Several studies have suggested that menopause may increase the risk of hearing loss, possibly due to lower estrogen levels, and that postmenopausal hormone replacement therapy might slow the decline. But researchers at Brigham and Women’s Hospital found that hormone therapy actually increased the risk of hearing loss.
Researchers examined links between menopausal status, oral hormone therapy, and risk of self-reported hearing loss in more than 80,000 women in the Nurses’ Health Study II.
During the 22-year study period, 23 percent of the participants developed hearing loss. Although no significant association was found between menopausal status and the risk, using postmenopausal hormone therapy was linked to a higher risk of hearing loss. The longer women used hormone therapy, the greater their risk.
“Our research focuses on identifying preventable contributors to hearing loss,” said lead author Dr. Sharon Curhan. “Although the role of sex hormones in hearing is complex and incompletely understood, these findings suggest that women who undergo natural menopause at an older age may have a higher risk. In addition, longer duration of postmenopausal hormone therapy use is associated with higher risk.
“These findings suggest that hearing health may be a consideration for women when evaluating the risks and benefits of hormone therapy,” she said.
The findings are published online May 10, 2017 in Menopause, The Journal of the North American Menopause Society.
An earlier study by Dr. Curhan of 65,000 women found that those who eat at least two servings of fish every week have a lower risk of age-related hearing loss.
Although hearing loss is often considered an inevitable part of aging, those who ate two or more servings a week had a 20 percent lower risk of hearing loss when compared to women who rarely ate fish. “Consumption of any type of fish tended to be associated with lower risk,” said Dr. Curhan. “These findings suggest that diet may be important in the prevention of acquired hearing loss.”
Approximately 48 million Americans suffer from hearing loss, and the number is expected to increase as the population ages.
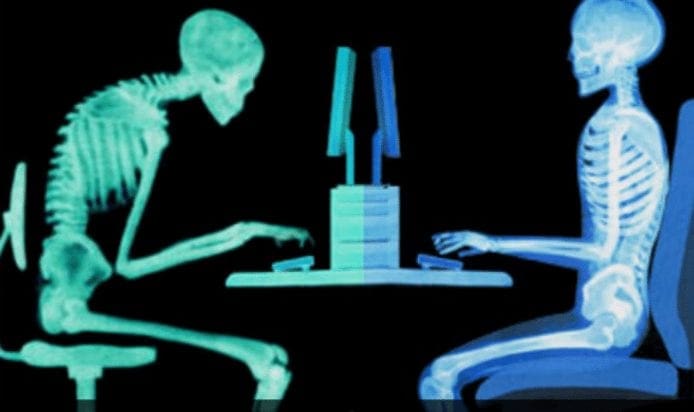
Poor posture is an incredibly common problem in today�s world. With the increase in technology and decrease in physical exercise, many people find their posture slipping more than ever before. While we know that good posture certainly looks better, is it really cause for concern? Take a look at these ways in which poor posture may negatively impact health, followed by some tips for improving it a little more every day.
The Effects of Poor Posture
Pain in the Back, Neck, and Shoulders – Poor posture can cause stiffness or pain in any of these areas. The longer you sit or stand with bad posture, the more pronounced these pains are likely to be.
Slow Digestion – Poor posture is almost always because of slumping or slouching the shoulders and core. This can cause the digestive tract to be pressed, which can make any sort of digestion painful and more troublesome.
Poor Self Perception – Our minds often take cues from the body. If slouching is a constant, our minds get the message that we feel poorly about ourselves, and our self-esteem and perception is likely to take a hit.
Solutions for Bad Posture
Exercise – Both regular exercise as well as posture specific exercises can help strengthen the body and improve overall posture. This might include moves that especially work the core, back, and shoulders.
Find Some Triggers – Bad posture is a tough habit to break. It can help to give yourself constant reminders. Ask a friend to remind you when they see you slouching. Post sticky notes all over the mirror or your desk at work. Set intermittent alarms on your phone. Do whatever it takes to bring good posture to the forefront of your mind.
Get Chiropractic Care – This is actually a great place to start for correcting poor posture. Chiropractors can eliminate painful areas of the spine that may be contributing to poor posture. They may also help to increase flexibility, improve mobility, as well as give you some simple everyday tips for getting your posture and basic spinal health in check.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Additional Topics: Preventing Spinal Degeneration
As we age, it’s natural for the spine, as well as the other complex structures of the spine, to begin degenerating. Without the proper care, however, the overall health and wellness of the spine can develop complications, such as degenerative disc disease, among others, which could potentially lead to back pain and other painful symptoms. Chiropractic care is a common alternative treatment option utilized to maintain and improve spine health.
Kicking the sugar habit is no easy task. But if you�re considering giving it a try, here�s some inspiration to help you succeed: it�ll have profound effects on your short- and long-term health.
A little of the sweet stuff is okay; the American Heart Association recommends consuming no more than 6 teaspoons of added sugar a day for women and 9 teaspoons daily for men. (Quick comparison: a 12-ounce can of cola has approximately 8 teaspoons.) And you can keep eating unprocessed foods that contain natural sugar, like fruits and vegetables. Unlike added sugar, natural sugar hasn�t been stripped of the vitamins, minerals, and fiber Mother Nature packaged them in.
But if you can dial your intake of added sugar way back, you�ll start to rack up some amazing body benefits, like these.
Your skin will look younger
Think less sag and fewer wrinkles. Studies suggest that the amount of sugar in the blood (which is affected by how much sugar you eat) sets up a molecular domino effect called glycation, which ultimately leaves skin less firm and elastic. Already bothered by premature lines? Cutting your sugar intake can reduce visible signs of aging, research shows.
You�ll have less belly fat
This is the visceral or �deep� fat that builds up around vital organs like your liver, pancreas, and intestines. Stubborn and hard to get rid of, it�s also dangerous; visceral fat is a known risk factor for heart disease and diabetes. In 2016, data from more than 1,000 people who are part of the ongoing Framingham Heart Study showed that the more sugar-sweetened beverages they consumed, the higher their level of visceral fat.
Added sugars are simple carbohydrates. This means they�re digested fast and enter your bloodstream quickly, providing that sugar high that helps jump-start your energy and alertness. But as anyone who relies on a candy bar or pastry for a pick-me-up knows, once that shot of sugar is metabolized, you’re in for a crash.
When you need fuel, swap the sugar-sweetened meals and snacks for items that are low in sugar yet high in protein and/or fat, like almonds. Because they take longer to digest, they�ll supply you with a steadier stream of energy that will last longer, says Diane Sanfilippo, a certified nutrition consultant and author of The 21-Day Sugar Detox.
You�ll lower your risk of obesity
Epidemiological studies show a striking correlation between weight gain and sugar consumption. One study that looked at data from 75 different countries between 1997 and 2010 found that a 1 percent rise in soft drink consumption across a nation was linked to an additional 4.8 people out of 100 being overweight and an additional 2.3 people out of 100 being obese.
Here are some more numbers: sugar has 16 calories per teaspoon, which may not sound like a big deal. But considering how much added sugar is loaded into tons of products, consuming sweetened foods can easily add hundreds of calories to your diet�calories that you may not need and may end up as dangerous fat around your middle.
A healthy heart helps you power through your day, from that a.m. spin class to a late deadline at work. But the more added sugar in your diet, the higher your risk of dying of heart disease, even if your weight is in a healthy range.
In one 2014 JAMA study, researchers found that those who consumed the highest amount of sugar � accounting for more than 21 percent of their totally daily calories �had double the heart disease death risk of people who took in 17 to 21 percent of their daily calories from the sweet stuff. This group in turn had a 38 percent higher risk of dying from cardiovascular disease compared to those who kept their sugar intake to 8 percent of their daily calories (The FDA says getting 10% of your daily calories from added sugar is a solid guideline).
Researchers have long debated whether there was a direct connection between eating sugar and developing type 2 diabetes. But recent research has lent support to this theory. A 2014 Stanford University study of 175 countries found that the more sugar that is available in a population’s food supply, the higher the diabetes rate�and this was true even when a country’s obesity rate was not factored in. (Obesity itself can set a person up for diabetes).
Epidemiological data also suggests that among other factors, diets high in sugar�even in diets that are not necessarily high in calories�cause the body to store visceral fat around the middle, and that can lead to insulin resistance and a diabetes diagnosis.
Scientists believe that turmeric my hold the key to better bone density
The study involved fit, healthy and slim men and women who all suffered declining bone density.
In just six months, those taking a daily tablet of the turmeric and soy lecithin formulation boosted bone density by seven per cent compared with a group given a placebo.
The quality of bone in the heels, jaws and fingers of the group – who had an average age of 70 – was measured at the start of the project using specialized ultrasound scanning.
Related articles
Weight loss tips: Adding TURMERIC to your diet sheds fat FAST
Dementia could be cured with THIS ingredient in your curry
By the end of the trial bone density had increased in all three sites by up to 7 per cent above the placebo, suggesting a significant benefit.
Curcumin researchers from the University of Sydney, Australia, along with INSERM the French government’s medical research laboratories, and a team of doctors from four prestigious American universities, have published similar conclusions.
Doctors are increasingly concerned that almost three quarters of elderly people lose strength-providing bone mineral.
GETTY
The spice may hold the secret to battling osteoporosis in the elderly
The condition called osteopenia, mostly caused by a lack of exercise, can worsen into osteoporosis and lead to fatal fractures if untreated.
We’re are delighted by these results
Alf Lindberg
Every year about 65,000 people suffer hip fractures caused by bone fragility, leading to the deaths of up to 35 per cent of victims in the older age groups.
Turmeric+, which comes from the powerful root of the curcumin plant, is sold in Britain by the Cambridge bioscience company Cambridge Nutraceuticals under the brand FutureYou.
Alf Lindberg, a former Nobel prize committee member who is a scientific spokesman for Cambridge Nutraceuticals, said: �We’re are delighted by these results, and we are stepping up our osteoporosis research programme with turmeric as a result.
�Our formulation is better absorbed by the human body than turmeric in its natural form, and we believe it could offer an earlier side-effect free alternative for people at risk from osteoporosis.�
Bone mineral density is regulated by maintaining a balance between bone-building osteoblast cells and osteoclasts, which are designed to mop up ageing bone cells for replacement.
In older people osteoclast activity may outweigh the rate of bone replacement.
GETTY – STOCK IMAGE
Almost three quarters of elderly people lose strength-providing bone mineral
Stefano Togni, is scientific spokesman for the world’s largest researcher into plant based treatments, Indena, which developed the raw material for Turmeric+.
He said the Italian company had produced similar promising bone-building results with the uniquely bioavailable compound in animal studies.
He said: �Our work suggests this form of curcumin dampens down the rate of bone resorption which could be very good news, because it would mean that people who are in the early stages of bone loss will now have a treatment.”
Elise Verron, a specialist in the evaluation of medicines for INSERM from the University of Nantes in France, was a co-author of a review of the bone-building properties of curcumin and turmeric in the Nature journal Bonekey.
Tue, April 25, 2017
The TEN foods to eat to live past a hundred.
Getty
1 of 11
10 things to eat to live past 100
She agrees that the key to harnessing its power will depend on developing strategies to improve absorption.
She said: �In the past decade there has been growing interest in curcumin because of its low toxicity and multiple therapeutic actions including anti-cancer, anti-inflammatory and anti-microbial activities, but few studies have looked at its effect on bone tissue.
�At the moment it is too early to get a clear idea of the benefit.�
GETTY
Turmeric comes from the powerful root of the curcumin plant
Luca Giacomelli, of the department of integrated diagnostics at Genoa University, who was one of the leaders of the new Italian study, said the results were promising.
But he cautioned that the effect cannot be replicated simply by adding regular curry to the diet because turmeric in food is less easily absorbed.
He said: �People need to take this kind of high quality supplement under medical supervision.�
The findings may also come as good news for thousands of people advised by doctors to take bisphosphonate drugs designed to maintain bone density by reducing the rate of bone breakdown.
Latest research has suggested that long term users of these drugs may suffer ‘microcracks’.
Intense physiological stress can change the composition of our gut microbiota
Imbalances in the gut arelinked to diabetes, obesity and some cancers
Findings raise concerns for endurance athletes and military personnel
The study is the first to investigate gut bateria during military training
Long periods of intense exercise can change the composition of your gut bacteria, a new study has found.
The research looked at soldiers taking part in an intensive training programme and found that pro-longed exercise caused the protective barrier in their guts to become permeable.
In other words, the prolonged exertion triggered �leaky guy syndrome� � a condition that could let harmful substances leak into the bloodstream.
With our gut health and overall health believed to be strongly linked, intense physiological stress could therefore raise the risks of many types of illnesses.
The new research is the first to investigate the response of gut microbiome � the term for the population of microbes in the intestine � during military training.
It provides a stark warning for endurance athletes and military personnel.
The study suggests physical stress can increase intestinal permeability, which can raise the risk of inflammation and illness
Most of us are aware that the bacteria in our gut play an important role in digestion. Furthermore, they are known to aid the production of certain vitamins � such as vitamins B and K � and play a key role in immune function.
But increasingly, research is emerging showing how poor gut health is linked to conditions ranging from irritable bowel syndrome, diabetes, high blood pressure, depression, obesity, childhood asthma, to colitis and colon cancer.
The study is the first to investigate the response of gut microbiome � the term for the population of microbes in the intestine � during military training.
It looked at a group of 73 Norwegian Army soldiers taking part in a military-style cross country skiing training programme.
Recent research suggests our gut bacteria holds the key to improving our health � and may be the key to tackling obesity
The group skied 31 miles (51 km) while carrying 99-pound (45 kg) packs, across four days.
Before and after the training exercise, researchers collected blood and stool samples from the soldiers.
It was found that the microbiome and metabolites � the substance formed in or necessary for metabolism � in the soldiers� blood and stool altered �significantly� by the end of the aggressive training period.
Furthermore, sucralose excretion in their urine samples rose considerably, indicating an increase in intestinal permeability (IP).
Scientists know that healthy intestines have a semi-permeable barrier, which acts as a defense to keep bacteria and other harmful substances out, while allowing healthy nutrients into the bloodstream.
It is thought that physical stress can increase IP, increasing the risk of inflammation, illness and symptoms such as diarrhoea.
The findings may spell bad news for endurance athletes and military personnel
The researchers wrote: �Intestinal microbiota appear to be one influencing factor in the gut�s response to physical stress.
�Our findings suggest that the intestinal microbiota may be one mediator of IP responses to severe physiologic stress, and that targeting the microbiota before stress exposure may be one strategy for maintaining IP.�
The study was published ahead of print in the American Journal of Physiology � Gastrointestinal and Liver Physiology.
MICROBIOME: DOES IT CONTROL EVERYTHING?
Researchers now estimate that a typical human body is made up of about 30 trillion human cells and 39 trillion bacteria.
These are key in harvesting energy from our food, regulating our immune function, and keeping the lining of our gut healthy.
Interest in, and knowledge about, the microbiota has recently exploded as we now recognise just how essential they are to our health.
A healthy, balanced microbiome helps us break down foods, protects us from infection, trains our immune system and manufactures vitamins, such as K and B12.
It also sends signals to our brain that can affect mood, anxiety and appetite.
Imbalances in the gut are increasingly being linked to a range of conditions. Last year, scientists at California Institute of Technology found the first ever link between the gut and Parkinson�s symptoms.
The composition of our gut microbiota is partly determined by our genes but can also be influenced by lifestyle factors such as our diet, alcohol intake and exercise, as well as medications.
Do you yearn for a strong and flexible back along with a super flat tummy? So, what�s the relationship between a strong back and super flat tummy? When your back is strong and flexible, you will be able to work on strengthening and toning your core muscles. And, when your core shrinks and tones, you will enjoy a flat tummy. Bonus � better posture, better digestion, regular bowels, more energy, and a happier you!
In this article, we�ll be looking at some poses, 7 to be precise, that will stretch, strengthen, and tone your back. So are you ready?
7 Yoga Postures for a Strong and Flexible Back
Parivrtta Trikonasana � Revolved Triangle Pose
As the name suggests, it involves a twist. Just make sure you twist from your abdomen while maintaining the length of your spine to reap the most out of this posture.
Stand with your feet together, palms resting along the body. Inhale and separate your feet about 4 feet apart. Raise your arms at shoulder level, palms facing the floor. Roll your shoulders down and away from your ears. Engage your core and lengthen your spine. Exhale and turn both feet to your right. Inhale and square your hips to the right.
Exhale and place your left palm inside your right foot. Inhale, twist your torso and lift your right arm up, fingertips pointing to the ceiling. Gaze at the fingertips. Beginning students should keep their head in a neutral position, looking straight forward, or turn it to look at the floor.
Hold the posture without compromising on your breath for seven breaths. Exhale, release the twist, and bring your torso back to upright with an inhalation. Repeat for the same length of time with the legs reversed, twisting to the left.
Marjariasana � Bitilasana � Cat Cow Pose
This flow is one of the simplest movements practiced in Yoga Vinyasas to warm up your back and core. But those who practice it daily vouch for its core and back strengthening benefits.
After completing Parivrtta Trikonasana on both sides, join the feet together. Inhale and swing your arms over your head. Exhale and fold forward, placing your palms on either side of your feet. Walk your legs back and drop your knees down to come into Table Top position.
Adjust your knees to stack them under your hips. Stack your shoulders over your palms. Allow the tops of your feet to press on the floor; toes extended backward. Spread the fingers and press the palms into the floor.
Inhale, arch your back, and gaze up, stretching your neck [Cow]. Hold for seven breaths. Exhale, round your back, pull your navel towards your spine, engage your gluteus muscles, and tuck your chin to the chest. Gaze down [Cat] and hold the posture for seven breaths.
Repeat the movement slowly ten times.
Tips: If you have a knee injury, fold your mat or use a folded blanket to add additional cushioning for your knees.
Bhujangasana � Cobra Pose
This backbend works wonderfully stretching your upper and lower back, toning the muscles, and strengthening them. Just do this stretch after a long day of sitting and experience its soothing impact!
Once you complete Cat Pose for the last time, bring your spine to a neutral position in Table Top. Gently walk your arms forward and lower your body to the floor. Stretch your legs backward. Allow the forehead to rest on the ground.
Adjust your palms to align them along with your chest, wrists stacked under your shoulders. Press the tops of your feet on the floor, toes extended back. Keep your legs active. Roll your shoulders down and away from the ears so that the shoulder blades come closer.
On an inhale, press the palms firmly into the floor and lift your forehead and chest off the mat until your ribs are completely away from the floor. Allow your hips to rest on the ground. Exhale and on the next inhalation, bend backward, tilting your head slightly back.
Deepen the stretch until your experience a tingle on your lower back. Hold the posture, squeezing your gluteus and pulling your navel to the spine, for seven deep breaths.
Exhale and slowly come back to lying.
Tips: Gaze forward if you have any neck injury.
Dhanurasana � Bow Pose
Bending your body like a bow improves the suppleness of your back. As you pull your heels away from the buttocks, the legs stretch, and tone. Other benefits � better digestion, flatter stomach, and toned arms.
From Bhujangasana, exhale and lie with your forehead on the floor. Separate your legs as wide as your hips. Bend your knees and allow the heels to come close to your buttocks. Let the big toes to come into contact. Hold the ankles with your palms. Inhale and lift your head and chest off the mat until your entire rib cage is up from the floor.
Balance on your lower abdomen and pull your legs away from your buttocks. Squeeze your buttocks to feel the stretch on your back. Hold the posture, breathing deeply, for seven deep breaths.
Variation: Practice Parsva Dhanurasana by turning your torso sideways on an exhalation. Maintain the legs. Come back to center before repeating on the other side.
Setu Bhandasana � Bridge Pose
This posture strengthens your core, legs, back, and hips. Feel free to use a block or anything else to support your lower back.
Release your legs and palms and lie down on your abdomen, resting the forehead on the floor. Take five deep breaths to relax your body and breath. Turn to your right and lie down on your back, hands resting on the sides, palms flat on the floor.
Roll your shoulders down to rest them firmly on the floor. Bend your knees, separating them hip-distance apart. Allow your knees to fall towards each other slightly. Pressing the feet and palms into the floor, inhale, and lift your hips away from the floor.
Exhale, squeeze your thighs and roll them inward. Lift your hips higher to bring your chest closer to the chin. If possible, interlace your fingers beneath you.
Hold the posture breathing for seven long, deep breaths.
Exhale and slowly release your hips to the floor.
Variation: Once you are in Bridge Pose, inhale and lift your right leg perpendicular to the floor and hold for five breaths. Exhale, release the right leg, and repeat on your left.
Chakrasana � Wheel Pose
It is a complete body strengthener and toner. However, if you have a meniscus, ligament, wrist, or shoulder injury, please refrain from practicing this pose as it could worsen the pain and inflammation.
Keep your legs just as you kept for Setu Bhandasana. Place your palms at shoulder level, fingers pointing towards you. Pressing the palms and feet into the floor, lift your head and body off the floor. Tilt your head backward and gaze up to feel the stretch on your neck.
Stretch your thighs and shoulders. In the final position, your body looks like an arch, almost like a wheel. Breathing deeply, hold the posture for seven deep breaths.
To release the position, lower your body till it touches the ground. Straighten your legs.
Tips: Avoid the posture if you have hypertension or vertigo and during menstruation.
Ardha Matsyendrasana � Half Spinal Twist
Ardha Matsyendrasana translates into the half twist pose of the king of fishes. An excellent detoxifying pose, it works on stretching and strengthening your upper back.
After completing Chakrasana, turn to your right and sit with your legs extended forward. Bend the right leg, lift it and place it close to your left hip. Bend the left leg and place it under the right buttocks. Inhale and lift your left arm up. Exhale and bring the left arm around your right leg and hold your right toes. The left armpit should rest outside the left knee.
Place your right arm on your back, allowing the right fingertips to rest on your left thigh. Exhale and twist to your right. Look over your right shoulder and fix your gaze at one point. Hold for seven breaths.
Inhale and come back to center slowly and stretch out your legs. Repeat on your left side.
While certain poses outlined above might feel terrible during the first practice, regular practice will make you perfect.
So start practicing these poses to tone your back and improve your core!
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Additional Topics: Preventing Spinal Degeneration
As we age, it’s natural for the spine, as well as the other complex structures of the spine, to begin degenerating. Without the proper care, however, the overall health and wellness of the spine can develop complications, such as degenerative disc disease, among others, which could potentially lead to back pain and other painful symptoms. Chiropractic care is a common alternative treatment option utilized to maintain and improve spine health.
Besides your personality body alignment says a lot about how your muscles and joints are working. Learn more about assessing your postural deviations and how to fix them!
Many studies show that how you feel and look is directly linked to your posture. Even the people know how important is to have good posture, most them don�t do anything to improve it.
Many of you probably live with deformed backs and imbalanced hips, and, of course, deal with the pain that you think is normal.
How dangerous can be to live with bad posture? It can lead to plenty of problems:
� Chronic back, shoulder and neck pain
� Headaches
� Injuries to feet, knees and hips
� Fatigue
� Stiffness
� Difficulty breathing
� Muscle atrophy and weakness
� Impingement and nerve compression
� Digestion issues
� Carpal tunnel syndrome
� Sciatica
If you are suffering from any of these problems, you should understand proper posture and learn about your own postural deviations.
Correcting Your Alignment
To solve a problem, you first need to find out what causes it. Most of the postural deviations occur as the muscles that work to hold a joint in place are imbalanced.
You can correct imbalances by strengthening the underactive muscles and to stretching the overactive muscles
Standing Assessment
For you who are not sure whether your posture is good or it needs a little correction, do this standing assessment first:
� Put on form-fitting clothes,
� Stand shoeless, tall but comfortable, do not trying to force yourself to stay in perfect posture.
� For an honest assessment, close your eyes and march slowly in place a few times.
� Have a friend take a full body picture of you
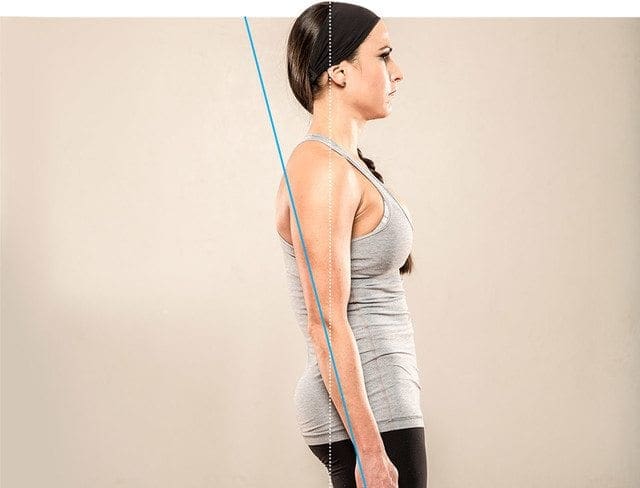
Here�s what a properly postured body should look like:
� Picture � posture
Standing Assessment Postural Deviations
I � Back, Shoulders, Hips, And Head
Here�s how you can correct these deviations:
Deviation 1: Sway Back � Hips Press Forward and Sit In Front Of the Ribs
Overactive muscles: erector spinae, gluteus maximus and medius, hamstrings and quadratus lumborum Stretches: Runner�s stretch, seated glute stretch, world�s greatest stretch, hamstring stretch, lying crossover, hamstring self-myofascial release (foam rolling)
Underactive muscles: Iliopsoas, rectus femoris (hip flexors and lower abs) and external obliques
Strengthening exercises: Cocoon, hanging leg raise, exercise ball pull-in and scissor kick
Deviation 2: Lower-Cross Syndrome
Excessive Curve In The Low Back, Pelvis Is Tilted Forward
Overactive muscles: erector spinae (hip flexors and low back) and Iliopsoas
Stretches: quadriceps self-myofascial release, quadriceps stretch, pyramid stretch over ball, hug knees to chest and kneeling hip flexor,
Underactive muscles: gluteus maximus and abdominals
Strengthening exercises: Pelvic tilt to bridge, exercise-ball hip bridge, single-leg glute bridge, frog sit-up and leg elevated crunch,
Deviation 3: Rounded Shoulders
Shoulders In Front Of Ears
Overactive muscles: Pectoralis minor and major (chest)
Stretches: Front deltoid stretch, chest stretch on stability ball, dynamic chest stretch, elbows-back stretch, chair upper-body stretch
Underactive muscles: Rotator cuff, serratus anterior (muscles in the back surrounding the shoulder blades and rear delts) and lower trapezius,
Strengthening exercises: Seated cable row, shoulder external rotation, back fly with band, rear- delt row
Deviation 4: Forward Head
Ears In Front Of Shoulders
Overactive muscles: Neck extensors, levator scapula (muscles behind the neck that tilt the head back) and upper trapezius,
Stretches: Neck self-myofascial release, sternocleidomastoid stretch and chin to chest,
Underactive muscles: Neck flexors (muscles in front of the neck that tilt the head forward)
Deviation 5: Upper-Cross Syndrome
Rounded Shoulders With An Excessive Curve
Overactive muscles: Trapezius, pectoralis major and minor, levator scapula, neck extensors (the back of your neck, upper back, traps, and chest)
Stretches: Neck self-myofascial release, front-delt stretch, chin to chest, chest stretch on stability ball, elbows-back stretch, chair upper-body stretch and dynamic chest stretch
Underactive muscles: Rotator cuff, rhomboids, lower trapezius, deep neck flexors (muscles in the back surrounding the shoulder blades, rear delts, and in front of the neck) and serratus anterior
Strengthening exercises: back fly with band, seated cable row, isometric front-neck exercise, rear-delt row and shoulder external rotation,
Deviation 6: Head Tilt
Head Tilted To One Side (Can Be Accompanied By Rotation toward That Side)
Overactive muscles: Sternocleidomastoid tilted toward the midline.
Stretches: Side neck stretch, sternocleidomastoid stretch and neck self-myofascial release,
Underactive muscles: Sternocleidomastoid tilted away from the midline.
Strengthening exercises: Perform daily activities (e.g., chewing, pulling, lifting, carrying, and using a cell phone) evenly on both sides, isometric side-neck exercise
Deviation 7: Uneven Shoulders
One Shoulder Sits Higher Than The Other
Overactive muscle: Trapezius (muscle running from the back of the neck into the shoulder girdle) on the elevated side
Stretches: Side neck stretch, neck self-myofascial release
Underactive muscles: Serratus anterior
Strengthening exercises: single-arm high-pulley row, perform daily activities on both sides
Deviation 8: Uneven Hips
One Hip Sits Higher Can Give The Perception Of Leg Length Discrepancy
Overactive muscles: hip abductors, internal and external obliques, erector spinae and quadratus lumborum on the raised side
PUSH-as-Rx � is leading the field with laser focus supporting our youth sport programs.� The PUSH-as-Rx � System is a sport specific athletic program designed by a strength-agility coach and physiology doctor with a combined 40 years of experience working with extreme athletes. At its core, the program is the multidisciplinary study of reactive agility, body mechanics and extreme motion dynamics. Through detailed and continued assessments of the athletes in motion and under stress loads offer a clear scientific picture of body dynamics. This system also has helped many athletes come back from injury faster, stronger, and ready to safely return to their sport without losing a beat after recovery. Results demonstrate clear improved agility, speed, decreased reaction time and advantageous postural-torque mechanics.� PUSH-as-Rx � offers specialized extreme performance enhancements to our athletes no matter the age.
Here at PUSH we Are Experts In Specialized Techniques To Accommodate Your Body To What Ever Sport You Are Practicing.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
PUSH-as-Rx �� is leading the field with laser focus supporting our youth sport programs. The PUSH-as-Rx �� System is a sport specific athletic program designed by a strength-agility coach and physiology doctor with a combined 40 years of experience working with extreme athletes. At its core, the program is the multidisciplinary study of reactive agility, body mechanics and extreme motion dynamics. Through continuous and detailed assessments of the athletes in motion and while under direct supervised stress loads, a clear quantitative picture of body dynamics emerges. Exposure to the biomechanical vulnerabilities are presented to our team. Immediately, we adjust our methods for our athletes in order to optimize performance. This highly adaptive system with continual dynamic adjustments has helped many of our athletes come back faster, stronger, and ready post injury while safely minimizing recovery times. Results demonstrate clear improved agility, speed, decreased reaction time with greatly improved postural-torque mechanics. PUSH-as-Rx �� offers specialized extreme performance enhancements to our athletes no matter the age.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Malik Decquir shares his reason for staying determined in sports by never giving up and being consistent. Malik found Push-as-Rx �� in order to enhance his physical performance and his experience changed his outlook. He expresses how happy and comfortable he is at Push as Rx and offers his greatest gratitude to the trainers who were there when he needed them the most, giving him great advice, and pushing him to become the best at Push-as-Rx �.
PUSH-as-Rx ���is leading the field with laser focus supporting our youth sport programs.� The�PUSH-as-Rx ���System is a sport specific athletic program designed by a strength-agility coach and physiology doctor with a combined 40 years of experience working with extreme athletes. At its core, the program is the multidisciplinary study of reactive agility, body mechanics and extreme motion dynamics. Through continuous and detailed assessments of the athletes in motion and while under direct supervised stress loads, a clear quantitative picture of body dynamics emerges. Exposure to the biomechanical vulnerabilities are presented to our team. �Immediately,�we adjust our methods for our athletes in order to optimize performance.� This highly adaptive system with continual�dynamic adjustments has helped many of our athletes come back faster, stronger, and ready post injury while safely minimizing recovery times. Results demonstrate clear improved agility, speed, decreased reaction time with greatly improved postural-torque mechanics.��PUSH-as-Rx ���offers specialized extreme performance enhancements to our athletes no matter the age.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine