There are a number of important factors to take into consideration, such as the timing of when an MRI scan must be performed and limitations with interpretation of findings, to get an MRI scan for herniated discs.
To begin with, the difficulty with the results of an MRI scan, as with a number of other diagnostic studies, is that the abnormality may not always be the source of an individual’s back pain or other symptoms. Numerous studies have shown that approximately 30 percent of people in their twenties and forties have a lumbar disc herniation in their MRI scan, even though they don’t have any pain.
An MRI scan cannot be interpreted on its own. Everything Has to Be well-correlated into the individual patient’s condition, for example:
Symptoms (such as the duration, location, and severity of pain)
Any deficits in their examination
Another concern with MRI scans is the time of when the scan is done. When a patient has experienced the following symptoms would be the only time that an MRI scan is needed immediately:
Bowel or bladder incontinence
Progressive weakness due to nerve damage in the legs.
Herniated Disc Analysis with MRI
Obtaining an MRI (magnetic resonance imaging) can be an important step in correctly assessing a herniated disc in the spine. Unlike an X-ray, MRI uses a magnetic field and a computer to create and record detailed pictures of the internal workings of your entire body. This technology can also be capable of producing cross-sectional views in identifying a disc of the body, which greatly help doctors. MRI scans are based on new technology, but they have become essential in diagnosing a number of back and neck issues, such as spinal stenosis, herniated discs and bone spurs.
An MRI scan has a number of benefits that greatly help a herniated disc patient. The advantages of an MRI can be:
Unobtrusive
Painless and free of radiation
Can focus on a particular part of the entire body
Extremely accurate
Diagnosing Disc Herniation
Should you believe you have a herniated disc in the neck or back, the very first step would be to visit a physician. Your physician will have the ability to supply you with a complete evaluation and inspection of your medical history to create a identification. Following that, you may be referred to execute an MRI stabilize and to confirm the herniated disc.
At the imaging center you’ll be put to the tubular MRI machine to get a body scan. You may remain enclosed in the MRI device for up to an hour while the comprehensive scan of place where the herniated disc along the spine is completed. The MRI can reveal the exact condition of the herniated disc and surrounding arrangements. This allows your doctor to produce the treatment plan that is right for you and to understand the origin of the disc damage and pain.
Herniated Disc Follow-Up Treatment
Most patients are able to successfully treat herniated disc pain using nonsurgical standard treatments prescribed by their physician. These include relaxation, compression treatment and mild exercise. Surgery can then be explored when months or weeks of treatment do not bring a return to previous action.
If you’re researching surgical options and have become concerned by a number of the risks and unsuccessful results of traditional open back operation, contact a specialist. Spine surgery specialists perform minimally invasive spine surgery, including invasive stabilization surgeries and minimally invasive decompression, which can treat a number of the very acute herniated discs. They may review your MRI to determine if you are a candidate for minimally invasive spine surgery, which may help you get your life back.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sciatica
Lower back pain is one of the most commonly reported symptoms among the general population. Sciatica, is well-known group of symptoms, including lower back pain, numbness and tingling sensations, which often describe the source of an individual’s lumbar spine issues. Sciatica can be due to a variety of injuries and/or conditions, such as spinal misalignment, or subluxation, disc herniation and even spinal degeneration.
The importance of Magnetic Resonance Imaging to evaluate the integrity of the lumbar posterior ligament complex post trauma.
Abstract: Posterior ligamentous complex(PLC), consisting of the supraspinous ligament, interspinous ligament, ligamentum flavum, and the facet joint capsules is thought to contribute significantly to the stability of the lumbar spine. There has been much debate on whether Magnetic Resonance Imaging(MRI) is specific and sensitive in diagnosing pathology to the PLC. The objective is to determine the necessity of MRI imaging for evaluating the integrity of the lumbar posterior ligament complex post trauma.
Key Words: Magnetic Resonance Imaging(MRI), interspinous ligament, posterior ligament complex, low back pain, ligament laxity, electromyography, impairment rating
A 41-year-old male, presented to my office for an examination with complaints of low back pain with numbness, tingling and weakness into the left lower extremity after he was the restraint driver in a motor vehicle collision approximately three and a half months� post trauma.�He�rated the pain as a�3/10 on a visual analog scale with 10/10 being the worst and the pain and noted the pain as being�present most of the time.� He stated that he was on pain killers daily and this helped manage his daily activities. Without pain killers his pain levels are rated 8/10 being present most of the time. The pain killers stated by the patient are Oxycodone and Naproxen. He�reported that the pain would be aggravated by activities which required excessive standing, repetitive bending, and lifting. He further noted that in the morning the pain was increased and his left leg would be numb and weak for about the first hour.
The patient stated that his care to date had been managed by a pain management clinic and that he had minimal improvement with treatment which has included physical therapy and massage therapy. He reported the pain clinic next recommended steroid injections which he refused. He states there has been was no imaging ordered and that an Electromyography(EMG) had been performed. He was told the test was negative for pathology.
Prior History: No significant medical history was reported. Clinical Findings:�The patient is 6�0� and weighs 210 lbs.
Physical Exam Findings:
Cervical Spine:
Cervical spine range of motion is full and unrestricted. Maximum cervical compression is negative. Motor and other regional sensory exam are unremarkable at this time.
Thoracic Spine:
Palpation of the thoracic spine region reveals taught and tender fibers in the area of the bilateral upper and mid thoracic musculature. Thoracic spine range of motion is restricted in flexion, extension, bilateral lateral flexion, and bilateral rotation. Regional motor and sensory exam are unremarkable at this time.
Lumbar Spine:
Palpation of the lumbosacral spine region reveals taught and tender fibers in the area of the lumbar paraspinal musculature. Lumbar spine range of motion is limited in flexion, extension, bilateral lateral flexion and bilateral rotation. Extension restriction is due to pain and spasm. Straight leg raise causes pain at approximately 50 degrees when testing either side in the left low back. There is no radicular symptomatology down the leg. Kemp�s maneuver recreates pain in the L4 region on the left. No radicular symptoms are noted. The patient is able to heel and toe walk. Regional motor and sensory exam is unremarkable at this time other than L4, L5 and S1 dermatomes having decreased sensation with light touch.
Muscle testing of the upper and lower extremities was tested at a 5/5 with the exception of the left quadricep tested at a 4/5.� The patient�s deep tendon reflexes of the upper and lower extremities were tested including triceps, biceps, brachioradialis, patella, and Achilles and all were tested at 2+ bilaterally except the left patellar reflex was 1+.
RANGES OF MOTION EVALUATION
All range of motions are based on the�American Medical Association�s Guides to the Evaluation of Permanent Impairment, 5th�Edition1�and performed by a dual inclinometer for the lumbar spine.
�� Range of Motion������Normal�������� Examination�������� % Deficit
Flexion
60
48
20
Extension
25
12
52
Left Lateral Flexion
25
16
36
Right Lateral Flexion
25
18
28
An MRI was ordered to rule out gross pathology.
Imaging:
�
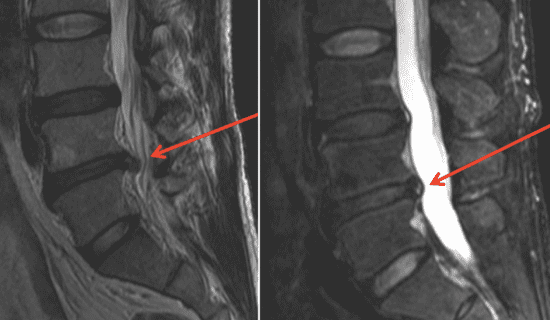
A lumbar MRI reveals;
1)��� Mild disc bulges at T11-T12, T12-L1, L1-L2 and L5-S1
2)��� Low disc signals indicative of disc desiccation at T11-T12, T12-L1, L1-L2, L2-L3, L3-L4 and L4-L5
3)��� Retrolisthesis of 2mm at L3-L4
4)��� Mild ligamentous hypertrophy at L1-L2, L2-L3, L3-L4, L4-L5 and L5-S1
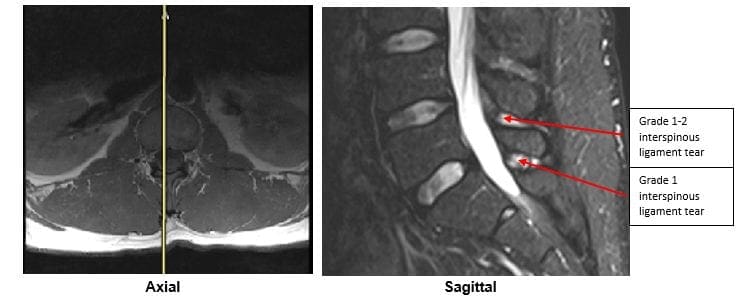
5)��� L4-L5 has a Grade 1-2 tear of the interspinous ligament with mild inflammation
6)��� L5-S1 has a Grade 1 interspinous ligament tear with mild inflammation
After reviewing the MRI I ordered lumbar x-rays to rule out ligament laxity.
X-RAY STUDIES
Lumbar x-rays reveal the following:
1)��� Left lateral tilt
2)��� Retrolisthesis at L1 of 3mm
3)��� Retrolisthesis at L2 of 3mm
4)��� Combined excessive translation of 4mm of L1 during flexion-extension
5)��� Combined excessive translation of 4mm of L2 during flexion-extension
6)��� Excessive translation of L3 in extension posteriorly of 2.5mm
7)��� Decreased disc space at L5-S1
Chiropractic care was initiated. The patient was placed on an initial care plan of 2-3x/week for 3 months and then a recommended break in care for one month so the patient could be evaluated for permanency while he was not care dependent.
At maximum medical improvement, he had continued low back pain rated 4/10, continued numbness and tingling into his left leg and left quadricep weakness rated 4/5. He does not need pain killers for pain management anymore. He continues chiropractic care every two weeks to manage his symptoms.
Conclusion:
In this specific case, pathology to the posterior ligament complex diagnosed on MRI lead to the x-ray finding of excessive translation at L1-L2 and L2-L3. The patient was given a permanent impairment rating of 22% based on my interpretation of the American Medical Association�s Guides to the Evaluation of Permanent Impairment, 5th�Edition1. The interspinous ligament tears at the L4-L5 and L5-S1 level would not have been diagnosed without the MRI.
There has been much debate on whether MRI imaging has a role in evaluating lumbar PLC. MRI is a powerful diagnostic tool that can provide important clinical information regarding the condition of the PLC. Useful sequences for spinal MRI in trauma include sagittal and axial T1-weighted images, T2-weighted FSE, fat-saturated T2-weighted FSE, and STIR sequences to highlight bone edema.2�Ligamentous injuries are best identified on T2-weighted images with fat saturation because the ligaments are thin and bonded on either side by fat, which can appear as hyperintense on both T1 and T2 images.3�T1-weighted images are inadequate in isolation for identifying ligamentous injuries.4�
The diagnostic accuracy for MRI was reported for both supraspinous ligament and interspinous ligament injury with a sensitivity of 89.4% and 98.5%, respectively, and a specificity of 92.3% and 87.2% in 35 patients.5
For patients with persistent symptoms after trauma an MRI may be indicated to evaluate posterior ligamentous complex integrity.
Competing Interests:� There are no competing interests in the writing of this case report.
De-Identification: All of the patient�s data has been removed from this case.
References:
1. Cocchiarella L., Anderson G. Guides to the Evaluation of Permanent Impairment, 5th Edition, Chicago IL, 2001 AMA Press.
2. Cohen, W.A., Giauque, A.P., Hallam, D.K., Linnau, K.F. and Mann, F.A., 2003. Evidence-based approach to use of MR imaging in acute spinal trauma.�European journal of radiology,�48(1), pp.49-60.
3. Terk, M.R., Hume-Neal, M., Fraipont, M., Ahmadi, J. and Colletti, P.M., 1997. Injury of the posterior ligament complex in patients with acute spinal trauma: evaluation by MR imaging.�AJR. American journal of roentgenology,�168(6), pp.1481-1486.
4. Saifuddin, A., Green, R. and White, J., 2003. Magnetic resonance imaging of the cervical ligaments in the absence of trauma.�Spine,�28(15), pp.1686-1691.
5. Haba H, Taneichi H, Kotani Y, et al. Diagnostic accuracy of magnetic resonance imaging for detecting posterior ligamentous complex injury associated with thoracic and lumbar fractures.�J Neurosurg. 2003; 99(1 Suppl):20-26.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine