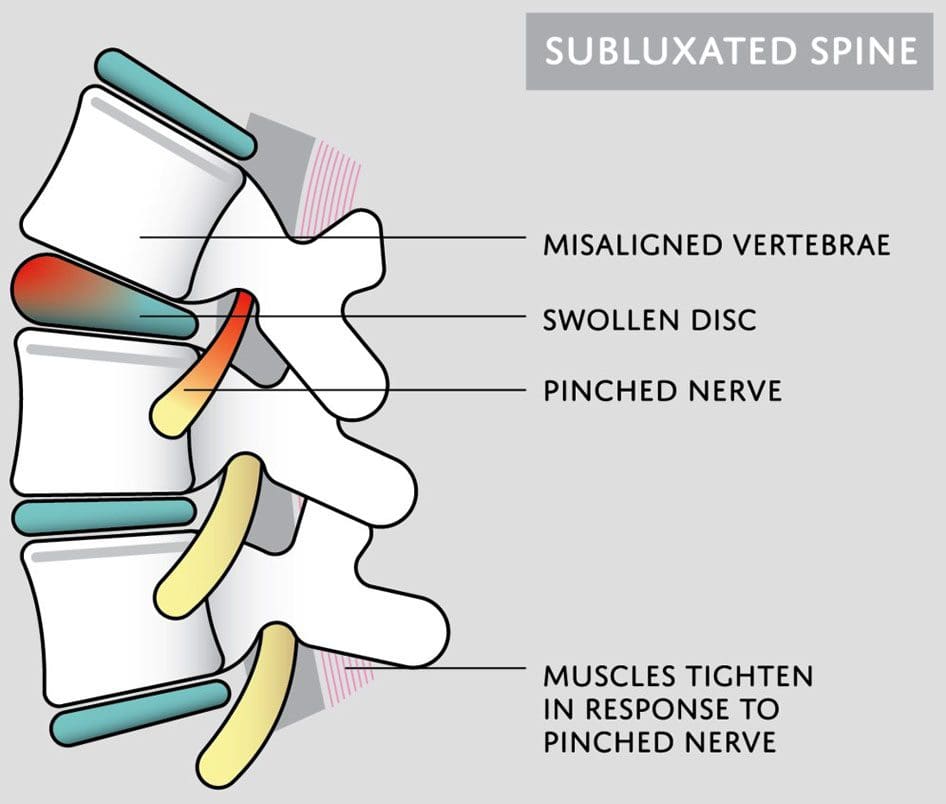
Subluxation is when a joint shifts out of alignment, which can happen to any joint in the body. Spinal subluxation indicates a misalignment of one or more portions of the spinal vertebrae. It is common in the spine from all the reaching, bending, twisting, and flexing the body goes through. Spinal subluxations, if left untreated, can cause disc degeneration, permanent nerve damage, neurological conditions, and chronic pain symptoms. A subluxation chiropractor will realign and decompress the spine combined with massage therapy to relax the muscles and restore mobility and function.
Subluxation Chiropractor
Some subluxations don’t cause any problems or pain, but that doesn’t mean they aren’t affecting the back and body. A spinal subluxation can cause long-term problems by:
Research shows that spinal subluxations can affect many facets of the body. Long-term effects may include:
Sleep problems
Low energy
Brain fog
Mood swings
Anxiety and depression
Digestive issues
Respiratory problems
Bone spurs
Spinal arthritis
Chiropractic Care
When the spine is out of alignment, it can cause issues throughout the body. Changes in one area affect the rest of the body. A subluxation chiropractor looks at the spine’s neurological and mechanical components and aims to reset everything back into its proper position. Similar to the way a massage helps the mind and body relax and de-stress, a spinal adjustment helps by:
Increasing circulation
Relieving discomfort and pain
Releasing tension
Improving mood
Reducing stress levels
Improving sleep function
Increasing energy levels
When the spine is properly aligned, the body can operate at its full potential.
Adrenal Dysfunction
References
Brian S. Budgell, Reflex effects of subluxation: the autonomic nervous system, Journal of Manipulative and Physiological Therapeutics, Volume 23, Issue 2,
2000, Pages 104-106, ISSN 0161-4754, https://doi.org/10.1016/S0161-4754(00)90076-9. (https://www.sciencedirect.com/science/article/pii/S0161475400900769)
Green, J D et al. “Anterior subluxation of the cervical spine: hyperflexion sprain.” AJNR. American journal of neuroradiology vol. 2,3 (1981): 243-50.
Meyer, S. “Thoracic spine trauma.” Seminars in roentgenology vol. 27,4 (1992): 254-61. doi:10.1016/0037-198x(92)90004-l
Neva MH, Häkkinen A, Mäkinen H, et al. High prevalence of asymptomatic cervical spine subluxation in patients with rheumatoid arthritis waiting for orthopedic surgeryAnnals of the Rheumatic Diseases 2006;65:884-888.
Nourollahi, Maryam, et al. “Awkward trunk postures and their relationship with low back pain in hospital nurses.” Work (Reading, Mass.) vol. 59,3 (2018): 317-323. doi:10.3233/WOR-182683
Vernon, Howard. “Historical overview and update on subluxation theories().” Journal of chiropractic humanities vol. 17,1 (2010): 22-32. doi:10.1016/j.echu.2010.07.001
Back pain for no reason that is non-specific is also known as idiopathic, meaning there is no definitive cause like a herniated disc, vehicle accident/crash, falling accident, work, school, or sports injury. An aching sore back that came out of nowhere can be baffling. However, there are reasons for pain, including age, unhealthy posture, work occupation, muscle spasms, lifestyle habits, family medical history, and viscerosomatic reflexes.
Back Pain No Reason
Individuals will trace back their steps and often find that there was no heavy lifting of packages, overdoing it working out, or bending, twisting awkwardly, but the pain is present.
Age
Age is a primary cause of back pain. After the age of 20, the discs in the spine begin to dehydrate, shrink, and compress/flatten out. This can cause everyday activities to generate back strain and pain as the discs begin to slip, slide, and rub against each other. This is known as degenerative disc disease and is a process that continues as the body gets older.
Back Muscle Spasms
Muscle spasms are a common manifestation of back pain and occur when the muscles involuntarily contract. Spasms often happen from bending, heavy lifting, or other physical activities.
Lifestyle Factors
Lifestyle factors can be a causation factor for back pain that comes out of nowhere.
Smoking increases the risk as nicotine increases the wear and tear on the discs as well as other organs.
The smoke/nicotine causes the discs to age faster because it breaks down the collagen, an essential part of the discs.
Individuals that are out of shape, overweight, and/or obese are more likely to have back pain from the added weight.
Unhealthy Posture/Mechanics
Practicing unhealthy postures will no doubt begin to cause back or some type of pain from the strain and awkward positioning placed on the muscles being used. Strains, twists, pulls, or tears can occur if repeating the same motion.
Viscerosomatic Reflex
Viscera means organ, and somatic refers to the body or musculoskeletal system. A viscerosomatic reaction happens when a pain signal from an organ is transmitted via the spinal cord, where neurons and motor structures like the muscles, blood vessels, and skin are interconnected. The body’s organs can become distressed or suffer an infection/disease that causes signals to be sent that there is something wrong. However, the signal could be pain that materializes in the spine/back muscles but is not a spinal injury or condition.
Diagnosis and Treatment
The first step to successfully treating back pain is scheduling an appointment with a spine specialist or chiropractor. A series of specific questions will be asked to gain insight into the underlying cause of the pain. These include:
Location of the pain
Intensity of the pain
Frequency of the pain
Medical history
Diet habits
A careful examination is necessary for the doctor to identify the reasons in any individual patient. Once the physician has learned about the symptoms and history, they can determine a possible cause and create a personalized treatment/rehabilitation plan to get the body back to optimal health.
Decompression Patient Testimonials
References
Koes, B W et al. “Diagnosis and treatment of low back pain.” BMJ (Clinical research ed.) vol. 332,7555 (2006): 1430-4. doi:10.1136/bmj.332.7555.1430
Lankhorst, G J et al. “The natural history of idiopathic low back pain. A three-year follow-up study of spinal motion, pain and functional capacity.” Scandinavian journal of rehabilitation medicine vol. 17,1 (1985): 1-4.
Walker, Bruce F et al. “Combined chiropractic interventions for low-back pain.” The Cochrane database of systematic reviews vol. 2010,4 CD005427. 14 Apr. 2010, doi:10.1002/14651858.CD005427.pub2
Injury Medical Spinal Decompression: Spinal decompression therapy/treatment can be surgical or non-surgical, with differences in the procedure, recovery time, and results. Individuals who experience compression-related problems can have severe and prolonged spinal conditions that can lead to various health issues. Individuals experiencing persistent or chronic neck, back, or leg pain should know the differences between surgical and non-surgical spinal decompression. Spinal decompression aims to relieve pressure on the discs and reduce stress on the nervesto eliminate the pain associated with compression on the spine,restoring optimal circulation and improving spinal function.
Surgical Procedure
It is invasive, must be performed by a surgeon, and can have a recovery time of up to 6 weeks.
Surgery is usually suggested as a last resort after alternative therapies have not succeeded or when the compression is so severe that surgery is the only option.
Surgical spinal decompression is directed towards removal to reduce pressure instead of adjusting or stretching the discs.
In cases of severe nerve compression, surgery can be an effective option.
Risks include infection, damage to the spinal cord, and blood clots.
Types of Spinal Decompression Surgery
Types of surgeries; spinal fusion could be necessary to stabilize the spine. Common types of back surgery:
Discectomy
This procedure removes a portion of the disc to relieve pressure on nerves.
Laminotomy
The procedureremoves a small portion of the bone or a section of the bony arch to increase the size of the spinal canal and relieve pressure.
Laminectomy
The procedureremoves theentire bony arch or lamina to increase the size of the spinal canal and relieve pressure.
Foraminotomy
This procedure removes bone and other tissue to widen the openings for the nerve roots to pass through.
The procedure removes a vertebral body along with discs.
Injury Medical Spinal Decompression
Surgery for a damaged/injured spine is not always necessary. Treatment regimes vary depending on each individual’s medical condition. Non-surgical motorized spinal decompression is a non-invasive back treatment that uses a mechanized decompression table to slowly and gently stretch the spine. The therapy gradually relieves the pressure on the compressed nerve root/s resulting in reduced or complete alleviation of pain.
Oxygen, water, and nutrients circulate abundantly, promoting healing as the discs re-hydrate, and are re-nourished, improving and enhancing spine function. Individuals can enjoy increased levels of mobility, strength in the spine and muscles, and more flexibility.
Descompresión Espinal Con La DRX9000
References
American Spinal Decompression Association: “Spinal Decompression Therapy.”
Daniel, D.M. Chiropractic and Osteopathy, 2007.
Macario, Alex, and Joseph V Pergolizzi. “Systematic literature review of spinal decompression via motorized traction for chronic discogenic low back pain.” Pain practice: the official journal of World Institute of Pain vol. 6,3 (2006): 171-8. doi:10.1111/j.1533-2500.2006.00082.x
O’Hara K, editor. Decompression: a treatment for back pain. Vol. 11. National Association of Healthcare Professionals; 2004. pp. 1-2.http://www.naohp.com/menu/publications/mccu/bibliography.htm#10 [Google Scholar]
The pelvis is designed to bear and distribute the weight of the body along with regular everyday movement. It is built to properly distribute weight between the upper and lower body that utilizes the core muscles, ligaments, and joints creating a complex pelvic girdle that helps the body function properly. The bones of the pelvis house and protect organs like the:
Reproductive system
Bladder
Below the digestive tract
When pain in the pelvis presents, daily physical activities can become difficult to get through. Chiropractic treatment combined with lifestyle adjustments can bring pain relief and strengthen the pelvis muscles/bones to maintain optimal function.
Causes of Pelvic Pain
When pain presents there can be a variety of underlying causes contributing to it. Certain causes are more serious than others. This is why seeking professional medical guidance is highly recommended for the best outcomes. Possible causes include:
These are a few causes that can contribute to mechanical changes and imbalances within the pelvis anatomy. If the pain is thought to be caused by an internal organ issue with nausea, fever, vomiting, or severe pain contact a healthcare provider immediately.
Chiropractic Relief
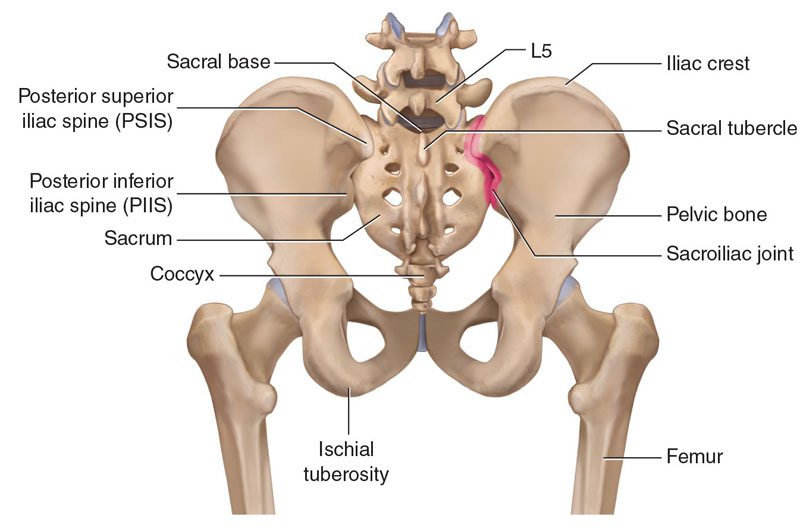
The pelvis can be thought of as a direct continuation of the spine. The lowest fused five vertebrae are known as the sacrum and are part of the pelvic girdle complex. Individuals dealing with pelvic pain typically experience the sensation within the joints themselves. These are the pubic symphysis and/or sacroiliac joints. These joints interact with the entire skeletal system. Learning how they operate can help bring relief and recovery. This is where a chiropractor can help.
Chiropractors are experts in total body alignment, restoring balance to the pelvis and spine. Plus through the treatment, they help increase the body’s natural ability to heal itself. When the lower back or pelvis is out of alignment the entire body along with its systems can be thrown off balance causing dysfunction. Chiropractic promotes and increases balance with pelvic adjustments and diverse therapies that include:
A professional chiropractor is one of the best options for the management and alleviation of pelvis pain. Pelvis misalignment can impede nerve energy and adequate blood flow. Chiropractic restoration strengthens and maintains optimal long-lasting results. Whether the pelvic pain comes from an injury, pregnancy, or pelvic shift/imbalance, a chiropractic provider can help address and alleviate the pain.
Body Composition
Lifestyle Adjustments for Optimal Kidney Health
The kidneys are small organs that work twenty-four-seven to filter blood and flush waste. In one day the kidneys pump more than 400 gallons of recycled blood throughout the body. When the kidneys do not function properly the body can be engulfed with waste. This is why it is vital to keep them healthy. Individuals usually don’t realize how an unhealthy lifestyle can harm/injure the kidneys. Chronic kidney disease slowly progresses over years, and it is not reversible. Incorporating some basic healthy lifestyle adjustments can lower the risk of developing kidney-related diseases. Here are a few lifestyle adjustments that can keep the kidneys healthy.
Drinking plenty of water
An adequate supply of water in the kidneys flushes out sodium, urea, and toxins helping avoid kidney stones. The goal is to drink eight 8-ounce glasses of water every day. Everyone’s water levels are different but body composition analysis can calculate what a normal level should be.
Healthy foods maintain a healthy body
Poor diet and visceral fat gain have been linked to chronic kidney disease. Reducing visceral fat can be achieved by eating a restricted caloric diet of vegetables, fruit, and lean protein, as well as cutting back on processed foods.
Be cautious consuming supplements, antibiotics, and over the counter medications
Regular use of common medications and supplements can cause kidney damage and disease. Consult with a doctor before taking medications and supplements if there is kidney function impairment.
Fitness and activity
Individuals need to participate in regular cardiovascular and weight-resistance physical activity/exercise. High blood sugar levels have been shown to stress the kidneys. Building adequate muscle mass helps control blood sugar.
Smoking and kidney health issues
Smoking narrows the blood vessels in the kidneys. This reduces proper blood flow and accelerates kidney malfunction.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
Kim DH, Cho D, Dickman CA, Kim I, et al. Surgical Anatomy & Techniques to the Spine. 2nd Ed. Saunders, Elsevier, Inc. Philadelphia, PA.
Lirette LS, Chaiban G, Tolba R, Eissa H. Coccydynia: An Overview of the Anatomy, Etiology, and Treatment of Coccyx Pain. Ochsner J. 2014 Spring;14(1): 84-87.
How does pain become chronic? Pain can be a complex condition, as it involves both physiological and psychological components. When an individual experiences an injury, the damaged tissues trigger and send pain signals to the brain. This is how the body alerts that there is something wrong, and thus prevents further damage. Those pain signals travel to the brain, stimulate the nerves, and cause a sensation known as pain.
�
Nerves and the brain
Nerves control the body�s functions like the organs, sensation, and movement. The nervous system receives information and generates the correct response. Two major types of nerves are sensory and motor. Sensory nerves relay information like touch, temperature, and pain to the brain and spinal cord. Motor nerves relay signals from the brain back to the muscles, which causes them to contract voluntarily or reflexively.
The peripheral nervous system is the combined millions of nerves throughout the body. The peripheral nervous system’s nerves relay signals/messages to the central nervous system, which is comprised of the brain and spinal cord. �
�
When pain becomes chronic the brain fails to process these signals correctly and the individual continues to feel pain after the injury has healed or improved. As time goes on the nerves that send the pain signals are more methodical in their signaling. This means more signals than normally will be sent and are far more intense. Conditions like cancer and diabetes can cause tissue and nerve damage throughout the body.
�
Acute vs. Chronic
Acute pain has a short duration of around three months or less. The causes are usually clear and not as difficult to diagnose. The underlying factor/s like an injury is resolved the pain also goes away. As the pain is gone, the individual no longer has problems carrying out daily activities. A few causes of acute pain are:
Surgical procedures
Dental procedures
Bone fractures
Burns
Open wounds
Childbirth
Chronic pain is defined as pain that lasts three to six months with some conditions going for years. Individuals can experience chronic pain weeks and months possibly years after the injury took place. And it can happen without any apparent cause. Many cases often involve more than one factor. This causes significant problems with daily activities. When pain becomes chronic it is often associated with conditions like cancer, diabetes, and arthritis.
�
CP and CPS
Chronic pain is defined as any type of pain that persists for six months or longer. Chronic pain syndrome is a collection of conditions that are associated with chronic pain. These conditions can make the pain worse or cause other complications like sleep problems, anger, anxiety, and depression. �
�
Causes
Doctors don’t know exactly what causes chronic pain syndrome. It often starts with an injury or painful condition such as:
A doctor will go over an individual’s medical history, illnesses, or injuries that could have started the pain. They will ask questions to learn more about the type of pain being felt and how long. Questions can include:
When did the pain begin?
Where on the body does it hurt?
What does the pain feel like – Throbbing, Pounding, Shooting, Sharp, Pinching, Stinging, Burning
The severity of the pain on a scale of 1 to 10
What sets the pain off?
What makes it worse?
Have any treatments helped?
Imaging tests can show if there is joint damage or other problems:
Computed tomography is a powerful X-ray that generates detailed images.
Magnetic resonance imaging uses magnets and radio waves to take pictures of the organs and structures.
X-rays use radiation in very low doses to create images of the body’s structures.
Talk with a chiropractor to understand how a customized treatment plan for chronic pain is developed.
Chronic Hand Pain Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Two surgeons discuss the diagnosis and treatment of acromioclavicular injuries in athletes. El Paso, TX. Chiropractor, Dr. Alexander Jimenez follows the discussion.
Acromioclavicular (AC) joint injuries most often occur in athletic young adults involved in collision sports, throwing sports, along with overhead activities like upper-extremity strength training. They account for 3% of all shoulder injuries and 40% of shoulder sports injuries. Athletes in their second and third decade of life are more often affected(1), and men are injured more commonly than women (5:1 to 10:1)(1,2).
Acromioclavicular dislocation was known as early as 400 BC by Hippocrates(3). He cautioned against mistaking it for glenohumeral (shoulder joint) dislocation and advocated treating with a compressive bandage in an attempt to hold the distal (outer) end of the clavicle in a diminished position. Almost 600 decades later Galen (129 AD) recognized his own acromioclavicular dislocation, which he sustained while wrestling(3). He left the tight bandage holding the clavicle down as it was too uneasy. In today’s era this injury is better known, but its treatment remains a source of fantastic controversy.
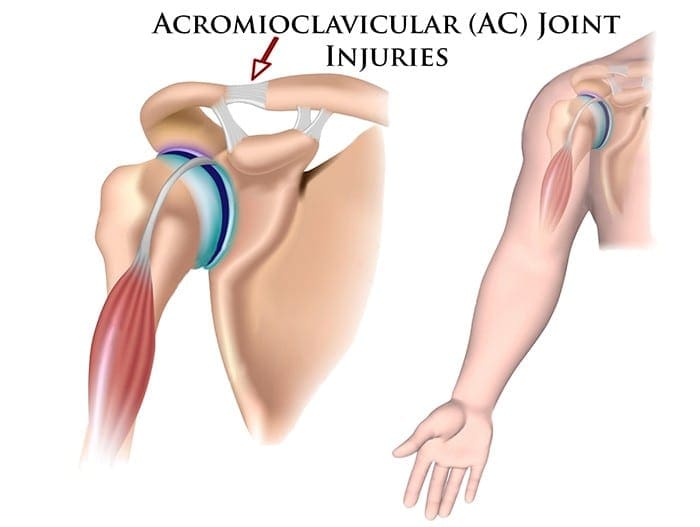
Anatomy
The acromioclavicular joint combines the collarbone to the shoulder blade and therefore links the arm to the axial skeleton. The articular surfaces are originally hyaline cartilage, which affects to fibrocartilage toward the end of adolescence. The average joint size is 9mm by 19mm(4). The acromioclavicular joint contains an intra-articular, fibrocartilaginous disc which may be complete or partial (meniscoid). This helps absorb forces in compression. There is marked variability in the plane of the joint.
Stabilizers
There is little inherent bony stability in the AC joint. Stability is provided by the dynamic stabilizers — namely, the anterior deltoid muscle arising from the clavicle and the trapezius muscle arising from the acromion.
Additionally, there are ligamentous stabilizers. The AC ligaments are divided into four — superior, inferior, anterior and posterior. The superior is most powerful and blends with muscles. The acromioclavicular ligaments contribute around two- thirds of the constraining force to superior and posterior displacement; however, with greater displacement the coracoclavicular ligaments contribute the major share of the resistance. The coracoclavicular ligament consists of the conoid and trapezoid. The conoid ligament is fan-shaped and resists forwards motion of the scapula, while the more powerful trapezoid ligament is level and resists backward movement. The coracoclavicular ligament helps bunch scapular and glenohumeral (shoulder joint) motion and the interspace averages 1.3 cm.
Mechanism Of Injury
The athlete who sustains an acromioclavicular injury commonly reports either one of two mechanisms of harm: direct or indirect.
Direct force: This is when the athlete falls onto the point of the shoulder, with the arm usually at the side and adducted. The force drives the acromion downwards and medially. Nielsen(5) found that 70 percent of acromioclavicular joint injuries are caused by an direct injury.
Indirect force: This is when the athlete falls onto an outstretched arm. The pressure is transmitted via the humeral head into the acromion, therefore the acromioclavicular ligament is disrupted and the coracoclavicular ligament is stretched.
On Examination
The athlete presents soon after the severe injury with his arm splinted to his side. The patient may state that the arm feels better using superiorly directed support on the arm. Most motions are limited secondary to pain near the top of the shoulder; the degree varies with the grade of sprain. The hallmark finding is localized swelling and tenderness over the acromioclavicular joint.
In dislocations, the outer part of the collarbone will appear superiorly displaced using a noticeable step deformity (in fact, it is the shoulder which sags beneath the clavicle). Occasionally, the deformity may only be apparent later, if first muscle spasm reduces acromioclavicular separation. Forced cross-body adduction (yanking the affected arm across the opposite shoulder) provokes discomfort. The clavicle can frequently be moved relative to the acromion.
Acromioclavicular Visualisation
The typical joint width measures 1-3mm. It’s regarded as abnormal if it is more than 7mm in men, and 6mm in women. Routine anteroposterior views of the shoulder reveal the glenohumeral jointnonetheless, that the acromioclavicular joint is over penetrated and so dark to interpret. Reduced exposure enhances visualization. The individual stands with both arms hanging unsupported, both acromioclavicular joints on one film. Weighted viewpoints (stress X-rays) are obtained with 10-15 lb weights not held but suspended from the individual’s wrists. They help differentiate type II-III injuries, but are of little clinical significance and therefore are no longer recommended in our practice.
Classification Of AC Separation
The importance of identifying the injury kind can’t be over emphasized because the treatment and prognosis hinge on an accurate diagnosis. The injuries are graded on the basis of that ligaments are injured and how badly they’re torn.
Allman (6) classified acromioclavicular sprains as grades I, II and III, representing respectively, no involvement, partial tearing, and total disruption of the coracoclavicular ligaments. More recently, Rockwood (1) has further classified the more severe injuries as standard III-VI.
The injuries are classified into six categories:
Type I This is the most common injury encountered. Only a mild force is needed to sustain such an injury. The acromioclavicular ligament is sprained with an intact coracoclavicular ligament. The acromioclavicular joint remains stable and symptoms resolve in seven to 10 days. This injury has an excellent prognosis.
Type II The coracoclavicular ligaments are sprained; however, the acromioclavicular ligaments are ruptured. Most players can return to their sport within three weeks. There is anecdotal evidence to suggest that steroid injections into the acromioclavicular joint speed up the resolution of symptoms, but this practice is not universal.
Type III The acromioclavicular joint capsule and coracoclavicular ligaments are completely disrupted. The coracoclavicular interspace is 25-100% greater than the normal shoulder.
Type IV This is a type III injury with avulsion of the coracoclavicular ligament from the clavicle, with the distal clavicle displaced posteriorly into or through the trapezius.
Type V This is type III but with exaggeration of the vertical displacement of the clavicle from the scapula-coracoclavicular interspace 100-300% greater than the normal side, with the clavicle in a subcutaneous position.
Type VI This is a rare injury. This is type III with inferior dislocation of the lateral end of the clavicle below the coracoid
Treatment
The treatment of acromioclavicular joint injuries varies based on the seriousness or grade of the injury.
Initial treatment: These can be quite painful injuries. Ice packs, anti-inflammatories plus a sling are utilized to immobilize the shoulder and then take the weight of the arm. As pain starts to subside, it is important to start moving the fingers, wrist and elbow to prevent shoulder stiffness. Next, it’s important to begin shoulder motion in order to stop shoulder stiffness.
Un-displaced injuries only require rest, ice, and then a slow return to activity over two to six weeks. Major dislocations require surgical stabilization in athletes if their dominant arm is involved, and if they participate in upper-limb sports
Type I & II: Ice pack, anti-inflammatory agents and a sling are used. Early motion based on symptoms is introduced. Pain usually subsides in about 10 days. Range-of-motion exercises and strength training to restore normal motion and strength are instituted as the patient�s symptoms permit. Some symptoms may be relieved by taping (taking stress off acromioclavicular joint). The length of time needed to regain full motion and function depends upon the severity or grade of the injury. The sport and the position played determine when a player can return to a sporting activity. A football player, who does not have to elevate his arm, can return sooner than a tennis or rugby player. When a patient returns to practice and competition in collision sports, protection of the acromioclavicular joint with special padding is important. A simple �doughnut� cut from foam or felt padding can provide effective protection. Special shoulder- injury pads, or off-the-shelf shoulder orthoses, can be used to protect the acromioclavicular joint after injury.
Some Type II injuries may develop late degenerative joint changes and will need a resection of the distal end of the clavicle for pain relief. It is important to note that after a resection of the distal end of the clavicle, particularly in a throwing athlete, there may be formation of heterotopic bone on the under surface of the clavicle which can cause a painful syndrome which presents like shoulder impingement.
Type III: The treatment of type III injury is less controversial than in past years. In the 1970s, most orthopaedic surgeons recommended surgery for type III acromioclavicular sprains(7). By 1991, most type III injuries were treated conservatively(8). This change in treatment philosophy was prompted by a series of retrospective studies(9). These showed no outcome differences between operative and nonoperative groups.
What’s more, the patients treated non-operatively returned to full activity (work or athletics) earlier than surgically treated groups(10, 11). The exceptions to this recommendation include people who perform repetitive, heavy lifting, people who operate with their arms above 90 degrees, and thin patients who have prominent lateral ends of the clavicles. These patients may benefit from surgical repair(12).
Any discussion about the management of acute injuries to the AC joint must deal with which of the many methods of surgical therapy described is the best for their situation, but whether surgery should be considered at all. Surgery is generally avoided in athletes participating in contact sports since they will often re-injure the shoulder later on.
Type IV-VI: Account for more than 10-15% of total acromioclavicular dislocations and should be managed surgically. Failure to reduce and fix these will lead to chronic pain and dysfunction.
Surgery
Surgical repair can be divided into anatomical or non- anatomical, or historically into four types:
? Coracoclavicular repairs (Bosworth screws(13), cerclage, Copeland and Kessel repair).
? Distal clavicular excision.
? Dynamic muscle transfers.
? Disadvantages of surgery are that there are risks of infection, a longer time to return to full function and continued pain in some cases.
For the individual with a chronic AC joint dislocation or subluxation that remains painful after three to six months of closed treatment and rehabilitation, surgery is indicated to improve functioning and comfort.
For sequelae of untreated type IV-VI, or painful type II and III injuries, the Weaver Dunn technique is advocated. This�entails removing the lateral 2cm of the clavicle and reattaching the acromial end of the coracoacromial ligament to the cut end of the clavicle, thus reducing the clavicle to a more anatomical position.
Postoperatively, the arm is supported in a sling for up to six weeks. Following the first two weeks, the patient is permitted to use the arm for daily activities at waist level. After six weeks, the sling or orthosis is discontinued, overhead actions are allowed, formal passive stretching is instituted, and light stretching using elastic straps is initiated. Stretching and strengthening are begun slowly and gradually. The athlete shouldn’t return to their sport without restriction until full strength and range of motion has been recovered. This usually occurs four to six months following operation.
Conclusion
AC joint injuries are an important source of pain at the shoulder area and have to be assessed carefully. The management of these injuries is nonoperative in the majority of cases. Type I and II injuries are treated symptomatically. The present trend in uncomplicated type III injuries are a non operative strategy. In the event the athlete develops following problems, a delayed reconstruction might be undertaken. In athletes involved in heavy lifting or prolonged overhead activities, surgery may be considered acutely. Type IV-VI injuries are generally treated operatively.
No matter what kind of treatment is chosen, the ultimate purpose is to restore painless function to the wounded AC joint so as to reunite the athlete safely and as quickly as possible back to their sport. It is possible in the vast majority of acromioclavicular joint injuries.
References
Reza Jenabzadeh and Fares Haddad
1. Rockwood CA Jr, Williams GR, Young CD. Injuries of the Acromioclavicular Joint. In CA Rockwood Jr, et al (eds), Fractures in Adults. Philadelphia: Lippincott-Raven, 1996; 1341-1431.
2. Dias JJ, Greg PJ. Acromioclavicular Joint Injuries in Sport: Recommendations for Treatment. Sports Medicine 1991; 11: 125-32.
3. Adams FL. The Genuine Works of Hippocrates (Vols 1,2). New York, William Wood 1886.
4. Bosworth BM. Complete Acromioclavicular Dislocation. N Eng J Med 2 41: 221-225,1949.
5. Nielsen WB. Injury to the Acromioclavicular Joint. J Bone Joint Surg 1963; 45B:434-9.
6. Allman FL Jr. Fractures and Ligamentous Injuries of the Clavicle and its Articulation. J Bone Joint Surg Am 1967;
49:774- 784.
7. Powers JA, Bach PJ: Acromioclavicular Separations: Closed or Open Treatment? Clin Orthop 1974; 104 (Oct): 213-223
8. Cox JS: Current Methods of Treatment of Acromioclavicular Joint Dislocations. Orthopaedics 1992; 15(9): 1041-1044
9. Clarke HD, Mc Cann PD: Acromioclavicular Joint Injuries. Orthop Clin North Am 2000; 31(2): 177-187
10. Press J, Zuckerman JD, Gallagher M, et al: Treatment of Grade III Acromioclavicular Separations: Operative versus
Nonoperative Management. Bull Hosp Jt Dis 1997;56(2):77-83
11. Galpin RD, Hawkins RJ, Grainger RW: A Comparative Analysis of Operative versus Nonoperative Treatment of Grade III Acromioclavicular Separations. Clin Orthop 1985; 193 (Mar): 150-155
12. Larsen E, Bjerg-Nielsen A, Christensen P: Conservative or Surgical Treatment of AC Dislocation: A Prospective, Controlled, Randomized Study. J Bone Joint Surg Am 1986;68(4):552-555
13. Bosworth BM. Complete Acromioclavicular Dislocation. N Engl. J. Med. 241: 221-225,1949.
For many athletes following any major endurance event they will return to their houses, to recover, celebrate, reflect and rebuild to their next career step. Some, like the athlete in this case study will need to now focus attention on delayed decisions concerning whether to go under the knife to sort out a chronic injury.�El Paso, TX’s Injury scientist, Dr. Alexander Jimenez takes a look at the study.
My client has been competing in triathlon for 10 or more years, although his career has included a range of serious injuries which have kept him from races for months on end. In the previous two to three decades, however, he’s enjoyed a sustained period of injury-free training and racing, and has climbed to the peak of the world rankings. But the emergence of hip pain has seen him once more return to the physio’s table.
The triathlete’s accident history highlights a common pattern among sportspeople: 2 tibial stress fractures, a femoral neck stress fracture and a serious ankle sprain — every one of these on his right side. The significant contributing element to the bone stress injuries is a 1.5cm leg-length gap (his right leg is shorter).
He’d first experienced comparable hip pain in 2004; it kept him from running for three months. At that time, nothing was detected on a bone scan or MRI, or so the pain went paralyzed. An intra-articular cortisone injection (CSI) elicited no improvement. The athlete remembers that he chose to train on his painful hip, never allowing the symptoms to settle. The nearest he ever came into an investigation was a hypothesis that he could have a little, undetected, labral lesion.
The present episode of hip pain began initially at night after a hard three-hour bicycle ride. Earlier this, however, he hadn’t cycled for five times. He described his initial symptom as a profound hip tightness (lateral and lateral), together with slight pain in his groin. He was able to continue to train however, was feeling that the hip tightness and pain following both cycling and running (swimming was symptom-free).
A week later his symptoms dramatically worsened when he flew from Australia to Singapore, on his way to a French high- altitude camp. As he got off the airplane, he felt deep hip pain as well as the tightness. As elite athletes tend to do, he coached anyway, running a tricky track session, which made the hip much worse: he was unable to ride or run without pain. He instantly started a course of anti- inflammatories.
I met him in Singapore and evaluated him in the airport, initially ruling out any prospect of a disease or systemic matter. He explained he had been feeling an ache during the night, lying in bed; on waking, the hip would be OK, but got worse the longer he walked.
On assessment, he had the following physical signs:
� walking with obvious limp
� pain on hopping (6/10)
�painful right hip quadrant/impingement test (full hip flexion/adduction)
� reduced right hip flexion (-10 degrees compared to left)
� reduced right hip internal rotation (-10 degrees compared to left)
� increased tone on palpation of TFL, adductors, hip flexors, gluteal, piriformis and deep rotators
� lumbar spine and SIJ were OK
� femoral shaft bone stress test was OK � leg length discrepancy (right side 1.5cm shorter)
� right innominate (pelvis) anteriorly rotated
� weakness in right hip abductors/extensors
� reduced calf endurance on right side (-5 reps)
� ankle dorsiflexion range of movement was OK
� reduced proprioception on right (single leg stance, eyes closed).
I thought the differential diagnoses were:
� femoral neck stress fracture
� labral tear, possibly with hip synovitis
� FAI (femoro-acetabular impingement), possibly with hip synovitis.
I initially treated the triathlete with soft- tissue techniques to reduce the tone around the hip joint. Trigger-point releases were performed on his TFL, adductors, gluteals, piriformis, deep rotators and iliopsoas.�This reduced his jump pain into 3/10. Manual long-leg grip further decreased the strain on hopping (2/10). He still had pain and stiffness on walking but it sensed “simpler. As he prepared to embark on his long run flight to Europe, I counseled him to not sit for too long and maintain his stylish as straight as possible to decrease any potential impingement from hip flexion.
Luckily, the hip didn’t get worse throughout the flight. On arrival at the French high-altitude training centre, we initiated a strategy of two swims and two intensive treatments a day, aiming at reducing muscle tone, restoring his range of hip movement and normal muscle control and stamina. We had been expecting that the problem was not a stress fracture, but just minor hip synovitis that could settle quickly. Following a week of conservative treatment, though, we were just able to keep his hop pain in 2/10, and that he still could not run 20 meters without any pain and limping.
In collaboration with medics, we flew to London to see a sports doctor and get MRI scans. The scans revealed no bone stress reaction, fracture or labral ripping — which was a big relief; however, it did show signs consistent with FAI (femoro-acetabular impingement). He had hip synovitis with a rectal lesion on his femur.
Hip injuries aren’t much reported among triathletes — in fact they are notably absent from reports on Olympic and Ironman triathlons, which mention knee, back, H/ Achilles, lower leg, ankle and shoulder as the most common accidents (1-3).
In this state, when the hip is in maximum flexion and internal rotation, the labrum and cartilage abut and impinge; damage to the articular cartilage and acetabular labrum results from this pathologic bony contact. The contact generally results in a structural abnormality of the femur (“camera impingement”) along with the acetabulum (“pincer impingement”) or a combination of both (“mixed impingement”). Over time, via repetitive micro-trauma, the aggravating motion hurts the hip cartilage or labrum (or both) during normal joint motion. This happens along the anterior femoral neck and the anterior–superior acetabular rim. FAI is a possible trigger of early hip joint degeneration (4).
Arthroscopic surgery is the direction of choice for FAI if symptoms do not settle; however as his next Competition was only three and a half a year off, surgery was not an option. Instead, over a five-day interval, the athlete had two cortisone (CSI) and local anesthetic injections into the hip joint (under ultrasound guidance) to settle the indicators.
Our aim was to grow the hip range of motion and extend the capsule to reduce any additional impingement, slowly returning to regular training. Following the competition, the athlete would then should see a hip arthroscopic surgeon to acquire a surgical opinion to the best option for long-term direction.
Injection Relief
After both shots my customer felt sore for five days. The initial CSI settled his pain on hopping to 1/10 and after seven days he managed to operate without symptoms. But minor hip stiffness and aching at the end of the day prevented him from progressing to optimal training, so that he then underwent a second steroid injection. This settled the hop pain into 0/10 and decreased the aching; so after five times he returned to mild cycling and after seven days he started running again, also.
The athlete admitted that, following the first shot, he had done more and gone tougher in training than directed, as he had felt “good. This mistake of “too much too soon — all too common in elite athletes — had led to excessive inflammation and aching in the hip nightly after training. After the next injection he returned to normal intensity slower and more gradually.
My client built his training up to regular levels by four months following the final injection (swimming five times per week, cycling four days and running six to seven days). He began with very easy cycling on a wind trainer for 30 minutes, building slowly to 90 minutes before cycling on the street. He cycled two days on and one day away and avoided hills to the first two weeks. He started jogging on the apartment for 15 minutes and slowly built up to 90 minutes after three weeks. He did not run hills or about the track; and as he ran only on every single day, he would diligently concentrate on technique.
From week six to week 11, my client remained on anti inflammatory medication and underwent two treatments a day.
The hands-on treatment continued to:
� increase hip range of movement
� stretch the hip capsule
� normalise pelvic symmetry and hip muscle tone
� improve muscle control and strength � improve proprioception
� ensure optimal biomechanics via video assessment (cycling and running).
Eleven weeks after he first felt his hip pain, the triathlete returned to racing; however he failed to finish the first race, partially because of minor hip stiffness but mainly due to “fitness. Fortunately there were not any prolonged symptoms after the race and a week after he successfully returned to competition, coming second in a really strong field. His very minor ongoing symptoms were handled with anti-inflammatory drugs and hands-on treatments.
If this athlete wants to pursue a long- term triathlon career up to the London Olympics, then he will now require surgery. The arthroscopic surgical technique initially assesses the cartilage and labral surfaces, debrides any abnormalities of the hip joint cartilage and hip labrum, removes the non-spherical segments of the femoral head�and any prominent sections of the anterior femoral neck and bony growths on the acetabular rim that may continue to contribute to hip joint impingement.�The alternative is early joint degeneration and onset of osteoarthritis.
References:
1. Wilk B et al: �The incidence of musculoskeletal injuries in an amateur triathlete racing club�. J Orthop Sports Phys
Ther 1995 Sep;22(3):108-12.
2. Collins K et al: �Overuse injuries in triathletes. A study of the 1986 Seafair Triathlon�. Am J Sports Med 1989 SepOct;17(5):675-80.
3. Korkia PK et al: �An epidemiological investigation of training and injury patterns in British triathletes�. Br J Sports Med 1994 Sep;28(3):191-6.
4. Ganz R. et al (2003): �Femoroacetabular impingement: a cause for osteoarthritis of the hip�. Clin Orthop Relat Res. 417:112�120. For more information see: www.hipfai.com
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine