Can incorporating electrical muscle stimulation help control pain, strengthen muscles, increase physical function, retrain lost movements, and/or manage inflammation for individuals experiencing neck and back pain?
Female doctor placing myostimulation physical therapy equipment on patient’s back
Electric Muscle Stimulation
Electrical muscle stimulation or E-stim is a physical therapy used to reactivate the muscles’ ability to contract. E-stim uses devices that transmit electrical impulses through the skin to target nerves and/or muscles. The most common forms include
Transcutaneous electric nerve stimulation, or TENS, is the most well-known type of electrical stimulation that offers devices that can be used at home or on the go.
Electrical muscle stimulation or EMS.
In physical therapy, E-stim stimulates muscles to contract, strengthening them and encouraging blood circulation.
Blood circulation can directly affect the condition of muscle tissue.
Electrical muscle stimulation is also used in spinal cord injury and other neuromuscular conditions. (Ho, C. H. et al., 2014)
E-stim
During treatment, electrodes are hooked to an electric stimulation machine and placed around the affected neck or back area.
The electrodes will be placed on the skin for most neck or back injuries.
The placement of the electrodes depends on the reason for treatment and the depth or superficiality of the electrical stimulation.
The electrodes are often placed near a motor point of a muscle to ensure the correct contraction.
The therapist will adjust the controls of the stimulation machine to achieve thorough muscle contraction with minimal discomfort.
Stimulation can last 5 – 15 minutes, depending on the treatment plan and injury severity.
Spinal Joint Stabilization
Activation of the muscles may help increase spinal joint stability, improving problems with spinal instability. (Ho, C. H. et al., 2014) Electric muscle stimulation is thought to enhance the exercise program a therapist prescribes to help maintain joint stability. Electrical stimulation may also help build muscle strength and endurance. (Veldman, M. P. et al., 2016) Muscle endurance is the repetitions a muscle can contract before it fatigues.
Healing and Pain Management
Electric muscle stimulation therapy can enhance tissue healing and help manage inflammation by reducing swelling and increasing circulation. It can reduce pain sensations by blocking nerve transmission at the spinal cord. (Johnson, M. I. et al., 2019) A healthcare professional may suggest a TENS or take-home electric stimulation unit to manage symptoms. (Johnson, M. I. et al., 2019)
Treatment
Interdisciplinary therapies tailored to an individual’s specific back or neck pain have been found to provide positive results. Exercise, yoga, short-term cognitive behavioral therapy, biofeedback, progressive relaxation, massage, manual therapy, and acupuncture are recommended for neck or back pain. (Chou, R. et al., 2018) Taking non-steroidal anti-inflammatory medications may also help. Electrical muscle stimulation could be an effective neck or back treatment.
Individuals unsure whether they need or would benefit from electrical should discuss symptoms and conditions with a primary physician, healthcare provider, or specialist to guide them in the right direction and determine the best treatment. Injury Medical Chiropractic and Functional Medicine Clinic focuses on what works for the patient and strives to better the body through researched methods and total wellness programs. Using an integrated approach, we treat injuries and chronic pain syndromes through personalized care plans that improve ability through flexibility, mobility, and agility programs personalized to the individual to relieve pain. If other treatment is needed, Dr. Jimenez has teamed up with the top surgeons, clinical specialists, medical researchers, and premier rehabilitation providers to provide the most effective treatments.
Thoracic Spine Pain
References
Ho, C. H., Triolo, R. J., Elias, A. L., Kilgore, K. L., DiMarco, A. F., Bogie, K., Vette, A. H., Audu, M. L., Kobetic, R., Chang, S. R., Chan, K. M., Dukelow, S., Bourbeau, D. J., Brose, S. W., Gustafson, K. J., Kiss, Z. H., & Mushahwar, V. K. (2014). Functional electrical stimulation and spinal cord injury. Physical medicine and rehabilitation clinics of North America, 25(3), 631–ix. https://doi.org/10.1016/j.pmr.2014.05.001
Veldman, M. P., Gondin, J., Place, N., & Maffiuletti, N. A. (2016). Effects of Neuromuscular Electrical Stimulation Training on Endurance Performance. Frontiers in physiology, 7, 544. https://doi.org/10.3389/fphys.2016.00544
Johnson, M. I., Jones, G., Paley, C. A., & Wittkopf, P. G. (2019). The clinical efficacy of transcutaneous electrical nerve stimulation (TENS) for acute and chronic pain: a protocol for a meta-analysis of randomised controlled trials (RCTs). BMJ open, 9(10), e029999. https://doi.org/10.1136/bmjopen-2019-029999
Chou, R., Côté, P., Randhawa, K., Torres, P., Yu, H., Nordin, M., Hurwitz, E. L., Haldeman, S., & Cedraschi, C. (2018). The Global Spine Care Initiative: applying evidence-based guidelines on the non-invasive management of back and neck pain to low- and middle-income communities. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 27(Suppl 6), 851–860. https://doi.org/10.1007/s00586-017-5433-8
Can knowing treatment options for a dislocated hip help individuals expedite rehabilitation and recovery?
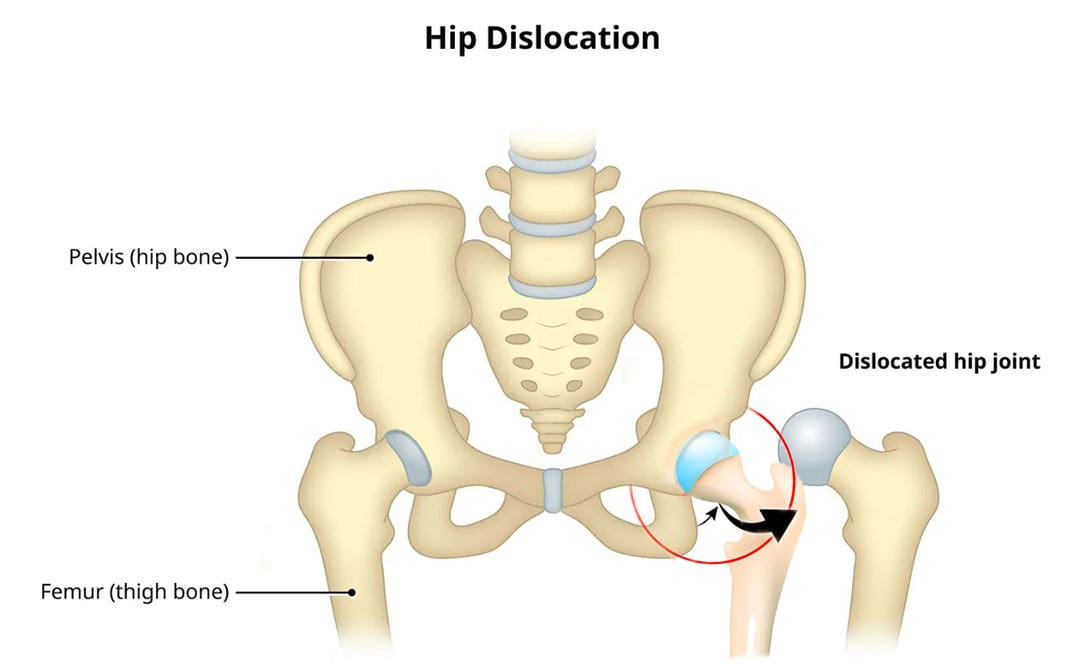
Dislocated Hip
A dislocated hip is an uncommon injury but can happen due to trauma or following hip replacement surgery. It usually occurs after severe trauma, including motor vehicle collisions, falls, and sometimes sports injuries. (Caylyne Arnold et al., 2017) A dislocated hip can also occur after hip replacement surgery. Other injuries like ligament tears, cartilage damage, and bone fractures can occur alongside the dislocation. Most hip dislocations are treated with a joint reduction procedure that resets the ball into the socket. It is usually done with sedation or general anesthesia. Rehabilitation takes time and could be a few months before full recovery. Physical therapy can help restore motion and strength in the hip.
What Is It?
If the hip is only partially dislocated, it’s called a hip subluxation. When this happens, the hip joint head only partially emerges from the socket. A dislocated hip is when the head or ball of the joint shifts or pops out of the socket. Because an artificial hip differs from a normal hip joint, the risk of dislocation increases after joint replacement. A study found that around 2% of individuals who undergo total hip replacement will experience hip dislocation within a year, with the cumulative risk increasing by approximately 1% over five years. (Jens Dargel et al., 2014) However, new technological prosthetics and surgical techniques are making this less common.
Hip Anatomy
The hip ball-and-socket joint is called the femoroacetabular joint.
The socket is called the acetabulum.
The ball is called the femoral head.
The bony anatomy and strong ligaments, muscles, and tendons help to create a stable joint. Significant force must be applied to the joint for a hip dislocation to occur. Some individuals report feeling a snapping sensation of the hip. This usually is not a hip dislocation but indicates a different disorder known as snapping hip syndrome. (Paul Walker et al., 2021)
Posterior Hip Dislocation
Around 90% of hip dislocations are posterior.
In this type, the ball is pushed backward from the socket.
A hip dislocation increases the risk of developing joint arthritis following the injury and can raise the risk of needing a hip replacement later in life. (Hsuan-Hsiao Ma et al., 2020)
Developmental Dislocation of the Hip
Some children are born with developmental dislocation of the hip or DDH.
Children with DDH have hip joints that did not form correctly during development.
This causes a loose fit in the socket.
In some cases, the hip joint is completely dislocated.
Joint reduction is the most common way to treat a dislocated hip. The procedure repositions the ball back into the socket and is usually done with sedation or under general anesthesia. Repositioning a hip requires significant force. A hip dislocation is considered an emergency, and reduction should be performed immediately after the dislocation to prevent permanent complications and invasive treatment. (Caylyne Arnold et al., 2017)
Once the ball is back in the socket, the healthcare provider will look for bone, cartilage, and ligament injuries.
Depending on what the healthcare provider finds, further treatment may be necessary.
Fractured or broken bones may need to be repaired to keep the ball within the socket.
Damaged cartilage may have to be removed.
Surgery
Surgery could be necessary to return the joint to its normal position. Hip arthroscopy can minimize the invasiveness of certain procedures. A surgeon inserts a microscopic camera into the hip joint to help the surgeon repair the injury using instruments inserted through other small incisions.
Hip replacement surgery replaces the ball and socket, a common and successful orthopedic surgical procedure. This surgery may be performed for various reasons, including trauma or arthritis, as it is common to develop early arthritis of the hip after this type of trauma. This is why many who have a dislocation ultimately need hip replacement surgery. As a major surgical procedure, it is not without risks. Possible complications include:
Infection
Aseptic loosening (the loosening of the joint without infection)
Hip dislocation
Recovery
Recovering from a hip dislocation is a long process. Individuals will need to walk with crutches or other devices early in recovery. Physical therapy will improve the range of motion and strengthen the muscles around the hip. Recovery time will depend on whether other injuries, such as fractures or tears, are present. If the hip joint was reduced and there were no other injuries, it may take six to ten weeks to recover to the point where weight can be placed on the leg. It could be between two and three months for a full recovery. Keeping weight off the leg is important until the surgeon or physical therapist gives the all-clear. Injury Medical Chiropractic and Functional Medicine Clinic will work with an individual’s primary healthcare provider and other surgeons or specialists to develop an optimal personalized treatment plan.
Chiropractic Solutions for Osteoarthritis
References
Arnold, C., Fayos, Z., Bruner, D., Arnold, D., Gupta, N., & Nusbaum, J. (2017). Managing dislocations of the hip, knee, and ankle in the emergency department [digest]. Emergency medicine practice, 19(12 Suppl Points & Pearls), 1–2.
Dargel, J., Oppermann, J., Brüggemann, G. P., & Eysel, P. (2014). Dislocation following total hip replacement. Deutsches Arzteblatt international, 111(51-52), 884–890. https://doi.org/10.3238/arztebl.2014.0884
Walker, P., Ellis, E., Scofield, J., Kongchum, T., Sherman, W. F., & Kaye, A. D. (2021). Snapping Hip Syndrome: A Comprehensive Update. Orthopedic reviews, 13(2), 25088. https://doi.org/10.52965/001c.25088
Cornwall, R., & Radomisli, T. E. (2000). Nerve injury in traumatic dislocation of the hip. Clinical orthopaedics and related research, (377), 84–91. https://doi.org/10.1097/00003086-200008000-00012
American Academy of Orthopaedic Surgeons. (2021). Hip dislocation. https://orthoinfo.aaos.org/en/diseases–conditions/hip-dislocation
Kellam, P., & Ostrum, R. F. (2016). Systematic Review and Meta-Analysis of Avascular Necrosis and Posttraumatic Arthritis After Traumatic Hip Dislocation. Journal of orthopaedic trauma, 30(1), 10–16. https://doi.org/10.1097/BOT.0000000000000419
Ma, H. H., Huang, C. C., Pai, F. Y., Chang, M. C., Chen, W. M., & Huang, T. F. (2020). Long-term results in the patients with traumatic hip fracture-dislocation: Important prognostic factors. Journal of the Chinese Medical Association : JCMA, 83(7), 686–689. https://doi.org/10.1097/JCMA.0000000000000366
American Academy of Orthopaedic Surgeons. (2022). Developmental dislocation (dysplasia) of the hip (DDH). https://orthoinfo.aaos.org/en/diseases–conditions/developmental-dislocation-dysplasia-of-the-hip-ddh/
Can individuals with joint hypermobility find relief through nonsurgical treatments in reducing pain and restoring body mobility?
Introduction
When a person moves their body, the surrounding muscles, joints, and ligaments are incorporated into various tasks that allow them to stretch and be flexible without pain or discomfort. Many repetitive motions enable the individual to continue their routine. However, when the joints, muscles, and ligaments are stretched farther than normal in the upper and lower extremities without pain, it is known as joint hypermobility. This connective tissue disorder can correlate with other symptoms that affect the body and cause many people to seek treatment to manage joint hypermobility symptoms. In today’s article, we will look at joint hypermobility and how various non-surgical treatments can help reduce pain caused by joint hypermobility and restore body mobility. We talk with certified medical providers who consolidate our patients’ information to assess how their pain may be associated with joint hypermobility. We also inform and guide patients on how integrating various non-surgical treatments can help improve joint function while managing the associated symptoms. We encourage our patients to ask their associated medical providers intricate and insightful questions about incorporating non-surgical therapies as part of their routine to reduce pain and discomfort from joint hypermobility. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
What Is Joint Hypermobility?
Do you often feel your joints locked up in your hands, wrists, knees, and elbows? Do you experience pain and fatigue in your joints when your body feels constantly tired? Or when you stretch your extremities, do they extend farther than usual to feel the relief? Many of these various scenarios are often correlated with individuals experiencing joint hypermobility. Joint hypermobility is an inherited disorder with autosomal dominant patterns that characterize joint hyperlaxity and musculoskeletal pain within the body extremities. (Carbonell-Bobadilla et al., 2020) This connective tissue condition is often related to the flexibility of the connected tissues like ligaments and tendons in the body. An example would be if a person’s thumb is touching their inner forearm without feeling pain or discomfort, they have joint hypermobility. Additionally, many individuals dealing with joint hypermobility will often have a difficult diagnosis as they will develop skin and tissue fragility over time, causing musculoskeletal complications. (Tofts et al., 2023)
When individuals deal with joint hypermobility over time, many often have symptomatic joint hypermobility. They will present with musculoskeletal and systemic symptoms that lead to displaying skeletal deformities, tissue and skin fragility, and structural differences in the body’s system. (Nicholson et al., 2022) Some of the symptoms that joint hypermobility are shown in a diagnosis include:
Muscle pain and joint stiffness
Clicking joints
Fatigue
Digestive issues
Balance issues
Luckily, there are various treatments that many people can use to help restrengthen the surrounding muscles around the joints and reduce the correlating symptoms caused by joint hypermobility.
Movement As Medicine-Video
Nonsurgical Treatments For Joint Hypermobility
When dealing with joint hypermobility, many individuals need to seek treatments to reduce the correlating pain-like symptoms of joint hypermobility and help relieve the body’s extremities while restoring mobility. Some excellent treatments for joint hypermobility are non-surgical therapies that are non-invasive, gentle on the joints and muscles, and cost-effective. Various non-surgical treatments can be customized for the individual depending on how severe their joint hypermobility and comorbidities affect the person’s body. Non-surgical treatments can relieve the body from joint hypermobility by treating the causes of the pain through reduction and maximizing functional capacity and restoring a person’s quality of life. (Atwell et al., 2021) The three non-surgical treatments that are excellent for reducing pain from joint hypermobility and helping strengthen the surrounding muscles are below.
Chiropractic Care
Chiropractic care utilizes spinal manipulation and helps restore joint mobility in the body to reduce the effects of joint hypermobility by stabilizing the affected joints from the hypermobile extremities. (Boudreau et al., 2020) Chiropractors incorporate mechanical and manual manipulation and various techniques to help many individuals improve their posture by being more mindful of their bodies and work with multiple other therapies to emphasize controlled movements. With other comorbidities associated with joint hypermobility, like back and neck pain, chiropractic care can reduce these comorbidity symptoms and allow the individual to regain their quality of life.
Acupuncture
Another non-surgical treatment that many individuals can incorporate to reduce joint hypermobility and its comorbidities is acupuncture. Acupuncture utilizes small, thin, solid needles that acupuncturists use to block pain receptors and restore the body’s energy flow. When many individuals are dealing with joint hypermobility, their extremities in the legs, hands, and feet are in pain over time, which can cause the body to be unstable. What acupuncture does is help reduce the pain caused by joint hypermobility associated with the extremities and restore balance and functionality to the body (Luan et al., 2023). This means that if a person is dealing with stiffness and muscle pain from joint hypermobility, acupuncture can help rewire the pain by placing the needles in the body’s acupoints to provide relief.
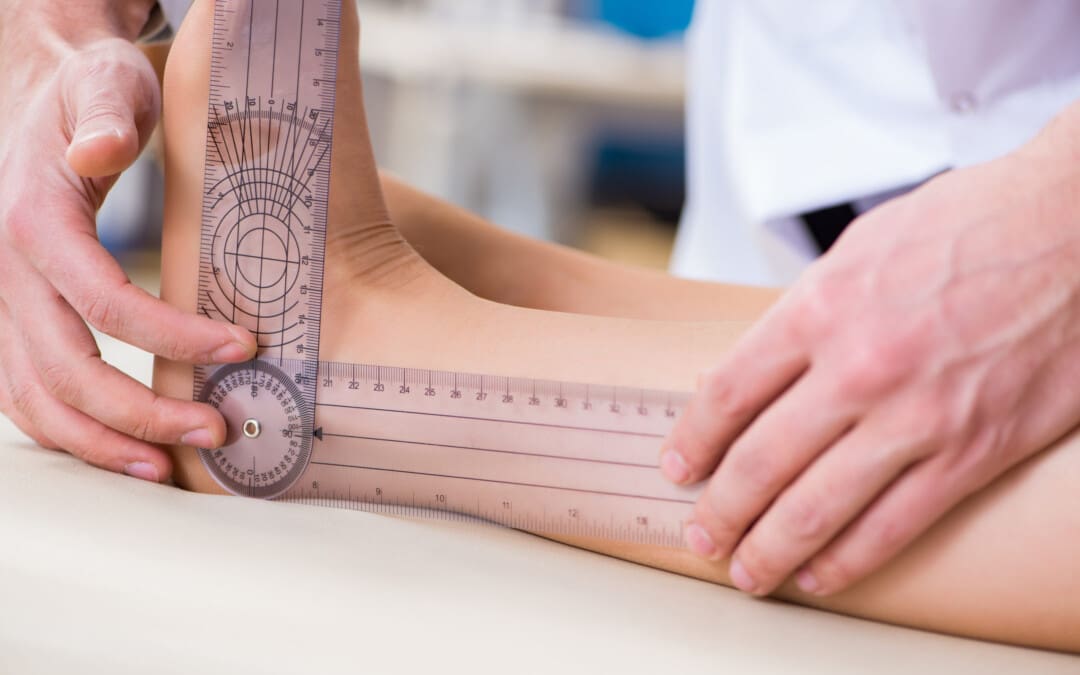
Physical Therapy
Physical therapy is the last non-surgical treatment many people can incorporate into their daily routine. Physical therapy can help manage joint hypermobility that are tailored to help strengthen weak muscles that are surrounding the affected joints, improving a person’s stability and helping reduce the risk of dislocation. Additionally, many individuals can use low-impact exercise to ensure optimal motor control when doing regular exercises without putting excessive strain on the joints. (Russek et al., 2022)
By incorporating these three non-surgical treatments as part of a customized treatment for joint hypermobility, many individuals will begin to feel a difference in their balance. They will not experience joint pain by being more mindful of the body and incorporating small changes in their routine. Even though living with joint hypermobility can be a challenge for many individuals, by integrating and utilizing the right combination of non-surgical treatments, many can begin to lead active and fulfilling lives.
References
Atwell, K., Michael, W., Dubey, J., James, S., Martonffy, A., Anderson, S., Rudin, N., & Schrager, S. (2021). Diagnosis and Management of Hypermobility Spectrum Disorders in Primary Care. J Am Board Fam Med, 34(4), 838-848. https://doi.org/10.3122/jabfm.2021.04.200374
Boudreau, P. A., Steiman, I., & Mior, S. (2020). Clinical management of benign joint hypermobility syndrome: a case series. J Can Chiropr Assoc, 64(1), 43-54. https://www.ncbi.nlm.nih.gov/pubmed/32476667
Carbonell-Bobadilla, N., Rodriguez-Alvarez, A. A., Rojas-Garcia, G., Barragan-Garfias, J. A., Orrantia-Vertiz, M., & Rodriguez-Romo, R. (2020). [Joint hypermobility syndrome]. Acta Ortop Mex, 34(6), 441-449. https://www.ncbi.nlm.nih.gov/pubmed/34020527 (Sindrome de hipermovilidad articular.)
Luan, L., Zhu, M., Adams, R., Witchalls, J., Pranata, A., & Han, J. (2023). Effects of acupuncture or similar needling therapy on pain, proprioception, balance, and self-reported function in individuals with chronic ankle instability: A systematic review and meta-analysis. Complement Ther Med, 77, 102983. https://doi.org/10.1016/j.ctim.2023.102983
Nicholson, L. L., Simmonds, J., Pacey, V., De Wandele, I., Rombaut, L., Williams, C. M., & Chan, C. (2022). International Perspectives on Joint Hypermobility: A Synthesis of Current Science to Guide Clinical and Research Directions. J Clin Rheumatol, 28(6), 314-320. https://doi.org/10.1097/RHU.0000000000001864
Russek, L. N., Block, N. P., Byrne, E., Chalela, S., Chan, C., Comerford, M., Frost, N., Hennessey, S., McCarthy, A., Nicholson, L. L., Parry, J., Simmonds, J., Stott, P. J., Thomas, L., Treleaven, J., Wagner, W., & Hakim, A. (2022). Presentation and physical therapy management of upper cervical instability in patients with symptomatic generalized joint hypermobility: International expert consensus recommendations. Front Med (Lausanne), 9, 1072764. https://doi.org/10.3389/fmed.2022.1072764
Tofts, L. J., Simmonds, J., Schwartz, S. B., Richheimer, R. M., O’Connor, C., Elias, E., Engelbert, R., Cleary, K., Tinkle, B. T., Kline, A. D., Hakim, A. J., van Rossum, M. A. J., & Pacey, V. (2023). Pediatric joint hypermobility: a diagnostic framework and narrative review. Orphanet J Rare Dis, 18(1), 104. https://doi.org/10.1186/s13023-023-02717-2
For individuals dealing with knee pain symptoms from injury and/or arthritis, can incorporating an acupuncture and/or electroacupuncture treatment plan help in pain relief and management?
Acupuncture For Knee Pain
Acupuncture involves inserting very thin needles into the skin at specific acupoints on the body. It is based on the premise that the needles restore the flow of the body’s energy to activate and promote healing, relieve pain, and help the body relax.
Acupuncture can help address various health conditions, including knee pain caused by arthritis or injury.
Depending on the type and severity of pain, treatments can help reduce the pain for days or weeks.
Acupuncture is often used as a complementary therapy – treatment in addition to other treatment or therapy strategies like massage and chiropractic.
Acupuncture Benefits
Knee pain caused by osteoarthritis or injury can reduce flexibility, mobility, and quality of life. Acupuncture can help provide relief.
When the acupuncture needles are placed on the body, a signal is sent along the spinal cord to the brain, which triggers a release of endorphins/pain hormones. Medical researchers believe this helps reduce pain. (Qian-Qian Li et al., 2013) Acupuncture also helps decrease the production of cortisol, a hormone that helps control inflammation. (Qian-Qian Li et al., 2013) With reduced pain sensations and less inflammation after acupuncture treatments, knee function and mobility can be improved.
Various factors play a role in the pain relief experienced from acupuncture. Some evidence suggests that an individual’s expectations may impact the results of acupuncture treatment. (Stephanie L. Prady et al., 2015)
Researchers are currently assessing whether the expectation that acupuncture is beneficial contributes to a better outcome after treatment. (Zuoqin Yang et al., 2021)
In 2019, acupuncture was recommended in treating knee osteoarthritis in the American College of Rheumatology/Arthritis Foundation guidelines for hand, hip, and knee osteoarthritis pain management. (Sharon L. Kolasinski et al., 2020)
Research
Different clinical studies support acupuncture’s ability to help in knee pain relief and management.
One study found that acupuncture helps manage various conditions that cause chronic pain. (Andrew J. Vickers et al., 2012)
A scientific review analyzed previous studies on pain management interventions after knee surgery and found supporting evidence that the treatments delayed and reduced the use of medications for pain relief post-surgery. (Dario Tedesco et al., 2017)
Osteoarthritis
A systematic review analyzed randomized control studies to determine whether or not acupuncture reduced pain and improved joint function in individuals with chronic osteoarthritis knee pain. (Xianfeng Lin et al., 2016)
Individuals received six to twenty-three weekly acupuncture sessions for three to 36 weeks.
The analysis determined that acupuncture can improve short and long-term physical function and mobility and provide up to 13 weeks of pain relief in individuals with chronic knee pain caused by osteoarthritis.
Rheumatoid Arthritis
Rheumatoid arthritis is a chronic disease that affects joints, including the knee joint, causing pain and stiffness.
Acupuncture is beneficial in treating rheumatoid arthritis/RA.
A review found that acupuncture alone and in combination with other treatment modalities benefits individuals with RA. (Pei-Chi, Chou Heng-Yi Chu 2018)
Acupuncture is believed to have anti-inflammatory and antioxidant effects to help regulate immune system function.
Chronic Knee Pain
Various conditions and injuries can cause chronic knee pain, making mobility difficult.
Individuals with joint pain often turn to complementary therapies for pain relief management, with acupuncture being one of the popular modalities. (Michael Frass et al., 2012)
Working with a licensed, professional acupuncture practitioner can reduce the risk of unwanted side effects and complications.
Types
Other acupuncture options that may be offered include:
Electroacupuncture
A modified form of acupuncture where a mild electrical current passes through the needles, providing additional stimulation to the acupoints.
In one research study, individuals with knee osteoarthritis reported significant improvements in their pain, stiffness, and physical function after electroacupuncture treatment. (Ziyong Ju et al., 2015)
Auricular
Auricular or ear acupuncture works on acupoints in the ear corresponding to the body’s different parts.
A research review analyzed several studies on auricular acupuncture for pain relief and found that it can provide relief within 48 hours of pain onset. (M. Murakami et al., 2017)
Battlefield Acupuncture
The military and veteran healthcare facilities use a unique form of auricular acupuncture for pain management.
Studies show that it is effective at providing immediate pain relief, but more research is necessary to determine long-term pain relief effectiveness. (Anna Denee Montgomery, Ronovan Ottenbacher 2020)
Before trying acupuncture, consult a healthcare professional for guidance, as it may be integrated with other therapies and lifestyle adjustments.
Overcoming an ACL Injury
References
Li, Q. Q., Shi, G. X., Xu, Q., Wang, J., Liu, C. Z., & Wang, L. P. (2013). Acupuncture effect and central autonomic regulation. Evidence-based complementary and alternative medicine : eCAM, 2013, 267959. https://doi.org/10.1155/2013/267959
Prady, S. L., Burch, J., Vanderbloemen, L., Crouch, S., & MacPherson, H. (2015). Measuring expectations of benefit from treatment in acupuncture trials: a systematic review. Complementary therapies in medicine, 23(2), 185–199. https://doi.org/10.1016/j.ctim.2015.01.007
Yang, Z., Li, Y., Zou, Z., Zhao, Y., Zhang, W., Jiang, H., Hou, Y., Li, Y., & Zheng, Q. (2021). Does patient’s expectation benefit acupuncture treatment?: A protocol for systematic review and meta-analysis. Medicine, 100(1), e24178. https://doi.org/10.1097/MD.0000000000024178
Kolasinski, S. L., Neogi, T., Hochberg, M. C., Oatis, C., Guyatt, G., Block, J., Callahan, L., Copenhaver, C., Dodge, C., Felson, D., Gellar, K., Harvey, W. F., Hawker, G., Herzig, E., Kwoh, C. K., Nelson, A. E., Samuels, J., Scanzello, C., White, D., Wise, B., … Reston, J. (2020). 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis care & research, 72(2), 149–162. https://doi.org/10.1002/acr.24131
Vickers, A. J., Cronin, A. M., Maschino, A. C., Lewith, G., MacPherson, H., Foster, N. E., Sherman, K. J., Witt, C. M., Linde, K., & Acupuncture Trialists’ Collaboration (2012). Acupuncture for chronic pain: individual patient data meta-analysis. Archives of internal medicine, 172(19), 1444–1453. https://doi.org/10.1001/archinternmed.2012.3654
Tedesco, D., Gori, D., Desai, K. R., Asch, S., Carroll, I. R., Curtin, C., McDonald, K. M., Fantini, M. P., & Hernandez-Boussard, T. (2017). Drug-Free Interventions to Reduce Pain or Opioid Consumption After Total Knee Arthroplasty: A Systematic Review and Meta-analysis. JAMA surgery, 152(10), e172872. https://doi.org/10.1001/jamasurg.2017.2872
Lin, X., Huang, K., Zhu, G., Huang, Z., Qin, A., & Fan, S. (2016). The Effects of Acupuncture on Chronic Knee Pain Due to Osteoarthritis: A Meta-Analysis. The Journal of bone and joint surgery. American volume, 98(18), 1578–1585. https://doi.org/10.2106/JBJS.15.00620
Chou, P. C., & Chu, H. Y. (2018). Clinical Efficacy of Acupuncture on Rheumatoid Arthritis and Associated Mechanisms: A Systemic Review. Evidence-based complementary and alternative medicine : eCAM, 2018, 8596918. https://doi.org/10.1155/2018/8596918
Frass, M., Strassl, R. P., Friehs, H., Müllner, M., Kundi, M., & Kaye, A. D. (2012). Use and acceptance of complementary and alternative medicine among the general population and medical personnel: a systematic review. Ochsner journal, 12(1), 45–56.
Hinman, R. S., McCrory, P., Pirotta, M., Relf, I., Forbes, A., Crossley, K. M., Williamson, E., Kyriakides, M., Novy, K., Metcalf, B. R., Harris, A., Reddy, P., Conaghan, P. G., & Bennell, K. L. (2014). Acupuncture for chronic knee pain: a randomized clinical trial. JAMA, 312(13), 1313–1322. https://doi.org/10.1001/jama.2014.12660
National Center for Complementary and Integrative Health. (2022). Acupuncture in depth. National Center for Complementary and Integrative Health. https://www.nccih.nih.gov/health/acupuncture-what-you-need-to-know
Harvard Medical School. (2023). Acupuncture: what is it? Harvard Health Publishing Harvard Medical School Blog. https://www.health.harvard.edu/a_to_z/acupuncture-a-to-z#:~:text=The%20most%20common%20side%20effects,injury%20to%20an%20internal%20organ.
Ju, Z., Guo, X., Jiang, X., Wang, X., Liu, S., He, J., Cui, H., & Wang, K. (2015). Electroacupuncture with different current intensities to treat knee osteoarthritis: a single-blinded controlled study. International journal of clinical and experimental medicine, 8(10), 18981–18989.
Murakami, M., Fox, L., & Dijkers, M. P. (2017). Ear Acupuncture for Immediate Pain Relief-A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pain medicine (Malden, Mass.), 18(3), 551–564. https://doi.org/10.1093/pm/pnw215
Montgomery, A. D., & Ottenbacher, R. (2020). Battlefield Acupuncture for Chronic Pain Management in Patients on Long-Term Opioid Therapy. Medical acupuncture, 32(1), 38–44. https://doi.org/10.1089/acu.2019.1382
Can individuals dealing with joint pain incorporate acupuncture therapy to manage lupus symptoms and restore body mobility?
Introduction
The immune system is highly important to the body as its main job is to protect vital structures from foreign invaders that can cause pain-like issues and discomfort. The immune system has a healthy relationship with the different body systems, including the musculoskeletal system, as the inflammatory cytokines help heal muscle and tissue damage when the body is injured. Over time, however, when normal environmental and genetic factors start to develop in the body, the immune system will begin to send out these cytokines to healthy, normal cells. To that point, the body starts at risk of developing autoimmune diseases. Now, autoimmune diseases in the body can cause havoc over time when they are not managed, leading to chronic disorders that can cause overlapping symptoms in the musculoskeletal system. One of the most common autoimmune diseases is systemic lupus erythematosus or lupus, and it can cause a person to be in consistent pain and discomfort while correlating with muscle and joint pain. Today’s article looks at the factors and effects of lupus, the burden of joint pain in lupus, and how holistic approaches like acupuncture can help manage lupus while restoring body mobility. We talk with certified medical providers who consolidate our patients’ information to assess how to minimize the pain effects caused by lupus on the joints. We also inform and guide patients on how acupuncture can help manage lupus and combine other therapies to reduce its pain-like symptoms affecting the musculoskeletal system. We encourage our patients to ask their associated medical providers intricate and important questions about incorporating acupuncture therapy to relieve the inflammatory effects of lupus while finding natural ways to restore mobility. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
The Factors & Effects Of Lupus
Have you been experiencing joint pain in your upper or lower extremities, making it difficult to function throughout the day? Have you been feeling the constant effects of fatigue? Many individuals experiencing these pain-like issues could risk developing systemic lupus erythematosus. In this autoimmune disease, the body’s own immune system mistakenly starts to attack its tissues, thus leading to inflammation and a range of pain-like symptoms. Lupis is tricky to diagnose because of its complex immune dysregulation that can lead to an overproduction of cytokines that can affect the body. (Lazar & Kahlenberg, 2023) At the same time, lupus can affect a diverse population, with symptoms and severity varying depending on how mild or severe the factors affect the body. Lupus can impact various body parts, including the joints, skin, kidneys, blood cells, and other vital body parts and organs, as environmental and hormonal factors can influence its development. (Tsang & Bultink, 2021) Additionally, lupus can be closely associated with other comorbidities that are causing overlapping risk profiles with inflammation that can affect the joints in the musculoskeletal system.
The Burden of Joint Pain In Lupus
Lupus is tricky to diagnose since it often mimics other ailments; the most common pain symptom that lupus affects is the joints. Individuals with lupus experience joint pain, which can cause inflammatory effects and structural damage to the joints, tendons, muscles, and bones, causing pathological abnormalities. (Di Matteo et al., 2021) Since lupus causes inflammatory effects in the joints, many individuals will think that they are experiencing inflammatory arthritis, and it can cause overlapping risk profiles as it is accompanied by lupus, thus causing localized pain in the joints regardless of its origin. (Senthelal et al., 2024) Joint pain in lupus individuals can significantly hinder daily activities, reducing mobility and overall quality of life as they are trying to find relief.
Unlocking The Secrets of Inflammation-Video
A Holistic Approach to Managing Lupus
While standard treatments for lupus involve medication and immunosuppressants to reduce the inflammation caused by lupus, many people want to seek out holistic approaches to manage lupus and reduce the inflammatory effects from affecting their joints by making small changes in their lives. Many people incorporate anti-inflammatory foods rich in antioxidants to dampen the inflammatory effects. Various supplements, like vitamin D, calcium, zinc, etc., can help reduce inflammation caused by lupus and strengthen bone health. Additionally, non-surgical treatments can even improve cardiorespiratory capacity and decrease fatigue while improving psychological function, which can help improve a person’s quality of life by managing the symptoms caused by lupus. (Fangtham et al., 2019)
How Acupuncture Could Help Lupus & Restore Mobility
One of the oldest forms of non-surgical and holistic approaches to reducing inflammation and managing lupus is acupuncture. Acupuncture involves solid, thin needles used by highly trained professionals to be inserted into specific body points to balance the body’s qi (energy) by stimulating the nervous system and releasing beneficial chemicals into the affected muscles, spinal cord, and brain. Additionally, acupuncture, with its minimal side effects and holistic approach, can help manage lupus. This is because when acupuncture needles are placed at the acupoints of the body, it can disrupt the pain signals that are causing pain in the affected area and regulate the inflammatory cytokines from lupus to provide relief. (Wang et al., 2023) This is due to its philosophy of addressing not only the physical pain but also the emotional and psychological symptoms of living with a chronic condition like lupus.
Additionally, acupuncture can help restore joint mobility while managing lupus through consecutive treatments, as many people notice that their joint mobility is improved and their pain is diminished. This is because the insertion and manipulation of the needles in the body’s acupoints cause alterations in afferent sensory input to the central nervous system, which increases alpha motoneuron excitability and reduces inflammation. (Kim et al., 2020) When individuals are dealing with lupus and are trying to find alternative holistic methods to relieve inflammation and joint pain caused by lupus, acupuncture, and non-surgical treatments can offer a ray of hope in managing the daily challenges of lupus.
References
Di Matteo, A., Smerilli, G., Cipolletta, E., Salaffi, F., De Angelis, R., Di Carlo, M., Filippucci, E., & Grassi, W. (2021). Imaging of Joint and Soft Tissue Involvement in Systemic Lupus Erythematosus. Curr Rheumatol Rep, 23(9), 73. https://doi.org/10.1007/s11926-021-01040-8
Fangtham, M., Kasturi, S., Bannuru, R. R., Nash, J. L., & Wang, C. (2019). Non-pharmacologic therapies for systemic lupus erythematosus. Lupus, 28(6), 703-712. https://doi.org/10.1177/0961203319841435
Kim, D., Jang, S., & Park, J. (2020). Electroacupuncture and Manual Acupuncture Increase Joint Flexibility but Reduce Muscle Strength. Healthcare (Basel), 8(4). https://doi.org/10.3390/healthcare8040414
Tsang, A. S. M. W. P., & Bultink, I. E. M. (2021). New developments in systemic lupus erythematosus. Rheumatology (Oxford), 60(Suppl 6), vi21-vi28. https://doi.org/10.1093/rheumatology/keab498
Wang, H., Wang, B., Huang, J., Yang, Z., Song, Z., Zhu, Q., Xie, Z., Sun, Q., & Zhao, T. (2023). Efficacy and safety of acupuncture therapy combined with conventional pharmacotherapy in the treatment of systemic lupus erythematosus: A systematic review and meta-analysis. Medicine (Baltimore), 102(40), e35418. https://doi.org/10.1097/MD.0000000000035418
Facet hypertrophy is an incurable, chronic disease that affects the facet joints in the spine. Can recognizing symptoms, help in diagnosis, and treatment?
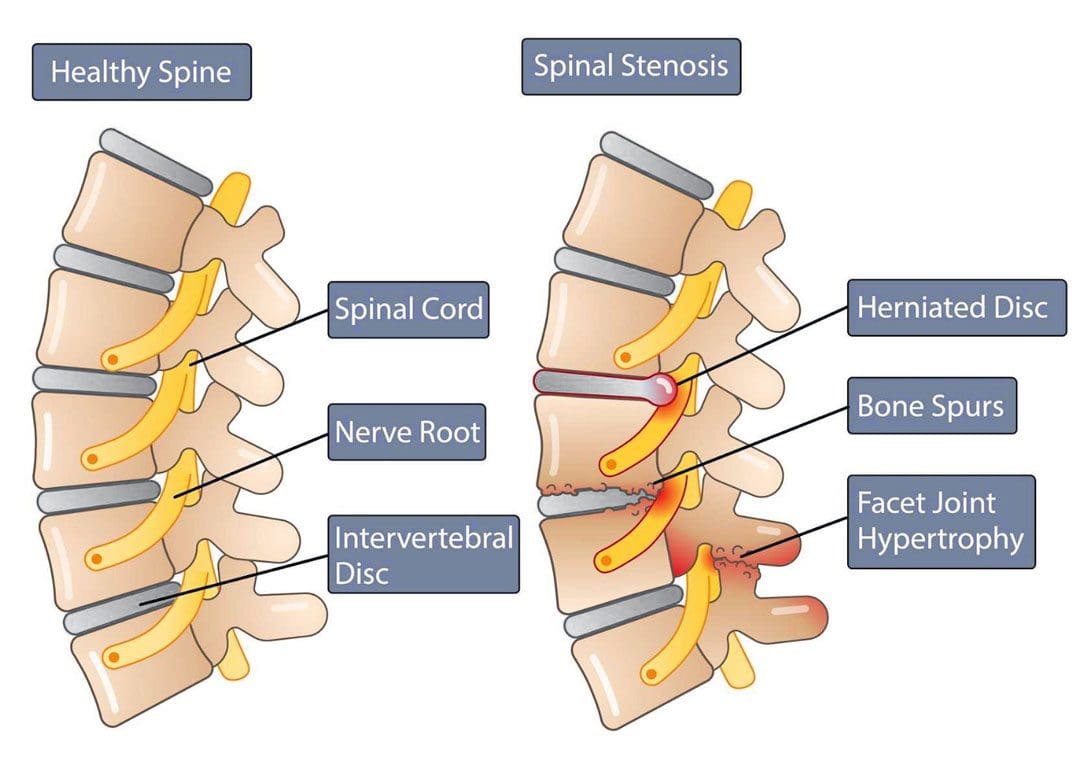
Facet Hypertrophy
Facet hypertrophy causes the facet joints in the spine to enlarge. They are found where the vertebrae come into contact on the back of the vertebrae that form the backbone. These joints stabilize the spine when twisting and bending. Hypertrophy results when damage wears down the cartilage that cushions the bones that meet in the joint. This can include:
Aging
Wear and tear
Arthritis
Other joint diseases can damage facet joints.
Swelling, new bone growth, and bone spurs can occur as the joint tries to repair the damaged cartilage. The swelling and new bone growth can narrow the spinal canal and compress surrounding nerves, causing pain and other sensation symptoms. This ailment does not have a cure and worsens over time. The objective of treatment is to manage the pain symptoms and slow down the disease’s progress.
Types
Facet hypertrophy can be described as unilateral or bilateral.
Symptoms can have a wide range of intensity, from a dull ache to chronic, disabling pain. The location of symptoms depends on the affected joint and the nerves involved, Pain manifests when the enlarged joints and new bone growth compresses the nearby nerves. The result leads to nerve damage and the following symptoms: (Weill Cornell Medicine Brain & Spine Center. 2023) (Cedars Sinai. 2022)
Stiffness, especially when standing up or getting out of a chair.
Inability to stand straight when walking.
Inability to look up to the left or right without turning the whole body.
Reduced range of motion and mobility.
Numbness or a tingling sensation of pins and needles.
Radiating pain from the affected joint into the buttocks, hips, and upper thigh when the affected joint/s are in the lower back.
Radiating pain from the affected joint into the shoulder, neck, and back of the head when the affected joint/s are in the upper back.
Headaches when the affected joint is in the neck.
Causes
A common cause is the age-related degeneration of the joints, called spondylosis. Research indicates that more than 80% of individuals who are 40 or older have radiologic evidence of spondylosis, even though they may not have symptoms. (The University of Toledo Medical Center. N.D.) The following conditions can also increase the risk of facet hypertrophy (Weill Cornell Medicine Brain & Spine Center. 2023)
Unhealthy posture
Being overweight or obese
Sedentary lifestyle
Injury or trauma to the spine
Inflammatory conditions like rheumatoid arthritis or ankylosing spondylitis
Osteoarthritis
Genetic predisposition to the condition
Diagnosis
Diagnosis can be challenging when neck or back pain is the main complaint, as symptoms can mimic conditions such as sciatica from a herniated disc or hip arthritis. (Weill Cornell Medicine Brain & Spine Center. 2023)
A healthcare provider will conduct a complete physical examination, medical history, and discussion of symptoms.
CT scans with or without myelogram – the use of contrast dye in the space around the spinal cord.
MRI
X-rays with or without a myelogram
A diagnosis is confirmed by injecting a diagnostic block that involves administering an anesthetic injection, sometimes with an anti-inflammatory like cortisone, into the joint or nerves near the affected joint. Two injections are given at different times to confirm the effect. (Romain Perolat et al., 2018)
If immediate relief improves after each injection, the facet joint is confirmed as the source of the pain symptoms.
If the block does not decrease the pain, the facet joint is probably not the source of the pain symptoms. (Brigham and Women’s Hospital. 2023)
Treatment
There is no cure for facet hypertrophy.
The goal of treatment is to make the pain more manageable.
Conservative treatment is usually successful in making a difference.
Nonsteroidal anti-inflammatory – aspirin, ibuprofen, and naproxen.
Muscle relaxers – cyclobenzaprine or metaxalone.
Steroid injection into the facet joints.
Injection of platelet-rich plasma/PRP into the joints.
Medial Branch or Facet Block
A medial branch block injects local anesthetic near the medial nerves that connect to an inflamed joint.
Medial nerves are small nerves outside the joint space near the nerve that transmit signals and other impulses to the brain.
A facet block injects the medication outside the joint space near the nerve that supplies the joint called the medial branch.
Neurolysis
Neurolysis, also known as rhizotomy or neurotomy, is a procedure that destroys affected nerve fibers to relieve pain, reduce disability, and reduce the need for analgesics. This treatment can relieve pain for six to 12 months until the nerve regenerates, where further treatments may be necessary. (Matthew Smuck et al., 2012) Neurolysis can be performed using one of the following techniques (Romain Perolat et al., 2018)
Radiofrequency ablation RFA – the application of heat through radiofrequency.
Cryoneurolysis – the application of cold temperatures to the targeted nerve.
Chemical neurolysis – applying chemical agents, like a combination of phenol and alcohol.
Severing the nerves with surgical instrumentation.
Surgery
When one or more facet joints are severely damaged, they can become nonfunctional and painful. Surgery may be recommended when symptoms are not relieved by other therapies. (Ali Fahir Ozer, et al., 2015)
Prognosis
Facet hypertrophy is a chronic condition that progresses with age and does not affect life expectancy. (Weill Cornell Medicine Brain & Spine Center. 2023) The disorder is incurable, but symptoms can be managed with conservative therapies
A healthcare provider can help develop a treatment plan based on the extent and location of the joint affected.
Early diagnosis and treatment can help individuals achieve the best results.
Maintaining an active lifestyle and healthy weight can help prevent further joint stress. Individuals may be recommended to do regular stretching and strengthening exercises to lower inflammation, reduce stress, and improve overall health.
Facet Syndrome Treatment
References
Perolat, R., Kastler, A., Nicot, B., Pellat, J. M., Tahon, F., Attye, A., Heck, O., Boubagra, K., Grand, S., & Krainik, A. (2018). Facet joint syndrome: from diagnosis to interventional management. Insights into imaging, 9(5), 773–789. https://doi.org/10.1007/s13244-018-0638-x
Smuck, M., Crisostomo, R. A., Trivedi, K., & Agrawal, D. (2012). Success of initial and repeated medial branch neurotomy for zygapophysial joint pain: a systematic review. PM & R : the journal of injury, function, and rehabilitation, 4(9), 686–692. https://doi.org/10.1016/j.pmrj.2012.06.007
Ozer, A. F., Suzer, T., Sasani, M., Oktenoglu, T., Cezayirli, P., Marandi, H. J., & Erbulut, D. U. (2015). Simple facet joint repair with dynamic pedicular system: Technical note and case series. Journal of craniovertebral junction & spine, 6(2), 65–68. https://doi.org/10.4103/0974-8237.156049
Finger sprains and dislocations are common hand injuries that can happen during work, physical/sports activities, or in automobile collisions and accidents. Can recognizing the symptoms help in developing an effective treatment strategy?
Finger Sprains and Dislocations
Finger sprains and dislocations are common injuries of the hand that cause pain and swelling.
A sprain happens when the finger tissue that supports a joint gets stretched beyond its limits in a way that stresses the ligaments and tendons.
The ligament tissue can be partially or completely torn. If the damage is bad enough, the joint comes apart.
This is a dislocation – A dislocation happens when the joint in the finger gets shifted out of its normal position.
Both injuries can cause pain and stiffness in the finger and hand.
Sprains
Finger sprains can happen any time the finger bends in an awkward or unusual way. This can happen from falling on the hand or getting hurt when engaged in physical activities like sports or household chores. Sprains can occur in any of the knuckle joints in the finger. However, most commonly, the joint in the middle of the finger gets sprained. It’s known as the proximal interphalangeal or PIP joint. (John Elfar, Tobias Mann. 2013) Symptoms of a finger sprain can include:
Other treatments to help a sprained finger include:
Elevate the hand if swelling and inflamed.
Gentle finger exercises/movements to prevent stiffness.
Icing the injured finger.
Take an anti-inflammatory medication.
Individuals who have not broken bones or dislocated the joint will probably be able to move their finger in about a week. A doctor will set a timeline for when to start using the finger normally.
Individuals who sprain their finger that feels swollen and stiff for longer than a few weeks are recommended to consult a doctor or specialist.
Thumb sprains and finger sprains in children may need to be splinted or taped for longer periods, as the ligament is not fully developed or as strong, which could lead to a tear.
Dislocations
A finger dislocation is a more severe injury involving the ligament, joint capsule, cartilage, and other tissues that causes misalignment of the finger. The ligaments and the joint capsule get torn when a joint is dislocated. The joint needs to be reset, which can be a simple process, or in severe cases, patients may need to be placed under anesthesia or undergo surgery to reset the joint properly.
In these cases, tendons or other tissues might be preventing the joint from getting into position.
Putting the finger back into the right position is known as”reduction.” Once reduced, the finger needs to be splinted.
Individuals also need an X-ray to ensure the joint is lined up correctly and that any bones were not broken or fractured when they sustained the injury. (James R. Borchers, Thomas M. Best. 2012)
Once reset, caring for a dislocated finger is basically the same as a sprained finger. Using ice on the finger, keeping the hand elevated to reduce swelling.
Elfar, J., & Mann, T. (2013). Fracture-dislocations of the proximal interphalangeal joint. The Journal of the American Academy of Orthopaedic Surgeons, 21(2), 88–98. https://doi.org/10.5435/JAAOS-21-02-88
OrthoInfo from the American Academy of Orthopaedic Surgeons. (2022) Hand fractures.
Hung, C. Y., Varacallo, M., & Chang, K. V. (2023). Gamekeeper’s Thumb. In StatPearls. StatPearls Publishing.
OrthoInfo from the American Academy of Orthopaedic Surgeons. (2022) Finger fractures.
Borchers, J. R., & Best, T. M. (2012). Common finger fractures and dislocations. American family physician, 85(8), 805–810.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine