Texas employers are invited to join the Division of Workers� Compensation in Austin for the Texas Safety Summit on May 9-11. The 21st annual workplace safety and health conference offers important information for everyone who plays a role in safeguarding employees, from the beginner to the seasoned safety professional.
Employers will hear from top safety experts about some of the most critical safety and health issues facing Texas businesses. Attendees will learn practical tools and techniques to use in their workplaces to better protect their employees.
�The Safety Summit is a proactive way for us to help Texas businesses,� says Commissioner of Workers� Compensation, Ryan Brannan. �Not only does it help foster a positive safety culture for your company and its employees, it ultimately helps reduce costs associated with on-the-job injuries and illnesses.�
What to Expect
Presentations from experts at the National Safety Council, the Occupational Safety and Health Administration (OSHA), and many more.
Interactive exhibits on transportation safety.
Great networking opportunities with safety professionals from across the state.
Early-bird registration is $375 through April 17, 2017. The cost is $400 after that date.
For more information, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Additional Topics: Preventing Work Disability with Chiropractic
After being involved in an unfortunate accident at work, injuries and aggravated conditions resulting from the incident can often lead to a variety of painful symptoms and complications, if left untreated, along with missed days at work and lost wages. A new research study showed that workers who received regular chiropractic care experienced less work-related injuries.
So many buzzy new workouts, so little time. But we promise, Orangetheory Fitness deserves a spot near the top of your list of sweat tests this year for its smart system and crazy calorie burn.
While it’s not brand new�Orangetheory is close to celebrating its sixth anniversary with more than 330 studios in 28 states, and more overseas�the company only recently opened in big cities like New York and Los Angeles. And it has quickly become a known name (and color) in even the most competitive fitness-focused metropolises. (According to Google, it was one of the 10 Biggest Workout Trends of 2015.)
The model is smart and simple: Enthusiastic, experienced instructors plus a heart-rate monitored cardio and strength session equals max results in just an hour. Here’s everything a first-timer should know before joining the “orange nation.”
The hour blends the perks of traditional workout classes (think good music and an energetic leader) and the one-on-one benefits of small-group personal training.
The instructors remember every client’s name, make an effort to cheer you on and give you constructive feedback during class, and urge everyone to work within their personal fitness level. This means you won’t be overwhelmed by confusing choreography, annoyed by close quarters, or trampled by the stampede rushing to grab the last medicine ball. Everyone goes to work within their own station, complete with various sets of weights, TRX straps, a step, and more.
Being Early is a Must
You’ll receive a welcome email or text message a day or two before your scheduled class, and the message will instruct you to arrive 30 minutes before the start time. Even if you’re experienced using just about any gym tool and have tried every workout under the sun, that half hour is crucial at Orangetheory.
You need about 10 minutes to introduce yourself at the front desk and fill out paperwork. Then, the trainer will chat with you about the types of workouts you do and your fitness goals (as a top-tier trainer should). Are you an Olympic rower? It doesn’t matter; your instructor will want to check out and assist with your form on the WaterRower and also give you a rundown of class lingo (you’ll hear terms like “base push” and “all out” throughout the hour).
You don’t have to memorize everything; there are television screens around the studio that show both a graphic of the move and number of reps per set while you’re doing strength on the floor and treadmill signs hanging on the mirror to guide your speed choices.
High-intensity interval training focuses on working at an all-out effort for shorter intervals of time in order to shoot your heart rate up, followed by brief periods of active recovery. Studies have continuously shown that HIIT is an extremely efficient way to maximize calorie burn.
Before you start class, a staffer will provide a heart-rate monitor that you strap right beneath your bust, directly on your skin. The goal is to work in your “orange zone”�which is 84-91% of your max heart rate�for 12 to 20 minutes during the class. How do you know where you stand? There’s an overhead screen that displays a chart with everybody’s name, vitals, and progression between the five “zones” (grey, blue, green, orange and red) in real time. This is both good and bad (depending on how much you like a competitive atmosphere): it means if you start slacking off, everyone in class will know it.
The major pro, however: Wearing the monitor makes you much more in tune with just how hard you’re working at any given time, and your results are emailed to you after class so you can see how you did and track improvement over time.
The instructors switch up the routine every time, offering a unique challenge every time you show up. In general, though, you can expect the 55-minute session to involve a combination of treadmill, indoor rowing, and strength training (with weights, body-weight exercises, or possibly TRX moves).
With folks rowing, running, jumping around on the floor, and screens holding your cue cards all around, it may feel as if there’s a lot going on in the room. But just focus on your movement and form during your first class; the trainer can walk you through your results afterward�then help you set new goals for when you return for round two.
For more information, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Additional Topics: Preventing Sports Injuries
A variety of athletes, including running athletes, commonly seek chiropractic care to diagnose and treat numerous sports injuries. Chiropractic focuses on the treatment of injuries and conditions related to the musculoskeletal and nervous system, making it an ideal care option for athletes. Recent research has demonstrated that chiropractic care can additionally help prevent a variety of sports injuries in athletes.
Regular exercise is potent medicine for older adults with heart disease, a new American Heart Association scientific statement says.
Physical activity should be a key part of care for older adults with heart disease who want to reduce their symptoms and build their stamina, said geriatric cardiologist Dr. Daniel Forman. He’s chair of the panel that wrote the new statement.
“Many health-care providers are focused only on the medical management of diseases — such as heart failure, heart attacks, valvular heart disease and strokes — without directly focusing on helping patients maximize their physical function,” Forman said in a heart association news release.
Yet, after a heart attack or other cardiac event, patients need to gain strength. Their independence may require the ability “to lift a grocery bag and to carry it to their car,” said Forman, a professor of medicine at the University of Pittsburgh Medical Center and VA Pittsburgh Healthcare System.
“Emphasizing physical function as a fundamental part of therapy can improve older patients’ quality of life and their ability to carry out activities of daily living,” he added.
And, no one is too old to get moving. “Patients in their 70s, 80s and older can benefit,” Forman said.
Cardiac rehabilitation is a crucial tool for elderly patients, providing exercise counseling and training to promote heart health, and manage stress and depression. But Forman said it’s not prescribed often enough.
“When treating cardiac patients in their 70s, 80s and 90s, health-care providers often stress medications and procedures without considering the importance of getting patients back on their feet, which is exactly what cardiac rehabilitation programs are designed to do,” he noted.
Daily walking and tackling more chores at home also can be helpful, Forman said. Resistance training and balance training can help prevent falls. Tai chi and yoga employ strength, balance and aerobic features, he explained.
The statement also outlines ways for heart doctors to assess patients’ levels of physical functioning.
The statement was published March 23 in the journal Circulation.
Heart disease in older Americans is a growing concern because the number of people 65 and older in the United States is expected to double between 2010 and 2050.
Pediatricians have long suggested that fruit juice may prompt weight gain in children, but a new review finds it harmless when consumed in moderation.
“Based on the current evidence, we didn’t find that consuming one serving [of 100 percent fruit juice] a day contributes to weight gain in children,” said study author Dr. Brandon Auerbach. He is acting instructor of medicine at the University of Washington, in Seattle.
To come to that conclusion, the investigators analyzed the results of eight published studies involving over 34,000 children that looked at fruit juice intake and the effect on weight.
Children under the age of 6 who drank a serving a day gained a small amount of weight, but not enough to be clinically significant, the findings showed.
The amount was truly tiny, less than a pound over a year’s time, Auerbach noted. And the review did not prove that fruit juice consumption caused the weight gain.
In addition, children aged 7 to 18 who drank a serving a day saw no clinical effects on weight, the researchers said.
The younger children favored apple juice, while the older ones were more likely to drink orange juice. The study authors explained that orange juice, which has a lower glycemic index, may be linked with less weight gain. Food and drink with a lower glycemic index are linked with lower and slower rises in blood sugar levels.
The researchers stressed that their report specifically focused on 100-percent fruit juice, not fruit-flavored drinks or fruit sodas.
Senior study author, Dr. James Krieger, is executive director of Healthy Food America. He said, “The evidence on weight gain, diabetes [risk] and other health conditions for [drinking] sugar-sweetened beverages — like soda and fruit drinks — is very solid.”
What has been debated, according to Krieger, is whether sugar in 100-percent fruit juice is linked with the same health effects.
For now, Krieger and Auerbach said, they advise parents to follow the American Academy of Pediatrics’ recommendations for 100-percent fruit juice consumption: 4 to 6 ounces a day for children aged 6 and younger, and 8 to 12 ounces a day for kids aged 7 to 18.
Connie Diekman, director of university nutrition for Washington University in St. Louis, said that the new findings put the issue in perspective.
“Concerns around childhood obesity have caused many to try to find ‘the food’ that is the cause,” Diekman explained.
“This study did a nice job in assessing the impact of 100-percent fruit juice on weight, a food often blamed for the growing incidence of childhood obesity,” she said.
“As a registered dietitian, this study reinforces the messages I provide my clients: 100-percent fruit juice — not fruit drinks or beverages — can fit into a healthful eating plan. But it is important, as with all foods, to learn portion sizes,” Diekman stressed.
“In addition, I always remind people that whole fruit — whether fresh, frozen or canned — can provide more satiety since we don’t seem to recognize fullness from liquids, while we do from solids,” she said.
The study was published online March 23 in the journal Pediatrics.
If you like to run but don�t looove to run, here�s some news that�s sure to put a bounce in your step. A recent review of studies found that to score the major health perks of running, you don�t have to pound the pavement for long: Jogging just five or six milesa week is enough.
The researchers report that people who logged that many miles over the course of one or two runs (and less than 51 cumulative minutes) per week had a lower risk of certain cancers, stroke, osteoarthritis, high blood pressure, and high cholesterol compared to people who jogged less or not at all.
It gets even better: When the reviewers looked at the effect of running on cardiovascular mortality and death from any cause, they found that the low-mileage group had the same reduction in risk as people who laced up more often and covered more ground every week.
�Maximal health benefits of running appear to occur at quite low doses, well below those suggested by the US physical activity guidelines,� the researchers write in the study, which was published in the journal Mayo Clinic Proceedings. (The government recommends 75 minutes of vigorous activity per week.)
But of course, if you�re running to lose weight, the same logic still applies: More steps means more calories burned. You may want to stick to your usual schedule and route. But for anyone who�s been pushing herself on long-distance jaunts in pursuit of optimal health, the new findings may offer some sweet relief.
So�what is a good goal to shoot for, according to science?
Carl J. Lavie, MD, the review�s lead author and the medical director of cardiac rehabilitation and prevention at the Ochsner Medical Center in New Orleans, offered this�advice to�the New York Times: �Running for 20 to 30 minutes, or about a mile-and-a-half to three miles, twice per week would appear to be perfect.�
Let’s face it: whether you’re an experienced exerciser or totally new to working out, very few of us have the time to dedicate hours upon hours to our sweat sessions. That’s why it’s important to make every minute count. These proven tips and techniques will turn up your calorie burn during every workout you do, helping you bust through fitness plateaus and melt fat away in less time.
Pump up the jams
Pop in your earbuds, cue up your favorite playlist and get cranking. Listening to music is one of the easiest�and most fun�ways to rev up your calorie burn. When a team of University of Wisconsin researchers asked men and women to perform two 8-minute exercise sessions on a stationary bike, one with music and one in silence, the exercisers increased their average heart rate by 10 beats per minute, worked harder, and burned 7% more calories when they pedaled to tunes.
Pair up with an inspirational partner
Exercising with someone just a little better than you can bring out your calorie-scorching best. In one study, researchers from Kansas State University found that people who exercised with a partner they thought was a little fitter and stronger than they were increased their workout time and intensity by as much as 200%.
Let go of the rails
The more muscles you use, the more calories you burn. That means letting go of the rails on the treadmill and not leaning on the elliptical so your lower body and supporting core muscles have to work harder to keep you upright and in motion.
Put your arms into it
Race-walkers have an adage: As your arms go, your legs follow. If you want to speed up your pace and turn up your burn, pump your arms faster and your feet will follow. You�ll also engage more upper body muscles for another calorie burning bonus. Ditto for your elliptical machine sessions. Research shows that exercisers use more fat-burning oxygen when they get their arms into the action by using the elliptical machines handles than when they churn along with their legs alone.
Find your sweet spot
High intensity interval training (HIIT) may be great for getting a big metabolic bump for your exercise time, but because it’s so hard, many people burn out and don�t do it enough to see results. For a better, consistently higher, calorie burn, you want to hit your �sweet spot,� says Daniel Frankl, PhD, kinesiology professor at California State University, Los Angeles. �That�s the highest submaximal exercise intensity you can tolerate for 30 minutes.� You know you�re there when your breathing is slightly labored, but you can still talk in short sentences.
Wear some weights
Heavier people burn more calories because their bodies have to work harder to keep them in motion. You obviously don�t want to gain weight to burn calories, but you can fake it by wearing a weighted vest or adjustable weight garment like the TITIN Force Shirt System, a compression shirt that lets you slip up to 8 pounds of weight into 14 pockets. Research shows adding weight to your workouts can increase your calorie burn by 7% during moderate walks and more than 13% during step-climbing exercise.
Use the force
Gravity is an unexpected, but effective calorie burner�you have to work exponentially harder to fight its forces when you walk, bike, or run at an incline. Head to the hills: you can burn 50% more calories when you go from pancake-level terrain to a more challenging 6% incline.
Drink some java
Caffeine not only revs your metabolism, but also is a proven performance enhancer. Studies show that the energizing chemical found in coffee reduces your perception of exercise, so hard efforts feel easier and you can go harder, longer and burn more calories.
Cool your jets
Hydrate with icy-cold water for a one-two metabolic calorie burning punch. For one, downing a couple cups of cold water can raise your metabolism by about 5% as your body works to warm the fluid. Also drinking an icy beverage before exercising in the heat can help you feel fresher and crank out longer and harder efforts before fatiguing, so you can easily burn more calories.
Tune in, not out
Texting, watching TV, and flipping through a magazine are good ways to multitask while spinning away on the stationary bike or churning through an elliptical workout, says Frankl. �But they take your attention away your workout so you may not be giving it your best effort,� says Frankl. �Paying attention to your effort�your heart rate, your breathing, the sensation in your muscles�helps you maintain a steady effort so you can burn more calories,� he says.
“Runners need an incredible amount of nourishment to stay healthy, since running puts stress on not only muscles but every system in our body,” notes Elyse Kopecky, a chef, nutrition coach, and coauthor (with four-time Olympian Shalane Flanagan) of Run Fast. Eat Slow. “We often obsess about having the right amount of protein, carbs, and fat in our diet while forgetting about important micronutrients, including vitamins and minerals like iron, magnesium, potassium, and calcium, all of which can become depleted from distance training.”
Her post-run smoothie to replenish muscle stores and restock nutrients: whole-milk yogurt, frozen blueberries and banana, peeled carrot, a handful of kale, ginger, coconut water (or regular water), and coconut oil.
The truth is, the appearance of your butt is partially out of your control,�says Harley Pasternak, celebrity trainer and Fitbit ambassador.��Genetics�is the number-one component of the size and shape of your butt,� he says. �Different ethnicities also have certain biological predispositions for adiposity in different parts of the butt, or different waist-to-hip ratios that give the butt and hips a particular look,� he adds.
Pasternak also notes that how you’ve used your glutes throughout your life may also dictate the natural development of your butt. �So someone who was a gymnast as a kid might have more developed glutes, or an easier time toning the glutes as they get older, than someone who maybe didn�t do any sports as a child,� he explains.
Now for the good news: Just because you can’t necessarily battle the natural curve of your booty doesn’t mean you can’t amp up the assets you have, he assures. Plus, there are so many benefits of developing a strong, toned tush that go beyond how it fills out your jeans. Having strong glutes can make you a better runner, improve your posture, and more.
So genetics aside, what else could be�stalling your dream derriere? There are other little�errors that people unknowingly make that can take the emphasis off of the glutes,�Pasternak says.�Make these�exercise and lifestyle adjustments to accelerate your results.
Don’t rely on the same old butt exercises
Certain moves that we often associate with the glutes�actually recruit other large lower-body muscles (namely�the quadriceps) to do most of the work.�”This tends to be�the case with basic body-weight squats and leg presses,” Pasternak says.
Instead, Pasternak recommends focusing more on unilateral movement, or working one side of the body at a time so that other large muscles in both legs don’t dominate.�”Unilateral training�will�allow you to access the�glutes more directly,” he says. Moves to work into your butt�routine: single-leg deadlifts, lunges, and lying single-leg hip thrusts.
“Your butt is mainly fat. That�s just a fact,” Pasternak says�and fighting flab requires�a combo of cardio and a healthy diet. But you should be doing more with your�cardio than steady treadmill runs if you want to zero in on the�glutes, he says. “Steady running can actually�shorten the hamstrings and cause the glutes to become disengaged,” he says.
Instead, opt for walking or sprinting.�”Walking forces you into�a longer stride, which gives you the opportunity to access your glutes�better. Sprinting requires your knees to lift higher, which also fires up the glutes,” Pasternak explains.
For�even more effective butt-targeting cardio, add incline. “I think stairs are just the most underrated glute�blaster�there is,” Pasternak says. “I recommend that all my clients hit a step goal of 10,000 or 15,000 steps per day, and at least 1,500 of those should be on hills or stairs if you want to really want to tone the glutes fast.”
Sit less, stretch more
Putting all of your bodyweight on your butt for hours upon hours each day�can actually change the shape of it, Pasternak says.��Sitting also shortens and tightens the hip flexors, which impacts our ability to really activate both our�glutes�and core even when we’re not seated,” adds�physical therapist David Reavy, owner of React Physical Therapy in Chicago, Ill.
After a period of being sedentary (and especially before going from desk chair to workout), Reavy suggests doing�these three exercises to help lengthen the front of your body and�re-activate the glutes:
Mobilization backbend: Start in a split stance, with one foot slightly behind you and the heel slightly raised. Reach back with the arm of the same side and place your�fist on your sacrum. Lean back as far as you can and hold for a few seconds.�Repeat the movement on the other side.�Do about 10 reps on each side, bending back as far as you can each time.
Hip-flexor release:�Lay on your stomach and put a lacrosse ball under your psoas. Allow your bodyweight to release onto the ball as much as possible�without pain and lay�until you feel your hip flexor relax.
Hip thrusts:�Put your shoulders on a flat bench, heels on the ground. Using your glutes, lift your hips up to a bridge position, hold for a few seconds and lower your hips. Reavy suggests putting a resistance band around your thighs for added challenge: �This helps turn on your external rotators, which are part of your glutes, so you�ll be working your butt all the way around,� he says. Do three sets of 10 to 15 reps.
Working out in the gym is great, but even the biggest treadmill loyalists can get bored on the moving belt. Our advice? Mix up your sweat sessions whenever you can. Introducing different types of movement into your fitness routine can actually help you get in shape faster because they challenge your muscles in new ways.
That�s why we love with this samba reggae dance workout. It�s a total change of pace from your standard barre class. And you don�t need to be a pro dancer to try the moves either.
Samba Workout
In the video, dance teacher Quenia�Ribeiro, of the�renowned dance school Ailey Extension demonstrates basic samba reggae moves that work up a solid sweat. Ready to get down and groove? Follow along for a heart-pumping, fat-blasting workout you�ll actually have fun doing.
Samba reggae basic step: Standing with your feet slightly wider than hip-width, bounce from one foot to the other, moving your hips from side to side as you bounce.
The snake: Adding on to the basic step, roll your upper body and arms in a snake-like movement to the right as you step to the right side. Clap as you return your torso to center, then repeat on the left.
The shake: Standing with your feet slightly wider than hip-width, step your right leg out to the side as you sit into a squat and pop the hips forward and back. Continue to stay low as you repeat this movement on the other side, stepping out with the left leg. Stay loose in the hips as you alternate stepping out onto each leg.
Cross-and-pull: From standing, step and cross the right leg over the left as you pull the right arm down in front of the body. Return to center and repeat on the left. Bounce from side to side as you alternate doing this cross-and-pull movement on the left and right.
Window washers: Standing with your feet slightly wider than hip-width, shift your weight as you bounce your hips from one side to the other, holding your arms out to each side and moving them in quick circular movements, as if washing windows.
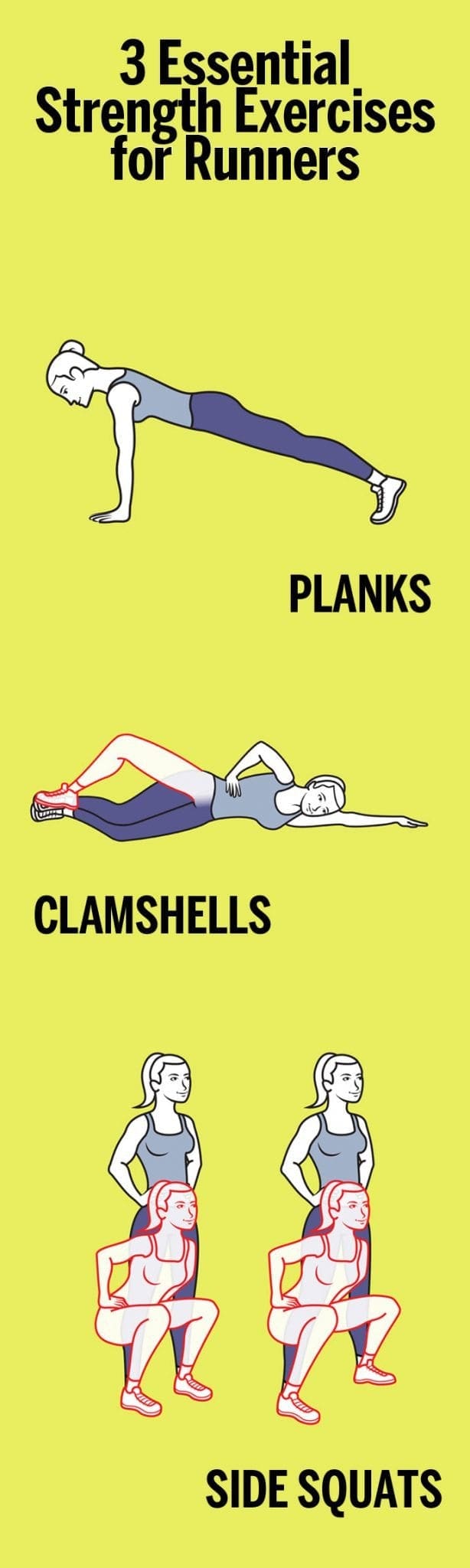
Trying to be a better runner? It’s not just about logging miles (although that certainly helps). The key to running strong and long also has a lot to do with shoring up your muscles, activating your core and back in addition to your lower body,�and keeping your movements fluid. To help do that, start incorporating these full-body strengthening�moves from Nike+ Run Club coach Julia Lucas to your routine three days a week, before or after a run. You’ll start noticing a difference in your strength in no time.
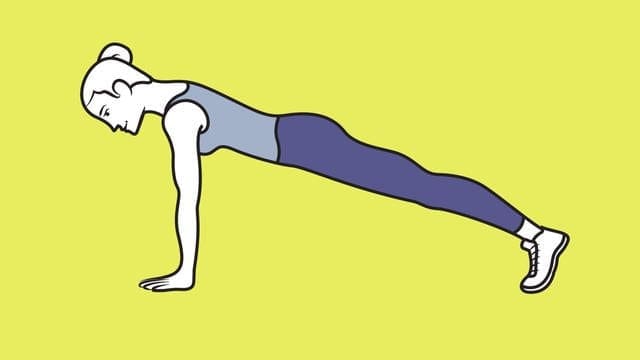
1. Planks
�
Planks have long been considered one of the best exercises for your core. In addition to your abs, this move engages your back, quads, and hamstrings, making it a great full-body exercise for runners. To do it, get into the �up� part of a push-up, with palms�on the floor directly under shoulders and legs extended behind you, forming a straight�line from head to heels. Hold for 10 to 30 seconds, keeping abs tight. Do�2 or 3 sets.
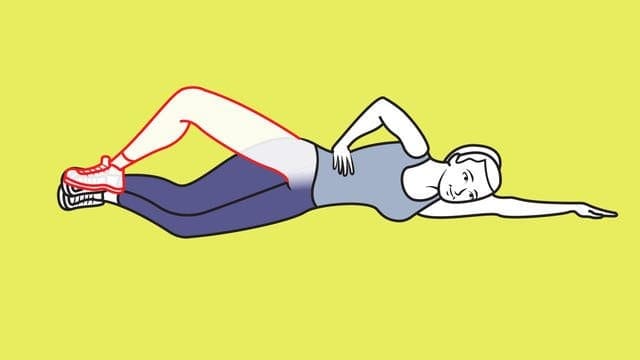
Clamshells work your hips and glutes, parts of the body that runners regularly need to activate. To do them, start out by lying�on your side with legs stacked and knees bent at 45 degrees. Rest head on arm; place top hand on hip. With inside edges of feet touching, lift top knee as high as you can without shifting hips or pelvis. Pause; lower knee. Do 2 or 3 sets of 10 reps per side.
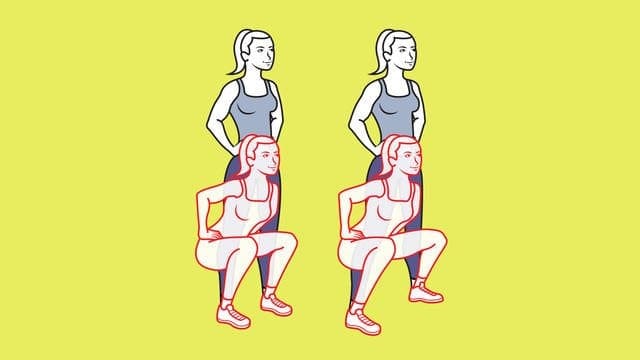
3. Side squats
Side squats are a great way to strengthen your outer highs, hips, and glutes. To do, stand with feet hip-width apart, hands on hips; squat. Stand; move left foot a step out. Squat again; step left foot in as you rise. Continue, alternating sides. Do 2 or 3 sets of 10 to 12 reps per side.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine