Occlusion training involves restricting the flow of blood to a muscle group while training. That is why it is also commonly called �blood flow restriction training.�
Basically you take a wrap or band and apply it to the top of your limb.
The aim of this�isn�t�to completely cut off circulation to the area as that is dangerous and painful.
This means that you aren�t restricting arterial flow to the area, but you are restricting the venous return from the muscles.
Arteries are what takes the blood from your heart to your muscles and it is then returned to your heart through a system of veins.
Restricting the blood flow back to your heart causes a pooling of the blood in the area that you are working.
This is what occlusion training uses to create an�anabolic effect�on your muscles.�
HOW DOES OCCLUSION TRAINING WORK?
The bloodstream is the network that connects the muscles in your body, providing oxygen and nutrients and carrying away waste products
Muscles require a steady flow of blood to operate.
That is why we aren�t cutting off the flow to the muscle, we are only slowing the rate at which the blood releases from it.
When performing any kind of resistance training your body directs more blood to your muscles performing the exercise.
The reason you get a �pump� when working out is that the speed at which your body is pumping blood into your muscles is faster than the amount of blood going out of them.
Your pump reduces when you rest between your sets as more blood is released from your muscle groups.
Blood flow restriction training prolongs and intensifies your pump.
This is done by placing wraps in one of two places during your working sets.
You wrap above your bicep for movements that involve your bicep�s, triceps, forearms, and even chest and back can benefit from this.
While wrapping in this position it makes sense that it would benefit your arms but how does it help your chest and back?
There is no possible way that you can restrict blood flow to your chest and back because of the positions they are located in.
However wrapping your arm allows you to pre-fatigue your arms and as a result chest and back exercises that you perform are going to require more involvement from those muscles rather than your biceps or triceps.
Wrap your upper thigh for movements that involve your quads, hamstrings, glutes and calves.
Building Muscle With Occlusion Training
During training you have two�types of muscle�that are responsible for all muscle growth in the gym.
Fast twitch fibers and slow twitch fibers.
Slow twitch muscle fibers are smaller muscle fibers and generate less power and strength than fast twitch fibers. However slow twitch fibers fatigue slower and can sustain activity for longer.
Fast twitch fibers are larger muscle fibers, generate more power and strength and have the most potential for growth.
Fast twitch fibers are recruited last during contractions and mostly don�t use oxygen. Slow twitch fibers on the other hand use oxygen and are recruited first in the movement.
This means that by restricting the blood flow to a muscle group you are pre-fatiguing the slow twitch fibers and forcing the fast twitch fibers to take control even when you�re using low weights.
Occlusion training seems to�trick your body�into thinking you are lifting heavy weights. This means you can get very�similar benefits�of heavy training by using 20-30% of your 1 rep max.
There are two main factors that lead to muscle growth during training. These are:
Metabolic Stress
Cellular Swelling
Metabolic Stress
When you�re working out your body is burning energy. As your body chews through its fuel stores, metabolic by-product accumulates in your muscles.
Metabolic by-products act as an anabolic signal, telling your body to increase size and strength.
Under normal training most of these by-products would be washed out by blood flow.
Occlusion training keeps them near the muscle helping to increase the anabolic effect that the by-products have on the muscles.�
Cellular Swelling
During resistance training your cells expand and fill with fluid and nutrients. This is known as cellular swelling and has also been shown to be an anabolic�signal for muscle growth.
Occlusion training isn�t a better option than heavy training, but that said it is a nice supplement.
Regularly pushing your muscles to the point of failure or at least close to it (1-2 reps) is an important factor of increasing your strength and muscle mass.
Occlusion training allows you to replicate this without putting anywhere near as much strain on your joints, ligaments and tendons as you would to get the same result from lifting heavy.
This means that you can do more volume without the risk of�overtraining.
Here are a couple of scenarios where this could be really beneficial for you:
If you suffer from joint issues
If you�re travelling and only have access to hotel weights
If you�re injured or have nagging aches and pains.
In short your body might not always feel up to another heavy training day. Occlusion training can be a great way to get a good workout in and help you maintain muscle mass.�
How To Do Blood Flow Restriction Training
As I mentioned earlier you only ever wrap yourself at the top of your biceps and the top of your thighs.
Elastic knee wraps, medical tourniquets and exercise band �are good options to use for your wraps.
Here�s two videos explaining how to wrap your arms and legs
Blood flow restriction training works best when with isolation exercises. If you are going to do compound movements do them at the start of your workout and save the blood flow restricted exercises for the end.
Layne Norton recommends performing lifts at 20%-30% of your 1rm for 20-30 reps of the first set and then the next three sets at 10-15 reps. Have a 30 second rest between sets before going again.
You want to keep the cuffs on your limbs for the entire 4 sets and then release them at the end.
If you�re in pain before the exercise starts that�s a good sign that your wraps are too tight.
Also if you can�t complete the prescribed sets either the wraps are too tight or the weight is too heavy.�
Conclusion
Blood flow restriction training has been getting a lot of hype lately.
While it isn�t better than regular strength training, it is a good supplement for it and can be beneficial when used in conjunction with your regular training.
This is more of an advanced training technique so if you are just starting out lifting it probably won�t give you any more benefits than your normal heavy training.
If you�re an advanced lifter, are injured, or don�t have access to heavier weights than this training technique could benefit you.
Even though the effects of overweight and obesity on diabetes, cardiovascular disease, all-cause mortality, and other health outcomes are widely known, there is less awareness that overweight, obesity, and weight gain are associated with an increased risk of certain cancers. A recent review of more than 1000 studies concluded that sufficient evidence existed to link weight gain, overweight, and obesity with 13 cancers, including adenocarcinoma of the esophagus; cancers of the gastric cardia, colon and rectum, liver, gallbladder, pancreas, corpus uteri, ovary, kidney, and thyroid; postmenopausal female breast cancer; meningioma; and multiple myeloma.1�An 18-year follow-up of almost 93?000 women in the Nurses� Health Study revealed a dose-response association of weight gain and obesity with several cancers.2
Obesity Increase
The prevalence of obesity in the United States has been increasing for almost 50 years. Currently, more than two-thirds of adults and almost one-third of children and adolescents are overweight or obese. Youths who are obese are more likely to be obese as adults, compounding their risk for health consequences such as cardiovascular disease, diabetes, and cancer. Trends in many of the health consequences of overweight and obesity (such as type 2 diabetes and coronary heart disease) also are increasing, coinciding with prior trends in rates of obesity. Furthermore, the sequelae of these diseases are related to the severity of obesity in a dose-response fashion.2�It is therefore not surprising that obesity accounts for a significant portion of health care costs.
Cancers
A report released on October 3, 2017, by the US Centers for Disease Control and Prevention assessed the incidence of the 13 cancers associated with overweight and obesity in 2014 and the trends in these cancers over the 10-year period from 2005 to 2014.3�In 2014, more than 630?000 people were diagnosed as having a cancer associated with overweight and obesity, comprising more than 55% of all cancers diagnosed among women and 24% of cancers among men. Most notable was the finding that cancers related to overweight and obesity were increasingly diagnosed among younger people.
From 2005 to 2014, there was a 1.4% annual increase in cancers related to overweight and obesity among individuals aged 20 to 49 years and a 0.4% increase in these cancers among individuals aged 50 to 64 years. For example, if cancer rates had stayed the same in 2014 as they were in 2005, there would have been 43?000 fewer cases of colorectal cancer but 33?000 more cases of other cancers related to overweight and obesity. Nearly half of all cancers in people younger than 65 years were associated with overweight and obesity. Overweight and obesity among younger people may exact a toll on individuals� health earlier in their lifetimes.2�Given the time lag between exposure to cancer risk factors and cancer diagnosis, the high prevalence of overweight and obesity among adults, children, and adolescents may forecast additional increases in the incidence of cancers related to overweight and obesity.
Clinical Intervention
Since the release of the landmark 1964 surgeon general�s report on the health consequences of smoking, clinicians have counseled their patients to avoid tobacco and on methods to quit and provided referrals to effective programs to reduce their risk of chronic diseases including cancer. These efforts, coupled with comprehensive public health and policy approaches to reduce tobacco use, have been effective�cigarette smoking is at an all-time low. Similar efforts are warranted to prevent excessive weight gain and treat children, adolescents, and adults who are overweight or obese. Clinician referral to intense, multicomponent behavioral intervention programs to help patients with obesity lose weight can be an important starting point in improving a patient�s health and preventing diseases associatedwith obesity. The benefits of maintaining a healthy weight throughout life include improvements in a wide variety of health outcomes, including cancer. There is emerging but very preliminary data that some of these cancer benefits may be achieved following weight loss among people with overweight or obesity.4
The US Preventive Services Task Force (USPSTF)
The US Preventive Services Task Force (USPSTF) recommends screening for obesity and intensive behavioral interventions delivered over 12 to 16 visits for adults and 26 or more visits for children and adolescents with obesity.5,6�Measuring patients� weight, height, and body mass index (BMI), consistent with USPSTF recommendations, and counseling patients about maintaining a healthy weight can establish a foundation for preventive care in clinical care settings. Scientific data continue to emerge about the negative health effects of weight gain, including an increased risk of cancer.1�Tracking patients� weight over time can identify those who could benefit from counseling and referral early and help them avoid additional weight gain. Yet less than half of primary care physicians regularly assess the BMI of their adult, child, and adolescent patients. Encouraging discussions about weight management in multiple health care settings, including physicians� offices, clinics, emergency departments, and hospitals, can provide multiple opportunities for patients and reinforce messages across contexts and care environments.
Weight Loss Programs
Implementation of clinical interventions, including screening, counseling, and referral, has major challenges. Since 2011, Medicare has covered behavioral counseling sessions for weight loss in primary care settings. However, the benefit has not been widely utilized.7�Whether the lack of utilization is a consequence of lack of clinician or patient knowledge or for other reasons remains uncertain. Few medical schools and residency programs provide adequate training in prevention and management of obesity or in understanding how to make referrals to such services. Obesity is a highly stigmatized condition; many clinicians find it difficult to initiate a conversation about obesity with patients, and some may inadvertently use alienating language when they do. Studies indicate that patients with obesity prefer the use of terms such as�unhealthy weight�or�increased BMI�rather than�overweight�or�obesity�and�improved nutrition and physical activity�rather than�diet and exercise.8�However, it is unknown if switching to these terms will lead to more effective behavioral counseling. Effective clinical decision support tools to measure BMI and guide physicians through referral and counseling interventions can provide clinicians needed support within the patient-clinician encounter. Inclusion of recently developed competencies for prevention and management of obesity into the curricula of health care professionals may improve their ability to deliver effective care. Because few primary care clinicians are trained in behavior change strategies like cognitive behavioral therapy or motivational interviewing, other trained health care professionals, such as nurses, pharmacists, psychologists, and dietitians could assist by providing counseling and appropriate referrals and help people manage their own health.
Achieving sustainable weight loss requires comprehensive strategies that support patients� efforts to make significant lifestyle changes. The availability of clinical and community programs and services to which to refer patients is critically important. Although such programs are available in some communities, there are gaps in availability. Furthermore, even when these programs are available, enhancing linkages between clinical and community care could improve patients� access. Linking community obesity prevention, weight management, and physical activity programs with clinical services can connect people to valuable prevention and intervention resources in the communities where they live, work, and play. Such linkages can give individuals the encouragement they need for the lifestyle changes that maintain or improve their health.
The high prevalence of overweight and obesity in the United States will continue to contribute to increases in health consequences related to obesity, including cancer. Nonetheless, cancer is not inevitable; it is possible that many cancers related to overweight and obesity could be prevented, and physicians have an important responsibility in educating patients and supporting patients� efforts to lead healthy lifestyles. It is important for all health care professionals to emphasize that along with quitting or avoiding tobacco, achieving and maintaining a healthy weight are also important for reducing the risk of cancer.
Corresponding Author:�Greta M. Massetti, PhD, Centers for Disease Control and Prevention, 4770 Buford Hwy NE, Atlanta, GA 30341 (gmassetti@cdc.gov).
Conflict of Interest Disclosures:�All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflict of Interest. Dr Dietz reports receipt of scientific advisory board fees from Weight Watchers and consulting fees from RTI. No other disclosures were reported.
Disclaimer:�The findings and conclusions in this report are those of the authors and not necessarily the official position of the Centers for Disease Control and Prevention.
References
1. Lauby-Secretan B, Scoccianti C, Loomis D, Grosse Y, Bianchini F, Straif K; International Agency for Research on Cancer Handbook Working Group. Body fatness and cancer�viewpoint of the IARC Working Group. N Engl J Med. 2016;375(8):794-798. PubMedArticle
2. Zheng Y, Manson JE, Yuan C, et al. Associations of weight gain from early to middle adulthood with major health outcomes later in life. JAMA. 2017;318(3):255-269. PubMedArticle
4. Byers T, Sedjo RL. Does intentional weight loss reduce cancer risk? Diabetes Obes Metab. 2011;13(12):1063-1072. PubMedArticle
5. Grossman DC, Bibbins-Domingo K, Curry SJ, et al; US Preventive Services Task Force. Screening for obesity in children and adolescents: US Preventive Services Task Force recommendation statement. JAMA. 2017;317(23):2417-2426. PubMedArticle
7. Batsis JA, Bynum JPW. Uptake of the centers for Medicare and Medicaid obesity benefit: 2012-2013. Obesity (Silver Spring). 2016;24(9):1983-1988. PubMedArticle
8. Puhl R, Peterson JL, Luedicke J. Motivating or stigmatizing? public perceptions of weight-related language used by health providers. Int J Obes (Lond). 2013;37(4):612-619. PubMedArticle
Science based Chiropractor Dr. Alexander Jimenez takes a look at oxidative stress, what it is, how it affects the body and the antioxidant defense to remedy the situation.
Esra Birben PhD,1 Umit Murat Sahiner MD,1 Cansin Sackesen MD,1 Serpil Erzurum MD,2 and Omer Kalayci, MD1
Abstract: Reactive oxygen species (ROS) are produced by living organisms as a result of normal cellular metabolism and environ- mental factors, such as air pollutants or cigarette smoke. ROS are highly reactive molecules and can damage cell structures such as carbohydrates, nucleic acids, lipids, and proteins and alter their functions. The shift in the balance between oxidants and antioxidants in favor of oxidants is termed �oxidative stress.� Regulation of reducing and oxidizing (redox) state is critical for cell viability, activation, proliferation, and organ function. Aerobic organisms have integrated antioxidant systems, which include enzymatic and non- enzymatic antioxidants that are usually effective in blocking harmful effects of ROS. However, in pathological conditions, the antioxidant systems can be overwhelmed. Oxidative stress contributes to many pathological conditions and diseases, including cancer, neurological disorders, atherosclerosis, hypertension, ischemia/perfusion, diabetes, acute respiratory distress syndrome, idiopathic pulmonary fibrosis, chronic obstructive pulmonary disease, and asthma. In this review, we summarize the cellular oxidant and antioxidant systems and discuss the cellular effects and mechanisms of the oxidative stress.
Reactive oxygen species (ROS) are produced by living organisms as a result of normal cellular metabolism. At low to moderate concentrations, they function in physiological cell processes, but at high concentrations, they produce adverse modifications to cell components, such as lipids, proteins, and DNA.1�6 The shift in balance between oxidant/ antioxidant in favor of oxidants is termed �oxidative stress.� Oxidative stress contributes to many pathological conditions, including cancer, neurological disorders,7�10 atherosclerosis, hypertension, ischemia/perfusion,11�14 diabetes, acute respiratory distress syndrome, idiopathic pulmonary fibrosis, chronic obstructive pulmonary disease,15 and asthma.16�21 Aerobic organisms have integrated antioxidant systems,� which include enzymatic and nonenzymatic antioxidants that are usually effective in blocking harmful effects of ROS. However, in pathological conditions, the antioxidant systems can be overwhelmed. In this review, we summarize the cellular oxidant and antioxidant systems and regulation of the reducing and oxidizing (redox) state in health and disease states.
OXIDANTS
Endogenous Sources of ROS
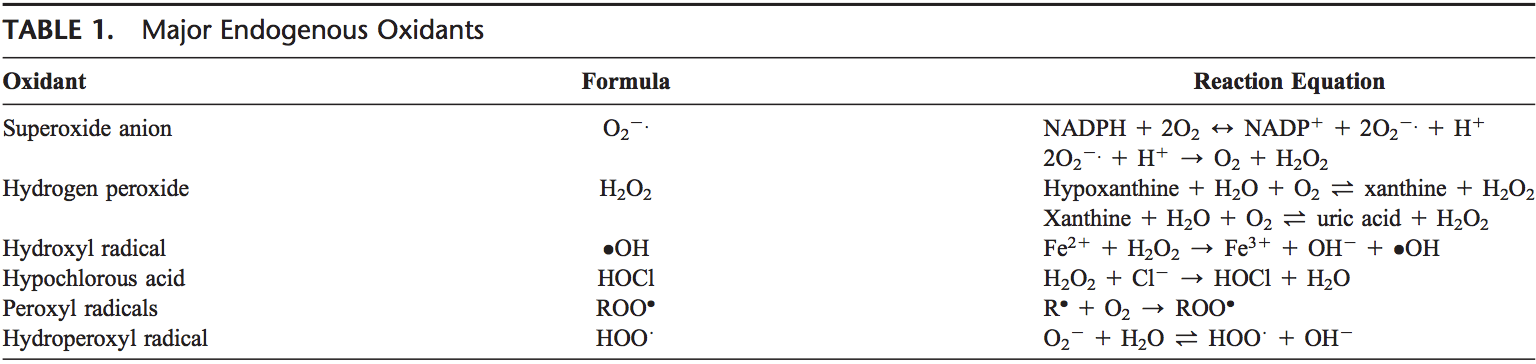
ROS are produced from molecular oxygen as a result of normal cellular metabolism. ROS can be divided into 2 groups: free radicals and nonradicals. Molecules containing one or more unpaired electrons and thus giving reactivity to the molecule are called free radicals. When 2 free radicals share their unpaired electrons, nonradical forms are created. The 3 major ROS that are of physiological significance are superoxide anion (O22.), hydroxyl radical ( OH), and hydro- gen peroxide (H2O2). ROS are summarized in Table 1.
Superoxide anion is formed by the addition of 1 electron to the molecular oxygen.22 This process is mediated by nicotine adenine dinucleotide phosphate [NAD(P)H] oxidase or xanthine oxidase or by mitochondrial electron trans- port system. The major site for producing superoxide anion is the mitochondria, the machinery of the cell to produce adenosine triphosphate. Normally, electrons are transferred through mitochondrial electron transport chain for reduction of oxygen to water, but approximately 1 to 3% of all electrons leak from the system and produce superoxide. NAD(P)H oxidase is found in polymorphonuclear leukocytes, monocytes, and macrophages. Upon phagocytosis, these cells produce a burst of superoxide that lead to bactericidal activity. Superoxide is converted into hydrogen peroxide by the action of superoxide dismutases (SODs, EC 1.15.1.1). Hydrogen peroxide easily diffuses across the plasma membrane. Hydrogen peroxide is also produced by xanthine oxidase, amino acid oxidase, and NAD(P)H oxidase�23,24 and in peroxisomes by consumption of molecular oxygen in metabolic reactions. In a succession of reactions called Haber�Weiss and Fenton reactions,H2O2 can breakdown to OH2 in the presence of transmission metals like Fe21 or Cu21.25
Fe31 +�.O2�?Fe2 +�O2 Haber Weiss
Fe2 +�H2O2�?Fe3 +�OH�+ .OH Fenton reaction
O 2 �itself can also react with H2 O2 and generate OH�.26,27 Hydroxyl radical is the most reactive of ROS and can damage proteins, lipids, and carbohydrates and DNA. It can also start lipid peroxidation by taking an electron from polyunsaturated fatty acids.
Granulocytic enzymes further expand the reactivity of H2O2 via eosinophil peroxidase and myeloperoxidase (MPO). In activated neutrophils, H2O2 is consumed by MPO. In the presence of chloride ion, H2O2 is converted to hypochlorous acid (HOCl). HOCl is highly oxidative and plays an important role in killing of the pathogens in the airways.28 However, HOCl can also react with DNA and induce DNA�protein interactions and produce pyrimidine oxidation products and add chloride to DNA bases.29,30 Eosinophil peroxidase and MPO also contribute to the oxidative stress by modification of proteins by halogenations, nitration, and protein cross-links via tyrosyl radicals.31�33
Other oxygen-derived free radicals are the peroxyl radicals (ROO$ ). Simplest form of these radicals is hydro- peroxyl radical (HOO$ ) and has a role in fatty acid peroxidation. Free radicals can trigger lipid peroxidation chain reactions by abstracting a hydrogen atom from a side- chain methylene carbon. The lipid radical then reacts with oxygen to produce peroxyl radical. Peroxyl radical initiates a chain reaction and transforms polyunsaturated fatty acids into lipid hydroperoxides. Lipid hydroperoxides are very unstable and easily decompose to secondary products, such as aldehydes (such as 4-hydroxy-2,3-nonenal) and malondialdehydes (MDAs). Isoprostanes are another group of lipid peroxidation products that are generated via the peroxidation of arachidonic acid and have also been found to be elevated in plasma and breath condensates of asthmatics.34,35 Peroxidation of lipids disturbs the integrity of cell membranes and leads to rearrangement of membrane structure.
Hydrogen peroxide, superoxide radical, oxidized glutathione (GSSG), MDAs, isoprostanes, carbonyls, and nitrotyrosine can be easily measured from plasma, blood, or bronchoalveolar lavage samples as biomarkers of oxidation by standardized assays.
Exogenous Source of Oxidants
Cigarette Smoke
Cigarette smoke contains many oxidants and free radicals and organic compounds, such as superoxide and nitric oxide.36 In addition, inhalation of cigarette smoke into the lung also activates some endogenous mechanisms, such as accumulation of neutrophils and macrophages, which further increase the oxidant injury.
Ozone Exposure
Ozone exposure can cause lipid peroxidation and induce influx of neutrophils into the airway epithelium. Short-term exposure to ozone also causes the release of inflammatory mediators, such as MPO, eosinophil cationic proteins and also lactate dehydrogenase and albumin.37 Even in healthy subjects, ozone exposure causes a reduction in pulmonary functions.38 Cho et al39 have shown that particulate matter (mixture of solid particles and liquid droplets suspended in the air) catalyzes the reduction of oxygen.
Hyperoxia
Hyperoxia refers to conditions of higher oxygen levels than normal partial pressure of oxygen in the lungs or other body tissues. It leads to greater production of reactive oxygen and nitrogen species.40,41
Ionizing Radiation
Ionizing radiation, in the presence of O2, converts hydroxyl radical, superoxide, and organic radicals to hydrogen peroxide and organic hydroperoxides. These hydroperoxide species react with redox active metal ions, such as Fe and Cu, via Fenton reactions and thus induce oxidative stress.42,43 Narayanan et al44 showed that fibroblasts that were exposed to alpha particles had significant increases in intracellular O2 2. and H2O2 production via plasma membrane-bound NADPH oxidase.44 Signal transduction molecules, such as extracellular signal-regulated kinase 1 and 2 (ERK1/2), c-Jun N-terminal kinase (JNK), and p38, and transcription factors, such as activator protein-1 (AP-1), nuclear factor-kB (NF-kB), and p53, are activated, which result in the expression of radiation response�related genes.45�50 Ultraviolet A (UVA) photons trigger oxidative reactions by excitation of endogenous photosensitizers, such as porphyrins, NADPH oxidase, and riboflavins. 8-Oxo-7,8- dihydroguanine (8-oxoGua) is the main UVA-mediated DNA oxidation product formed by the oxidation of OH radical, 1-electron oxidants, and singlet oxygen that mainly reacts with guanine.51 The formation of guanine radical cation in isolated DNA has been shown to efficiently occur through the direct effect of ionizing radiation.52,53 After exposure to ionizing radiation, intracellular level of glutathione (GSH) decreases for a short term but then increases again.54
Heavy Metal Ions
Heavy metal ions, such as iron, copper, cadmium, mercury, nickel, lead, and arsenic, can induce generation of reactive radicals and cause cellular damage via depletion of enzyme activities through lipid peroxidation and reaction with nuclear proteins and DNA.55
One of the most important mechanisms of metal- mediated free radical generation is via a Fenton-type reaction. Superoxide ion and hydrogen peroxide can interact with transition metals, such as iron and copper, via the metal catalyzed Haber�Weiss/Fenton reaction to form OH radicals.
Besides the Fenton-type and Haber�Weiss-type mechanisms, certain metal ions can react directly with cellular molecules to generate free radicals, such as thiol radicals, or induce cell signaling pathways. These radicals may also react with other thiol molecules to generate O22.. O22. is converted to H2O2, which causes additional oxygen radical generation. Some metals, such as arsenite, induce ROS formation indirectly by activation of radical producing systems in cells.56
Arsenic is a highly toxic element that produces a variety of ROS, including superoxide (O2 2), singlet oxygen (1O2), peroxyl radical (ROO ), nitric oxide (NO ), hydrogen peroxide (H2O2), and dimethylarsinic peroxyl radicals [(CH3)2AsOO ].57�59 Arsenic (III) compounds can inhibit antioxidant enzymes, especially the GSH-dependent enzymes, such as glutathione-S-transferases (GSTs), glutathione peroxidase (GSH-Px), and GSH reductase, via bind- ing to their sulfhydryl (�SH) groups.60,61
Lead increases lipid peroxidation.62 Significant decreases in the activity of tissue SOD and brain GPx have been reported after lead exposure.63,64 Replacement of zinc, which serves as a cofactor for many enzymes by lead, leads to inactivation of such enzymes. Lead exposure may cause inhibition of GST by affecting tissue thiols.
ROS generated by metal-catalyzed reactions can mod- ify DNA bases. Three base substitutions, G / C, G / T, and C / T, can occur as a result of oxidative damage by metal ions, such as Fe21, Cu21, and Ni21. Reid et al65 showed that G / C was predominantly produced by Fe21 while C / T substitution was by Cu21 and Ni21.
ANTIOXIDANTS
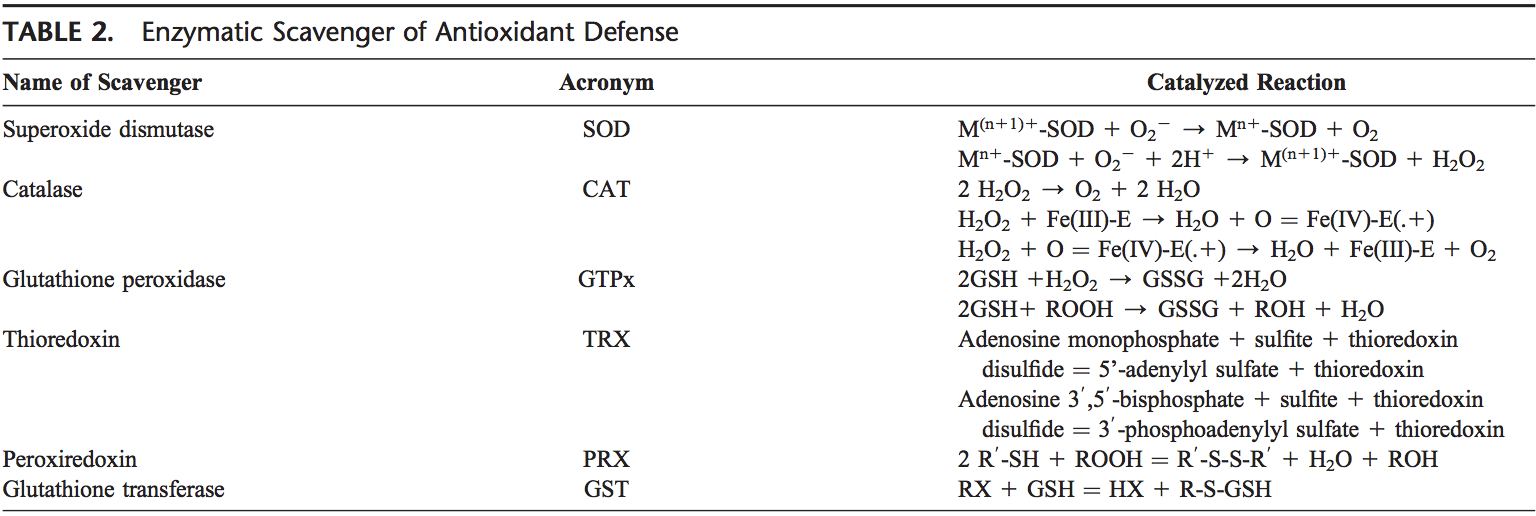
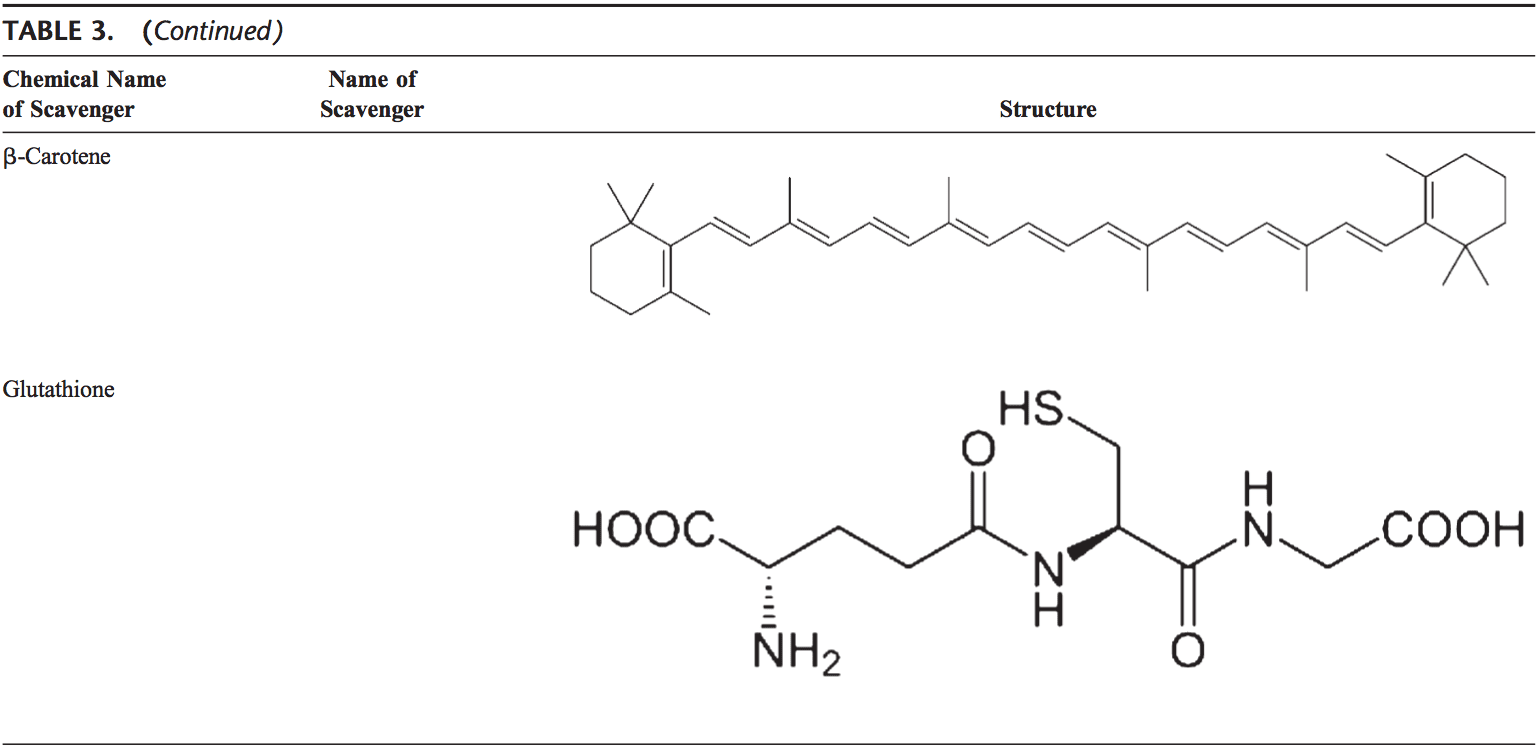
The human body is equipped with a variety of antioxidants that serve to counterbalance the effect of oxidants. For all practical purposes, these can be divided into 2 categories: enzymatic (Table 2) and nonenzymatic (Table 3).
Enzymatic Antioxidants
The major enzymatic antioxidants of the lungs are SODs (EC 1.15.1.11), catalase (EC 1.11.1.6), and GSH-Px (EC 1.11.1.9). In addition to these major enzymes, other antioxidants, including heme oxygenase-1 (EC 1.14.99.3), and redox proteins, such as thioredoxins (TRXs, EC 1.8.4.10), peroxiredoxins (PRXs, EC 1.11.1.15), and glutaredoxins, have also been found to play crucial roles in the pulmonary antioxidant defenses.
Since superoxide is the primary ROS produced from a variety of sources, its dismutation by SOD is of primary importance for each cell. All 3 forms of SOD, that is, CuZn- SOD, Mn-SOD, and EC-SOD, are widely expressed in the human lung. Mn-SOD is localized in the mitochondria matrix. EC-SOD is primarily localized in the extracellular matrix, especially in areas containing high amounts of type I collagen fibers and around pulmonary and systemic vessels. It has also been detected in the bronchial epithelium, alveolar epithelium, and alveolar macrophages.66,67 Overall, CuZn- SOD and Mn-SOD are generally thought to act as bulk scavengers of superoxide radicals. The relatively high EC-SOD level in the lung with its specific binding to the extracellular matrix components may represent a fundamental component of lung matrix protection.68
H2O2 that is produced by the action of SODs or the action of oxidases, such as xanthine oxidase, is reduced to water by catalase and the GSH-Px. Catalase exists as a tetra- mer composed of 4 identical monomers, each of which con- tains a heme group at the active site. Degradation of H2O2 is accomplished via the conversion between 2 conformations of catalase-ferricatalase (iron coordinated to water) and com- pound I (iron complexed with an oxygen atom). Catalase also binds NADPH as a reducing equivalent to prevent oxidative inactivation of the enzyme (formation of compound II) by H2O2 as it is reduced to water.69
Enzymes in the redox cycle responsible for the reduction of H2O2 and lipid hydroperoxides (generated as a result of membrane lipid peroxidation) include the GSH-Pxs.70 The GSH-Pxs are a family of tetrameric enzymes that contain the unique amino acid selenocysteine within the active sites and use low-molecular-weight thiols, such as GSH, to reduce H2O2 and lipid peroxides to their corresponding alcohols. Four GSH- Pxs have been described, encoded by different genes: GSH- Px-1 (cellular GSH-Px) is ubiquitous and reduces H2O2 and fatty acid peroxides, but not esterified peroxyl lipids.71 Esterified lipids are reduced by membrane-bound GSH-Px-4 (phospholipid hydroperoxide GSH-Px), which can use several different low-molecular-weight thiols as reducing equivalents. GSH-Px-2 (gastrointestinal GSH-Px) is localized in gastrointestinal epithelial cells where it serves to reduce dietary peroxides.72 GSH-Px-3 (extracellular GSH-Px) is the only member of the GSH-Px family that resides in the extracellular compartment and is believed to be one of the most important extracellular antioxidant enzyme in mammals. Of these, extracellular GSH-Px is most widely investigated in the human lung.73
In addition, disposal of H2O2 is closely associated with several thiol-containing enzymes, namely, TRXs (TRX1 and TRX2), thioredoxin reductases (EC 1.8.1.9) (TRRs), PRXs (which are thioredoxin peroxidases), and glutaredoxins.74
Two TRXs and TRRs have been characterized in human cells, existing in both cytosol and mitochondria. In the lung, TRX and TRR are expressed in bronchial and alveolar epithelium and macrophages. Six different PRXs have been found in human cells, differing in their ultrastructural compartmentalization. Experimental studies have revealed the importance of PRX VI in the protection of alveolar epithelium. Human lung expresses all PRXs in bronchial epithelium, alveolar epithelium, and macrophages.75 PRX V has recently been found to function as a peroxynitrite reductase,76 which means that it may function as a potential protective compound in the development of ROS-mediated lung injury.77
Common to these antioxidants is the requirement of NADPH as a reducing equivalent. NADPH maintains catalase in the active form and is used as a cofactor by TRX and GSH reductase (EC 1.6.4.2), which converts GSSG to GSH, a co-substrate for the GSH-Pxs. Intracellular NADPH, in turn, is generated by the reduction of NADP1 by glucose-6-phosphate dehydrogenase, the first and rate-limiting enzyme of the pen- tose phosphate pathway, during the conversion of glucose- 6-phosphate to 6-phosphogluconolactone. By generating NADPH, glucose-6-phosphate dehydrogenase is a critical determinant of cytosolic GSH buffering capacity (GSH/ GSSG) and, therefore, can be considered an essential, regulatory antioxidant enzyme.78,79
GSTs (EC 2.5.1.18), another antioxidant enzyme family, inactivate secondary metabolites, such as unsaturated aldehydes, epoxides, and hydroperoxides. Three major families of GSTs have been described: cytosolic GST, mitochondrial GST,80,81 and membrane-associated microsomal GST that has a role in eicosanoid and GSH metabolism.82 Seven classes of cytosolic GST are identified in mammalian, designated Alpha, Mu, Pi, Sigma, Theta, Omega, and Zeta.83�86 During non-stressed conditions, class Mu and Pi GSTs interact with kinases Ask1 and JNK, respectively, and inhibit these kinases.87�89 It has been shown that GSTP1 dissociates from JNK in response to oxidative stress.89 GSTP1 also physically interacts with PRX VI and leads to recovery of PRX enzyme activity via glutathionylation of the oxidized protein.90
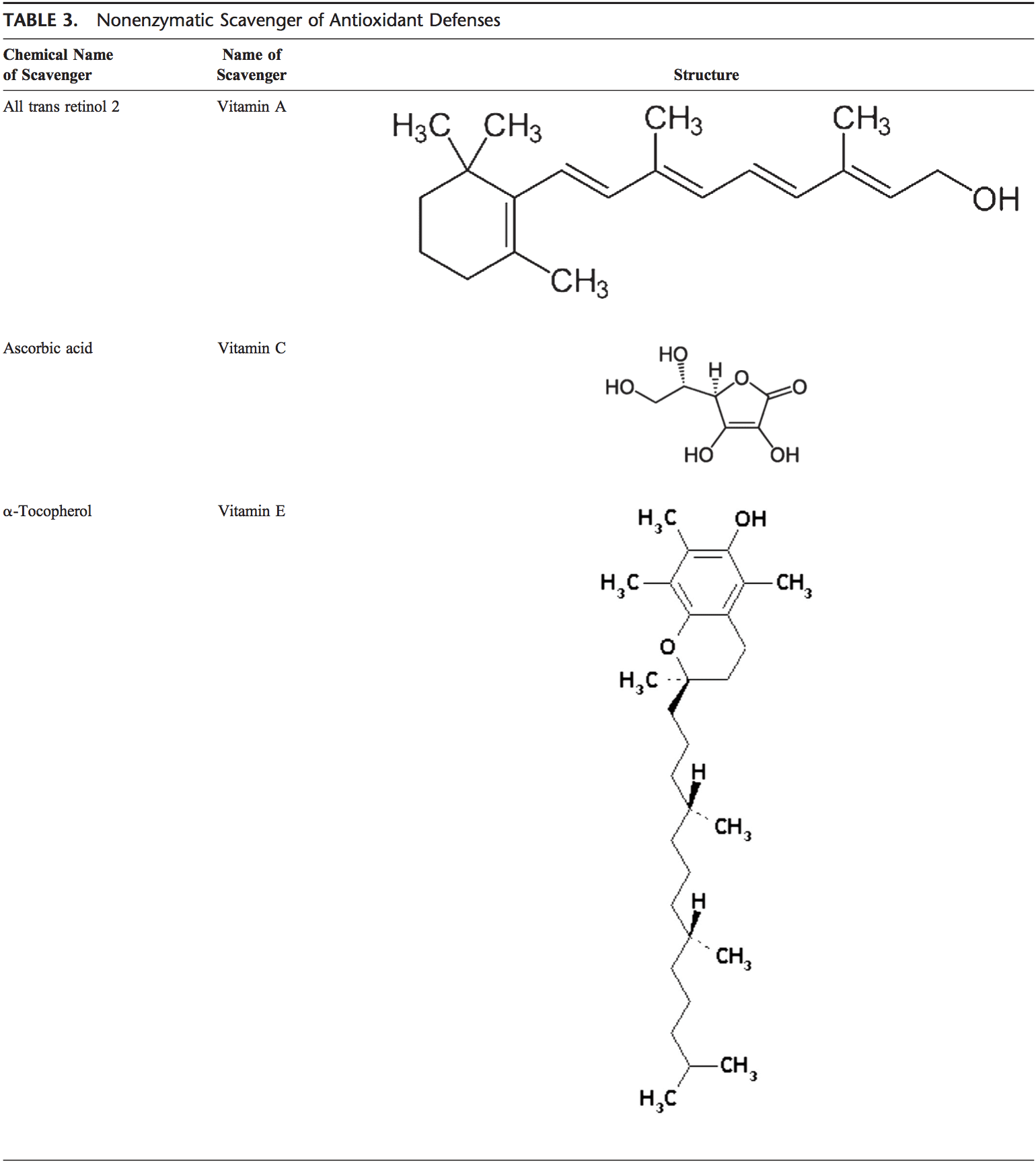
Nonenzymatic Antioxidants
Nonenzymatic antioxidants include low-molecular-weight compounds, such as vitamins (vitamins C and E), b-carotene, uric acid, and GSH, a tripeptide (L-g-glutamyl-L-cysteinyl-L- glycine) that comprise a thiol (sulfhydryl) group.
Vitamin C (Ascorbic Acid)
Water-soluble vitamin C (ascorbic acid) provides intracellular and extracellular aqueous-phase antioxidant capacity primarily by scavenging oxygen free radicals. It converts vitamin E free radicals back to vitamin E. Its plasma levels have been shown to decrease with age.91,92
Vitamin E (a-Tocopherol)
Lipid-soluble vitamin E is concentrated in the hydrophobic interior site of cell membrane and is the principal defense against oxidant-induced membrane injury. Vitamin E donates electron to peroxyl radical, which is produced during lipid peroxidation. a-Tocopherol is the most active form of vitamin E and the major membrane-bound antioxidant in cell. Vitamin E triggers apoptosis of cancer cells and inhibits free radical formations.93
Glutathione
GSH is highly abundant in all cell compartments and is the major soluble antioxidant. GSH/GSSG ratio is a major determinant of oxidative stress. GSH shows its antioxidant effects in several ways.94 It detoxifies hydrogen peroxide and lipid peroxides via action of GSH-Px. GSH donates its electron to H2O2 to reduce it into H2O and O2. GSSG is again reduced into GSH by GSH reductase that uses NAD(P)H as the electron donor. GSH-Pxs are also important for the pro- tection of cell membrane from lipid peroxidation. Reduced glutathione donates protons to membrane lipids and protects them from oxidant attacks.95
GSH is a cofactor for several detoxifying enzymes, such as GSH-Px and transferase. It has a role in converting vitamin C and E back to their active forms. GSH protects cells against apoptosis by interacting with proapoptotic and antiapoptotic signaling pathways.94 It also regulates and activates several transcription factors, such as AP-1, NF-kB, and Sp-1.
Carotenoids (b-Carotene)
Carotenoids are pigments found in plants. Primarily, b-carotene has been found to react with peroxyl (ROO ), hydroxyl ( OH), and superoxide (O22.) radicals.96 Carotenoids show their antioxidant effects in low oxygen partial pressure but may have pro-oxidant effects at higher oxygen concentrations.97 Both carotenoids and retinoic acids (RAs) are capable of regulating transcription factors.98 b-Carotene inhibits the oxidant-induced NF-kB activation and interleukin (IL)-6 and tumor necrosis factor-a production. Carotenoids also affect apoptosis of cells. Antiproliferative effects of RA have been shown in several studies. This effect of RA is mediated mainly by retinoic acid receptors and vary among cell types. In mammary carcinoma cells, retinoic acid receptor was shown to trigger growth inhibition by inducing cell cycle arrest, apoptosis, or both.99,100
THE EFFECT OF OXIDATIVE STRESS: GENETIC, PHYSIOLOGICAL, & BIOCHEMICAL MECHANISMS
Oxidative stress occurs when the balance between antioxidants and ROS are disrupted because of either depletion of antioxidants or accumulation of ROS. When oxidative stress occurs, cells attempt to counteract the oxidant effects and restore the redox balance by activation or silencing of genes encoding defensive enzymes, tran- scription factors, and structural proteins.101,102 Ratio between oxidized and reduced glutathione (2GSH/GSSG) is one of the important determinants of oxidative stress in the body. Higher production of ROS in body may change DNA structure, result in modification of proteins and lipids, activation of several stress-induced transcription factors, and production of pro-inflammatory and anti-inflammatory cytokines.
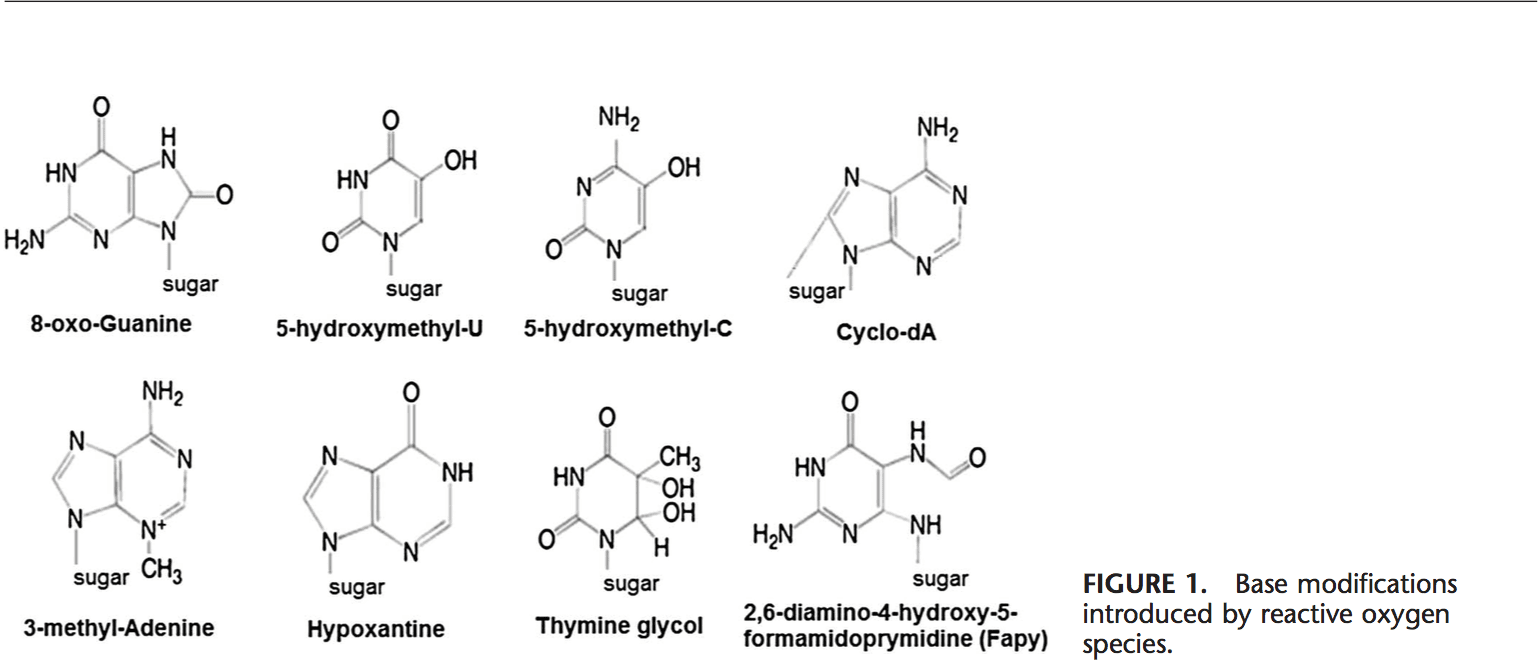
Effects Of Oxidative Stress On DNA
ROS can lead to DNA modifications in several ways, which involves degradation of bases, single- or double- stranded DNA breaks, purine, pyrimidine or sugar-bound modifications, mutations, deletions or translocations, and cross-linking with proteins. Most of these DNA modifications (Fig. 1) are highly relevant to carcinogenesis, aging, and neurodegenerative, cardiovascular, and autoimmune diseases. Tobacco smoke, redox metals, and nonredox metals, such as iron, cadmium, chrome, and arsenic, are also involved in carcinogenesis and aging by generating free radicals or bind- ing with thiol groups. Formation of 8-OH-G is the best- known DNA damage occurring via oxidative stress and is a potential biomarker for carcinogenesis.
Promoter regions of genes contain consensus sequences for transcription factors. These transcription factor�binding sites contain GC-rich sequences that are susceptible for oxidant attacks. Formation of 8-OH-G DNA in transcription factor binding sites can modify binding of transcription factors and thus change the expression of related genes as has been shown for AP-1 and Sp-1 target sequences.103 Besides 8-OH-G, 8,59 -cyclo-29 -deoxyadenosine (cyclo-dA) has also been shown to inhibit transcription from a reporter gene in a cell system if located in a TATA box.104 The TATA-binding protein initiates transcription by changing the bending of DNA. The binding of TATA-binding protein may be impaired by the presence of cyclo-dA.
Oxidative stress causes instability of microsatellite (short tandem repeats) regions. Redox active metal ions, hydroxyl radicals increase microsatellite instability.105 Even though single-stranded DNA breaks caused by oxidant injury can easily be tolerated by cells, double-stranded DNA breaks induced by ionizing radiation can be a significant threat for the cell survival.106
Methylation at CpG islands in DNA is an important epigenetic mechanism that may result in gene silencing. Oxidation of 5-MeCyt to 5-hydroxymethyl uracil (5-OHMeUra) can occur via deamination/oxidation reactions of thymine or 5-hydroxymethyl cytosine intermediates.107 In addition to the modulating gene expression, DNA methylation also seems to affect chromatin organization.108 Aberrant DNA methylation patterns induced by oxidative attacks also affect DNA repair activity.
Effects Of Oxidative Stress On Lipids
ROS can induce lipid peroxidation and disrupt the membrane lipid bilayer arrangement that may inactivate membrane-bound receptors and enzymes and increase tissue permeability.109 Products of lipid peroxidation, such as MDA and unsaturated aldehydes, are capable of inactivating many cellular proteins by forming protein cross-linkages.110�112 4-Hydroxy-2-nonenal causes depletion of intracellular GSH and induces of peroxide production,113,114 activates epidermal growth factor receptor,115 and induces fibronectin production.116 Lipid peroxidation products, such as isoprostanes and thiobarbituric acid reactive substances, have been used as indirect biomarkers of oxidative stress, and increased levels were shown in the exhaled breath condensate or bronchoalveolar lavage fluid or lung of chronic obstructive pulmonary disease patients or smokers.117�119
Effects Of Oxidative Stress on Proteins
ROS can cause fragmentation of the peptide chain, alteration of electrical charge of proteins, cross-linking of proteins, and oxidation of specific amino acids and therefore lead to increased susceptibility to proteolysis by degradation by specific proteases.120 Cysteine and methionine residues in proteins are particularly more susceptible to oxidation.121 Oxidation of sulfhydryl groups or methionine residues of proteins cause conformational changes, protein unfolding, and degradation.8,121�123 Enzymes that have metals on or close to their active sites are especially more sensitive to metal catalyzed oxidation. Oxidative modification of enzymes has been shown to inhibit their activities.124,125
In some cases, specific oxidation of proteins may take place. For example, methionine can be oxidized methionine sulfoxide126 and phenylalanine to o-tyrosine127; sulfhydryl groups can be oxidized to form disulfide bonds;128 and carbonyl groups may be introduced into the side chains of proteins. Gamma rays, metal-catalyzed oxidation, HOCl, and ozone can cause formation of carbonyl groups.129
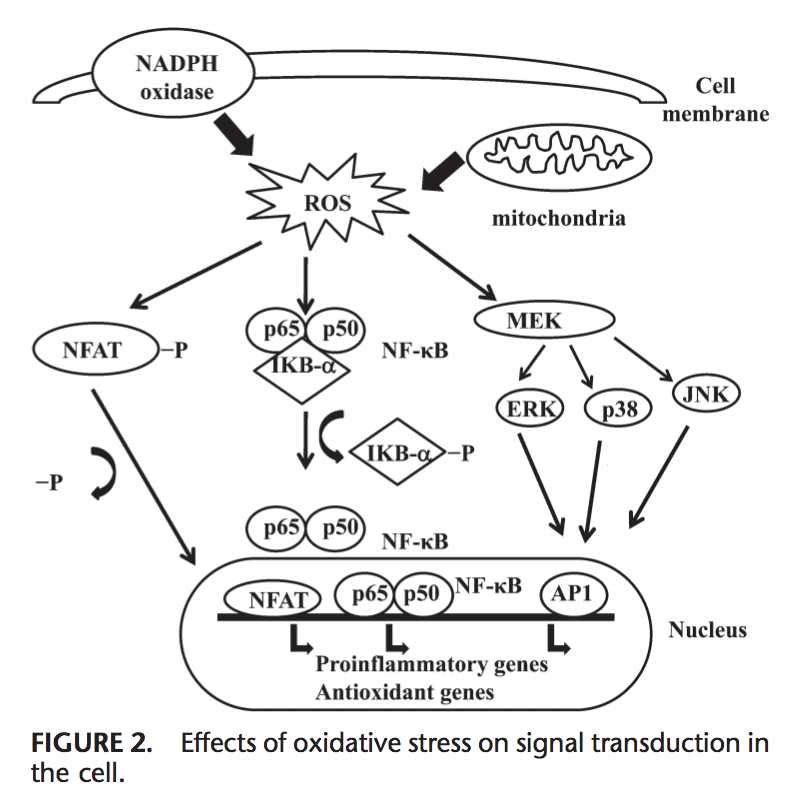
Effects of Oxidative Stress on Signal Transduction
ROS can induce expression of several genes involved in signal transduction.1,130 A high ratio for GSH/GSSG is important for the protection of the cell from oxidative dam- age. Disruption of this ratio causes activation of redox sensitive transcription factors, such as NF-kB, AP-1, nuclear factor of activated T cells and hypoxia-inducible factor 1 , that are involved in the inflammatory response. Activation of transcription factors via ROS is achieved by signal transduction cascades that transmit the information from outside to the inside of cell. Tyrosine kinase receptors, most of the growth factor receptors, such as epidermal growth factor receptor, vascular endothelial growth factor receptor, and receptor for platelet-derived growth factor, protein tyrosine phosphatases, and serine/threonine kinases are targets of ROS.131�133 Extra- cellular signal-regulated kinases, JNK, and p38, which are the members of mitogen-activated protein kinase family and involved in several processes in cell including proliferation, differentiation, and apoptosis, also can be regulated by oxidants.
Under oxidative stress conditions, cysteine residues in the DNA-binding site of c-Jun, some AP-1 subunits, and inhibitory k-B kinase undergo reversible S-glutathiolation. Glutaredoxin and TRX have been reported to play an important role in regulation of redox-sensitive signaling pathways, such as NF-kB and AP-1, p38 mitogen-activated protein kinase, and JNK.134�137
NF-kB can be activated in response to oxidative stress conditions, such as ROS, free radicals, and UV irradiation.138 Phosphorylation of IkB frees NF-kB and allows it to enter the nucleus to activate gene transcription.139 A number of kinases have been reported to phosphorylate IkBs at the serine residues. These kinases are the targets of oxidative signals for activation of NF-kB.140 Reducing agents enhance NF-kB DNA binding, whereas oxidizing agents inhibit DNA binding of NF-kB. TRX may exert 2 opposite actions in regulation of NF-kB: in the cytoplasm, it blocks degradation of IkB and inhibits NF-kB activation but enhances NF-kB DNA binding in the nucleus.141 Activation of NF-kB via oxidation-related degradation of IkB results in the activation of several antioxidant defense�related genes. NF-kB regulates the expression of several genes that participate in immune response, such as IL-1b, IL-6, tumor necrosis factor-a, IL-8, and several adhesion molecules.142,143 NF-kB also regulates angiogenesis and proliferation and differentiation of cells.
AP-1 is also regulated by redox state. In the presence of H2O2, some metal ions can induce activation of AP-1. Increase in the ratio of GSH/GSSG enhances AP-1 binding while GSSG inhibits the DNA binding of AP-1.144 DNA binding of the Fos/Jun heterodimer is increased by the reduction of a single conserved cysteine in the DNA-binding domain of each of the proteins,145 while DNA binding of AP-1 can be inhibited by GSSG in many cell types, suggesting that disulphide bond formation by cysteine residues inhibits AP-1 DNA binding.146,147 Signal transduction via oxidative stress is summarized in Figure 2.
CONCLUSIONS
Oxidative stress can arise from overproduction of ROS by metabolic reactions that use oxygen and shift the balance between oxidant/antioxidant statuses in favor of the oxidants. ROS are produced by cellular metabolic activities and environmental factors, such as air pollutants or cigarette smoke. ROS are highly reactive molecules because of unpaired electrons in their structure and react with several biological macromolecules in cell, such as carbohydrates, nucleic acids, lipids, and proteins, and alter their functions. ROS also affects the expression of several genes by upregulation of redox-sensitive transcription factors and chromatin remodeling via alteration in histone acetylation/ deacetylation. Regulation of redox state is critical for cell viability, activation, proliferation, and organ function.
REFERENCES
1. Valko M, Rhodes CJ, Moncol J, Izakovic M, Mazur M. Free radicals, metals and antioxidants in oxidative stress-induced cancer. Chem Biol Interact. 2006;160:1�40.
2. Halliwell B, Gutteridge JMC. Free Radicals in Biology and Medicine. 3rd ed. New York: Oxford University Press;1999.
3. Marnett LJ. Lipid peroxidationdDNA damage by malondialdehyde. Mutat Res. 1999;424:83�95.
4. Siems WG, Grune T, Esterbauer H. 4-Hydroxynonenal formation during ischemia and reperfusion of rat small intestine. �Life Sci. 1995;57:785�789.
5. Stadtman ER. Role of oxidant species in aging. Curr Med Chem. 2004;11:1105�1112.
6. Wang MY, Dhingra K, Hittelman WN, Liehr JG, deAndrade M, Li DH. Lipid peroxidation-induced putative malondialdehyde�DNA adducts in human breast tissues. Cancer Epidemiol Biomarkers Prev. 1996;5:705�710.
7. Jenner P. Oxidative stress in Parkinson�s disease. Ann Neurol. 2003;53: S26�S36.
8. Lyras L, Cairns NJ, Jenner A, Jenner P, Halliwell B. An assessment of oxidative damage to proteins, lipids, and DNA in brain from patients with Alzheimer�s disease. J Neurochem. 1997;68:2061�2069.
9. Sayre LM, Smith MA, Perry G. Chemistry and biochemistry of oxidative stress in neurodegenerative disease. Curr Med Chem. 2001;8:721�738.
10. Toshniwal PK, Zarling EJ. Evidence for increased lipid peroxidation in multiple sclerosis. Neurochem Res. 1992;17:205�207.
11. Dhalla NS, Temsah RM, Netticadan T. Role of oxidative stress in cardiovascular diseases. J Hypertens. 2000;18:655�673.
12. Kasparova S, Brezova V, Valko M, Horecky J, Mlynarik V, et al. Study of the oxidative stress in a rat model of chronic brain hypoperfusion. Neurochem Int. 2005;46:601�611.
13. Kerr S, Brosnan MJ, McIntyre M, Reid JL, Dominiczak AF, Hamilton CA. Superoxide anion production is increased in a model of genetic hypertension: role of the endothelium. Hypertension. 1999;33:1353�1358.
14. Kukreja RC, Hess ML. The oxygen free-radical system: from equations through membrane�protein interactions to cardiovascular injury and protection. Cardiovasc Res. 1992;26:641�655.
15. Asami S, Manabe H, Miyake J, Tsurudome Y, Hirano T, et al. Cigarette smoking induces an increase in oxidative DNA damage, 8-hydroxydeoxyguanosine, in a central site of the human lung. Carcinogenesis. 1997;18:1763�1766.
16. Andreadis AA, Hazen SL, Comhair SA, Erzurum SC. Oxidative and nitrosative events in asthma. Free Radic Biol Med. 2003;35:213�225.
17. Comhair SA, Ricci KS, Arroliga M, Lara AR, Dweik RA, et al. Correlation of systemic superoxide dismutase deficiency to airflow obstruction in asthma. Am J Respir Crit Care Med. 2005;172:306�313.
18. Comhair SA, Xu W, Ghosh S, Thunnissen FB, Almasan A, et al. Superoxide dismutase inactivation in pathophysiology of asthmatic airway remodeling and reactivity. Am J Pathol. 2005;166:663�674.
19. Dut R, Dizdar EA, Birben E, Sackesen C, Soyer OU, Besler T, Kalayci O. Oxidative stress and its determinants in the airways of children with asthma. Allergy. 2008;63:1605�1609.
20. Ercan H, Birben E, Dizdar EA, Keskin O, Karaaslan C, et al. Oxidative stress and genetic and epidemiologic determinants of oxidant injury in childhood asthma. J Allergy Clin Immunol. 2006;118:1097�1104.
21. Fitzpatrick AM, Teague WG, Holguin F, Yeh M, Brown LA. Severe Asthma Research Program. Airway glutathione homeostasis is altered in children with severe asthma: evidence for oxidant stress. J Allergy Clin Immunol. 2009;123:146�152.
22. Miller DM, Buettner GR, Aust SD. Transition metals as catalysts of “autoxidation” reactions. Free Radic Biol Med. 1990;8:95�108.
23. Dupuy C, Virion A, Ohayon R, Kaniewski J, D�me D, Pommier J. Mechanism of hydrogen peroxide formation catalyzed by NADPH oxidase in thyroid plasma membrane. J Biol Chem. 1991;266:3739�3743.
24. Granger DN. Role of xanthine oxidase and granulocytes in ischemiareperfusion injury. Am J Physiol. 1988;255:H1269�H1275.
25. Fenton HJH. Oxidation of tartaric acid in the presence of iron. J Chem Soc. 1984;65:899�910.
26. Haber F, Weiss JJ. The catalytic decomposition of hydrogen peroxide by iron salts. Proc R Soc Lond Ser A. 1934;147:332�351.
27. Liochev SI, Fridovich I. The Haber�Weiss cycled70 years later: an alternative view. Redox Rep. 2002;7:55�57.
28. Klebanoff SJ. Myeloperoxidase: friend and foe. J Leukoc Biol. 2005;77:598�625.
29. Whiteman M, Jenner A, Halliwell B. Hypochlorous acid-induced base modifications in isolated calf thymus DNA. Chem Res Toxicol. 1997;10:1240�1246.
30. Kulcharyk PA, Heinecke JW. Hypochlorous acid produced by the myeloperoxidase system of human phagocytes induces covalent cross-links between DNA and protein. Biochemistry. 2001;40:3648�3656.
31. Brennan ML, Wu W, Fu X, Shen Z, Song W, et al. A tale of two controversies: defining both the role of peroxidases in nitrotyrosine formation in vivo using eosinophil peroxidase and myeloperoxidasedeficient mice, and the nature of peroxidase-generated reactive nitrogen species. J Biol Chem. 2002;277:17415�17427.
32. Denzler KL, Borchers MT, Crosby JR, Cieslewicz G, Hines EM, et al. Extensive eosinophil degranulation and peroxidase-mediated oxidation of airway proteins do not occur in a mouse ovalbumin-challenge model of pulmonary inflammation. J Immunol. 2001;167:1672�1682.
33. van Dalen CJ, Winterbourn CC, Senthilmohan R, Kettle AJ. Nitrite as a substrate and inhibitor of myeloperoxidase. Implications for nitration and hypochlorous acid production at sites of inflammation. J Biol Chem. 2000;275:11638�11644.
34. Wood LG, Fitzgerald DA, Gibson PG, Cooper DM, Garg ML. Lipid peroxidation as determined by plasma isoprostanes is related to disease severity in mild asthma. Lipids. 2000;35:967�974.
35. Montuschi P, Corradi M, Ciabattoni G, Nightingale J, Kharitonov SA, Barnes PJ. Increased 8-isoprostane, a marker of oxidative stress, in exhaled condensate of asthma patients. Am J Respir Crit Care Med. 1999;160:216�220.
36. Church DF, Pryor WA. Free-radical chemistry of cigarette smoke and its toxicological implications. Environ Health Perspect. 1985;64:111�126.
37. Hiltermann JT, Lapperre TS, van Bree L, Steerenberg PA, Brahim JJ, et al. Ozone-induced inflammation assessed in sputum and bronchial lavage fluid from asthmatics: a new noninvasive tool in epidemiologic studies on air pollution and asthma. Free Radic Biol Med. 1999;27:1448�1454.
38. Nightingale JA, Rogers DF, Barnes PJ. Effect of inhaled ozone on exhaled nitric oxide, pulmonary function, and induced sputum in normal and asthmatic subjects. Thorax. 1999;54:1061�1069.
39. Cho AK, Sioutas C, Miguel AH, Kumagai Y, Schmitz DA, et al. Redox activity of airborne particulate matter at different sites in the Los Angeles Basin. Environ Res. 2005;99:40�47.
40. Comhair SA, Thomassen MJ, Erzurum SC. Differential induction of extracellular glutathione peroxidase and nitric oxide synthase 2 in airways of healthy individuals exposed to 100% O(2) or cigarette smoke. Am J Respir Cell Mol Biol. 2000;23:350�354.
41. Matthay MA, Geiser T, Matalon S, Ischiropoulos H. Oxidant-mediated lung injury in the acute respiratory distress syndrome. Crit Care Med. 1999;27:2028�2030.
42. Biaglow JE, Mitchell JB, Held K. The importance of peroxide and superoxide in the X-ray response. Int J Radiat Oncol Biol Phys. 1992;22:665�669.
43. Chiu SM, Xue LY, Friedman LR, Oleinick NL. Copper ion-mediated sensitization of nuclear matrix attachment sites to ionizing radiation. Biochemistry. 1993;32:6214�6219.
44. Narayanan PK, Goodwin EH, Lehnert BE. Alpha particles initiate biological production of superoxide anions and hydrogen peroxide in human cells. Cancer Res. 1997;57:3963�3971.
45. Tuttle SW, Varnes ME, Mitchell JB, Biaglow JE. Sensitivity to chemical oxidants and radiation in CHO cell lines deficient in oxidative pentose cycle activity. Int J Radiat Oncol Biol Phys. 1992;22: 671�675.
46. Guo G, Yan-Sanders Y, Lyn-Cook BD, Wang T, Tamae D, et al. Manganese
superoxide dismutase-mediated gene expression in radiationinduced
adaptive responses. Mol Cell Biol. 2003;23:2362�2378.
47. Azzam EI, de Toledo SM, Spitz DR, Little JB. Oxidative metabolism
modulates signal transduction and micronucleus formation in bystander
cells from a-particle irradiated normal human fibroblasts. Cancer Res.
2002;62:5436�5442.
48. Leach JK, Van Tuyle G, Lin PS, Schmidt-Ullrich R, Mikkelsen RB.
Ionizing radiation-induced, mitochondria-dependent generation of reactive
oxygen/nitrogen. Cancer Res. 2001;61:3894�3901.
49. Dent P, Yacoub A, Fisher PB, Hagan MP, Grant S. MAPK pathways in
radiation responses. Oncogene. 2003;22:5885�5896.
50. Wei SJ, Botero A, Hirota K, Bradbury CM, Markovina S, et al. Thioredoxin
nuclear translocation and interaction with redox factor-1 activates the AP-1 transcription factor in response to ionizing radiation. Cancer Res. 2000;60:6688�6695.
51. Cadet J, Douki T, Gasparutto D, Ravanat JL. Oxidative damage to DNA: formation, measurement and biochemical features. Mutat Res. 2003;531:5�23.
52. Yokoya A, Cunniffe SM, O�Neill P. Effect of hydration on the induction of strand breaks and base lesions in plasmid DNA films by gammaradiation. J Am Chem Soc. 2002;124:8859�8866.
53. Janssen YM, Van Houten B, Borm PJ, Mossman BT. Cell and tissue responses to oxidative damage. Lab Invest. 1993;69:261�274.
54. Iwanaga M, Mori K, Iida T, Urata Y, Matsuo T, et al. Nuclear factor kappa B dependent induction of gamma glutamylcysteine synthetase by ionizing radiation in T98G human glioblastoma cells. Free Radic Biol Med. 1998;24:1256�1268.
55. Stohs SJ, Bagchi D. Oxidative mechanisms in the toxicity of metal ions. Free Radic Biol Med. 1995;18:321�336.
56. Leonard SS, Harris GK, Shi X. Metal-induced oxidative stress and signal transduction. Free Radic Biol Med. 2004;37:1921�1942.
57. Shi H, Shi X, Liu KJ. Oxidative mechanism of arsenic toxicity and carcinogenesis. Mol Cell Biochem. 2004;255:67�78.
58. Pi J, Horiguchi S, Sun Y, Nikaido M, Shimojo N, Hayashi T. A potential mechanism for the impairment of nitric oxide formation caused by prolonged oral exposure to arsenate in rabbits. Free Radic Biol Med.2003;35:102�113.
59. Rin K, Kawaguchi K, Yamanaka K, Tezuka M, Oku N, Okada S. DNAstrand breaks induced by dimethylarsinic acid, a metabolite of inorganic arsenics, are strongly enhanced by superoxide anion radicals. Biol Pharm Bull. 1995;18:45�58.
60. Waalkes MP, Liu J, Ward JM, Diwan LA. Mechanisms underlying arsenic carcinogenesis: hypersensitivity of mice exposed to inorganic arsenic during gestation. Toxicology. 2004;198:31�38.
61. Schiller CM, Fowler BA, Woods JS. Effects of arsenic on pyruvate dehydrogenase activation. Environ Health Perspect. 1977;19:205�207.
62. Monterio HP, Bechara EJH, Abdalla DSP. Free radicals involvement in neurological porphyrias and lead poisoning. Mol Cell Biochem. 1991;103:73�83.
63. Tripathi RM, Raghunath R, Mahapatra S. Blood lead and its effect on Cd, Cu, Zn, Fe and hemoglobin levels of children. Sci Total Environ. 2001;277:161�168.
64. Nehru B, Dua R. The effect of dietary selenium on lead neurotoxicity. J Environ Pathol Toxicol Oncol. 1997;16:47�50.
65. Reid TM, Feig DI, Loeb LA. Mutagenesis by metal-induced oxygen radicals. Environ Health Perspect. 1994;102(suppl 3):57�61.
66. Kinnula VL, Crapo JD. Superoxide dismutases in the lung and human lung diseases. Am J Respir Crit Care Med. 2003;167:1600�1619.
67. Kinnula VL. Production and degradation of oxygen metabolites during inflammatory states in the human lung. Curr Drug Targets Inflamm Allergy. 2005;4:465�470.
68. Zelko IN, Mariani TJ, Folz RJ. Superoxide dismutase multigene family: a comparison of the CuZn-SOD (SOD1), Mn-SOD (SOD2), and EC-SOD (SOD3) gene structures, evolution, and expression. Free Radic Biol Med. 2002;33:337�349.
69. Kirkman HN, Rolfo M, Ferraris AM, Gaetani GF. Mechanisms of protection of catalase by NADPH. Kinetics and stoichiometry. J Biol Chem. 1999;274:13908�13914.
70. Floh� L. Glutathione peroxidase. Basic Life Sci. 1988;49:663�668.
71. Arthur JR. The glutathione peroxidases. Cell Mol Life Sci. 2000;57:1825�1835.
72. Chu FF, Doroshow JH, Esworthy RS. Expression, characterization, and tissue distribution of a new cellular selenium-dependent glutathione peroxidase, GSHPx-GI. J Biol Chem. 1993;268:2571�2576.
73. Comhair SA, Bhathena PR, Farver C, Thunnissen FB, Erzurum SC. Extracellular glutathione peroxidase induction in asthmatic lungs: evidence for redox regulation of expression in human airway epithelial cells. FASEB J. 2001;15:70�78.
74. Gromer S, Urig S, Becker K. The thioredoxin systemdfrom science to clinic. Med Res Rev. 2004;24:40�89.
75. Kinnula VL, Lehtonen S, Kaarteenaho-Wiik R, Lakari E, P��kk� P, et al. Cell specific expression of peroxiredoxins in human lung and pulmonary sarcoidosis. Thorax. 2002;57:157�164.
76. Dubuisson M, Vander Stricht D, Clippe A, Etienne F, Nauser T, et al. Human peroxiredoxin 5 is a peroxynitrite reductase. FEBS Lett. 2004;571:161�165.
77. Holmgren A. Antioxidant function of thioredoxin and glutaredoxin systems. Antioxid Redox Signal. 2000;2:811�820.
78. Dickinson DA, Forman HJ. Glutathione in defense and signaling: lessons from a small thiol. Ann N Y Acad Sci. 2002;973:488�504.
79. Sies H. Glutathione and its role in cellular functions. Free Radic Biol Med. 1999;27:916�921.
80. Ladner JE, Parsons JF, Rife CL, Gilliland GL, Armstrong RN. Parallel evolutionary pathways for glutathione transferases: structure and mechanism of the mitochondrial class kappa enzyme rGSTK1-1. Biochemistry. 2004;43:52�61.
81. Robinson A, Huttley GA, Booth HS, Board PG. Modelling and bioinformatics studies of the human kappa class glutathione transferase predict a novel third transferase family with homology to prokaryotic 2-hydroxychromene-2-carboxylate isomerases. Biochem J. 2004;379:541�552.
82. Jakobsson P-J, Morgenstern R, Mancini J, Ford-Hutchinson A, Persson B. Common structural features of MAPEGda widespread superfamily of membrane associated proteins with highly divergent functions in eicosanoid and glutathione metabolism. Protein Sci. 1999;8:689�692.
83. Hayes JD, Pulford DJ. The glutathione S-transferase supergene family: regulation of GST and the contribution of the isoenzymes to cancer chemoprotection and drug resistance. Crit Rev Biochem Mol Biol. 1995;30:445�600.
84. Armstrong RN. Structure, catalytic mechanism, and evolution of the glutathione transferases. Chem Res Toxicol. 1997;10:2�18.
85. Hayes JD, McLellan LI. Glutathione and glutathione-dependent enzymes represent a co-ordinately regulated defence against oxidative stress. Free Radic Res. 1999;31:273�300.
86. Sheehan D, Meade G, Foley VM, Dowd CA. Structure, function and evolution of glutathione transferases: implications for classification of nonmammalian members of an ancient enzyme superfamily. Biochem J. 2001;360:1�16.
87. Cho S-G, Lee YH, Park H-S, Ryoo K, Kang KW, et al. Glutathione S-transferase Mu modulates the stress activated signals by suppressing apoptosis signal-regulating kinase 1. J Biol Chem. 2001;276:12749�12755.
88. Dorion S, Lambert H, Landry J. Activation of the p38 signaling pathway by heat shock involves the dissociation of glutathione S-transferase Mu from Ask1. J Biol Chem. 2002;277:30792�30797.
89. Adler V, Yin Z, Fuchs SY, Benezra M, Rosario L, et al. Regulation of JNK signalling by GSTp. EMBO J. 1999;18:1321�1334.
90. Manevich Y, Feinstein SI, Fisher AB. Activation of the antioxidant enzyme 1-CYS peroxiredoxin requires glutathionylation mediated by heterodimerization with pGST. Proc Natl Acad Sci U S A. 2004;101:3780�3785.
91. Bunker VW. Free radicals, antioxidants and ageing. Med Lab Sci. 1992;49:299�312.
92. Mezzetti A, Lapenna D, Romano F, Costantini F, Pierdomenico SD, et al. Systemic oxidative stress and its relationship with age and illness. J Am Geriatr Soc. 1996;44:823�827.
93. White E, Shannon JS, Patterson RE. Relationship between vitamin and
calcium supplement use and colon cancer. Cancer Epidemiol Biomarkers Prev. 1997;6:769�774.
94. Masella R, Di Benedetto R, Vari R, Filesi C, Giovannini C. Novel mechanisms of natural antioxidant compounds in biological systems: involvement of glutathione and glutathione-related enzymes. J Nutr Biochem. 2005;16:577�586.
95. Curello S, Ceconi C, Bigoli C, Ferrari R, Albertini A, Guarnieri C. Changes in the cardiac glutathione status after ischemia and reperfusion. Experientia. 1985;41:42�43.
96. El-Agamey A, Lowe GM, McGarvey DJ, Mortensen A, Phillip DM, Truscott TG. Carotenoid radical chemistry and antioxidant/pro-oxidant properties. Arch Biochem Biophys. 2004;430:37�48.
97. Rice-Evans CA, Sampson J, Bramley PM, Holloway DE. Why do we expect carotenoids to be antioxidants in vivo? Free Radic Res. 1997;26:381�398.
98. Niles RM. Signaling pathways in retinoid chemoprevention and treatment of cancer. Mutat Res. 2004;555:81�96.
99. Donato LJ, Noy N. Suppression of mammary carcinoma growth by retinoic acid: proapoptotic genes are targets for retinoic acid receptor and cellular retinoic acid-binding protein II signaling. Cancer Res. 2005;65:8193�8199.
100. Niizuma H, Nakamura Y, Ozaki T, Nakanishi H, Ohira M, et al. Bcl-2 is a key regulator for the retinoic acid-induced apoptotic cell death in neuroblastoma. Oncogene. 2006;25:5046�5055.
101. Dalton TP, Shertzer HG, Puga A. Regulation of gene expression by reactive oxygen. Ann Rev Pharmacol Toxicol. 1999;39:67�101.
102. Scandalios JG. Genomic responses to oxidative stress. In: Meyers RA, ed. Encyclopedia of Molecular Cell Biology and Molecular Medicine. Vol 5. 2nd ed. Weinheim, Germany: Wiley-VCH; 2004: 489�512.
103. Ghosh R, Mitchell DL. Effect of oxidative DNA damage in promoter elements on transcription factor binding. Nucleic Acids Res. 1999;27:3213�3218.
104. Marietta C, Gulam H, Brooks PJ. A single 8, 50-cyclo-20-deoxyadenosine lesion in a TATA box prevents binding of the TATA binding protein and strongly reduces transcription in vivo. DNA Repair (Amst). 2002;1:967�975.
105. Jackson AL, Chen R, Loeb LA. Induction of microsatellite instability
by oxidative DNA damage. Proc Natl Acad Sci U S A. 1998;95:12468�12473.
106. Caldecott KW. Protein-protein interactions during mammalian DNA single-strand break repair. Biochem Soc Trans. 2003;31:247�251.
107. Cooke MS, Evans MD, Dizdaroglu M, Lunec J. Oxidative DNA damage: mechanisms, mutation, and disease. FASEB J. 2003;17:1195�1214.
108. Jones PL, Wolffe AP. Relationships between chromatin organization and DNA methylation in determining gene expression. Semin Cancer Biol. 1999;9:339�347.
109. Girotti AW. Mechanisms of lipid peroxidation. J Free Radic Biol Med. 1985;1:87�95.
110. Siu GM, Draper HH. Metabolism of malonaldehyde in vivo and in vitro. Lipids. 1982;17:349�355.
111. Esterbauer H, Koller E, Slee RG, Koster JF. Possible involvement of the lipid-peroxidation product 4-hydroxynonenal in the formation of fluorescent chromolipids. Biochem J. 1986;239:405�409.
112. Hagihara M, Nishigaki I, Maseki M, Yagi K. Age-dependent changes in lipid peroxide levels in the lipoprotein fractions of human serum. J Gerontol. 1984;39:269�272.
113. Keller JN, Mark RJ, Bruce AJ, Blanc E, Rothstein JD, et al. 4- Hydroxynonenal, an aldehydic product of membrane lipid peroxidation, impairs glutamate transport and mitochondrial function in synaptosomes. Neuroscience. 1997;806:85�96.
114. Uchida K, Shiraishi M, Naito Y, Torii Y, Nakamura Y, Osawa T. Activation of stress signaling pathways by the end product of lipid peroxidation. 4-hydroxy-2-nonenal is a potential inducer of intracellular peroxide production. J Biol Chem. 1999;274:2234�2242.
115. Suc I, Meilhac O, Lajoie-Mazenc I, Vandaele J, Jurgens G, Salvayre R, Negre-Salvayre A. Activation of EGF receptor by oxidized LDL. FASEB J. 1998;12:665�671.
116. Tsukagoshi H, Kawata T, Shimizu Y, Ishizuka T, Dobashi K, Mori M. 4-Hydroxy-2-nonenal enhances fibronectin production by IMR-90 human lung fibroblasts partly via activation of epidermal growth factor receptor-linked extracellular signal-regulated kinase p44/42 pathway. Toxicol Appl Pharmacol. 2002;184:127�135.
117. Montuschi P, Collins JV, Ciabattoni G, Lazzeri N, Corradi M, Kharitonov SA, Barnes PJ. Exhaled 8-isoprostane as an in vivo biomarker of lung oxidative stress in patients with COPD and healthy smokers. Am J Respir Crit Care Med. 2000;162:1175�1177.
118. Morrison D, Rahman I, Lannan S, MacNee W. Epithelial permeability, inflammation, and oxidant stress in the air spaces of smokers. Am J Respir Crit Care Med. 1999;159:473�479.
119. Nowak D, Kasielski M, Antczak A, Pietras T, Bialasiewicz P. Increased content of thiobarbituric acid-reactive substances and hydrogen peroxide in the expired breath condensate of patients with stable chronic obstructive pulmonary disease: no significant effect of cigarette smoking. Respir Med. 1999;93:389�396.
120. Kelly FJ, Mudway IS. Protein oxidation at the air-lung interface. Amino Acids. 2003;25:375�396.
121. Dean RT, Roberts CR, Jessup W. Fragmentation of extracellular and intracellular polypeptides by free radicals. Prog Clin Biol Res. 1985;180:341�350.
122. Keck RG. The use of t-butyl hydroperoxide as a probe for methionine oxidation in proteins. Anal Biochem. 1996;236:56�62.
123. Davies KJ. Protein damage and degradation by oxygen radicals. I. General aspects. J Biol Chem. 1987;262:9895�9901.
124. Stadtman ER. Metal ion-catalyzed oxidation of proteins: biochemical mechanism and biological consequences. Free Radic Biol Med.
1990;9:315�325.
125. Fucci L, Oliver CN, Coon MJ, Stadtman ER. Inactivation of key metabolic enzymes by mixed-function oxidation reactions: possible implication in protein turnover and ageing. Proc Natl Acad Sci U S A. 1983;80:1521�1525.
126. Stadtman ER, Moskovitz J, Levine RL. Oxidation of methionine residues of proteins: biological consequences. Antioxid Redox Signal. 2003;5:577�582.
127. Stadtman ER, Levine RL. Free radical-mediated oxidation of free amino acids and amino acid residues in proteins. Amino Acids. 2003;25:207�218.
128. Stadtman ER. Protein oxidation in aging and age-related diseases. Ann N Y Acad Sci. 2001;928:22�38.
129. Shacter E. Quantification and significance of protein oxidation in biological samples. Drug Metab Rev. 2000;32:307�326.
130. Poli G, Leonarduzzi G, Biasi F, Chiarpotto E. Oxidative stress and cell signalling. Curr Med Chem. 2004;11:1163�1182.
131. Neufeld G, Cohen T, Gengrinovitch S, Poltorak Z. Vascular endothelial growth factor (VEGF) and its receptors. FASEB J. 1999;13:9�22.
132. Sundaresan M, Yu ZX, Ferrans VJ, Sulciner DJ, Gutkind JS, et al. Regulation of reactive-oxygen species generation in fibroblasts by Rac1. Biochem J. 1996;318:379�382.
133. Sun T, Oberley LW. Redox regulation of transcriptional activators. Free Radic Biol Med. 1996;21:335�348.
134. Klatt P, Molina EP, De Lacoba MG, Padilla CA, Martinez-Galesteo E, Barcena JA, Lamas S. Redox regulation of c-Jun DNA binding by reversible S-glutathiolation. FASEB J. 1999;13:1481�1490.
135. Reynaert NL, Ckless K, Guala AS, Wouters EF, van der Vliet A, Janssen Heininger
YM. In situ detection of S-glutathionylated proteins following glutaredoxin-1 catalyzed cysteine derivatization. Biochim Biophys Acta. 2006;1760:380�387.
136. Reynaert NL, Wouters EF, Janssen-Heininger YM. Modulation of glutaredoxin-1
expression in a mouse model of allergic airway disease. Am J Respir Cell Mol Biol. 2007;36:147�151.
137. Filomeni G, Rotilio G, Ciriolo MR. Cell signalling and the glutathione redox system. Biochem Pharmacol. 2002;64:1057�1064.
138. Pande V, Ramos MJ. Molecular recognition of 15-deoxydelta (12,14) prostaglandin J(2) by nuclear factor-kappa B and other cellular proteins. Bioorg Med Chem Lett. 2005;15:4057�4063.
139. Perkins ND. Integrating cell-signalling pathways with NF-kappaB and IKK function. Nat Rev Mol Cell Biol. 2007;8:49�62.
140. Gilmore TD. Introduction to NF-kappaB: players, pathways, perspectives. Oncogene. 2006;25:6680�6684.
141. Hirota K, Murata M, Sachi Y, Nakamura H, Takeuchi J, Mori K, Yodoi J. Distinct roles of thioredoxin in the cytoplasm and in the nucleus. A two-step mechanism of redox regulation of transcription factor NF-kappaB. J Biol Chem. 1999;274:27891�27897.
142. Ward PA. Role of complement, chemokines and regulatory cytokines in acute lung injury. Ann N Y Acad Sci. 1996;796:104�112.
143. Akira S, Kishimoto A. NF-IL6 and NF-kB in cytokine gene regulation. Adv Immunol. 1997;65:1�46.
144. Meyer M, Schreck R, Baeuerle PA. H2O2 and antioxidants have opposite effects on activation of NF-kappa B and AP-1 in intact cells: AP-1 as secondary antioxidant-responsive factor. EMBO J. 1993;12:2005�2015.
145. Abate C, Patel L, Rausher FJ, Curran T. Redox regulation of fos and jun DNA-binding activity in vitro. Science. 1990;249:1157�1161.
146. Galter D, Mihm S, Droge W. Distinct effects of glutathione disulphide on the nuclear transcription factors kB and the activator protein-1. Eur J Biochem. 1994;221:639�648.
147. Hirota K, Matsui M, Iwata S, Nishiyama A, Mori K, Yodoi J. AP-1 transcriptional activity is regulated by a direct association between thioredoxin and Ref-1. Proc Natl Acad Sci U S A. 1997;94: 3633�3638.
El Paso, Tx. Wellness chiropractor, Dr. Alexander Jimenez examines Functional Medicine.�What it�is and how it can help in having a healthy lifestyle.
The Challenge
Of total healthcare costs in the United States, more than 86% is due to chronic conditions.1 In 2015, health care spending reached $3.2 trillion, accounting for 17.8% of GDP.2 This exceeded the combined federal expenditures for national defense, homeland security, education, and welfare. By 2023, if we don�t change how we confront this challenge, annual healthcare costs in the U.S. will rise to over $4 trillion,3,4 the equivalent�in a single year�of four Iraq wars, making the cost of care using the current model economically unsustainable. If our health outcomes were commensurate with such costs, we might decide they were worth it. Unfortunately, the U.S. spends twice the median per-capita costs of other industrialized countries, as calculated by the Organization for Economic Cooperation and Development (OECD),5 despite having relatively poor outcomes for such a massive investment.6
Our current healthcare model fails to confront both the causes of and solutions for chronic disease and must be replaced with a model of comprehensive care geared to effectively treating and reversing this escalating crisis.This transformation requires something different than is usually available in our very expensive healthcare system.7
A Contributing Factor�Outdated Clinical Model
Despite notable advances in treating and preventing infectious disease and trauma, the acute-care model that dominated 20th century medicine has not been effective in treating and preventing chronic disease.
Adopting a new operating system for 21st century medicine requires that we:
Recognize and validate more appropriate and successful clinical models
Re-shape the education and clinical practices of health professionals to help them achieve proficiency in the assessment, treatment, and prevention of chronic disease
Reimburse equitably for lifestyle medicine and expanded preventive strategies, acknowledging that the greatest health threats now arise from how we live, work, eat, play, and move
This problem can�t be solved by drugs and surgery, however helpful those tools may be in managing acute signs and symptoms. It can�t be solved be adding new or unconventional tools, such as botanical medicine and acupuncture, to a failing model. It can�t be solved by pharmacogenomics (although advances in that discipline should help reduce deaths from inappropriately prescribed medication�estimated to be the fourth leading cause of hospital deaths12). The costly riddle of chronic disease can only be solved by shifting our focus from suppression and management of symptoms to addressing their underlying causes. Specifically, we must integrate what we know about how the human body works with individualized, patient-centered, science-based care that addresses the causes of complex, chronic disease, which are rooted in lifestyle choices, environmental exposures, and genetic influences.
This perspective is completely congruent with what we might call the �omics� revolution. Formerly, scientists believed that once we deciphered the human genome we would be able to answer almost all the questions about the origins of disease.What we actually learned, however, is that human biology is far more complex than that. In fact, humans are not genetically hardwired for most diseases; instead, gene expression is altered by myriad influences, including environment, lifestyle, diet, activity patterns, psycho-social-spiritual factors, and stress.These lifestyle choices and environmental exposures can push us toward (or away from) disease by turning on�or o � certain genes.That insight has helped to fuel the global interest in Functional Medicine, which has that principle at its very core.
A Strategic Response
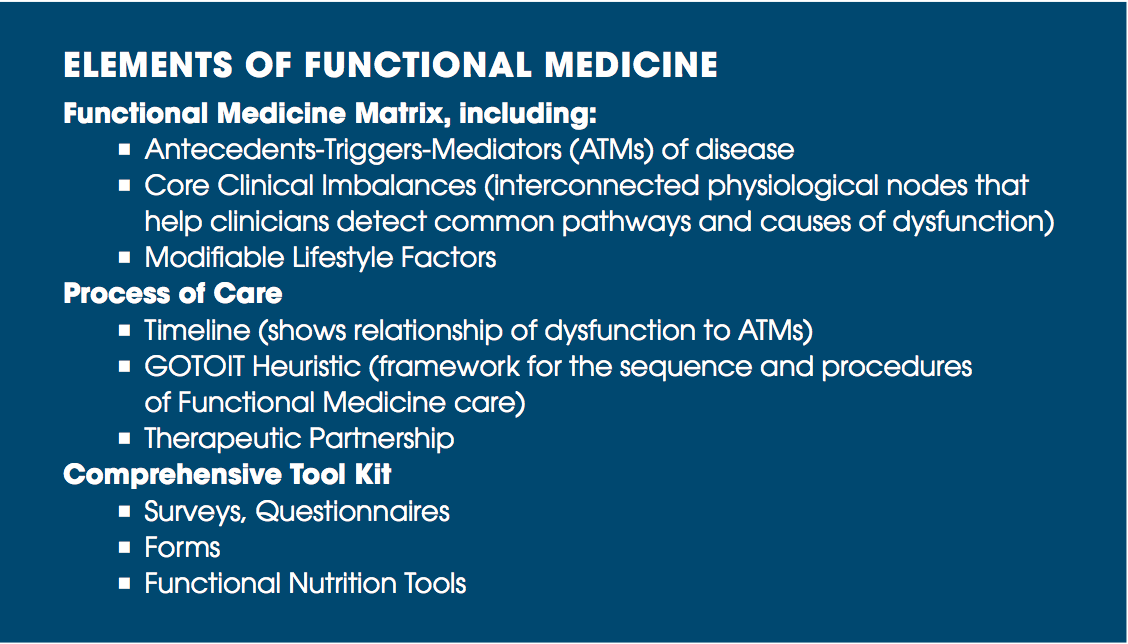
Functional Medicine directly addresses the underlying causes of disease by using a systems-oriented approach with transformative clinical concepts, original tools, an advanced process of care (see box below), and by engaging both patient and practitioner in a therapeutic partnership.
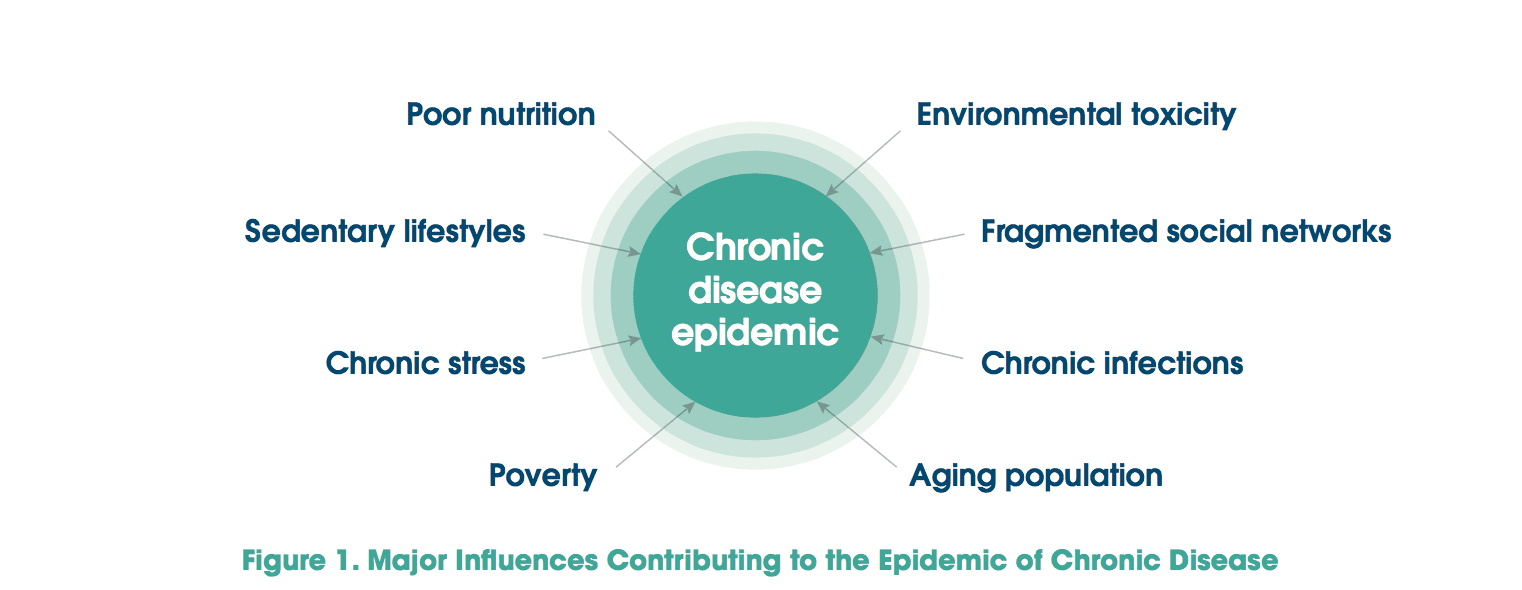
Functional Medicine practitioners look closely at the myriad interactions among genetic, environmental, and lifestyle factors that can influence long-term health and complex, chronic disease (see Figure 1).A major premise of Functional Medicine is that, with science, clinical wisdom, and innovative tools, we can identify many of the underlying causes of chronic disease and intervene to remediate the clinical imbalances, even before overt disease is present.
Functional Medicine exemplifies just the kind of systems-oriented, personalized medicine that is needed to transform clinical practice.The Functional Medicine model of comprehensive care and primary prevention for complex, chronic illness is grounded in both science (evidence about common underlying mechanisms and pathways of disease as well as evidence about the contributions of environmental and lifestyle factors to disease) and art (the healing partnership and the search for insight in the therapeutic encounter).
What Is Functional Medicine?
Functional Medicine asks how and why illness occurs and restores health by addressing the root causes of disease for each individual. It is an approach to health care that conceptualizes health and illness as part of a continuum in which all components of the human biological system interact dynamically with the environment, producing patterns and effects that change over time. Functional Medicine helps clinicians identify and ameliorate dysfunctions in the physiology and biochemistry of the human body as a primary method of improving patient health. Chronic disease is almost always preceded by a period of declining function in one or more of the body�s systems. Functional Medicine is often described as the clinical application of systems biology. Restoring health requires reversing (or substantially improving) the specific dysfunctions that have contributed to the disease state. Each patient represents a unique, complex, and interwoven set of environmental and lifestyle influences on intrinsic functionality (their genetic vulnerabilities) that have set the stage for the development of disease or the maintenance of health.
To manage the complexity inherent in this approach, IFM has created practical models for obtaining and evaluating clinical information that lead to individualized, patient-centered, science-based therapies. Functional Medicine concepts, practices, and tools have evolved considerably over a 30-year period, reflecting the dramatic growth in the evidence base concerning the key common pathways to disease (e.g., inflammation, oxidative stress); the role of diet, stress, and physical activity; the emerging sciences of genomics, proteomics, and metabolomics; and the effects of environmental toxins (in the air, water, soil, etc.) on health.
Elements Of Functional Medicine
The knowledge base�or �footprint��of Functional Medicine is shaped by six core foundations:
Gene-Environment Interaction: Functional Medicine is based on understanding the metabolic processes of each individual at the cellular level. By knowing how each person�s genes and environment interact to create their unique biochemical phenotype, it is possible to design targeted interventions that correct the specific issues that lead to destructive processes such as inflammation and oxidation, which are at the root of many diseases.
Upstream Signal Modulation: Functional Medicine interventions seek to influence biochemical pathways �upstream� and prevent the overproduction of damaging end products, rather than blocking the effects of those end products. For example, instead of using drugs that block the last step in the production of inflammatory mediators (NSAIDs, etc.), Functional Medicine treatments seek to prevent the upregulation of those mediators in the first place.
Multimodal Treatment Plans: The Functional Medicine approach uses a broad range of interventions to achieve optimal health including diet, nutrition, exercise and movement; stress management; sleep and rest, phytonutrient, nutritional and pharmaceutical supplementation; and various other restorative and reparative therapies.These interventions are all tailored to address the antecedents, triggers, and mediators of disease or dysfunction in each individual patient.
Understanding the Patient in Context: Functional Medicine uses a structured process to uncover the significant life events of each patient�s history to gain a better understanding of who they are as an individual. IFM tools (the �Timeline� and the �Matrix� model) are integral to this process for the role they play in organizing clinical data and mediating clinical insights.This approach to the clinical encounter ensures that the patient is heard, engenders the therapeutic relationship, expands therapeutic options, and improves the collaboration between patient and clinician.
Systems Biology-Based Approach: Functional Medicine uses systems biology to understand and identify how core imbalances in specific biological systems can manifest in other parts of the body. Rather than an organ systems-based approach, Functional Medicine addresses core physiological processes that cross anatomical boundaries including: assimilation of nutrients, cellular defense and repair, structural integrity, cellular communication and transport mechanisms, energy production, and biotransformation.The �Functional Medicine Matrix� is the clinician�s key tool for understanding these network effects and provides the basis for the design of effective multimodal treatment strategies.
Patient-Centered and Directed: Functional Medicine practitioners work with the patient to find the most appropriate and acceptable treatment plan to correct, balance, and optimize the fundamental underlying issues in the realms of mind, body, and spirit. Beginning with a detailed and personalized history, the patient is welcomed into the process of exploring their story and the potential causes of their health issues. Patients and providers work together to determine the diagnostic process, set achievable health goals, and design an appropriate therapeutic approach.
To assist clinicians in understanding and applying Functional Medicine, IFM has created a highly innovative way of representing the patient�s signs, symptoms, and common pathways of disease. Adapting, organizing, and integrating into the Functional Medicine Matrix the seven biological systems in which core clinical imbalances are found actually creates an intellectual bridge between the rich basic science literature concerning physiological mechanisms of disease and the clinical studies, clinical diagnoses, and clinical experience acquired during medical training.These core clinical imbalances serve to marry the mechanisms of disease with the manifestations and diagnoses of disease.
Structural integrity: sub-cellular membranes to musculoskeletal integrity
Using this construct, it is possible to see that one disease/condition may have multiple causes (i.e., multiple clinical imbalances), just as one fundamental imbalance may be at the root of many seemingly disparate conditions (see Figure 2).
Constructing The Model & Putting It Into Practice
The scientific community has made incredible strides in helping practitioners understand how environment and lifestyle, interacting continuously through an individual�s genetic heritage, psychosocial experiences, and personal beliefs, can impair one or all of the seven core clinical imbalances. IFM has developed concepts and tools that help to collect, organize, and make sense of the data gathered from an expanded history, physical exam, and laboratory evaluation, including:
The GOTOIT system, which presents a logical method for eliciting the patient�s whole story and ensuring that assessment and treatment are in accord with that story:
G = Gather Information
O = Organization Information
T = Tell the Complete Story Back to the Patient
O = Order and Prioritize
I = InitiateTreatment
T = Track Outcomes
The Functional Medicine Timeline, which helps to connect key events in the patient�s life with the onset of symptoms of dysfunction.
The Functional Medicine Matrix, which provides a unique and succinct way to organize and analyze all of a patient�s health data (see Figure 3).
The patient�s lifestyle influences are entered across the bottom of the Matrix, and the Antecedents,Triggers, and Mediators (ATMs) of disease/dysfunction are entered in the upper left corner.The centrality of the patient�s mind, spirit, and emotions, with which all other elements interact, is clearly shown in the figure. Using this information architecture, the clinician can create a comprehensive snapshot of the patient�s story and visualize the most important clinical elements of Functional Medicine:
1. Identifying each patient�s ATMs of disease and dysfunction.
2. Discovering the factors in the patient�s lifestyle and environment that influence the expression of health or disease.
3. Applying all the data collected about a patient to a matrix of biological systems, within which disturbances in function originate and are expressed.
4. Integrating all this information to create a comprehensive picture of what is causing the patient�s problems, where they are originating, what has influenced their development, and�as a result of this critical analysis�where to intervene to begin reversing the disease process or substantially improving health.
A Functional Medicine treatment plan may involve one or more of a broad range of therapies, including many different dietary interventions (e.g., elimination diet, high phytonutrient diversity diet, low glycemic-load diet), nutraceuticals (e.g., vitamins, minerals, essential fatty acids, botanicals), and lifestyle changes (e.g., improving sleep quality/quantity, increasing physical activity, decreasing stress and learning stress management techniques, quitting smoking). Nutrition is so vital to the practice of Functional Medicine that IFM has established a core emphasis on Functional Nutrition and has funded the development of a set of unique, innovative tools for developing and applying dietary recommendations.
Scientific support for the Functional Medicine approach to treatment can be found in a large and rapidly expanding evidence base about the therapeutic effects of nutrition (including both dietary choices and the clinical use of vitamins, minerals, and other nutrients such as sh oils)13,15,15; botanicals16,17,18; exercise19 (aerobics, strength training, flexibility); stress management 20; detoxification 21,22,23; acupuncture�24,25,26; manual medicine (massage, manipulation)27,28,29; and mind/body techniques 30,31,32 such as meditation, guided imagery, and biofeedback.
All of this work is done within the context of an equal partnership between the practitioner and patient.The practitioner engages the patient in a collaborative relationship, respecting the patient�s role and knowledge of self, and ensuring that the patient learns to take responsibility for their own choices and for complying with the recommended interventions. Learning to assess a patient�s readiness to change and then providing the necessary guidance, training, and support are just as important as ordering the right lab tests and prescribing the right therapies.
Summary
The practice of Functional Medicine involves four essential components: (1) eliciting the patient�s complete story during the Functional Medicine intake; (2) identifying and addressing the challenges of the patient�s modifiable lifestyle factors and environmental exposures; (3) organizing the patient�s clinical imbalances by underlying causes of disease in a systems biology matrix framework; and (4) establishing a mutually empowering partnership between practitioner and patient.
A great strength of Functional Medicine is its relevance to all healthcare disciplines and medical specialties, any of which can�to the degree allowed by their training and licensure�apply a Functional Medicine approach, using the Matrix as a basic template for organizing and coupling knowledge and data. In addition to providing a more effective approach to preventing, treating, and reversing complex chronic disease, Functional Medicine can also provide a common language and a uni ed model that can be applied across a wide variety of health professions to facilitate integrated care.
Functional Medicine is playing a key role in the effort to solve the modern epidemic of chronic disease that is creating a health crisis both nationally and globally. Because chronic disease is a food- and lifestyle-driven, environment- and genetics-influenced phenomenon, we must have an approach to care that integrates all these elements in the context of the patient�s complete story. Functional Medicine does just that and provides an original and creative approach to the collection and analysis of this broad array of information. Using all the concepts and tools that IFM has developed, Functional Medicine practitioners contribute vital skills for treating and reversing complex, chronic disease.
3 DeVol R, Bedroussian A. An unhealthy America: the economic burden of chronic disease�charting a new course to save lives and increase productivity and economic growth. Milken Institute; 2007. Accessed April 14, 2017, assets1c.milkeninstitute.org/assets/Publication/ResearchReport/PDF/chronic_disease_report.pdf.
4 Bodenheimer T, Chen E, Bennett H. Confronting the growing burden of chronic disease: can the U.S. health care workforce do the job? Health Aff. 2009;28(1):64-74. doi: 10.1377/hlthaff.28.1.64.
5 Bureau of Labor Education, University of Maine. The U.S. Health Care System: Best in the World, Or Just the Most Expensive? 2001. Accessed April 14, 2017, www.suddenlysenior.com/pdf_files/U.S.healthcare.pdf.
6 Radley DC, McCarthy D, Hayes SL. Aiming higher: results from the Commonwealth Fund scorecard on state health system performance (2017 ed.). The Commonwealth Fund; 2017. Accessed April 14, 2017, www.commonwealthfund.org/interactives/2017/mar/state-scorecard/.
7 Jones DS, Hofmann L, Quinn S. 21st century medicine: a new model for medical education and practice. Gig Harbor, WA: The Institute for Functional Medicine; 2011.
8 Jones DS, Hofmann L, Quinn S. 21st century medicine: a new model for medical education and practice. Gig Harbor, WA: The Institute for Functional Medicine; 2009.
9 Willett WC. Balancing life-style and genomics research for disease prevention. Science. 2002; 296(5568):695-97. doi: 10.1126/science.1071055.
10 Thorpe KE, Florence CS, Howard H, Joski P. The rising prevalence of treated disease: effects on private health insurance spending. Health Aff. 2005;Suppl Web Exclusives: W5-317-W5-325. doi: 10.1377/hlthaff.w5.317.
11 Heaney RP. Long-latency deficiency disease: insights from calcium and vitamin D. Am J Clin Nutr. 2003;78(5):912-9.
12 Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA. 1998; 279(15):1200-05.
13 Ames BN, Elson-Schwab I, Silver EA. High-dose vitamin therapy stimulates variant enzymes with decreased coenzyme binding affinity (increased K(m)): relevance to genetic disease and polymorphisms. Am J Clin Nutr. 2002;75(4):616-58.
14 Lands B. Prevent the cause, not just the symptoms. Prostaglandins Other Lipid Mediat. 201;96(1-4):90-3. doi: 10.1016/j.prostaglandins.2011.07.003.
15 Sofi F, Abbate R, Gensini GF, Casini A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: an updated systematic review and meta-analysis. Am J Clin Nutr. 2010;92(5):1189-96. doi: 10.3945/ajcn.2010.29673.
16 Mulrow C, Lawrence V, Jacobs B, et al. Milk thistle: effects on liver disease and cirrhosis and clinical adverse effects (No. 21). Rockville, MD: Agency for Healthcare Research and Quality; 2000. Accessed April 14, 2017, www.pkids.org/files/milkthistle.pdf.
17 National Center for Complementary and Integrative Health. Green Tea; 2016. Accessed April 14, 2017, nccih.nih.gov/health/greentea.
18 National Center for Complementary and Integrative Health. St. John�s Wort; 2016. Accessed April 14, 2017, nccih.nih.gov/health/stjohnswort/ataglance.htm.
19 McArdle WD, Katch EI, Katch VL. Exercise Physiology: Energy, Nutrition, and Human Performance. Philadelphia: Lippincott Williams and Wilkins; 2001.
20 McCraty R, Childre D. Coherence: bridging personal, social, and global health. Altern Ther Health Med. 2010;16(4):10-24.
21 Yi B, Kasai H, Lee HS, Kang Y, Park JY, Yang M. Inhibition by wheat sprout (Triticum aestivum) juice of bisphenol A-induced oxidative stress in young women. Mutat Res. 2011;724(1-2):64-68. doi: 10.1016/j.mrgentox.2011.06.007.
22 Johnson CH, Patterson AD, Idle JR, Gonzalez FJ. Xenobiotic metabolomics: major impact on the metabolome. Annu Rev Pharmacol Toxicol. 2012;52:37-56. doi: 10.1146/annurev-pharmtox-010611-134748.
23 Scapagnini G, Caruso C, Calabrese V. Therapeutic potential of dietary polyphenols against brain ageing and neurodegenerative disorders. Adv Exp Med Biol. 2010;698:27-35.
24 Colak MC, Kavakli A, Kilin� A, Rahman A. Postoperative pain and respiratory function in patients treated with electroacupuncture following coronary surgery. Neurosciences (Riyadh). 2010;15(1):7-10.
25 Cao H, Pan X, Li H, Liu J. Acupuncture for treatment of insomnia: a systematic review of randomized controlled trials. J Altern Complement Med. 2009;15(11):1171-86. doi: 10.1089/acm.2009.0041.
26 Lee A, Fan LT. Stimulation of the wrist acupuncture point P6 for preventing postoperative nausea and vomiting. Cochrane Database Syst Rev. 2009;15(2):CD003281. doi: 10.1002/14651858.
27 Rubinstein SM, Leboeuf-Yde C, Knol DL, de Koekkoek TE, Pfeifle CE, van Tulder MW. The benefits outweigh the risks for patient undergoing chiropractic care for neck pain: a prospective, multicenter, cohort study. J Manipulative Physiol Ter. 2007;30(6):408-1. doi: 10.1016/j.jmpt.2007.04.013.
28 Beyerman KL, Palmerino MB, Zohn LE, Kane GM, Foster KA. Efficacy of treating low back pain and dysfunction secondary to osteoarthritis: chiropractic care compared to moist heat alone. J Manipulative Physiol Ther. 2006;29(2):107-14. doi: 10.1016/j.jmpt.2005.10.005.
29 Kshettry VR, Carole LF, Henly SJ, Sendelbach S, Kummer B. Complementary alternative medical therapies for heart surgery patients: feasibility, safety, and impact. Ann Thorac Surg. 2006;81(1):201-5. doi: 10.1016/j.athoracsur.2005.06.016.
30 Ornish D, Magbanua MJM, Weidner G, et al. Changes in prostate gene expression in men undergoing an intensive nutrition and lifestyle intervention. PNAS. 2008;105(24):8369-74. doi: 10.1073/pnas.0803080105.
31 Xiong GL, Doraiswamy PM. Does meditation enhance cognition and brain plasticity? Ann NY Acad Sci. 2009;1172:63-9. doi: 10.1196/annals.1393.002.
32 H�lzel BK, Carmody J, Vangel M, et al. Mindfulness practice leads to increases in regional brain gray matter density. Psychiatry Res. 2011;191(1):36-43. doi: 10.1016/j.pscychresns.2010.08.006.
Question: I’ve had back pain for awhile and I was able to function through it for a time. But now it’s taking its toll on me, as well as my family. I never believed in chiropractors, but now I’ll try anything. What should I ask my physician about chiropractic?
El Paso, TX. Chiropractor, Dr. Alexander Jimenez has seen this scenario all too often and is happy to inform anyone about chiropractic care and it’s benefits.
About two out of every three people will likely experience significant low back pain at some point. A doctor might suggest any range of potential treatments and therapies. But one that almost is never considered is a referral for spinal manipulation.
It seems doctors have been mistaken for initial treatment of lower back pain.�It may be time for doctors to rethink their chiropractic biases.
Spinal Manipulation:
Along with other less traditional therapies like heat, acupuncture and meditation, chiropractic appears to be as powerful as any other medical treatments doctors prescribe and as safe, if not safer.
Physicians are traditionally wary of spinal manipulation (applying pressure on bones and joints), in part because the practitioners are often not doctors. Patients with back pain don’t seem as skeptical. A survey from 2002 through 2008 found that over 30 percent sought chiropractic care, significantly more than those who sought massage, acupuncture or homeopathy.
Researchers have been looking at the evidence supporting spinal manipulation for a while. Nearly 35 years ago, a systematic review assessed the available research found that there may be some short-term benefits from the process. Two reviews from 2003 agreed for the most part, finding that spinal manipulation worked better than a “sham procedure”, or placebo, but no better or worse than other options.
Recently, in The Journal of the American Medical Association, researchers looked for new studies since 2011, in addition to those that had been performed before.
Evidence from 15 randomized controlled trials, which included more than 1,700 patients, revealed that spinal manipulation minimized their back pain of about 10 points on a 100-point scale. The evidence from 12 randomized controlled trials that overlapped of almost 1,400 patients showed that spinal manipulation also resulted in improved mobility and function.
In February, in Annals of Internal Medicine, another systematic review of non-pharmacologic therapies generally agreed with the recent trials. Based on this review, and other evidence, the American College of Physicians released new clinical practice guidelines for the noninvasive treatment of back pain. They recommended that patients should try spinal manipulation, heat, massage and acupuncture as first-line therapies.
What If The Spinal Adjustment Causes Other Injuries:
Because of the fear of those injuries, physicians are hesitant to refer patients to chiropractors or physical therapists for care. However, in the studies outlined above, there were no serious adverse events reported. It is possible to find stories of injury to the spine from improper adjustments, but these are rare, and almost never involve the lower spine.
What About The Cost:
Some doctors are concerned about the cost of chiropractic, especially since many insurance carriers don’t cover chiropractic. Seeing a chiropractor costs more than taking many non-narcotic pain medications. However, more invasive interventions cost a lot of money. In addition, studies have proven that, in general, users of complementary and alternative medicine spend less for back pain compared to users of only traditional medicine.
Medication and surgery may also result in injuries and prescription pain medicines, like opioids, may result in huge costs, particularly when they’re misused.
Some physicians are uncomfortable that they do not have a clear picture of how spinal manipulation actually works. The reality is that doctors don’t understand why a number of other therapies work either.
Back pain is still the issue and no matter what you do, chiropractic is definitely an option to consider.
Chiropractic: Alternative Approach To Treating Chronic Pain
Question: My car was rear-ended. Since then, my neck hurts, feels rigid, and I have upper back pain. My wife says it’s whiplash and that I should see a physician. Is there anything that I can do to accelerate my recovery? Should I see my physician and/or chiropractor? How long will my pain last?
El Paso, TX
Answer: Your symptoms are typical of a whiplash injury caused by a vehicle accident. Whiplash is cervical spine strain caused when the head and neck are thrust quickly forward and backward. To fully grasp how whiplash can lead to neck pain, you want to recognize the head, which weighs 8-13 pounds and is supported and moved by the neck. Because of this, it’s easy to understand how soft neck muscles and ligaments are stretched during a whiplash accident!
The seriousness of whiplash is dependent on the force of the impact, the way you were seated in your vehicle, and if you were properly restrained with a shoulder and seat belt. By way of instance, if your head was turned, your neck injury may be more painful.
Whiplash Home Treatment Tips
1. Even though your neck injury occurred last week, you may try ice and heat. Ice will help to reduce swollen overstretched muscles and ligaments. Heat increases circulation and eases tight stiff muscles.
Ice: Apply an ice pack for 15 minutes as often as once each hour.
Heat: Apply warmth (moist is greatest!) For 15 minutes every 2 or 3 hours.
Skin Safety:
Never sleep with a ice or heat pack!
Wrap heat or ice in a towel to protect your skin.
Discard punctured store-bought ice or heat products.
2. If your doctor agrees, try an over-the-counter anti-inflammatory medication.
3. Move your neck softly to assist in preventing additional stiffness.
4. Should you work in a computer or desk, take regular breaks to relax your neck muscles.
5. Avoid cradling the phone between your shoulder and head.
6. Avoid carrying heavy packages, especially things such as a pocket book or backpack slung over only one shoulder.
Check With Your Doctor & Chiropractor
Neck pain is common either immediately after or several days following a whiplash injury. Other symptoms can develop too. Fortunately, most symptoms go away in two to four weeks. If your symptoms worsen, or you develop headache, dizziness, blurred vision, difficulty swallowing, arm or hand numbness, check-in with your physician or chiropractor. If necessary, you’ll be referred to a spine specialist.
Your physician or chiropractor will carry out a physical and neurological examination, and acquire a neck X-ray. After they produce a diagnosis, treatment is coordinated for your recovery! Treatment may include prescription pain medication, anti inflammatory drugs, muscle relaxants, a cervical collar, massage and physical therapy.
Other�Symptoms Associated With Whiplash Or Neck Strain:
Headache
Dizziness
Ringing in your ears
Blurred vision
Difficulty concentrating
Difficulty chewing or swallowing
Hoarse voice
Upper back, shoulder, and/ or arm pain
Back pain
Abnormal sensations such as numbness, burning or prickling
Fatigue and sleep problems
Keep in Mind
Most individuals with whiplash improve quickly within a matter of weeks. When you have concerns, we recommend you to speak to a doctor or chiropractor.
For many athletes following any major endurance event they will return to their houses, to recover, celebrate, reflect and rebuild to their next career step. Some, like the athlete in this case study will need to now focus attention on delayed decisions concerning whether to go under the knife to sort out a chronic injury.�El Paso, TX’s Injury scientist, Dr. Alexander Jimenez takes a look at the study.
My client has been competing in triathlon for 10 or more years, although his career has included a range of serious injuries which have kept him from races for months on end. In the previous two to three decades, however, he’s enjoyed a sustained period of injury-free training and racing, and has climbed to the peak of the world rankings. But the emergence of hip pain has seen him once more return to the physio’s table.
The triathlete’s accident history highlights a common pattern among sportspeople: 2 tibial stress fractures, a femoral neck stress fracture and a serious ankle sprain — every one of these on his right side. The significant contributing element to the bone stress injuries is a 1.5cm leg-length gap (his right leg is shorter).
He’d first experienced comparable hip pain in 2004; it kept him from running for three months. At that time, nothing was detected on a bone scan or MRI, or so the pain went paralyzed. An intra-articular cortisone injection (CSI) elicited no improvement. The athlete remembers that he chose to train on his painful hip, never allowing the symptoms to settle. The nearest he ever came into an investigation was a hypothesis that he could have a little, undetected, labral lesion.
The present episode of hip pain began initially at night after a hard three-hour bicycle ride. Earlier this, however, he hadn’t cycled for five times. He described his initial symptom as a profound hip tightness (lateral and lateral), together with slight pain in his groin. He was able to continue to train however, was feeling that the hip tightness and pain following both cycling and running (swimming was symptom-free).
A week later his symptoms dramatically worsened when he flew from Australia to Singapore, on his way to a French high- altitude camp. As he got off the airplane, he felt deep hip pain as well as the tightness. As elite athletes tend to do, he coached anyway, running a tricky track session, which made the hip much worse: he was unable to ride or run without pain. He instantly started a course of anti- inflammatories.
I met him in Singapore and evaluated him in the airport, initially ruling out any prospect of a disease or systemic matter. He explained he had been feeling an ache during the night, lying in bed; on waking, the hip would be OK, but got worse the longer he walked.
On assessment, he had the following physical signs:
� walking with obvious limp
� pain on hopping (6/10)
�painful right hip quadrant/impingement test (full hip flexion/adduction)
� reduced right hip flexion (-10 degrees compared to left)
� reduced right hip internal rotation (-10 degrees compared to left)
� increased tone on palpation of TFL, adductors, hip flexors, gluteal, piriformis and deep rotators
� lumbar spine and SIJ were OK
� femoral shaft bone stress test was OK � leg length discrepancy (right side 1.5cm shorter)
� right innominate (pelvis) anteriorly rotated
� weakness in right hip abductors/extensors
� reduced calf endurance on right side (-5 reps)
� ankle dorsiflexion range of movement was OK
� reduced proprioception on right (single leg stance, eyes closed).
I thought the differential diagnoses were:
� femoral neck stress fracture
� labral tear, possibly with hip synovitis
� FAI (femoro-acetabular impingement), possibly with hip synovitis.
I initially treated the triathlete with soft- tissue techniques to reduce the tone around the hip joint. Trigger-point releases were performed on his TFL, adductors, gluteals, piriformis, deep rotators and iliopsoas.�This reduced his jump pain into 3/10. Manual long-leg grip further decreased the strain on hopping (2/10). He still had pain and stiffness on walking but it sensed “simpler. As he prepared to embark on his long run flight to Europe, I counseled him to not sit for too long and maintain his stylish as straight as possible to decrease any potential impingement from hip flexion.
Luckily, the hip didn’t get worse throughout the flight. On arrival at the French high-altitude training centre, we initiated a strategy of two swims and two intensive treatments a day, aiming at reducing muscle tone, restoring his range of hip movement and normal muscle control and stamina. We had been expecting that the problem was not a stress fracture, but just minor hip synovitis that could settle quickly. Following a week of conservative treatment, though, we were just able to keep his hop pain in 2/10, and that he still could not run 20 meters without any pain and limping.
In collaboration with medics, we flew to London to see a sports doctor and get MRI scans. The scans revealed no bone stress reaction, fracture or labral ripping — which was a big relief; however, it did show signs consistent with FAI (femoro-acetabular impingement). He had hip synovitis with a rectal lesion on his femur.
Hip injuries aren’t much reported among triathletes — in fact they are notably absent from reports on Olympic and Ironman triathlons, which mention knee, back, H/ Achilles, lower leg, ankle and shoulder as the most common accidents (1-3).
In this state, when the hip is in maximum flexion and internal rotation, the labrum and cartilage abut and impinge; damage to the articular cartilage and acetabular labrum results from this pathologic bony contact. The contact generally results in a structural abnormality of the femur (“camera impingement”) along with the acetabulum (“pincer impingement”) or a combination of both (“mixed impingement”). Over time, via repetitive micro-trauma, the aggravating motion hurts the hip cartilage or labrum (or both) during normal joint motion. This happens along the anterior femoral neck and the anterior–superior acetabular rim. FAI is a possible trigger of early hip joint degeneration (4).
Arthroscopic surgery is the direction of choice for FAI if symptoms do not settle; however as his next Competition was only three and a half a year off, surgery was not an option. Instead, over a five-day interval, the athlete had two cortisone (CSI) and local anesthetic injections into the hip joint (under ultrasound guidance) to settle the indicators.
Our aim was to grow the hip range of motion and extend the capsule to reduce any additional impingement, slowly returning to regular training. Following the competition, the athlete would then should see a hip arthroscopic surgeon to acquire a surgical opinion to the best option for long-term direction.
Injection Relief
After both shots my customer felt sore for five days. The initial CSI settled his pain on hopping to 1/10 and after seven days he managed to operate without symptoms. But minor hip stiffness and aching at the end of the day prevented him from progressing to optimal training, so that he then underwent a second steroid injection. This settled the hop pain into 0/10 and decreased the aching; so after five times he returned to mild cycling and after seven days he started running again, also.
The athlete admitted that, following the first shot, he had done more and gone tougher in training than directed, as he had felt “good. This mistake of “too much too soon — all too common in elite athletes — had led to excessive inflammation and aching in the hip nightly after training. After the next injection he returned to normal intensity slower and more gradually.
My client built his training up to regular levels by four months following the final injection (swimming five times per week, cycling four days and running six to seven days). He began with very easy cycling on a wind trainer for 30 minutes, building slowly to 90 minutes before cycling on the street. He cycled two days on and one day away and avoided hills to the first two weeks. He started jogging on the apartment for 15 minutes and slowly built up to 90 minutes after three weeks. He did not run hills or about the track; and as he ran only on every single day, he would diligently concentrate on technique.
From week six to week 11, my client remained on anti inflammatory medication and underwent two treatments a day.
The hands-on treatment continued to:
� increase hip range of movement
� stretch the hip capsule
� normalise pelvic symmetry and hip muscle tone
� improve muscle control and strength � improve proprioception
� ensure optimal biomechanics via video assessment (cycling and running).
Eleven weeks after he first felt his hip pain, the triathlete returned to racing; however he failed to finish the first race, partially because of minor hip stiffness but mainly due to “fitness. Fortunately there were not any prolonged symptoms after the race and a week after he successfully returned to competition, coming second in a really strong field. His very minor ongoing symptoms were handled with anti-inflammatory drugs and hands-on treatments.
If this athlete wants to pursue a long- term triathlon career up to the London Olympics, then he will now require surgery. The arthroscopic surgical technique initially assesses the cartilage and labral surfaces, debrides any abnormalities of the hip joint cartilage and hip labrum, removes the non-spherical segments of the femoral head�and any prominent sections of the anterior femoral neck and bony growths on the acetabular rim that may continue to contribute to hip joint impingement.�The alternative is early joint degeneration and onset of osteoarthritis.
References:
1. Wilk B et al: �The incidence of musculoskeletal injuries in an amateur triathlete racing club�. J Orthop Sports Phys
Ther 1995 Sep;22(3):108-12.
2. Collins K et al: �Overuse injuries in triathletes. A study of the 1986 Seafair Triathlon�. Am J Sports Med 1989 SepOct;17(5):675-80.
3. Korkia PK et al: �An epidemiological investigation of training and injury patterns in British triathletes�. Br J Sports Med 1994 Sep;28(3):191-6.
4. Ganz R. et al (2003): �Femoroacetabular impingement: a cause for osteoarthritis of the hip�. Clin Orthop Relat Res. 417:112�120. For more information see: www.hipfai.com
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine



 The prevalence of obesity in the United States has been increasing for almost 50 years. Currently, more than two-thirds of adults and almost one-third of children and adolescents are
The prevalence of obesity in the United States has been increasing for almost 50 years. Currently, more than two-thirds of adults and almost one-third of children and adolescents are 
 From 2005 to 2014, there was a 1.4% annual increase in cancers related to overweight and obesity among individuals aged 20 to 49 years and a 0.4% increase in these cancers among individuals aged 50 to 64 years. For example, if cancer rates had stayed the same in 2014 as they were in 2005, there would have been 43?000 fewer cases of colorectal cancer but 33?000 more cases of other cancers related to overweight and obesity. Nearly half of all cancers in people younger than 65 years were associated with overweight and obesity. Overweight and obesity among younger people may exact a toll on individuals� health earlier in their lifetimes.
From 2005 to 2014, there was a 1.4% annual increase in cancers related to overweight and obesity among individuals aged 20 to 49 years and a 0.4% increase in these cancers among individuals aged 50 to 64 years. For example, if cancer rates had stayed the same in 2014 as they were in 2005, there would have been 43?000 fewer cases of colorectal cancer but 33?000 more cases of other cancers related to overweight and obesity. Nearly half of all cancers in people younger than 65 years were associated with overweight and obesity. Overweight and obesity among younger people may exact a toll on individuals� health earlier in their lifetimes.
 The
The  Implementation of clinical interventions, including screening, counseling, and referral, has major challenges. Since 2011, Medicare has covered behavioral counseling sessions for weight loss in primary care settings. However, the benefit has not been widely utilized.
Implementation of clinical interventions, including screening, counseling, and referral, has major challenges. Since 2011, Medicare has covered behavioral counseling sessions for weight loss in primary care settings. However, the benefit has not been widely utilized. Achieving sustainable weight loss requires comprehensive strategies that support patients� efforts to make significant lifestyle changes. The availability of clinical and community programs and services to which to refer patients is critically important. Although such programs are available in some communities, there are gaps in availability. Furthermore, even when these programs are available, enhancing linkages between clinical and community care could improve patients� access. Linking community obesity prevention, weight management, and physical activity programs with clinical services can connect people to valuable prevention and intervention resources in the communities where they live, work, and play. Such linkages can give individuals the encouragement they need for the lifestyle changes that maintain or improve their health.
Achieving sustainable weight loss requires comprehensive strategies that support patients� efforts to make significant lifestyle changes. The availability of clinical and community programs and services to which to refer patients is critically important. Although such programs are available in some communities, there are gaps in availability. Furthermore, even when these programs are available, enhancing linkages between clinical and community care could improve patients� access. Linking community obesity prevention, weight management, and physical activity programs with clinical services can connect people to valuable prevention and intervention resources in the communities where they live, work, and play. Such linkages can give individuals the encouragement they need for the lifestyle changes that maintain or improve their health. The high prevalence of overweight and obesity in the United States will continue to contribute to increases in health consequences related to obesity, including cancer. Nonetheless, cancer is not inevitable; it is possible that many cancers related to overweight and obesity could be prevented, and physicians have an important responsibility in educating patients and supporting patients� efforts to lead healthy lifestyles. It is important for all health care professionals to emphasize that along with quitting or avoiding tobacco, achieving and maintaining a healthy weight are also important for reducing the risk of cancer.
The high prevalence of overweight and obesity in the United States will continue to contribute to increases in health consequences related to obesity, including cancer. Nonetheless, cancer is not inevitable; it is possible that many cancers related to overweight and obesity could be prevented, and physicians have an important responsibility in educating patients and supporting patients� efforts to lead healthy lifestyles. It is important for all health care professionals to emphasize that along with quitting or avoiding tobacco, achieving and maintaining a healthy weight are also important for reducing the risk of cancer.