Cyclists: Now that summer is upon us and the chilly winds of winter are gone for at least a few months, more people are taking their fitness and recreational activities outside. Cycling is popular activity that fits both bills. It is a great way to unwind and enjoy the great outdoors, but it is also an excellent form of exercise.
Cyclists
Chiropractic provides excellent benefits for the cycler, whether you hit the trails on the weekend, incorporate cycling as part of your fitness regimen, or commute to work on your bike every day.
Relief from Pain
Faster Healing from Injuries
Better Muscle Tone and Balance
Improved Range of Motion
Enriched Cycling Biomechanics
In short, chiropractic can help make you a better cyclist and help you get the most out of your cycling. It will help keep your body aligned and balanced physically, but it also treats the whole body.
That means that your chiropractor will also make nutritional recommendations and even recommend various supplements if necessary. This will give your energy a boost and improve your performance, while helping you stay healthy and fit. This is how chiropractic helps you have more stamina and endurance.
Chiropractic For Cycling Injuries
As with any type of physical activity, there is always a chance that injuries will occur. Chiropractic helps keep your body balanced and improves your flexibility. This, in turn, decreases your chance for injury.
However, if you are injured, chiropractic can help you recover and heal much faster. You start with a healthy, balanced body through regular chiropractic care, and that helps you bounce back faster if you sustain an injury.
Chiropractic care can also be used to treat injuries. Cycling can cause pain and injury in the ligaments, muscles, knees, ankles, hips, hands, wrists, feet, neck, back, and shoulders.
Regular adjustments can help decrease the likelihood of pain in these areas, but sometimes the soreness can creep in anyway. When that happens, chiropractic treatments have been shown to be very effective in treating pain without pain medication and associated harmful side effects.
Spinal alignment is one of the most common chiropractic techniques, but it goes much farther than that. Adjustments to the legs and feet can help with ankle, knee, hip, and foot pain. Adjustments to the arms and shoulders can help relieve pain in those areas. Special attention to the joints help keep them flexible and functioning as they should.
Chiropractic Allows The Body�s Natural Ability To Heal
Chiropractic is completely natural and does not rely on invasive treatments or surgeries. It does not use medications of any kind. It uses nutrition and supplements that rely on the body�s natural ability to heal. It simply realigns the body so that the neural pathways are unobstructed. This allows blood flow to be more efficient and reach the organs much easier.
Chiropractic involves gentle spinal manipulations that realign the body and restore movement in the joints as well as muscle trigger points and soft tissue. It may include electrical muscular current therapies, massage, cold laser therapy, ultrasonic waves, and other therapies in addition to the spinal manipulations.
A chiropractic patient may be advised to rest, ice an area, elevate it, or be given specific exercises to work that area. Chiropractic is not a rote therapy as many traditional medical practices tend to be. It adjusts to each patient, taking into account their unique lifestyle, activity level, nutritional needs, and other elements that influence that particular patient�s healing process.
Chiropractic sees each patient as individual and treat them as such. This is what makes it such an effective treatment for cyclists. The benefits it offers them can not only keep them pain free and participating in their activity; it can also make them better at it.
Injury Medical Clinic: Back Pain Care & Treatments
5 benefits of�walking in order to achieve better health is not new. Doctors and fitness experts have been touting its benefits for decades. When you walk, you engage more than 200 muscles � this includes your pelvis and spine. This makes it an exceptional complement to chiropractic treatment. However, if you aren�t convinced, these five compelling reasons that chiropractic patients should walk are sure to win you over.
5 Benefits Of Walking
Helps With Weight Loss & Weight Management
When you are carrying around excess weight it can lead to back pain and impaired mobility. Fat around your middle, especially in the stomach area, throws your body off balance. There is extra weight in front and it pulls that portion of your body forward, causing a swayback effect.
The pain in the lower back that is caused by this pressure can be excruciating. Over the long term this can cause damage to your spine and cause misalignment. While girdles or slings may help, the permanent remedy is to lose the weight. Walking is an excellent, low impact exercise that helps you lose weight, stay active, and stay healthy.
Improves Mobility & Flexibility
As we age we become less flexible and we don�t have the mobility of youth. As you walk, your circulation increases and that helps improve flexibility and mobility.
Add a little light stretching to the mix, along with regular chiropractic treatments and you will have a much better range of motion. Your posture will improve and you will reduce your chance of injury during physical activity. All this greatly enhances your spinal health making walking a great complement to chiropractic care.
Relieves Back Pain
Back pain is one of the top reasons that Americans miss work and worldwide it is the number one cause of disability. It is also expensive. Each year, Americans spend upwards of $50 billion trying to escape back pain.
Walking is recommended by the American Chiropractic Association (ACA) to help ease back pain. It is a very good, low impact exercise that helps you manage your weight and stay active � excess weight can cause your back to hurt. Walking helps relieve back pain, but it can help to prevent it as well. Even walking for just 30 minutes a day 3 to 5 times a week is beneficial.
Rehydrates Spinal Discs
There are small, fluid filled disks that lie between each vertebrae, acting as a cushion. As you move about during the day, gravity and certain movements cause your spinal disks to compress, squeezing the water out of them. This can lead to back pain and mobility issues.
The increased circulation from walking helps to force water into this area and the disks absorb that water and are rehydrated. This allows them to continue doing what they are supposed to � act as shock absorbers for your spine. It also helps if you drink plenty of water and stay hydrated throughout the day.
Improves Circulation
Good circulation is integral to spinal health as well as a properly functioning central nervous system. When you walk it increases your circulation allowing your blood to carry vital nutrients to your spine, organs, and your entire body. The soft tissues are enriched and nourished as toxins are flushed out.
Another benefit of this increased circulation is a decrease in blood pressure. It brings your body into balance so your muscles, ligaments, and joints are nourished. This, in turn, helps to make your chiropractic treatments more productive and beneficial.
5 benefits of walking is beneficial for whole body wellness. It can help you reduce your risk of many serious health conditions including diabetes, heart attack, stroke, and high blood pressure. It is also great for giving you a mental health boost and make you less prone to osteoporosis. So commit to walking just 30 minutes a day, 3 to 5 days a week. You will be astounded at the difference it will make.
Injury Medical Clinic: Elderly & Geriatric Fitness
Daniel Alvarado, owner of PUSH Fitness, first met Dr. Alex Jimenez through the connection of a good friend and they became workout partners. Daniel Alvarado learned a lot regarding chiropractic alignment and physiology by training with Dr. Jimenez. After experiencing upper and mid back pain as well as shoulder pain, Daniel Alvarado began receiving regular chiropractic care with Dr. Alex Jimenez in order to restore the original alignment of his spine and improve the symptoms of his injury. Daniel Alvarado highly recommends Dr. Jimenez as the non surgical choice for sports injuries, as he discusses how Dr. Alex Jimenez’s relationship with his patients can ensure a positive environment for a better, more improved treatment. Together with Dr. Alex Jimenez’s chiropractic care and his own rehabilitation and sports therapy, Daniel Alvarado emphasizes the dynamic of their services.
Chiropractic Alignment
Sports injuries are injuries which occur in athletic activities or exercising. There are kids and approximately 30 million teens alone that participate in some form of sport. About 3 million sports athletes experience sports injuries annually, which causes some loss of time of participation in the sport. Prevention helps reduce sport injuries. It’s crucial to set up participation in warm-ups and exercises which focus on primary muscle groups utilized in the game of interest. Also, establishing an accident prevention program as a staff, including education on rehydration, nutrition, tracking staff members “in danger”, tracking behavior, skills, and techniques.
Our team has takes great�pride in bringing our families and injured patients only�clinically proven treatments protocols. �By teaching complete holistic wellness as a lifestyle,�we also change not only our patients lives but their families as well.� We do this so that we may reach as many El Pasoans who need us, no matter the affordability issues.
There is no reason we cannot help you.�?
Our uplifting southwest community surrounded by it limitless beauty is an amazing place to live and enjoy our families; it is therefore our mission to help each of our patients to�live,�to�love,�to�matter�and�to�thrive�pain free�in this wonderful special place.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
When you walk, more than 200 individual muscles spring into action which includes all of the muscles in your spine and pelvic area. There�s no denying that walking is good for you and very beneficial to overall health. It is also very effective for spinal health. In most cases, walking is an excellent complement to chiropractic care. Here are 5 good reasons for chiropractic patients to get moving.
Walking Benefits:
Prevents & Relieves Back Pain
The American Chiropractic Association (ACA) recommends walking to help relieve back pain. It is a low impact exercise and very gentle on the back, burning around 265 calories in 30 minutes.
You should avoid walking on uneven terrain or concrete to keep it low impact and avoid injury. Exercise also releases pain relieving endorphins in addition to aiding in other conditions that can relieve pain which includes improving flexibility and mobility, helps rehydrate spinal discs, increases circulation, and aids in weight loss and weight management.
Increases Circulation
Walking increases circulation throughout your body, including your spine. This ensures that you have a continual flow of blood to the muscles and nutrients to the spine. Soft tissues are nourished and enriched while harmful toxins are drained away.
Walking is integral for spinal health. It increases circulation which, in turn, lowers blood pressure. This helps bring the body into balance and increases your stamina. As blood is moved through your body it nourishes all of your muscles, making you stronger and making it easier for you to exercise. Basically, the more you walk, the more you are able to walk.
Improves Flexibility & Mobility
As walking increases circulation, flexibility and mobility are enhanced. When combined with a regimen of light stretching, walking can increase flexibility and a better range of motion. This has the added benefits of reducing the risk of injury and improving posture.
The ACA recommends a series of stretches combined with cardio, including walking, to help with back pain management and good spinal health. It is a very good accompaniment to chiropractic care and is an effective supporting activity which will help your treatment work even better.
Helps Rehydrate Spinal Disks
During the day movement causes compression of your spinal discs, squeezing out the water that fills the discs so they provide a cushion or your vertebrae. The increased circulation that comes from walking also helps to move vital water to the area.
The discs absorb this water, rehydrating them so they can continue to do their job as shock absorbers for the spinal column. This is also a great case for staying well hydrated by drinking lots of water not only while you walk, but also throughout the day.
Aids With Weight Loss & Weight Management
Extra body weight can cause significant stress on the spine. Abdominal fat can create excess weight in the front, causing a swayback effect in the spine. This puts pressure on the lower back, resulting in pain in that area.
The spine is part of the body�s core and the muscles that surround the spine aid in balance and movement. When excess weight is present those muscles become strained as they must work harder to maintain balance. Walking helps with weight management and weight loss eliminating or reducing the effects of excessive weight.
Walking benefits your whole body. It reduces your risk of heart disease, improves blood sugar and blood pressure, reduces your risk of osteoporosis, helps you maintain body weight, improves your mental health, and can even reduce your risk of certain cancers. With your spine at the core of your body, good spinal health plays a part in every one of these conditions. By combining walking with chiropractic care, you are giving your body its best chance at good health and optimal function.
Chiropractic Clinic Extra: Pablo Mena & Son | PUSH-as-Rx ��
In association with professional experience in fitness and chiropractic care,�symptoms of back pain have been determined to improve in people who participate in physical activity and exercise, as directed by a physiotherapist, or physical therapist, or any other healthcare professional, such as a chiropractor. Various complementary and alternative treatment options for back pain also involve the use of functional fitness therapy, however, additional evidence-based research studies on the effectiveness of physical activity and exercise are still needed.
On a personal note, chiropractic care utilizes spinal adjustments and manual manipulations to carefully correct misalignments on the spine, or spinal subluxations. Along with chiropractic treatment, a doctor of chiropractor may also recommend a series of stretches and exercises to help increase flexibility, strength and mobility, improving the overall function of the spine. Physical activity for low back pain has been evaluated in the randomized controlled trial below.
Abstract
Objective
To evaluate effectiveness of an exercise programme in a community setting for patients with low back pain to encourage a return to normal activities.
Design
Randomised controlled trial of progressive exercise programme compared with usual primary care management. Patients� preferences for type of management were elicited independently of randomisation.
Participants
187 patients aged 18-60 years with mechanical low back pain of 4 weeks to 6 months� duration.
Interventions
Exercise classes led by a physiotherapist that included strengthening exercises for all main muscle groups, stretching exercises, relaxation session, and brief education on back care. A cognitive-behavioural approach was used.
Main Outcome Measures
Assessments of debilitating effects of back pain before and after intervention and at 6 months and 1 year later. Measures included Roland disability questionnaire, Aberdeen back pain scale, pain diaries, and use of healthcare services.
Results
At 6 weeks after randomisation, the intervention group improved marginally more than the control group on the disability questionnaire and reported less distressing pain. At 6 months and 1 year, the intervention group showed significantly greater improvement in the disability questionnaire score (mean difference in changes 1.35, 95% confidence interval 0.13 to 2.57). At 1 year, the intervention group also showed significantly greater improvement in the Aberdeen back pain scale (4.44, 1.01 to 7.87) and reported only 378 days off work compared with 607 in the control group. The intervention group used fewer healthcare resources. Outcome was not influenced by patients� preferences.
Conclusions
The exercise class was more clinically effective than traditional general practitioner management, regardless of patient preference, and was cost effective.
Key Messages
Patients with back pain need to return to normal activities as soon as possible but are often afraid that movement or activity may be harmful
An exercise programme led by a physiotherapist in the community and based on cognitive-behavioural principles helped patients to cope better with their pain and function better even one year later
Patients� preferences for type of management did not affect outcome
Patients in the intervention group tended to use fewer healthcare resources and took fewer days off work
This type of exercise programme should be more widely available
Introduction
Low back pain is common and, although it may settle quickly, recurrence rates are about 50% in the following 12 months. Recent management guidelines recommend that an early return to physical activities should be encouraged, but patients are often afraid of movement after an acute onset of back pain. Trials of specific exercise programmes for acute back pain have not shown them to be effective, but a specific exercise programme may have to be tailored to suit the individual patient and so is less likely to be effective for a heterogeneous group of patients.
However, there is some evidence that a general exercise programme, which aims to increase individuals� confidence in the use of their spine and overcome the fear of physical activity, can be effective for patients with chronic back pain (of more than six months� duration). A recent randomised trial of a supervised exercise programme in a hospital setting reported significantly better outcomes at six months and two years for the exercise group compared with the control group. Whether this approach would be effective and cost effective for patients with low back pain of less than six months� duration in a primary care setting is unknown.
An important methodological problem occurs when it is not possible to blind subjects to the treatment they receive, since outcome is probably directly influenced by their preconceived ideas regarding the effectiveness of intervention. Thus, in trials where a double blind procedure is not feasible, participants who are not randomised to their treatment of choice may be disappointed and suffer from resentful demoralisation, whereas those randomised to their preferred treatment may have a better outcome irrespective of the physiological efficacy of the intervention. However, this problem may be partly ameliorated if patients� treatment preferences are elicited before randomisation, so that they can be used to inform the analysis of costs and outcomes.
In this paper, we report a fully randomised trial for the treatment of subacute low back pain in which the analysis was informed by patient preference.
Subjects and Methods
Recruitment of Subjects
Eighty seven general practitioners agreed to participate in the study, and the principal investigator (JKM) visited each practice to discuss participation. Selection of general practitioners was based in the York area and restricted by the need to provide easy access for patients to the classes. Only one invited practice declined to participate. Single handed practices were not invited. The general practitioners referred patients directly to the research team or sent a monthly list of patients who had consulted with back pain. Inclusion criteria were patients with mechanical low back pain of at least four weeks� duration but less than six months, aged between 18 and 60, declared medically fit by their general practitioner to undertake the exercise, and who had consulted one of the general practitioners participating in the study. Patients with any potentially serious pathology were excluded, as were any who would have been unable to attend or participate in the classes. The exclusion criteria were the same as described by Frost et al except that concurrent physiotherapy rather than previous physiotherapy was an exclusion criterion in this trial.
Evaluation
Patients who seemed eligible were contacted by telephone and if they were interested in participating in the study were invited to an initial interview, at which the study and its implications for participants were explained. Patients who met all the eligibility criteria and consented to participate attended a first assessment a week later.
This included a physical examination (to exclude possible serious spinal pathology) and collection of baseline data by means of validated measures of health status. The main outcome measures were the Roland back pain disability questionnaire, which measures functional limitations due to back pain, and the Aberdeen back pain scale, which is more a measure of clinical status. The Roland disability questionnaire consists of a 24 point scale: a patient scoring three points on the scale means that he or she reports, for example, �Because of my back I am not doing any of the jobs that I usually do around the house, I use a handrail to get upstairs, and I lie down to rest more often.� We also administered the EuroQoL health index (EQ-5D) and the fear and avoidance beliefs questionnaire (FABQ).
The second assessment was carried out at the patients� general practice six weeks after randomisation to treatment. The brief physical examination was repeated, and the patients were asked to complete the same outcome questionnaires.
In addition, patients were asked to complete pain diaries in the week before their first assessment and in the week before their second assessment. The diaries were used to assess subjective pain reports and asked �How strong is the pain?� and �How distressing is the pain?�
We also evaluated patients at six and 12 months� follow up by sending them outcome questionnaires to complete and return.
Randomisation and Treatments
A pre-prepared randomisation list was generated from a random numbers table and participants were stratified by practice in blocks of six. The trial coordinator ensured concealment of allocation from the clinical researchers by providing the research physiotherapist with a sealed envelope for a named patient before baseline assessment. A note inside the envelope invited the participant either to attend exercise classes or to continue with the current advice or treatment offered by his or her general practitioner. (One of the referring general practitioners used manipulation as usual treatment on most of his patients so that up to 37 patients in each arm of the study could also have received manipulation.) Each patient had an equal chance of being allocated to the intervention or the control group. Before patients were given their envelope they were asked whether they had any preference for the treatment assignment. The participants opened the envelope after leaving the surgery.
Intervention group�The exercise programme consisted of eight sessions, each lasting an hour, spread out over four weeks, with up to 10 participants in each class. The programme was similar to the Oxford fitness programme and included stretching exercises, low impact aerobic exercises, and strengthening exercises aimed at all the main muscle groups. The overall aim was to encourage normal movement of the spine. No special equipment was needed. Participants were discouraged from viewing themselves as invalids and from following the precept of �Let pain be your guide.� They were encouraged to improve their individual record and were selectively rewarded with attention and praise. Although partly based on a traditional physiotherapy approach, the programme used cognitive-behavioural principles. One simple educational message encouraging self reliance was delivered at each class. Participants were told that they should regard the classes as a stepping stone to increasing their own levels of activity.
Controls�Patients allocated to the control group continued under the care of their doctor and in some cases were referred to physiotherapy as usual. No attempt was made to regulate the treatment they received, but it was recorded.
Economic Analysis
We recorded patients� use of healthcare services using a combination of retrospective questionnaires and prospective diary cards, which they returned at 6 and 12 months� follow up. From this information we estimated the cost of each patient�s treatment. We compared the mean costs of treatment for the two groups by using Student�s t tests and standard confidence intervals. However, as cost data were highly positively skewed, these results were checked with a non-parametric �bootstrap.� The economic evaluation addressed both costs to the NHS and the costs to society. Participants were not charged for the classes, in line with any treatment currently available on the NHS.
Statistical Analysis
Our original intention was to recruit 300 patients, which, given a standard deviation of 4, would have provided 90% power at the 5% significance level to detect a 1.5 point difference between the two groups in the mean change on the Roland disability questionnaire. However, recruitment of patients to the study proved much slower than expected, and, because of the limitations of study resources, recruiting was stopped after 187 patients had been included into the study. This smaller sample reduced the power to detect such a difference to 72%, but there was still 90% power to detect a 2 point difference in outcome.
Our analysis was based on intention to treat. We estimated the effects of treatment on the outcome measures by means of analysis of covariance, with the change in scores as the dependent variable and adjustment being made for baseline score and patient preference. We used Student�s t tests to analyse the data from the pain diaries as the baseline scores were quite similar.
Dr. Alex Jimenez’s Insight
In consideration with the research study regarding a randomized controlled trial coordinated to determine the effectiveness of functional fitness towards the improvement of low back pain, we supplement our philosophies of overall health and wellness to our patients and we make sure to take their recovery and rehabilitation to the next level. Our fitness and chiropractic care treatment goes beyond many other medically advanced methods. The proprietary treatment methods offered at our clinic promote true well-being and fitness practices with a primary goal on the calibration of the human body. The outcome measures of the randomized controlled trial on exercise for low back pain involved two groups of participants, an intervention group and a control group. The results are recorded below.
Results
Study Population
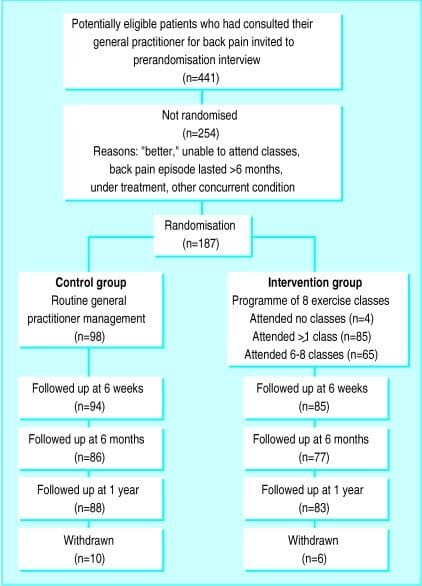
Of the 187 patients included in the trial, 89 were randomised to the intervention and 98 to the control group. The figure shows their progress through the trial. In both groups those with the most severe back pain at randomisation were less likely to return follow up questionnaires: the mean Roland disability questionnaire score for responders at one year follow up was 5.80 (SD 3.48) compared with a mean score of 9.06 (4.58) for non responders respectively (P=0.002).
Baseline Characteristics
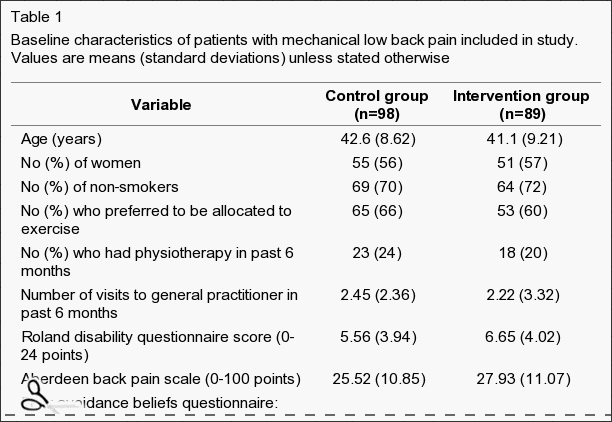
The clinical and demographic characteristics of the patients in the two groups were fairly well balanced at randomisation (Table 1), although those allocated to the intervention group tended to report more disability on the Roland disability questionnaire than did the control group. Most patients (118, 63%), when asked, would have preferred to be allocated to the exercise programme. Attendance of the classes was considered quite good, with 73% of the intervention group attending between six and eight of the classes. Four people failed to attend any classes and were included in the intention to treat analysis. No patients allocated to the control group took part in the exercise programme.
Table 1: Baseline characteristics of patients with mechanical low back pain included in study. Values are means (standard deviations) unless stated otherwise.
Clinical Outcomes
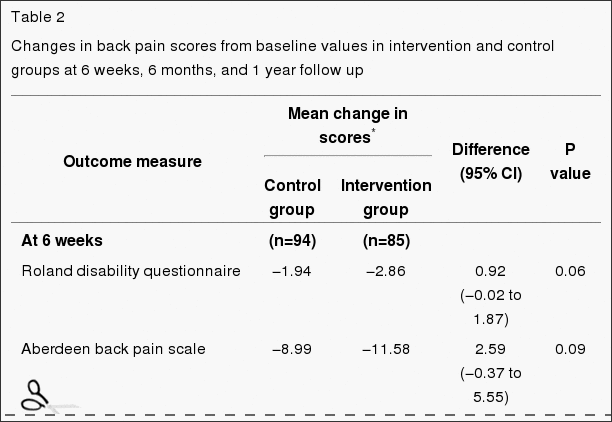
Table ?2 shows the mean changes in outcome measures over time, from randomisation to final follow up at one year. After adjustment for baseline scores, the intervention group showed greater decreases in all measures of back pain and disability compared with the controls. At six weeks after randomisation, patients in the intervention group reported less distressing pain than the control group (P=0.03) and a marginally significant difference on the Roland disability questionnaire scores. Other variables were not significantly different, but the differences in change were all in favour of the intervention group. At six months the difference of the mean change scores of the Roland disability questionnaire was significant, and at one year the differences in changes of both the Roland disability questionnaire and the Aberdeen back pain scale were significant (Table ?2). Most of the intervention group improved by at least three points on the Roland disability questionnaire: 53% (95% confidence interval 42% to 64%) had done so at six weeks, 60% (49% to 71%) at six months, and 64% (54% to 74%) at one year. A smaller proportion of the control group achieved this clinically important improvement: 31% (22% to 40%) at six weeks, 40% (29% to 50%) at six months, and 35% (25% to 45%) at one year.
Table 2: Changes in back pain scores from baseline values in intervention and control groups at 6 weeks, 6 months, and 1 year follow up.
Patients� Preference
We examined the effect of patients� baseline preference for treatment on outcome after adjusting for baseline scores and main effects. Preference did not significantly affect response to treatment. The intervention had similar effects on both costs and outcomes regardless of baseline preference. For example, the change in the Roland disability questionnaire score at 12 months in the control group was ?1.93 for patients who preferred intervention and ?1.18 for those who were indifferent (95% confidence interval of difference ?1.05 to 2.55), and in the intervention group the change in score was ?3.10 for those who preferred intervention and ?3.15 for those who were indifferent ((95% confidence interval of difference ?1.47 to 3.08). As the interaction term (preference by random allocation) was non-significant, the results shown in Table ?2 exclude the preference term.
Economic Evaluation
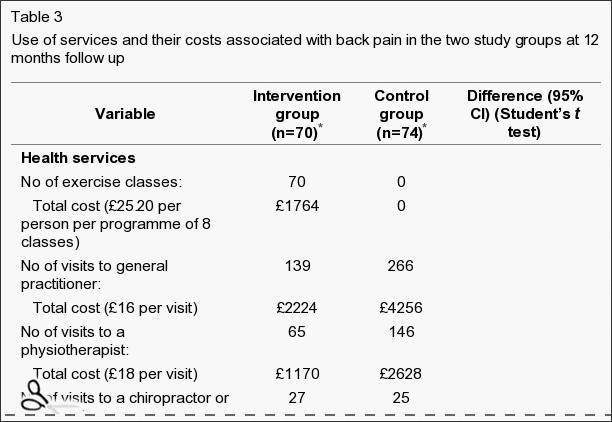
Patients in the intervention group tended to use fewer healthcare and other resources compared with those in the control group (Table ?3). However, the mean difference, totalling �148 per patient, was not significant: the 95% confidence interval suggests there could have been a saving of as much as �442 per patient in the intervention group or an additional cost of up to �146. Patients in the control group took a total of 607 days off work during the 12 months after randomisation compared with 378 days taken off by the intervention group.
Table 3: Use of services and their costs associated with back pain in the two study groups at 12 months follow up.
Discussion
Our results support the hypothesis that a simple exercise class can lead to long term improvements for back pain sufferers. Studies have shown that a similar programme for patients with chronic back pain can be effective in the hospital setting. In this study we show the clinical effectiveness for patients with subacute or recurrent low back pain who were referred by their general practitioner to a community programme.
Current management guidelines for low back pain recommend a return to physical activity and taking exercise. In particular, they recommend that patients who are not improving at six weeks after onset of back pain, which may be a higher proportion than previously realised, should be referred to a reactivation programme. The programme we evaluated fits that requirement well. It shows participants how they can safely start moving again and increase their levels of physical activity. It is simple and less costly than individual treatment.
It seemed to have beneficial effects even one year later, as measured by functional disability (Roland disability questionnaire) and clinical status (Aberdeen back pain scale). The mean changes in scores on these instruments were small, with many patients reporting mild symptoms on the day of entry to the trial. However, a substantially larger proportion of participants in the exercise classes gained increases of over three points on the Roland disability questionnaire at six weeks, six months, and one year, which might be clinically important. At six weeks, participants in the exercise classes reported significantly less distressing pain compared with the control group, although the intensity of pain was not significantly different. This is consistent with findings from a study of chronic back pain patients in Oxford, in which changes in distressing pain were much greater than were the changes in intensity of pain.
People with back pain who use coping strategies that do not avoid movement and pain have less disability. In our study the participants in the exercise classes were able to function better according to Roland disability questionnaire scores than the control group at six months and one year after randomisation to treatment, and at one year they also showed a significantly greater improvement in clinical status as measured by the Aberdeen back pain scale. This increase in differences in effect between the intervention and control groups over time is consistent with the results from long term follow up in comparable back pain trials.
Study Design
The design of this study was a conventional randomised controlled trial in that all eligible patients were randomised. However, the participants were asked to state their preferred treatment before they knew of their allocation. A study of antenatal services showed that preferences can be an important determinant of outcome, but we did not find any strong effect of preference on the outcome, although a much larger sample size would be needed to confidently exclude any modest interaction between preference and outcome. This information may be useful to clinicians in that it suggests that exercise classes are effective even in patients who are not highly motivated. Our trial design, of asking patients for their preferences at the outset, has substantial advantages over the usual patient preference design, in which costs and outcomes cannot be reliably controlled for confounding by preference.
Conclusions
Our exercise programme did not seem to influence the intensity of pain but did affect the participants� ability to cope with the pain in the short term and even more so in the longer term. It used a cognitive-behavioural model, shifting the emphasis away from a disease model to a model of normal human behaviour, and with minimal extra training a physiotherapist can run it. Patients� preferences did not seem to influence the outcome.
Figure 1: Flow chart describing patients’ progress through the trial.
Footnotes
Funding: This research was funded by the Arthritis Research Campaign, the Northern and Yorkshire Regional Health Authority, and the National Back Pain Association.
Competing interests: None declared.
In conclusion,�the participation of patients in functional fitness and/or exercise as recommended by a physiotherapist, or physical therapist, or any other healthcare professional, such as a chiropractor, is essential towards the improvement of their symptoms of low back pain. The exercise programme helped patients better cope with their symptoms of back pain where the intervention group showed that they used fewer healthcare resources and took fewer day off work, according to the outcome measures of the research study. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
3.�Waddell G, Feder G, McIntosh A, Lewis M, Hutchinson A.�Low back pain evidence review.�London: Royal College of General Practitioners; 1996.
4.�Malmivaara A, Hakkinen U, Aro T, Heinrichs M, Koskenniemi L, Kuosma E, et al. The treatment of acute low back pain�bed rest, exercises or ordinary activity?�N Engl J Med.�1995;332:351�355.[PubMed]
5.�Faas A, Chavannes A, van Eijk JTM, Gubbels J. A randomized, placebo-controlled trial of exercise therapy in patients with acute low back pain.�Spine.�1993;18:1388�1395.�[PubMed]
6.�Frost H, Klaber Moffett J, Moser J, Fairbank J. Evaluation of a fitness programme for patients with chronic low back pain.�BMJ.�1995;310:151�154.�[PMC free article]�[PubMed]
7.�Frost H, Lamb S, Klaber Moffett J, Fairbank J, Moser J. A fitness programme for patients with chronic low back pain: 2 year follow-up of a randomised controlled trial.�Pain.�1998;75:273�279.�[PubMed]
8.�McPherson K, Britton A, Wennberg J. Are randomised controlled trials controlled? Patient preferences and unblind trials.�J R Soc Med.�1997;90:652�656.�[PMC free article]�[PubMed]
9.�Bradley C. Designing medical and educational studies.�Diabetes Care.�1993;16:509�518.�[PubMed]
10.�Clement S, Sikorski J, Wilson J, Candy B. Merits of alternative strategies for incorporating patient preferences into clinical trials must be considered carefully [letter]�BMJ.�1998;317:78.�[PubMed]
11.�Torgerson D, Klaber Moffett J, Russell I. Patient preferences in randomised trials: threat or opportunity?�J Health Serv Res Policy.�1996;1(4):194�197.�[PubMed]
12.�Roland M, Morris R. A study of the natural causes of back pain. Part 1: Development of a reliable and sensitive measure of disability in low-back pain.�Spine.�1983;8:141�144.�[PubMed]
13.�Ruta D, Garratt A, Wardlaw D, Russell I. Developing a valid and reliable measure of health outcome for patients with low back pain.�Spine.�1994;19:1887�1896.�[PubMed]
14.�Brooks R.with EuroQoL Group.�EuroQoL: the current state of play�Health Policy�19963753�72.[PubMed]
15.�Waddell G, Newton M, Henderson I, Somerville D, Main C. A fear-avoidance beliefs questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability.�Pain.�1993;52:157�168.�[PubMed]
16.�Jensen M, McFarland C. Increasing the reliability and validity of pain intensity measurement in chronic pain patients.�Pain.�1993;55:195�203.�[PubMed]
17.�Efron B, Tibshirani R.�An introduction to bootstrap.�New York: Chapman and Hall; 1993.
18.�Williams D, Keefe F. Pain beliefs and use of cognitive-behavioral coping strategies.�Pain.�1991;46:185�190.�[PubMed]
19.�Estlander A, Harkapaa K. Relationships between coping strategies, disability and pain levels in patients with chronic low back pain.�Scand J Behav Ther.�1989;18:56�69.
20.�Holmes J, Stevenson C. Differential effects of avoidant and attentional coping strategies on adaption to chronic and recent-onset pain.�Health Psychology.�1990;9:577�584.�[PubMed]
21.�Rosenstiel A, Keefe F. The use of coping strategies in chronic low back pain patients: relationship to patient characteristics and current adjustments.�Pain.�1983;17:33�44.�[PubMed]
22.�Slade P, Troup J, Lethem J, Bentley G. The fear avoidance model of exaggerated pain perception II Preliminary studies of coping strategies for pain.�Behav Res Ther.�1983;21:409�416.�[PubMed]
23.�Meade T, Dyer S, Browne W, Frank A. Randomised comparison of chiropractic and hospital outpatient management for low back pain: results from extended follow up.�BMJ.�1995;311:349�351.[PMC free article]�[PubMed]
24.�Cherkin D, Deyo R, Battie M, Street J, Barlow W. A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain.�N Engl J Med.�1998;339:1021�1029.�[PubMed]
Chiropractic care is designed to alleviate pain and restore the body to its natural balance. For chiropractors, injury prevention is key for a healthy body. Good practices combined with solid exercises creates toned muscles that protect the body and spine from harm. While each patient receives exercise instructions for their specific condition, the following exercise tips for chiropractic patients apply to everyone.
Take Time To Warm Up Before You Exercise
Before starting any exercises, it’s important to warm up. A series of dynamic moves will boost your heart rate and heat up the muscles that you will be using during your work out.
Select whole body movements such as leg lunges paired with arm motion or walk in place while raising and lowering your arms. Once you’ve warmed up, you can safely stretch without risk of injury.
Introduce Ergonomics Into Your Home And Work Space
One of the most important exercise tips for chiropractic patients is to take steps to keep your body in alignment as you move through your day. In the workplace, check with an ergonomics consultant to ensure proper positioning, especially if you spend most of the day seated or doing repetitive tasks.
A comfortable chair reduces muscle strain and prevents injury. Make sure that your feet sit firmly on the floor and that lumbar support is in place. At home, you should have a good mattress and supportive furniture.
Choose The Right Shoes
Before you buy your next pair of shoes, check for stability, flexibility, and comfort. During your test drive, make sure that the shoes feel firmly in place as you move through your entire range of motion for a stable gait during wear.
Footwear should be flexible enough to give easily at the base of the toe for a smooth gait, and there should be cushioning at all the right places with plenty of room for the toes to move. Shoes that properly fit your feet means that your walk will be more natural and healthy during exercise and in daily motion.
Sit And Stand With Posture In Mind
Perhaps the biggest reason that these exercise tips for chiropractic patients are so important is that strong and flexible muscles will help you have good posture. Be mindful of the following as you move through your day:
When sitting, your feet should be on the floor, your shoulders should be relaxed, and your forearms should remain parallel with the ground.
If you will be standing for a time, make sure that you maintain posture by tucking your stomach muscles in.
When standing for an especially long period of time, be sure to shift your weight from one foot to the other and from the heels to the toes and back again.
These simple tips for maintaining good posture will passively work your muscles and result in a healthier spine.
Passive Stretches For Large Muscles
Finally, it is important to target large muscle groups with passive exercises. Use your weight to slowly stretch your hamstrings, your piriformis, and your entire back. Passive stretching is gentle and relieves stress points that cause back pain. These gentle exercises provide a great deal of relief and are easily adjusted to suit your current ability.
Your chiropractor will work with you to design an exercise program that is optimal for you. Be sure to follow through with the plan and include these tips in your regular work out to experience the joy of healing from chiropractic care.
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
The thyroid gland may be small but it plays a big role in how well your body functions. That is because the thyroid produces a hormone that regulates your metabolism, the process which converts everything you drink and eat into energy. However, when your metabolism slows, causing you to lose weight and feel sluggish and fatigued, you may have an underactive thyroid, medically referred to as hypothyroidism.
How can hypothyroidism affect your body?
Decreased levels of the thyroid hormone can lead to an increase in LDL cholesterol, or fat, in your blood. The thyroid hormone helps the liver break down the cholesterol circulating in your blood and stimulates. Triglycerides and your LDL cholesterol may substantially increase whenever you don’t have enough of the thyroid hormone. What’s more, hypothyroidism may also negatively affect your mood. The thyroid gland helps regulate the chemical messengers, or neurotransmitters, which your brain utilizes to communicate with your own nerves. These messengers can go haywire, causing one to feel anxious and depressed when your thyroid doesn’t function properly.
“The most important thing that you can do for hypothyroidism is to see your doctor and get on the right dose of thyroid hormone,” says R. Mack Harrell, MD, president-elect of the American Association of Clinical Endocrinologists and an endocrinologist at Memorial Regional Hospital in Hollywood, Fla..
Visiting your local healthcare professional’s office is a fundamental first step towards diagnosing and treating an underactive thyroid, or hypothyroidism, but what can you do to help yourself? Add exercise on your list. Regular exercise is an important part of your overall strategy to manage hypothyroidism symptoms. Exercise can offset the effects of your sluggish metabolism and burns calories to prevent weight gain. A good fitness routine may be a mood-booster as well because while you exercise, your body releases endorphins and other substances.
The Hypothyroidism-Exercise Link
What is the best type of exercise for hypothyroidism? A program of high heeled aerobic exercises and strength training is recommended by Yaroslav Gofnung, MD, an endocrinologist at Los Robles Hospital in Thousand Oaks, Calif.. Low-impact aerobics get your heart rate up and your lungs moving without putting too much strain on your joints, which can be vital because joint pain is another common hypothyroidism symptom, Dr. Gofnung says.
A stationary reclining or recumbent bicycle and a low-impact elliptical machine are exceptional machine choices for cardio exercise. “Walking is a fantastic exercise too, as long as you don’t have swelling in your knees or ankles,” Gofnung adds. Additionally, Pilates or gentle yoga may improve core muscles and alleviate the spine and hip pain which could be associated with hypothyroidism.
Individuals with hypothyroidism can also benefit from strength training exercises, such as lunges, leg lifts, and push-ups while other people may benefit from other strength training exercises involving weight-training machines. Strength training builds muscle mass, and muscle burns more calories even when you’re at rest. Building muscle can help prevent potential weight gain from an underactive thyroid gland.
The Best Exercises for Hypothyroidism
For people with hypothyroidism, Igor Klibanov, a personal coach in Toronto, founder of Fitness Solutions Plus, and also writer of “Unlimited Progress: The Way To Unlock Your Body’s Potential,” recommends cardio along with a strength-training routine that incorporates these six exercises:
One-legged dead lift: Stand on one leg while holding onto something for balance (not for support). Keep one hand relaxed in front of your thighs. Push on your hips up as far as you can, until your hand touches the ground. Come back up. This ought to be felt at the buttocks muscles. The back shouldn’t curve; but does not have to be upright.
Squats: Stand up straight and then bend at your knees and hips till you are at a sitting position. Go all of the way down. (Klibanov says it’s a myth that this may damage your knees if you have healthy knees to start with.) .
Overhead press or comparable vertical push movement. Boost a set of dumbbells to shoulder height. So they are facing forward switch your arms. Lift up the dumbbells until your elbows are right. Then lower them back down.
Lat pull-down or similar vertical pull move. Catch a pull-down bar with an overhand grip (palms facing away), and pull it down into your collar bone. Make certain that that the bar travels near to your face as you can.
Push-up or comparable horizontal push movement. Place both hands on the floor, shoulder width apart. Feet must be extended out and together. Till you are close to the ground, Bend your elbows and shoulders. In case a push is too hard, do the same thing either together with your hands on a table (while feet stay on the ground) or a wall socket.
Rowing or similar horizontal pull move. Sit with your hands holding the grip that’s connected to the cable. Keep your back straight, and lean back about 10 to15 degrees. Pull on back the cable until your mid-stomach touches. Then release under control.
Start with 15 repetitions of each exercise and work up to around 20. “Most people with joint issues find these to be easy on the joints,” Klibanov says. When you’re starting out, it might take you 15 to 20 minutes to finish your routine. A eventual aim: Work up which should take about 40 to 45 minutes, he adds. Schedule aerobic exercise a few times a week and participate in strength training routines with these motions two to three days weekly, Klibanov recommends. Doing this can get you on the ideal track to feeling better and losing weight.
Ease Into Exercise
Start slowly and build up. “If you go too quickly, it is possible to injure yourself and set yourself back,” Gofnung warns. Choose exercises that you enjoy and that your body is able to tolerate to increase the probability of your sticking to your regular, ” he advises.
Adjust the number of repetitions as you progress. “In just two weeks, you’ll have another body and you should have a different pattern,” Klibanov states. And do not be timid about progressing, he adds, “The further out of shape you are, the faster progress will come.”
If something hurts, you may have to make a small change like the angle or position of an exercise or motion. If it hurts, stop and find another exercise that does not cause discomfort. If you’re having difficulty by yourself, invest with a trainer that will make recommendations in time and explain to you how you can lose weight through the exercises you select.
Always talk with your doctor before beginning any exercise regimen. And never make exercise a substitute for thyroid drugs. With the right medication, you should feel better within a few weeks and have the motivation to get back to (or get into) a regular exercise regimen, Dr. Harrell says.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

 Chiropractic For Cycling Injuries
Chiropractic For Cycling Injuries
 Relieves Back Pain
Relieves Back Pain