Dr. Alex Jimenez Discusses What to Eat to Improve DNA Methylation
�
Methylation is a fundamental process which occurs in every cell of the human body. It is utilized to promote a variety of bodily processes, such as producing and regulating hormones and neurotransmitters, developing immune cells, and managing the detoxification of exogenous substances, as well as clearing histamine, among other essential processes. Methylation is also important for cellular renewal to help modify genetic expression.
By changing your diet and lifestyle you can optimize your DNA methylation to improve your overall health and wellness. If you have a methylation deficit, such as an altered MTHFR gene or increased homocysteine levels, you can improve your DNA methylation by eating a variety of healthy foods.
Methylation support can benefit many health issues, including; aging, pregnancy preparation, pregnancy lactation, prolonged strenuous physical activity, ADD/ADHD, addiction, allergies, Alzheimer’s disease, anxiety, asthma, atherosclerosis, autism, behavioral changes, bipolar disorder, cancer, chemical sensitivities, chronic fatigue, cleft palate, diabetes, dementia, depression, Down syndrome, hypertension, fertility problems, fibromyalgia, insomnia, multiple sclerosis, neural tube defects, neuropathy, ocular disease, Parkinson’s disease, schizophrenia, and thyroid disease.
�
�
What to Eat for Methylation Support
�
The following articles will focus on what you can eat to promote methylation support. The utilization of supplements as well as drugs and/or medications to improve DNA methylation can cause a variety of undesirable side-effects if these are not monitored accordingly by healthcare professionals and patients alike. In part 1, we will demonstrate what you can eat to improve DNA methylation from the category of fruits, vegetables, nuts and seeds, legumes, and grains, as well as herbs and spices. Our ultimate goal is to help you achieve optimal methylation support.
�
Fruits
�
Fruits are an excellent source of nutrients which can provide a variety of methylation adaptogens. Fruits with a low-glycemic index, such as wild berries, have less sugar than their larger, commercially-produced counterparts.
The following list of fruits can promote methylation support while those in bold are especially high in methylation adaptogens, including; apples, apricots, avocado, bananas, blackberries, blackcurrant, blueberries, cantaloupe, cherries, clementines, coconut, cranberries, elderberries, figs, gooseberries, grapefruit, grapes, guava, honeydew melon, kiwi, kumquat, lemons, limes, lychees, mandarins, mango, mulberries, nectarines, olives, oranges, papaya, passion fruit, peaches, pears, persimmon, pineapple, plums, pomegranate, quince, raspberries, rhubarb, strawberries, tamarind, tangerines, and watermelon.
�
Vegetables
�
Vegetables are a key component for methylation support because they provide many nutrients and flavonoids which are methylation adaptogens. Methylation adaptogens help regulate methylation status in the human body, particularly at our DNA level. These adaptogens have been demonstrated to prevent or reverse over-methylation as well as support healthy methylation activity. Moreover, dietary fiber is essential to promote a balanced microbiome as well as the efficient removal of toxins. The healthy microbes in our gut actually produce considerable amounts of methylation nutrients. But only when consuming a proper diet that includes fiber. Low-glycemic vegetables are an excellent source of fiber. Color variation will provide the most diverse amount of flavonoid methylation adaptogens.
The following list of vegetables can promote methylation support while those in bold are especially supportive of methylation activity, including; alfalfa sprouts, artichokes, arugula, asparagus, bamboo shoots, basil, beet leaves, beets, bok choy, broccoflower, broccoli, broccoli leaves, broccoli raab, rapini, broccoli sprouts, brussels sprouts, cabbage, capers, carrots, cauliflower, celeriac, celery, chicory, collard greens, daikon radish, dandelion greens, eggplant, endive, escarole, fennel, garlic, grape leaves, green beans, heart of palm, horseradish, jerusalem artichokes, jicama, kale, kohlrabi, lambsquarters, leeks, lettuces, mushrooms (all other), mustard greens, okra, olives, onions, parsnips, peppers, pumpkin, pumpkin Flower, purslane, radicchio, radish sprouts, radishes, rutabaga, scallion, sea vegetables (e.g. kelp, kombu, nori, bladderwrack, wakame), shallots, shiitake mushrooms, snap peas, snow peas, spinach, summer squash, sun-dried tomatoes, swiss chard, tomatillos, tomatoes, turnip greens, turnips, water chestnut, watercress, winter squash, yam, and zucchini.
�
Nuts and Seeds
�
Nuts and seeds are an important factor to improve DNA methylation. They are high in Omega-3 fatty acids, minerals, and B vitamins as well as fiber and antioxidants. Raw, unprocessed nuts and seeds, with skins where appropriate (e.g. almonds), are more densely concentrated with antioxidants.
The following list of nuts and seeds can promote methylation support while those in bold are considered methylation superfoods, including; almonds, Brazil nuts, cashews, chestnuts, chia seeds, flaxseeds, hazelnuts, hemp seeds, macadamia nuts, pecans, pine nuts, poppy seeds, pumpkin seeds, sesame seeds, sunflower seeds, and walnuts.
�
Legumes
�
Legumes can be valuable sources of a variety of methylation-associated nutrients, such as magnesium, potassium, folate, choline, and sulfur. They are also an excellent source of fiber to support a healthy microbiome.
Healthcare professionals recommend that you soak and sprout your legumes before cooking to improve their digestibility and nutrient bioavailability. This also reduces leptin levels, which can be helpful for people with gut symptoms and/or worsened autoimmune symptoms. You can do this by soaking the legumes overnight in plenty of water, then drain, rinse, and return them to their container. Leave loosely covered with a clean tea towel between 6 to 24 hours until you see tiny sprout ends starting to appear. They are now ready to cook.
The following list of vegetables can promote methylation support while those in bold are especially supportive of methylation activity, including; adzuki beans, black beans, black lentils, black-eyed peas, brown lentils, cannellini beans, fava beans, garbanzo beans, great northern beans, green lentils, kidney beans, lima beans, mung beans, navy beans, pinto beans, red beans, red lentils, soy/soybeans (especially fermented varieties such as tempeh, miso, tamari, natto, pickled tofu), split peas, and turtle beans.
�
Grains
�
Grains can also be an excellent source of magnesium, B vitamins and chromium, which helps regulate blood sugar levels. Some grains, such as oats, provide sulfur which can help decrease the depletion of methylation nutrients to support sulfur detoxification. Whole grains are also an excellent source of fiber. However, many individuals do not tolerate grains. Gluten-sensitivity or Celiac Disease, by way of instance, requires avoiding the consumption of grains with gluten, such as barley, bulgur, Kamut, regular oats, rye, spelt, and wheat. Grains, especially whole grains, also contain leptin, which some individuals may not tolerate. Moreover, the consumption of grains can make it difficult to control blood sugar levels.
If you are going to eat grains, always make sure to choose whole grains. Furthermore, decrease or completely avoid grains which have been ground into flour because the human body can absorb their glucose too rapidly when they have been milled. You can also soak your grains before cooking them to improve their digestibility and nutrient bioavailability. Some soaked grains, such as quinoa, can also be sprouted before cooking, to further improve their nutrient levels and help reduce their leptin content.
The following list of grains can promote methylation support while those in bold are especially good choices for methylation support, including; amaranth, barley, buckwheat, bulgur, corn, Kamut, millet, quinoa, oats, rice (basmati, bran, brown, wild), rye (dark rye), sorghum, spelt, tapioca, teff, and wheat.
�
Herbs and Spices
�
Herbs and spices are ultimately an important additional category of methylation adaptogens. As a matter of fact, they are extremely important and effective even in seemingly-small quantities. There are a variety of ways in which people can incorporate herbs and spices into their cooking, such as in marinades, rubs, dressings, drinks, and even sprinkled into and/or onto dishes.
The following list of herbs and spices can promote methylation support while those in bold are especially rich in methylation adaptogens, including; allspice, anise, basil, bay leaves, black pepper, caraway, cardamom, cayenne pepper, chamomile, chili, chives, cilantro (coriander leaves), cinnamon, cloves, coriander seeds, cumin, curry leaves, dill, fennel seeds, fenugreek, garlic, ginger, lemongrass, marjoram, methi, mint, mustard seeds, nigella seeds (black cumin), nutmeg, oregano, paprika, parsley, rosemary, sage, sumac, tarragon, thyme, turmeric, and vanilla bean.
�
DNA methylation is a fundamental process in charge of a variety of essential bodily functions. Many individuals, however, can develop methylation activity deficits which can tremendously affect their overall health and wellness. Supplements and medicines can be utilized to help improve DNA methylations but these may often cause several undesirable side-effects, A balanced nutrition can help safely and effectively treat these deficits and improve methylation support. The purpose of the following articles is to easily demonstrate what you can eat to improve DNA methylation from a variety of different food groups. Dr. Alex Jimenez D.C., C.C.S.T. Insight
�
Smoothies and Juices for Methylation Support
�
�
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
�
ProLon� Fasting Mimicking Diet
�
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
�
�
Many doctors and functional medicine practitioners can recommend nutritional advice and/or guidelines to help improve DNA methylation. Proper nutrition and lifestyle habits can ultimately help improve DNA methylation. In part 2 of this article, we will continue to discuss what you can eat to improve DNA methylation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
�
Additional Topic Discussion: Acute Back Pain
�
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
�
�
Formulas for Methylation Support
�
�
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
As a business owner at El Paso, Texas, Louie Martinez depends upon his general health to have the ability to execute his daily physical activities. And thanks to Dr. Alex Jimenez, a chiropractor in El Paso, Texas, Louie has found pain relief for a variety of wellness issues.
Louie describes how Dr. Jimenez has revived his wellness. Louie Martinez is thankful for the chiropractic care Dr. Jimenez has provided for him, and he highly recommends him as the non-surgical choice for many different health issues, including back pain and sports injuries.
El Paso Back Clinic
We are blessed to present to you El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend us.
Piano players will sit or stand at a piano or keyboard, often in the same position for hours. A clarinet player must keep their head, neck, and jaw in a precise position in order to play properly. A guitarist must sit for long periods while holding the guitar in a certain position while moving their fingers over the frets in a very precise manner.
In other words, musicians put their bodies through some vigorous training. They practice for hours a day and engage their bodies in repetitive motions for long periods of time.
It’s no wonder that many musicians complain of headaches, migraines, carpal tunnel, clicking jaw, numbness in the fingers, and back and neck pain!
Some of this pain can be debilitating and make it more difficult for them to perform their normal activities. Many live with chronic pain.
There was a time when these conditions were considered to be just a part of playing an instrument and the musician would push through the pain. However, many are turning to chiropractic and are enjoying not only a pain-free life but improved performance as well.
The Way Playing an Instrument Affects the Body
Some doctors liken musicians to athletes � instrumental athletes. They do have very similar practices such as practicing for hours a day so that they can perfect their abilities and skills. And like athletes, they also experience certain break downs within the body.
Posture is a common malady as the musician may stand or sit a certain way in order to play their instrument. This prolonged activity can lead to imbalances in the spine, pelvis, and other parts of the body.
When the body is not in balance, it cannot function as it should. Organs are affected and other the body may try to make accommodations for the imbalance which only exacerbates the problem.
This is further compounded each time the musician plays their instrument because by doing so they are consistently underworking and overworking certain muscles. This can lead to further imbalance.
The muscles that are worked, the ones used to play the instrument, get shorter, tighter, and stronger as scar tissue forms. By contrast, the underworked muscle groups stay underdeveloped and get weak. This muscular imbalance puts a great deal of stress on the spine and other joints in the body like the fingers, wrists, and elbows
They may also experience Repetitive Strain Injury or RSI. This condition is often quite painful and is concentrated in the soft tissues, nerves, tendons, and muscles.
These areas may become painful or inflamed when performing repetitive activities, pressing against hard surfaces, vibrations, awkward sustained positions, and forceful exertions. This causes the body to become out of alignment but also impacts the function of the skeletal system, nervous system, and muscular system.
Chiropractic
Chiropractors are very good for musicians because the can assess misalignments in their spine and make adjustments. When proper original alignment is stored to the body, it begins to function properly. This leads to a decrease in pain and other symptoms that may be experienced due to the long hours of playing an instrument.
Musicians also benefit from chiropractic because it can make them better at what they do. When the pain is decreased or eliminated and the other symptoms are relieved, it is easier to play.
When the spine is in proper alignment and the body is balanced, the musician will experience a boost in energy, their muscles will not fatigue as quickly, and their muscles will be more relaxed. With all those benefits, it�s no wonder that chiropractors and musicians make beautiful music together.
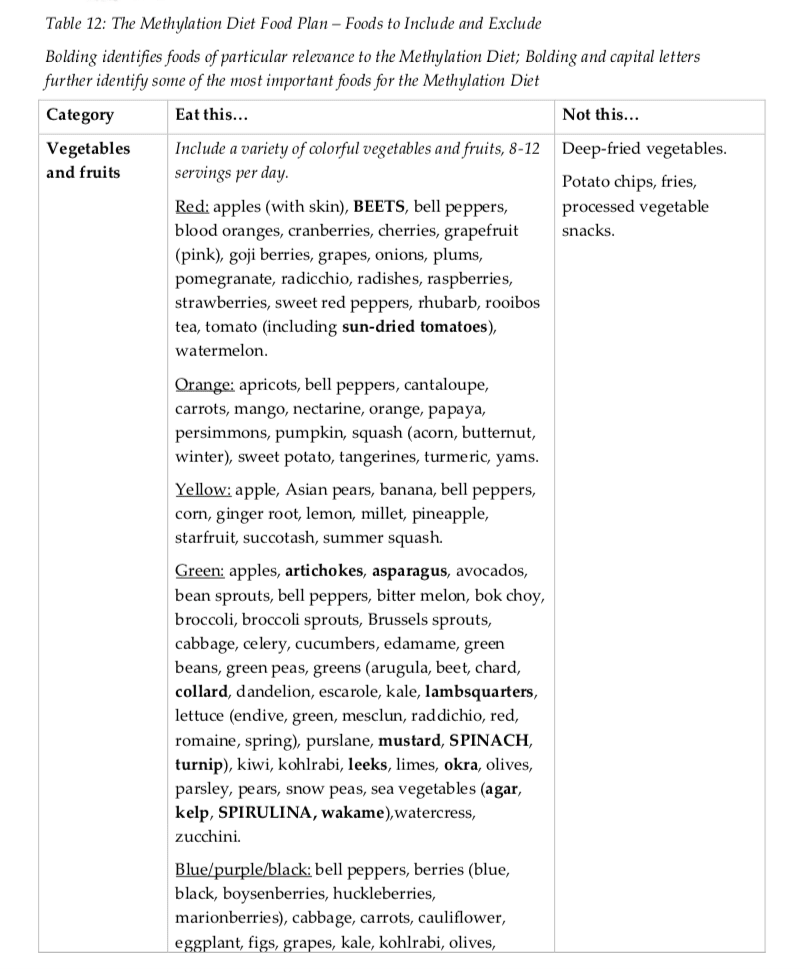
As demonstrated in previous articles, research studies have determined that promoting methylation support with nutrition by following a diet food plan includes different nutrient needs and avoids factors which can negatively affect DNA methylation status and activity. A diet food plan for methylation support should be nutritionally replete, anti-inflammatory, low-glycemic, antioxidant-rich, and supportive of detoxification processes.
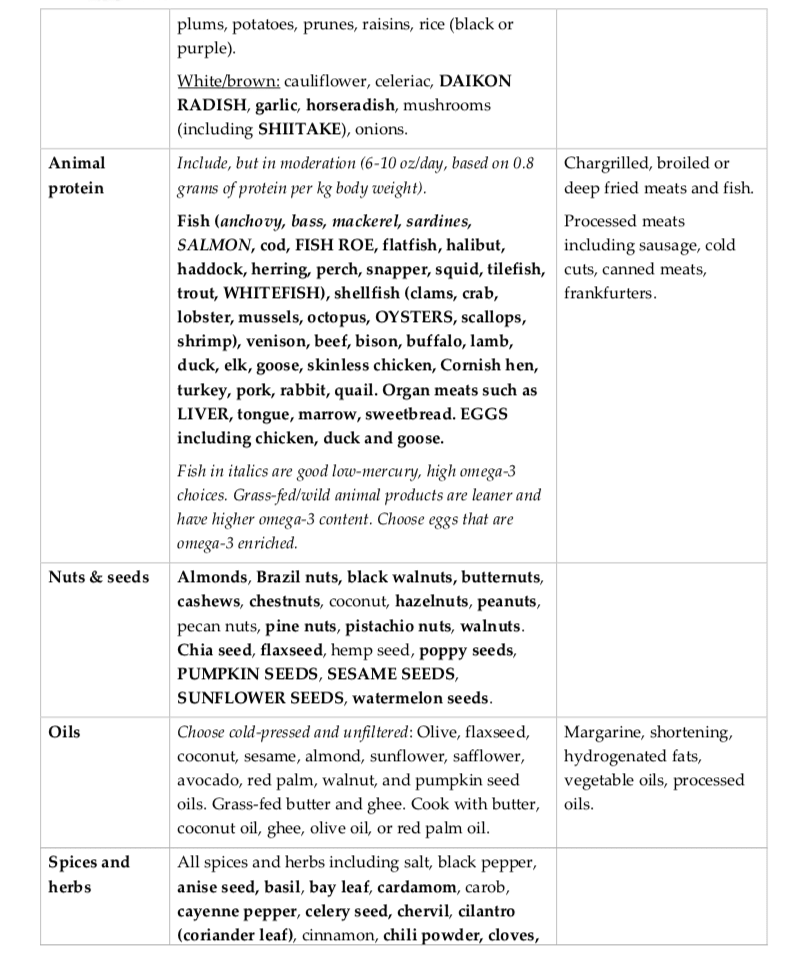
A balanced diet consisting of fruits, vegetables, legumes, nuts, seeds, complete proteins, and whole grains can help provide enough nutrients to support optimal methylation. Moreover, superfoods, such as beets, spinach, sea vegetables, daikon radish, shiitake mushrooms, salmon, fish roe, whitefish, oysters, eggs, pumpkin seeds, sesame seeds, and sunflower seeds, provide increased levels of nutrients for DNA methylation. Organ meats, such as liver, are also good sources of nutrients, including vitamin B2, B3, B6, folate, choline, and betaine, to promote methylation support.
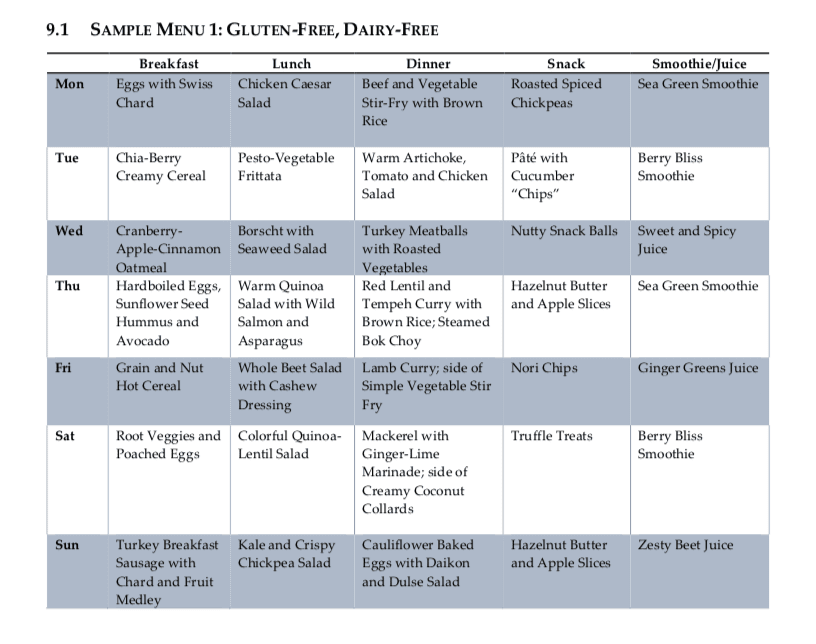
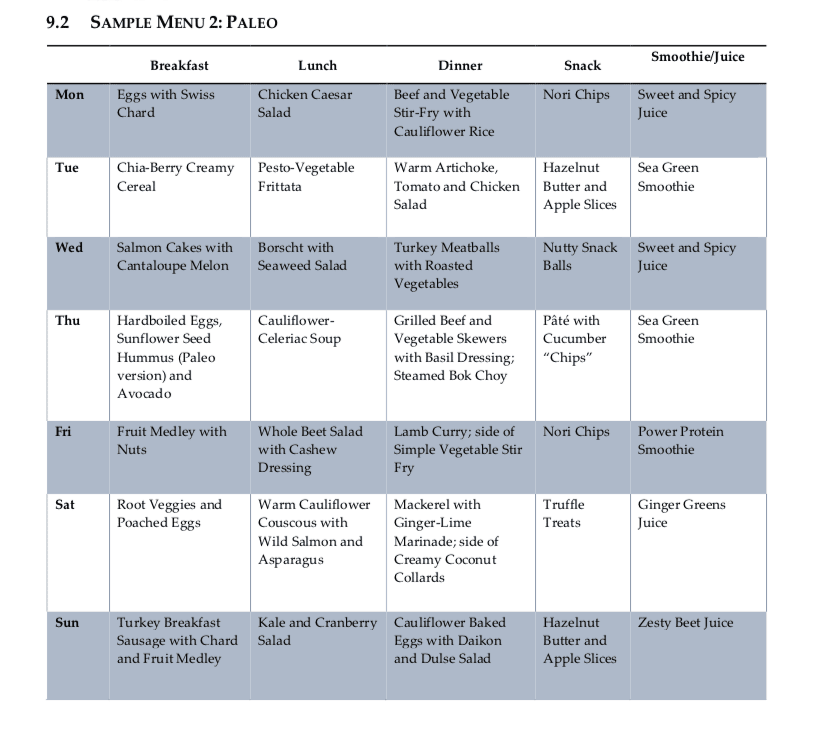
Following a diet food plan is essential to continue to achieve proper nutrient intake. Even “healthy” diets can be lacking in nutrients or they may fail to provide treatment nutrient levels if they are utilized incorrectly. Healthcare professionals can also recommend regular nutrient intake evaluations, especially in the early stages of following a diet food plan, to make any changes which may be required to optimize a patients methylation support and help promote overall health and wellness. The following menu plans (Table 9.1 and 9.2) offer guidelines of what patients can eat throughout their day to improve methylation through nutrition.
Menu Plan Samples for DNA Methylation
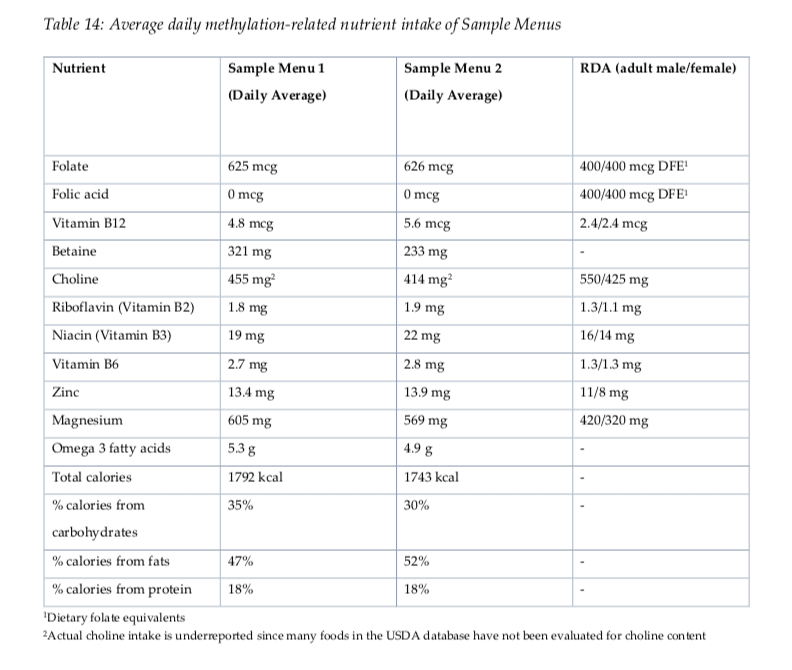
Evaluating Nutrients in Menu Plans
Both menu plan samples provided above demonstrate a wide variety of nutrients which are ultimately essential for DNA methylation status and activity (Table 14). Doctors and functional medicine practitioners may also recommend regular nutrient intake evaluations on patients following a long-term, diet food plan to make sure that patients are able to maintain appropriate levels of nutrient intake throughout the treatment. It’s essential for patients to communicate accordingly with their healthcare professionals so they can customize their diet food plan as necessary.
Supplements and medications used to promote methylation support may often cause side-effects if they’re not managed accordingly by doctors and functional medicine practitioners. A diet food plan is a safe and effective alternative treatment option which can help promote methylation support without the side-effects of supplements and medications. In addition, a qualified doctor and functional medicine practitioner can customize a patient’s diet food plan and provide advice and guidelines to help promote overall health and wellness. Menu plan samples, such as those provided in the article, are several examples of a diet food plan which can help improve methylation status and activity. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many doctors and functional medicine practitioners can recommend nutritional advice and/or guidelines to help improve DNA methylation. Proper nutrition and lifestyle habits can ultimately help improve DNA methylation. Following menu plans or samples can promote methylation support. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download* All the above XYMOGEN policies remain strictly in force.
Individuals with Bell�s Palsy are faced with limited treatment options. As the condition affects everybody differently, there is no cure-all treatment.
Steroids such as prednisone are often prescribed, but many harmful side effects are possible. Massage and physical therapy may also be used, but results may vary. Chiropractic care is a noninvasive, medication-free way to treat Bell�s Palsy. Here are several studies that prove it.
Bell�s Palsy?
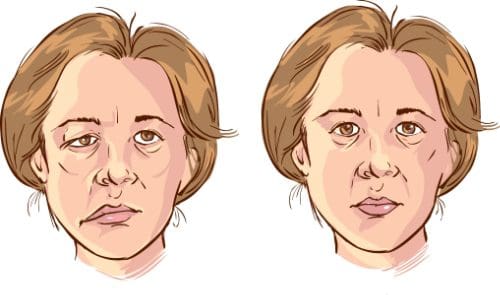
Bell�s Palsy is a condition that is marked by temporary facial paralysis due to trauma or damage done to the nerves in the face. The facial nerve, called the 7th cranial nerve, resided in the skull, traveling through the Fallopian canal (a bony, narrow canal in the skull) and extending from just under each ear to the muscles that are located on either side of the face.
This nerve is mostly in a hard, bony shell with just small portions that are exposed, allowing it to move the muscles on each respective side of the face. The facial nerve controls the mouth (smiling, forming words, etc.), closing the eyelids or blinking, frowning, and similar movements. It also transmits nerve impulses to the saliva glands, tear glands, taste sensations, and the muscles of the stapes (small bone located in the middle ear)
Bell�s Palsy affects the facial nerve, disrupting its function so that messages from the brain cannot reach the associated muscles. This results in facial paralysis or weakness.
This condition is not related to stroke, although some people may mistake it for a symptom of stroke. It usually only affects one side of the face. Incidences of Bell�s Palsy affecting both sides of the face at the same time is very rare.
Bell�s Palsy Symptoms
Bell�s palsy symptoms can vary widely from patient to patient, depending on severity. Some common symptoms include:
Paralysis on one side of the face
Weakness on one side of the face may range from mild to severe
Muscle twitching in the face
Drooping of one corner of the mouth
Drooping on the eyelid on one eye
Drooling
Dry eye
Dry mouth
Excessive tearing that occurs in only one eye
Impaired sense of taste
Discomfort of pain behind the ear and around the jaw
Tinnitus (ringing in the ears) � can be one ear or both
Sound hypersensitivity on the side that is affected
Headache
Impaired or slurred speech
Difficulty drinking or eating
Dizziness
The symptoms usually come on suddenly and progress fairly rapidly, reaching their full effect within about 48 hours. It can leave the face very distorted during the time that the patient is experiencing a flare-up or symptoms.
Bell�s Palsy Care
Milder cases of Bell�s Palsy are typically not treated and the symptoms will subside on their own in 10 to 14 days. More serious cases may require medical intervention such as medications like the steroid prednisone, acyclovir, and even ibuprofen or acetaminophen.
In severe cases where the eye is affected, the patient may not be able to close the eyelid so protecting that eye is a necessity as is keeping it from drying out by using lubricating eye drops. Facial massage, physical therapy, and acupuncture may also be used. Surgery for Bell�s Palsy is very rare due to its controversial nature.
The Causes of Bell�s Palsy?
The cause of Bell�s Palsy is not known. Doctors do know that it is the result of the facial nerves becoming inflamed, swollen, or compressed, but why this happens is still a mystery.
Some researchers speculate that a viral infection could be the culprit. The theory is that an illness like the common cold sore virus or viral meningitis causes the nerves to become inflamed and swell in the Fallopian canal. This causes pressure on the nerve, cutting off the oxygen and blood supply to its cells.
Some common conditions that Bell�s Palsy has been associated with include:
Chronic middle ear infection
Sarcoidosis
Lyme disease
The flu or illnesses that are similar to the flu
High blood pressure
Tumors
Headaches
Diabetes
Facial injury
Skull fracture
Chiropractic Care
Case studies show that chiropractic for Bell�s Palsy is very effective. In some cases, the patient sees results almost immediately.
The chiropractor traditionally will deliver a chiropractic adjustment to the cervical spine. It is a safe treatment and generally works faster than other Bell�s Palsy treatments, including medication.
According to research studies, methylation support through nutrition involves using a diet food plan which includes different nutrient needs and avoids factors that can negatively affect DNA methylation. A diet food plan for methylation support should be nutritionally replete, anti-inflammatory, low-glycemic, antioxidant-rich, and supportive of detoxification processes.
A balanced diet of fruits, vegetables, legumes, nuts, seeds, complete proteins, and whole grains provides enough nutrients for methylation. Superfoods, such as beets, spinach, sea vegetables, daikon radish, shiitake mushrooms, salmon, fish roe, whitefish, oysters, eggs, pumpkin seeds, sesame seeds, and sunflower seeds, provide increased levels of nutrients for DNA methylation. Organ meats, such as liver, are also good sources of nutrients, including vitamin B2, B3, B6, folate, choline, and betaine.
Nutrition for DNA Methylation
Bioactive chemicals and substances in food can affect DNA methylation, which generally appear to be site-selective and dose-dependent. By way of instance, phytochemicals like selenium have been demonstrated to limit the production of DNMT enzymes. These include compounds found in plant foods, such as apigenin, betanin, biochanin A, caffeic acid, catechin, chlorogenic acid, coumaric acid, curcumin, cyanidin, daidzein, ellagic acid, epicatechin, epicatechin gallate, epigallocatechin, epigallocatechin 3-gallate or EGCG, galangin, genistein, hesperidin, luteolin, lycopene, myricetin, naringenin, quercetin, resveratrol, rosmarinic acid, and sulforaphane.
One of the processes affecting the anti-cancer benefits of compounds, such as genistein, anthocyanins and green tea polyphenols, includes the selective de-methylation of the promoter regions in tumor suppressor genes. Bioactive chemicals and substances in food have been demonstrated to regulate gene expression in processes, such as Phase I and Phase II detoxification. Moreover, including whole, colorful, and varied plant foods in the diet may help benefit nutrient status, anti-inflammatory, and anti-oxidant effects, as well as DNA methylation and epigenetic expression.
Oxidative stress can be further reduced in the diet by avoiding food preparation techniques that promote the development of pro-oxidative advanced glycation end products. Advanced glycation end products develop when animal-derived foods are cooked in high, dry heat. Their development can also be tremendously reduced by cooking at lower heats with moisture. Proper hydration is also an important factor in reducing oxidative stress. Phytonutrients are fundamental because of their function as beneficial enzyme regulators as well as powerful antioxidants.
Calorie restriction may frequently be recommended because it is believed to slow or reverse the age-related decline in global DNA methylation. Calorie restriction has also been demonstrated to help regulate the methylation of genes associated with diseases like cancer. Together with a low carbohydrate diet, an extended night-time fast, such as by finishing all food intake by 7 pm, can trigger the production of ?-hydroxybutyrate, an important ketone body which may ultimately have protective effects on the epigenome and may provide considerable anti-inflammatory effects.
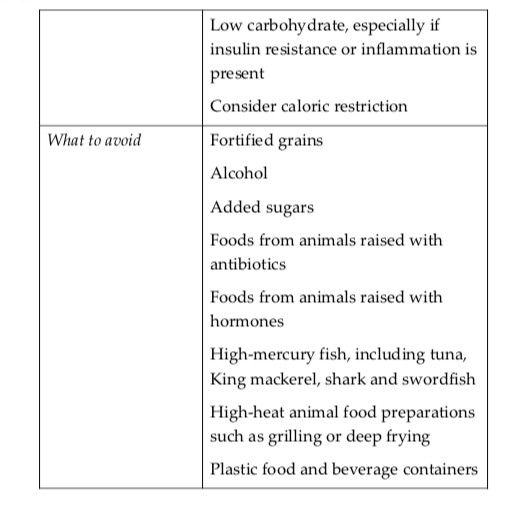
While doctors and functional medicine practitioners can commonly utilize short-term, targeted ketogenic diets due to their anti-inflammatory and weight loss results, it should be noted that a full ketogenic diet, although recommended as an effective treatment for epilepsy and certain cancers, may not be suitable for long-term methylation support due to the restriction on amino acid intake that can decrease overall methionine status. Furthermore, fortified grains should be reduced or eliminated, especially if methyl donors are not tolerated. Alcohol is inadvisable because it produces unfavorable DNA methylation patterns which may interfere with SAMe activity and prevents folate metabolism through MTR enzymes.
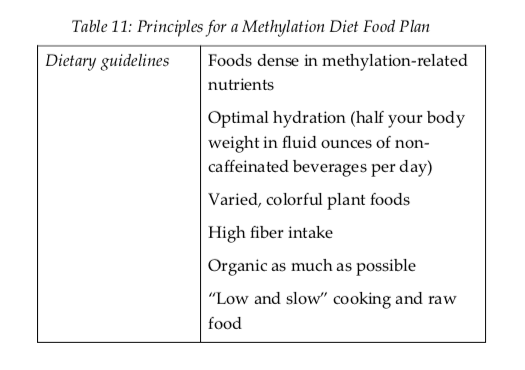
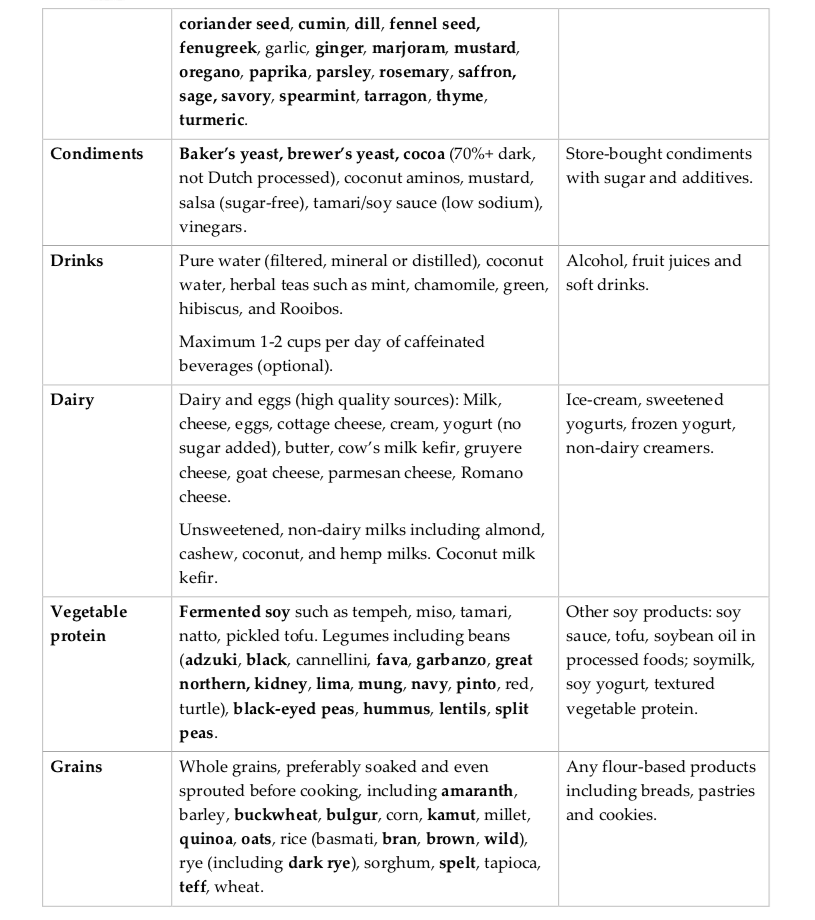
Further details of the diet food plan for methylation support is demonstrated in Table 12 below, which shows what foods to include, and what foods to exclude to ultimately help improve DNA methylation status and activity. Bolded foods are especially notable for their contribution to methylation-associated nutrients. Bolded and capitalized foods are the most significant contributors to methylation-associated nutrients. The following case discusses how a combination of diet, supplements, and lifestyle habits can help decrease homocysteine and improve overall health and wellness.
Case 2.0: Lowering Homocysteine with a Combination of Diet, Supplements, and Lifestyle Habits
Susan described feeling healthy until she gave birth to her first child. felt that she had been healthy up until having her first child. Now postmenopausal at age 57, she was currently diagnosed with latent autoimmune diabetes of adults, or LADA, and Hashimoto�s thyroiditis. Her blood glucose was 335 ng/dL, with an HbA1C of 12.1. Susan’s treatment was multi-faceted, customized to address the various underlying factors which were associated with these health issues, among other common concerns.
Her initial program included a low carbohydrate, anti-inflammatory diet and micronutrient for gut repair, detoxification, and blood sugar control. A modest methyl donor prescription included 400 mcg 5- mTHF and 1000 mcg methyl-B12. At two months, Susan�s blood sugar was 108. However, her homocysteine was 14.0. She was also characterized as heterozygous for both the MTHFR 677 and 1298 mutations. These findings helped healthcare professionals develop diet food plans for methylation support. Methyl donor prescription was modestly increased to 800 mcg 5-mTHF and 5000 mcg methylcobalamin.
Susan started a gluten-free, dairy-free, diet food plan which also addressed her ongoing needs for blood sugar control, curbing inflammation, and balancing immune function. This helped Susan emphasize foods rich in methylation nutrients, such as leafy greens, beets, daikon, shiitake, spinach, seeds, and high-quality protein. One of the main challenges for Susan was her frequent business travels to Asia. Careful advice and guidelines for navigating restaurant food as well as dry food supplies to take with her for meal replacements and snacks as needed, helped her continue to follow the diet food plan. Guidance for reducing mercury exposure in food, as her mercury levels were initially too high and she did have remaining amalgams which also contributed to that result, and participating in �clean� living and stress management techniques, promoted her diet food plan.
Four months after her evaluation, her lab tests demonstrated remarkable results. Her fasting blood glucose went down to 82 and her homocysteine is at 7.1. Susan reports feeling very well and is motivated to continue following the diet food plan as well as following through with the recommendations the healthcare professionals recommended to her.
Following a diet food plan is fundamental to continue to ensure desired levels of nutrient intake. Even “healthy” diets can be lacking in nutrients or they may fail to achieve enough treatment nutrient levels if they are utilized incorrectly. Healthcare professionals also recommend regular nutrient intake evaluations, especially in the early stages of following a diet food plan, to make any adjustments which may be needed to optimize a patients methylation support and help promote overall health and wellness.
As previously discussed in other articles, supplements and medications can be utilized to help improve DNA methylation, however, these may often cause a variety of side-effects if they’re not monitored carefully by healthcare professionals and patients. The use of a diet food plan is a safe and effective alternative which can help promote methylation support naturally without the side-effects of supplements and medications. In addition, a qualified doctor and functional medicine practitioner can customize a patient’s diet food plan and provide advice and guidelines to help promote overall health and wellness. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there�are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many doctors and functional medicine practitioners can recommend nutritional advice and/or guidelines to help improve DNA methylation. Proper nutrition and lifestyle habits can ultimately help improve DNA methylation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
https://youtu.be/Pdn9FEoUjMA
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
When seasons change, you may notice some pain in your joints. Fortunately, there is chiropractic care that can help. When people hear chiropractic care they usually think of spine problems and back pain. This is true, but chiropractic medicine treats many conditions other than spine pain.
Chiropractic can be used for joints all over the body, including ankles, knees, shoulders, hips, and wrists. It is a natural, whole-body approach to health care and wellness as a very effective way to manage chronic joint pain such as arthritis, or joint pain due to injury.
What Causes Joint Pain and Immobility?
There are several reasons that a joint may become painful and immobile. Injury or trauma to the joint, such as a fall, being hit while playing sports, or being involved in a car accident, can cause injury. Microtrauma occurs due to a repetitive use injury such as working on an assembly line or using a computer all day, can also cause damage resulting in pain.
Sometimes an inflammatory diet can cause problems and stress can also certainly be a factor. Stress affects the entire body, including its chemicals and hormones that can lead to joint damage or weakness, making you more prone to injury.
Finally, age may be a factor. As we get older, our bodies don�t hold up like they once did. This can mean joint pain and decreased range of motion. The colder months can instigate pain in the major joints, including the knees, back, hips, and shoulders.
Why does Cold Weather Exacerbate Joint Pain?
The short answer to this is that researchers aren�t really sure. One of the most popular theories is that low-pressure systems typically accompany the cooler temps. The lower pressure can cause the tissues in already sensitive joints to expand, creating a perfect environment for inflammation including aches, tenderness, decreased range of motion, and swelling.
Other factors that may also affect joint pain in cooler weather are low-level dehydration, a sedentary lifestyle, and depression or �the blues.� Low-level dehydration is more common than you may think; most people do not have adequate water intake.
Sodas don�t count as hydration and this can be a real problem. Generally, people don�t hydrate as much when the weather is cool � or not as much as they did during the warm summer months.
When the weather cools down people become less active, especially if there is snow and ice on the ground. Lack of exercise can lead to serious joint troubles.
Depression can also impact your entire body, including your joints. Many people suffer from Seasonal Affective Disorder or SAD. Doctors believe that it occurs because of the shorter days and generally darker skies during the winter months. Depression and anxiety have strong ties to chronic pain as a whole, including joint pain.
How Chiropractic Helps Relieve Joint Pain
Chiropractic provides an all-natural, holistic approach to health care and pain management. It does not use medications or invasive medical procedures.
The chiropractor usually begins by aligning the spine, which is called an �adjustment.� This brings the body back into alignment so that it can function more efficiently and with less pain. The patient may also be given recommendations on lifestyle changes, dietary adjustments, exercise, and supplements.
When the body is aligned, the entire system is balanced. This allows the body to work at a more optimal rate. As a result, the range of motion improves and the pain is decreased or even completely eliminated.
Involvement in a car crash is an unfortunate situation that can result in various automobile accident injuries. People suffering from whiplash, neck pain, and back pain due to an auto accident can struggle to continue their regular activities. Dr. Alexander Jimenez is a personal injury chiropractor who focuses on treating automobile accident injuries, among other health issues.
Patients describe how their quality of life was affected after a car crash and discuss how chiropractic care with Dr. Jimenez helped them recover their overall health and wellness. The patients highly recommend Dr. Alex Jimenez as the non-surgical choice for personal injuries and auto accident injuries, among other health issues, such as whiplash, neck pain, and back pain.
El Paso Back Clinic
https://youtu.be/1MFwLhYbTRU
We are blessed to present El Paso’s Premier Wellness & Injury Care Clinic to you.
As El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we are passionately focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend us.
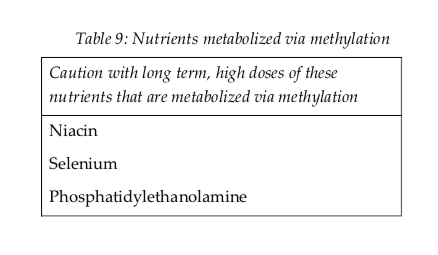
According to research studies, understanding possible nutraceutical interactions for methylation support with the utilization of long-term supraphysiological supplementation of niacin, selenium, and phosphatidylethanolamine can ultimately help promote overall health and wellness. Doctors and functional medicine practitioners must be aware of the nutraceutical interactions for methylation through supplementation.
Nutraceutical supplements utilized in integrative functional medicine as well as in nutrition practice can have tremendously powerful effects on physiology. Nutraceutical supplements are one of the primary tools which healthcare professionals utilize to help their patients achieve optimal well-being. However, as mentioned above, healthcare professionals must be aware of possible nutraceutical interactions, especially those which may negatively affect methylation. These are listed in Table 9 below.
Nutrients are metabolized in the human body through methylation, such as niacin, selenium, and phosphatidylethanolamine. Therefore, high dose supplemental regimens of these nutrients can ultimately decrease available methyl donors and cause a methylation deficit. Niacin can also prevent the production of pyridoxal kinase, which is generally known to trigger vitamin B6. High doses of this nutrient may affect overall vitamin B6 status.
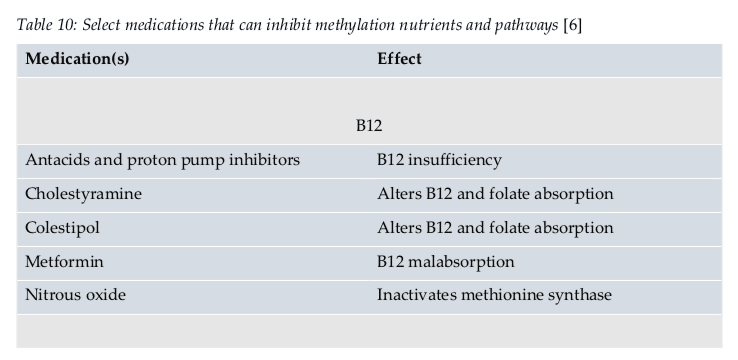
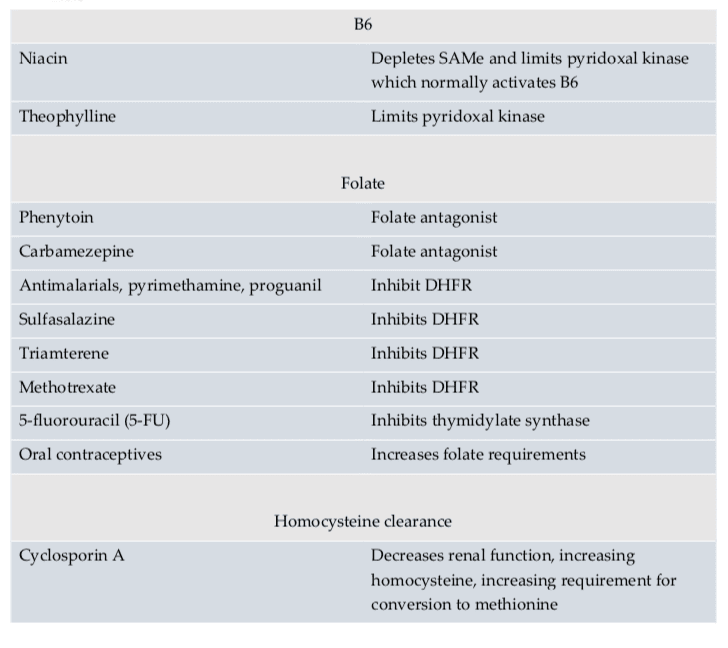
Medication Interactions
According to research studies, doctors and functional medicine practitioners must also understand possible medication interactions for methylation support. Moreover, healthcare professionals must be aware that medication interactions can ultimately affect methylation status. Several medications have been demonstrated to affect methylation status in a variety of ways. Several medications may even prevent proper nutrient absorption, while several others may restrict enzyme function, and several others still may decrease SAMe. An understanding of these medication interactions is essential to promote optimal methylation support.
Doctors and functional medicine practitioners can recommend a variety of supplements and/or medications to promote methylation support, however, these can also cause a variety of side-effects on every individual. Healthcare professionals must be aware of these nutraceutical and medication interactions and their use must be carefully considered for each patient. Nutrition and lifestyle habits are safe and effective treatment options which can help promote methylation support without the chance of developing side effects.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many healthcare professionals can recommend a variety of nutraceutical and medication interactions to help improve DNA methylation. Proper nutrition and lifestyle habits can ultimately help improve DNA methylation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
In the same ways that it helps human patients, it also helps animals. It offers a less invasive, medication-free way to manage pain and correct many health issues, including arthritis and joint injuries. A number of pet owners claim chiropractic is not only great for their pets but that their pets are excited to go to appointments and see their chiropractors.
Which animals benefit from veterinary chiropractic care?
Any species of animal can benefit from chiropractic. The most common animals to receive this specialized type of care are dogs, cats, and horses. However, any vertebrate species, including birds, can reap the benefits.
Chiropractic for animals has long been a standard form of treatment with many show horses, race horses, and barrel racers. It is considered a viable, beneficial treatment to help the animals combat the stress their bodies are put under due to their jobs. It is also very good for injuries, speeding healing while managing pain.
It is often used on dogs and cats to help with injuries, arthritis, and aging. Sometimes an animal can hurt but they are unable to communicate that to their owners. If you notice behavioral changes or grumpiness, you may want to check your pet out. He or she may be hurt and can�t tell you � and chiropractic could be the answer.
Most often treated conditions
Veterinary chiropractic helps pets with many conditions that are biomechanical or neurological in origin � much like it helps humans. Some of these conditions include spondylosis, hip dysplasia, and other types of degenerative joint diseases, intervertebral disk disease, neck pain, back pain, and cervical instability. It can also address problems of the autonomic nervous system like musculoskeletal weakness, fecal and urinary incontinence, chronic neck and back pain, and other pain that don�t respond to conventional treatments.
Serious injuries like ligament tears or fractures may require surgical intervention, but chiropractic can help post-surgery. It can help relieve the pain as well as correct secondary problems that could occur due to the animal overcompensating in response to the injury. In performance animals, regular chiropractic care can help prevent injury by maintaining flexibility and a good range of motion.
How does it work?
Chiropractic is designed to help keep the joints and spine in their natural, healthy alignment. The nerves that surround the joints and run along the spine communicate with the central nervous system. This connects to all of the organs in the body, including the brain.
When the spine is out of alignment, even just a little, it can cause disruptions in how the messages are relayed through the central nervous system and to the organs and brain. A misaligned spine can affect the entire body, causing pain in muscles and joints, affecting organ function, and impact the animal�s overall health and wellbeing. When the spine is not aligned, the body will not function as it should.
Give the best possible chiropractic experience.
When you meet with the veterinary chiropractor, make sure that you have all of your pet�s information available, including vaccinations, health care history, any conditions they have, their diet (including supplements), medications they are taking, and their daily activities. If the doctor is treating an injury, explain how the injury occurred if you know.
When the adjustment is over, make sure that you understand any therapy or exercises to do at home, post adjustment. If there is something you don�t understand, ask. The doctor may also provide recommendations regarding lifestyle changes including saddle fit, collar fit, exercise, conditioning, or shoeing. Make sure you follow these as well. Your pet can�t make those decisions for his or her own health, that is up to you. Don�t let them down.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine