms, many have neurologic symptoms at the time of the injury, such as paresthesias or weakness, that have subsequently resolved.32
It is important to inform the parents of young patients with neck trauma about this possibility so that they will be alert for any developing symptoms or signs. Fortunately, most children with SCIWORA syndrome have a complete recovery, especially if the onset is delayed.33 It is possible to evaluate these injuries with MRI, which will show the abnormality and help determine the prognosis: a patient with complete cord transection is unlikely to recover.3
The treatment of SCIWORA syndrome has not been well studied. However, the general consensus is that steroid therapy should be used.34 In addition, any child who has sustained a significant degree of trauma but has recovered completely should be restricted from physical activities for several weeks.34
Cervical spine radiographs include three standard views, such as the coned odontoid peg view, the anteroposterior view of the entire cervical spine, and the lateral view of the entire cervical spine. Most qualified and experienced healthcare professionals, including chiropractors, offer additional views to visualize the cervicothoracic junction as well as to evaluate the proper alignment of the spine in all patients.�
Dr. Alex Jimenez D.C., C.C.S.T.
About the Authors
MARK A. GRABER, M.D., is associate professor of clinical family medicine and surgery (emergency medicine) at the University of Iowa Hospitals and Clinics, Iowa City. He received his medical degree from Eastern Virginia Medical School, Norfolk, and served a residency in family medicine at the University of Iowa College of Medicine, Iowa City.
MARY KATHOL, M.D., is associate professor of radiology at the University of Iowa Hospitals and Clinics. She is also head of the musculoskeletal radiology section. She received her medical degree from the University of Kansas School of Medicine, Kansas City, Kan., and served a residency in radiology at the University of Iowa College of Medicine.
Address correspondence to Mark A. Graber, M.D., Department of Family Medicine, Steindler Bldg., University of Iowa Hospitals and Clinics, Iowa City, Iowa 52242. Reprints are not available from the authors.
In conclusion,�it is essential to evaluate all views of the cervical spine through imaging diagnostic assessments. While cervical spine radiographs can reveal injuries and conditions, not all neck injuries are detected through radiography. Computed tomography, or CT, scans of the cervical spine are highly accurate in the diagnosis of neck fractures which can help with treatment. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
1.�Kreipke DL, Gillespie KR, McCarthy MC, Mail JT, Lappas JC, Broadie TA. Reliability of indications for cervical spine films in trauma patients.�J Trauma. 1989;29:1438�9.
2.�Ringenberg BJ, Fisher AK, Urdaneta LF, Midthun MA. Rational ordering of cervical spine radiographs following trauma.�Ann Emerg Med. 1988;17:792�6.
3.�Bachulis BL, Long WB, Hynes GD, Johnson MC. Clinical indications for cervical spine radiographs in the traumatized patient.�Am J Surg. 1987;153:473�8.
4.�Hoffman JR, Schriger DL, Mower W, Luo JS, Zucker M. Low-risk criteria for cervical-spine radiography in blunt trauma: a prospective study.�Ann Emerg Med. 1992;21:1454�60.
5.�Saddison D, Vanek VW, Racanelli JL. Clinical indications for cervical spine radiographs in alert trauma patients.�Am Surg. 1991;57:366�9.
6.�Kathol MH, El-Khoury GY. Diagnostic imaging of cervical spine injuries.�Seminars in Spine Surgery. 1996;8(1):2�18.
7.�Lally KP, Senac M, Hardin WD Jr, Haftel A, Kaehler M, Mahour GH. Utility of the cervical spine radiograph in pediatric trauma.�Am J Surg. 1989;158:540�1.
8.�Rachesky I, Boyce WT, Duncan B, Bjelland J, Sibley B. Clinical prediction of cervical spine injuries in children. Radiographic abnormalities.�Am J Dis Child. 1987;141:199�201.
9.�Laham JL, Cotcamp DH, Gibbons PA, Kahana MD, Crone KR. Isolated head injuries versus multiple trauma in pediatric patients: do the same indications for cervical spine evaluation apply?�Pediatr Neurosurg. 1994;21:221�6.
10.�McKee TR, Tinkoff G, Rhodes M. Asymptomatic occult cervical spine fracture: case report and review of the literature.�J Trauma. 1990;30:623�6.
11.�Woodring JH, Lee C. Limitations of cervical radiography in the evaluation of acute cervical trauma.�J Trauma. 1993;34:32�9.
12.�Spain DA, Trooskin SZ, Flancbaum L, Boyarsky AH, Nosher JL. The adequacy and cost effectiveness of routine resuscitation-area cervical-spine radiographs.�Ann Emerg Med. 1990;19:276�8.
13.�Tintinalli JE, Ruiz E, Krome RL, ed. Emergency medicine: a comprehensive study guide. 4th ed. New York: McGraw-Hill, 1996.
15.�Davis JW, Phreaner DL, Hoyt DB, Mackersie RC. The etiology of missed cervical spine injuries.�J Trauma. 1993;34:342�6.
16.�Apple JS, Kirks DR, Merten DF, Martinez S. Cervical spine fractures and dislocations in children.�Pediatr Radiol. 1987;17:45�9.
17.�Turetsky DB, Vines FS, Clayman DA, Northup HM. Technique and use of supine oblique views in acute cervical spine trauma.�Ann Emerg Med. 1993;22:685�9.
18.�Freemyer B, Knopp R, Piche J, Wales L, Williams J. Comparison of five-view and three-view cervical spine series in the evaluation of patients with cervical trauma.�Ann Emerg Med. 1989;18:818�21.
19.�Lewis LM, Docherty M, Ruoff BE, Fortney JP, Keltner RA Jr, Britton P. Flexion-extension views in the evaluation of cervical-spine injuries.�Ann Emerg Med. 1991;20:117�21.
20.�Mace SE. Emergency evaluation of cervical spine injuries: CT versus plain radiographs.�Ann Emerg Med. 1985;14:973�5.
21.�Kirshenbaum KJ, Nadimpalli SR, Fantus R, Cavallino RP. Unsuspected upper cervical spine fractures associated with significant head trauma: role of CT.�J Emerg Med. 1990;8:183�98.
22.�Woodring JH, Lee C. The role and limitations of computed tomographic scanning in the evaluation of cervical trauma.�J Trauma. 1992;33:698�708.
23.�Schaefer DM, Flanders A, Northrup BE, Doan HT, Osterholm JL. Magnetic resonance imaging of acute cervical spine trauma. Correlation with severity of neurologic injury.�Spine. 1989;14:1090�5.
24.�Levitt MA, Flanders AE. Diagnostic capabilities of magnetic resonance imaging and computed tomography in acute cervical spinal column injury.�Am J Emerg Med. 1991;9:131�5.
25.�Templeton PA, Young JW, Mirvis SE, Buddemeyer EU. The value of retropharyngeal soft tissue measurements in trauma of the adult cervical spine. Cervical spine soft tissue measurements.�Skeletal Radiol. 1987;16:98�104.
26.�DeBehnke DJ, Havel CJ. Utility of prevertebral soft tissue measurements in identifying patients with cervical spine fractures.�Ann Emerg Med. 1994;24:1119�24.
29.�Bracken MB, Shepard MJ, Collins WF Jr, Holford TR, Baskin DS, Eisenberg HM, et al. Methylprednisolone or naloxone treatment after acute spinal cord injury: 1-year follow-up data. Results of the second National Acute Spinal Cord Injury Study.�J Neurosurg. 1992;76:23�31.
30.�Galandiuk S, Raque G, Appel S, Polk HC Jr. The two-edged sword of large-dose steroids for spinal cord trauma.�Ann Surg. 1993;218:419�25.
31.�Grabb PA, Pang D. Magnetic resonance imaging in the evaluation of spinal cord injury without radiographic abnormality in children.�Neurosurgery. 1994;35:406�14.
32.�Pang D, Pollack IF. Spinal cord injury without radiographic abnormality in children�the SCIWORA syndrome.�J Trauma. 1989;29:654�64.
33.�Hadley MN, Zabramski JM, Browner CM, Rekate H, Sonntag VK. Pediatric spinal trauma. Review of 122 cases of spinal cord and vertebral column injuries.�J Neurosurg. 1988;68:18�24.
34.�Kriss VM, Kriss TC. SCIWORA (spinal cord injury without radiographic abnormality) in infants and children.�Clin Pediatr. 1996;35:119�24.
The editors of AFP welcome the submission of manuscripts for the Radiologic Decision-Making series. Send submissions to Jay Siwek, M.D., following the guidelines provided in �Information for Authors.�
Coordinators of this series are Thomas J. Barloon, M.D., associate professor of radiology and George R. Bergus, M.D., assistant professor of family practice, both at the University of Iowa College of Medicine, Iowa City.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine