Abstract Objective: This article presents an overview of metabolic syndrome (MetS), which is a collection of risk factors that can lead to diabetes, stroke, and heart disease. The purposes of this article are to describe the current literature on the etiology and pathophysiology of insulin resistance as it relates to MetS and to suggest strategies for dietary and supplemental management in chiropractic practice.
Methods: The literature was searched in PubMed, Google Scholar, and the Web site of the American Heart Association, from the earliest date possible to May 2014. Review articles were identified that outlined pathophysiology of MetS and type 2 diabetes mellitus (T2DM) and relationships among diet, supplements, and glycemic regulation, MetS, T2DM, and musculoskeletal pain.
Results: Metabolic syndrome has been linked to increased risk of developing T2DM and cardiovascular disease and increased risk of stroke and myocardial infarction. Insulin resistance is linked to musculoskeletal complaints both through chronic inflammation and the effects of advanced glycosylation end products. Although diabetes and cardiovascular disease are the most well-known diseases that can result from MetS, an emerging body of evidence demonstrates that common musculoskeletal pain syndromes can be caused by MetS.
Conclusions: This article provides an overview of lifestyle management of MetS that can be undertaken by doctors of chiropractic by means of dietary modification and nutritional support to promote blood sugar regulation.
Introduction: Metabolic Syndrome
Metabolic syndrome (MetS) has been described as a cluster of physical examination and laboratory findings�that directly increases the risk of degenerative metabolic disease expression. Excess visceral adipose tissue, insulin resistance, dyslipidemia, and hypertension are conditions that significantly contribute to the syndrome. These conditions are united by a pathophysiological basis in low-grade chronic inflammation and increase an individual’s risk of cardiovascular disease, type 2 diabetes mellitus (T2DM), and all-cause mortality.1
The National Health and Nutrition Examination Survey (NHANES) 2003-2006 estimated that approximately 34% of United States adults aged 20 years and more had MetS.2 The same NHANES data found that 53% had abdominal adiposity, a condition that is closely linked to visceral adipose stores. Excess visceral adiposity generates increased systemic levels of pro-inflammatory mediator molecules. Chronic, low- grade inflammation has been well documented as an associated and potentially inciting factor for the development of insulin resistance and T2DM.1
NHANES 2003-2006 data showed that 39% of subjects met criteria for insulin resistance. Insulin resistance is a component of MetS that significantly contributes to the expression of chronic, low-grade inflammation and predicts T2DM expression. T2DM costs the United States in excess of $174 billion in 2007. 3 It is estimated that 1 in 4 adults will have T2DM by the year 2050.3 Currently, more than one third of US adults (34.9%) are obese, 4 and, in 2008, the annual medical cost of obesity was $147 billion.4,5 This clearly represents a health care concern.
The pervasiveness of MetS dictates that doctors of chiropractic will see a growing proportion of patients who fit the syndrome criteria.6 Chiropractic is most commonly used for musculoskeletal complaints believed to be mechanical in nature;6 however, an emerging body of evidence identifies MetS as a biochemical promoter of musculoskeletal complaints such as neck pain, shoulder pain, patella tendinopathy, and widespread musculoskeletal pain. 7�13 As an example, the cross-linking of collagen fibers can be caused by increased advanced glycation end-product (AGE) formation as seen in insulin resistance.14 Increased collagen cross-linking is observed in both osteoarthritis and degenerative disc disease, 15 and reduced mobility in elderly patients with T2DM has also been attributed to AGE-induced collagen cross-linking. 16,17
A diagnosis of MetS is made from a patient having 3 of the 5 findings presented in Table 1. Fasting hyperglycemia is termed impaired fasting glucose and indicates insulin resistance. 18,19 An elevated hemoglobin A1c (HbA1c) level measures long-term blood glucose�regulation and is diagnostic for T2DM when elevated in the presence of impaired fasting glucose. 3,18
The emerging evidence demonstrates that we cannot view musculoskeletal pain as only coming from conditions that are purely mechanical in nature. Doctors of chiropractic must demonstrate prowess in identification and management of MetS and an understanding of insulin resistance as its main pathophysiological feature. The purposes of this article are to describe the current literature on the etiology and pathophysiology of insulin resistance as it relates to MetS and to suggest strategies for dietary and supplemental management in chiropractic practice.
Methods
PubMed was searched from the earliest possible date to May 2014 to identify review articles that outlined the pathophysiology of MetS and T2DM. This led to further search refinements to identify inflammatory mechanisms that occur in the pancreas, adipose tissue, skeletal muscle, and hypothalamus. Searches were also refined to identify relationships among diet, supplements, and glycemic regulation. Both animal and human studies were reviewed. The selection of specific supplements was based on those that were most commonly used in the clinical setting, namely, gymnema sylvestre, vanadium, chromium and ?-lipoic acid.
Discussion
Insulin Resistance Overview
Under normal conditions, skeletal muscle, hepatic, and adipose tissues require the action of insulin for cellular glucose entry. Insulin resistance represents an inability of insulin to signal glucose passage into insulin-dependent cells. Although a genetic predisposition can exist, the�etiology of insulin resistance has been linked to chronic low-grade inflammation.1 Combined with insulin resistance-induced hyperglycemia, chronic low-grade inflammation also sustains MetS pathophysiology.1
Two thirds of postprandial blood glucose metabolism occurs within skeletal muscle via an insulin-dependent mechanism.18,19 Insulin binding to its receptor triggers glucose entry and subsequently inhibits lipolysis within the target tissue.21,22 Glucose enters skeletal muscles cells by way of a glucose transporter designated Glut4. 18 Owing to genetic variability, insulin-mediated glucose uptake can vary more than 6-fold among non-diabetic individuals. 23
Prolonged insulin resistance leads to structural changes within skeletal muscle such as decreased Glut4 transporter number, intramyocellular fat accu- mulation, and a reduction in mitochondrial con- tent.19,24 These events are thought to impact energy generation and functioning of affected skeletal mus- cle.24 Insulin-resistant skeletal muscle is less able to suppress lipolysis in response to insulin binding.25 Subsequently, saturated free fatty acids accumulate and generate oxidative stress. 22 The same phenomenon within adipose tissue generates a rapid adipose cell expansion and tissue hypoxia.26 Both these processes increase inflammatory pathway activation and the generation of proinflammatory cytokines (PICs).27
Multiple inflammatory mediators are associated with the promotion of skeletal muscle insulin resistance. The PICs tumor necrosis factor ? (TNF-?), interleukin 1 (IL- 1), and IL-6 have received much attention because of their direct inhibition of insulin signaling.28�30 Since cytokine testing is not performed clinically, elevated levels of high- sensitivity C-reactive protein (hsCRP) best represent the low-grade systemic inflammation that characterizes insulin resistance.31,32
Insulin resistance�induced hyperglycemia can lead to irreversible changes in protein structure, termed glycation, and the formation of AGEs. Cells such as those of the vascular endothelium are most vulnerable to hyperglycemia due to utilization of an insulin-independent Glut1 transporter. 33 This makes AGE generation responsible for most diabetic complications, 15,33,34 including collagen cross-linking.15
If unchanged, prolonged insulin resistance can lead to T2DM expression. The relationship between chronic low-grade inflammation and T2DM has been well characterized. 35 Research has demonstrated that patients with T2DM also have chronic inflammation within the pancreas, termed insulitis, and it worsens hyperglycemia due to the progressive loss of insulin- producing ? cells.36�39
Visceral Adiposity And Insulin Resistance
Caloric excess and a sedentary lifestyle contribute to the accumulation of subcutaneous and visceral adipose tissue. Adipose tissue was once thought of as a metabolically inert passive energy depot. A large body of evidence now demonstrates that excess visceral adipose tissue acts as a driver of chronic low-grade inflammation and insulin resistance.27,34
It has been documented that immune cells infiltrate rapidly expanding visceral adipose tissue. 26,40 Infil- trated macrophages become activated and release PICs that ultimately cause a phenotypic shift in resident macrophage phenotype to a classic inflammatory M1 profile.27 This vicious cycle creates a chronic inflam- matory response within adipose tissue and decreases the production of adipose-derived anti-inflammatory cytokines.43 As an example, adiponectin is an adipose- derived anti-inflammatory cytokine. Macrophage- invaded adipose tissue produces less adiponectin, and this has been correlated with increasing insulin resistance. 26
Hypothalamic Inflammation And Insulin Resistance
Eating behavior in the obese and overweight has been popularly attributed to a lack of will power or genetics. However, recent research has demonstrated a link between hypothalamic inflammation and increased body weight.41,41
Centers that govern energy balance and glucose homeostasis are located within the hypothalamus. Recent studies demonstrate that inflammation in the hypothalamus coincides with metabolic inflammation and an increase in appetite.43 These hypothalamic centers simultaneously become resistant to anorexigenic stimuli, leading to altered energy intake. It has been suggested that this provides a neuropathological basis for MetS and drives a progressive increase in body weight. 41
Central metabolic inflammation pathologically activates hypothalamic immune cells and disrupts central insulin and leptin signaling.41 Peripherally, this has been associated with dysregulated glucose homeostasis that also impairs pancreatic ? cell functioning.41,44 Hypothalamic inflammation contributes to hypertension through similar mechanisms, and it is thought that central inflammation parallels chronic low-grade systemic inflammation and insulin resistance.41�44
Feeding generally leads to a short-term increase in both oxidative stress and inflammation. 41 Total�calories consumed, glycemic index, and fatty acid profile of a meal all influence the degree of postprandial inflammation. It is estimated that the average American consumes approximately 20% of calories from refined sugar, 20% from refined grains and flour, 15% to 20% from excessively fatty meat products, and 20% from refined seed/legume oils.45 This pattern of eating contains a macronutrient composition and glycemic index that promote hyperglycemia, hyperlipemia, and an acute postprandial inflammatory response. 46 Collectively referred to as postprandial dysmetabolism, this pro-inflammatory response can sustain levels of chronic low-grade inflammation that leads to excess body fat, coronary heart disease (CHD), insulin resistance, and T2DM.28,29,47
Recent evidence suggests that several MetS criteria may not sufficiently identify all individuals with postprandial dysmetabolism. 48,49 A 2-hour oral glucose tolerance test (2-h OGTT) result greater than 200 mg/dL can be used clinically to diagnose T2DM. Although MetS includes a fasting blood glucose level less than 100 mg/dL, population studies have shown that a fasting glucose as low as 90 mg/dL can be associated with an 2-h OGTT level greater than 200 mg/dL.49 Further, a recent large cohort study indicated that an increased 2-h OGTT was independently predictive of cardiovascular and all-cause mortality in a nondiabetic population. 48 Mounting evidence indicates that post- prandial glucose levels are better correlated with MetS and predicting future cardiovascular events than fasting blood glucose alone.41,48
Fasting triglyceride levels generally correlate with postprandial levels, and a fasting triglyceride level greater than 150 mg/dL reflects MetS and insulin resistance. Contrastingly, epidemiologic data indicate that a fasting triglyceride level greater than 100 mg/dL influences CHD risk via postprandial dysmetabolism. 48 The acute postprandial inflammatory response that contributes to CHD risk includes an increase in PICs, free radicals, and hsCRP.48,49 These levels are not measured clinically but, monitoring fasting glucose, 2-hour postprandial glucose and fasting triglycerides can be used as correlates of postprandial dysmetabolic and low-grade systemic inflammation.
MetS And Disease Expression
Diagnosis of MetS has been linked to an increased risk of developing T2DM and cardiovascular disease over the following 5 to 10 years. 1 It further increases a patient’s risk of stroke, myocardial infarction, and death from any of the aforementioned conditions.1
Facchini et al47 followed 208 apparently healthy, non-obese subjects for 4 to 11 years while monitoring the incidence of clinical events such as hypertension, stroke, CHD, cancer, and T2DM. Approximately one fifth of participants experienced clinical events, and all of these subjects were either classified as intermediately or severely insulin resistant. It is important to note that all of these clinical events have a pathological basis in chronic low-grade inflammation,50 and no events were experienced in the insulin-sensitive groupings. 47
Insulin resistance is linked to musculoskeletal com- plaints both through chronic inflammation and the effects of AGEs. Advanced glycation end-products have been shown to extensively accumulate in osteoarthritic cartilage and treatment of human chondrocytes with AGEs increased their catabolic activity. 51 Advanced glycation end-products increase collagen stiffness via cross-linking and likely contribute to reduced joint mobility seen in elderly patients with T2DM.52 Com- pared to non-diabetics, type II diabetic patients are known to have altered proteoglycan metabolism in their intervertebral discs. This altered metabolism may pro- mote weakening of the annular fibers and subsequently, disc herniation.53 The presence of T2DM increases a person’s risk of expressing disc herniation in both the cervical and lumbar spines.17,54 Patients with T2DM are also more likely to develop lumbar stenosis compared with non-diabetics, and this has been documented as a plausible relationship between MetS risk factors and physician-diagnosed lumbar disc herniation. 55�57
There are no specific symptoms that denote early skeletal muscle structural changes. Fatty infiltration and decreased muscle mitochondria content are observed within age-related sarcopenia 58 ; however, it is still being argued whether fatty infiltration is a risk factor for low back pain. 59,60
Clinical management of MetS should be geared toward improving insulin sensitivity and reducing chronic low-grade inflammation. 1 Regular exercise without weight loss is associated with reduced insulin resistance, and at least 30 minutes of aerobic activity and resistance training is recommended daily. 61,62 Although frequently considered preventative, exercise, dietary, and weight loss interventions should be considered alongside pharmacological management in those with MetS. 1
Data regarding the exact amount of weight loss needed to improve chronic inflammation are inconclusive. In overweight individuals without diagnosed MetS, a very-low-carbohydrate diet (b 10% calories from carbohydrate) has significantly reduced plasma inflammatory markers (TNF-?, hsCRP, and IL-6) with�as little as 6% reduction in body weight.63,64 Individuals who meet MetS criteria may require 10% to 20% body weight loss to reduce inflammatory markers. 65 Interestingly, the Mediterranean Diet has been shown to reduce markers of systemic inflammation independent of weight loss65 and was recommended in the American College of Cardiology and American Heart Association Adult Treatment Panel 4 guidelines.66
A growing body of research has examined the effects of the Spanish ketogenic Mediterranean diet, including olive oil, green vegetables and salads, fish as the primary protein, and moderate red wine consumption. In a sample of 22 patients, adoption of the Spanish ketogenic Mediterranean diet with 9 g of supplemental salmon oil on days when fish was not consumed has led to complete resolution of MetS.67 Significant reductions in markers of chronic systemic inflammation were seen in 31 patients following this diet for 12 weeks.68
A Paleolithic diet based on lean meat, fish, fruits, vegetables, root vegetables, eggs, and nuts has been described as more satiating per calorie than a diabetes diet in patients with T2DM.69 In a randomized crossover study, a Paleolithic diet resulted in lower mean HbA1c values, triglycerides, diastolic blood pressure, waist circumference, improved glucose tolerance, and higher high-density lipoprotein (HDL) values compared to a diabetes diet.70 Within the context of these changes, a referral for medication management may be advisable.
Irrespective of name, a low-glycemic diet that focuses on vegetables, fruits, lean meats, omega-3 fish, nuts, and tubers can be considered anti-inflammatory and has been shown to ameliorate insulin resistance. 49,71�73 Inflammatory markers and insulin resistance further improve when weight loss coincides with adherence to an anti-inflammatory diet.70 A growing body of evidence suggests that specific supplemental nutrients also reduce insulin resistance and improve chronic low-grade inflammation.
Key Nutrients That Promote Insulin Sensitivity
Research has identified nutrients that play key roles in promoting proper insulin sensitivity, including vitamin D, magnesium, omega-3 (n-3) fatty acids, curcumin, gymnema, vanadium, chromium, and ?-lipoic acid. It is possible to get adequate vitamin D from sun exposure and adequate amounts of magnesium and omega-3 fatty acids from food. Contrastingly, the therapeutic levels of chromium and ?-lipoic acid that affect insulin sensitivity and reduce�insulin resistance cannot be obtained in food and must be supplemented.
Vitamin D, magnesium, and n-3 fatty acids have multiple functions, and generalized inflammation reduction is a common mechanism of action.74�80 Their supplemental use should be considered in the context of low-grade inflammation reduction and health promotion, rather than as a specific treatment for MetS or T2DM.
Evidence pertaining to the precise role of vitamin D in MetS and insulin resistance is inconclusive. Increas- ing dietary and supplemental vitamin D intake in young men and women may lower the risk of MetS and T2DM development,81 and a low serum vitamin D level has been associated with insulin resistance and T2DM expression. 82 Supplementation to improve low serum vitamin D (reference range, 32-100 ng/mL) is effective, but its impact on improving central glycemia and insulin sensitivity is conflicting. 83 Treating insulin resistance and MetS with vitamin D as a monotherapy appears to be unsuccessful. 82,83 Achieving normal vitamin D blood levels through adequate sun exposure and/or supplementation is advised for general health. 84�86
The average American diet commonly contains a low magnesium intake.80 Recent studies suggest that supple- mental magnesium can improve insulin sensitivity. 81,82 Taking 365 mg/d may be effective in reducing fasting glucose and raising HDL cholesterol in T2DM,83 as well as normomagnesemic, overweight, nondiabetics. 84
Diets high in the omega-6 fat linoleic acid have been associated with insulin resistance85 and higher levels of serum pro-inflammatory mediator markers including IL-6, IL-1?, TNF-?, and hsCRP.87 Supplementation to increase dietary omega-3 fatty acids at the expense of omega-6 fatty acids has been shown to improve insulin sensitivity. 88�90 Six months of omega-3 supplementation at 3 g/d with meals has been shown to reduce MetS markers including fasting triglycerides, HDL cholesterol, and an increase in anti-inflammatory adiponectin. 91
Curcumin is responsible for the yellow pigmentation of the spice turmeric. Its biological effects can be characterized as antidiabetic and antiobesity via down- regulating TNF-?, suppressing nuclear factor ?B activation, adipocytokine expression, and leptin level modulation,. 92�95 Curcumin has been reported to activate peroxisome proliferator-activated receptor-?, the nuclear target of the thiazolidinedione class of antidiabetic drugs,93 and it also protects hepatic and pancreatic cells. 92,93 Numerous studies have reported�weight loss, hsCRP reduction, and improved insulin sensitivity after curcumin supplementation.92�95
There is no established upper limit for curcumin, and doses of up to 12 g/d are safe and tolerable in humans. 96 A randomized, double-blinded, placebo- controlled trial (N = 240) showed a reduced progression of prediabetes to T2DM after 9 months of 1500 mg/d curcumin supplementation.97
Curcumin, 98 vitamin D, 84 magnesium, 91 and omega-3 fatty acids80 are advocated as daily supplements to promote general health. A growing body of evidence supports the views of Gymnema sylvestre, vanadium, chromium, and ?-lipoic acid should as therapeutic supplements to assist in glucose homeostasis.
G Sylvestre
Gymnemic acids are the active component of the G sylvestre plant leaves. Gymnemic acids are the active component of the G sylvestre plant leaves. Studies evaluating G sylvestre’s effects on diabetes in humans have generally been of poor methodological quality. Experimental animal studies have found that gymnemic acids may decrease glucose uptake in the small intestine, inhibit gluconeogenesis, and reduce hepatic and skeletal muscle insulin resistance.99 Other animal studies suggest that gymnemic acids may have comparable efficacy in reducing blood sugar levels to the first-generation sulfonylurea, tolbutamide.100
Evidence from open-label trials suggests its use as a supplement to oral antidiabetic hypoglycemic agents. 96 One quarter of patients were able to discontinue their drug and maintain normal glucose levels on an ethanolic gymnema extract alone. Although the evidence to date suggests its use in humans and animals is safe and well tolerated, higher quality human studies are warranted.
Vanadyl Sulfate
Vanadyl sulfate has been reported to prolong the events of insulin signaling and may actually improve insulin sensitivity.101 Limited data suggest that it inhibits gluconeogenesis, possibly ameliorating hepatic insulin resistance. 100,101 Uncontrolled clinical trials have reported improvements in insulin sensitivity using 50 to 300 mg daily for periods ranging from 3 to 6 weeks. 101�103 Contrastingly, a recent randomized, double-blind, placebo-controlled trial found that 50 mg of vanadyl sulfate twice daily for 4 weeks had no effect in individuals with impaired glucose tolerance. 104 Limited clinical and experimental data exist supporting the use of vanadyl sulfate to improve insulin resistance,�and further research is warranted regarding its safety and efficacy.
Chromium
Diets high in refined sugar and flour are deficient in chromium (Cr) and lead to an increased urinary excretion of chromium. 105,106 The progression of MetS is not likely caused by a chromium deficiency, 107 and dosages that benefit glycemic regulation are not achievable through food. 106,108,109
A recent randomize, double-blind trial demonstrated that 1000 ?g Cr per day for 8 months improved insulin sensitivity by 10% in subjects with T2DM.110 Cefalu et al110 further suggested that these improvements might be more applicable to patients with a greater degree of insulin resistance, impaired fasting plasma glucose, and higher HbA1c values. Chromium’s mechanism of action for improving insulin sensitivity is through increased Glut4 translocation via prolonging insulin receptor signaling.109 Chromium has been well tolerated at 1000 ?g/d,105 and animal models using significantly more than 1000 ? Cr per day were not associated with toxicological consequences.109
?-Lipoic Acid
Humans derive ?-lipoic acid through dietary means and from endogenous synthesis. 111 The foods richest in ?-lipoic acid are animal tissues with extensive metabolic activity such as animal heart, liver, and kidney, which are not consumed in large amounts in the typical American diet. 111 Supplemental amounts of ?-lipoic acid used in the treatment of T2DM (300-600 mg) are likely to be as much as 1000 times greater than the amounts that could be obtained from the diet.112
Lipoic acid synthase (LASY) appears to be the key enzyme involved in the generation of endogenous lipoic acid, and obese mice with diabetes have reduced LASY expression when compared with age-and sex- matched controls.111 In vitro studies to identify potential inhibitors of lipoic acid synthesis suggest a role for diet-induced hyperglycemia and the PIC TNF- ? in the down-regulation of LASY.113 The inflammatory basis of insulin resistance may therefore drive lowered levels of endogenous lipoic acid via reducing the activity of LASY.
?-Lipoic acid has been found to act as insulin mimetic via stimulating Glut4-mediated glucose trans- port in muscle cells. 110,114?-Lipoic acid is a lipophilic free radical scavenger and may affect glucose homeostasis through protecting the insulin receptor from damage114 and indirectly via decreasing nuclear factor ?B�mediated TNF-? and IL-1 production. 110 In�postmenopausal women with MetS (presence of at least 3 ATPIII clinical criteria) 4 g/d of a combined inositol and ?-lipoic acid supplement for 6 months significantly improved OGTT scores by 20% in two thirds of the subjects. 114 A recent randomized double-blinded placebo-controlled study showed that 300 mg/d ?- lipoic acid for 90 days significantly decreased HbA1c values in subjects with T2DM.115
Side effects to ?-lipoic acid supplementation as high as 1800 mg/d have largely been limited to nausea. 116 It may be best to take supplemental ?-lipoic acid on an empty stomach (1 hour before or 2 hours after eating) because food intake reportedly reduces its bioavailability.117 Clinicians should be aware that ?-lipoic acid supplementation might increase the risk of hypoglycemia in diabetic patients using insulin or oral antidiabetic agents.117
Limitations
This is a narrative overview of the topic of MetS. A systematic review was not performed; therefore, there may be relevant information missing from this review. The contents of this overview focuses on the opinions of the authors, and therefore, others may disagree with our opinions or approaches to management. This overview is limited by the studies that have been published. To date, no studies have been published that identify the effectiveness of a combination of a dietary intervention, such as the Spanish ketogenic diet, and nutritional supplementation on the expression of the MetS. Similarly, this approach has not been studied in patients with musculoskeletal pain who also have the MetS. Consequently, the information presented in this article is speculative. Longitudinal studies are needed before any specific recommendations can be made for patients with musculoskeletal that may be influenced by the MetS.
Conclusion: Metabolic Syndrome
This overview suggests that MetS and type 2 diabetes are complex conditions, and their prevalence is expected to increase substantially in the coming years. Thus, it is important to identify if the MetS may be present in patients who are nonresponsive to manual care and to help predict who may not respond adequately.
We suggest that diet and exercise are essential to managing these conditions, which can be supported with key nutrients, such as vitamin D, magnesium, and�omega-3 fatty acids. We also suggest that curcumin, G sylvestre, vanadyl sulfate chromium, and ?-lipoic acid could be viewed as specific nutrients that may be taken during the process of restoring appropriate insulin sensitivity and signaling.
Chiropractic Care
David R. Seaman DC, MS,?, Adam D. Palombo DC
Professor, Department of Clinical Sciences, National University of Health Sciences, Pinellas Park, FL Private Chiropractic Practice, Newburyport, MA
Funding Sources and Conflicts of Interest
No funding sources were reported for this study. David Seaman is a paid consultant for Anabolic Laboratories, a manufacturer of nutritional products for health care professionals. Adam Palombo was sponsored and remunerated by Anabolic laboratories to speak at chiropractic conventions/meetings.
Blank
References:
1. Kaur J. A comprehensive review on metabolic syndrome.<br />
Cardiol Res Pract 2014:943162, http://dx.doi.org/10.1155/<br />
2014/943162.<br />
2. Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic<br />
syndrome among US adults. Findings from the Third National<br />
Health and Nutrition Examination Survey. J Am Med Assoc<br />
2006;287:356�9.<br />
3. Boyle JP, Thompson TJ, Gregg EW, Barker LE, Williamson<br />
DF. Projection of the year 2050 burden of diabetes in the US<br />
adult population: dynamic modeling of incidence, mortality,<br />
and prediabetes prevalence. Popul Health Metr 2010;8:29,<br />
http://dx.doi.org/10.1186/1478-7954-8-29.<br />
4. [Internet]Centers for Disease Control and Prevention.<br />
Adult Obesity Facts. Atlanta: CDC; 2014. [Available from<br />http://www.cdc.gov/obesity/data/adult.html].<br />
5. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of<br />
childhood and adult obesity in the United States, 2011�2012.<br />
JAMA 2014;311(8):806�14.<br />
6. Riksman JS, Williamson OD, Walker BF. Delineating<br />
inflammatory and mechanical sub-types of low back pain: a<br />
pilot survey of fifty low back pain patients in a chiropractic<br />
setting. Chiropr Man Therap 2011;19(1):5, http://dx.doi.org/<br />
10.1186/2045-709X-19-5.<br />
7. Dobretsov M, Ghaleb AH, Romanovsky D, Pablo CS, Stimers<br />
JR. Impaired insulin signaling as a potential trigger of<br />
pain in diabetes and prediabetes. Int Anesthesiol Clin<br />
2007;45(2):95�105.<br />
8. Mantyselka P, Miettola J, Niskanen L, Kumpusalo E. Glucose<br />
regulation and chronic pain at multiple sites. Rheumatology<br />
2008;47(8):1235�8.<br />
9. M�ntyselk� P, Miettola J, Niskanen L, Kumpusalo E.<br />
Persistent pain at multiple sites�connection to glucose<br />
derangement. Diabetes Res Clin Pract 2009;84(2):e30�2.<br />
10. Mantyselka P, Kautianen H, Vanhala M. Prevalence of neck<br />
pain in subjects with metabolic syndrome�a cross-sectional<br />
population-based study. BMC Musculoskelet Disord 2010;11:<br />
171, http://dx.doi.org/10.1186/1471-2474-11-171.<br />
11. Rechardt M, Shiri R, Karppinen J, Jula A, Heli�vaara M,<br />
Viikari-Juntura E. Lifestyle and metabolic factors in relation<br />
to shoulder pain and rotator cuff tendinitis: a population-based<br />
study. BMC Musculoskelet Disord 2010;11:165.<br />
12. Gaida JE, Alfredson L, Kiss ZS, Wilson AM, Alfredson H,<br />
Cook JL. Dyslipidemia in Achilles tendinopathy is<br />
characteristic of insulin resistance. Med Sci Sports Exerc<br />
2009;41:1194�7.<br />
13. Malliaras P, Cook JL, Kent PM. Anthropometric risk factors<br />
for patellar tendon injury among volleyball players. Br J<br />
Sports Med 2007;41:259�63.<br />
14. Skrzynski S. DSC study of collagen in disc disease. J Biophys<br />
2009;2009:819635, http://dx.doi.org/10.1155/2009/819635.<br />
15. Luevano-Contreras C, Chapman-Novakofski K. Dietary<br />
advanced glycation end products and aging. Nutrients<br />
2010;2(12):1247�65 [2009;2009:819635].<br />
16. Abate M, Schiavone C, Pelotti P, Salini V. Limited joint<br />
mobility (LJM) in elderly subjects with type II diabetes<br />
mellitus. Arch Gerontol Geriatrics 2011;53:135�40.<br />
17. Sakellaridis N. The influence of diabetes mellitus on lumbar<br />
intervertebral disk herniation. Surg Neurol 2006;66:152�4.<br />
18. Shepherd PR, Kahn BB. Glucose transporters and insulin<br />
action: implications for insulin resistance and diabetes<br />
mellitus. New Eng J Med 1999;341(4):248�57.<br />
19. Abdul-Ghani MA, DeFronzo RA. Pathogenesis of insulin<br />
resistance in skeletal muscle. J Biomed Biotechnol 2010:19,<br />
http://dx.doi.org/10.1155/2010/476279 [Article ID 476279].<br />
20. [Internet]American Heart Association. About metabolic<br />
syndrome. Dallas: The Association; 2014. [Available from<br />http://www.heart.org/HEARTORG/Conditions/More/<br />MetabolicSyndrome/About-Metabolic-Syndrome_UCM_<br />301920_Article.jsp].<br />
21. Hotamisligil GS. Inflammation and metabolic disorders.<br />
Nature 2006;444:860�7.<br />
22. Glass CK, Olefsky JM. Inflammation and lipid signaling in the<br />
etiology of insulin resistance. Cell Metab 2012;15(5):635�45.<br />
23. Reaven GM. All obese individuals are not created equal:<br />
insulin resistance is the major determinant of cardiovascular<br />
disease in overweight/obese individuals. Diabetes Vasc Dis<br />
Res 2005;2:105�12.<br />
24. Ritov VB, Menshikova EV, He J, Ferrell RE, Goodpaster<br />
BH, Kelley DE. Deficiency of subsarcolemmal mitochondria<br />
in obesity and type 2 diabetes. Diabetes 2005;54:8�14.<br />
25. Corcoran MP, Lamon-Fava S, Fielding RA. Trans fats and<br />
insulin resistance: skeletal muscle lipid deposition and insulin<br />
resistance: effect of dietary fatty acids and exercise. Am J Clin<br />
Nutr 2007;85:662�77.<br />
26. Schipper HS, Prakken B, Kalkhoven E, Boes M. Adipose<br />
tissue-resident immune cells: key players in immunometabolism.<br />
Trends Endocrinol Metab 2012;23:407�15.<br />
27. Antuna-Puente B, Feve B, Fellahi S, Bastard JP. Adipokines:<br />
the missing link between insulin resistance and obesity.<br />
Diabetes Metab 2008;34:2�11.<br />
28. Grimble RF. Inflammatory status and insulin resistance. Curr<br />
Opin Clin Nutr Metab Care 2003;5:551�9.<br />
29. Tilg H, Moschen AR. Inflammatory mechanisms in<br />
the regulation of insulin resistance. Mol Med 2008;3�4:222�31.<br />
30. Johnson DR, O’Conner JC, Satpathy A, Freund GG.<br />
Cytokines in type 2 diabetes. Vitam Horm 2006;74:405�41.<br />
31. Ridker PM, Wilson PW, Grundy SM. Should C-reactive<br />
protein be added to the metabolic syndrome and to<br />
assessment of global cardiovascular risk? Circulation 2004;<br />
109:2818�25.<br />
32. Gelaye B, Revilla L, Lopez T, et al. Association between<br />
insulin resistance and c-reactive protein among Peruvian<br />
adults. Diabetol Metab Syn 2010;2:30.<br />
33. Singh VP, Bali A, Singh N, et al. Advanced glycation end<br />
products and diabetic complications. Korean J Physiol<br />
Pharmacol 2014;18(1):1�14.<br />
34. Baker RG, Hayden MS. NF-kB, inflammation and metabolic<br />
disease. Cell Metab 2011;13(1):11�22.<br />
35. Purkayastha S, Cair D. Neuroinflammatory basis of metabolic<br />
syndrome. Mol Metab Nov 2013;2(4):356�63.<br />
36. Ehse JA, Boni-Schnetzler M, Faulenbach M, Donath MY.<br />
Macrophages, cytokines and beta-cell death in type 2 diabetes.<br />
Biochem Soc Trans 2008;36(3):340�2.<br />
37. Boni-Schnetzler M, Ehses JA, Faulenbach M, Donath MY.<br />
Insulitis in type 2 diabetes. Diabetes Obes Metab 2008;10<br />
(Suppl 4):201�4.<br />
38. Donath MY, Schumann DM, Faulenbach M, Ellingsgaard H,<br />
Perren A, Ehses JA. Islet inflammation in type 2<br />
diabetes: from metabolic stress to therapy. Diabetes Care<br />
2008;31(Suppl 2):S161�4.<br />
39. Donath MY, Boni-Schnetzler M, Ellingsgaard H, Ehses JA.<br />
Islet inflammation impairs the pancreatic beta-cell in type 2<br />
diabetes. Physiology 2009;24:325�31.<br />
40. Harford KA, Reynolds CM, McGillicuddy FC, Roche HM.<br />
Fats, inflammation and insulin resistance: insights to the role<br />
of macrophage and T-cell accumulation in adipose tissue.<br />
Proc Nutr Soc 2011;70:408�17.<br />
41. Munoz A, Costa M. Nutritionally mediated oxidative stress and<br />
inflammation. Oxid Med Cell Longev 2013;2013:610950, http://<br />
dx.doi.org/10.1155/2013/610950.<br />
42. Wisse BE, Schwartz MW. Does hypothalamic inflammation<br />
cause obesity? Cell Metab 2009;10(4):241�2.<br />
43. Purkayastha S, Cair D. Neuroinflammatory basis of metabolic<br />
syndrome. Mol Metab Nov 2013;2(4):356�63.<br />
44. Calegari VC, Torsoni AS, Vanzela EC, Ara�jo EP, Morari<br />
J, Zoppi CC, et al. Inflammation of the hypothalamus leads<br />
to defective pancreatic islet function. J Biol Chem 2011;<br />
286(15):12870�80.<br />
45. Cordain L, Eaton SB, Sebastian A, et al. Origins and evolution<br />
of the Western diet: health implications for the 21st century.<br />
Am J Clin Nutr 2005;81:341�54.<br />
46. Barclay AW, Petocz P, McMillan-Price J, et al. Glycemic<br />
index, glycemic load, and chronic disease risk�a metaanalysis<br />
of observational studies. Am J Clin Nutr<br />
2008;87:627�37.<br />
47. Facchini FS, Hua N, Abbasi F, Reaven GM. Insulin resistance<br />
as a predictor of age-related disease. J Clin Endocrinol Metab<br />
2001;86:3574�8.<br />
48. Lin H, Lee B, Ho Y, et al. Postprandial glucose improves the<br />
risk prediction of cardiovascular death beyond the metabolic<br />
syndrome in the nondiabetic population. Diabetes Care Sep<br />
2009;32(9):1721�6.<br />
49. O’Keefe JH, Bell DS. Postprandial hyperglycemia/<br />
hyperlipidemia (postprandial dysmetabolism) is a cardiovascular<br />
risk factor. Am J Cardiol 2007;100:899�904.<br />
50. Cao H. Adipocytokines in obesity and metabolic disease.<br />
J Endocrinol 2014;220(2):T47�59.<br />
51. Nah SS, Choi IY, Lee CK, et al. Effects of advanced glycation<br />
end products on the expression of COX2, PGE2 and NO in human osteoarthritic chondrocytes. Rheumatology (Oxford)<br />
2008;47(4):425�31.<br />
52. Abate M, Schiavone C, Pelotti P, Salini V. Limited joint<br />
mobility (LJM) in elderly subjects with type II diabetes<br />
mellitus. Arch Gerontol Geriatr 2011;53:135�40.<br />
53. Robinson D, Mirovsky Y, Halperin N, Evron Z, Nevo Z.<br />
Changes in proteoglycans of intervertebral disc in diabetic<br />
patients: a possible cause of increased back pain. Spine<br />
1998;23:849�56.<br />
54. Sakellaridis N, Androulis A. Influence of diabetes mellitus on<br />
cervical intervertebral disc herniation. Clin Neurol Neurosurg<br />
2008;110:810�2.<br />
55. Jhawar BS, Fuchs CS, Colditz GA, Stampfer MJ. Cardiovascular<br />
risk factors for physician-diagnosed lumbar disc<br />
herniation. Spine J 2006;6:684�91.<br />
56. Lotan R, Oron A, Anekstein Y, Shalmon E, Mirovsky Y.<br />
Lumbar stenosis and systemic diseases: is there any relevance.<br />
J Spinal Disord Tech 2008;21:247�51.<br />
57. Anekstein Y, Smorgick Y, Lotan R, et al. Diabetes mellitus as<br />
a risk factor for the development of lumbar spinal stenosis. Isr<br />
Med Assoc J 2010;12:16�20.<br />
58. Choi KM. Sarcopenia and sarcopenic obesity. Endocrinol<br />
Metab (Seoul) 2013;28(2):86�9.<br />
59. D’hooge R, Cagnie B, Crombez G, et al. Increased<br />
intramuscular fatty infiltration without differences in lumbar<br />
muscle cross-sectional area during remission of unilateral<br />
recurrent low back pain. Man Ther 2012 Dec;17(6):5584�8.<br />
60. Chen YY, Pao JL, Liaw CK, et al. Image changes of paraspinal<br />
muscles and clinical correlations in patients with unilateral<br />
lumbar spinal stenosis. Eur Spine J 2014;23(5):999�1006.<br />
61. Kim Y, Park H. Does regular exercise without weight loss<br />
reduce insulin resistance in children and adolescents? In J<br />
Endocrinol 2013:402592, http://dx.doi.org/10.1155/2013/<br />
402592 [Epub 2013 Dec 12].<br />
62. Strasser B, Siebert U, Schobersberger W. Resistance training<br />
in the treatment of the metabolic syndrome: a systematic<br />
review and meta-analysis of the effect of resistance training on<br />
metabolic clustering in patients with abnormal glucose<br />
metabolism. Sports Med 2010;40:397�415.<br />
63. Sharman MJ, Volek JS. Weight loss leads to reductions in<br />
inflammatory biomarkers after a very-low-carbohydrate diet<br />
and a low-fat diet in overweight men. Clin Sci (Lond)<br />
2004;13:365�9.<br />
64. Teng KT, Chang CY, Chang LF, et al. Modulation of obesityinduced<br />
inflammation by dietary fats: mechanisms and<br />
clinical evidence. Nutr J 2014;13:12, http://dx.doi.org/<br />
10.1186/1475-2891-13-12.<br />
65. Tzotzas T, Evangelou P, Kiortsis DN. Obesity, weight loss<br />
and conditional cardiovascular risk factors. Obes Rev 2011;12<br />
(5):e282�9.<br />
66. Stone N, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA<br />
Guideline on the Treatment of Blood Cholesterol to Reduce<br />
Atherosclerotic Cardiovascular Risk in Adults: A report of<br />
the American College of Cardiology/American Heart<br />
Association Task Force on practice guidelines. Circulation<br />
2014;129(25 Suppl 2):S1�S45.<br />
67. P�rez-Guisado J, Mu�oz-Serrano A. A pilot study of the<br />
Spanish ketogenic Mediterranean diet: an effective therapy for<br />
the metabolic syndrome. J Med Food 2011;14(7�8):681�7.<br />
68. P�rez-Guisado J, Mu�oz-Serrano A, Alonso-Moraga A.<br />
Spanish ketogenic Mediterranean diet: a healthy cardiovascular<br />
diet for weight loss. Nutr J 2008;7:30, http://dx.doi.org/<br />
10.1186/1475-2891-7-30.<br />
69. Jonsson T, Granfeldt Y, Lindeberg S, et al. Subjective satiety<br />
and other experiences of a Paleolithic diet compared to a<br />
diabetes diet in patients with T2DM. Nutr J 2013;12:105,<br />
http://dx.doi.org/10.1186/1475-2891-12-105.<br />
70. Jonsson T, Granfeldt Y, Ahren B, et al. Beneficial effects of a<br />
Paleolithic diet on cardiovascular risk factors in T2DM: a<br />
randomized cross-over pilot study. Cardiovasc Diabetol<br />
2009;8:35, http://dx.doi.org/10.1186/1475-2840-8-35.<br />
71. Nicklas BJ, You T, Pahor M. Behavioural treatments<br />
for chronic system inflammation: effects of dietary<br />
weight loss and exercise training. Can Med Assoc J<br />
2005;172(9):1199�209.<br />
72. O’Keefe JH, Gheewala NM, O’Keefe JO. Dietary<br />
strategies for improving post-prandial glucose, lipids, inflammation,<br />
and cardiovascular health. J Am Coll Cardiol<br />
2008;51:249�55.<br />
73. O’Keefe Jr JH, Cordain L. Cardiovascular disease resulting<br />
from a diet and lifestyle at odds with our Paleolithic genome:<br />
how to become a 21st-century hunter�gatherer. Mayo Clin<br />
Proc 2004;79(1):101�8.<br />
74. Ames BN. Low micronutrient intake may accelerate the<br />
degenerative diseases of aging through allocation of scarce<br />
micronutrients by triage. Proc Natl Acad Sci U S A 2006;103<br />
(47):17589�94.<br />
75. Holick MF, Chen TC. Vitamin D deficiency: a worldwide<br />
problem with health consequences. Am J Clin Nutr<br />
2008;87:1080S�6S [Suppl.].<br />
76. Toubi E, Shoenfeld Y. The role of vitamin D in regulating<br />
immune responses. Isr Med Assoc J 2010;12(3):174�5.<br />
77. King DE, Mainous AG, Geesey ME, Egan BM, Rehman S.<br />
Magnesium supplement intake and C-reactive protein levels<br />
in adults. Nutr Res 2006;26:193�6.<br />
78. Rosanoff A, Weaver CM, Rude RK. Suboptimal magnesium<br />
status in the United States: are the health consequences<br />
underestimated? Nutr Rev 2012;70(3):153�64.<br />
79. Simopoulos AP. Omega-3 fatty acids in inflammation and<br />
autoimmune diseases. J Am Coll Nutr 2002;21(6):495�505.<br />
80. Simopoulos AP. The importance of the omega-6/omega-3<br />
fatty acid ratio in cardiovascular disease and other chronic<br />
diseases. Exp Biol Med 2008;233:674�88.<br />
81. Fung GJ, Steffen LM, Zhou X, et al. Vitamin D intake is<br />
inversely related to risk of developing metabolic syndrome<br />
in African American and white men and women over 20 y:<br />
the Coronary Artery Risk Development in Young Adults<br />
study. Am J Clin Nutr 2012;96(1):24�9 [Published online<br />2012 May 30].<br />
82. Palomer X, Gonzalez-Clemente JM, Blanco-Vaca F, Mauricio<br />
D. Role of vitamin D in the pathogenesis of type 2 diabetes<br />
mellitus. Diabetes Obes Metab 2008;10:185�97.<br />
83. Guadarrama-Lopez AL, Valdes-Ramos R, Martinex-Carrillo<br />
BE. T2DM, PUFAs, and vitamin D: their relation to<br />
inflammation. J Immunol Res 2014;2014:860703, http://dx.<br />
doi.org/10.1155/2014/860703.<br />
84. Cannell JJ, Hollis BW. Use of vitamin D in clinical practice.<br />
Altern Med Rev 2008;13(1):6�20.<br />
85. Davidson MB, Duran P, Lee ML, Friedman TC. High-dose<br />
vitamin D supplementation in people with prediabetes and<br />
hypovitaminosis D. Diabetes Care 2013;36(2):260�6, http://<br />
dx.doi.org/10.2337/dc12-1204.<br />
86. Schwalfenberg G. Vitamin D, and diabetes: improvement of<br />
glycemic control with vitamin D3 repletion. Can Fam<br />
Physician 2008;54:864�6.<br />
87. Kim DJ, Xun P, Liu K, et al. Magnesium intake in relation to<br />
systemic inflammation, insulin resistance, and the incidence<br />
of diabetes. Diabetes Care 2010;33(12):2604�10, http://dx.<br />
doi.org/10.2337/dc10-0994.<br />
88. Guerrero-Romero F, Tamez-Perez HE, Gonz�lez-Gonz�lez G,<br />
et al. Oral magnesium supplementation improves insulin<br />
sensitivity in non-diabetic subjects with insulin resistance. A<br />
double-blind placebo-controlled randomized trial. Diabetes<br />
Metab 2004;30(3):253�8.<br />
89. Rodr�guez-Mor�n M, Guerrero-Romero F. Oral magnesium<br />
supplementation improves insulin sensitivity and metabolic<br />
control in type 2 diabetic subjects: a randomized double-blind<br />
controlled trial. Diabetes Care 2003;26(4):1147�52.<br />
90. Song Y, He K, Levitan EB, Manson JE, Liu S. Effects of oral<br />
magnesium supplementation on glycaemic control in type 2<br />
diabetes: a meta-analysis of randomized double-blind controlled<br />
trials. Diabet Med 2006;23(10):1050�6.<br />
91. Mooren FC, Kr�ger K, V�lker K, Golf SW,Wadepuhl M, Kraus<br />
A. Oral magnesium supplementation reduces insulin resistance<br />
in non-diabetic subjects�a double-blind, placebo-controlled,<br />
randomized trial. Diabetes Obes Metab 2011;13(3):281�4.<br />
92. Aggarwal BB. Targeting inflammation induced obesity and<br />
metabolic diseases by curcumin and other nutraceuticals.<br />
Annu Rev Nutr 2010;30:173�9.<br />
93. Alappat L, Awad AB. Curcumin and obesity: evidence and<br />
mechanisms. Nutr Rev 2010;68(12):729�38.<br />
94. Gonzales AM, Orlando RA. Curcumin and resveratrol inhibit<br />
nuclear factor-kappaB-mediated cytokine expression in adipocytes.<br />
Nutr Metab 2008;5:17, http://dx.doi.org/10.1186/<br />
1743-7075-5-17.<br />
95. Sahebkar A. Why it is necessary to translate curcumin into<br />
clinical practice for the prevention and treatment of metabolic<br />
syndrome? Biofactors 2012, http://dx.doi.org/10.1002/<br />
biof.1062 [Epub ahead of print].<br />
96. Hsu CH, Cheng AL. Clinical studies with curcumin. Adv Exp<br />
Med Biol 2007;595:471�80.<br />
97. Chuengsamarn S, Rattanamongkolgul S, Luechapudiporn R,<br />
Phisalaphong C, Jirawatnotai S. Curcumin extract for prevention<br />
of type 2 diabetes. Diabetes Care 2012;35(11):2121�7.<br />
98. Jurenka JS. Anti-inflammatory properties of curcumin, a<br />
major constituent of curcuma longa: a review of preclinical<br />
and clinical research. Altern Med Rev 2009;14(2):141�53.<br />
99. Leach M. Gymnema sylvestre for diabetes mellitus: a systematic<br />
review. J Altern Complement Med 2007;13(9):977�83.<br />
100. Chattopadhyay R. A comparative evaluation of some blood<br />
sugar lowering agents of plant origin. J Ethnopharmacol<br />
1999;67:367�72.<br />
101. Nahas R, Moher M. Complementary and alternative medicine<br />
for the treatment of type 2 diabetes. Can Fam Physician<br />
2009;55:591�6.<br />
102. Vanadium/Vanadyl sulfate: monograph. Altern Med Rev<br />
2009;14:17�80.<br />
103. Boden G, Chen X, Ruiz J, et al. Effects of vanadyl sulfate<br />
on carbohydrate and lipid metabolism in patients with noninsulin-dependent<br />
diabetes mellitus. Metabolism 1996;45:<br />
1130�5.<br />
104. Jacques-Camarena O, Gonz�lez-Ortiz M, Mart�nez-Abundis E,<br />
et al. Effect of vanadium on insulin sensitivity in patients with<br />
impaired glucose tolerance. Ann Nutr Metab 2008;53:195�8.<br />
105. Vincent JB. The biochemisty of chromium. J Nutr<br />
2000;130:715�8.<br />
106. Anderson RA. Chromium and insulin resistance. Nutr Res<br />
Rev 2003;16:267�75.<br />
107. Vincent JB. Chromium: celebrating 50 years as an essential<br />
element? Dalton Trans 2010;39:3787�94.<br />
108. Office of Dietary Supplements. [Internet]. Dietary supplement<br />
fact sheet: Chromium. Washington, DC: United States<br />
Department of Health and Human Services. http://ods.od.nih.<br />
gov/factsheets/chromium/. Reviewed November 4, 2013.<br />
109. Anderson RA. Chromium, glucose intolerance and diabetes.<br />
J Am Coll Nutr 1998;17(6):548�55.<br />
110. Cefalu WT, Rood J, Patricia Pinsonat P, et al. Characterization<br />
of the metabolic and physiologic response to chromium<br />
supplementation in subjects with type 2 diabetes mellitus.<br />
Metab Clin Exp 2010;59:755�62.<br />
111. Heimbach JT, Anderson RA. Chromium: recent studies regarding<br />
nutritional roles and safety. Nutr Today 2005;40(4):180�95.<br />
112. Shay KP, Moreau RF, Smith EJ, Smith AR, Hagen TM.<br />
Alpha-lipoic acid as a dietary supplement: molecular<br />
mechanisms and therapeutic potential. Biochim Biophys<br />
Acta 2009;1790:1149�60.<br />
113. Morikawa T, Yasuno R, Wada H. Do mammalian cells<br />
synthesize lipoic acid? Identification of a mouse cDNA<br />
encoding a lipoic acid synthase located in mitochondria.<br />
FEBS Lett 2001;498:16�21.<br />
114. Singh U, Jialal I. Alpha-lipoic acid supplementation and<br />
diabetes. Nutr Rev 2008;66(11):646�57.<br />
115. Padmalayam I, Hasham S, Saxena U, Pillarisetti S. Lipoic acid<br />
synthase (LASY): a novel role in inflammation, mitochondrial<br />
function, and insulin resistance. Diabetes 2009;58:600�8.<br />
116. Capasso I, Esposito E, Maurea N, et al. Combination of<br />
inositol and alpha lipoic acid in metabolic syndrome-affected<br />
women: a randomized placebo-controlled trial. Trial<br />
2013;14:273, http://dx.doi.org/10.1186/1745-6215-14-273.<br />
117. Udupa A, Nahar P, Shah S, et al. A comparative study of<br />
effects of omega-3 fatty acids, alpha lipoic acid and vitamin E<br />
in T2DM. Ann Med Health Sci Res 2013;3(3):442�6.
The thyroid gland may be small but it plays a big role in how well your body functions. That is because the thyroid produces a hormone that regulates your metabolism, the process which converts everything you drink and eat into energy. However, when your metabolism slows, causing you to lose weight and feel sluggish and fatigued, you may have an underactive thyroid, medically referred to as hypothyroidism.
How can hypothyroidism affect your body?
Decreased levels of the thyroid hormone can lead to an increase in LDL cholesterol, or fat, in your blood. The thyroid hormone helps the liver break down the cholesterol circulating in your blood and stimulates. Triglycerides and your LDL cholesterol may substantially increase whenever you don’t have enough of the thyroid hormone. What’s more, hypothyroidism may also negatively affect your mood. The thyroid gland helps regulate the chemical messengers, or neurotransmitters, which your brain utilizes to communicate with your own nerves. These messengers can go haywire, causing one to feel anxious and depressed when your thyroid doesn’t function properly.
“The most important thing that you can do for hypothyroidism is to see your doctor and get on the right dose of thyroid hormone,” says R. Mack Harrell, MD, president-elect of the American Association of Clinical Endocrinologists and an endocrinologist at Memorial Regional Hospital in Hollywood, Fla..
Visiting your local healthcare professional’s office is a fundamental first step towards diagnosing and treating an underactive thyroid, or hypothyroidism, but what can you do to help yourself? Add exercise on your list. Regular exercise is an important part of your overall strategy to manage hypothyroidism symptoms. Exercise can offset the effects of your sluggish metabolism and burns calories to prevent weight gain. A good fitness routine may be a mood-booster as well because while you exercise, your body releases endorphins and other substances.
The Hypothyroidism-Exercise Link
What is the best type of exercise for hypothyroidism? A program of high heeled aerobic exercises and strength training is recommended by Yaroslav Gofnung, MD, an endocrinologist at Los Robles Hospital in Thousand Oaks, Calif.. Low-impact aerobics get your heart rate up and your lungs moving without putting too much strain on your joints, which can be vital because joint pain is another common hypothyroidism symptom, Dr. Gofnung says.
A stationary reclining or recumbent bicycle and a low-impact elliptical machine are exceptional machine choices for cardio exercise. “Walking is a fantastic exercise too, as long as you don’t have swelling in your knees or ankles,” Gofnung adds. Additionally, Pilates or gentle yoga may improve core muscles and alleviate the spine and hip pain which could be associated with hypothyroidism.
Individuals with hypothyroidism can also benefit from strength training exercises, such as lunges, leg lifts, and push-ups while other people may benefit from other strength training exercises involving weight-training machines. Strength training builds muscle mass, and muscle burns more calories even when you’re at rest. Building muscle can help prevent potential weight gain from an underactive thyroid gland.
The Best Exercises for Hypothyroidism
For people with hypothyroidism, Igor Klibanov, a personal coach in Toronto, founder of Fitness Solutions Plus, and also writer of “Unlimited Progress: The Way To Unlock Your Body’s Potential,” recommends cardio along with a strength-training routine that incorporates these six exercises:
One-legged dead lift: Stand on one leg while holding onto something for balance (not for support). Keep one hand relaxed in front of your thighs. Push on your hips up as far as you can, until your hand touches the ground. Come back up. This ought to be felt at the buttocks muscles. The back shouldn’t curve; but does not have to be upright.
Squats: Stand up straight and then bend at your knees and hips till you are at a sitting position. Go all of the way down. (Klibanov says it’s a myth that this may damage your knees if you have healthy knees to start with.) .
Overhead press or comparable vertical push movement. Boost a set of dumbbells to shoulder height. So they are facing forward switch your arms. Lift up the dumbbells until your elbows are right. Then lower them back down.
Lat pull-down or similar vertical pull move. Catch a pull-down bar with an overhand grip (palms facing away), and pull it down into your collar bone. Make certain that that the bar travels near to your face as you can.
Push-up or comparable horizontal push movement. Place both hands on the floor, shoulder width apart. Feet must be extended out and together. Till you are close to the ground, Bend your elbows and shoulders. In case a push is too hard, do the same thing either together with your hands on a table (while feet stay on the ground) or a wall socket.
Rowing or similar horizontal pull move. Sit with your hands holding the grip that’s connected to the cable. Keep your back straight, and lean back about 10 to15 degrees. Pull on back the cable until your mid-stomach touches. Then release under control.
Start with 15 repetitions of each exercise and work up to around 20. “Most people with joint issues find these to be easy on the joints,” Klibanov says. When you’re starting out, it might take you 15 to 20 minutes to finish your routine. A eventual aim: Work up which should take about 40 to 45 minutes, he adds. Schedule aerobic exercise a few times a week and participate in strength training routines with these motions two to three days weekly, Klibanov recommends. Doing this can get you on the ideal track to feeling better and losing weight.
Ease Into Exercise
Start slowly and build up. “If you go too quickly, it is possible to injure yourself and set yourself back,” Gofnung warns. Choose exercises that you enjoy and that your body is able to tolerate to increase the probability of your sticking to your regular, ” he advises.
Adjust the number of repetitions as you progress. “In just two weeks, you’ll have another body and you should have a different pattern,” Klibanov states. And do not be timid about progressing, he adds, “The further out of shape you are, the faster progress will come.”
If something hurts, you may have to make a small change like the angle or position of an exercise or motion. If it hurts, stop and find another exercise that does not cause discomfort. If you’re having difficulty by yourself, invest with a trainer that will make recommendations in time and explain to you how you can lose weight through the exercises you select.
Always talk with your doctor before beginning any exercise regimen. And never make exercise a substitute for thyroid drugs. With the right medication, you should feel better within a few weeks and have the motivation to get back to (or get into) a regular exercise regimen, Dr. Harrell says.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Abstract Objective: The purpose of this case report is to describe a patient with chronic, multisite muscle fasciculations who presented to a chiropractic teaching clinic and was treated with dietary modifications.
Clinical features: A 28-year-old man had muscle fasciculations of 2 years. The fasciculations began in his eye and progressed to the lips and lower extremities. In addition, he had gastrointestinal distress and fatigue. The patient was previously diagnosed as having wheat allergy at the age of 24 but was not compliant with a gluten-free diet at that time. Food sensitivity testing revealed immunoglobulin G�based sensitivity to multiple foods, including many different grains and dairy products. The working diagnosis was gluten neuropathy.
Intervention and outcome: Within 6 months of complying with dietary restrictions based on the sensitivity testing, the patient�s muscle fasciculations completely resolved. The other complaints of brain fog, fatigue, and gastrointestinal distress also improved.
Conclusions: This report describes improvement in chronic, widespread muscle fasciculations and various other systemic symptoms with dietary changes. There is strong suspicion that this case represents one of gluten neuropathy, although testing for celiac disease specifically was not performed.
Introduction:�Muscle Fasciculations
There are 3 known types of negative reactions to wheat proteins, collectively known as wheat protein reactivity: wheat allergy (WA), gluten sensitivity (GS),�and celiac disease (CD). Of the 3, only CD is known to involve autoimmune reactivity, generation of antibodies, and intestinal mucosal damage. Wheat allergy involves the release of histamine by way of immunoglobulin (Ig) E cross-linking with gluten peptides and presents within hours after ingestion of wheat proteins. Gluten sensitivity is considered to be a diagnosis of exclusion; sufferers improve symptomatically with a gluten-free diet (GFD) but do not express antibodies or IgE reactivity.1
The reported prevalence of WA is variable. Prevalence ranges from 0.4% to 9% of the population.2,3 The prevalence of GS is somewhat difficult to determine, as it does not have a standard definition and is a diagnosis of exclusion. Gluten sensitivity prevalence of 0.55% is based on National Health and Nutrition Examination Survey data from 2009 to 2010.4 In a 2011 study, a GS prevalence of 10% was reported in the US population.5 In contrast to the above 2 examples, CD is well defined. A 2012 study examining serum samples from 7798 patients in the National Health and Nutrition Examination Survey database from 2009 to 2010 found an overall prevalence of 0.71% in the United States.6
Neurologic manifestations associated with negative reactions to wheat proteins have been well documented. As early as 1908, �peripheral neuritis� was thought to be associated with CD.7 A review of all published studies on this topic from 1964 to 2000 indicated that the most common neurologic manifestations associated with GS were ataxia (35%), peripheral neuropathy (35%), and myopathy (16%). 8 Headaches, paresthesia, hyporeflexia, weakness, and vibratory sense reduction were reported to be more prevalent in CD patients vs controls.9 These same symptoms were more prevalent in CD patients who did not strictly follow a GFD vs those who were compliant with GFD.
At present, there are no case reports describing the chiropractic management of patient with gluten neuropathy. Therefore, the purpose of this case study is to describe a patient presentation of suspected gluten neuropathy and a treatment protocol using dietary modifications.
Case Report
A 28-year-old man presented to a chiropractic teaching clinic with complaints of constant muscle fasciculations of 2 years� duration. The muscle fasciculations originally started in the left eye and remained there for about 6 months. The patient then noticed that the fasciculations began to move to other areas of his body. They first moved into the right eye, followed by the lips,�and then to the calves, quadriceps, and gluteus muscles. The twitching would sometimes occur in a single muscle or may involve all of the above muscles simultaneously. Along with the twitches, he reports a constant �buzzing� or �crawling� feeling in his legs. There was no point during the day or night when the twitches ceased.
The patient originally attributed the muscle twitching to caffeine intake (20 oz of coffee a day) and stress from school. The patient denies the use of illicit drugs, tobacco, or any prescription medication but does drink alcohol (mainly beer) in moderation. The patient ate a diet high in meats, fruits, vegetables, and pasta. Eight months after the initial fasciculations began, the patient began to experience gastrointestinal (GI) distress. Symptoms included constipation and bloating after meals. He also began to experience what he describes as �brain fog,� a lack of concentration, and a general feeling of fatigue. The patient noticed that when the muscle fasciculations were at their worst, his GI symptoms correspondingly worsened. At this point, the patient put himself on a strict GFD; and within 2 months, the symptoms began to alleviate but never completely ceased. The GI symptoms improved, but he still experienced bloating. The patient�s diet consisted mostly of meats, fruit, vegetables, gluten-free grains, eggs, and dairy.
At the age of 24, the patient was diagnosed with WA after seeing his physician for allergies. Serum testing revealed elevated IgE antibodies against wheat, and the patient was advised to adhere to a strict GFD. The patient admits to not following a GFD until his fasciculations peaked in December 2011. In July of 2012, blood work was evaluated for levels of creatine kinase, creatine kinase�MB, and lactate dehydrogenase to investigate possible muscle breakdown. All values were within normal limits. In September of 2012, the patient under- went food allergy testing once again (US Biotek, Seattle, WA). Severely elevated IgG antibody levels were found against cow�s milk, whey, chicken egg white, duck egg white, chicken egg yolk, duck egg yolk, barley, wheat gliadin, wheat gluten, rye, spelt, and whole wheat (Table 1). Given the results of the food allergy panel, the patient was recommended to remove this list of foods from his diet. Within 6 months of complying with the dietary changes, the patient�s muscle fasciculations completely resolved. The patient also experienced much less GI distress, fatigue, and lack of concentration.
Discussion
The authors could not find any published case studies related to a presentation such as the one�described here. We believe this is a unique presentation of wheat protein reactivity and thereby represents a contribution to the body of knowledge in this field.
This case illustrates an unusual presentation of a widespread sensorimotor neuropathy that seemed to respond to dietary changes. Although this presentation is consistent with gluten neuropathy, a diagnosis of CD was not investigated. Given the patient had both GI and neurologic symptoms, the likelihood of gluten neuropathy is very high.
There are 3 forms of wheat protein reactivity. Because there was confirmation of WA and GS, it was decided that testing for CD was unnecessary. The treatment for all 3 forms is identical: GFD.
The pathophysiology of gluten neuropathy is a topic that needs further investigation. Most authors agree it involves an immunologic mechanism, possibly a direct or indirect neurotoxic effect of antigliadin anti- bodies. 9,10 Briani et al 11 found antibodies against ganglionic and/or muscle acetylcholine receptors in 6 of 70 CD patients. Alaedini et al12 found anti-ganglioside antibody positivity in 6 of 27 CD patients and proposed that the presence of these antibodies may be linked to gluten neuropathy.
It should also be noted that both dairy and eggs showed high responses on the food sensitivity panel. After reviewing the literature, no studies could be located linking either food with neuromuscular symp- toms consistent with the ones presented here. There- fore, it is unlikely that a food other than gluten was responsible for the muscle fasciculations described in this case. The other symptoms described (fatigue, brain fog, GI distress) certainly may be associated with any number of food allergies/sensitivities.
Limitations
One limitation in this case is the failure to confirm CD. All symptoms and responses to dietary change point to this as a likely possibility, but we cannot confirm this diagnosis. It is also possible that the�symptomatic response was not due directly to dietary change but some other unknown variable. Sensitivity to foods other than gluten was documented, including reactions to dairy and eggs. These food sensitivities may have contributed to some of the symptoms present in this case. As is the nature of case reports, these results cannot necessarily be generalized to other patients with similar symptoms.
Conclusion:�Muscle Fasciculations
This report describes improvement in chronic, widespread muscle fasciculations and various other systemic symptoms with dietary change. There is strong suspicion that this case represents one of gluten neuropathy, although testing for CD specifically was not performed.
Brian Anderson DC, CCN, MPHa,?, Adam Pitsinger DCb
Attending Clinician, National University of Health Sciences, Lombard, IL Chiropractor, Private Practice, Polaris, OH
Acknowledgment
This case report is submitted as partial fulfillment of the requirements for the degree of Master of Science in Advanced Clinical Practice in the Lincoln College of Post-professional, Graduate, and Continuing Education at the National University of Health Sciences.
Funding Sources and Conflicts of Interest
No funding sources or conflicts of interest were reported for this study.
References:
1. Sapone A, Bai J, Ciacci C, et al. Spectrum of gluten-related
disorders: consensus on new nomenclature and classification.
BMC Med 2012;10:13.
2. Matricardi PM, Bockelbrink A, Beyer K, et al. Primary versus
secondary immunoglobulin E sensitization to soy and wheat in
the Multi-Centre Allergy Study cohort. Clin Exp Allergy
2008;38:493�500.
3. Vierk KA, Koehler KM, Fein SB, Street DA. Prevalence of
self-reported food allergy in American adults and use of food
labels. J Allergy Clin Immunol 2007;119:1504�10.
4. DiGiacomo DV. Prevalence and characteristics of non-celiac
gluten sensitivity in the United States: results from the
continuous National Health and Nutrition Examination Survey
2009-2010. Presented at: the 2012 American College of
Gastroenterology Annual Scientific Meeting; Oct. 19-24, Las
Vegas.; 2012.
5. Sapone A, Lammers KM, Casolaro V. Divergence of gut
permeability and mucosal immune gene expression in two
gluten-associated conditions: celiac disease and gluten sensitivity.
BMC Med 2011;9:23.
6. Rubio-Tapia A, Ludvigsson JF, Brantner TL, Murray JA,
Everhart JE. The prevalence of celiac disease in the United
States. Am J Gastroenterol 2012 Oct;107(10):1538�44.
7. Hadjivassiliou M, Grunewald RA, Davies-Jones GAB. Gluten
sensitivity as a neurological illness. J Neurol Neurosurg
Psychiatr 2002;72:560�3.
8. Hadjivassiliou M, Chattopadhyay A, Grunewald R, et al.
Myopathy associated with gluten sensitivity. Muscle Nerve
2007;35:443�50.
9. Cicarelli G, Della Rocca G, Amboni C, et al. Clinical and
neurological abnormalities in adult celiac disease. Neurol Sci
2003;24:311�7.
10. Hadjivassiliou M, Grunewald RA, Kandler RH. Neuropathy
associated with gluten sensitivity. J Neurol Neurosurg
Psychiatry 2006;77:1262�6.
11. Briani C, Doria A, Ruggero S, et al. Antibodies to muscle and
ganglionic acetylcholine receptors in celiac disease. Autoimmunity
2008;41(1):100�4.
12. Alaedini A, Green PH, Sander HW, et al. Ganglioside reactive
antibodies in the neuropathy associated with celiac disease.
J Neuroimmunol 2002;127(1�2):145�8.
Hypothyroidism can be a tricky condition to handle, and what you eat could interfere with your treatment. Some nutrients influence the function of the thyroid gland, and certain foods can inhibit your body’s ability to absorb them.
What foods can affect thyroid disease?
Having a thyroid condition is often difficult, but you are not alone with this particular health issue. According to the American Thyroid Association, more than 12 percent of the populace may wind up coping with a thyroid disease.
As with many health conditions, some factors are out of your control, such as your family history and the environment around you. But nutrition and diet also plays a role in thyroid health and since you’re the one in control of your plate, then you can decide which thyroid-friendly foods to pick as you handle hypothyroidism and its symptoms.
Foods with Soy (Edamame, Tofu, and Miso)
There’s long been concern over the potential negative effects that certain compounds in soy, called isoflavones, may have on the thyroid gland. Some researchers think that a person’s risk for hypothyroidism can increase. However others theorize that those with both hypothyroidism and an iodine deficiency should observe their intake.
So there are no specific nutritional guidelines regarding the consumption of soy, but some studies do indicate that the ingestion of soy may interfere with the ability to intake thyroid drugs and medications. Because of this, you may want to wait four hours before taking your dose, after eating these foods. Check with your doctor.
Cruciferous Vegetables (Broccoli and Cauliflower)
Cruciferous vegetables, such as broccoli and cabbage, are full of fiber and other nutrients, but they could interfere with the production of thyroid gland when you experience an iodine deficiency. Therefore, in case you do, it is a great idea to restrict your intake of Brussels sprouts, cabbage, cauliflower, kale, turnips, and bok choy, since research indicates digesting these veggies may block the thyroid’s ability to utilize iodine, which is vital for normal thyroid function.
If you have been diagnosed with both hypothyroidism and iodine deficiency, there are a number of things you can do to make these vegetables less dangerous. Cooking them can reduce the impact that cruciferous vegetables have on the thyroid gland, and limiting your intake of these (cooked) vegetables to 5 ounces a day can help too, because that amount appears to have no negative impact on thyroid functioning.
Gluten (Bread, Pasta, and Rice)
People who have migraines might wish to look at decreasing their intake of gluten, a protein found in foods processed from barley, wheat, rye, and other grains, ” says Ruth Frechman, RDN, a dietitian in the Los Angeles area and a spokesperson for the Academy of Nutrition and Dietetics. And in case you’re diagnosed with celiac disease, gluten may hamper absorption of thyroid hormone replacement medication, and can irritate the small intestine.
An article published in May 2017 in the journal “Endocrine Connections” noted that celiac and rheumatoid disease tend to be present together, and while no research has demonstrated that a gluten-free diet can treat thyroid problems, you might want to speak to a healthcare professional about whether it might be well worth eliminating gluten, or becoming tested for celiac disease. If you do decide to eat gluten, make sure to choose whole-grains varieties of bread, pasta, and rice, that are high in fiber and other nutrients and can help improve bowel irregularity, a symptom of hypothyroidism.
Fatty Foods (Butter, Meat, and Fried Foods)
Fats have been found to disrupt the human body’s ability to absorb thyroid hormone replacement medicines, says Stephanie Lee, MD, PhD, associate chief of endocrinology, nutrition, and diabetes in Boston Medical Center and an associate professor in the Boston University School of Medicine in Massachusetts.
Fats may also interfere with the thyroid’s ability to produce hormone as well. Some healthcare professionals recommend that you just cut out on foods that are fried and lower your intake of fats from resources such as butter, mayonnaise, margarine, and fatty cuts of beef.
Sugary Foods (Chocolate and Desserts)
Hypothyroidism may cause the body’s metabolism to slow down, Frechman states. That means it’s simple to put on pounds if you aren’t careful. “You would like to avoid foods with excess amounts of sugar because it’s a lot of calories without the nourishment,” she states. Attempt to eliminate it completely or it is best to decrease.
Processed Foods in Packages
“Processed foods generally get lots of sodium, and individuals with hypothyroidism should avoid sodium,” Frechman states. Having an underactive thyroid increases a individual’s risk for high blood pressure, and sodium that is an excessive amount of increases this risk.
Read the “Nutrition Facts” label on the packaging of processed foods to seek out options lowest in sodium. Individuals with an increased risk for hypertension should restrict their sodium intake according to the American Heart Association.
Excessive Fiber (Beans, Legumes, and Vegetables)
Getting enough fiber is good for you, but also much may complicate your hypothyroidism therapy. The government Strategies for Americans recommends that adults choose in 20 to 35 g of fiber a day. Amounts of fiber from fruits, vegetables, whole grains, beans, and legumes which go above that amount affect your digestive tract and may interfere with absorption of thyroid hormone replacement drugs.
If you’re on a high-fiber diet, ask your physician if you will need a higher dose of thyroid medicine. If you aren’t absorbing enough medication your maintenance dose may have to be increased.
Coffee (Time your First Cup Carefully)
Caffeine has been shown to block absorption of thyroid hormone replacement, says Dr. Lee. “People who had been taking their thyroid medication with their morning coffee had uncontrollable thyroid levels, and we couldn’t figure it out,” she states. “I now must be very careful to tell people, ‘Simply take your medicine with water.'” You should wait at least 30 minutes before having a cup of coffee after taking your medication.
Alcohol and Thyroid Health
Alcohol consumption can cause a mess on both thyroid hormone levels in the body and the ability of the thyroid gland to produce these hormones. Alcohol appears to have a toxic effect in the thyroid gland and it also suppresses the ability of the body to utilize thyroid gland hormones. Ideally, individuals with migraines should cut out alcohol completely..
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
The thyroid gland is a butterfly-shaped gland in your neck. Among its primary functions is to pump out a hormone called thyroxine. It is that hormone which sets the rate of the human body. It’s what regulates energy generation. Some of thyroid hormone’s imbalances common indicators include tiredness, bloating, hair loss, dry skin, joint pain, muscle stiffness, elevated cholesterol, sleep disturbance, infertility, melancholy, cold hands and feet, along with weight gain.
How do you recognize thyroid gland imbalances?
Patients eliminate weight with hypothyroidism while gaining weight is a textbook symptom of hypothyroidism. In some cases a part of their disease is that their gut is so broken down that their thyroid is malfunctioning however they’re currently slimming down and that they’re malabsorbing nourishment. If we fall into those health care conceptions with by each person who has hypothyroidism then we are likely to miss a great deal of individuals.
Identifying Thyroid Disease
Traditional diagnosis is made depending on the lab test TSH (thyroid stimulating hormone) normally ordered by a general physician, internist, or endocrinologist. One of the many problems with this strategy is that it isn’t comprehensive. If your TSH comes back high, the physician tends to diagnose you. This approach often times contributes to treatment with thyroid hormone replacement medication without further investigation. Keep in mind one fundamental point, taking thyroid medication and using a minimal thyroid diagnosis doesn’t fix the problem.
Ultimately, the objective of the healthcare professional and patient should be to recognize why the thyroid levels are abnormal. And that requires a basic knowledge of biochemistry and nutrition. Let us take a deeper look at a few of the common items, in the diet and nutrition standpoint, that can contribute to low thyroid hormone production:
Gluten
Sugar
Goitrogenic foods
Dairy
Nutritional deficiencies
Gluten and your Thyroid Gland
Gluten sensitivity contributes to thyroid disease in many of different ways. Gluten induced gastrointestinal harm is one of the mechanisms of action. It is this mechanism that leads to a domino-like effect. The very first step in this process is the invention of intestinal hyper-permeability, or Leaky Gut. When the barrier is compromised, a cascade of inflammation, immune over-stimulation, and mimicry may ensue. Over time these procedures can result in an autoimmune thyroid response leading to Hashimoto’s thyroid disease or Graves’ disease.
Gluten induced gastrointestinal damage may contribute to inadequate digestion and absorption of thyroid crucial nutrients. Gluten can alter gut bacteria that are ordinary. These bacteria play a important role in thyroid gland conversion. Physicians will assert that no study exists between thyroid free and gluten disorder. They are incorrect.
Where do we find gluten? Folks will say that barley, wheat and rye are the grains that contain gluten. In reality there are distinct sorts of gluten and they’re observed in all the different forms of grain.
Sugar
This refers specifically to processed sugar like dextrose, glucose, fructose, maltodextrin, all the different kinds of sugar that is processed, even organic processed sugars. Many of the food manufacturers have gotten wise about people wanting to prevent sugar so they’ve started saying it. For example sucanat is processed sugar. Avoidance of processed sugar must be a priority to prevent imbalances with the thyroid gland and thyroid disease.
Goitrogens
There are numerous foods that can suppress thyroid hormone production and bring about goiter (thyroid enlargement). Listed below are several foods which can cause this. You can get in trouble if you consume excessive quantities of these foods, for example if you are doing a great deal of juicing and using a pound of each time or if it’s raw and it hasn’t been cooked. If you also have a thyroid condition and if you’re eating cruciferous vegetables, its advice not to stop eating them just cook them and do not make them the key foods in your diet plan.
Soy (prevent soy, particularly GMO soy)
Brussels Sprouts
Bok choy
Cabbage
Cauliflower
Collards
Cassava
Broccoli
Kale
Bamboo shoots
Spinach
Radishes
Rutabaga
Turnips
Watercress
Kohlrabi
Mustard greens
Flax
Pine nuts
Peanuts
The protein casein in milk can mimic glutenfree. Therefore it may be the dairy in their diet that mimics gluten. Gluten, sugar, goitrogenic foods, and dairy are the most usual food-based causes for thyroid hormone disturbance.
Nutrition is Vital for a Healthy Thyroid
Now let’s discuss a food component that is going to be helpful for the thyroid gland to function. There are a number of nutrients necessary for thyroid function. Vitamins and minerals help drive the chemistry behind the production of the thyroid hormones. Additionally they help these hormones and other organs and both the DNA communicate to improve and regulate metabolism.
As mentioned before, often times healthcare professionals will only conduct one laboratory test known as TSH (thyroid stimulating hormone) for the identification and treatment of thyroid disease. If TSH is above normal, you’re diagnosed “hypothyroid”. If TSH is below normal, you’re diagnosed “hyperthyroid”. Simple, right? No, far from it.
TSH is a regulatory hormone produced in the brain from the pituitary gland. TSH then travels to the thyroid gland in your neck out of the brain and tells it to produce the thyroid hormone T4. TSH needs to be made first. What ingredients does your body need to generate TSH? The number one ingredient is protein. How much is enough protein? To get a mean calculation, take your body weight in kilograms (whatever you weigh in pounds split that by 2.2 to give you your weight in kilograms) and multiply that by 0.8 and that’s how many grams of protein you need daily. Another way to calculate this amount is to multiply the amount 0.36 by your weight in lbs. As an instance, for a woman, that could be 54 g of protein. This number is individual for each individual and varies by the individual’s level of physical activity. Speak with your doctor if you suffer from kidney dysfunction. What else does our body need to generate TSH? Magnesium, Vitamin B12, and zinc. Without adequate levels of these ingredients your body cannot produce TSH and you will have low thyroid function from the start.
Now lets discuss thyroxine, T4. Thyroid hormone is potassium and protein. Protein is crucial to form the thyroid hormone (particularly the amino acid in protein called tyrosine). The “4” in T4 signifies the number of molecules of iodine are present. You need iodine for that sport car to run smoothly. Where do we get iodine? Iodine is got by us from things found not in lakes, not from rivers. Seafood, kelp, and seaweed are great sources of iodine. Consider the thyroid gland as a car factory. Internally on your thyroid gland, your thyroid uses a ton of vitamin C. Vitamin C is very important to add those iodine tires to that thyroid gland. You also need vitamin B2. There is something in your thyroid gland known as. It when you consume the iodine and iodine-rich foods is absorbed into the bloodstream. The symporter necessitates B2 to function. Is vitamin B3. To make thyroid hormone T4, you need Vitamin B3, Vitamin B2, Vitamin C, C, and vitamin.
T4 is inactive thyroid hormone. Protein is responsible for carrying T4 to your own tissues including muscle and your liver in which it has converted to T3 thyroid gland through the blood stream. Think of the proteins into your bloodstream that take the T4 thyroid hormone. The inactive T4 thyroid hormone is being hauled to the liver, muscle, and other tissues in which they are converted to the active T3 hormone. There is a process called deiodinization, where the body takes that T4 thyroid gland and eliminates one molecule of iodine to convert it. A whole lot of the conversion of T4 to T3 happens in the liver and that is because their liver is not good at converting T4 to T3, the reason why a person who has liver problems can also have thyroid problems. This conversion takes place in the muscle which is the reason why people with muscle inflammation frequently have thyroid issues. Which nutrient is required for this conversion? Selenium. You require selenium to eliminate that one molecule of iodine to convert T4 into T3 thyroid gland. You need iron to the conversion of T4 into T3.
It’s T3 we consider the active thyroid hormone. Each cell of the body has. There are receptors that act like a gap. T3 is your key that activates the enzymes that ramp up your metabolism and binds to all those receptors around the nucleus. You need Vitamin vitamin D to bind to a T3 to make a super key that unlocks your DNA and fits the nuclear receptors.
In the conclusion, you need Omega-3 fatty acids around the membrane of these cells for the hormone to be received appropriately. If you’re missing even one of those nutrients, you will have some kind of biochemical thyroid suppression.
This seems different for different people. For instance, some people have severe selenium deficiency in which they are currently converting T4 thyroid hormone that is hardly any inactive . Their physician is prescribing a sort of synthetic thyroxine T4 thyroid hormone (levothyroxine, Synthroid, etc.), however they can not convert the T4 in thyroxine into the active T3. They believe much worse being on the medication. I see other people with a genetic susceptibility for Vitamin B2 deficiency who can’t get iodine. You can fix them with foods rich in the nutrients and/or with supplements, if you have one of those nutrient deficiencies. The first step is deciding whether or not you have one or more of these deficiencies.
The following is a summary of nutrition your doctor should measure when evaluating your thyroid:
Protein
Magnesium
Zinc
Selenium
Iodine
Iron
Vitamin C
Vitamin B2
Vitamin B3
Vitamin D
Vitamin A
Vitamin B12
Omega-3
If you don’t have your healthcare professional test for these nutrient deficiencies, then you’ll never know why you’ve got a thyroid problem. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
The thyroid gland is a 2-inch butterfly-shaped organ located in the front part of the neck. Although small, the thyroid glans is a major gland in the endocrine system and affects virtually every organ in the body.
What is the function of the thyroid gland?
The thyroid gland regulates fat and carbohydrate metabolism, respiration, body temperature, brain growth, cholesterol levels, the heart and nervous system, blood glucose levels cycle, skin integrity, and more.
Thyroid Diseases Explained
Thyroid disease generally involves an underactive thyroid gland, also known as hypothyroidism. In the USA, an autoimmune reaction called autoimmune thyroiditis or Hashimoto’s disease usually causes hypothyroidism. As with all autoimmune disorders, the body identifies its own tissues as an invader and strikes until the organ is destroyed. This chronic attack will finally prevent the thyroid gland from producing thyroid hormones. The lack of these hormones may slow down metabolism and also cause weight gain, fatigue, dry skin and hair loss as well as lead to difficulty concentrating. Hashimoto’s thyroid disease affects approximately 5 percent of the US population, is seven times more prevalent in women than men, and generally occurs during middle age.
Hyperthyroidism, or an overactive thyroid gland, is another frequent thyroid disease. The form is Graves’ disease in which the body’s autoimmune reaction causes the thyroid gland to make too much T3 and T4. Symptoms of hyperthyroidism may include weight loss, high blood pressure, nausea, and a rapid heartbeat. The disease also disproportionately affects women and presents until the age of 40.
Hashimoto’s thyroid disease is more common than Graves’ disease, but both are known as autoimmune thyroid disease (ATD), which has a strong genetic link and is associated with other autoimmune disorders, such as type 1 diabetes, rheumatoid arthritis, lupus, and celiac disease. A goiter, or enlargement of the thyroid gland, may be caused by hypothyroidism, hyperthyroidism, excessive or insufficient consumption of iodine from the diet, or thyroid gland, the most frequent endocrine cancer whose prevalence studies imply is increasing.
Key Nutrients for Thyroid Disease
Many dietary factors play a role in optimizing thyroid function. But, excesses and both nutrient deficiencies could cause or exacerbate symptoms. Working in collaboration with a doctor is ideal to determine status for optimal thyroid health. Many functional medicine practitioners specialize in functional nutrition, which can help with thyroid disease.
Iodine
Iodine is a vital nutrient in the human body and essential to thyroid function; thyroid hormones have been constituted of iodine. Iodine deficiency is the cause while disorder is the primary cause of thyroid dysfunction in the United States
Iodine deficiency has been considered uncommon in america since the 1920s, largely as a result of widespread utilization of iodized salt. This, along with poultry, milk, and grains, is a major source of iodine in the conventional American diet.
However, iodine intake has decreased during the last few decades. Americans get approximately 70 percent of their salt intake from foods which, in the USA and Canada, don’t contain iodine. A 2012 Centers for Disease Control and Prevention report indicates that, on average, Americans are receiving sufficient amounts of iodine, together with the potential exclusion of women of childbearing age.
Both iodine deficiency and surplus have significant dangers; thus, supplementation ought to be approached with care. Supplemental iodine might lead to symptom flare-ups in individuals with Hashimoto’s thyroid disease because it stimulates antibodies.
Iodine intake often is not easily apparent on a dietary recall because the quantity in foods is largely determined by levels from the soil and extra salt. But, experts state that, “Clients carrying iodine tablets are a red flag. Frequent intake of foods such as seaweed or an avoidance of all iodized salt may serve as signals that further exploration is required.”
Vitamin D
Vitamin D deficiency is connected to Hashimoto’s, according to one study showing that over 90 percent of patients studied were deficient. It’s uncertain whether the low vitamin D levels were the direct cause of Hashimoto’s or the result of the disease process itself.
Hyperthyroidism, especially Graves’ disease, is known to cause bone loss, which can be compounded by the vitamin D deficiency commonly seen in people with hyperthyroidism. This bone mass could be recovered with therapy for hyperthyroidism, and specialists indicate that sufficient nourishment, such as vitamin D, which are particularly important during and following
Foods which contain some vitamin D include fatty fish, milk, legumes, eggs, and mushrooms. Sunlight also is a source, but the sum of vitamin production depends upon the season and latitude. Supplemental D3 could be necessary, if clients have low vitamin D levels, along with the customer’s doctor should monitor progress to ensure the individual’s levels stay within a suitable range.
Selenium
The maximum concentration of selenium is found in the thyroid gland, and it has been demonstrated to be a necessary element of enzymes integral to thyroid function. Selenium is a vital trace mineral and was shown to have a deep effect in the immune system, cognitive function, fertility in both women and men, and mortality rate.
A meta-analysis of randomized, placebo-controlled studies has shown advantages of selenium on both the thyroid antibody titers and mood in patients with Hashimoto’s, but this impact appears more pronounced in people who have a selenium deficiency or insufficiency in the outset. Conversely, an excessive intake of selenium can lead to gastrointestinal distress or perhaps raise the risk of type 2 diabetes and cancer. So clients will benefit from getting their selenium levels tested and integrating healthful foods into their diets, including Brazil nuts, tuna, crab, and lobster.
Vitamin B12
Studies show that about 30 percent of people with ATD experience a vitamin B12 deficiency. Food sources of B12 include salmon, sardines, mollusks, organ meats such as liver, muscle meat, and dairy. Vegan sources include fortified cereals and yeast. Severe B12 deficiency may be irreversible, therefore it is important for dietitians to suggest clients have their levels analyzed.
Goitrogens
Cruciferous vegetables like broccoli, cauliflower, and cabbage naturally discharge a chemical known as goitrin when they are hydrolyzed, or broken down. Goitrin can interfere with the synthesis of thyroid hormones. Nonetheless, this is usually a concern only when combined with an iodine deficiency. Heating cruciferous vegetables denatures much or all of this possible goitrogenic effect.
Soy is another possible goitrogen. The isoflavones in soy may lower thyroid hormone synthesis, but many studies have discovered that consuming soy does not result in hypothyroidism in individuals with adequate iodine stores. But Dean cautions clients to consume soy in moderation.
The potential exclusion is millet, a nutritious gluten-free grain, which might suppress thyroid function even in people with adequate iodine intake. If a dietary recall indicates frequent millet ingestion in patients with hypothyroidism, it may be wise to indicate they choose another grain.
Foods, Supplements, and Medication Interactions
When it comes to thyroid medications, it is very important to RDs to know the drugs can interact with common nutritional supplements. Calcium supplements have the capacity to interfere with absorption of thyroid medications, so when taking the two patients need to consider the timing. Studies recommend limiting calcium supplements and thyroid drugs by at least four hours. Coffee and fiber nutritional supplements reduced the absorption of thyroid drugs, so patients should take them one hour apart. Dietitians should affirm whether customers have received and are adhering to these guidelines for optimum wellness.
Chromium picolinate, which is marketed for blood sugar control and weight reduction, also impairs the absorption of thyroid medications. If clients decide to take chromium picolinate, then they ought to take it three to four hours apart from thyroid drugs. Flavonoids in vegetables, fruits, and tea have been shown to have potential cardiovascular benefits. But, high-dose flavonoid supplements can suppress thyroid function. The Natural Standards Database provides a comprehensive list of nutritional supplements with a possible impact on thyroid function, thus taking precautions and coordinating patient care with a knowledgeable practitioner is sensible.
Exercise
A discussion on thyroid disorder and good health is not complete without stressing the importance of physical activity. Lisa Lilienfield, MD, a thyroid disorder specialist in the Kaplan Center for Integrative Medicine in McLean, Virginia, and a certified yoga teacher, is a firm believer in the value of exercise, especially. “With hypothyroid patients, certainly exercise can assist with weight gain, fatigue, and depression. With hyperthyroidism, anxiety and sleep disturbances are so common, and exercise might help regulate both.”
In addition to the obvious impact exercise has on weight and metabolism, a study of patients with Graves’ disease found that a structured exercise plan revealed remarkable improvements in fatigue levels, and significantly more patients have been able to successfully quit taking antithyroid medications with no relapse.
In Conclusion
Celiac disease presents unique challenges as a result of unwanted weight changes, significant cardiovascular disease, and symptoms such as fatigue, mood changes, and gastrointestinal upset, which can hinder the growth of healthful behaviors. It’s vital that dietitians focus when counselling clients on setting goals that are realistic for adjustments and routine exercise. With so many nutrient deficiencies and interactions with medications and nutritional supplements, it will be important for dietitians to coordinate with their clients’ health care team for health outcomes.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
The increased prevalence of obesity and related comorbidities is a major public health problem. While genetic factors undoubtedly play a role in determining individual susceptibility to weight gain and obesity, the identified genetic variants only explain part of the variation. This has led to growing interest in understanding the potential role of epigenetics as a mediator of gene-environment interactions underlying the development of obesity and its associated comorbidities. Initial evidence in support of a role of epigenetics in obesity and type 2 diabetes mellitus (T2DM) was mainly provided by animal studies, which reported epigenetic changes in key metabolically important tissues following high-fat feeding and epigenetic differences between lean and obese animals and by human studies which showed epigenetic changes in obesity and T2DM candidate genes in obese/diabetic individuals. More recently, advances in epigenetic methodologies and the reduced cost of epigenome-wide association studies (EWAS) have led to a rapid expansion of studies in human populations. These studies have also reported epigenetic differences between obese/T2DM adults and healthy controls and epigenetic changes in association with nutritional, weight loss, and exercise interventions. There is also increasing evidence from both human and animal studies that the relationship between perinatal nutritional exposures and later risk of obesity and T2DM may be mediated by epigenetic changes in the offspring. The aim of this review is to summarize the most recent developments in this rapidly moving field, with a particular focus on human EWAS and studies investigating the impact of nutritional and lifestyle factors (both pre- and postnatal) on the epigenome and their relationship to metabolic health outcomes. The difficulties in distinguishing consequence from causality in these studies and the critical role of animal models for testing causal relationships and providing insight into underlying mechanisms are also addressed. In summary, the area of epigenetics and metabolic health has seen rapid developments in a short space of time. While the outcomes to date are promising, studies are ongoing, and the next decade promises to be a time of productive research into the complex interactions between the genome, epigenome, and environment as they relate to metabolic disease.
Keywords: Epigenetics, DNA methylation, Obesity, Type 2 diabetes, Developmental programming
Introduction
Obesity is a complex, multifactorial disease, and better understanding of the mechanisms underlying the interactions between lifestyle, environment, and genetics is critical for developing effective strategies for prevention and treatment [1].
In a society where energy-dense food is plentiful and the need for physical activity is low, there is a wide variation in individuals� susceptibility to develop�obesity and metabolic health problems. Estimates of the role of heredity in this variation are in the range of 40�70 %, and while large genome-wide association studies (GWAS) have identified a number of genetic loci associated with obesity risk, the ~100 most common genetic variants only account for a few percent of variance in obesity [2, 3]. Genome-wide estimates are higher, accounting for ~20 % of the variation [3]; however, a large portion of the heritability remains unexplained.
Recently, attention has turned to investigating the role of epigenetic changes in the etiology of obesity. It has been argued that the epigenome may represent the mechanistic link between genetic variants and environmental�factors in determining obesity risk and could help explain the �missing heritability.� The first human epigenetic studies were small and only investigated a limited number of loci. While this generally resulted in poor reproducibility, some of these early findings, for instance the relationship between PGC1A methylation and type 2 diabetes mellitus (T2DM) [4] and others as discussed in van Dijk et al. [5], have been replicated in later studies. Recent advances and increased affordability of high- throughput technologies now allow for large-scale epigenome wide association studies (EWAS) and integration of different layers of genomic information to explore the complex interactions between the genotype, epigenome, transcriptome, and the environment [6�9]. These studies are still in their infancy, but the results thus far have shown promise in helping to explain the variation in obesity susceptibility.
There is increasing evidence that obesity has develop mental origins, as exposure to a suboptimal nutrient supply before birth or in early infancy is associated with an increased risk of obesity and metabolic disease in later life [10�13]. Initially, animal studies demonstrated that a range of early life nutritional exposures, especially those experienced early in gestation, could induce epigenetic changes in key metabolic tissues of the offspring that persisted after birth and result in permanent alterations in gene function [13�17]. Evidence is emerging to support the existence of the same mechanism in humans. This has led to a search for epigenetic marks present early in life that predict later risk of metabolic disease, and studies to determine whether epigenetic programming of metabolic disease could be prevented or reversed in later life.
This review provides an update of our previous systematic review of studies on epigenetics and obesity in humans [5]. Our previous review showcased the promising outcomes of initial studies, including the first potential epigenetic marks for obesity that could be detected at birth (e.g., RXRA) [18]. However, it also highlighted the limited reproducibility of the findings and the lack of larger scale longitudinal investigations. The current review focuses on recent developments in this rapidly moving field and, in particular, on human EWAS and studies investigating the impact of (pre- and postnatal) nutritional and lifestyle factors on the epigenome and the emerging role of epigenetics in the pathology of obesity. We also address the difficulties in identifying causality in these studies and the importance of animal models in providing insight into mechanisms.
Review
Epigenetic Changes In Animal Models Of Obesity
Animal models provide unique opportunities for highly controlled studies that provide mechanistic insight into�the role of specific epigenetic marks, both as indicators of current metabolic status and as predictors of the future risk of obesity and metabolic disease. A particularly important aspect of animal studies is that they allow for the assessment of epigenetic changes within target tissues, including the liver and hypothalamus, which is much more difficult in humans. Moreover, the ability to harvest large quantities of fresh tissue makes it possible to assess multiple chromatin marks as well as DNA methylation. Some of these epigenetic modifications either alone or in combination may be responsive to environmental programming. In animal models, it is also possible to study multiple generations of offspring and thus enable differentiation between trans-generational and intergenerational transmission of obesity risk mediated by epigenetic memory of parental nutritional status, which cannot be easily distinguished in human studies. We use the former term for meiotic transmission of risk in the absence of continued exposure while the latter primarily entails direct transmission of risk through metabolic reprogramming of the fetus or gametes.
Animal studies have played a critical role in our current understanding of the role of epigenetics in the developmental origins of obesity and T2DM. Both increased and decreased maternal nutrition during pregnancy have been associated with increased fat deposition in offspring of most mammalian species studied to date (reviewed in [11, 13�15, 19]). Maternal nutrition during pregnancy not only has potential for direct effects on the fetus, it also may directly impact the developing oocytes of female fetuses and primordial germ cells of male fetuses and therefore could impact both the off- spring and grand-offspring. Hence, multigenerational data are usually required to differentiate between maternal intergenerational and trans-generational transmission mechanisms.
Table 1 summarizes a variety of animal models that have been used to provide evidence of metabolic and epigenetic changes in offspring associated with the parental plane of nutrition. It also contains information pertaining to studies identifying altered epigenetic marks in adult individuals who undergo direct nutritional challenges. The table is structured by suggested risk transmission type.
(i) Epigenetic Changes In Offspring Associated With Maternal Nutrition During Gestation
Maternal nutritional supplementation, undernutrition, and over nutrition during pregnancy can alter fat deposition and energy homeostasis in offspring [11, 13�15, 19]. Associated with these effects in the offspring are changes in DNA methylation, histone post-translational modifications, and gene expression for several target genes,�especially genes regulating fatty acid metabolism and insulin signaling [16, 17, 20�30]. The diversity of animal models used in these studies and the common metabolic pathways impacted suggest an evolutionarily conserved adaptive response mediated by epigenetic modification. However, few of the specific identified genes and epigenetic changes have been cross-validated in related studies, and large-scale genome-wide investigations have typically not been applied. A major hindrance to comparison of these studies is the different develop mental windows subjected to nutritional challenge, which may cause considerably different outcomes. Proof that the epigenetic changes are causal rather than being associated with offspring phenotypic changes is also required. This will necessitate the identification of a parental nutritionally induced epigenetic �memory� response that precedes development of the altered phenotype in offspring.
(ii)Effects Of Paternal Nutrition On Offspring Epigenetic Marks
Emerging studies have demonstrated that paternal plane of nutrition can impact offspring fat deposition and epigenetic marks [31�34]. One recent investigation using mice has demonstrated that paternal pre-diabetes leads to increased susceptibility to diabetes in F1 offspring with associated changes in pancreatic gene expression and DNA methylation linked to insulin signaling [35]. Importantly, there was an overlap of these epigenetic changes in pancreatic islets and sperm suggesting germ line inheritance. However, most of these studies, although intriguing in their implications, are limited in the genomic scale of investigation and frequently show weak and somewhat transient epigenetic alterations associated with mild metabolic phenotypes in offspring.
(iii)Potential Trans-generational Epigenetic Changes Promoting Fat Deposition In Offspring
Stable transmission of epigenetic information across multiple generations is well described in plant systems and C. elegans, but its significance in mammals is still much debated [36, 37]. An epigenetic basis for grand- parental transmission of phenotypes in response to dietary exposures has been well established, including in livestock species [31]. The most influential studies demonstrating effects of epigenetic transmission impacting offspring phenotype have used the example of the viable yellow agouti (Avy) mouse [38]. In this mouse, an insertion of a retrotransposon upstream of the agouti gene causes its constitutive expression and consequent yellow coat color and adult onset obesity. Maternal transmission through the germ line results in DNA methylation�mediated silencing of agouti expression resulting in wild-type coat color and lean phenotype of the offspring [39, 40]. Importantly, subsequent studies in these mice demonstrated that maternal exposure to methyl donors causes a shift in coat color [41]. One study has reported transmission of a phenotype to the F3 generation and alterations in expression of large number of genes in response to protein restriction in F0 [42]; however, alterations in expression were highly variable and a direct link to epigenetic changes was not identified in this system.
(iv) Direct Exposure Of Individuals To Excess Nutrition In Postnatal Life
While many studies have identified diet-associated epigenetic changes in animal models using candidate site-specific regions, there have been few genome-wide analyses undertaken. A recent study focussed on determining the direct epigenetic impact of high-fat diets/ diet-induced obesity in adult mice using genome-wide gene expression and DNA methylation analyses [43]. This study identified 232 differentially methylated regions (DMRs) in adipocytes from control and high-fat fed mice. Importantly, the corresponding human regions for the murine DMRs were also differentially methylated in adipose tissue from a population of obese and lean humans, thereby highlighting the remarkable evolutionary conservation of these regions. This result emphasizes the likely importance of the identified DMRs in regulating energy homeostasis in mammals.
Human Studies
Drawing on the evidence from animal studies and with the increasing availability of affordable tools for genome- wide analysis, there has been a rapid expansion of epigenome studies in humans. These studies have mostly focused on the identification of site-specific differences in DNA methylation that are associated with metabolic phenotypes.
A key question is the extent to which epigenetic modifications contribute to the development of the metabolic phenotype, rather than simply being a con- sequence of it (Fig. 1). Epigenetic programming could contribute to obesity development, as well as playing a role in consequent risk of cardiovascular and metabolic problems. In human studies, it is difficult to prove causality [44], but inferences can be made from a number of lines of evidence:
(i) Genetic association studies. Genetic polymorphisms that are associated with an increased risk of developing particular conditions are a priori linked to the causative genes. The presence of differential�methylation in such regions infers functional relevance of these epigenetic changes in controlling expression of the proximal gene(s). There are strong cis-acting genetic effects underpinning much epigenetic variation [7, 45], and in population-based studies, methods that use genetic surrogates to infer a causal or mediating role of epigenome differences have been applied [7, 46�48]. The use of familial genetic information can also lead to the identification of potentially causative candidate regions showing phenotype-related differential methylation [49].
(ii)Timing of epigenetic changes. The presence of an epigenetic mark prior to development of a phenotype is an essential feature associated with causality. Conversely, the presence of a mark in association with obesity, but not before its development, can be used to exclude causality but would not exclude a possible role in subsequent obesity-related pathology.
(iii)Plausible inference of mechanism. This refers to epigenetic changes that are associated with altered expression of genes with an established role in regulating the phenotype of interest. One such example is the association of methylation at two CpG sites at the CPT1A gene with circulating triglyceride levels [50]. CPT1A encodes carnitine palmitoyltransferase 1A, an enzyme with a central role in fatty acid metabolism, and this is strongly indicative that differential methylation of this gene may be causally related to the alterations in plasma triglyceride concentrations.
Epigenome-Wide Association Studies: Identifying Epigenetic Biomarkers Of Metabolic Health
A number of recent investigations have focused on exploring associations between obesity/metabolic diseases�and DNA methylation across the genome (Table 2). The largest published EWAS so far, including a total of 5465 individuals, identified 37 methylation sites in blood that were associated with body mass index (BMI), including sites in CPT1A, ABCG1, and SREBF1 [51]. Another large-scale study showed consistent associations between BMI and methylation in HIF3A in whole blood and adipose tissue [52], a finding which was also partially replicated in other studies [9, 51]. Other recently reported associations between obesity-related measures and DNA methylation include (i) DNA methylation differences between lean and obese individuals in LY86 in blood leukocytes [53]; (ii) associations between PGC1A promoter methylation in whole blood of children and adiposity 5 years later [54]; (iii) associations between waist-hip ratio and ADRB3 methylation in blood [55]; and (iv) associations between BMI, body fat distribution measures, and multiple DNA methylation sites in adipose tissue [9, 56]. EWAS have also shown associations between DNA methylation sites and blood lipids [55, 57�59], serum metabolites [60], insulin resistance [9, 61], and T2DM [48, 62, 63] (Table 2).
From these studies, altered methylation of PGC1A, HIF3A, ABCG1, and CPT1A and the previously described RXRA [18] have emerged as biomarkers associated with, or perhaps predictive of, metabolic health that are also plausible candidates for a role in development of metabolic disease.
Interaction Between Genotype And The Epigenome
Epigenetic variation is highly influenced by the underlying genetic variation, with genotype estimated to explain ~20�40 % of the variation [6, 8]. Recently, a number of studies have begun to integrate methylome and genotype data to identify methylation quantitative trait loci (meQTL) associated with disease phenotypes. For instance, in adipose tissue, an meQTL overlapping�with a BMI genetic risk locus has been identified in an enhancer element upstream of ADCY3 [8]. Other studies have also identified overlaps between known obesity and T2DM risk loci and DMRs associated with obesity and T2DM [43, 48, 62]. Methylation of a number of such DMRs was also modulated by high-fat feeding in mice [43] and weight loss in humans [64]. These results identify an intriguing link between genetic variations linked with disease susceptibility and their association with regions of the genome that undergo epigenetic modifications in response to nutritional challenges, implying a causal relationship. The close connection between genetic and epigenetic variation may signify their essential roles in generating individual variation [65, 66]. However, while these findings suggest that DNA methylation may be a mediator of genetic effects, it is also important to consider that both genetic and epigenetic processes could act independently on the same genes. Twin studies [8, 63, 67] can provide important insights and indicate that inter-individual differences in levels of DNA methylation arise predominantly from non-shared environment and stochastic influences, minimally from shared environmental effects, but also with a significant impact of genetic variation.
The Impact Of The Prenatal And Postnatal Environment On The Epigenome
Prenatal environment: Two recently published studies made use of human populations that experienced �natural� variations in nutrient supply to study the impact of maternal nutrition before or during pregnancy on DNA methylation in the offspring [68, 69]. The first study used a Gambian mother-child cohort to show that both seasonal variations in maternal methyl donor intake during pregnancy and maternal pre-pregnancy BMI were associated with altered methylation in the infants [69]. The second study utilized adult offspring from the Dutch Hunger Winter cohort to investigate the effect of prenatal exposure to an acute period of severe maternal undernutrition on DNA methylation of genes involved in growth and metabolism in adulthood [68]. The results highlighted the importance of the timing of the exposure in its impact on the epigenome, since significant epigenetic effects were only identified in individuals exposed to famine during early gestation. Importantly, the epigenetic changes occurred in conjunction with increased BMI; however, it was not possible to establish in this study whether these changes were present earlier in life or a consequence of the higher BMI.
Other recent studies have provided evidence that prenatal over-nutrition and an obese or diabetic maternal environment are also associated with DNA methylation changes in genes related to embryonic development, growth, and metabolic disease in the offspring [70�73].
While human data are scarce, there are indications that paternal obesity can lead to altered methylation of imprinted genes in the newborn [74], an effect thought to be mediated via epigenetic changes acquired during spermatogenesis.
Postnatal environment: The epigenome is established de novo during embryonic development, and therefore, the prenatal environment most likely has the most significant impact on the epigenome. However, it is now clear that changes do occur in the �mature� epigenome under the influence of a range of conditions, including aging, exposure to toxins, and dietary alterations. For example, changes in DNA methylation in numerous genes in skeletal muscle and PGC1A in adipose tissue have been demonstrated in response to a high-fat diet [75, 76]. Interventions to lose body fat mass have also been associated with changes in DNA methylation. Studies have reported that the DNA methylation profiles of adipose tissue [43, 64], peripheral blood mononuclear cells [77], and muscle tissue [78] in formerly obese patients become more similar to the profiles of lean subjects following weight loss. Weight loss surgery also partially reversed non-alcoholic fatty liver disease-associated methylation changes in liver [79] and in another study led to hypomethylation of multiple obesity candidate genes, with more pronounced effects in subcutaneous compared to omental (visceral) fat [64]. Accumulating evidence suggests that exercise interventions can also influence DNA methylation. Most of these studies have been conducted in lean individuals [80�82], but one exercise study in obese T2DM subjects also demonstrated changes in DNA methylation, including in genes involved in fatty acid and glucose transport [83]. Epigenetic changes also occur with aging, and recent data suggest a role of obesity in augmenting them [9, 84, 85]. Obesity accelerated the epigenetic age of liver tissue, but in contrast to the findings described above, this effect was not reversible after weight loss [84].
Collectively, the evidence in support of the capacity to modulate the epigenome in adults suggests that there may be the potential to intervene in postnatal life to modulate or reverse adverse epigenetic programming.
Effect Sizes And Differences Between Tissue Types
DNA methylation changes associated with obesity or induced by diet or lifestyle interventions and weight loss are generally modest (<15 %), although this varies depending on the phenotype and tissue studied. For instance, changes greater than 20 % have been reported in adipose tissue after weight loss [64] and associations between HIF3A methylation and BMI in adipose tissue were more pronounced than in blood [52].
The biological relevance of relatively small methylation changes has been questioned. However, in tissues consisting of a mixture of cell types, a small change in DNA methylation may actually reflect a significant change in a specific cell fraction. Integration of epigenome data with transcriptome and other epigenetic data, such as histone modifications, is important, since small DNA methylation changes might reflect larger changes in chromatin structure and could be associated with broader changes in gene expression. The genomic context should also be considered; small changes within a regulatory element such as a promotor, enhancer, or insulator may have functional significance. In this regard, DMRs for obesity, as well as regions affected by prenatal famine exposure and meQTL for metabolic trait loci have been observed to overlap enhancer elements [8, 43, 68]. There is evidence that DNA methylation in famine-associated regions could indeed affect enhancer activity [68], supporting a role of nutrition-induced methylation changes in gene regulation.
A major limitation in many human studies is that epigenetic marks are often assessed in peripheral blood, rather than in metabolically relevant tissues (Fig. 2). The heterogeneity of blood is an issue, since different cell populations have distinct epigenetic signatures, but algorithms have been developed to estimate the cellular composition to overcome this problem [86]. Perhaps more importantly, epigenetic marks in blood cells may not necessarily report the status of the tissues of primary interest. Despite this, recent studies have provided clear evidence of a relationship between epigenetic marks in blood cells and BMI. In the case of HIF3A for which the level of methylation (beta-value) in the study population ranged from 0.14�0.52, a 10 % increase in methylation was associated with a BMI increase of 7.8 %�[52]. Likewise, a 10 % difference in PGC1A methylation may predict up to 12 % difference in fat mass [54].
Conclusions
The study of the role of epigenetics in obesity and metabolic disease has expanded rapidly in recent years, and evidence is accumulating of a link between epigenetic modifications and metabolic health outcomes in humans. Potential epigenetic biomarkers associated with obesity and metabolic health have also emerged from recent studies. The validation of epigenetic marks in multiple cohorts, the fact that several marks are found in genes with a plausible function in obesity and T2DM development, as well as the overlap of epigenetic marks with known obesity and T2DM genetic loci strengthens the evidence that these associations are real. Causality has so far been difficult to establish; however, regardless of whether the associations are causal, the identified epigenetic marks may still be relevant as biomarkers for obesity and metabolic disease risk.
Effect sizes in easily accessible tissues such as blood are small but do seem reproducible despite variation in ethnicity, tissue type, and analysis methods [51]. Also, even small DNA methylation changes may have biological significance. An integrative �omics� approach will be crucial in further unraveling the complex interactions between the epigenome, transcriptome, genome, and metabolic health. Longitudinal studies, ideally spanning multiple generations, are essential to establishing causal relationships. We can expect more such studies in the future, but this will take time.
While animal studies continue to demonstrate an effect of early life nutritional exposure on the epigenome and metabolic health of the offspring, human data are still limited. However, recent studies have provided clear�evidence that exposure to suboptimal nutrition during specific periods of prenatal development is associated with methylation changes in the offspring and therefore have the potential to influence adult phenotype. Animal studies will be important to verify human findings in a more controlled setting, help determine whether the identified methylation changes have any impact on metabolic health, and unravel the mechanisms underlying this intergenerational/transgenerational epigenetic regulation. The identification of causal mechanisms underlying metabolic memory responses, the mode of transmission of the phenotypic effects into successive generations, the degree of impact and stability of the transmitted trait, and the identification of an overarching and unifying evolutionary context also remain important questions to be addressed. The latter is often encapsulated by the predictive adaptive response hypothesis, i.e., a response to a future anticipated environment that increases fitness of the population. However, this hypothesis has increasingly been questioned as there is limited evidence for increased fitness later in life [87].
In summary, outcomes are promising, as the epigenetic changes are linked with adult metabolic health and they act as a mediator between altered prenatal nutrition and subsequent increased risk of poor metabolic health outcomes. New epigenetic marks have been identified that are associated with measures of metabolic health. Integration of different layers of genomic information has added further support to causal relationships, and there have been further studies showing effects of pre- and postnatal environment on the epigenome and health. While many important questions remain, recent methodological advances have enabled the types of large-scale population-based studies that will be required to address the knowledge gaps. The next decade promises to be a period of major activity in this important research area.
Susan J. van Dijk1, Ross L. Tellam2, Janna L. Morrison3, Beverly S. Muhlhausler4,5� and Peter L. Molloy1*�
Competing interests
The authors declare that they have no competing interests.
Authors� contributions
All authors contributed to the drafting and critical revision of the manuscript, and all authors read and approved the final manuscript.
Authors� information
Beverly S. Muhlhausler and Peter L. Molloy are joint last authors.
Acknowledgements
This work has been supported by a grant from the Science and Industry Endowment Fund (Grant RP03-064). JLM and BSM are supported by the National Health and Medical Research Council Career Development Fellowships (JLM, APP1066916; BSM, APP1004211). We thank Lance Macaulay and Sue Mitchell for critical reading and comments on the manuscript.
Author details
1CSIRO Food and Nutrition Flagship, PO Box 52, North Ryde, NSW 1670, Australia. 2CSIRO Agriculture Flagship, 306 Carmody Road, St Lucia, QLD 4067, Australia. 3Early Origins of Adult Health Research Group, School of Pharmacy and Medical Sciences, Sansom Institute for Health Research, University of South Australia, GPO Box 2471, Adelaide, SA 5001, Australia�4FOODplus Research Centre, Waite Campus, The University of Adelaide, PMB 1, Glen Osmond, SA 5064, Australia. 5Women�s and Children�s Health Research Institute, 72 King William Road, North Adelaide, SA 5006, Australia.
Blank
References:
1. WHO. WHO | Overweight and obesity. http://www.who.int/gho/ncd/
risk_factors/overweight/en/index.html. Accessed 29 January 2015.
2. Visscher PM, Brown MA, McCarthy MI, Yang J. Five years of GWAS discovery.
Am J Hum Genet. 2012;90:7�24.
3. Locke AE, Kahali B, Berndt SI, Justice AE, Pers TH, Day FR, et al. Genetic
studies of body mass index yield new insights for obesity biology. Nature.
2015;518:197�206.
4. Ling C, Del Guerra S, Lupi R, R�nn T, Granhall C, Luthman H, et al.
Epigenetic regulation of PPARGC1A in human type 2 diabetic islets and
effect on insulin secretion. Diabetologia. 2008;51:615�22.
5. Van Dijk SJ, Molloy PL, Varinli H, Morrison JL, Muhlhausler BS. Epigenetics
and human obesity. Int J Obes (Lond). 2015;39:85�97.
6. Teh AL, Pan H, Chen L, Ong M-L, Dogra S, Wong J, et al. The effect of
genotype and in utero environment on interindividual variation in neonate
DNA methylomes. Genome Res. 2014;24:1064�74.
7. Olsson AH, Volkov P, Bacos K, Dayeh T, Hall E, Nilsson EA, et al. Genomewide
associations between genetic and epigenetic variation influence
mRNA expression and insulin secretion in human pancreatic islets. PLoS
Genet. 2014;10:e1004735.
8. Grundberg E, Meduri E, Sandling JK, Hedman AK, Keildson S, Buil A, et al.
Global analysis of DNA methylation variation in adipose tissue from twins
reveals links to disease-associated variants in distal regulatory elements.
Am J Hum Genet. 2013;93:876�90.
9. Ronn T, Volkov P, Gillberg L, Kokosar M, Perfilyev A, Jacobsen AL, et al.
Impact of age, BMI and HbA1c levels on the genome-wide DNA
methylation and mRNA expression patterns in human adipose tissue
and identification of epigenetic biomarkers in blood. Hum Mol Genet.
2015;24:3792�813.
10. Waterland RA, Michels KB. Epigenetic epidemiology of the developmental
origins hypothesis. Annu Rev Nutr. 2007;27:363�88.
11. McMillen IC, Rattanatray L, Duffield JA, Morrison JL, MacLaughlin SM, Gentili
S, et al. The early origins of later obesity: pathways and mechanisms. Adv
Exp Med Biol. 2009;646:71�81.
12. Ravelli A, van der Meulen J, Michels R, Osmond C, Barker D, Hales C, et al.
Glucose tolerance in adults after prenatal exposure to famine. Lancet.
1998;351:173�7.
13. McMillen IC, MacLaughlin SM, Muhlhausler BS, Gentili S, Duffield JL,
Morrison JL. Developmental origins of adult health and disease: the role of
periconceptional and foetal nutrition. Basic Clin Pharmacol Toxicol.
2008;102:82�9.
14. Zhang S, Rattanatray L, McMillen IC, Suter CM, Morrison JL. Periconceptional
nutrition and the early programming of a life of obesity or adversity. Prog
Biophys Mol Biol. 2011;106:307�14.
15. Bouret S, Levin BE, Ozanne SE. Gene-environment interactions controlling
energy and glucose homeostasis and the developmental origins of obesity.
Physiol Rev. 2015;95:47�82.
16. Borengasser SJ, Zhong Y, Kang P, Lindsey F, Ronis MJ, Badger TM, et al.
Maternal obesity enhances white adipose tissue differentiation and alters
genome-scale DNA methylation in male rat offspring. Endocrinology.
2013;154:4113�25.
17. Gluckman PD, Lillycrop KA, Vickers MH, Pleasants AB, Phillips ES, Beedle AS,
et al. Metabolic plasticity during mammalian development is directionally
dependent on early nutritional status. Proc Natl Acad Sci U S A.
2007;104:12796�800.
18. Godfrey KM, Sheppard A, Gluckman PD, Lillycrop KA, Burdge GC, McLean C,
et al. Epigenetic gene promoter methylation at birth is associated with
child�s later adiposity. Diabetes. 2011;60:1528�34.
19. McMillen IC, Adam CL, Muhlhausler BS. Early origins of obesity:
programming the appetite regulatory system. J Physiol. 2005;565(Pt 1):9�17.
20. Begum G, Stevens A, Smith EB, Connor K, Challis JR, Bloomfield F, et al.
Epigenetic changes in fetal hypothalamic energy regulating pathways are
associated with maternal undernutrition and twinning. FASEB J.
2012;26:1694�703.
21. Ge ZJ, Liang QX, Hou Y, Han ZM, Schatten H, Sun QY, et al. Maternal obesity
and diabetes may cause DNA methylation alteration in the spermatozoa of
offspring in mice. Reprod Biol Endocrinol. 2014;12:29.
22. Jousse C, Parry L, Lambert-Langlais S, Maurin AC, Averous J, Bruhat A, et al.
Perinatal undernutrition affects the methylation and expression of the leptin
gene in adults: implication for the understanding of metabolic syndrome.
FASEB J. 2011;25:3271�8.
23. Lan X, Cretney EC, Kropp J, Khateeb K, Berg MA, Penagaricano F, et al.
Maternal diet during pregnancy induces gene expression and DNA
methylation changes in fetal tissues in sheep. Front Genet. 2013;4:49.
24. Li CC, Young PE, Maloney CA, Eaton SA, Cowley MJ, Buckland ME, et al.
Maternal obesity and diabetes induces latent metabolic defects and
widespread epigenetic changes in isogenic mice. Epigenetics. 2013;8:602�11.
25. Lillycrop KA, Phillips ES, Jackson AA, Hanson MA, Burdge GC. Dietary protein
restriction of pregnant rats induces and folic acid supplementation prevents
epigenetic modification of hepatic gene expression in the offspring. J Nutr.
2005;135:1382�6.
26. Radford EJ, Ito M, Shi H, Corish JA, Yamazawa K, Isganaitis E, et al. In utero
effects. In utero undernourishment perturbs the adult sperm methylome
and intergenerational metabolism. Science. 2014;345(80):1255903.
27. Suter M, Bocock P, Showalter L, Hu M, Shope C, McKnight R, et al.
Epigenomics: maternal high-fat diet exposure in utero disrupts
peripheral circadian gene expression in nonhuman primates. FASEB J.
2011;25:714�26.
28. Suter MA, Ma J, Vuguin PM, Hartil K, Fiallo A, Harris RA, et al. In utero
exposure to a maternal high-fat diet alters the epigenetic histone code in a
murine model. Am J Obs Gynecol. 2014;210:463 e1�463 e11.
29. Tosh DN, Fu Q, Callaway CW, McKnight RA, McMillen IC, Ross MG, et al.
Epigenetics of programmed obesity: alteration in IUGR rat hepatic IGF1
mRNA expression and histone structure in rapid vs. delayed postnatal
catch-up growth. Am J Physiol Gastrointest Liver Physiol.
2010;299:G1023�9.
30. Sandovici I, Smith NH, Nitert MD, Ackers-Johnson M, Uribe-Lewis S, Ito Y,
et al. Maternal diet and aging alter the epigenetic control of a promoterenhancer
interaction at the Hnf4a gene in rat pancreatic islets. Proc Natl
Acad Sci U S A. 2011;108:5449�54.
31. Braunschweig M, Jagannathan V, Gutzwiller A, Bee G. Investigations on
transgenerational epigenetic response down the male line in F2 pigs. PLoS
One. 2012;7, e30583.
32. Carone BR, Fauquier L, Habib N, Shea JM, Hart CE, Li R, et al. Paternally
induced transgenerational environmental reprogramming of metabolic
gene expression in mammals. Cell. 2010;143:1084�96.
33. Ost A, Lempradl A, Casas E, Weigert M, Tiko T, Deniz M, et al. Paternal diet
defines offspring chromatin state and intergenerational obesity. Cell.
2014;159:1352�64.
34. Mart�nez D, Pentinat T, Rib� S, Daviaud C, Bloks VW, Cebri� J, et al. In utero
undernutrition in male mice programs liver lipid metabolism in the secondgeneration
offspring involving altered Lxra DNA methylation. Cell Metab.
2014;19:941�51.
35. Wei Y, Yang C-R, Wei Y-P, Zhao Z-A, Hou Y, Schatten H, et al. Paternally
induced transgenerational inheritance of susceptibility to diabetes in
mammals. Proc Natl Acad Sci U S A. 2014;111:1873�8.
36. Grossniklaus U, Kelly WG, Kelly B, Ferguson-Smith AC, Pembrey M, Lindquist
S. Transgenerational epigenetic inheritance: how important is it? Nat Rev
Genet. 2013;14:228�35.
37. Pembrey M, Saffery R, Bygren LO. Human transgenerational responses to
early-life experience: potential impact on development, health and
biomedical research. J Med Genet. 2014;51:563�72.
38. Wolff GL, Kodell RL, Moore SR, Cooney CA. Maternal epigenetics and methyl
supplements affect agouti gene expression in Avy/a mice. FASEB J.
1998;12:949�57.
39. Jirtle RL, Skinner MK. Environmental epigenomics and disease susceptibility.
Nat Rev Genet. 2007;8:253�62.
40. Morgan HD, Sutherland HG, Martin DI, Whitelaw E. Epigenetic inheritance at
the agouti locus in the mouse. Nat Genet. 1999;23:314�8.
41. Cropley JE, Suter CM, Beckman KB, Martin DI. Germ-line epigenetic
modification of the murine A vy allele by nutritional supplementation. Proc
Natl Acad Sci U S A. 2006;103:17308�12.
42. Hoile SP, Lillycrop KA, Thomas NA, Hanson MA, Burdge GC. Dietary protein
restriction during F0 pregnancy in rats induces transgenerational changes in
the hepatic transcriptome in female offspring. PLoS One. 2011;6, e21668.
43. Multhaup ML, Seldin MM, Jaffe AE, Lei X, Kirchner H, Mondal P, et al. Mousehuman
experimental epigenetic analysis unmasks dietary targets and
genetic liability for diabetic phenotypes. Cell Metab. 2015;21:138�49.
44. Michels KB, Binder AM, Dedeurwaerder S, Epstein CB, Greally JM, Gut I, et al.
Recommendations for the design and analysis of epigenome-wide
association studies. Nat Methods. 2013;10:949�55.
45. Dayeh TA, Olsson AH, Volkov P, Almgren P, R�nn T, Ling C. Identification of
CpG-SNPs associated with type 2 diabetes and differential DNA methylation
in human pancreatic islets. Diabetologia. 2013;56:1036�46.
46. Relton CL, Davey Smith G. Two-step epigenetic Mendelian randomization: a
strategy for establishing the causal role of epigenetic processes in pathways
to disease. Int J Epidemiol. 2012;41:161�76.
47. Liu Y, Aryee MJ, Padyukov L, Fallin MD, Hesselberg E, Runarsson A, et al.
Epigenome-wide association data implicate DNA methylation as an
intermediary of genetic risk in rheumatoid arthritis. Nat Biotechnol.
2013;31:142�7.
48. Yuan W, Xia Y, Bell CG, Yet I, Ferreira T, Ward KJ, et al. An integrated
epigenomic analysis for type 2 diabetes susceptibility loci in monozygotic
twins. Nat Commun. 2014;5:5719.
49. Nitert MD, Dayeh T, Volkov P, Elgzyri T, Hall E, Nilsson E, et al. Impact of an
exercise intervention on DNA methylation in skeletal muscle from firstdegree
relatives of patients with type 2 diabetes. Diabetes. 2012;61:3322�32.
50. Gagnon F, A�ssi D, Carri� A, Morange P-E, Tr�gou�t D-A. Robust validation of
methylation levels association at CPT1A locus with lipid plasma levels.
J Lipid Res. 2014;55:1189�91.
51. Demerath EW, Guan W, Grove ML, Aslibekyan S, Mendelson M, Zhou Y-H,
et al. Epigenome-wide association atudy (EWAS) of BMI, BMI change, and
waist circumference in African American adults identifies multiple replicated
loci. Hum Mol Genet. 2015:ddv161�.
52. Dick KJ, Nelson CP, Tsaprouni L, Sandling JK, A�ssi D, Wahl S, et al. DNA
methylation and body-mass index: a genome-wide analysis. Lancet.
2014;6736:1�9.
53. Su S, Zhu H, Xu X, Wang X, Dong Y, Kapuku G, et al. DNA methylation of
the LY86 gene is associated with obesity, insulin resistance, and
inflammation. Twin Res Hum Genet. 2014;17:183�91.
54. Clarke-Harris R, Wilkin TJ, Hosking J, Pinkney J, Jeffery AN, Metcalf BS, et al.
PGC1? promoter methylation in blood at 5�7 years predicts adiposity from
9 to 14 years (EarlyBird 50). Diabetes. 2014;63:2528�37.
55. Guay S-P, Brisson D, Lamarche B, Biron S, Lescelleur O, Biertho L, et al.
ADRB3 gene promoter DNA methylation in blood and visceral adipose
tissue is associated with metabolic disturbances in men. Epigenomics.
2014;6:33�43.
56. Agha G, Houseman EA, Kelsey KT, Eaton CB, Buka SL, Loucks EB. Adiposity is
associated with DNA methylation profile in adipose tissue. Int J Epidemiol.
2014:1�11.
57. Irvin MR, Zhi D, Joehanes R, Mendelson M, Aslibekyan S, Claas SA, et al.
Epigenome-wide association study of fasting blood lipids in the genetics of
lipid-lowering drugs and diet network study. Circulation. 2014;130:565�72.
58. Frazier-Wood AC, Aslibekyan S, Absher DM, Hopkins PN, Sha J, Tsai MY, et al.
Methylation at CPT1A locus is associated with lipoprotein subfraction
profiles. J Lipid Res. 2014;55:1324�30.
59. Pfeifferm L, Wahl S, Pilling LC, Reischl E, Sandling JK, Kunze S, et al. DNA
methylation of lipid-related genes affects blood lipid levels. Circ Cardiovasc
Genet. 2015.
60. Petersen A-K, Zeilinger S, Kastenm�ller G, R�misch-Margl W, Brugger M, Peters
A, et al. Epigenetics meets metabolomics: an epigenome-wide association
study with blood serum metabolic traits. Hum Mol Genet. 2014;23:534�45.
61. Hidalgo B, Irvin MR, Sha J, Zhi D, Aslibekyan S, Absher D, et al. Epigenomewide
association study of fasting measures of glucose, insulin, and HOMA-IR
in the genetics of lipid lowering drugs and diet network study. Diabetes.
2014;63:801�7.
62. Dayeh T, Volkov P, Sal� S, Hall E, Nilsson E, Olsson AH, et al. Genome-wide
DNA methylation analysis of human pancreatic islets from type 2 diabetic
and non-diabetic donors identifies candidate genes that influence insulin
secretion. PLoS Genet. 2014;10, e1004160.
63. Nilsson E, Jansson PA, Perfilyev A, Volkov P, Pedersen M, Svensson MK, et al.
Altered DNA methylation and differential expression of genes influencing
metabolism and inflammation in adipose tissue from subjects with type 2
diabetes. Diabetes. 2014;63:2962�76.
64. Benton MC, Johnstone A, Eccles D, Harmon B, Hayes MT, Lea RA, et al. An analysis of DNA methylation in human adipose tissue reveals differential modification of obesity genes before and after gastric bypass and weight
loss. Gene. 2015;16:1�21.
65. Bateson P, Gluckman P. Plasticity and robustness in development and
evolution. Int J Epidemiol. 2012;41:219�23.
66. Feinberg AP, Irizarry RA, Feinberg AP, Irizarry RA. Evolution in health and
medicine Sackler colloquium: stochastic epigenetic variation as a driving
force of development, evolutionary adaptation, and disease. Proc Natl Acad
Sci U S A. 2010;107(Suppl):1757�64.
67. Martino D, Loke YJ, Gordon L, Ollikainen M, Cruickshank MN, Saffery R, et al.
Longitudinal, genome-scale analysis of DNA methylation in twins from birth
to 18 months of age reveals rapid epigenetic change in early life and pairspecific
effects of discordance. Genome Biol. 2013;14:R42.
68. Tobi EW, Goeman JJ, Monajemi R, Gu H, Putter H, Zhang Y, et al. DNA
methylation signatures link prenatal famine exposure to growth and
metabolism. Nat Commun. 2014;5:5592.
69. Dominguez-Salas P, Moore SE, Baker MS, Bergen AW, Cox SE, Dyer RA, et al.
Maternal nutrition at conception modulates DNA methylation of human
metastable epialleles. Nat Commun. 2014;5:3746.
70. Quilter CR, Cooper WN, Cliffe KM, Skinner BM, Prentice PM, Nelson L, et al.
Impact on offspring methylation patterns of maternal gestational diabetes
mellitus and intrauterine growth restraint suggest common genes and
pathways linked to subsequent type 2 diabetes risk. FASEB J. 2014:1�12.
71. Morales E, Groom A, Lawlor DA, Relton CL. DNA methylation signatures in
cord blood associated with maternal gestational weight gain: results from
the ALSPAC cohort. BMC Res Notes. 2014;7:278.
72. Ruchat SM, Houde AA, Voisin G, St-Pierre J, Perron P, Baillargeon JP, et al.
Gestational diabetes mellitus epigenetically affects genes predominantly
involved in metabolic diseases. Epigenetics. 2013;8:935�43.
73. Liu X, Chen Q, Tsai H-J, Wang G, Hong X, Zhou Y, et al. Maternal
preconception body mass index and offspring cord blood DNA
methylation: exploration of early life origins of disease. Environ Mol
Mutagen. 2014;55:223�30.
74. Soubry A, Murphy SK, Wang F, Huang Z, Vidal AC, Fuemmeler BF, et al.
Newborns of obese parents have altered DNA methylation patterns at
imprinted genes. Int J Obes (Lond). 2015;39:650�7.
75. Jacobsen SC, Br�ns C, Bork-Jensen J, Ribel-Madsen R, Yang B, Lara E, et al.
Effects of short-term high-fat overfeeding on genome-wide DNA
methylation in the skeletal muscle of healthy young men. Diabetologia.
2012;55:3341�9.
76. Gillberg L, Jacobsen SC, R�nn T, Br�ns C, Vaag A. PPARGC1A DNA
methylation in subcutaneous adipose tissue in low birth weight subjects�
impact of 5 days of high-fat overfeeding. Metabolism. 2014;63:263�71.
77. Huang Y-T, Maccani JZJ, Hawley NL, Wing RR, Kelsey KT, McCaffery JM.
Epigenetic patterns in successful weight loss maintainers: a pilot study. Int J
Obes (Lond). 2015;39:865�8.
78. Barres R, Kirchner H, Rasmussen M, Yan J, Kantor FR, Krook A, N�slund E,
Zierath JR. Weight loss after gastric bypass surgery in human obesity
remodels promoter methylation. Cell Rep. 2013:1�8.
79. Ahrens M, Ammerpohl O, von Sch�nfels W, Kolarova J, Bens S, Itzel T, et al.
DNA methylation analysis in nonalcoholic fatty liver disease suggests
distinct disease-specific and remodeling signatures after bariatric surgery.
Cell Metab. 2013;18:296�302.
80. Voisin S, Eynon N, Yan X, Bishop DJ. Exercise training and DNA methylation
in humans. Acta Physiol (Oxf). 2014;213:39�59.
81. Lindholm ME, Marabita F, Gomez-Cabrero D, Rundqvist H, Ekstr�m TJ,
Tegn�r J, et al. An integrative analysis reveals coordinated reprogramming
of the epigenome and the transcriptome in human skeletal muscle after
training. Epigenetics. 2014;9:1557�69.
82. Denham J, O�Brien BJ, Marques FZ, Charchar FJ. Changes in the leukocyte
methylome and its effect on cardiovascular related genes after exercise.
J Appl Physiol. 2014:jap.00878.2014.
83. Rowlands DS, Page RA, Sukala WR, Giri M, Ghimbovschi SD, Hayat I, et al.
Multi-omic integrated networks connect DNA methylation and miRNA with
skeletal muscle plasticity to chronic exercise in type 2 diabetic obesity.
Physiol Genomics. 2014;46:747�65.
84. Horvath S, Erhart W, Brosch M, Ammerpohl O, von Schonfels W, Ahrens M,
et al. Obesity accelerates epigenetic aging of human liver. Proc Natl Acad
Sci. 2014;111:15538�43.
85. Alm�n MS, Nilsson EK, Jacobsson JA, Kalnina I, Klovins J, Fredriksson R, et al.
Genome-wide analysis reveals DNA methylation markers that vary with
both age and obesity. Gene. 2014.;548:61�7
86. Houseman EA, Molitor J, Marsit CJ. Reference-free cell mixture adjustments
in analysis of DNA methylation data. Bioinformatics. 2014;30:1431�9.
87. Wells JC. A critical appraisal of the predictive adaptive response hypothesis.
Int J Epidemiol. 2012;41:229�35.
88. Williams-Wyss O, Zhang S, MacLaughlin SM, Kleemann D, Walker SK, Suter
CM, et al. Embryo number and periconceptional undernutrition in the
sheep have differential effects on adrenal epigenotype, growth, and
development. Am J Physiol Endocrinol Metab. 2014;307:E141�50.
89. Zhang S, Rattanatray L, Morrison JL, Nicholas LM, Lie S, McMillen IC.
Maternal obesity and the early origins of childhood obesity: weighing up
the benefits and costs of maternal weight loss in the periconceptional
period for the offspring. Exp Diabetes Res. 2011;2011:585749.
90. Zhang S, Williams-Wyss O, MacLaughlin SM, Walker SK, Kleemann DO, Suter
CM, et al. Maternal undernutrition during the first week after conception
results in decreased expression of glucocorticoid receptor mRNA in the
absence of GR exon 17 hypermethylation in the fetal pituitary in late
gestation. J Dev Orig Heal Dis. 2013;4:391�401.
91. Lie S, Morrison JL, Williams-Wyss O, Suter CM, Humphreys DT, Ozanne SE,
et al. Periconceptional undernutrition programs changes in insulin-signaling
molecules and microRNAs in skeletal muscle in singleton and twin fetal
sheep. Biol Reprod. 2014;90:5.
92. Van Straten EM, van Meer H, Huijkman NC, van Dijk TH, Baller JF, Verkade
HJ, et al. Fetal liver X receptor activation acutely induces lipogenesis but
does not affect plasma lipid response to a high-fat diet in adult mice. Am J
Physiol Endocrinol Metab. 2009;297:E1171�8.
93. Fernandez-Twinn DS, Alfaradhi MZ, Martin-Gronert MS, Duque-Guimaraes
DE, Piekarz A, Ferland-McCollough D, et al. Downregulation of IRS-1 in
adipose tissue of offspring of obese mice is programmed cellautonomously
through post-transcriptional mechanisms. Mol Metab.
2014;3:325�33.
94. Waterland RA, Travisano M, Tahiliani KG. Diet-induced hypermethylation at
agouti viable yellow is not inherited transgenerationally through the female.
FASEB J. 2007;21:3380�5.
95. Ge ZJ, Luo SM, Lin F, Liang QX, Huang L, Wei YC, et al. DNA methylation in
oocytes and liver of female mice and their offspring: effects of high-fat-dietinduced
obesity. Env Heal Perspect. 2014;122:159�64.
96. Ollikainen M, Ismail K, Gervin K, Kyll�nen A, Hakkarainen A, Lundbom J, et al.
Genome-wide blood DNA methylation alterations at regulatory elements
and heterochromatic regions in monozygotic twins discordant for obesity
and liver fat. Clin Epigenetics. 2015;7:1�13.
Thyroid disease is a common problem that can cause symptoms because of over- or under-function of the thyroid gland. The thyroid gland is located in the front of the neck below the Adam’s apple. The thyroid gland is an essential organ for producing thyroid hormones, which maintain are body metabolism.
Do I have a thyroid disease?
This is the common question many individuals ask, seeking for an answer from a healthcare professional. Grave’s disease, a sort of thyroid autoimmunity disease, has been illustrated to be caused by the following factors. Please note not all of these factors are treatable. From those, the factors that are treatable and most important are:
Selenium deficiencies
Infections
Stress
Gluten
Vitamin Deficiencies
Vitamin D, omega-3, folate
Gut Microflora
Leaky gut
Infections
Many different viruses and bacteria have been associated with autoimmunity. Some of the very researched are:
Bacteria:
Yersinia enterocolitis
Helicobacter pylori
Viruses:
Epstein Barr
Cytomegalovirus
Herpes Simplex Virus
This has caused researchers to recognize those infections as one of the contributors to developing autoimmunity. A number of studies have even shown as disease activity increases, so does the severity of the autoimmune process.
A meta analysis examining the association of H. Pylori infections and thyroid autoimmunity concluded, “Overall, H. pylori infection was associated with autoimmune thyroid disease; the association was significant for Graves’ disease. These findings indicate that H. pylori infection potentially plays a part in the progression of ATDs.” ATD signifies autoimmune thyroid disease (Hashimoto’s thyroid disease and Graves’ disease being the most common forms).
Three case studies were published showing that all three women with Graves’ had concurrent Epstein Barr virus reactivation. Note severe Epstein Barr is also known as mononucleosis.
“Though the etiology of Graves’ disease is still not clear, it is generally implied that environmental factors such as infections contribute to the growth of Graves’ disease. We report here three cases of Graves’ disease which presented simultaneously with infectious mononucleosis due to primary EBV infection.”
Some researchers’re theorizing the reason why Epstein Barr virus might lead to autoimmunity is essentially because the virus really gets inside the thyroid gland thus stimulating your immune cells to attack the gland.
While there are great studies demonstrating the correlation between infections and autoimmunity; and there is a suggested causal connection, researchers are still lacking further information. Released studies demonstrating a decrease of activity are impressive although sparse.
A study was conducted in Italy that exemplified how effective treatment of infections can be in halting the autoimmune procedure. Ten patients that had Hashimoto’s thyroid disease and also had an H. Pylori infection were chosen. Five failed treatment procedures and five responded well to the treatment procedures.
Again, the patients all had thyroid disorder and a H. Pylori bacterial disease. All of the patients’ levels were elevated to begin with, however. Treating a disease helped to stop the autoimmune process that damages the thyroid gland.
How important are the anti-body amounts?
A large study, known as meta-analyses, revealed that high antibodies levels are predictive of Graves’ relapse; so whatever we can do to lower these antibodies will be a good idea.
While there may not yet be some substantial scale randomized control trials looking at this, there are various clinicians in the area, that report that screening for and treating such infections seems to contribute greatly to halting the autoimmune procedure. It is a very simple inference to draw that removing a pathogenic bacteria overgrowth like Helicobacter Pylori, can be beneficial. Remember Graves and Hashimoto’s’ are immune disorders, infections trigger activation of the immune system allows the immune system to relax.
The H. Pylori Infection was shown to cause stomach burning, inflammation and nausea. Luckily, H. Pylori and many of these other infections can be safely eradicated with a class of antibiotic herbs. So there is great reason to screen for and treat those infections especially when we know for certain they have a strong connection. Most every infection will cause fatigue and treating an infection will help with sufferers energy levels.
Leaky Gut
The topic of infections ties in with that of gut health. Why is this? Well, a number of these infections can dwell therefore that they act not only as an infection which stimulated the immune systems but also damages your gut. H. Pylori and Yersinia are just two examples of these.
Why is gut health connected to my thyroid gland? Some researchers have stated that it is not even possible to develop autoimmunity unless the gut is first damaged. But why exactly is that?
This is because the gut is the barrier between you and the outside world. Remember ‘stuff’ from the external world increases entry therefore we need to have plenty of border patrol bronchial cells. When you have ‘leaky gut’ that the intestine or boarder barrier is compromised and also much ‘stuff’ is permitted in. This stuff may be viruses, bacteria, fungus, food particles, chemicals, etc.. Therefore, if you’ve got an underlying predisposition to autoimmunity and you then create leaky gut, the point may be set for you to develop autoimmunity, or specifically Graves’.
Gut Microflora
Here is a very simplified overview of a very exciting and complex subject. Good bacteria and fungus live in your intestines, more so on your colon. They are essential to help crowd out the bad bacteria, fungus and other infections. They are needed to prevent gut issues. Additionally they help increase nutrient absorption and breakdown nutrients. As though this isn’t sufficient, the microflora has been shown to have a direct effect on particular types of autoimmunity.
At a 2012 review published in the International Journal of Immunopathology and Pharmacology the authors remarked, “Alterations in both the structure and function of intestinal microbiota could be one of the typical causative triggers of esophageal or autoinflammatory disorders.”
Dr. David Brady, ND, DC recorded a very well referenced lecture going into great detail about the gut microflora-autoimmune connection. Brady does a great job covering the way the medical literature shows a strong association between autoimmunity and gut flora. This is mentioned in practice.
Stress
Stress in known to provocate almost any health complication. The consequences of stress are far reaching, but stress can impact Graves’ via two mechanisms. Stress can weaken your immune system, which can cause an illness you already have to become much more debatable or may make you more susceptible to acquiring an infection. Second, we also understand that stress modulates what’s called the balance in the immune system. Among the theories of autoimmunity indicates that a change in this balance is a predisposing factor to growing.
Gluten
Gluten intolerance might be connected to pancreatic gland, and especially Graves’ disease by way of a gene or genes. There is known as the CLTA-4 gene, a gene known to be related to Graves’.
A study printed in 2012 revealed that 60 percent of those with AIT (autoimmune thyroid) disorder had this gene, while just 25 percent of healthy controls had this gene. How can this link to gluten intolerance? In 2013 that a meta-analysis was published showing a link between the CTLA-4 receptor as well as celiac disease, celiac disease being the maximum level of gluten intolerance one can have. These finding are confirmed in other reviews too.
Other studies, in Hashimoto’s patients, have shown that a gluten free diet can decrease the need for drugs and interrupts the gastrointestinal attack. Irrespective of the specific gene or genes involvement, observational data is fairly clear that people who have celiac disease have a higher prevalence of autoimmune thyroid disease (Graves’ and Hashimoto’s). Now it is important to mention that there’s an increasing subset of our population that doesn’t have full blown celiac disease but does have what is known as ‘gluten intolerance’. Current clinical studies support the idea that those with ‘gluten intolerance’ may also derive health benefit from a gluten free diet.
Vitamin Deficiencies
Vitamin D
It’s becoming increasingly more agreed upon that vitamin D helps fight autoimmunity to a lesser or greater degree. Lets look at a few information. A 2012 study published in the journal Endocrine revealed that individuals who relapse after Graves’ therapy have lower vitamin D levels, while those who do not snore have high levels of vitamin D.
Interestingly other studies are suggesting that autoimmunity may be because of defects in the vitamin D receptor consequently producing the vitamin D in your body less powerful. A 2013 study performed in Turkey showed that a specific flaw in the vitamin D receptor left patients at greater risk for Hashimoto’s thyroid autoimmunity. Along these very same lines, certain viral diseases might actually block the vitamin D receptor, which might be another mechanism whereby chronic infections lead to autoimmunity.
Omega 3’s
Omega 3 fatty acids have become a significant dietary and supplemental factors since they’ve become deficient in the diet in industrialized nations. Omega 3’s serve numerous functions, regarding the function they confer is their impact on inflammation.
Every cell of your body has a coating around it know as a cell membrane. The cell membrane is comprised of fatty acids. If the cell membrane is composed of a lot of omega 6 and not enough omega 3 fats, then the cell is prone in inflammation. Increasing consumption of omega 3s can help make you susceptible to autoimmunity and inflammation and also restore balance to your cell membranes. But how can inflammation tie in with autoimmunity? Remember among the hallmarks of autoimmunity is to overzealous immune reaction. Your entire body mounts an immune response by sending out white blood cells which shoot inflammation at ‘guys’ to destroy them. This is great when it is controlled, but out of control the procedure rages also in people with autoimmunity. Restoring levels of omega 3s is like taking bullets from your systems guns preventing your system. Please remember its all about balance and over consumption of omega 3s may cause difficulties like a intake.
There’s a wealth of data available on the health benefits of omega 3s. Merely to quote 1 study regarding omega 3s effect on autoimmunity, the available evidence reveal that increased daily consumption of dietary n-3 FA reduces the severity of autoimmune disorders.”
Folate/MTHFR
Some individuals have a gene mutation referred to as the MTHFR mutation. Basically this mutation reduces one’s ability to break down acid. Folic acid is a synthetic form of the vitamin. Because food processing hurts folate, the synthetic form (folic acid), is added back to our meals. Patients with this gene mutation cannot absorb folic acid plus they become deficient in this vitamin.
Data on this subject is sparse and I wonder if treating this particular gene mutation will have any significant impact on thyroid autoimmunity. Some studies show an association for this mutation and autoimmune thyroid; one study showed that 30 percent of autoimmune thyroid patients had the MTHFR gene mutation.
Yet other studies show no correlation for this particular gene mutation and thyroid autoimmunity. Curing this gene polymorphism is safe and inexpensive as the treatment is through vitamin and diet treatment. If your functional medicine practitioner is up to date on this subject, even though this might not be the first item it may be worthwhile to explore this with your health care provider to achieve overall health and wellness.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Nutrition�Abstract: A number of factors contribute to success in sport, and diet is a key component. An athlete�s dietary requirements depend on several aspects, including the sport, the athlete�s goals, the environment, and practical issues. The importance of individualized dietary advice has been increasingly recognized, including day-to-day dietary advice and specific advice before, during, and after training and/or competition. Athletes use a range of dietary strategies to improve performance, with maximizing glycogen stores a key strategy for many. Carbohydrate intake during exercise maintains high levels of carbohydrate oxidation, prevents hypoglycemia, and has a positive effect on the central nervous system. Recent research has focused on athletes training with low carbohydrate availability to enhance metabolic adaptations, but whether this leads to an improvement in performance is unclear. The benefits of protein intake throughout the day following exercise are now well recognized. Athletes should aim to maintain adequate levels of hydration, and they should minimize fluid losses during exercise to no more than 2% of their body weight. Supplement use is widespread in athletes, with recent interest in the beneficial effects of nitrate, beta-alanine, and vitamin D on performance. However, an unregulated supplement industry and inadvertent contamination of supplements with banned substances increases the risk of a positive doping result. Although the availability of nutrition information for athletes varies, athletes will bene t from the advice of a registered dietician or nutritionist.
Introduction To The Importance & Influence Of Nutrition On Exercise
Nutrition is increasingly recognized as a key component of optimal sporting performance, with both the science and practice of sports nutrition developing rapidly.1 Recent studies have found that a planned scientific nutritional strategy (consisting of fluid, carbohydrate, sodium, and caffeine) compared with a self-chosen nutritional strategy helped non-elite runners complete a marathon run faster2 and trained cyclists complete a time trial faster.3 Whereas training has the greatest potential to increase performance, it has been estimated that consumption of a carbohydrate�electrolyte drink or relatively low doses of caffeine may improve a 40 km cycling time trial performance by 32�42 and 55�84 seconds, respectively.4
Evidence supports a range of dietary strategies in enhancing sports performance. It is likely that combining several strategies will be of greater bene t than one strategy in isolation.5 Dietary strategies to enhance performance include optimizing intakes of macronutrients, micronutrients, and fluids, including their composition and spacing throughout the day. The importance of individualized or personalized dietary advice�is becoming increasingly recognized,6 with dietary strategies varying according to the individual athlete�s sport, personal goals, and practicalities (eg, food preferences). �Athlete� includes individuals competing in a range of sport types, such as strength and power (eg, weight-lifting), team (eg, football), and endurance (eg, marathon running). The use of dietary supplements can enhance performance, provided these are used appropriately. This manuscript provides an overview of dietary strategies used by athletes, the efficacy of these strategies, availability of nutrition information to athletes, and risks associated with dietary supplement intake.
Review Of Diet Strategies Employed By Athletes
Maximizing Muscle Glycogen Stores Prior To Exercise
Carbohydrate loading aims to maximize an athlete�s muscle glycogen stores prior to endurance exercise lasting longer than 90 minutes. Benefits include delayed onset of fatigue (approximately 20%) and improvement in performance of 2%�3%.7 Initial protocols involved a depletion phase (3 days of intense training and low carbohydrate intake) followed by a loading phase (3 days of reduced training and high carbo- hydrate intake).8,9 Further research showed muscle glycogen concentrations could be enhanced to a similar level without the glycogen-depletion phase,10 and more recently, that 24 hours may be sufficient to maximize glycogen stores.11,12 Current recommendations suggest that for sustained or intermittent exercise longer than 90 minutes, athletes should consume 10�12 g of carbohydrate per kg of body mass (BM) per day in the 36�48 hours prior to exercise.13
There appears to be no advantage to increasing pre- exercise muscle glycogen content for moderate-intensity cycling or running of 60�90 minutes, as signi cant levels of glycogen remain in the muscle following exercise.7 For exercise shorter than 90 minutes, 7�12 g of carbohydrate/kg of BM should be consumed during the 24 hours preceding.13 Some14,15 but not all16 studies have shown enhanced performance of intermittent high-intensity exercise of 60�90 minutes with carbohydrate loading.
Carbohydrate eaten in the hours prior to exercise (com- pared with an overnight fast) has been shown to increase muscle glycogen stores and carbohydrate oxidation,17 extend cycle time to exhaustion,5 and improve exercise performance.5,18 Specific recommendations for exercise of longer than 60 minutes include 1�4 g of carbohydrate/kg of BM in the 1�4 hours prior.13 Most studies have not found improvements in performance from consuming low glycemic�index (GI) foods prior to exercise.19 Any metabolic or performance effects from low GI foods appear to be attenuated when carbohydrate is consumed during exercise.20,21
Carbohydrate Intake During The Event
Carbohydrate ingestion has been shown to improve performance in events lasting approximately 1 hour.6 A growing body of evidence also demonstrates beneficial effects of a carbohydrate mouth rinse on performance.22 It is thought that receptors in the oral cavity signal to the central nervous system to positively modify motor output.23
In longer events, carbohydrate improves performance primarily by preventing hypoglycemia and maintaining high levels of carbohydrate oxidation.6 The rate of exogenous carbohydrate oxidation is limited by the small intestine�s ability to absorb carbohydrate.6 Glucose is absorbed by the sodium- dependent transporter (SGLT1), which becomes saturated with an intake of approximately 1 g/minute. The simultaneous ingestion of fructose (absorbed via glucose transporter 5�[GLUT5]), enables oxidation rates of approximately 1.3 g/minute,24 with performance benefits apparent in the third hour of exercise.6 Recommendations reflect this, with 90 g of carbohydrate from multiple sources recommended for events longer than 2.5 hours, and 60 g of carbohydrate from either single or multiple sources recommended for exercise of 2�3 hours� duration (Table 1). For slower athletes exercising at a lower intensity,�carbohydrate requirements will be less due to lower carbohydrate oxidation.6 Daily training with high carbohydrate availability has been shown to increase exogenous carbohydrate oxidation rates.25
The �Train-Low, Compete-High� Approach
The �train-low, compete-high� concept is training with low carbohydrate availability to promote adaptations such as�enhanced activation of cell-signaling pathways, increased mitochondrial enzyme content and activity, enhanced lipid oxidation rates, and hence improved exercise capacity.26 However, there is no clear evidence that performance is improved with this approach.27 For example, when highly trained cyclists were separated into once-daily (train-high) or twice-daily (train-low) training sessions, increases in resting muscle glycogen content were seen in the low-carbohydrate- availability group, along with other selected training adaptations.28 However, performance in a 1-hour time trial after 3 weeks of training was no different between groups. Other research has produced similar results.29 Different strategies have been suggested (eg, training after an overnight fast, training twice per day, restricting carbohydrate during recovery),26 but further research is needed to establish optimal dietary periodization plans.27
Fat As A Fuel During Endurance Exercise
There has been a recent resurgence of interest in fat as a fuel, particularly for ultra endurance exercise. A high-carbohydrate strategy inhibits fat utilization during exercise,30 which may not be beneficial due to the abundance of energy stored in the body as fat. Creating an environment that optimizes fat oxidation potentially occurs when dietary carbohydrate is reduced to a level that promotes ketosis.31 However, this strategy may impair performance of high-intensity activity, by contributing to a reduction in pyruvate dehydrogenase activity and glycogenolysis. 32 The lack of performance benefits seen in studies investigating �high-fat� diets may be attributed to inadequate carbohydrate restriction and time for adaptation.31 Research into the performance effects of high fat diets continues.
Nutrition: Protein
While protein consumption prior to and during endurance and resistance exercise has been shown to enhance rates of muscle protein synthesis (MPS), a recent review found protein ingestion alongside carbohydrate during exercise does not improve time�trial performance when compared with the ingestion of adequate amounts of carbohydrate alone.33
Fluid And Electrolytes
The purpose of fluid consumption during exercise is primarily to maintain hydration and thermoregulation, thereby benefiting performance. Evidence is emerging on increased risk of oxidative stress with dehydration.34 Fluid consumption prior to exercise is recommended to ensure that the athlete is well-hydrated prior to commencing exercise.35 In addition,�carefully planned hyperhydration ( fluid overloading) prior to an event may reset fluid balance and increase fluid retention, and consequently improve heat tolerance.36 However, fluid overloading may increase the risk of hyponatremia 37 and impact negatively on performance due to feelings of fullness and the need to urinate.
Hydration requirements are closely linked to sweat loss, which is highly variable (0.5�2.0 L/hour) and dependent on type and duration of exercise, ambient temperature, and athletes� individual characteristics.35 Sodium losses linked to high temperature can be substantial, and in events of long duration or in hot temperatures, sodium must be replaced along with fluid to reduce risk of hyponatremia. 35
It has long been suggested that fluid losses greater than 2% of BM can impair performance,35 but there is controversy over the recommendation that athletes maintain BM by fluid ingestion throughout an event.37 Well-trained athletes who �drink to thirst� have been found to lose as much as 3.1% of BM with no impairment of performance in ultra-endurance events.38 Ambient temperature is important, and a review illustrated that exercise performance was preserved if loss was restricted to 1.8% and 3.2% of BM in hot and temperate conditions, respectively.39
Dietary Supplementation: Nitrates, Beta-Alanine & Vitamin D
Performance supplements shown to enhance performance include caffeine, beetroot juice, beta-alanine (BA), creatine, and bicarbonate.40 Comprehensive reviews on other supplements including caffeine, creatine, and bicarbonate can be found elsewhere.41 In recent years, research has focused on the role of nitrate, BA, and vitamin D and performance. Nitrate is most commonly provided as sodium nitrate or beetroot juice.42 Dietary nitrates are reduced (in mouth and stomach) to nitrites, and then to nitric oxide. During exercise, nitric oxide potentially influences skeletal muscle function through regulation of blood ow and glucose homeostasis, as well as mitochondrial respiration.43 During endurance exercise, nitrate supplementation has been shown to increase exercise efficiency (4%�5% reduction in VO at a steady attenuate oxidative stress.42 Similarly, a 4.2% improvement in performance was shown in a test designed to simulate a football game.44
BA is a precursor of carnosine, which is thought to have a number of performance-enhancing functions including the reduction of acidosis, regulation of calcium, and antioxidant properties.45 Supplementation with BA has been shown to�2�state; 0.9% improvement in time trials), reduce fatigue, and�augment intracellular carnosine concentration.45 A systematic review concluded that BA may increase power output and working capacity and decrease feelings of fatigue, but that there are still questions about safety. The authors suggest caution in the use of BA as an ergogenic aid.46
Vitamin D is essential for the maintenance of bone health and control of calcium homeostasis, but is also important for muscle strength,47,48 regulation of the immune system,49 and cardiovascular health.50 Thus inadequate vitamin D status has potential implications for the overall health of athletes and performance. A recent review found that the vitamin D status of most athletes reflects that of the population in their locality, with lower levels in winter, and athletes who train predominantly indoors are at greater risk of deficiency.51 There are no dietary vitamin D recommendations for athletes; however, for muscle function, bone health, and avoidance of respiratory infections, current evidence supports maintenance of serum 25-hydroxy vitamin D (circulating form) concentrations of 80�100 nmol/L.51
Diets Specific For Post Exercise
Recovery from a bout of exercise is integral to the athlete�s training regimen. Without adequate recovery of carbohydrate, protein, fluids, and electrolytes, beneficial adaptations and performance may be hampered.
Muscle Glycogen Synthesis
Consuming carbohydrates immediately post exercise to coincide with the initial rapid phase of glycogen synthesis has been used as a strategy to maximize rates of muscle glycogen synthesis. An early study found delaying feeding by 2 hours after glycogen-depleting cycling exercise reduced glycogen synthesis rates.52 However the importance of this early enhanced rate of glycogen synthesis has been questioned in the context of extended recovery periods with sufficient carbohydrate consumption. Enhancing the rate of glycogen synthesis with immediate carbohydrate consumption after exercise appears most relevant when the next exercise session is within 8 hours of the first.53,54 Feeding frequency is also irrelevant with extended recovery; by 24 hours post exercise, consumption of carbohydrate as four large meals or 16 small snacks had comparable effects on muscle glycogen storage.55
With less than 8 hours between exercise sessions, it is recommended that for maximal glycogen synthesis, 1.0�1.2 g/kg/hour is consumed for the first 4 hours, followed by resumption of daily carbohydrate requirements.13 Additional protein has been shown to enhance glycogen�synthesis rates when carbohydrate intake is suboptimal.56 The consumption of moderate to high GI foods post exercise is recommended;13 however, when either a high-GI or low-GI meal was consumed after glycogen-depleting exercise, no performance differences were seen in a 5 km cycling time trial 3 hours later.57
Muscle Protein Synthesis
An acute bout of intense endurance or resistance exercise can induce a transient increase in protein turnover, and, until feeding, protein balance remains negative. Protein consumption after exercise enhances MPS and net protein balance,58 predominantly by increasing mitochondrial protein fraction with endurance training, and myofibrillar protein fraction with resistance training.59
Only a few studies have investigated the effect of timing of protein intake post exercise. No significant difference in MPS was observed over 4 hours post exercise when a mixture of essential amino acids and sucrose was fed 1 hour versus 3 hours after resistance exercise.60 Conversely, when a protein and carbohydrate supplement was provided immediately versus 3 hours after cycling exercise, leg protein synthesis increased threefold over 3 hours.61 A meta-analysis found timed post exercise protein intake becomes less important with longer recovery periods and adequate protein intake,62 at least for resistance training.
Dose�response studies suggest approximately 20 g of high-quality protein is sufficient to maximize MPS at rest,63 following resistance,63,64 and after high-intensity aerobic exercise.65 Rate of MPS has been found to approximately triple 45�90 minutes after protein consumption at rest, and then return to baseline levels, even with continued availability of circulating essential amino acids (termed the �muscle full� effect).66 Since exercise-induced protein synthesis is elevated for 24�48 hours following resistance exercise67and 24�28 hours following high-intensity aerobic exercise,68 and feeding protein post exercise has an additive effect,58,64 then multiple feedings over the day post exercise might maximize muscle growth. In fact, feeding 20 g of whey protein every 3 hours was subsequently found to maximally stimulate muscle myofibrillar protein synthesis following resistance exercise.69,70
In resistance training, where post exercise intake of protein was balanced by protein intake later in the day, increased adaptation of muscle hypertrophy resulted in equivocal strength performance effects.71,72 Most studies have not found a subsequent bene t to aerobic performance with post exercise protein consumption.73,74 However, in two�well controlled studies in which post exercise protein intake was balanced by protein intake later in the day, improvements were seen in cycling time to exhaustion75 and in cycling sprint performance.76
Fluids And Electrolyte Balance
Fluid and electrolyte replacement after exercise can be achieved through resuming normal hydration practices. However, when euhydration is needed within 24 hours or substantial body weight has been lost (.5% of BM), a more structured response may be warranted to replace fluids and electrolytes.77
Availability Of Nutritional Information To Athletes At Varying Levels
The availability of nutrition information for athletes varies. Younger or recreational athletes are more likely to receive generalized nutritional information of poorer quality from individuals such as coaches.78 Elite athletes are more likely to have access to specialized sports-nutrition input from qualified professionals. A range of sports science and medicine support systems are in place in different countries to assist elite athletes,1 and nutrition is a key component of these services. Some countries have nutrition programs embedded within sports institutes (eg, Australia) or alternatively have National Olympic Committees that support nutrition programs (eg, United States of America).1 However, not all athletes at the elite level have access to sports-nutrition services. This may be due to financial constraints of the sport, geographical issues, and a lack of recognition of the value of a sports-nutrition service.78
Athletes eat several times per day, with snacks contributing to energy requirements.79 Dietary intake differs across sports, with endurance athletes more likely to achieve energy and carbohydrate requirements compared to athletes in weight-conscious sports.79 A review found daily intakes of carbohydrate were 7.6 g/kg and 5.7 g/kg of BM for male and female endurance athletes, respectively.80 Ten elite Kenyan runners met macronutrient recommendations but not guide- lines for fluid intake.81 A review of fluid strategies showed a wide variability of intake across sports, with several factors influencing intake, many outside the athlete�s control.82
Nutrition information may be delivered to athletes by a range of people (dietitians, nutritionists, medical practitioners, sports scientists, coaches, trainers) and from a variety of sources (nutrition education programs, sporting magazines, the media and Internet).83 Of concern is the provision of�nutrition advice from outside various professional�s scope of practice. For example, in Australia 88% of registered exercise professionals provided nutrition advice, despite many not having adequate nutrition training.84 A study of Canadian high-performance athletes from 34 sports found physicians ranked eighth and dietitians, 16th as choice of source of dietary supplement information.85
Risks Of Contravening The Doping Regulations
Supplement use is widespread in athletes.86,87 For example, 87.5% of elite athletes in Australia used dietary supplements88 and 87% of Canadian high-performance athletes took dietary supplements within the past 6 months85 (Table 2). It is difficult to compare studies due to differences in the criteria used to define dietary supplements, variations in assessing supplement intake, and disparities in the populations studied.85
Athletes take supplements for many reasons, including for proposed performance benefits, for prevention or treatment of a nutrient deficiency, for convenience, or due to fear of �missing out� by not taking a particular supplement.41
The potential benefits (eg, improved performance) of taking a dietary supplement must outweigh the risks.86,87 There are few permitted dietary supplements available that have an ergogenic effect.87,89 Dietary supplementation cannot compensate for poor food choices.87 Other concerns include lack of efficacy, safety issues (toxicity, medical concerns), negative nutrient interactions, unpleasant side effects, ethical issues, financial expense, and lack of quality control.41,86,87 Of major concern, is the consumption of prohibited substances by the World Anti-Doping Agency (WADA).
Inadequate regulation in the supplement industry (com- pounded by widespread Internet sales) makes it difficult for athletes to choose supplements wisely.41,86,87 In 2000�2001, a study of 634 different supplements from 13 countries found that 94 (14.8%) contained undeclared steroids, banned by WADA.90 Many contaminated supplements were routinely used by athletes (eg, vitamin and mineral supplements).86 Several studies have confirmed these findings. 41,86,89
A positive drug test in an athlete can occur with even a minute quantity of a banned substance.41,87 WADA maintains a �strict liability� policy, whereby every athlete is responsible for any substance found in their body regardless of how it got there.41,86,87,89 The World Anti-Doping Code (January 1, 2015) does recognize the issue of contaminated supplements.91 Whereas the code upholds the principle of strict liability, athletes may receive a lesser ban if they can��show �no significant fault� to demonstrate they did not intend to cheat. The updated code imposes longer bans on those who cheat intentionally, includes athlete support personnel (eg, coaches, medical staff), and has an increased focus on anti-doping education.91,99
In an effort to educate athletes about sports-supplement use, the Australian Institute of Sport�s sports-supplement program categorizes supplements according to evidence�of efficacy in performance and risk of doping outcome.40 Category A supplements have sound evidence for use and include sports foods, medical supplements, and performance supplements. Category D supplements should not be used by athletes, as they are banned or are at high risk for contamination. These include stimulants, pro-hormones and hormone boosters, growth hormone releasers, peptides, glycerol, and colostrum.40
Conclusion
Athletes are always looking for an edge to improve their performance, and there are a range of dietary strategies available. Nonetheless, dietary recommendations should be individualized for each athlete and their sport and provided by an appropriately qualified professional to ensure optimal performance. Dietary supplements should be used with caution and as part of an overall nutrition and performance plan.
Disclosure
The authors report no conflicts of interest in this work.
Kathryn L Beck1 Jasmine S Thomson2 Richard J Swift1 Pamela R von Hurst1
1School of Food and Nutrition, Massey institute of Food Science and Technology, College of Health, Massey University Albany, Auckland, 2School of Food and Nutrition, Massey institute of Food Science and Technology, College of Health, Massey University Manawatu, Palmerston North, New Zealand
Blank
References:
1. Burke LM, Meyer NL, Pearce J. National nutritional programs for the
2012 London Olympic Games: A systematic approach by three different
countries. In: van Loon LJC, Meeusen R, editors. Limits of Human
Endurance. Nestle Nutrition Institute Workshop Series, volume 76.
Vevey, Switzerland: Nestec Ltd; 2013:103�120.
2. Hansen EA, Emanuelsen A, Gertsen RM, S�rensen SSR. Improved
marathon performance by in-race nutritional strategy intervention.
Int J Sport Nutr Exerc Metab. 2014;24(6):645�655.
3. Hottenrott K, Hass E, Kraus M, Neumann G, Steiner M, Knechtle B.
A scientific nutrition strategy improves time trial performance by ?6%
when compared with a self-chosen nutrition strategy in trained cyclists:
a randomized cross-over study. Appl Physiol Nutr Metab. 2012;
37(4):637�645.
4. Jeukendrup AE, Martin J. Improving cycling performance: how should
we spend our time and money. Sports Med. 2001;31(7):559�569.
5. Wright DA, Sherman WM, Dernbach AR. Carbohydrate feedings
before, during, or in combination improve cycling endurance
performance. J Appl Physiol (1985). 1991;71(3):1082�1088.
6. Jeukendrup A. A step towards personalized sports nutrition: carbohydrate
intake during exercise. Sports Med. 2014;44 Suppl 1:
S25�S33.
7. Hawley JA, Schabort EJ, Noakes TD, Dennis SC. Carbohydrateloading
and exercise performance. An update. Sports Med. 1997;24(2):
73�81.
8. Bergstr�m J, Hermansen L, Hultman E, Saltin B. Diet, muscle glycogen
and physical performance. Acta Physiol Scand. 1967;71(2):140�150.
9. Karlsson J, Saltin B. Diet, muscle glycogen, and endurance performance.
J Appl Physiol. 1971;31(2):203�206.
10. Sherman WM, Costill DL, Fink WJ, Miller JM. Effect of exercise-diet
manipulation on muscle glycogen and its subsequent utilization during
performance. Int J Sports Med. 1981;2(2):114�118.
11. Bussau VA, Fairchild TJ, Rao A, Steele P, Fournier PA. Carbohydrate
loading in human muscle: an improved 1 day protocol. Eur J Appl
Physiol. 2002;87(3):290�295.
12. Fairchild TJ, Fletcher S, Steele P, Goodman C, Dawson B, Fournier PA.
Rapid carbohydrate loading after a short bout of near maximal-intensity
exercise. Med Sci Sports Exerc. 2002;34(6):980�986.
13. Burke LM, Hawley JA, Wong SH, Jeukendrup AE. Carbohydrates for
training and competition. J Sports Sci. 2011;29 Suppl 1:S17�S27.
14. Raman A, Macdermid PW, M�ndel T, Mann M, Stannard SR. The
effects of carbohydrate loading 48 hours before a simulated squash
match. Int J Sport Nutr Exerc Metab. 2014;24(2):157�165.
15. Balsom PD, Wood K, Olsson P, Ekblom B. Carbohydrate intake and
multiple sprint sports: with special reference to football (soccer). Int J
Sports Med. 1999;20(1):48�52.
16. Abt G, Zhou S, Weatherby R. The effect of a high-carbohydrate diet
on the skill performance of midfield soccer players after intermittent
treadmill exercise. J Sci Med Sport. 1998;1(4):203�212.
17. Coyle EF, Coggan AR, Hemmert MK, Lowe RC, Walters TJ. Substrate
usage during prolonged exercise following a preexercise meal. J Appl
Physiol (1985). 1985;59(2):429�433.
18. Neufer PD, Costill DL, Flynn MG, Kirwan JP, Mitchell JB, Houmard J.
Improvements in exercise performance: effects of carbohydrate feedings
and diet. J Appl Physiol (1985). 1987;62(3):983�988.
19. Burke LM, Collier GR, Hargreaves M. Glycemic index � a new tool
in sport nutrition? Int J Sport Nutr. 1998;8(4):401�415.
20. Burke LM, Claassen A, Hawley JA, Noakes TD. Carbohydrate intake
during prolonged cycling minimizes effect of glycemic index of preexercise
meal. J Appl Physiol (1985). 1998;85(6):2220�2226.
21. Wong SH, Chan OW, Chen YJ, Hu HL, Lam CW, Chung PK. Effect of
preexercise glycemic-index meal on running when CHO-electrolyte
solution is consumed during exercise. Int J Sport Nutr Exerc Metab.
2009;19(3):222�242.
22. Burke LM, Maughan RJ. The Governor has a sweet tooth � mouth
sensing of nutrients to enhance sports performance. Eur J Sport Sci.
2015;15(1):29�40.
23. Gant N, Stinear CM, Byblow WD. Carbohydrate in the mouth immediately
facilitates motor output. Brain Res. 2010;1350:151�158.
24. Jentjens RL, Moseley L, Waring RH, Harding LK, Jeukendrup AE.
Oxidation of combined ingestion of glucose and fructose during
exercise. J Appl Physiol (1985). 2004;96(4):1277�1284.
25. Cox GR, Clark SA, Cox AJ, et al. Daily training with high carbohydrate
availability increases exogenous carbohydrate oxidation during endurance
cycling. J Appl Physiol (1985). 2010;109(1):126�134.
26. Bartlett JD, Hawley JA, Morton JP. Carbohydrate availability and
exercise training adaptation: too much of a good thing? Eur J Sport
Sci. 2015;15(1):3�12.
27. Burke LM. Fueling strategies to optimize performance: training high
or training low? Scand J Med Sci Sports. 2010;20 Suppl 2:48�58.
28. Yeo WK, Paton CD, Garnham AP, Burke LM, Carey AL, Hawley JA.
Skeletal muscle adaptation and performance responses to once a day
versus twice every second day endurance training regimens. J Appl
Physiol (1985). 2008;105(5):1462�1470.
29. Morton JP, Croft L, Bartlett JD, et al. Reduced carbohydrate availability
does not modulate training-induced heat shock protein adaptations but
does upregulate oxidative enzyme activity in human skeletal muscle.
J Appl Physiol (1985). 2009;106(5):1513�1521.
30. Horowitz JF, Mora-Rodriguez R, Byerley LO, Coyle EF. Lipolytic suppression
following carbohydrate ingestion limits fat oxidation during
exercise. Am J Physiol. 1997;273(4 Pt 1):E768�E775.
31. Volek JS, Noakes T, Phinney SD. Rethinking fat as a fuel for endurance
exercise. Eur J Sport Sci. 2015;15(1):13�20.
32. Stellingwerff T, Spriet LL, Watt MJ, et al. Decreased PDH activation
and glycogenolysis during exercise following fat adaptation
with carbohydrate restoration. Am J Physiol Endocrinol Metab.
2006;290(2):E380�E388.
33. van Loon LJ. Is there a need for protein ingestion during exercise?
Sports Med. 2014;44 Suppl 1:S105�S111.
34. Hillman AR, Turner MC, Peart DJ, et al. A comparison of hyperhydration
versus ad libitum fluid intake strategies on measures of
oxidative stress, thermoregulation, and performance. Res Sports Med.
2013;21(4):305�317.
35. Sawka MN, Burke LM, Eichner ER, Maughan RJ, Montain SJ,
Stachenfeld NS; American College of Sports Medicine. American
College of Sports Medicine position stand. Exercise and fluid
replacement. Med Sci Sports Exerc. 2007;39(2):377�390.
36. Kristal-Boneh E, Glusman JG, Shitrit R, Chaemovitz C, Cassuto Y.
Physical performance and heat tolerance after chronic water loading and
heat acclimation. Aviat Space Environ Med. 1995;66(8):733�738.
37. Noakes TD. Drinking guidelines for exercise: what evidence is there that
athletes should drink �as much as tolerable�, �to replace the weight lost
during exercise� or �ad libitum�? J Sports Sci. 2007;25(7):781�796.
38. Hoffman MD, Stuempfle KJ. Hydration strategies, weight change
and performance in a 161 km ultramarathon. Res Sports Med.
2014;22(3):213�225.
Thyroid disease affects the thyroid gland, a butterfly-shaped gland found in the front of the neck. The thyroid has important roles to regulate numerous metabolic processes throughout the body. Different types of thyroid disorders affect either its structure or function. Hyperthyroidism, is one of the most common thyroid diseases, which causes the overproduction of the thyroid hormones in the human body.
What natural treatments can help hyperthyroidism?
While there are many treatment methods available to help ease the symptoms of and treat the condition, most individuals may prefer a natural treatment approach to treating their hyperthyroidism. Natural treatments for hyperthyroidism include the regulation of these hormones through the use of various compounds.
The best and most studied compounds proven to curb hyperthyroidism are:
L-carnitine
Selenium
Bugleweed and Lemon Balm
Iodine
L-Carnitine
A randomized, double-blind, placebo-controlled clinical trial (using a crossover arm) was conducted in a group of 50 girls. In this research scientists induced hyperthyroidism from the study participants. For various lengths of time which makes it excellent in assessing the effects of, this study utilized different doses of L-carnitine. This study demonstrated:
The authors of this study concluded, “L-carnitine is successful in both preventing and reversing symptoms of hyperthyroidism.” The authors also comment that L-carnitine can be utilized in pregnant women with Graves’ disease, a thyroid disease which attacks the thyroid gland itself. They also comment that L-carnitine may be used to prevent and cure the most acute kind of hyperthyroidism called thyroid storm. L-carnitine has no known toxicity, contraindications or interactions with other medications or side effect that is significant.
How long until L-carnitine will start working?
Its been observed that patients begin feeling a difference within days of starting L-carnitine, even though the most benefit may take weeks to months to realize based on some studies.
Selenium
The most research regarding selenium and thyroid has examined selenium’s effect on Hashimoto’s thyroid disease, an autoimmune disorder. That being said there have also been some promising findings regarding Alzheimer’s effect on Graves’ disease. While the data do not appear to be 100 percent conclusive, evidence suggests the following:
Selenium has the ability to lower the antibodies associated with Hashimoto’s
Selenium has the ability to lower the antibodies associated with Grave’s
Selenium can be used by pregnant women with thyroid disease to help avoid regression of thyroid health postpartum, and has no effect on the embryo and perhaps a small advantage
Selenium can diminish the eye complications associated with Grave’s
Selenium can lower the eye problems associated with Grave’s radioactive iodine treatment
Greater blood glucose levels correlate with a lower relapse rate of Grave’s
Patients with Grave’s tend to have lower selenium levels
Selenium seems to lower the symptoms related to Graves’
Patients given selenium along with radioactive iodine or anti-thyroid drugs (Methimizole) achieve regular thyroid position quicker than people not receiving selenium.
Bugleweed & Lemon Balm
Bugleweed and lemon balm, also known as Lycopus europaeus and Melissa officinalis respectively, are utilized for a long time in the management of moderate hyperthyroidism. Despite their history that is favorable, there aren’t many studies. This being said, however, Bugleweed and lemon balm appear to be safe and have a positive impact in hyperthyroidism that is handling. Here are a few highlights in what we know about these herbs:
Bugleweed and Lemon Balm may really work to obstruct TSH and cause a lowering of T4 and T3
Short term animal studies have demonstrated an ability to reduce TSH, T4 and T3
Decreased heart rate with no side effects in prospective human studies
Bugleweed was shown to reduce the higher heart rate and blood pressure associated with Grave’s. It was found to be as effective as the pharmaceutical beta block, Atenolol, in an animal study
Iodine
Iodine shouldn’t be used as a primary therapy, although it does seem to have utility as a brief term addition to help manage hyperthyroidism. One study showed that 150mg per day of potassium iodide resulted in reversal of hyperthyroidism. The effects, however, were short lived; just lasting for 21 times in certain but around 6 months in others. Due to this it appears Iodide is employed as a temporary add on to help dampen up a flare .
In short, many healthcare professionals who specialize in natural treatment, such as functional medicine practitioners, have utilized these four natural compounds as treatment alternatives for managing the hyperthyroidism associated with Graves’ disease, Hashimoto’s thyroid disease, as well as other thyroid issues. Its been found that these compounds are effective for most individuals and they have caused no side effects, with the exception to L-carnitine which can cause loose stools in large doses. When decreasing the dose, this issue resolves.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine
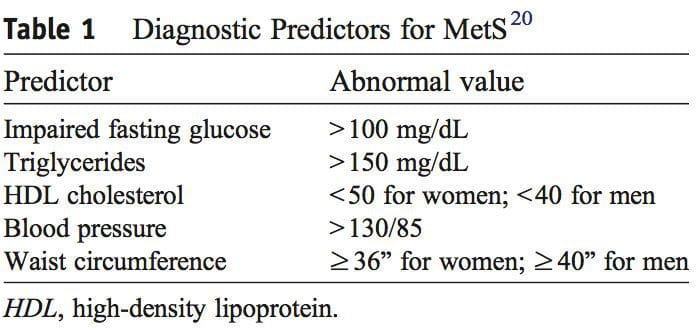
 PubMed was searched from the earliest possible date to May 2014 to identify review articles that outlined the pathophysiology of MetS and T2DM. This led to further search refinements to identify inflammatory mechanisms that occur in the pancreas, adipose tissue, skeletal muscle, and hypothalamus. Searches were also refined to identify relationships among diet, supplements, and glycemic regulation. Both animal and human studies were reviewed. The selection of specific supplements was based on those that were most commonly used in the clinical setting, namely, gymnema sylvestre, vanadium, chromium and ?-lipoic acid.
PubMed was searched from the earliest possible date to May 2014 to identify review articles that outlined the pathophysiology of MetS and T2DM. This led to further search refinements to identify inflammatory mechanisms that occur in the pancreas, adipose tissue, skeletal muscle, and hypothalamus. Searches were also refined to identify relationships among diet, supplements, and glycemic regulation. Both animal and human studies were reviewed. The selection of specific supplements was based on those that were most commonly used in the clinical setting, namely, gymnema sylvestre, vanadium, chromium and ?-lipoic acid. Under normal conditions, skeletal muscle, hepatic, and adipose tissues require the action of insulin for cellular glucose entry. Insulin resistance represents an inability of insulin to signal glucose passage into insulin-dependent cells. Although a genetic predisposition can exist, the�etiology of insulin resistance has been linked to chronic low-grade inflammation.1 Combined with insulin resistance-induced hyperglycemia, chronic low-grade inflammation also sustains MetS pathophysiology.1
Under normal conditions, skeletal muscle, hepatic, and adipose tissues require the action of insulin for cellular glucose entry. Insulin resistance represents an inability of insulin to signal glucose passage into insulin-dependent cells. Although a genetic predisposition can exist, the�etiology of insulin resistance has been linked to chronic low-grade inflammation.1 Combined with insulin resistance-induced hyperglycemia, chronic low-grade inflammation also sustains MetS pathophysiology.1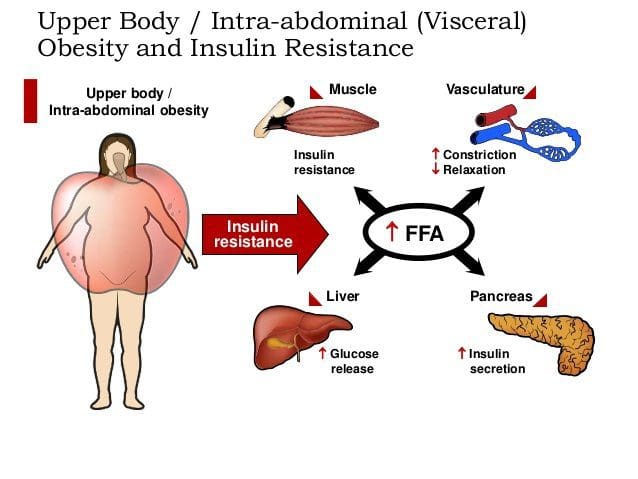 Caloric excess and a sedentary lifestyle contribute to the accumulation of subcutaneous and visceral adipose tissue. Adipose tissue was once thought of as a metabolically inert passive energy depot. A large body of evidence now demonstrates that excess visceral adipose tissue acts as a driver of chronic low-grade inflammation and insulin resistance.27,34
Caloric excess and a sedentary lifestyle contribute to the accumulation of subcutaneous and visceral adipose tissue. Adipose tissue was once thought of as a metabolically inert passive energy depot. A large body of evidence now demonstrates that excess visceral adipose tissue acts as a driver of chronic low-grade inflammation and insulin resistance.27,34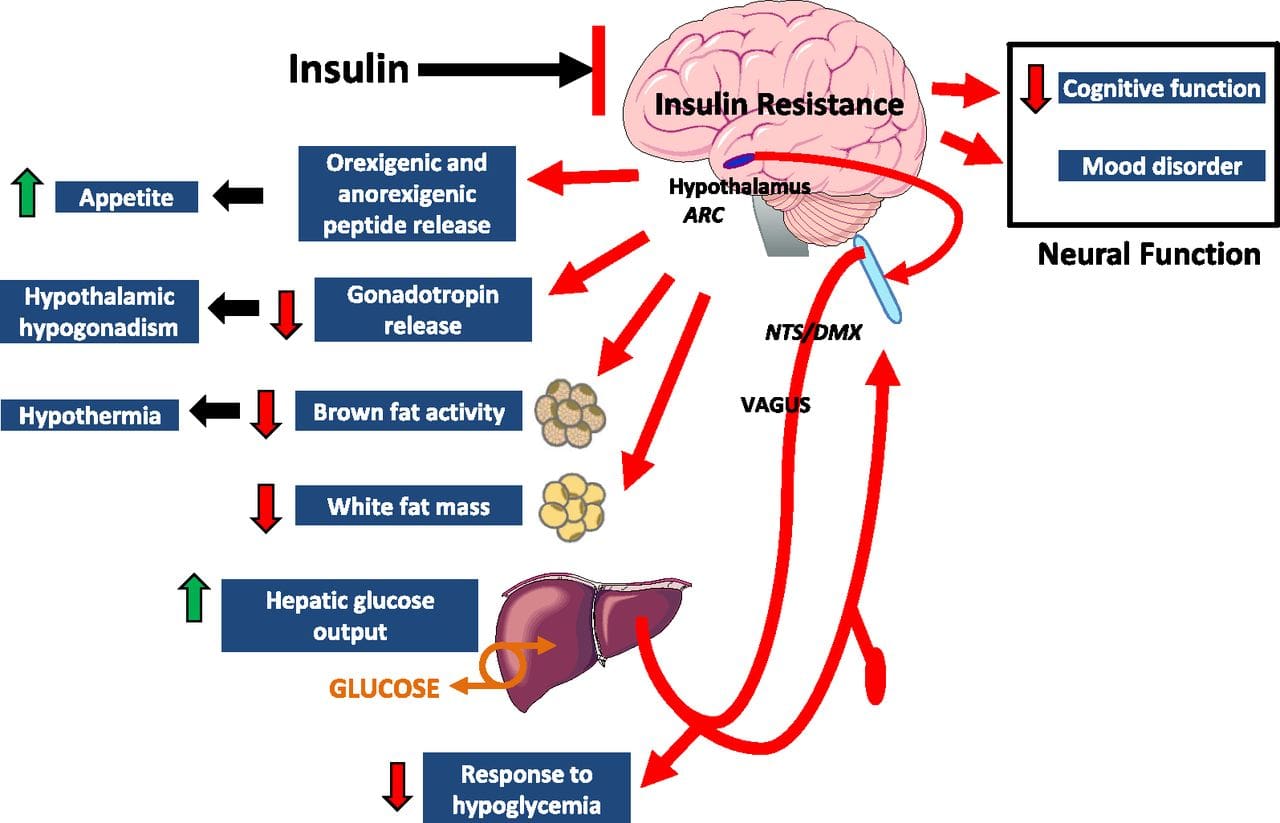 Eating behavior in the obese and overweight has been popularly attributed to a lack of will power or genetics. However, recent research has demonstrated a link between hypothalamic inflammation and increased body weight.41,41
Eating behavior in the obese and overweight has been popularly attributed to a lack of will power or genetics. However, recent research has demonstrated a link between hypothalamic inflammation and increased body weight.41,41 Feeding generally leads to a short-term increase in both oxidative stress and inflammation. 41 Total�calories consumed, glycemic index, and fatty acid profile of a meal all influence the degree of postprandial inflammation. It is estimated that the average American consumes approximately 20% of calories from refined sugar, 20% from refined grains and flour, 15% to 20% from excessively fatty meat products, and 20% from refined seed/legume oils.45 This pattern of eating contains a macronutrient composition and glycemic index that promote hyperglycemia, hyperlipemia, and an acute postprandial inflammatory response. 46 Collectively referred to as postprandial dysmetabolism, this pro-inflammatory response can sustain levels of chronic low-grade inflammation that leads to excess body fat, coronary heart disease (CHD), insulin resistance, and T2DM.28,29,47
Feeding generally leads to a short-term increase in both oxidative stress and inflammation. 41 Total�calories consumed, glycemic index, and fatty acid profile of a meal all influence the degree of postprandial inflammation. It is estimated that the average American consumes approximately 20% of calories from refined sugar, 20% from refined grains and flour, 15% to 20% from excessively fatty meat products, and 20% from refined seed/legume oils.45 This pattern of eating contains a macronutrient composition and glycemic index that promote hyperglycemia, hyperlipemia, and an acute postprandial inflammatory response. 46 Collectively referred to as postprandial dysmetabolism, this pro-inflammatory response can sustain levels of chronic low-grade inflammation that leads to excess body fat, coronary heart disease (CHD), insulin resistance, and T2DM.28,29,47 Diagnosis of MetS has been linked to an increased risk of developing T2DM and cardiovascular disease over the following 5 to 10 years. 1 It further increases a patient’s risk of stroke, myocardial infarction, and death from any of the aforementioned conditions.1
Diagnosis of MetS has been linked to an increased risk of developing T2DM and cardiovascular disease over the following 5 to 10 years. 1 It further increases a patient’s risk of stroke, myocardial infarction, and death from any of the aforementioned conditions.1 Research has identified nutrients that play key roles in promoting proper insulin sensitivity, including vitamin D, magnesium, omega-3 (n-3) fatty acids, curcumin, gymnema, vanadium, chromium, and ?-lipoic acid. It is possible to get adequate vitamin D from sun exposure and adequate amounts of magnesium and omega-3 fatty acids from food. Contrastingly, the therapeutic levels of chromium and ?-lipoic acid that affect insulin sensitivity and reduce�insulin resistance cannot be obtained in food and must be supplemented.
Research has identified nutrients that play key roles in promoting proper insulin sensitivity, including vitamin D, magnesium, omega-3 (n-3) fatty acids, curcumin, gymnema, vanadium, chromium, and ?-lipoic acid. It is possible to get adequate vitamin D from sun exposure and adequate amounts of magnesium and omega-3 fatty acids from food. Contrastingly, the therapeutic levels of chromium and ?-lipoic acid that affect insulin sensitivity and reduce�insulin resistance cannot be obtained in food and must be supplemented. Vitamin D, magnesium, and n-3 fatty acids have multiple functions, and generalized inflammation reduction is a common mechanism of action.74�80 Their supplemental use should be considered in the context of low-grade inflammation reduction and health promotion, rather than as a specific treatment for MetS or T2DM.
Vitamin D, magnesium, and n-3 fatty acids have multiple functions, and generalized inflammation reduction is a common mechanism of action.74�80 Their supplemental use should be considered in the context of low-grade inflammation reduction and health promotion, rather than as a specific treatment for MetS or T2DM. Gymnemic acids are the active component of the G sylvestre plant leaves. Gymnemic acids are the active component of the G sylvestre plant leaves. Studies evaluating G sylvestre’s effects on diabetes in humans have generally been of poor methodological quality. Experimental animal studies have found that gymnemic acids may decrease glucose uptake in the small intestine, inhibit gluconeogenesis, and reduce hepatic and skeletal muscle insulin resistance.99 Other animal studies suggest that gymnemic acids may have comparable efficacy in reducing blood sugar levels to the first-generation sulfonylurea, tolbutamide.100
Gymnemic acids are the active component of the G sylvestre plant leaves. Gymnemic acids are the active component of the G sylvestre plant leaves. Studies evaluating G sylvestre’s effects on diabetes in humans have generally been of poor methodological quality. Experimental animal studies have found that gymnemic acids may decrease glucose uptake in the small intestine, inhibit gluconeogenesis, and reduce hepatic and skeletal muscle insulin resistance.99 Other animal studies suggest that gymnemic acids may have comparable efficacy in reducing blood sugar levels to the first-generation sulfonylurea, tolbutamide.100 Vanadyl sulfate has been reported to prolong the events of insulin signaling and may actually improve insulin sensitivity.101 Limited data suggest that it inhibits gluconeogenesis, possibly ameliorating hepatic insulin resistance. 100,101 Uncontrolled clinical trials have reported improvements in insulin sensitivity using 50 to 300 mg daily for periods ranging from 3 to 6 weeks. 101�103 Contrastingly, a recent randomized, double-blind, placebo-controlled trial found that 50 mg of vanadyl sulfate twice daily for 4 weeks had no effect in individuals with impaired glucose tolerance. 104 Limited clinical and experimental data exist supporting the use of vanadyl sulfate to improve insulin resistance,�and further research is warranted regarding its safety and efficacy.
Vanadyl sulfate has been reported to prolong the events of insulin signaling and may actually improve insulin sensitivity.101 Limited data suggest that it inhibits gluconeogenesis, possibly ameliorating hepatic insulin resistance. 100,101 Uncontrolled clinical trials have reported improvements in insulin sensitivity using 50 to 300 mg daily for periods ranging from 3 to 6 weeks. 101�103 Contrastingly, a recent randomized, double-blind, placebo-controlled trial found that 50 mg of vanadyl sulfate twice daily for 4 weeks had no effect in individuals with impaired glucose tolerance. 104 Limited clinical and experimental data exist supporting the use of vanadyl sulfate to improve insulin resistance,�and further research is warranted regarding its safety and efficacy. Diets high in refined sugar and flour are deficient in chromium (Cr) and lead to an increased urinary excretion of chromium. 105,106 The progression of MetS is not likely caused by a chromium deficiency, 107 and dosages that benefit glycemic regulation are not achievable through food. 106,108,109
Diets high in refined sugar and flour are deficient in chromium (Cr) and lead to an increased urinary excretion of chromium. 105,106 The progression of MetS is not likely caused by a chromium deficiency, 107 and dosages that benefit glycemic regulation are not achievable through food. 106,108,109 Humans derive ?-lipoic acid through dietary means and from endogenous synthesis. 111 The foods richest in ?-lipoic acid are animal tissues with extensive metabolic activity such as animal heart, liver, and kidney, which are not consumed in large amounts in the typical American diet. 111 Supplemental amounts of ?-lipoic acid used in the treatment of T2DM (300-600 mg) are likely to be as much as 1000 times greater than the amounts that could be obtained from the diet.112
Humans derive ?-lipoic acid through dietary means and from endogenous synthesis. 111 The foods richest in ?-lipoic acid are animal tissues with extensive metabolic activity such as animal heart, liver, and kidney, which are not consumed in large amounts in the typical American diet. 111 Supplemental amounts of ?-lipoic acid used in the treatment of T2DM (300-600 mg) are likely to be as much as 1000 times greater than the amounts that could be obtained from the diet.112 This is a narrative overview of the topic of MetS. A systematic review was not performed; therefore, there may be relevant information missing from this review. The contents of this overview focuses on the opinions of the authors, and therefore, others may disagree with our opinions or approaches to management. This overview is limited by the studies that have been published. To date, no studies have been published that identify the effectiveness of a combination of a dietary intervention, such as the Spanish ketogenic diet, and nutritional supplementation on the expression of the MetS. Similarly, this approach has not been studied in patients with musculoskeletal pain who also have the MetS. Consequently, the information presented in this article is speculative. Longitudinal studies are needed before any specific recommendations can be made for patients with musculoskeletal that may be influenced by the MetS.
This is a narrative overview of the topic of MetS. A systematic review was not performed; therefore, there may be relevant information missing from this review. The contents of this overview focuses on the opinions of the authors, and therefore, others may disagree with our opinions or approaches to management. This overview is limited by the studies that have been published. To date, no studies have been published that identify the effectiveness of a combination of a dietary intervention, such as the Spanish ketogenic diet, and nutritional supplementation on the expression of the MetS. Similarly, this approach has not been studied in patients with musculoskeletal pain who also have the MetS. Consequently, the information presented in this article is speculative. Longitudinal studies are needed before any specific recommendations can be made for patients with musculoskeletal that may be influenced by the MetS.


 There are 3 known types of negative reactions to wheat proteins, collectively known as wheat protein reactivity: wheat allergy (WA), gluten sensitivity (GS),�and celiac disease (CD). Of the 3, only CD is known to involve autoimmune reactivity, generation of antibodies, and intestinal mucosal damage. Wheat allergy involves the release of histamine by way of immunoglobulin (Ig) E cross-linking with gluten peptides and presents within hours after ingestion of wheat proteins. Gluten sensitivity is considered to be a diagnosis of exclusion; sufferers improve symptomatically with a gluten-free diet (GFD) but do not express antibodies or IgE reactivity.1
There are 3 known types of negative reactions to wheat proteins, collectively known as wheat protein reactivity: wheat allergy (WA), gluten sensitivity (GS),�and celiac disease (CD). Of the 3, only CD is known to involve autoimmune reactivity, generation of antibodies, and intestinal mucosal damage. Wheat allergy involves the release of histamine by way of immunoglobulin (Ig) E cross-linking with gluten peptides and presents within hours after ingestion of wheat proteins. Gluten sensitivity is considered to be a diagnosis of exclusion; sufferers improve symptomatically with a gluten-free diet (GFD) but do not express antibodies or IgE reactivity.1 A 28-year-old man presented to a chiropractic teaching clinic with complaints of constant muscle fasciculations of 2 years� duration. The muscle fasciculations originally started in the left eye and remained there for about 6 months. The patient then noticed that the fasciculations began to move to other areas of his body. They first moved into the right eye, followed by the lips,�and then to the calves, quadriceps, and gluteus muscles. The twitching would sometimes occur in a single muscle or may involve all of the above muscles simultaneously. Along with the twitches, he reports a constant �buzzing� or �crawling� feeling in his legs. There was no point during the day or night when the twitches ceased.
A 28-year-old man presented to a chiropractic teaching clinic with complaints of constant muscle fasciculations of 2 years� duration. The muscle fasciculations originally started in the left eye and remained there for about 6 months. The patient then noticed that the fasciculations began to move to other areas of his body. They first moved into the right eye, followed by the lips,�and then to the calves, quadriceps, and gluteus muscles. The twitching would sometimes occur in a single muscle or may involve all of the above muscles simultaneously. Along with the twitches, he reports a constant �buzzing� or �crawling� feeling in his legs. There was no point during the day or night when the twitches ceased.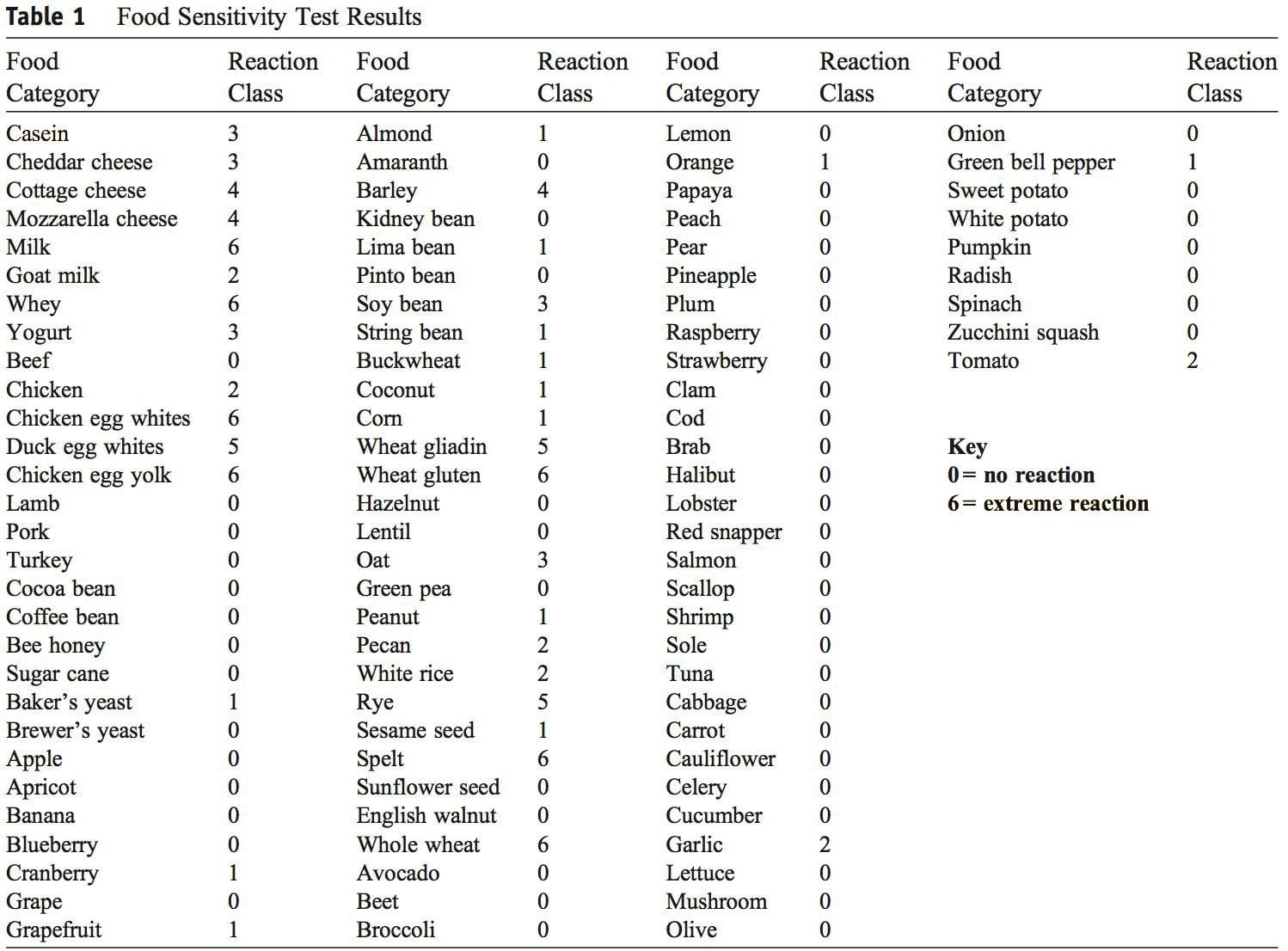 Discussion
Discussion The authors could not find any published case studies related to a presentation such as the one�described here. We believe this is a unique presentation of wheat protein reactivity and thereby represents a contribution to the body of knowledge in this field.
The authors could not find any published case studies related to a presentation such as the one�described here. We believe this is a unique presentation of wheat protein reactivity and thereby represents a contribution to the body of knowledge in this field. This report describes improvement in chronic, widespread muscle fasciculations and various other systemic symptoms with dietary change. There is strong suspicion that this case represents one of
This report describes improvement in chronic, widespread muscle fasciculations and various other systemic symptoms with dietary change. There is strong suspicion that this case represents one of


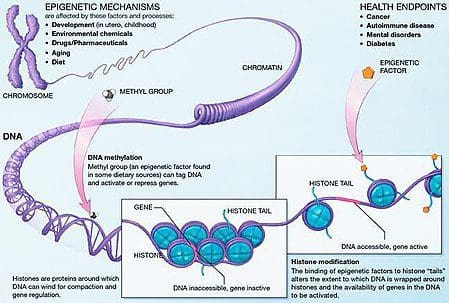 Obesity is a complex, multifactorial disease, and better understanding of the mechanisms underlying the interactions between lifestyle, environment, and genetics is critical for developing effective strategies for prevention and treatment [1].
Obesity is a complex, multifactorial disease, and better understanding of the mechanisms underlying the interactions between lifestyle, environment, and genetics is critical for developing effective strategies for prevention and treatment [1]. Animal models provide unique opportunities for highly controlled studies that provide mechanistic insight into�the role of specific epigenetic marks, both as indicators of current metabolic status and as predictors of the future risk of obesity and metabolic disease. A particularly important aspect of animal studies is that they allow for the assessment of epigenetic changes within target tissues, including the liver and hypothalamus, which is much more difficult in humans. Moreover, the ability to harvest large quantities of fresh tissue makes it possible to assess multiple chromatin marks as well as DNA methylation. Some of these epigenetic modifications either alone or in combination may be responsive to environmental programming. In animal models, it is also possible to study multiple generations of offspring and thus enable differentiation between trans-generational and intergenerational transmission of obesity risk mediated by epigenetic memory of parental nutritional status, which cannot be easily distinguished in human studies. We use the former term for meiotic transmission of risk in the absence of continued exposure while the latter primarily entails direct transmission of risk through metabolic reprogramming of the fetus or gametes.
Animal models provide unique opportunities for highly controlled studies that provide mechanistic insight into�the role of specific epigenetic marks, both as indicators of current metabolic status and as predictors of the future risk of obesity and metabolic disease. A particularly important aspect of animal studies is that they allow for the assessment of epigenetic changes within target tissues, including the liver and hypothalamus, which is much more difficult in humans. Moreover, the ability to harvest large quantities of fresh tissue makes it possible to assess multiple chromatin marks as well as DNA methylation. Some of these epigenetic modifications either alone or in combination may be responsive to environmental programming. In animal models, it is also possible to study multiple generations of offspring and thus enable differentiation between trans-generational and intergenerational transmission of obesity risk mediated by epigenetic memory of parental nutritional status, which cannot be easily distinguished in human studies. We use the former term for meiotic transmission of risk in the absence of continued exposure while the latter primarily entails direct transmission of risk through metabolic reprogramming of the fetus or gametes.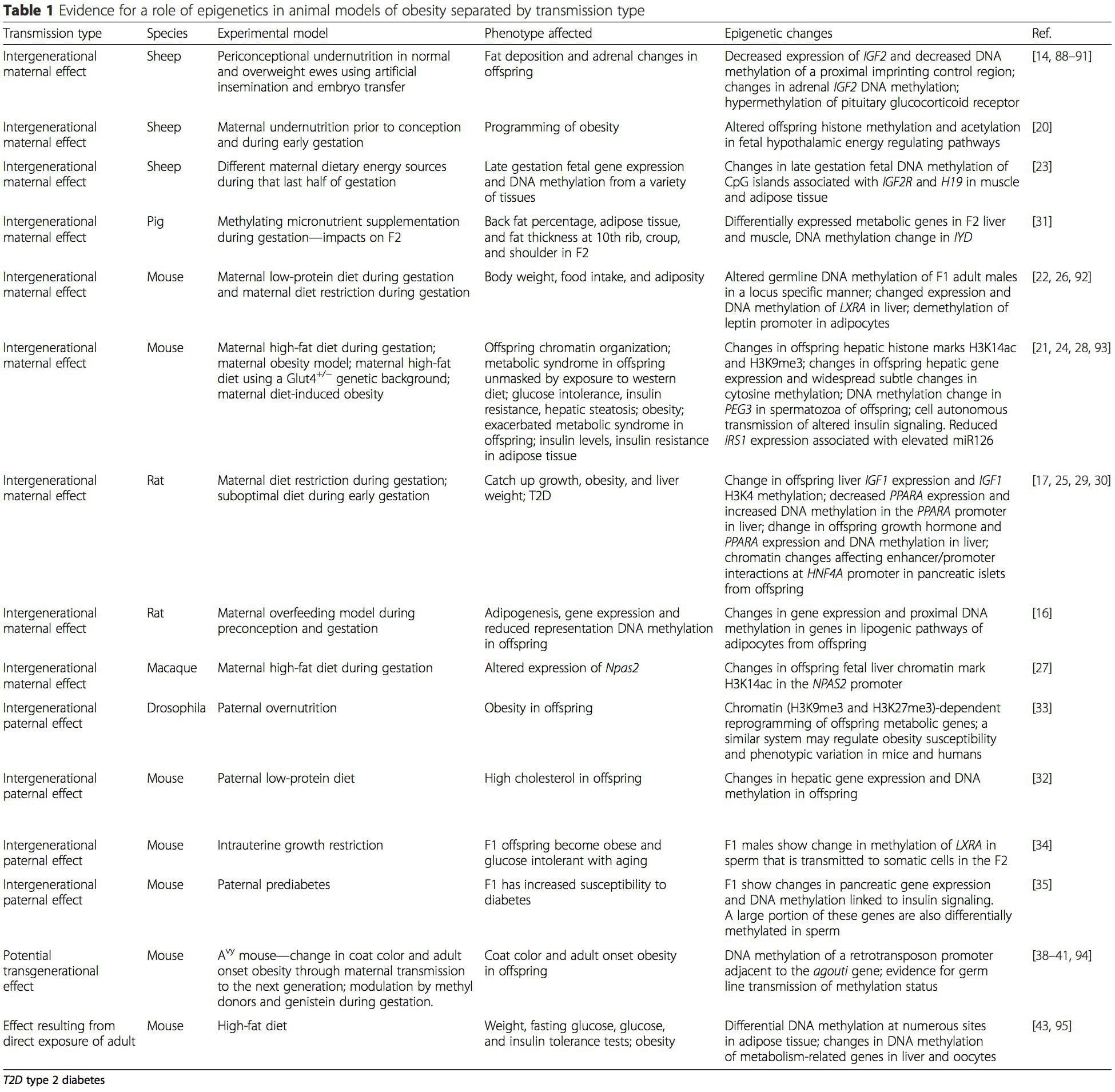 (i) Epigenetic Changes In Offspring Associated With Maternal Nutrition During Gestation
(i) Epigenetic Changes In Offspring Associated With Maternal Nutrition During Gestation Maternal nutritional supplementation, undernutrition, and over nutrition during pregnancy can alter fat deposition and energy homeostasis in offspring [11, 13�15, 19]. Associated with these effects in the offspring are changes in DNA methylation, histone post-translational modifications, and gene expression for several target genes,�especially genes regulating fatty acid metabolism and insulin signaling [16, 17, 20�30]. The diversity of animal models used in these studies and the common metabolic pathways impacted suggest an evolutionarily conserved adaptive response mediated by epigenetic modification. However, few of the specific identified genes and epigenetic changes have been cross-validated in related studies, and large-scale genome-wide investigations have typically not been applied. A major hindrance to comparison of these studies is the different develop mental windows subjected to nutritional challenge, which may cause considerably different outcomes. Proof that the epigenetic changes are causal rather than being associated with offspring phenotypic changes is also required. This will necessitate the identification of a parental nutritionally induced epigenetic �memory� response that precedes development of the altered phenotype in offspring.
Maternal nutritional supplementation, undernutrition, and over nutrition during pregnancy can alter fat deposition and energy homeostasis in offspring [11, 13�15, 19]. Associated with these effects in the offspring are changes in DNA methylation, histone post-translational modifications, and gene expression for several target genes,�especially genes regulating fatty acid metabolism and insulin signaling [16, 17, 20�30]. The diversity of animal models used in these studies and the common metabolic pathways impacted suggest an evolutionarily conserved adaptive response mediated by epigenetic modification. However, few of the specific identified genes and epigenetic changes have been cross-validated in related studies, and large-scale genome-wide investigations have typically not been applied. A major hindrance to comparison of these studies is the different develop mental windows subjected to nutritional challenge, which may cause considerably different outcomes. Proof that the epigenetic changes are causal rather than being associated with offspring phenotypic changes is also required. This will necessitate the identification of a parental nutritionally induced epigenetic �memory� response that precedes development of the altered phenotype in offspring. Emerging studies have demonstrated that paternal plane of nutrition can impact offspring fat deposition and epigenetic marks [31�34]. One recent investigation using mice has demonstrated that paternal pre-diabetes leads to increased susceptibility to diabetes in F1 offspring with associated changes in pancreatic gene expression and DNA methylation linked to insulin signaling [35]. Importantly, there was an overlap of these epigenetic changes in pancreatic islets and sperm suggesting germ line inheritance. However, most of these studies, although intriguing in their implications, are limited in the genomic scale of investigation and frequently show weak and somewhat transient epigenetic alterations associated with mild metabolic phenotypes in offspring.
Emerging studies have demonstrated that paternal plane of nutrition can impact offspring fat deposition and epigenetic marks [31�34]. One recent investigation using mice has demonstrated that paternal pre-diabetes leads to increased susceptibility to diabetes in F1 offspring with associated changes in pancreatic gene expression and DNA methylation linked to insulin signaling [35]. Importantly, there was an overlap of these epigenetic changes in pancreatic islets and sperm suggesting germ line inheritance. However, most of these studies, although intriguing in their implications, are limited in the genomic scale of investigation and frequently show weak and somewhat transient epigenetic alterations associated with mild metabolic phenotypes in offspring.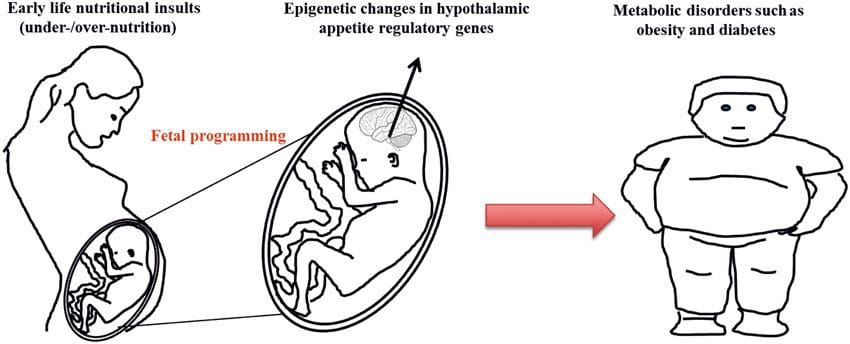 Stable transmission of epigenetic information across multiple generations is well described in plant systems and C. elegans, but its significance in mammals is still much debated [36, 37]. An epigenetic basis for grand- parental transmission of phenotypes in response to dietary exposures has been well established, including in livestock species [31]. The most influential studies demonstrating effects of epigenetic transmission impacting offspring phenotype have used the example of the viable yellow agouti (Avy) mouse [38]. In this mouse, an insertion of a retrotransposon upstream of the agouti gene causes its constitutive expression and consequent yellow coat color and adult onset obesity. Maternal transmission through the germ line results in DNA methylation�mediated silencing of agouti expression resulting in wild-type coat color and lean phenotype of the offspring [39, 40]. Importantly, subsequent studies in these mice demonstrated that maternal exposure to methyl donors causes a shift in coat color [41]. One study has reported transmission of a phenotype to the F3 generation and alterations in expression of large number of genes in response to protein restriction in F0 [42]; however, alterations in expression were highly variable and a direct link to epigenetic changes was not identified in this system.
Stable transmission of epigenetic information across multiple generations is well described in plant systems and C. elegans, but its significance in mammals is still much debated [36, 37]. An epigenetic basis for grand- parental transmission of phenotypes in response to dietary exposures has been well established, including in livestock species [31]. The most influential studies demonstrating effects of epigenetic transmission impacting offspring phenotype have used the example of the viable yellow agouti (Avy) mouse [38]. In this mouse, an insertion of a retrotransposon upstream of the agouti gene causes its constitutive expression and consequent yellow coat color and adult onset obesity. Maternal transmission through the germ line results in DNA methylation�mediated silencing of agouti expression resulting in wild-type coat color and lean phenotype of the offspring [39, 40]. Importantly, subsequent studies in these mice demonstrated that maternal exposure to methyl donors causes a shift in coat color [41]. One study has reported transmission of a phenotype to the F3 generation and alterations in expression of large number of genes in response to protein restriction in F0 [42]; however, alterations in expression were highly variable and a direct link to epigenetic changes was not identified in this system.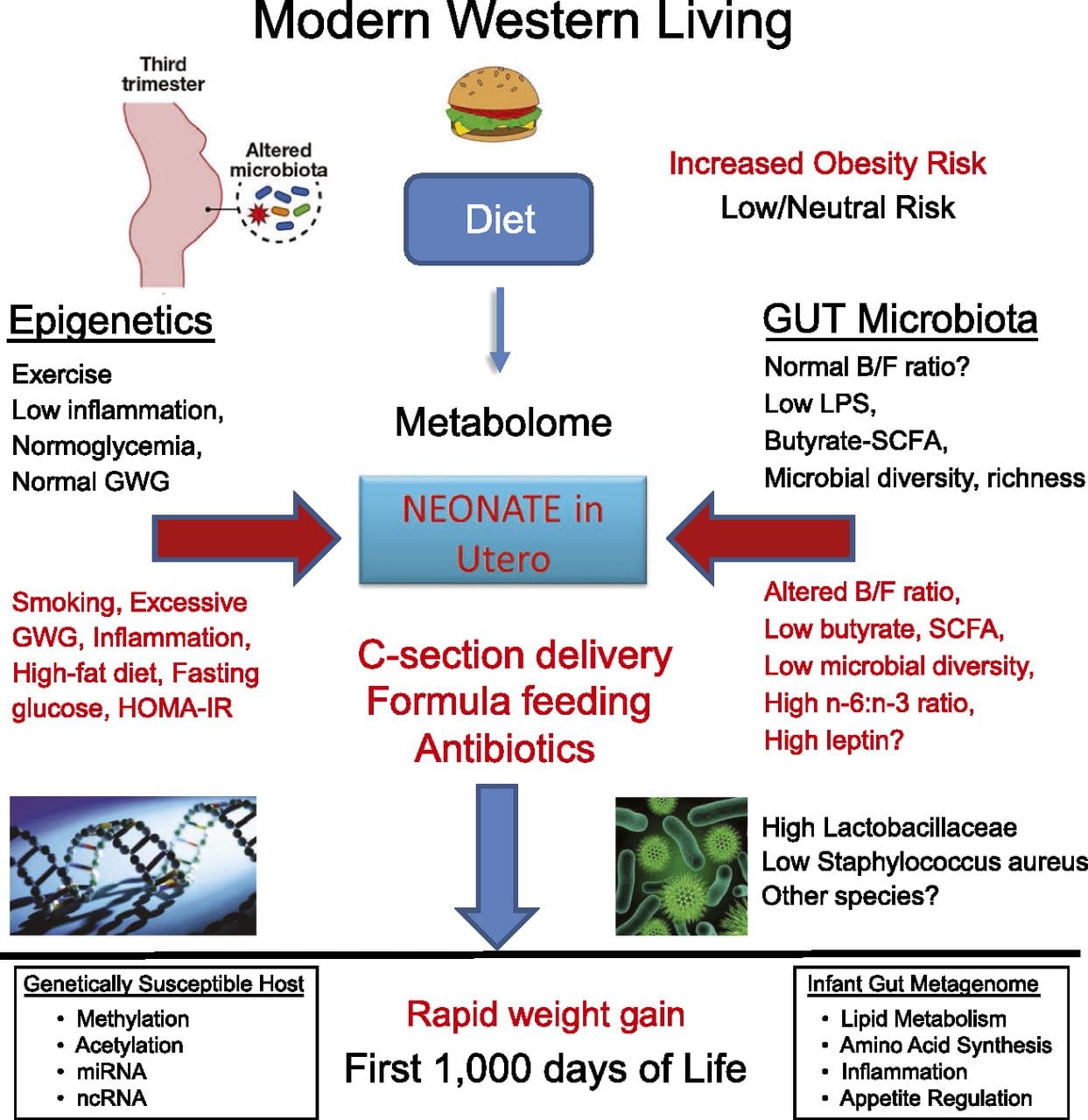 While many studies have identified diet-associated epigenetic changes in animal models using candidate site-specific regions, there have been few genome-wide analyses undertaken. A recent study focussed on determining the direct epigenetic impact of high-fat diets/ diet-induced obesity in adult mice using genome-wide gene expression and DNA methylation analyses [43]. This study identified 232 differentially methylated regions (DMRs) in adipocytes from control and high-fat fed mice. Importantly, the corresponding human regions for the murine DMRs were also differentially methylated in adipose tissue from a population of obese and lean humans, thereby highlighting the remarkable evolutionary conservation of these regions. This result emphasizes the likely importance of the identified DMRs in regulating energy homeostasis in mammals.
While many studies have identified diet-associated epigenetic changes in animal models using candidate site-specific regions, there have been few genome-wide analyses undertaken. A recent study focussed on determining the direct epigenetic impact of high-fat diets/ diet-induced obesity in adult mice using genome-wide gene expression and DNA methylation analyses [43]. This study identified 232 differentially methylated regions (DMRs) in adipocytes from control and high-fat fed mice. Importantly, the corresponding human regions for the murine DMRs were also differentially methylated in adipose tissue from a population of obese and lean humans, thereby highlighting the remarkable evolutionary conservation of these regions. This result emphasizes the likely importance of the identified DMRs in regulating energy homeostasis in mammals.
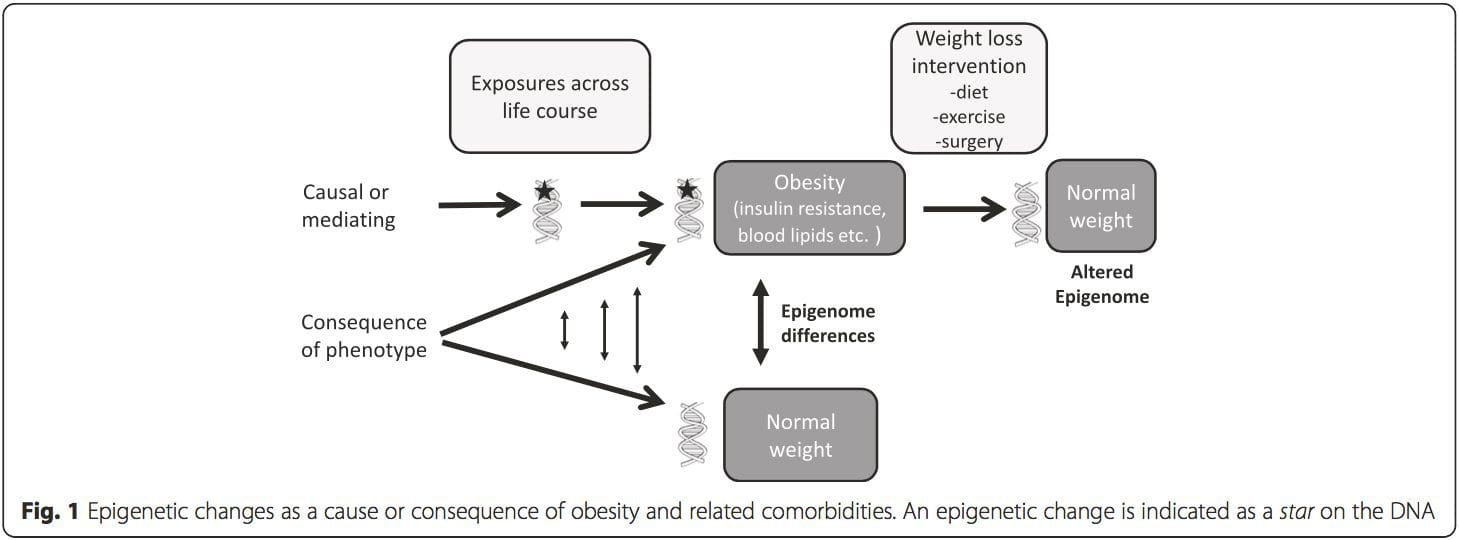 (i) Genetic association studies. Genetic polymorphisms that are associated with an increased risk of developing particular conditions are a priori linked to the causative genes. The presence of differential�methylation in such regions infers functional relevance of these epigenetic changes in controlling expression of the proximal gene(s). There are strong cis-acting genetic effects underpinning much epigenetic variation [7, 45], and in population-based studies, methods that use genetic surrogates to infer a causal or mediating role of epigenome differences have been applied [7, 46�48]. The use of familial genetic information can also lead to the identification of potentially causative candidate regions showing phenotype-related differential methylation [49].
(i) Genetic association studies. Genetic polymorphisms that are associated with an increased risk of developing particular conditions are a priori linked to the causative genes. The presence of differential�methylation in such regions infers functional relevance of these epigenetic changes in controlling expression of the proximal gene(s). There are strong cis-acting genetic effects underpinning much epigenetic variation [7, 45], and in population-based studies, methods that use genetic surrogates to infer a causal or mediating role of epigenome differences have been applied [7, 46�48]. The use of familial genetic information can also lead to the identification of potentially causative candidate regions showing phenotype-related differential methylation [49].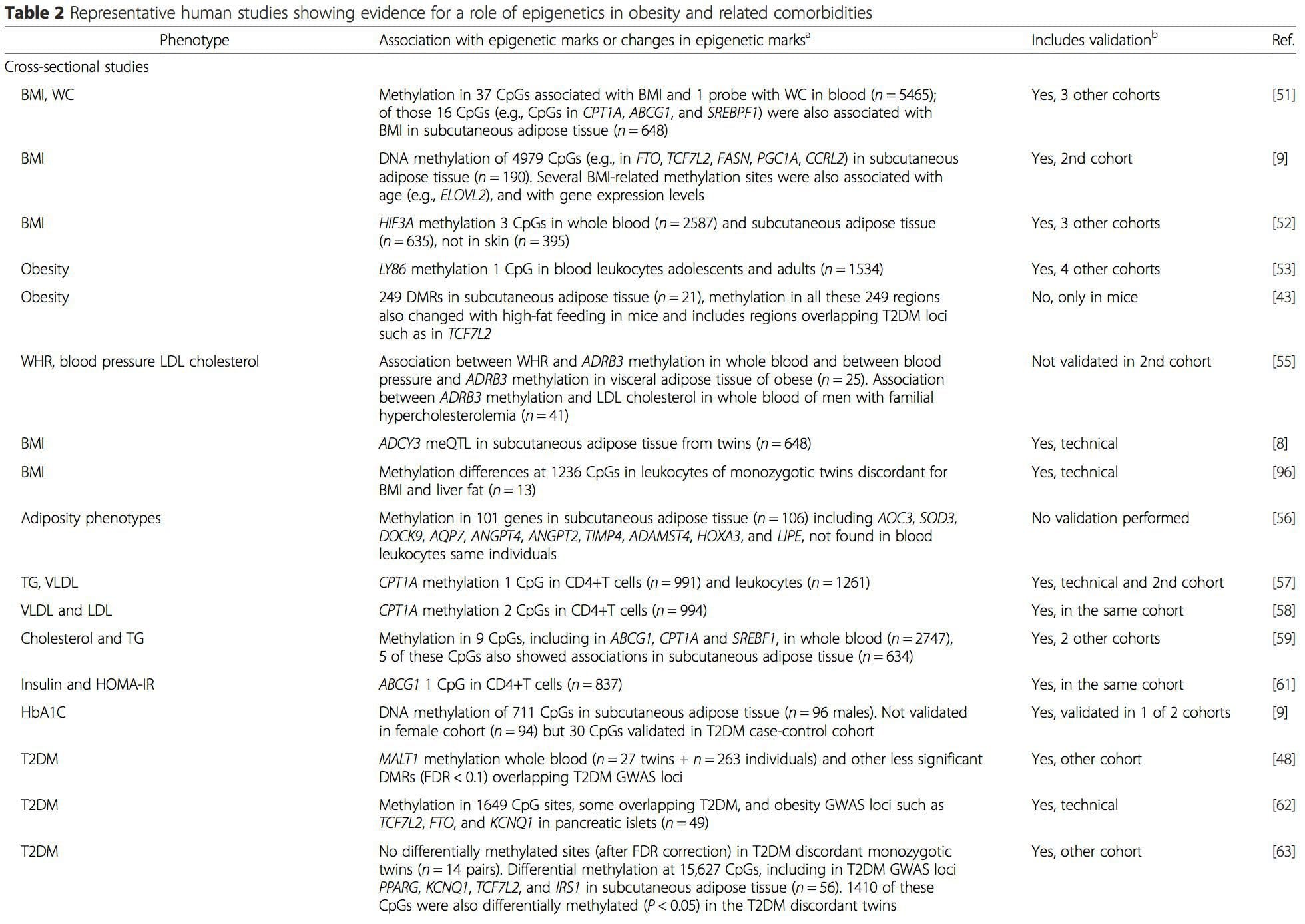
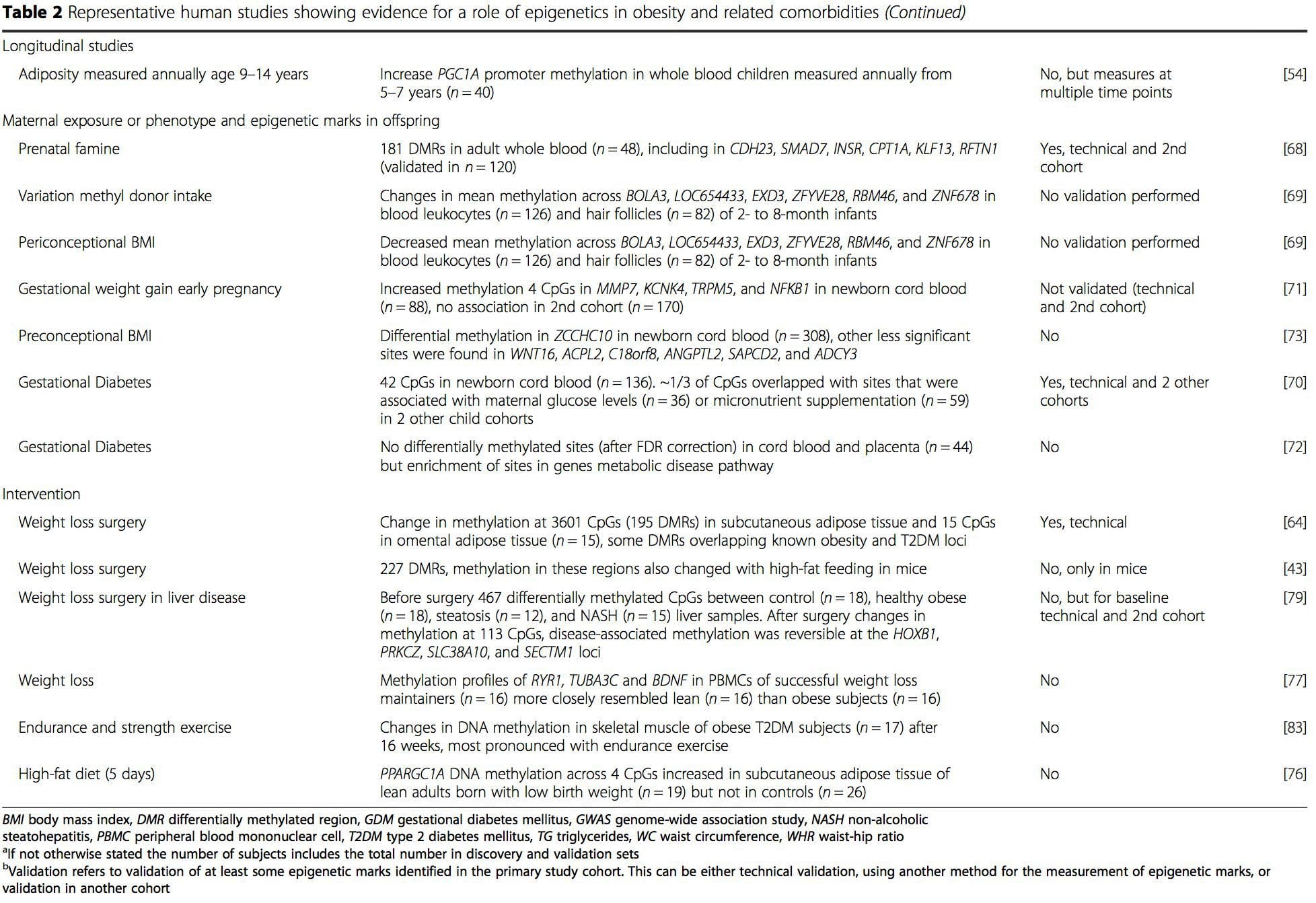 From these studies, altered methylation of PGC1A, HIF3A, ABCG1, and CPT1A and the previously described RXRA [18] have emerged as biomarkers associated with, or perhaps predictive of, metabolic health that are also plausible candidates for a role in development of metabolic disease.
From these studies, altered methylation of PGC1A, HIF3A, ABCG1, and CPT1A and the previously described RXRA [18] have emerged as biomarkers associated with, or perhaps predictive of, metabolic health that are also plausible candidates for a role in development of metabolic disease.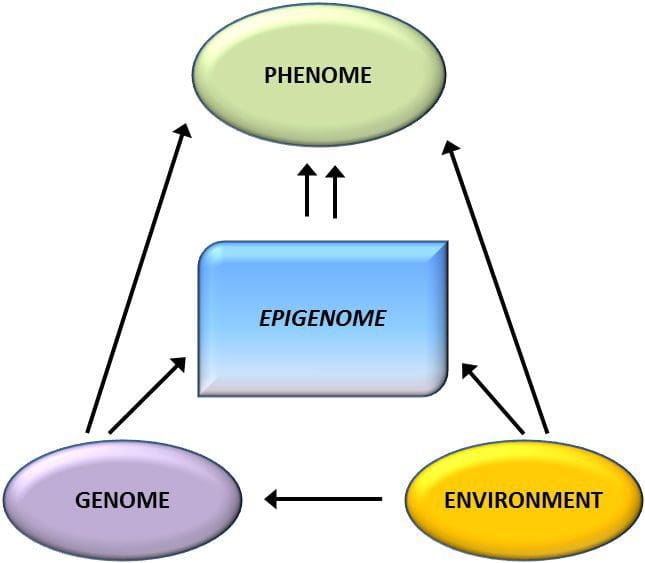 Epigenetic variation is highly influenced by the underlying genetic variation, with genotype estimated to explain ~20�40 % of the variation [6, 8]. Recently, a number of studies have begun to integrate methylome and genotype data to identify methylation quantitative trait loci (meQTL) associated with disease phenotypes. For instance, in adipose tissue, an meQTL overlapping�with a BMI genetic risk locus has been identified in an enhancer element upstream of ADCY3 [8]. Other studies have also identified overlaps between known obesity and T2DM risk loci and DMRs associated with obesity and T2DM [43, 48, 62]. Methylation of a number of such DMRs was also modulated by high-fat feeding in mice [43] and weight loss in humans [64]. These results identify an intriguing link between genetic variations linked with disease susceptibility and their association with regions of the genome that undergo epigenetic modifications in response to nutritional challenges, implying a causal relationship. The close connection between genetic and epigenetic variation may signify their essential roles in generating individual variation [65, 66]. However, while these findings suggest that DNA methylation may be a mediator of genetic effects, it is also important to consider that both genetic and epigenetic processes could act independently on the same genes. Twin studies [8, 63, 67] can provide important insights and indicate that inter-individual differences in levels of DNA methylation arise predominantly from non-shared environment and stochastic influences, minimally from shared environmental effects, but also with a significant impact of genetic variation.
Epigenetic variation is highly influenced by the underlying genetic variation, with genotype estimated to explain ~20�40 % of the variation [6, 8]. Recently, a number of studies have begun to integrate methylome and genotype data to identify methylation quantitative trait loci (meQTL) associated with disease phenotypes. For instance, in adipose tissue, an meQTL overlapping�with a BMI genetic risk locus has been identified in an enhancer element upstream of ADCY3 [8]. Other studies have also identified overlaps between known obesity and T2DM risk loci and DMRs associated with obesity and T2DM [43, 48, 62]. Methylation of a number of such DMRs was also modulated by high-fat feeding in mice [43] and weight loss in humans [64]. These results identify an intriguing link between genetic variations linked with disease susceptibility and their association with regions of the genome that undergo epigenetic modifications in response to nutritional challenges, implying a causal relationship. The close connection between genetic and epigenetic variation may signify their essential roles in generating individual variation [65, 66]. However, while these findings suggest that DNA methylation may be a mediator of genetic effects, it is also important to consider that both genetic and epigenetic processes could act independently on the same genes. Twin studies [8, 63, 67] can provide important insights and indicate that inter-individual differences in levels of DNA methylation arise predominantly from non-shared environment and stochastic influences, minimally from shared environmental effects, but also with a significant impact of genetic variation. Prenatal environment: Two recently published studies made use of human populations that experienced �natural� variations in nutrient supply to study the impact of maternal nutrition before or during pregnancy on DNA methylation in the offspring [68, 69]. The first study used a Gambian mother-child cohort to show that both seasonal variations in maternal methyl donor intake during pregnancy and maternal pre-pregnancy BMI were associated with altered methylation in the infants [69]. The second study utilized adult offspring from the Dutch Hunger Winter cohort to investigate the effect of prenatal exposure to an acute period of severe maternal undernutrition on DNA methylation of genes involved in growth and metabolism in adulthood [68]. The results highlighted the importance of the timing of the exposure in its impact on the epigenome, since significant epigenetic effects were only identified in individuals exposed to famine during early gestation. Importantly, the epigenetic changes occurred in conjunction with increased BMI; however, it was not possible to establish in this study whether these changes were present earlier in life or a consequence of the higher BMI.
Prenatal environment: Two recently published studies made use of human populations that experienced �natural� variations in nutrient supply to study the impact of maternal nutrition before or during pregnancy on DNA methylation in the offspring [68, 69]. The first study used a Gambian mother-child cohort to show that both seasonal variations in maternal methyl donor intake during pregnancy and maternal pre-pregnancy BMI were associated with altered methylation in the infants [69]. The second study utilized adult offspring from the Dutch Hunger Winter cohort to investigate the effect of prenatal exposure to an acute period of severe maternal undernutrition on DNA methylation of genes involved in growth and metabolism in adulthood [68]. The results highlighted the importance of the timing of the exposure in its impact on the epigenome, since significant epigenetic effects were only identified in individuals exposed to famine during early gestation. Importantly, the epigenetic changes occurred in conjunction with increased BMI; however, it was not possible to establish in this study whether these changes were present earlier in life or a consequence of the higher BMI. Postnatal environment: The epigenome is established de novo during embryonic development, and therefore, the prenatal environment most likely has the most significant impact on the epigenome. However, it is now clear that changes do occur in the �mature� epigenome under the influence of a range of conditions, including aging, exposure to toxins, and dietary alterations. For example, changes in DNA methylation in numerous genes in skeletal muscle and PGC1A in adipose tissue have been demonstrated in response to a high-fat diet [75, 76]. Interventions to lose body fat mass have also been associated with changes in DNA methylation. Studies have reported that the DNA methylation profiles of adipose tissue [43, 64], peripheral blood mononuclear cells [77], and muscle tissue [78] in formerly obese patients become more similar to the profiles of lean subjects following weight loss. Weight loss surgery also partially reversed non-alcoholic fatty liver disease-associated methylation changes in liver [79] and in another study led to hypomethylation of multiple obesity candidate genes, with more pronounced effects in subcutaneous compared to omental (visceral) fat [64]. Accumulating evidence suggests that exercise interventions can also influence DNA methylation. Most of these studies have been conducted in lean individuals [80�82], but one exercise study in obese T2DM subjects also demonstrated changes in DNA methylation, including in genes involved in fatty acid and glucose transport [83]. Epigenetic changes also occur with aging, and recent data suggest a role of obesity in augmenting them [9, 84, 85]. Obesity accelerated the epigenetic age of liver tissue, but in contrast to the findings described above, this effect was not reversible after weight loss [84].
Postnatal environment: The epigenome is established de novo during embryonic development, and therefore, the prenatal environment most likely has the most significant impact on the epigenome. However, it is now clear that changes do occur in the �mature� epigenome under the influence of a range of conditions, including aging, exposure to toxins, and dietary alterations. For example, changes in DNA methylation in numerous genes in skeletal muscle and PGC1A in adipose tissue have been demonstrated in response to a high-fat diet [75, 76]. Interventions to lose body fat mass have also been associated with changes in DNA methylation. Studies have reported that the DNA methylation profiles of adipose tissue [43, 64], peripheral blood mononuclear cells [77], and muscle tissue [78] in formerly obese patients become more similar to the profiles of lean subjects following weight loss. Weight loss surgery also partially reversed non-alcoholic fatty liver disease-associated methylation changes in liver [79] and in another study led to hypomethylation of multiple obesity candidate genes, with more pronounced effects in subcutaneous compared to omental (visceral) fat [64]. Accumulating evidence suggests that exercise interventions can also influence DNA methylation. Most of these studies have been conducted in lean individuals [80�82], but one exercise study in obese T2DM subjects also demonstrated changes in DNA methylation, including in genes involved in fatty acid and glucose transport [83]. Epigenetic changes also occur with aging, and recent data suggest a role of obesity in augmenting them [9, 84, 85]. Obesity accelerated the epigenetic age of liver tissue, but in contrast to the findings described above, this effect was not reversible after weight loss [84]. DNA methylation changes associated with obesity or induced by diet or lifestyle interventions and weight loss are generally modest (<15 %), although this varies depending on the phenotype and tissue studied. For instance, changes greater than 20 % have been reported in adipose tissue after weight loss [64] and associations between HIF3A methylation and BMI in adipose tissue were more pronounced than in blood [52].
DNA methylation changes associated with obesity or induced by diet or lifestyle interventions and weight loss are generally modest (<15 %), although this varies depending on the phenotype and tissue studied. For instance, changes greater than 20 % have been reported in adipose tissue after weight loss [64] and associations between HIF3A methylation and BMI in adipose tissue were more pronounced than in blood [52].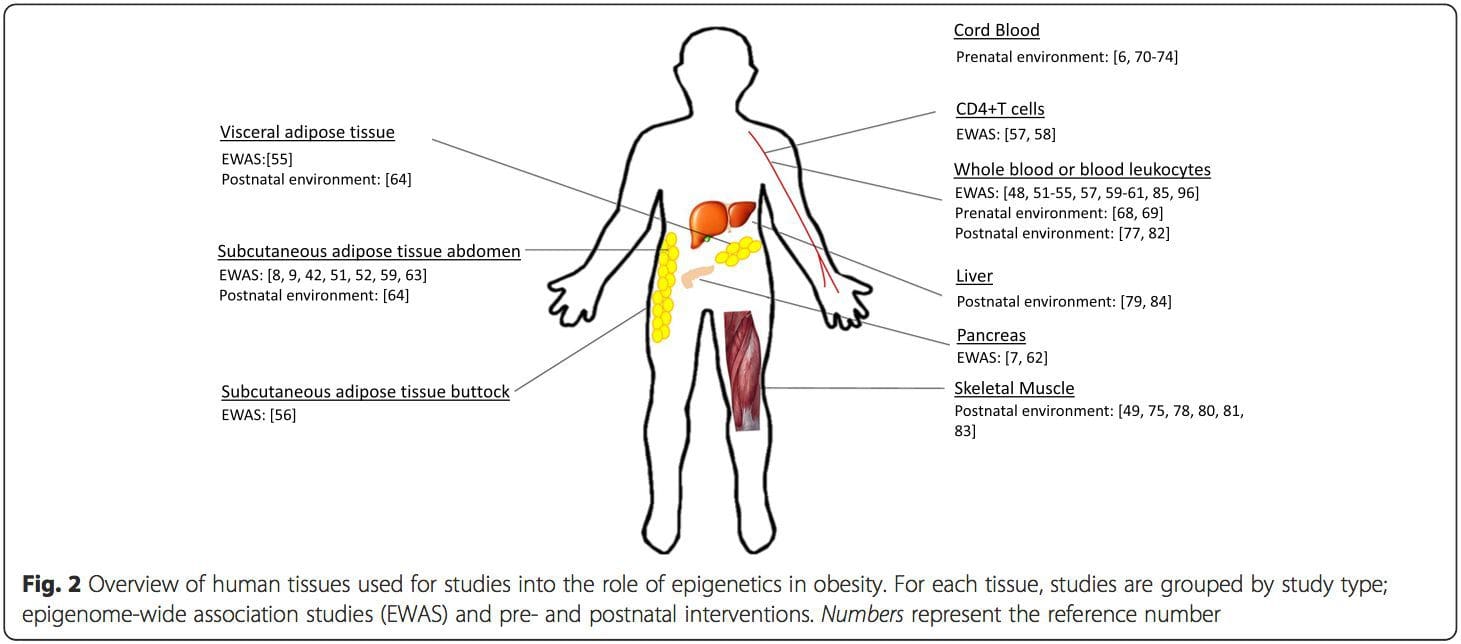 Conclusions
Conclusions

 Nutrition is increasingly recognized as a key component of optimal sporting performance, with both the science and practice of sports nutrition developing rapidly.1 Recent studies have found that a planned scientific nutritional strategy (consisting of fluid, carbohydrate, sodium, and caffeine) compared with a self-chosen nutritional strategy helped non-elite runners complete a marathon run faster2 and trained cyclists complete a time trial faster.3 Whereas training has the greatest potential to increase performance, it has been estimated that consumption of a carbohydrate�electrolyte drink or relatively low doses of caffeine may improve a 40 km cycling time trial performance by 32�42 and 55�84 seconds, respectively.4
Nutrition is increasingly recognized as a key component of optimal sporting performance, with both the science and practice of sports nutrition developing rapidly.1 Recent studies have found that a planned scientific nutritional strategy (consisting of fluid, carbohydrate, sodium, and caffeine) compared with a self-chosen nutritional strategy helped non-elite runners complete a marathon run faster2 and trained cyclists complete a time trial faster.3 Whereas training has the greatest potential to increase performance, it has been estimated that consumption of a carbohydrate�electrolyte drink or relatively low doses of caffeine may improve a 40 km cycling time trial performance by 32�42 and 55�84 seconds, respectively.4
 Carbohydrate ingestion has been shown to improve performance in events lasting approximately 1 hour.6 A growing body of evidence also demonstrates beneficial effects of a carbohydrate mouth rinse on performance.22 It is thought that receptors in the oral cavity signal to the central nervous system to positively modify motor output.23
Carbohydrate ingestion has been shown to improve performance in events lasting approximately 1 hour.6 A growing body of evidence also demonstrates beneficial effects of a carbohydrate mouth rinse on performance.22 It is thought that receptors in the oral cavity signal to the central nervous system to positively modify motor output.23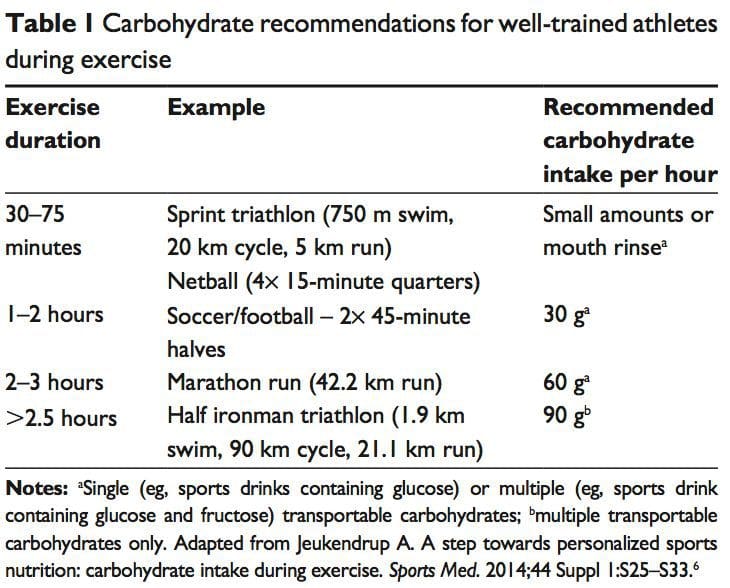
 The �train-low, compete-high� concept is training with low carbohydrate availability to promote adaptations such as�enhanced activation of cell-signaling pathways, increased mitochondrial enzyme content and activity, enhanced lipid oxidation rates, and hence improved exercise capacity.26 However, there is no clear evidence that performance is improved with this approach.27 For example, when highly trained cyclists were separated into once-daily (train-high) or twice-daily (train-low) training sessions, increases in resting muscle glycogen content were seen in the low-carbohydrate- availability group, along with other selected training adaptations.28 However, performance in a 1-hour time trial after 3 weeks of training was no different between groups. Other research has produced similar results.29 Different strategies have been suggested (eg, training after an overnight fast, training twice per day, restricting carbohydrate during recovery),26 but further research is needed to establish optimal dietary periodization plans.27
The �train-low, compete-high� concept is training with low carbohydrate availability to promote adaptations such as�enhanced activation of cell-signaling pathways, increased mitochondrial enzyme content and activity, enhanced lipid oxidation rates, and hence improved exercise capacity.26 However, there is no clear evidence that performance is improved with this approach.27 For example, when highly trained cyclists were separated into once-daily (train-high) or twice-daily (train-low) training sessions, increases in resting muscle glycogen content were seen in the low-carbohydrate- availability group, along with other selected training adaptations.28 However, performance in a 1-hour time trial after 3 weeks of training was no different between groups. Other research has produced similar results.29 Different strategies have been suggested (eg, training after an overnight fast, training twice per day, restricting carbohydrate during recovery),26 but further research is needed to establish optimal dietary periodization plans.27 There has been a recent resurgence of interest in fat as a fuel, particularly for ultra endurance exercise. A high-carbohydrate strategy inhibits fat utilization during exercise,30 which may not be beneficial due to the abundance of energy stored in the body as fat. Creating an environment that optimizes fat oxidation potentially occurs when dietary carbohydrate is reduced to a level that promotes ketosis.31 However, this strategy may impair performance of high-intensity activity, by contributing to a reduction in pyruvate dehydrogenase activity and glycogenolysis. 32 The lack of performance benefits seen in studies investigating �high-fat� diets may be attributed to inadequate carbohydrate restriction and time for adaptation.31 Research into the performance effects of high fat diets continues.
There has been a recent resurgence of interest in fat as a fuel, particularly for ultra endurance exercise. A high-carbohydrate strategy inhibits fat utilization during exercise,30 which may not be beneficial due to the abundance of energy stored in the body as fat. Creating an environment that optimizes fat oxidation potentially occurs when dietary carbohydrate is reduced to a level that promotes ketosis.31 However, this strategy may impair performance of high-intensity activity, by contributing to a reduction in pyruvate dehydrogenase activity and glycogenolysis. 32 The lack of performance benefits seen in studies investigating �high-fat� diets may be attributed to inadequate carbohydrate restriction and time for adaptation.31 Research into the performance effects of high fat diets continues. While protein consumption prior to and during endurance and resistance exercise has been shown to enhance rates of muscle protein synthesis (MPS), a recent review found protein ingestion alongside carbohydrate during exercise does not improve time�trial performance when compared with the ingestion of adequate amounts of carbohydrate alone.33
While protein consumption prior to and during endurance and resistance exercise has been shown to enhance rates of muscle protein synthesis (MPS), a recent review found protein ingestion alongside carbohydrate during exercise does not improve time�trial performance when compared with the ingestion of adequate amounts of carbohydrate alone.33 The purpose of fluid consumption during exercise is primarily to maintain hydration and thermoregulation, thereby benefiting performance. Evidence is emerging on increased risk of oxidative stress with dehydration.34 Fluid consumption prior to exercise is recommended to ensure that the athlete is well-hydrated prior to commencing exercise.35 In addition,�carefully planned hyperhydration ( fluid overloading) prior to an event may reset fluid balance and increase fluid retention, and consequently improve heat tolerance.36 However, fluid overloading may increase the risk of hyponatremia 37 and impact negatively on performance due to feelings of fullness and the need to urinate.
The purpose of fluid consumption during exercise is primarily to maintain hydration and thermoregulation, thereby benefiting performance. Evidence is emerging on increased risk of oxidative stress with dehydration.34 Fluid consumption prior to exercise is recommended to ensure that the athlete is well-hydrated prior to commencing exercise.35 In addition,�carefully planned hyperhydration ( fluid overloading) prior to an event may reset fluid balance and increase fluid retention, and consequently improve heat tolerance.36 However, fluid overloading may increase the risk of hyponatremia 37 and impact negatively on performance due to feelings of fullness and the need to urinate. Performance supplements shown to enhance performance include caffeine, beetroot juice, beta-alanine (BA), creatine, and bicarbonate.40 Comprehensive reviews on other supplements including caffeine, creatine, and bicarbonate can be found elsewhere.41 In recent years, research has focused on the role of nitrate, BA, and vitamin D and performance. Nitrate is most commonly provided as sodium nitrate or beetroot juice.42 Dietary nitrates are reduced (in mouth and stomach) to nitrites, and then to nitric oxide. During exercise, nitric oxide potentially influences skeletal muscle function through regulation of blood ow and glucose homeostasis, as well as mitochondrial respiration.43 During endurance exercise, nitrate supplementation has been shown to increase exercise efficiency (4%�5% reduction in VO at a steady attenuate oxidative stress.42 Similarly, a 4.2% improvement in performance was shown in a test designed to simulate a football game.44
Performance supplements shown to enhance performance include caffeine, beetroot juice, beta-alanine (BA), creatine, and bicarbonate.40 Comprehensive reviews on other supplements including caffeine, creatine, and bicarbonate can be found elsewhere.41 In recent years, research has focused on the role of nitrate, BA, and vitamin D and performance. Nitrate is most commonly provided as sodium nitrate or beetroot juice.42 Dietary nitrates are reduced (in mouth and stomach) to nitrites, and then to nitric oxide. During exercise, nitric oxide potentially influences skeletal muscle function through regulation of blood ow and glucose homeostasis, as well as mitochondrial respiration.43 During endurance exercise, nitrate supplementation has been shown to increase exercise efficiency (4%�5% reduction in VO at a steady attenuate oxidative stress.42 Similarly, a 4.2% improvement in performance was shown in a test designed to simulate a football game.44
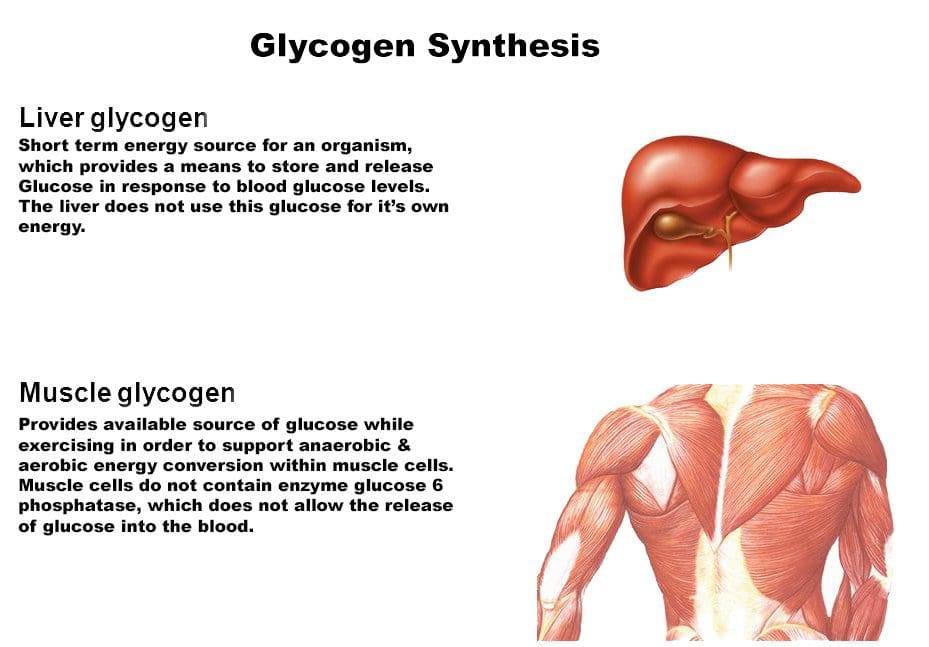 Consuming carbohydrates immediately
Consuming carbohydrates immediately  An acute bout of intense endurance or resistance exercise can induce a transient increase in protein turnover, and, until feeding, protein balance remains negative. Protein consumption after exercise enhances MPS and net protein balance,58 predominantly by increasing mitochondrial protein fraction with endurance training, and myofibrillar protein fraction with resistance training.59
An acute bout of intense endurance or resistance exercise can induce a transient increase in protein turnover, and, until feeding, protein balance remains negative. Protein consumption after exercise enhances MPS and net protein balance,58 predominantly by increasing mitochondrial protein fraction with endurance training, and myofibrillar protein fraction with resistance training.59 Fluid and electrolyte replacement after exercise can be achieved through resuming normal hydration practices. However, when euhydration is needed within 24 hours or substantial body weight has been lost (.5% of BM), a more structured response may be warranted to replace fluids and electrolytes.77
Fluid and electrolyte replacement after exercise can be achieved through resuming normal hydration practices. However, when euhydration is needed within 24 hours or substantial body weight has been lost (.5% of BM), a more structured response may be warranted to replace fluids and electrolytes.77 The availability of nutrition information for athletes varies. Younger or recreational athletes are more likely to receive generalized nutritional information of poorer quality from individuals such as coaches.78 Elite athletes are more likely to have access to specialized sports-nutrition input from qualified professionals. A range of sports science and medicine support systems are in place in different countries to assist elite athletes,1 and nutrition is a key component of these services. Some countries have nutrition programs embedded within sports institutes (eg, Australia) or alternatively have National Olympic Committees that support nutrition programs (eg, United States of America).1 However, not all athletes at the elite level have access to sports-nutrition services. This may be due to financial constraints of the sport, geographical issues, and a lack of recognition of the value of a sports-nutrition service.78
The availability of nutrition information for athletes varies. Younger or recreational athletes are more likely to receive generalized nutritional information of poorer quality from individuals such as coaches.78 Elite athletes are more likely to have access to specialized sports-nutrition input from qualified professionals. A range of sports science and medicine support systems are in place in different countries to assist elite athletes,1 and nutrition is a key component of these services. Some countries have nutrition programs embedded within sports institutes (eg, Australia) or alternatively have National Olympic Committees that support nutrition programs (eg, United States of America).1 However, not all athletes at the elite level have access to sports-nutrition services. This may be due to financial constraints of the sport, geographical issues, and a lack of recognition of the value of a sports-nutrition service.78 Supplement use is widespread in athletes.86,87 For example, 87.5% of elite athletes in Australia used dietary supplements88 and 87% of Canadian high-performance athletes took dietary supplements within the past 6 months85 (Table 2). It is difficult to compare studies due to differences in the criteria used to define dietary supplements, variations in assessing supplement intake, and disparities in the populations studied.85
Supplement use is widespread in athletes.86,87 For example, 87.5% of elite athletes in Australia used dietary supplements88 and 87% of Canadian high-performance athletes took dietary supplements within the past 6 months85 (Table 2). It is difficult to compare studies due to differences in the criteria used to define dietary supplements, variations in assessing supplement intake, and disparities in the populations studied.85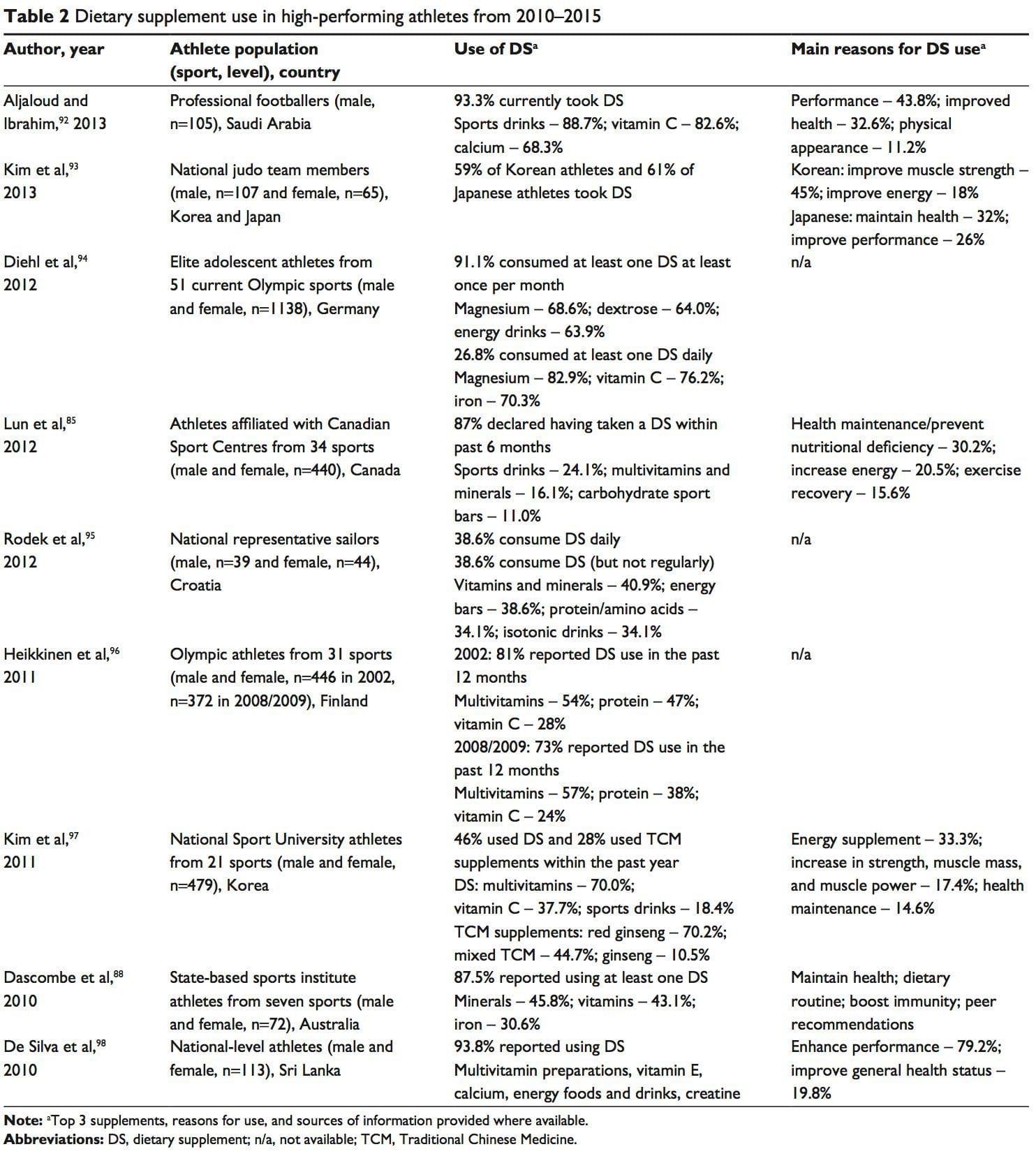 A positive drug test in an athlete can occur with even a minute quantity of a banned substance.41,87 WADA maintains a �strict liability� policy, whereby every athlete is responsible for any substance found in their body regardless of how it got there.41,86,87,89 The World Anti-Doping Code (January 1, 2015) does recognize the issue of contaminated supplements.91 Whereas the code upholds the principle of strict liability, athletes may receive a lesser ban if they can��show �no significant fault� to demonstrate they did not intend to cheat. The updated code imposes longer bans on those who cheat intentionally, includes athlete support personnel (eg, coaches, medical staff), and has an increased focus on anti-doping education.91,99
A positive drug test in an athlete can occur with even a minute quantity of a banned substance.41,87 WADA maintains a �strict liability� policy, whereby every athlete is responsible for any substance found in their body regardless of how it got there.41,86,87,89 The World Anti-Doping Code (January 1, 2015) does recognize the issue of contaminated supplements.91 Whereas the code upholds the principle of strict liability, athletes may receive a lesser ban if they can��show �no significant fault� to demonstrate they did not intend to cheat. The updated code imposes longer bans on those who cheat intentionally, includes athlete support personnel (eg, coaches, medical staff), and has an increased focus on anti-doping education.91,99







