For decades, health experts have warned about the dangers of being overweight, pointing to an increased risk of many conditions, including heart disease, stroke, diabetes, and some cancers. But several recent studies have found that sometimes being overweight — even obese — can actually be helpful, especially in seniors. The phenomenon is referred to as the “obesity paradox.”
“Society has often led to people being fixated with extreme thinness, particularly for appearance,” says Dr. Carl J. Lavie, a cardiologist at New Orleans’ Oschner Heart and Vascular Institute.
“However, almost every study shows that the underweight and the low end of ‘normal’ weight almost always have the highest mortality rates,” he tells Newsmax Health.
“The obesity paradox is even more noted in older folks than in the young,” says Dr. Lavie. “Older people can be very healthy with weights typically considered in the ‘overweight’ and ‘mildly obese’ ranges, especially if they are fit.”
Check out the following situations and conditions where a few extra pounds can not only be helpful, but could possibly save your life:
Heart attack. Cardiologists from the University of Texas Southwestern Medical Center studied patients who had suffered a major heart attack. They found that those who were mildly obese were 30 percent more likely to survive and spend fewer days in the hospital than those of normal weight. Researchers defined “mildly obese” as having a body mass index (BMI) of 30 to 34.9 compared to a BMI between 18.5 and 24.9, which is considered normal weight.
In an earlier study published in the European Heart Journal: Quality of Care and Clinical Outcomes, UT Southwestern researchers examined records from Medicare patients discharged after a heart attack involving total artery blockage. They then compared them with later treatment records to determine how the patients fared over the next three years. The mildly obese patients did better than all other groups, while those who were of normal weight or extremely obese fared the worst.
Stroke. Even though obesity increases the risk for stroke, a study from Boston University Medical Center found that people who are overweight or even mildly obese are more likely to survive strokes over the following 10-year period than those of normal body weight. The benefit was strongest in males and in those under than the age of 70.
Angioplasty. Dr. Luis Gruberg at the Cardiovascular Research Institute in Washington found that overweight and obese patients died at half the rate of normal-weight people following angioplasty, a procedure that unblocks arteries in the heart. He nicknamed the phenomenon the “obesity paradox.”
Longevity. An analysis of 97 studies published in the Journal of the American Medical Association found that although obesity raised the risk of death, people who were mildly obese (a BMI of 30 to 34.9) had a 5 percent less chance of dying than those with normal BMIs. Those who were considered overweight with a BMI between 25 and 29.9 had a mortality rate that was 6 percent lower than those with normal BMIs. In addition, a British study found that people with Type 2 diabetes who were overweight, but not obese, had a lower risk of dying over a decade than their counterparts who were normal weight or underweight.
Sexual stamina. Sex with a person with a higher BMI lasts an average of 7.3 minutes longer when compared to underweight men or those of average weight. The answer appears to be the hormone estradiol, a form of the female hormone estrogen. It is found in excess abdominal fat and is known to slow male orgasm.
Heart failure. In studying his patients who were recovering from heart failure, Dr. Levie found that for every 1 percent increase in body fat, overall survival increased 13 percent.
Dementia. Those extra pounds may help protect you from dementia, found a study published in The Lancet Diabetes & Endocrinology. Researchers found that those who were classified as overweight with a BMI of 24 to 29 had an 18 percent lower risk of developing dementia. The risk was even lower for those whose BMI was 30 or above. But people who were underweight increased their risk by 29 percent.
Arthritis. A Swiss study published in the journal Rheumatology found that the higher a man’s body mass index (BMI), the lower his chance of developing chronic arthritis. Overweight and obese men were found to have a decreased risk of up to 63 percent when compared to men of normal weight.
Unfortunately, many people can relate to having been involved in a car crash or motor vehicle crash (MVC) at a certain point in their lives. Whether it was a major accident or a little one, MVC’s are no fun and can cause a variety of injuries. These injuries can often be whiplash injuries.
The implications of a motor vehicle crash, in addition to interruption of your daily routine because of whiplash, can often lead to injuries or conditions which may take years to recover from.
With much more distracted drivers texting and speaking on their telephones, MVC’s are on the rise, making for even more dangerous roadways. While other people’s behaviors can not be controlled by us, we can drive more cautiously and defensively to avoid being in an auto accident. Because MVC’s can occur, however, having a plan in mind and being prepared is vital to getting up on our feet and recovering fast.
More serious automobile accidents mean more critical injuries, ranging from wounds and cuts to broken bones or fractures, brain damage, and even death. At first, less serious motor vehicle crashes may not look like a major deal, with sufferers walking away without a scratch, believing they’ve escaped the collision unscathed. Others may just complain of a small headache, neck pain, and/or a stiff neck, resorting to carrying over the counter pain killers, or even wearing a neck brace to assist with their healing — something that’s far from treating the source of the injury.
Cervical Lordosis in Whiplash Prevention
What many people don’t realize though is the extent to which the cervical lordosis, or curvature in your neck as seen from the side, can play an essential role in both: the extent of the initial injury to the occupant(s) and; the long term pain and suffering from whiplash injury to the occupants. Furthermore, the MVC itself will affect the cervical lordosis.
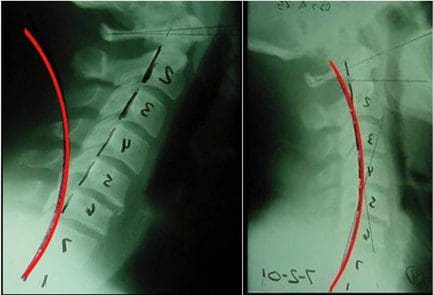
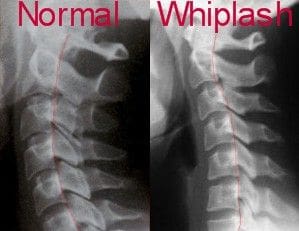
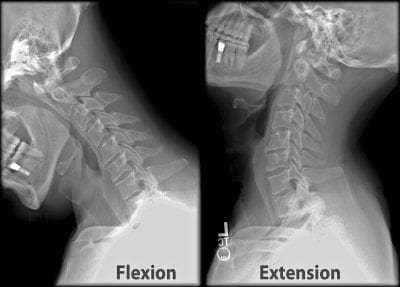
Concerning the degree of initial injury, researchers have found that a well maintained cervical lordosis actually prevents neck tissue damage to the sensitive cervical spine and its structures, in the case of an automobile accident. In the figure on top, the right hand picture demonstrates what a typical curve looks like when seen from�the side and the person is facing to the right. In contrast, the same researchers identified that straightened cervical curves and worse yet, reversed (kyphotic) cervical curves predisposed to more severe cervical spine tissue injuries due to more extreme forces acting on the neck during the exact same MVC circumstances. The x-rays above at the far left and the middle show abnormal neck curves where more severe injury to the person is likely to result should they be involved in an MVC.
Therefore, if you already have an abnormal cervical curvature prior to a MVC, it’s in your best interest to rehabilitate the form and volume of your cervical lordosis. You’re in a higher risk of having significant injuries should you be involved in an automobile collision or other type of accident.
Concerning long term pain and distress, many research studies have identified the patients who undergo long-term whiplash injuries and suffering are in fact the ones who have abnormal cervical lordosis. Straightened, abnormal s-curves and reversed cervical curvatures have been found to pre-dispose after MVC to the following conditions:
Neck pain and stiffness,
Headaches,
Arm pain,
Thoracic outlet symptoms,
Dizziness,
Lack of concentration,
Degenerative arthritis in the cervical spine,
Disc herinations.
What many individuals who’ve suffered whiplash injuries don’t see is that a small pain or neck pain is a genuine indication of a more serious injury to your cervical lordosis and inherent neck tissues. Misalignments as a consequence of motor vehicle crashes, or MVC’s, sudden jolt may manifest immediately, or not become evident at all for a period of time. But this doesn’t signify that the spine is healthy or that no harm was sustained.
Discussion
The fact is that MVC�s statistically damage the shape of your cervical lordosis. Researchers from Chiropractic BioPhysics have identified that the average patient exposed to a MVC will lose 10 degrees of their cervical lordosis, develop a mid cervical kyphosis, and have increased forward head posture as a result of the MVC.
A misaligned cervical curvature as a result of an MVC is a severe medical condition. Altered cervical curves will cause nerve interference � hindrance of critical nerve energy that is responsible for every function of our organs, and every movement of our limbs. Ignoring the cervical spinal misalignment can manifest into pain and discomfort, fatigue, sleep disorders, organ dysfunction, depression, and finally disease.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Automobile Accident Injuries
Whiplash, among other automobile accident injuries, are frequently reported by victims of an auto collision, regardless of the severity and grade of the accident. The sheer force of an impact can cause damage or injury to the cervical spine, as well as to the rest of the spine. Whiplash is generally the result of an abrupt, back-and-forth jolt of the head and neck in any direction. Fortunately, a variety of treatments are available to treat automobile accident injuries.
Definitely, the most frequent injury caused by automobile accidents is whiplash, amounting up to 80 percent of car crash injuries.
Whiplash is a cervical spine, or neck, injury that is caused when the head is jolted either backwards or forward by acceleration or deceleration. The acceleration or deceleration in automobile accidents is typically abrupt, which will cause the head to jerk unexpectedly and be stretched beyond its normal range of motion, straining the neck’s muscles and ligaments. Whiplash can happen at any speed �even when vehicles are traveling as slowly 25 mph.
Severe cases of whiplash can even cause fractures to the neck vertebrae. These accidents might need time off from work and physical activity in order to recover and are painful although a complete recovery is likely.
Level of Damage from Whiplash
Most commonly, whiplash is the result of a rear-end automobile collision, rather than a side impact or head-on collision, though that is possible. In the vehicle, kinetic energy will keep the bodies moving forward in the event of a car accident. Due to restraints like seat belts, the body will be stopped while the head will continue to be thrown backward. This unnatural movement of the neck leads to hypertension injuries. Depending on the seriousness of the impact and how fast the cars were traveling at the time of the incident, the extent of the whiplash will differ.
Traumatic brain injuries will be caused by the whiplash. A healthcare professional will often perform both a physical examination and an X-ray or CT scan to examine the possibility of whiplash in those who were involved in an auto collision. Doctors monitor and might examine brain function to be able to ascertain whether there was damage or injury to the structures surrounding the neck. With acceleration and deceleration injuries, the brain may swell and cause bruising and bleeding. This can be potentially life-threatening.
Cervical acceleration or deceleration injuries result in trauma to the deep anterior neck muscles. When a muscle is torn, it is strained. When a ligament is sprained, it is stretched or torn. As the ligaments in the neck are responsible for maintaining a curve of their neck this can be painful. Neck injuries of this sort will involve micro-tears, but hypertension will result in fractures and larger tears. Many vehicle crash victims after healing, will experience what’s known as myospasm. This symptom involves the sudden contraction of the neck muscles. These spasms can be painful.
Front impact crashes have a greater risk of death and serious injury. Whiplash resulting from a collision can cause injury to the cervical spine and hyperextension. Severe strain of this nature can leave a victim suffering from tension headaches, migraines, and even vision problems for some time even after the neck has healed. The extent of the injuries may depend on which type of vehicle the person traveled in. The size of the vehicles can have a tremendous effect on both severity and the nature of the injuries. Airbags are required in vehicles for safety purposes, but they can actually cause injuries because of their impact when deployed.
If you or a loved one were involved in an auto accident, then you may be suffering from the painful side effects of whiplash and cervical spine injuries. The driver who hit on you may have been cited with a violation, but you might be able to take actions and receive the proper healthcare you deserve.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Automobile Accident Injuries
Whiplash, among other automobile accident injuries, are frequently reported by victims of an auto collision, regardless of the severity and grade of the accident. The sheer force of an impact can cause damage or injury to the cervical spine, as well as to the rest of the spine. Whiplash is generally the result of an abrupt, back-and-forth jolt of the head and neck in any direction. Fortunately, a variety of treatments are available to treat automobile accident injuries.
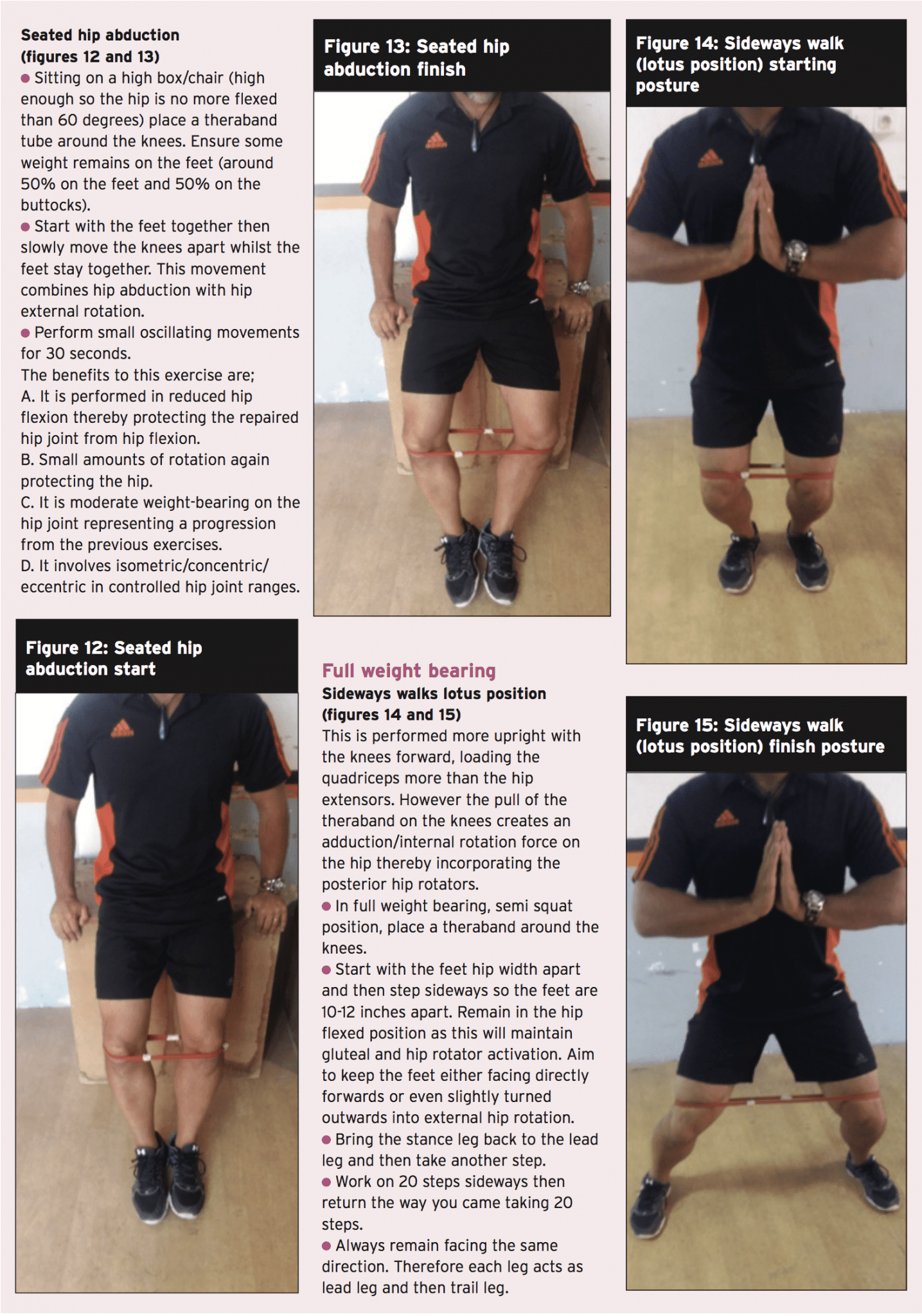
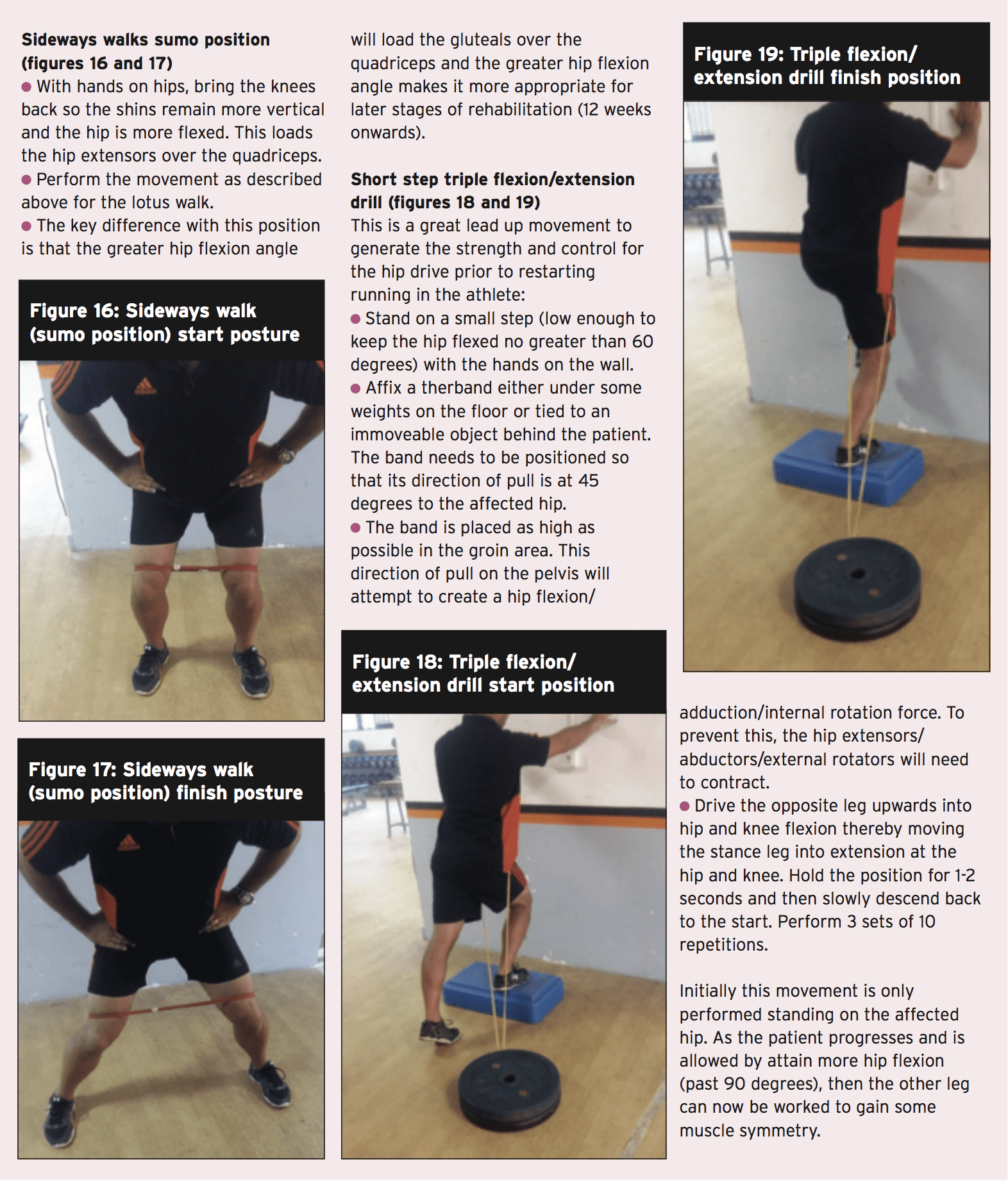
In the first part of the 2-part article on femoro-acetabular impingement (FAI), chiropractor, Dr. Alexander Jimenez discussed FAI and how it can lead to insidious onset abdominal pain and damage the hip joint labrum, leading to early arthritic changes. Given that conservative management generally fails in young athletes and needs operation, part two describes the post-operative rehabilitation period required to take an athlete back to full competition.
The post-operative rehabilitation period is highly dependent on the magnitude of pathology and the subsequent procedure; weight-bearing development is consequently variably reported in the literature.
If the labrum is surgically repaired, then protected weight bearing is encouraged to allow the repair site in order to be protected during the early healing phase. Also, avoiding extremes of flexion (beyond 60�) and also internal/external rotation for the initial 4 to 6 weeks is important to safeguard the repaired labrum. Any positions that possibly create an impingement and boost inflammation ought to be prevented. These include:
Deep squatting
Prolonged sitting
Low couch sitting
Lifting off the ground
Pivoting on a fixed foot
These positions are more safely tolerated following the six week post-operative period. But on account of the selection of hip flexion limitations imposed in the initial six months, usual activities of daily living are rather restricted, making yield to work and daily chores challenging if not impossible from the first few weeks following surgery. Therefore, the post- surgical patient does have to make substantial lifestyle changes and they need assistance in the first six weeks following surgery.
Special precautions in certain types of FAI processes. Reshaping of the femoral head- neck junction can weaken the rectal neck so particular care must be taken in this post- operative period. Fracture of the femoral neck is an unlikely but potentially serious complication after a reshaping process. The athlete may be allowed to bear full weight, but crutches are needed to avoid twisting movements during the initial four weeks after surgery. High impact pursuits and high torsion moves should be prevented in the first 3 months, as bone grafting requires around three weeks to attain full structural integrity.
Furthermore, if microfracture of this femoral head is also done for femoral head cartilage defects, then the athlete ought to be restricted to partial weight- bearing for two weeks so as to optimize the premature maturation of the fibrocartilaginous healing response.
Key points
1. Weight bearing status is dependent on the kind of reshaping procedure, whether the labrum was repaired, and also what the surgeon favors
2. Steer clear of hip flexion beyond 60� in the first 4-6 Weeks
3. Avoid extremes of rotation
Post-Surgical Rehab
Rehabilitation protocols provided in the literature have a tendency to be quite generic in their own advice and at best explain broad transitional phases during the rehab process. They usually describe the transition in weight bearing status, the development of gait through walking into jogging, and give general guidelines as to how to and when to progress activity based on a time dependant strategy.
They then progress describing transitions into twisting and affect actions — usually explained as beginning at 3 weeks following surgery — and generally the guidance is that the speed with which the athlete progresses is variable and might need yet another 1 to 3 months to get full return based on the game. Trainers are usually advised that return to sports after surgical correction of FAI can require 4 to 6 weeks. However it’s critical that progression through rehabilitation phases is driven more by subjective and objective measures during the transition phases. This allows the athlete and therapist to track load (type and quantity) and ascertain whether the joint arrangements are able to withstand changes in load securely.
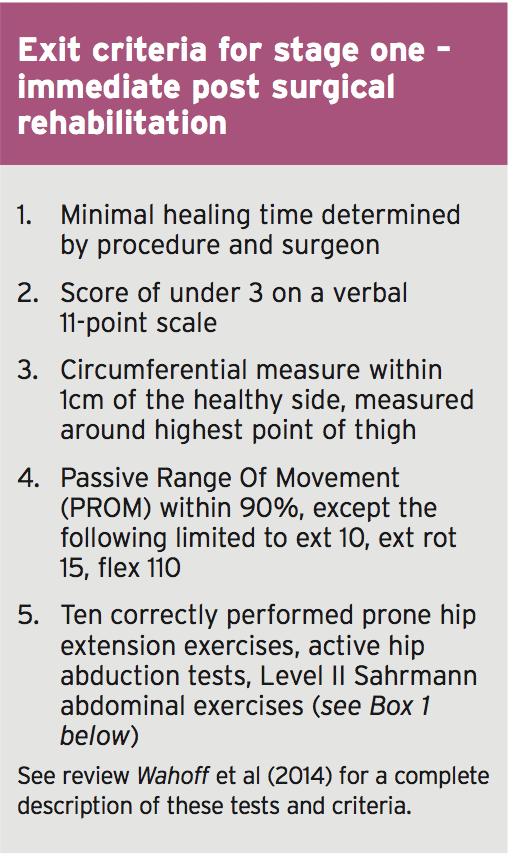
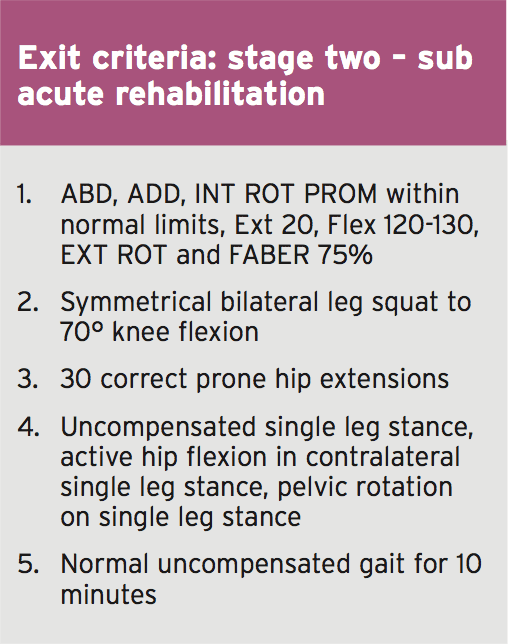
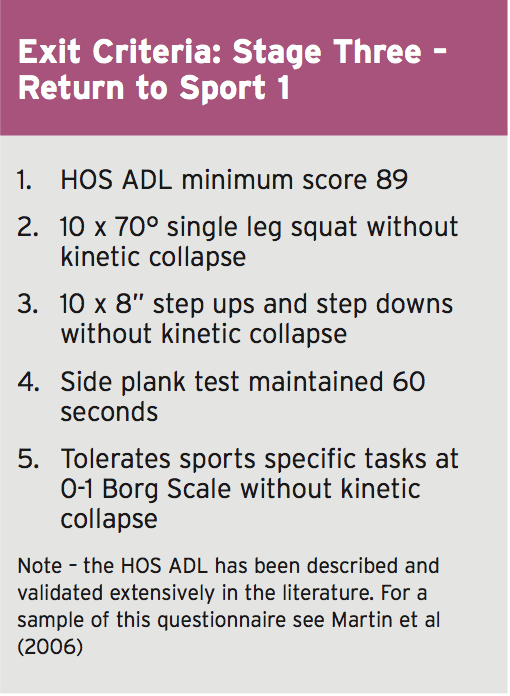
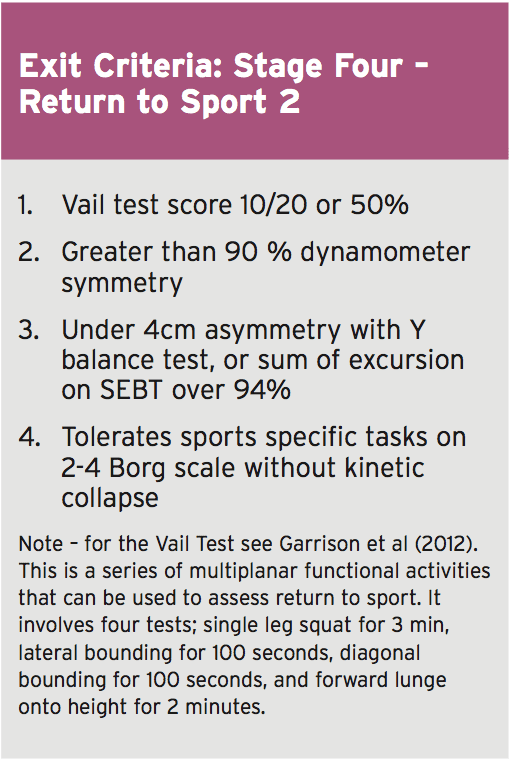
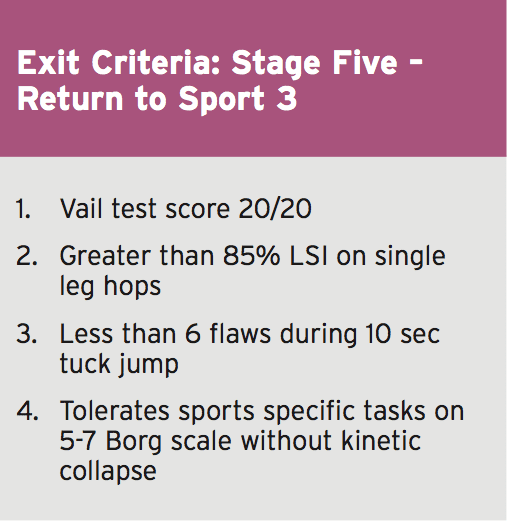
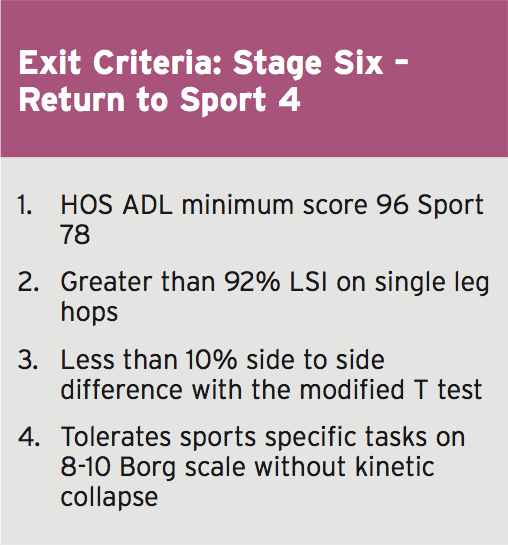
Wahoff et al (2014) have provided some standards which may be utilized to guide the transition from one point to the next(1). They describe their rationale and supply a complete description of all of the cited tests in their printed clinical comment. Essentially, the exit criteria they offer in each phase are as follows;
So as to advance through the six clarified stages, the athlete may undergo extensive physiotherapy, focusing on hip range of movement exercises, manual therapy and trigger point releases, active stretching, potentially deloaded activities like hydrotherapy or Alta G walking/ running and strong hip rotator and gluteal strengthening exercises. Much of this will be ‘controlled’ and led by the wishes of the surgeon as they will provide the framework on if and what happens concerning loading.
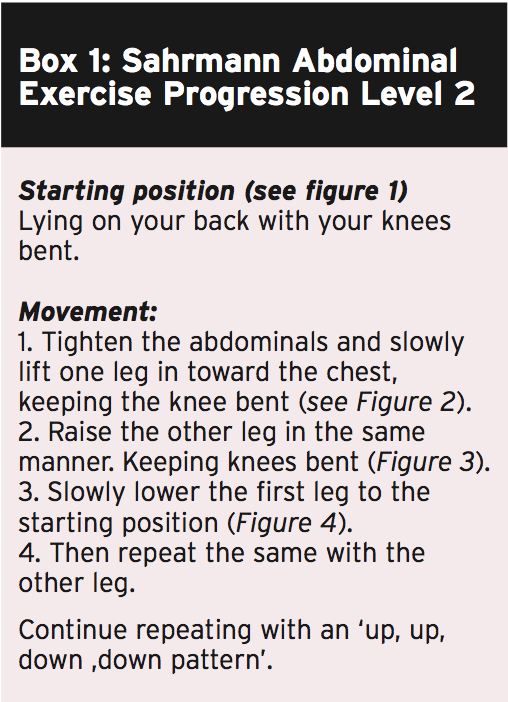
But more direct physiotherapy Interventions have been devised to direct the physiotherapist through the rehabilitation protocol. The Takla-O�Donnell Protocol (TOP) is a validated physiotherapy intervention program which may be utilized to induce the arthroscopically handled FAI patient (Bennel et al)(2).)�This protocol is shown in box 2.
Hip Muscle Control
The focus of the rest of this article Will be to summarize some common yet powerful hip strengthening exercises which may be used to progress the hip muscle control throughout the rehabilitation phases.
Regaining hip muscle power, particularly in the heavy hip external rotator group, is imperative from the FAI recovering athlete. Good muscle endurance and strength in those muscle groups will ensure adequate hip joint compression happens with motion to reduce any shearing effect between the head of femur and acetabulum(3). The muscle groups needing focus are (see figure 5):
Posterior fibres Gluteus Medius (PGMed)
Gluteus minimus
Superior and Inferior Gemellus
Internal and External Obturator
Quadratus Femoris
Piriformis
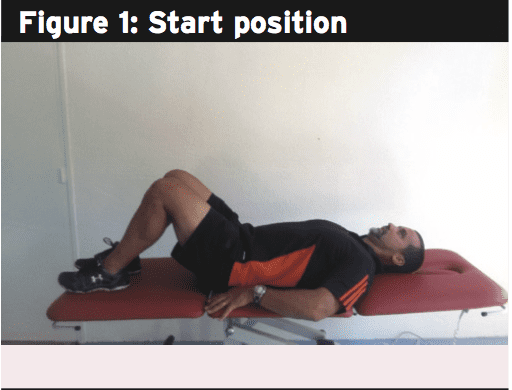
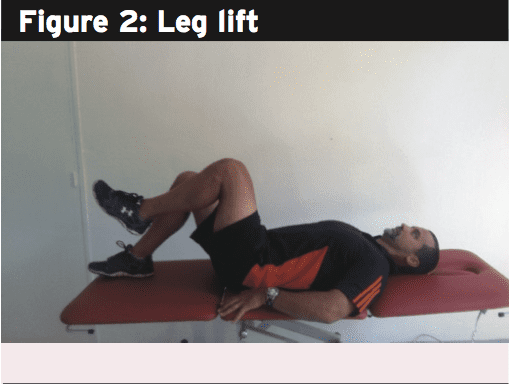
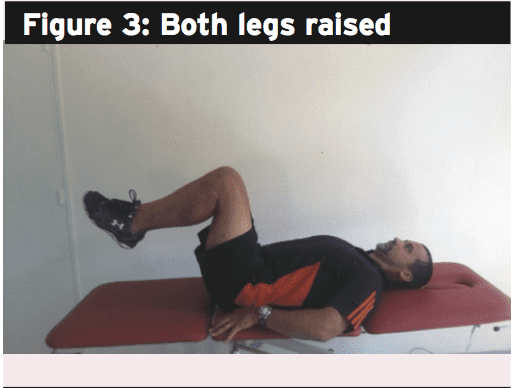
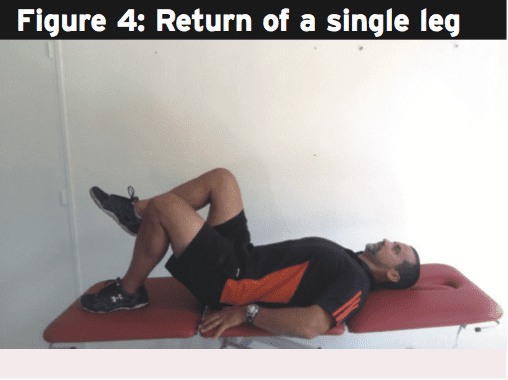
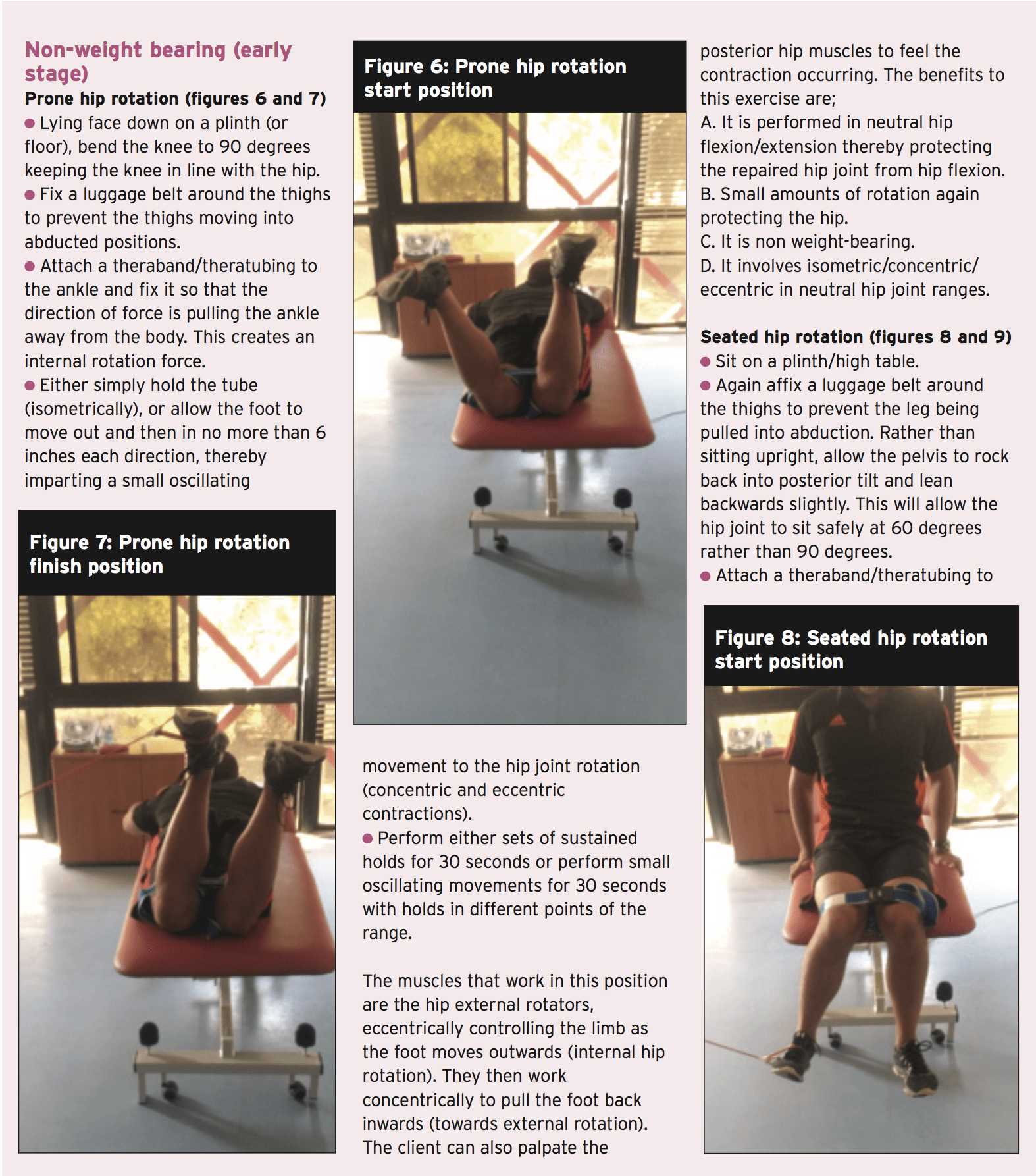
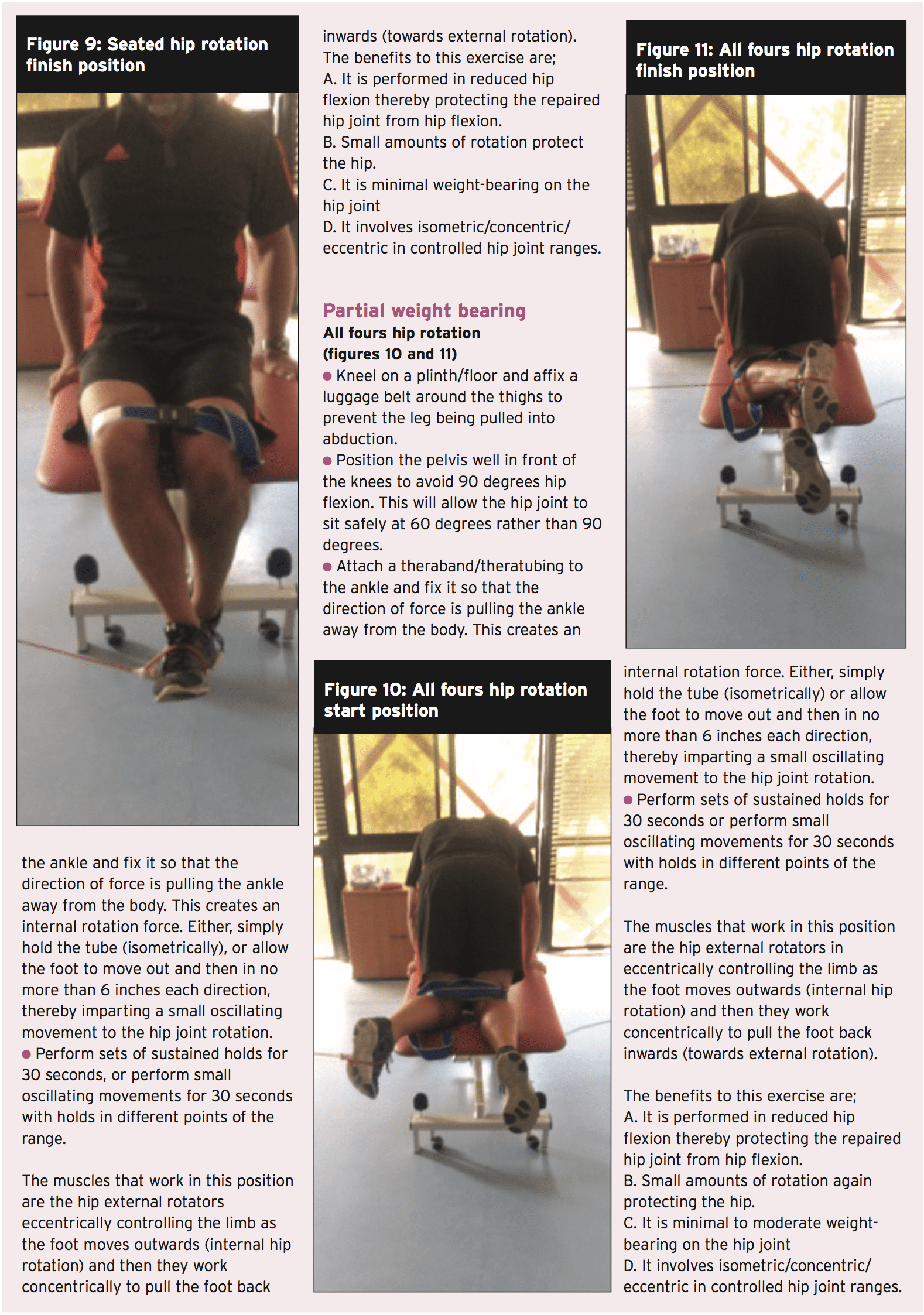
There’s plenty of exercises that can be utilized to fortify the hip joint musculature. The chosen ones below are a sample of some effective exercises that can be used throughout the rehabilitation phases. However, the key requirements of the contained exercises include:
1. Performed in neutral stylish places to no more than 60 degrees hip flexion. This range of movement protects the hip joint from any possibly damaging impingement.
2. Minimal rotation of the hip, letting them be used in most stages of the rehabilitation process.
3. Performed isometrically or utilizing little oscillating concentric/eccentric contractions — to contract and hold to maintain the hip joint compacted and stable. This represents how these muscles work in individual function.
Summary
In many ways. hip joint labral tears, capsule sprains, cartilage and muscle accidents and bony architectural issues like FAI can all lead to debilitating hip pain. FAI is a real concern for the athlete as the existence of a bone abnormality may lead to a painful hip impingement, damage to the acetabular labrum and premature onset degeneration. FAI’s don’t respond to conservative management. If the athlete suffers debilitating pain that affects competition then the options are either to cease competition all together or have the FAI surgically corrected. Once corrected by the surgeon, regaining complete motion and muscle strength and ultimate game related functional skills will require some time. Hip rotator muscle strengthening must shape the foundation of all handling post-surgical FAI issues.
References
1. International Journal of Sports Physical Therapy. 9(6); pp 813-826
2. Arthroscopy. 2006;22(12):1304-1311
3. Int J Sports Phys Ther. 2012;7(1):20-30.
A natural compound found in strawberries called fisetin reduces the mental effects of aging, says a study published in the Journals of Gerontology Series A. Researchers found it could help treat age-related mental decline and conditions like Alzheimer’s or stroke.
“Companies have put fisetin into various health products but there hasn’t been enough serious testing of the compound,” says Pamela Maher, a senior staff scientist in Salk’s Cellular Neurobiology Laboratory and senior author of the paper.
“Based on our ongoing work, we think fisetin might be helpful as a preventive for many age-associated neurodegenerative diseases, not just Alzheimer’s,” she said.
Maher has been studying fisetin, which is a type of flavonol that has powerful antioxidant properties, for more than a decade. Previous research found that it reduced memory loss related to Alzheimer’s disease (AD) in mice genetically modified to develop the disease.
When the scientists studied mice with Alzheimer’s, they found that the pathways involved in cellular inflammation were turned on. However, when the mice were given fisetin, they began producing anti-inflammatory molecules, and both memory loss and learning impairments were prevented. That particular research focused on genetic AD, which accounts for only 1 to 3 percent of cases.
For the recent study, Maher used a strain of laboratory mice that age prematurely and show signs of the disease at about 10 months in comparison to signs of physical and mental decline not seen in normal mice until two years of age.
The researchers fed the 3-month-old prematurely aging mice a daily dose of fisetin with their food for 7 months. Another group of the prematurely aging mice was fed the same food without fisetin.
During the study period, mice took various activity and memory tests. The team also examined levels of specific proteins related to brain function, as well as stress and inflammation.
“At 10 months, the differences between these two groups were striking,” says Maher, who hopes to conduct human trials. Mice not treated with fisetin had difficulties with all the cognitive tests as well as elevated markers of stress and inflammation. Brain cells called astrocytes and microglia, which are normally anti-inflammatory, were now driving rampant inflammation.
On the other hand, mice treated with fisetin were not noticeably different in behavior, cognitive ability or inflammatory markers at 10 months than a group of untreated 3-month-old mice with the same condition. In addition, fisetin was found to be safe even at high doses.
Strawberries have also been found to fight esophageal cancer. Chinese researchers gave volunteers freeze-dried strawberries each day for six months. A comparison of before-and-after biopsies showed that precancerous lesions in participants were decreased by 80 percent.
While too much fat, especially of the “bad” variety, can lead to weight gain and health problems, a moderate amount of fat is essential to a healthy lifestyle.
Adding a little fat to your food, either through cooking or drizzling over salads, can help to fill you up and feel more satisfied after a meal, as well as boost health by helping the body absorb several fat-soluble vitamins.
However, with the recent news that coconut oil, long believed to be a “healthy” fat, should actually be avoided, many of us may be wondering once again which fats are the good ones.
Here we round up some advice from the University of Kentucky on which oils to keep on hand in the kitchen, and which to avoid.
Canola oil
This oil is the lowest in saturated fat, just 7 percent, while also containing high levels of monounsaturated fatty acids, which lower LDL and in recent years have been studied for potentially helping control blood glucose.
This oil is great for stir-frying, grilling, and replacing many solid fats — the ones to avoid — in recipes.
Olive oil
An important ingredient in the popular and healthy Mediterranean diet, olive oil is well-known for its many health benefits, including lower risk of death from cardiovascular disease and a reduced level of inflammation in the body.
Use extra-virgin and virgin olive oils for uncooked dishes, like salads, and choose refined olive oils for cooking as they are better at higher temperatures.
Peanut oil
High in monounsaturated (good) fat, peanut oil also contains vitamin E, an antioxidant that helps maintain a strong immune system, healthy skin and eyes, and helps with the formation of red blood cells.
Thanks to a high smoke point, this oil is ideal for frying, roasting and grilling.
Avocado oil
This oil is also high in monounsaturated fats and vitamin E, and also has a tasty but mild flavor, making it great to add cold onto salads.
It also has a high smoke point for those who prefer to cook with it. However, if avocado oil is too expensive or difficult to find, canola oil makes a good budget-friendly alternative.
And the oils to avoid
Saturated or “solid fats” should be consumed sparingly — these are the oils that are solid at room temperature such as coconut oil, butter, palm oil, beef tallow, and lard.
Because saturated fat contributes to a rise in the level of LDL cholesterol, also known as “bad” cholesterol, the AHA recommends that saturated fat should make up a maximum of 10 percent of total caloric intake for healthy Americans, and a maximum of 6 percent for those who need to lower cholesterol levels.
Coffee addicts and aficionados often say drinking the bitter liquid makes life worth living, but the habit may also help them live longer, according to two major international studies Monday.
Experts cautioned, however, that the US and European reports, published in the Annals of Internal Medicine, failed to show that coffee was truly the reason that many drinkers appeared to have longer lives.
Rather, the studies were observational in nature, meaning they showed an association between coffee-drinking and a propensity toward longevity, but stopped short of proving cause and effect.
The first study, led by the International Agency for Research on Cancer (IARC) and Imperial College London, examined more than half a million people across 10 countries in Europe.
Those who drank about three cups a day tended to live longer than non-coffee drinkers, said the study, which researchers described as the largest analysis of the effects of coffee-drinking in a European population.
“We found that higher coffee consumption was associated with a lower risk of death from any cause, and specifically for circulatory diseases, and digestive diseases,” said lead author Marc Gunter of the IARC, formerly at Imperial’s School of Public Health.
“Importantly, these results were similar across all of the 10 European countries, with variable coffee drinking habits and customs.”
The second study included more than 180,000 participants of various ethnic backgrounds in the United States.
It found benefits to longevity whether the coffee was caffeinated or decaffeinated.
Coffee drinkers had a lower risk of death due to heart disease, cancer, stroke, diabetes, and respiratory and kidney disease.
Those who drank one cup a day were 12 percent less likely to die compared to those who didn’t drink coffee.
Those who drank two or three cups per day saw an even higher 18 percent reduced risk of death.
“We cannot say drinking coffee will prolong your life, but we see an association,” said lead author Veronica Setiawan, an associate professor of preventive medicine at the Keck School of Medicine of University of Southern California.
“If you like to drink coffee, drink up! If you’re not a coffee drinker, then you need to consider if you should start.”
Coffee is one of the most popular drinks in the world. Some 2.25 billion cups are consumed every day.
Many prior studies have hailed the benefits of coffee-drinking, saying the beverage imparts anti-oxidants, may improve liver function and reduce inflammation.
But coffee may carry risks for some people, and pregnant woman and children are urged to avoid caffeine, which can be fatal in high doses.
A report from the IARC last year that said drinking very hot beverages — coffee, tea or otherwise — is one probable cause of cancer of the esophagus, the tube that runs from the throat to the stomach.
Experts who were not involved in the latest studies urged caution in interpreting the results.
For instance, the European study excluded people who had cancer, heart disease or diabetes, meaning it took a measure of people over 35 who were already generally healthy.
It also asked about coffee consumption just once, at the beginning, and did not update this figure over the span of the study, which included an average follow-up time of 16 years.
Finally, it found signs of a link between women who drank large amounts of coffee and a higher risk of cancer death, but downplayed this finding, saying it “may be spurious.”
The “conclusions will not lead me to start drinking coffee or to recommend people drink more coffee as a way to lessen their risks for heart disease,” said Naveed Sattar, professor of metabolic medicine at the University of Glasgow.
“I remain unconvinced that the link between coffee and heart disease represents a true cause and effect relationship and that coffee is truly protective, regardless of how large a study suggests this.”
Sattar said that one downside to the research is the fact that many people stop drinking coffee — or drink less of it — when they are ill, a “bias is very hard to fully overcome.”
David Spiegelhalter, a professor at the University of Cambridge, described the research as “huge in size and carefully done,” but nevertheless unable to prove cause and effect.
“If these estimated reductions in all-cause mortality really are causal, then an extra cup of coffee every day would on average extend the life of a man by around three months, and a woman by around a month,” he added.
NORTHBROOK, Ill. ��Allstate Insurance Company and the American Football Coaches Association (AFCA) announced�on Monday�that UTEP quarterback Ryan Metz one of 146 nominees for the 2017 Allstate AFCA Good Work Team, a prestigious off-the-field honor in college football.
�Allstate is immensely honored to partner with the AFCA for the 10th�year to help pay tribute to these players and their off-the-field �good works� that often go unnoticed and unrewarded,� said Thomas Clarkson, president of the west territory for Allstate Insurance Company and a member of the 2017 Allstate AFCA Good Works Team�voting panel. �The individuals nominated to the 2017 Good Works Team�are making a positive impact and uniting communities across the country through service, showing what�s possible when you put all hands in and give back.�
The El Paso native is known for his on-field achievements and has also made an impact off the field. The junior completed 25 hours of community service hours last season, while the signal caller is known for volunteering his time to children in the community. Metz volunteered over 15 hours at children�s camps, where he assisted with football drills and activities for the future gridiron greats.
Metz was also a member of Project MOVE, where he played with children in the community in various activities like kickball, football and soccer. Metz is active in assisting with the football team�s weekly dinner with the Child Crisis Center. Metz, along with his teammates, spend time with the children in the Crisis Center, playing, working on homework and eating dinner together.
The student-athletes nominated for this esteemed award embody the true spirit of teamwork and selflessness, donating their limited free time to helping and serving others. From founding a non-profit that helps orphans secure jobs in the workforce to raising funds and awareness for childhood cancer research, the 2017 Allstate AFCA Good Works Team��nominees may wear different jerseys on the field, but they all exemplify a superior commitment to giving back off of it.
Comprised of 11 players from the NCAA Football Bowl Subdivision and 11 players from the NCAA Football Championship Subdivision, Divisions II, III and the NAIA, the final roster of 22 award recipients will be unveiled in September. From the nominees submitted by sports information directors across the nation on behalf of their schools, a special voting panel consisting of former Allstate AFCA Good Works Team�members and prominent college football media members will select the 2017 Good Works Team.
Two-time national champion, Heisman Trophy winner and 2009 Allstate AFCA Good Works Team�member Tim Tebow will headline the Allstate AFCA Good Works Team�voting panel.
Once the final team members are announced in September, college football fans are encouraged to visit the Allstate AFCA Good Works Team�website on ESPN.com, featuring profiles and images of the players, for the opportunity to vote for the 2017 Allstate AFCA Good Works Team�Captain. Throughout the season, fans can also follow along and join in on the conversation by searching and using #GoodWorksTeam on their social media channels.
In order to meet the criteria, set forth by Allstate and the AFCA, each player must be actively involved with a charitable organization or service group while maintaining a strong academic standing.
Metz has also excelled in the classroom, as he�s a three-time Conference USA Commissioner�s Honor Roll recipient with a 3.34 GPA in Mathematics. Metz completed 64.7 percent of his passes, ranked third in C-USA in 2016, while it�s the program�s second-best single-season performance. His 14 passing scores were the most for a UTEP quarterback since 2010.
Recently, Metz was one of 45 national collegiate quarterbacks, and the first UTEP quarterback, to be invited to the 2017 Manning Passing Academy supervised by the Manning Family (Archie, Cooper, Peyton and Eli). The camp was a four-day event that started on June 22 at Nicholls State University in which over 125 prep, college and professional coaches, counselors and staff members were involved.
Fractures of the process of the lower spine or upper thoracic spine are often referred to as clay-shoveler’s fractures.
Initially reported in 1940, these fractures were described among employees in Australia who dug drains in clay soil and also threw the clay overhead with shovels. The mud wouldn’t discharge from the spade, causing excess power to be transmitted into the supraspinous ligaments and leading to an avulsion fracture of one or more spinous processes.
The following frequently describes the mechanism of injury for clay shoveler’s fractures. The contraction of the paraspinal and trapezius muscles on the ligaments along with the attachment to the spinous processes make this a common injury during athletics with a flexed position of the shoulders and neck. The consequent fracture or apophyseal avulsion is painful and frequently requires a visit to the doctor, together with plain films, computed tomography (CT) scans, or magnetic resonance imaging (MRI) confirming the identification.
Often a period of rest will allow a return to activity, although treatment of these fractures hasn’t been clarified. We present a collection of adolescent athletes who underwent surgical interventions to treat the fracture of the spinous process, after rest and physical therapy with persistent symptoms.
Surgical Intervention Study
Dr. Hedequist operated on 3 patients using a spinous process nonunion within the study time period. The patients’ average age was 14 years; the location of the spinous process fracture was the T1 vertebra in all patients. Two patients sustained the injury while playing hockey and one while wrestling. The average duration of symptoms before surgery was 10 months; all patients had seen physicians without a diagnosis before test in institution. All patients had a trial of physical therapy and all had been unable to return after trauma to pain.
Examination of patients showed pain directly over the fracture site and accentuated by forward flexion of the neck and neck. Evaluation of harm plain films revealed a fracture fragment in two patients (Figure 1). All 3 patients underwent CT and MRI scans confirming the identification. MRI confirmed areas of increased signal at the tip of the T1 spinous process, with inflammation in the supraspinous ligament directly at that area (Figure 2). The CT scans confirmed the presence of a bony fragment correlating with the suggestion of the T1 spinous process (Figure 3).
Figure 1
Figure 2
Figure 3
Surgery was performed under general endotracheal anesthesia using a midline incision over the affected region down to the spinous procedure. The supraspinous ligament was opened showing an identified and ununited ossicle, which has been removed without taking down the ligament. All 3 nonunions have been noted to be atrophic with no evidence of surrounding inflammatory tissue or bursa. The residual end of the spinous process was smoothed down with a rongeur. Standard closure was performed. There were no surgical complications.
All patients had complete relief of pain at followup; 1 individual returned to full sports activity at 6 months and the other 2 returned to full sports activity at 3 months. There was no loss of peripheral movement or trapezial strength at follow-up. All patients expressed satisfaction together with the decision.
Discussion
Clinical practice suggests that most patients with spinous process fractures will become pain-free; however, that is not universal. This series demonstrates that a tiny subset of patients with this trauma will continue to have significant symptoms despite a period of rest. In those patients who want a yield to sports, we recommend consideration of surgical excision after confirmation of nonunion with studies. The inherent risks of surgical treatment are minimal with this procedure, and the advantages include return for athletes, with the physical and psychosocial benefits to pain-free sports activity.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Automobile Accident Injuries
Whiplash, among other automobile accident injuries, are frequently reported by victims of an auto collision, regardless of the severity and grade of the accident. The sheer force of an impact can cause damage or injury to the cervical spine, as well as to the rest of the spine. Whiplash is generally the result of an abrupt, back-and-forth jolt of the head and neck in any direction. Fortunately, a variety of treatments are available to treat automobile accident injuries.
Fractures of the cervical spinous processes are considered to be rare injuries. Isolated spinous process fractures are even rarer instances, some of which are rare injuries in rare case reports. Approximately xixteen percent of isolated process fractures of the cervical spine involve more than one level. Isolated cervical spinous process fractures are in fact, commonly referred to as clay-shoveler’s fractures.
The term “fracture” can be employed in medical scenarios that deal with a broken bone. This can vary from acute breaks to small fractures, or anything which will impact the integrity and stability of the bone.
Bone fractures could result from numerous distinct situations. Women in particular that suffer from osteoporosis or other conditions, or older people, may lose strength in their bones, making them more fragile and vulnerable to breaks and cracks, even with minimal impact. As the bones have not fully grown, young children are also vulnerable to bone fractures, particularly because they frequently participate in activities that heighten the risk of injury.
However, falls, automobile accidents, and also a number of other dangers can lead to bone fractures, and depending on the severity, these may often require a range of short and long-term treatment options.
What is a Clay Shoveler’s Fracture?
A clay shoveler’s fracture is an avulsion fracture of the spinous process. It happens with flexion of the head, like that reported with automobile accidents, diving, or even wrestling injuries. It also occurs with repeated stress caused by the pulling of the trapezius and rhomboid muscles on the cervical and thoracic spinous processes. Repetitive and forceful muscle contraction breaks the spinous process and pulls the avulsion segment away from the original spinous process.
A clay shovelers fracture commonly occurs from the cervical and upper thoracic spinous processes C6, C7, and T1. The avulsion and fractures are caused by damage or injury from direct blows to the base of the neck. This is usually a stable fracture and doesn’t create any additional deficits.
X-ray examination of the spine can help diagnose a clay-shoveler’s fracture. On the lateral side (side view) x-rays, an oblique radiolucent fracture line could be seen through the base of the spinous process. It’s more likely to maintain the trunk or distal tip of the lower cervical and upper thoracic spinous process. Serrated edges or rough margins are generally seen with the fractures, which distinguishes it from nonunion of this secondary growth centre of the process. Additionally, bones from the head and neck would not be displaced or have the serrated margins. The distal portion of the fractured spinous process is often displaced downward (caudally or poor). This is due to the pull on the avulsion segment of bone.
Chiropractic Care for Clay Shoveler’s Fractures
Chiropractors can help alleviate some of the long-term and immediate concerns associated with bone fractures, such as clay shoveler’s fractures. A chiropractor may not perform treatment procedures to the fracture until the damage or injury has started to heal and inflammation is reduced. A chiropractor can help with compression techniques which are beneficial in maintaining the bone in place for healing. A chiropractor may also advocate wellness techniques, such as appropriate diet, and this will optimize the body’s ability to restore its original health and wellness. Chiropractors may also educate a patient on a variety of exercises and stretches to reduce the likelihood of complications and which, if done properly and at fixed intervals, will promote quicker recovery.
The advantages of seeing a chiropractor for wellness and health are many and well documented, but chiropractors are particularly effective as first line and treatment practitioners for bone fractures of any sort. When many kinds of fractures and acute breaks may require immediate therapy, a chiropractor can help rebuild strength and ensure proper recovery, which makes the chiropractic procedure an excellent cure and ensuring long-term good health.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Automobile Accident Injuries
Whiplash, among other automobile accident injuries, are frequently reported by victims of an auto collision, regardless of the severity and grade of the accident. The sheer force of an impact can cause damage or injury to the cervical spine, as well as to the rest of the spine. Whiplash is generally the result of an abrupt, back-and-forth jolt of the head and neck in any direction. Fortunately, a variety of treatments are available to treat automobile accident injuries.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine






 So as to advance through the six clarified stages, the athlete may undergo extensive physiotherapy, focusing on hip range of movement exercises, manual therapy and trigger point releases, active stretching, potentially deloaded activities like hydrotherapy or Alta G walking/ running and strong hip rotator and gluteal strengthening exercises. Much of this will be ‘controlled’ and led by the wishes of the surgeon as they will provide the framework on if and what happens concerning loading.
So as to advance through the six clarified stages, the athlete may undergo extensive physiotherapy, focusing on hip range of movement exercises, manual therapy and trigger point releases, active stretching, potentially deloaded activities like hydrotherapy or Alta G walking/ running and strong hip rotator and gluteal strengthening exercises. Much of this will be ‘controlled’ and led by the wishes of the surgeon as they will provide the framework on if and what happens concerning loading.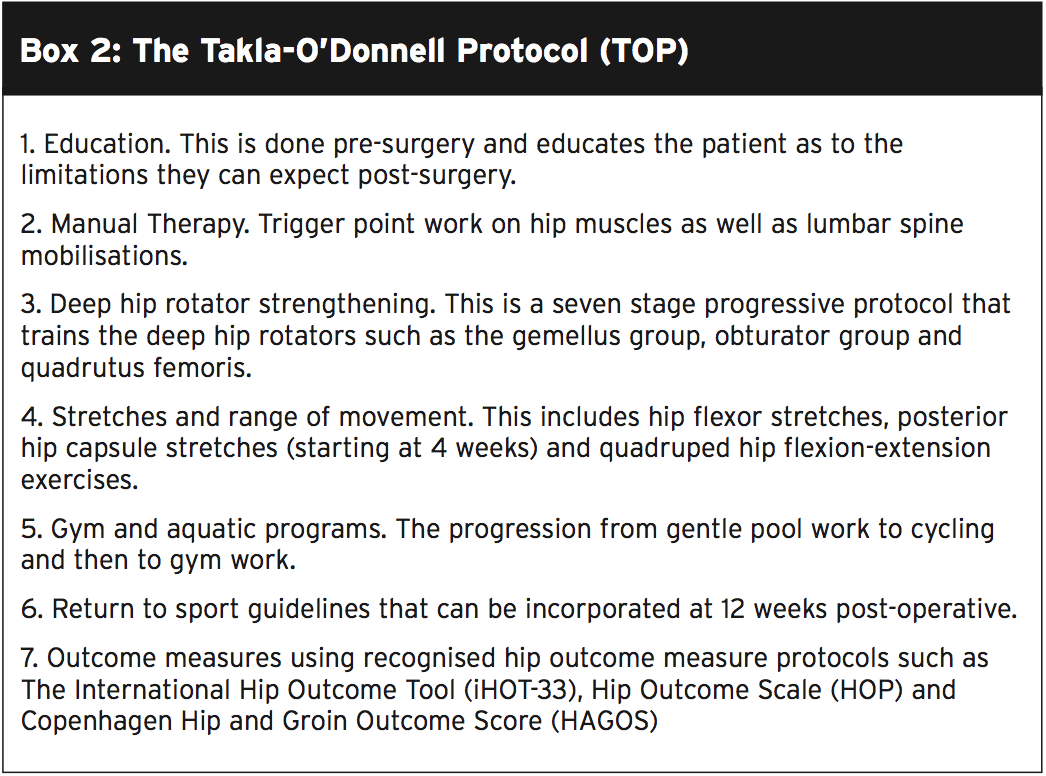 Hip Muscle Control
Hip Muscle Control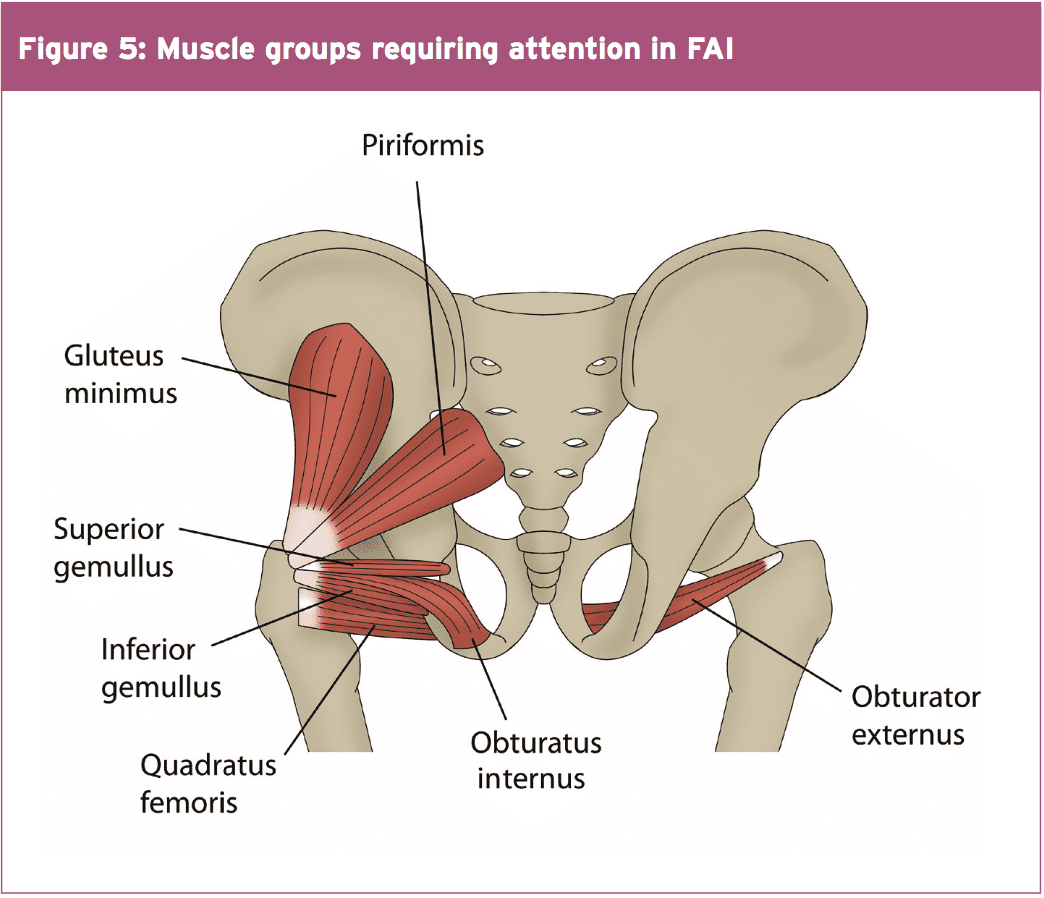
 Summary
Summary