Skateboarding is a popular activity among children, teenagers, and young adults. It is recreational, competitive, fun, and exciting but, like any sport, carries a risk of injury. There are around 70,000 skateboarding injuries requiring a visit to the emergency room every year. The most common injuries involve the shins, ankles, forearms, wrists, elbows, face, and skull, with many left untreated that worsen as they heal improperly, leading to further damages and complications. Chiropractic can treat the injuries, rehabilitate the muscles and joints, and strengthen the body to get the skater back on their board.
Skateboarding Injuries
Skateboarding injuries can range from scrapes, cuts, and bruises to sprains, strains, broken bones, and concussions.
Shin injuries often happen during flip/twist tricks where the board or axle hits the shin causing bruising and swelling.
Shoulder, wrist, and hand injuries are common when skaters lose their balance and fall with outstretched arms.
Ankle injuries include rolls/sprains, as well as dislocations and fractures.
Dislocations usually happen to the shoulders, wrists, and fingers.
Facial injuries include teeth knocked out, broken nose, or jaw are typically caused by fast forward hard falls.
Severe injuries include concussions and head injuries.
Injury causes
Skateboarding injuries typically occur from:
Skating on irregular surfaces locks up wheels and affects balance, causing falls.
Losing balance or losing control of the board and falling hard/slamming into the pavement.
Inexperience, slow reaction times, and less coordination lead to falls and slams.
Skating into another skater, a person walking or cycling, a car, or a road hazard.
Trying an advanced trick/maneuver too soon and beyond their skill level.
Help prevent further injuries and long-term effects.
Chiropractic Skateboarding Injury Treatment
References
Forsman, L, and A Eriksson. “Skateboarding injuries of today.” British journal of sports medicine vol. 35,5 (2001): 325-8. doi:10.1136/bjsm.35.5.325
Hunter, Jamie. “The epidemiology of injury in skateboarding.” Medicine and sport science vol. 58 (2012): 142-57. doi:10.1159/000338722
Partiali, Benjamin, et al. “Injuries to the Head and Face From Skateboarding: A 10-Year Analysis From National Electronic Injury Surveillance System Hospitals.” Journal of oral and maxillofacial surgery: official journal of the American Association of Oral and Maxillofacial Surgeons vol. 78,9 (2020): 1590-1594. doi:10.1016/j.joms.2020.04.039
Shuman, Kristin M, and Michael C Meyers. “Skateboarding injuries: An updated review.” The Physician and sportsmedicine vol. 43,3 (2015): 317-23. doi:10.1080/00913847.2015.1050953
Individuals drive to jobs, to school, run errands, take road trips, spending a lot of time on the road. Accidents and crashes happen more frequently with all kinds of injuries. The National Highway Traffic Safety Commission has found that 37% of car accidents and crashes involve leg injuries and damage. Chiropractic physical rehabilitation and functional medicine can help heal injuries getting the individual back to everyday life.
Bruising and cuts are typical from the impact and the body getting slammed around. Lacerations can be noticed right away, but bruising comes from blood pooling underneath the skin and can take time to present, possibly 24 to 48 hours. Most bruises and cuts heal independently from home first aid care. A standard recovery used to take care of bruising is R.I.C.E or rest, ice, compression, and elevation. This helps the healing process; however, if the injury/s are more severe, chiropractic can help with therapeutic massage to relieve pain and strengthen the injured muscles, tendons, and ligaments.
ACL Injuries
The femur or thigh bone has several bands of tissue connecting it to the patella or kneecap and tibia or shin bone. One of the bands is the anterior cruciate ligament or ACL. Injuries to this band of tissue are common in sports. Car accidents and crashes are another common cause, specifically tearing the ligament. Individuals experiencing a tear may notice some or all of the following symptoms:
A cracking or popping sound when the accident or crash took place.
Swelling in and around the knee.
Severe pain in and around the knee.
Unstable and unsteady when walking or standing.
Reduced range of motion that makes walking or moving difficult.
A chiropractor can help treat the injury and help correct any muscular imbalances.
Meniscus Tears
Tears to the meniscus are also common in car accidents and crashes. The meniscusis a part of the knee. Two wedge-shaped pieces of cartilage provide a cushion where the femur and tibia meet to absorb shock. The wedges are called menisci.
When the meniscus tears, individuals might feel or hear a pop and could feel the leg suddenly give out.
Swelling in the knee.
Some pain but still be able to walk.
The knee will be stiff for the next few days.
More difficulty bearing weight or walking.
The RICE method is a recommended method of self-care. Many meniscus tears do not require surgery to improve knee function. Mild to moderate meniscus tears can be successfully treated with chiropractic techniques like soft tissue work, corrective stretches, and exercises. Surgery could eventually be necessary for severe cases to repair the meniscus to prevent long-term complications.
Chiropractic care can help the body heal and recover from a bone fracture. A patient’s bone density is evaluated and tested with an individualized treatment plan to help regain and maintain optimal bone strength. The treatments strengthen the muscles, reduce stiffness, improve nutrition, and relieve pain. Manipulation adjustments, rehabilitation, relaxation techniques, and dietary health coaching help individuals heal faster and strengthen their bones. The objective is to help regain increased mobility and range of motion.
Sciatica
Car accidents and crashes are one instance where the spine can be damaged enough to bring on sciatic pain where no back problems were present before. The impact from a car accident can cause the discs to be knocked out of place, damaged, and/or rupture around the surrounding tissue. Any of these results can pinch the sciatic nerve, leading to pain and other sciatica symptoms. Chiropractic can realign the spine and relieve pressure from the nerve/s.
DOC Spinal Decompression Table
References
Atkinson, T, and P Atkinson. “Knee injuries in motor vehicle collisions: a study of the National Accident Sampling System database for the years 1979-1995.” Accident; analysis and prevention vol. 32,6 (2000): 779-86. doi:10.1016/s0001-4575(99)00131-1
Foulk, David M, and Brian H Mullis. “Hip dislocation: evaluation and management.” The Journal of the American Academy of Orthopaedic Surgeons vol. 18,4 (2010): 199-209. doi:10.5435/00124635-201004000-00003
Wilson, L S Jr et al. “Foot and ankle injuries in motor vehicle accidents.” Foot & ankle international vol. 22,8 (2001): 649-52. doi:10.1177/107110070102200806
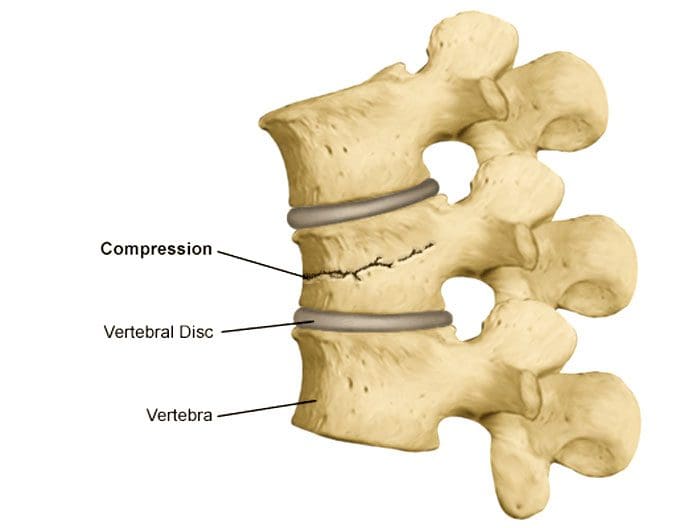
Sometimes the bones or vertebrae of the spine can crack and collapse under their weight. This is known as a compression fracture, vertebral compression fracture, or VCF. There are almost 1 million compression fractures every year, usually because the bones become weakened and crack under the weight of the vertebrae above them. These fractures can cause spinal weakness affect posture and the ability to stand up straight. They are often the cause for individuals to hunch over, also called kyphosis.
Compression Fracture
Compression fractures are small breaks or cracks in the vertebrae. The breaks occur in the vertebral body, the thick rounded part on the front of each vertebra. These fractures cause the spine to weaken and collapse. With time, these fractures affect posture as the spine curves forward. The fractures are often found in the middle/thoracic spine in the lower area. They often result from osteoporosis but can also happen after a trauma like an automobile accident, work, sports injury, or a tumor on the spine.
Symptoms
Compression fracture symptoms range from mild to severe or no symptoms. Many individuals can stand or walk without pain. They are often discovered when X-rays are taken for another condition. Symptoms include:
Back pain can come on suddenly and last for a significant time, often diagnosed as chronic back pain.
It usually develops between the shoulders and the lower back.
The pain and discomfort decrease when lying down and worsen when standing or walking.
Decreased mobility or flexibility in the spine. Individuals are unable to twist or bend.
Hunched over appearance, known as dowager’s hump or hunchback.
Loss of height from the vertebrae compression and the spine curving.
Pinched nerves
Nerve damage can cause tingling, numbness, and difficulty walking.
Loss of bladder or bowel control with severe, untreated fractures.
Individuals At Risk
Individuals who have had a compression fracture are more likely to have another one.
Women over 50 have a higher risk due to osteoporosis.
With age, the risk increases for men and women.
Diagnosis
A doctor will perform an examination and ask about symptoms. The exam will include:
Checking spinal alignment.
Posture analysis.
Gently palpates different areas of the back to identify the source of pain.
Examine for signs of nerve damage that include numbness, tingling, or muscle weakness.
A doctor will order imaging studies to examine the backbones, muscles, and soft tissues. Imaging studies include:
CT scan, X-ray, or MRI of the spine.
DEXA scan is a type of X-ray that measures bone loss bone density.
A myelogram is a procedure used along with imaging studies. A contrast dye is injected into the spine before the scan making the images easier to see.
Compression fracture treatment focuses on relieving pain, stabilizing the vertebrae, and ongoing fracture prevention. Treatment depends on the severity of the fracture and the individual’s overall health. Treatment can include:
Pain Medication
A doctor can recommend over-the-counter non-steroidal anti-inflammatory medication.
A doctor may prescribe muscle relaxers or prescription medication.
Follow instructions carefully when taking medications.
Back Brace
A special type of back brace helps to support the vertebrae.
The brace can also relieve pain by reducing how much the spine moves.
Strengthening Meds
Medications known as bisphosphonates can help slow down bone loss, stabilize the bones and prevent fractures.
This minimally invasive procedure relieves pain, stabilizes the bones, and improves mobility.
During vertebroplasty, the doctor inserts a needle in the vertebra and injects bone cement.
During kyphoplasty, the doctor inserts an inflatable device that they fill with cement.
Both are outpatient procedures allowing the individual to go home the same day.
Individuals over 65 or that have osteoporosis or a history of cancer are recommended to see their doctor. Individuals who present with sudden back pain that doesn’t get better after a day or two are advised to see a doctor and evaluate for back pain so the doctor can determine the cause and develop a treatment plan.
Body Composition
Vitamin D To Build Muscle
Skeletal Muscle Mass decreases as the body ages, primarily due to decreased physical activity. Vitamin D has been reported to influence muscle quality. This could be helpful for adults as they age. Muscle loss diminishes functional performance on activities that require strength and coordination. When this loss of muscle mass becomes significant, it becomes a condition known as sarcopenia. Treatments include:
All were found to slow down muscle loss and help regain muscle mass and strength.
Vitamin D supplementation is effective, especially in older adults whose blood levels are low.
References
American Academy of Orthopaedic Surgeons. Osteoporosis and Spinal Fractures. (https://orthoinfo.aaos.org/en/diseases–conditions/osteoporosis-and-spinal-fractures/) Accessed 10/25/2021.
American Association of Neurological Surgeons. Vertebral Compression Fractures. (https://www.aans.org/en/Patients/Neurosurgical-Conditions-and-Treatments/Vertebral-Compression-Fractures) Accessed 10/25/2021.
Bischoff-Ferrari, H A et al. “Vitamin D receptor expression in human muscle tissue decreases with age.” Journal of bone and mineral research: the official journal of the American Society for Bone and Mineral Research vol. 19,2 (2004): 265-9. doi:10.1359/jbmr.2004.19.2.265
Donnally III CJ, DiPompeo CM, Varacallo M. Vertebral Compression Fractures. [Updated 2021 Nov 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448171/
Hassan-Smith, Zaki K et al. “25-hydroxyvitamin D3, and 1,25-dihydroxyvitamin D3 exert distinct effects on human skeletal muscle function and gene expression.” PloS one vol. 12,2 e0170665. 15 Feb. 2017, doi:10.1371/journal.pone.0170665
McCarthy, Jason, and Amy Davis. “Diagnosis and Management of Vertebral Compression Fractures.” American family physician vol. 94,1 (2016): 44-50.
Individuals involved in slip and fall accidents lead to around 9 million emergency room visits a year. Recovering from a severe injury suffered in a slip and fall accident requires extensive medical care and physical rehabilitation. Older adults are susceptible to slip and fall injuries. According to the CDC, falls are the leading cause of nonfatal injuries of older adults and are a common hazard in nursing homes, where between half of the residents fall each year. The most common injuries sustained include:
Cuts and Abrasions
Cuts and abrasions can be minor to severe. Leg and arm abrasions are the most common, followed by wounds to the head and hips. These injuries require superficial treatment and possibly stitches. However, if the impact of the fall is severe, cuts and abrasions can overlap more severe injuries like concussions and broken bones.
Soft Tissue Injuries
Soft tissue injuries often do not get noticed, so individuals don’t realize they have a mild tissue injury until days or weeks after the fall.Soft tissue injuries can range from minor ankle and/or wrist sprains to severe tears in tendons and ligaments.Left untreated, these injuries can lead to chronic pain conditions making the body more vulnerable to further injuries.Even when individuals feel fine after a slip and fall accident, they are recommended to seek medical care or consult an injury specialist as soft tissue injuries don’t often produce immediate symptoms.
Sprains and Strains
A slip and fall accidents often happen as a result of taking an uneven or awkward step. Individuals also often react with their hands in front to try to cushion the fall. Both the awkward step and pushing the hands out can cause the wrist or ankle to tear, causing a sprain or a strain. The ligaments do not circulate a lot of blood, meaning that healing and recovery can take a significant amount of time.
Broken Bones
A fall can result in stressful forces on the bones of the body. In slip and fall accidents, hip, wrist, and ankle fractures are the most common bones that get broken. The older an individual is, the more likely they will break a bone from a slip and fall accident.
Hip Fractures
More than 95% of broken hips are caused by falls, according to the CDC.Hip fractures often require surgery that can include implantation of an artificial hip and hospitalization for about a week, followed by extensive physical therapy and rehabilitation.
Knee Injuries
Knee injuries can result from a slip and fall, especially if the knee gets rotated the wrong way or twisted. Knees are made up of bone and ligaments, meaning it could take a long to heal and recover. Dislocation of the patella is also a possibility that could require knee reconstruction.
Neck and Shoulder Injuries
Shoulder and neck injuries can be the result of landing on the shoulder or neck. They can also occur from overexertion when trying to right oneself during a fall. Neck injuries can range from:
Muscle sprains
Spinal injuries
Paralysis
Shoulder injuries can result in:
Shoulder dislocation
Torn nerves
Collarbone breaks
Even the most minor neck and shoulder injuries can require surgery and rehabilitation.
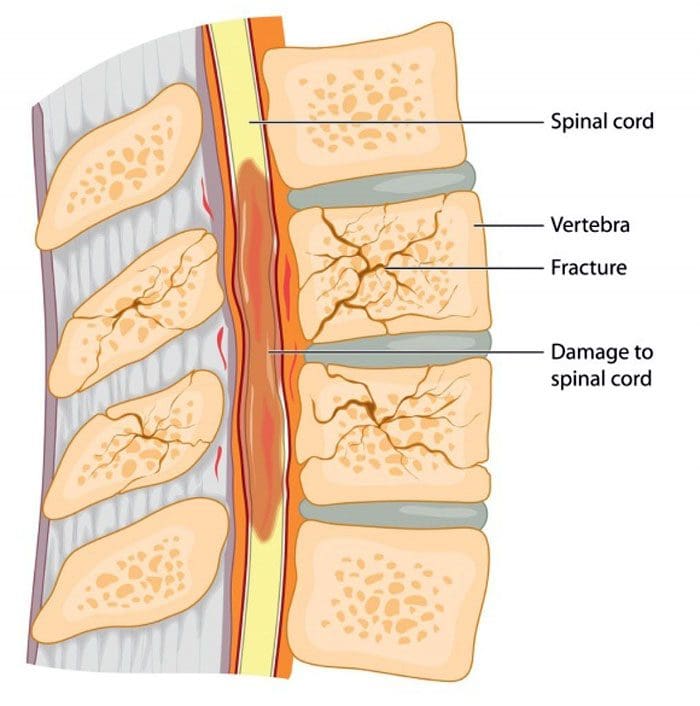
Back and Spinal Cord Injuries
Severe impact on the body in a slip and fall accident can cause slipped or herniated discs and fractured vertebrae, causing significant pain and limiting mobility. An injury to the spinal cord can lead to temporary paralysis, permanent paralysis, neurologic and sensory impairments. According to the Mayo Clinic, falls cause more than a quarter of spinal cord injuries and the majority of spinal injuries among adults 65 and older.
Traumatic Brain Injuries
Traumatic brain injuries occur when an individual hits their head on a hard surface during a fall. Traumatic brain injuries can range from:
A chiropractor will review imaging scans, medical history, and current symptoms to determine the best form of treatment. Inflammation is common and is the body’s defense to protect the injured area by slowing down the blood flow in that area to allow the body’s internal defenses to repair the injury. Sometimes the body overreacts to the problem and produces far more inflammation than is needed. Depending on the severity of the injury, various massage, manipulation techniques, and tools will be utilized to help the body heal itself.
Body Composition
Recovery and Swelling
Recovery is an essential part of individuals involved in physical training programs and after injury. A significant sign that the body has undergone intense physical exertion and requires recovery is swelling. Swelling occurs for several reasons and is the body’s response to tiny, microscopic muscle tears that arise from intense use. It is possible to see this swelling in body composition results. Recovery is about giving the body a chance to:
Relax
Recuperate
Recover from the swelling to resume normal physical activities.
References
Courtney, T K et al. “Occupational slip, trip, and fall-related injuries–can the contribution of slipperiness be isolated?.” Ergonomics vol. 44,13 (2001): 1118-37. doi:10.1080/00140130110085538
Kannus, Pekka et al. “Prevention of falls and consequent injuries in elderly people.” Lancet (London, England) vol. 366,9500 (2005): 1885-93. doi:10.1016/S0140-6736(05)67604-0
Reuben, David B et al. “The Strategies to Reduce Injuries and Develop Confidence in Elders Intervention: Falls Risk Factor Assessment and Management, Patient Engagement, and Nurse Co-management.” Journal of the American Geriatrics Society vol. 65,12 (2017): 2733-2739. doi:10.1111/jgs.15121
Rosen, Tony et al. “Slipping and tripping: fall injuries in adults associated with rugs and carpets.” Journal of injury & violence research vol. 5,1 (2013): 61-9. doi:10.5249/jivr.v5i1.177
Vitamin B12 and Shoulder Injuries. Most shoulder injuries involve the muscles, ligaments, and tendons. Individuals that perform repetitive arm motions/movements, constantly lift objects as part of their job, and athletes that use their arms repetitively have an increase in developing/experiencing shoulder injuries and problems. Shoulder injuries are commonly caused by physical activities that involve:
Excessive motions
Repetitive motions
Overhead motions
Sports like swimming, tennis, pitching, and weightlifting involve these repetitive arm/shoulder motions that contribute to shoulder injuries.
Injuries can also be brought on from everyday activities like washing/painting walls, hanging curtains/plants, and gardening.
Shoulder Injury Symptoms
If there is discomfort and/or pain in and around the shoulder here are a few ways to analyze the situation.
Does the shoulder feel like it could pop out or slide out of its socket?
Is there a lack of strength in the shoulder for normal daily activities?
If yes was an answer to any of these questions, individuals should consult an orthopedic surgeon and/or chiropractor for assistance in determining the problem and its severity.
Injury Categories
Individuals often underestimate the extent of an injury and usually just push/play through the discomfort and pain. This is how powerful the brain is as it ignores steady pain, weakness, or limitation of joint motion. Shoulder injuries and problems are grouped in the following categories.
Instability
This is when a shoulder joint moves/shifts or is forced out of its normal position. This is called instability and can result in dislocation of the joints in the shoulder. Individuals will experience pain when raising their arms. It can feel as if the shoulder is slipping out.
Impingement
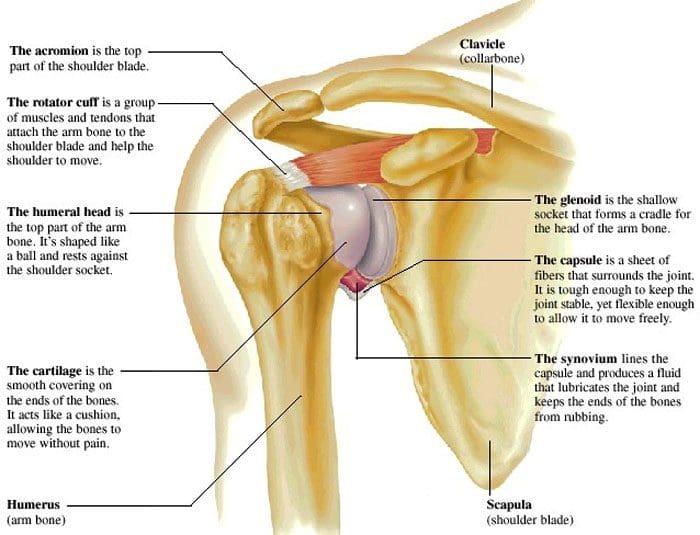
Impingement is caused by excessive rubbing/friction of the muscles against the top part of the shoulder blade, known as the acromion. Impingement can happen during physical activities that require excessive overhead arm motion. Medical examination and care are recommended for inflammation, as it could eventually lead to a more serious injury.
Injuries
Bursitis
The bursa is the fluid-filled sacs that cushions the joints. These can become swollen and irritated from repetitive motions, falls, or other injuries. Individuals will notice the pain most when moving/rotating the shoulder.
Cartilage tear
The cartilage – the rubbery padding that goes around the rim of the shoulder joint can get damaged from repetitive motions, overextending, falls, or from intense force to the shoulder. With this type of injury individuals feel pain when reaching overhead, weakness, and/or catching, locking, and grinding feelings.
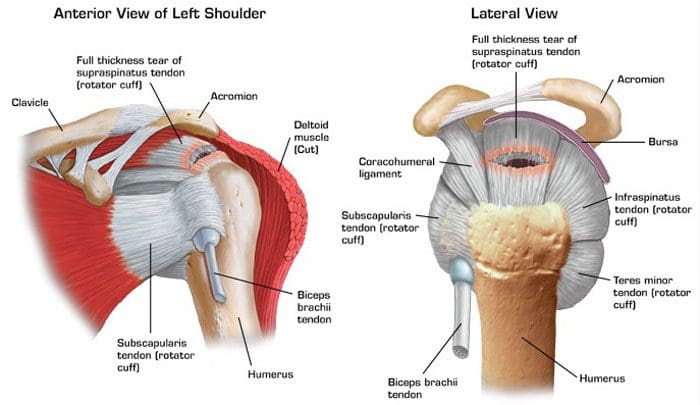
Rotator cuff tear
The rotator cuff consists of a group of muscles and tendons that hold the arm in place and allow for lifting the arm up and overhead. It can get damaged through overuse, falls, and regular wear and tear with age. Pain often presents at night, when lifting objects, and there could be a cracking sound when trying to move or rotate.
Frozen shoulder
This condition limits the joint’s movement. What happens is abnormal bands of tissue called adhesions build up in the joint and restrict movement. The shoulder can freeze up from not using it. This could be because pain or surgery causes an individual to use it less. This is when adhesions begin to build up.
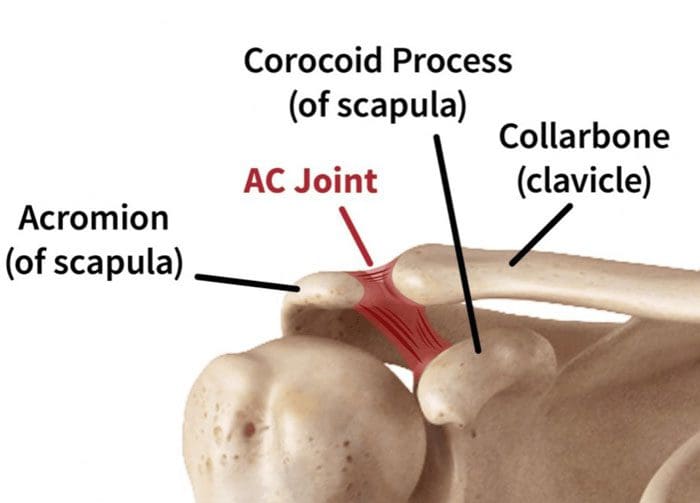
Separation
This injury affects the joint where the collarbone and shoulder blade join. It is known as the acromioclavicular or AC joint. A fall or hard impact can tear the ligaments that hold it together. If the collarbone gets pushed out of place a bump forms/develops on top of the shoulder.
Fracture
A bone can break or crack from a vehicle accident, fall, or takes a hard hit. The most common fractures are to the clavicle – collarbone and the humerus – arm bone closest to the shoulder. This type of injury causes a great deal of pain and bruising. If the collarbone is broken, the shoulder can sag with the inability to lift the arm.
Vitamin B12
Rotator cuff injuries involve dysfunctional and/or damaged connective tissue. This could be from impaired collagen synthesisVitamin B12 helps combat inflammation and plays a significant role in collagen formation. Low vitamin B12 status can be directly linked to pro-inflammatory cytokines. This means that a lack of vitamin B12 increases inflammation.
Researchers followed a group of individuals to determine if their individual vitamin B12 levels correlated with an increased risk of a rotator cuff tear. To begin the study, levels of vitamin B12 were measured along with other nutrients that included:
Vitamin D
Zinc
Calcium
Magnesium
Folate
Homocysteine and blood sugar biomarkers, which are both associated with B12 metabolism were also measured. Homocysteine is a metabolite that builds up in the blood when specific nutrients, like B12, folate, or B6 become deficient. Elevated levels of homocysteine can be harmful and cause damage to blood vessels and brain tissue when not detoxified properly. In the study, the homocysteine levels did not differ between the groups, but vitamin B12 levels were significantly different.
The patients that were included were a healthy group that did not have any rotator cuff injury during the study.
The second group all experienced a rotator cuff tear that required surgery during the study.
With the various nutrients measured, only vitamin B12 and vitamin D showed differences. With the B12 and D being lower in the group that had the shoulder injury.
Specifically, the B12 levels in the healthy group were 627 pg/mL compared to 528 pg/mL in the injured group. This was a 16% decrease.
These subclinical deficiencies are usually missed with traditional serum testing which is why functional nutritional testing is clinically recommended.
Body Compositional Testing
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP*, CIFM*, CTG*
email: [email protected]
phone: 915-850-0900
Licensed in Texas & New Mexico
References
American Society for Surgery of the Hand: Shoulder Pain.
American Academy of Family Physicians: Shoulder Pain.
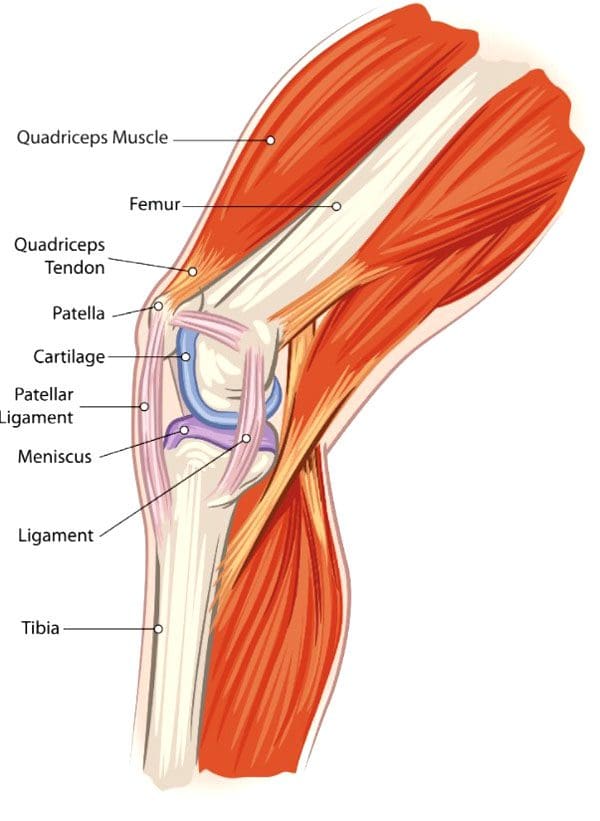
Knee Injuries, Surgeries, and Vitamin D Status. The knee joint is one of the largest and complex joints. It connects the thigh bone to the shinbone, which has a very important role in:
Supporting the body’s weight
Facilitating movement
Allowing the ability to bend the knee
Because of the complexity of the knee joint, it is highly susceptible to injuries. The most common injuries include tears in the:
Ligaments
Tendons
Cartilage
The kneecap itself can be fractured and/or dislocated.
Tears
Meniscal Tears
The meniscus is the cartilage between the knee joint that absorbs the impact/shock when running, playing sports, yard work, hiking, bicycling, etc. It cushions the joint and maintains stability.
Meniscus tears are common in sports that have a lot of jumping, starting/stopping quickly, changing direction suddenly, like volleyball, basketball, tennis, soccer, football. This is when the meniscus tears. Surgery can be required, depending on the severity/extent of the injury and tear.
Tendon Tears
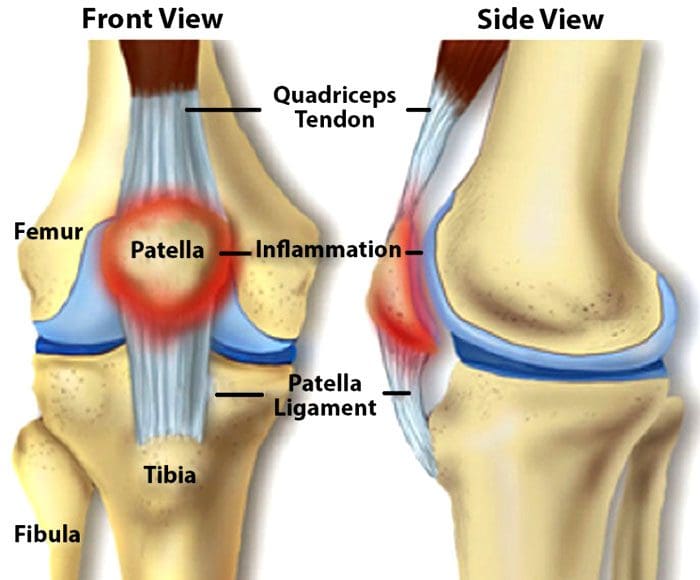
The patellar tendon works with the knee muscles in the front of the thigh to straighten the leg. Tears in the patellar tendon are common among middle-aged individuals and those that participate in running or jumping sports.
A complete tear is considered a disabling injury that requires surgery for full functional recovery.
Fortunately, most tears are partial and require rest and chiropractic/physical therapy to heal.
Dislocation
Knee dislocations happen when the knee bones shift out of position. This can happen after a fall, car crash, or high-speed impact. It can also be caused by twisting the knee while the foot stays planted. Dislocations require relocation. However, sometimes a dislocated kneecap corrects itself and returns to the proper position. Other cases can require a mild sedative to allow a doctor to relocate the knee. Dislocations generally take around six weeks to fully heal.
Anterior Cruciate Ligament – ACL Injury
The anterior cruciate ligament or ACL is knee tissue that joins the upper and lower leg bones and maintains the knees’ stability. The ACL can be torn if the lower leg over-extends forward or if the leg gets twisted. ACL injuries are common knee injuries and account for around 40% of sports-related injuries. These injuries can range from a small tear in the ligament to a severe injury where the ligament tears completely or gets separated from the bone. Treatment depends on the severity of the injury. Depending on various factors including the severity of the tear, surgery could be required.
Knee Surgery
For most cases, surgery is done using arthroscopytechnology. This procedure uses small incisions to insert a camera and surgical instruments into the joint. Usually, two or three incisions are needed with recovery time being quicker than large incision surgery where the whole knee is opened. Minimally invasive arthroscopic surgery is preferred by sports medicine experts. With this procedure:
There is no need to cut the tendons or muscles
Bleeding is reduced
Small incisions decrease scarring
Recovery time is shorter
However, sometimes a large incision is required for complex surgical techniques. Common knee surgery procedures include:
Arthroscopy Surgery
This method allows the ability to see inside the knee joint. The procedure is often recommended for:
Diagnosis
Minor repairs to ligaments and/or tendons
Cartilage or bone that needs to be removed
Total Knee Replacement
A full knee replacement is known as arthroplasty. When the joint is damaged beyond repair from injury or disease, an implant is placed in the knee joint restoring function. A small amount of cartilage and bone from the shinbone and thigh bone gets removed for perfect placement of the new knee joint.
Revision Knee Replacement
Most knee replacements last around 15 – 20 years. For individuals that have knee replacement early, then a new operation for new implants could be required. Here, the surgeon removes the original prosthesis and replaces it with a new one.
Partial Knee Replacement
Some knee injuries do not require complete replacement. Here, only the worn-out portion of the joint is replaced. As an example, the cartilage that has been lost in an area of the knee can be repaired with a partial replacement.
Vitamin D Status
A study on athletes that underwent ACL surgery looked at their vitamin d status and how it affected their recovery.
The research concluded that vitamin D status had no effect on surgery outcomes.
However, those with the lowest vitamin D status had three times the failure rate than those with higher vitamin D
The average age of the individuals was around twenty-four and were healthy athletes.
Each of the patients in this study had their vitamin levels measured before the operation and were grouped based on their vitamin D status:
Group 1 vitamin D below 20 ng/mL – considered deficient
Group 2 vitamin D between 20-30 ng/mL – considered low but in a technical range
Group 3 vitamin D above 30 ng/mL – considered sufficient, but not optimal
All were followed for two years with their surgery recovery being measured with two systems.
The Lysholm score, which is a 100 point scoring system that looks at an individual’s knee functions that include:
Mechanical locking
Instability
Pain
Swelling
Stair climbing
Squatting
The WOMAC score is a scoring system that measures:
After 2 years, the Lysholm score and the WOMAC scores were similar.
However, there was a difference in the graft failure rate which was about 6% in group 1 with the lowest vitamin D and around 2% in groups 2 and 3. This shows that the lowest vitamin D status has three times the failure rate compared with those that had increased vitamin D levels. Vitamin D is a known anti-inflammatory with metabolic functions that are documented. Therefore, vitamin D does improve surgical success and recovery in healthy athletes.
Body Composition
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP*, CIFM*, CTG*
email: [email protected]
phone: 915-850-0900
Licensed in Texas & New Mexico
References
Brambilla, Lorenzo, et al. “Outcome of total hip and total knee arthroplasty and vitamin D homeostasis.” British medical bulletin vol. 135,1 (2020): 50-61. doi:10.1093/bmb/ldaa018
European Journal of Orthopedic Surgery and Traumatology, January 2021
Zhang, Hao et al. “Vitamin D Status and Patient Outcomes after Knee or Hip Surgery: A Meta-Analysis.” Annals of nutrition & metabolism vol. 73,2 (2018): 121-130. doi:10.1159/000490670
Spinal vertebral compression fractures are a common injury in older individuals brought on from a lowered bone density. Hip and wrist fractures get most of the attention when it comes to osteoporosis. However, spinal fractures happen almost twice as often and affect around 700,000 individuals yearly. This is according to the American Academy of Orthopaedic Surgeons or the AAOS. These types of fractures are also known as:
Fragility fractures
Vertebral compression fractures
Osteoporotic compression fractures. These usually happen as a result of thinning and weakening bones caused by osteoporosis.
The Academy of Orthopedic Surgeons notes that changes in the body’s musculoskeletal bone structure can go unnoticed for years. This leads to the vertebrae narrowing and flattening, rounding the spine as a result, creating compression. Because of the weakened bone, the pressure, even from everyday low-impact movements like reaching, bending or twisting. There are strategies that can help prevent osteoporosis and osteoporotic compression fractures.
More Movement and Physical Activity
One prevention strategy that is highly recommended is more movement and physical activity. This does not include occasional gentle movements like taking a break from sitting. Improving the spine’s health means using the full range of motion and loading the bones so they can get build strength. This could be walking more, which creates spinal resistance. Also using light weights with high repetitions with five to ten pounds of a load is enough to challenge the spine without generating muscle stress.
Individuals think they need to rest more as they get older, but to build and maintain bone density to prevent osteoporotic compression fractures more physical activity is needed. Moving around for 10 to 15 minutes every hour is a good way to start. Incorporating more activity, and focusing on healthy diet changes will help shed excess weight. This will decrease pressure on the spine, reducing the risk of fractures. For individuals with osteoporosis of the spine, it is important to review any exercise plans with a physician or doctor of chiropractic to ensure that they are safe. The wrong types of movement or too much stress on a fragile spine can definitely cause a fracture.
Medications and Other Conditions
There are medications that can help build bone density, but there are also medications for conditions that can actually cause faster bone density loss. Individuals could be taking a medication that’s good for one issue/condition, but not realize it may be associated with a reduction in bone density. This is why it is important to review prescriptions with a doctor with bone density loss side effects in mind. Medications that can cause bone loss include:
Anti-seizure drugs like carbamazepine and phenytoin
Diuretics like furosemide
Also, review any underlying conditions that could affect osteoporosis. As an example, the National Institutes of Health or NIH note that individuals with diabetes, specifically type 1, can have poor bone quality increasing their risk of fractures.
Adding Calcium To The Diet
An adequate intake of calcium is essential for osteoporosis prevention and helps lower the risk of fragility fractures. A low calcium intake contributes significantly to lower bone density and faster bone loss with age. Vitamin D also helps in bone injury prevention.
Treatment
Compression fracture/s diagnosis are confirmed through imaging tests like:
X-rays
Magnetic resonance imaging MRI scan
Bone scan
Computed tomography CT scan
Bone density testing with dual-energy x-ray absorptiometry DEXA will determine bone mineral density. If a scan reveals there is a vertebral compression fracture, the most common approach is no treatment. According to the Academy of Orthopedic Surgeons, most individuals with this type of injury improve within three months with a combined rest period and limited pain medication use.
Some individuals are recommended to wear braces to restrict movement so the fracture can heal without any added compression or stress. For those that do not respond to non-surgical treatment, minimally invasive surgery could become an option. In both cases, a doctor will suggest similar aforementioned strategies to help strengthen the bones and prevent worsening or creating new issues.
More flab on the middle that gets harder to burn off
Performance at work, the gym, or on the road slows down or begins to reverse
Workouts, sporting events, physical activity that the body was able to bounce back from quite easily now take twice as long to recover from
Things start to change when the body enters its 30’s. Whether light exercise, playing weekend games, local sports, etc, the key is to just stay active. By paying close attention to nutrition and making minor adjustments, individuals can maintain and improve body composition, stay strong and healthy in their 30s and be ready for the future.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine