The body needs the energy to get through the entire day. Energy can come in various foods consumed and converted into three molecules: carbohydrates, proteins, and fats. Carbohydrates convert into glucose, which becomes energy used for bodily function. At the same time, protein helps repair and build body tissues that allow metabolic reactions and coordinate physical function. Healthy fats in the body help support cell function, provide energy, and produce essential hormones that the body needs. When the body has too much glucose, it can cause various metabolic factors to take over the body, resulting in metabolic disorders associated with chronic conditions over time. This is known as insulin resistance and today’s article looks at how insulin resistance is detected, the signs and symptoms, and treatments to manage insulin resistance. We refer patients to certified providers specializing in metabolic treatments to help many individuals with insulin resistance. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
How Is Insulin Resistance Detected?
Have you been feeling a tingling sensation along your hands and feet? Have you been experiencing headaches that go away when you eat food or drink something? Do you constantly go to the bathroom? Many of these issues are signs that you might be at risk of developing insulin resistance. Insulin resistance is an impaired biological response in the body that requires insulin stimulation to the targeted tissues: the liver, muscle, and adipose tissue. The liver supplies the glucose to the body by secreting it into the bloodstream to be used for energy. So when there is a high glucose level in the bloodstream, the pancreas, which is between the liver and the stomach, sends out insulin to help the glucose be absorbed into the body cells. Many individuals don’t realize their insulin levels are high until they go in for routine check-ups with their primary physicians.
The Signs & Symptoms Of Insulin Resistance
Various factors could lead to insulin resistance when the body has high glucose levels in the bloodstream. Many individuals do develop habits that do contribute to insulin resistance. Some of the signs that indicate that a person may have insulin resistance include:
Excess body fat
Physical inactivity
High-carb diet
Hormone disorder
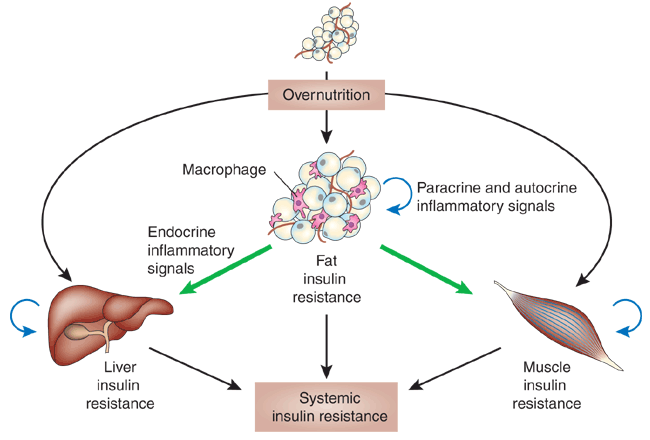
Studies reveal that obesity is considered the triggering factor for individuals with insulin resistance associated with diabetes. Since obesity is a factor that escalates the pathogenesis of diabetes through the stimulation of insulin resistance. When the body becomes overstimulated, the body starts to release elevated levels of pro-inflammatory cytokines that can lead to various abnormalities like organ dysfunction and tissue injury associated with insulin resistance. Studies show that chronic low-grade inflammation associated with obesity is responsible for the body to have a decrease in insulin sensitivity. Some of the risk factor symptoms related to insulin resistance include:
Increased thirst and hunger
Blurred vision
Obesity
Gut inflammation
Weight gain
Fatigue
Acanthosis nigricans
Numbness or tingling sensation on hands and feet
Thyroid issues
Metabolic syndrome
What Is Insulin Resistance-Video
Have you been feeling a tingling sensation on your hands or feet? Have you noticed your midsection becoming more prominent than normal? Or have you been feeling depressed or constantly more tired than usual? Many of these symptoms are signs that you could be at risk of developing insulin resistance. The video above explains insulin resistance and how it affects the body. Many symptoms like obesity and inflammation do play a factor in contributing to insulin resistance associated with weight gain. Studies reveal the association between obesity and insulin resistance through the link between visceral adipose tissue accumulation in the liver. When there is an accumulation of excess lipids in the liver makes the visceral adipose tissue prone to inflammatory cytokine production, which then contributes to insulin signaling impairment. Fortunately, there are available treatments to help manage insulin resistance.
Treatments To Manage Insulin Resistance
Some treatments available to manage insulin resistance can help many individuals feel better by making small changes in their lifestyle habits. Many individuals utilize the Mediterranean diet as it has many beneficial properties in lowering insulin resistance and managing diabetes by incorporating healthy polyunsaturated fatty acids from olive oil and seeds, resveratrol from grapes, and other anti-inflammatory foods to reduce inflammation associated with insulin resistance. Since other symptoms are associated with insulin resistance, like metabolic syndrome, getting a chiropractic adjustment may help lower the effects of inflammation associated with metabolic syndrome and manage insulin resistance. Chiropractic care is commonly used for musculoskeletal issues; however, since metabolic syndrome is a mediator for musculoskeletal problems like neck pain, shoulder pain, and back pain, it can make the body dysfunctional. To that point, it becomes a cross-link for insulin resistance, causing the body to have reduced mobility. Chiropractic care uses spinal manipulation to adjust the subluxation or spinal misalignment in the body and help improve mobility back to the joints.
Conclusion
The body needs the energy to get through the entire day by consuming various foods. When these foods are consumed, they are converted into three molecules:
Carbohydrates convert to glucose for bodily function.
Protein repairs and builds muscle tissues.
Healthy fats produce essential hormones and support cell function.
Watching the foods we consume can help us in the long run. When the body has too much glucose in its system, it can lead to insulin resistance and cause various metabolic factors like obesity and weight gain, resulting in metabolic disorders associated with chronic conditions. Insulin resistance can affect the body over time if not treated right away. Incorporating a healthy diet like the Mediterranean diet, chiropractic care, and physical activities into a person’s lifestyle can help manage insulin resistance from escalating to dangerous levels like diabetes affecting a person’s life.
References
Chen, Li, et al. “Mechanisms Linking Inflammation to Insulin Resistance.” International Journal of Endocrinology, Hindawi Publishing Corporation, 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4468292/.
Freeman, Andrew M, and Nicholas Pennings. “Insulin Resistance – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 4 July 2022, https://www.ncbi.nlm.nih.gov/books/NBK507839/.
Hardy, Olga T, et al. “What Causes the Insulin Resistance Underlying Obesity?” Current Opinion in Endocrinology, Diabetes, and Obesity, U.S. National Library of Medicine, Apr. 2012, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4038351/.
Wondmkun, Yohannes Tsegyie. “Obesity, Insulin Resistance, and Type 2 Diabetes: Associations and Therapeutic Implications.” Diabetes, Metabolic Syndrome and Obesity : Targets and Therapy, Dove, 9 Oct. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7553667/.
Everybody understands that exercise is necessary for optimal physical and mental health. Beginning a workout routine can be simple, but sticking with it long-term is the challenge. Knowing how to stay motivated can be overwhelming when facing various fitness options. Understanding the benefits of exercise and identifying the most significant motivating factors will help stick to the fitness plan.
Benefits of Exercise
The first step is identifying why you want to start exercising and the principal motivator/s. For most individuals exercising regularly helps:
Contribute to weight loss
Decrease risk of disease
Increase lifespan
Improve the quality of life
Improve mental health
Sticking to a plan tends to dissolve after a few months without serious motivation. It is recommended to focus on making the why as specific and personal as possible. The more specific the why, the less likely the individual will stray from the plan. For example, a middle-aged father wants to get and stay in shape because he wants to keep up with his kids and set a healthy example.
Starting Out
A small amount of regular exercise positively affects the body’s health. This is a common cause of burnout and is not necessary. Those who have never exercised or worked out regularly are often tempted to start with intense hours-long exercise routines.
Current physical activity recommendations suggest at least 150-300 minutes of moderate-intensity exercise per week or
That means that 30 minutes a day of moderate exercise/activity or 15 minutes a day of vigorous exercise/activity is the recommended amount to see and feel health benefits like improved metabolism and mental health.
Getting the body physically fit is a long-distance marathon, not a quick sprint.
Consistency is the objective.
Increasing the frequency and/or duration of workouts is fine, but doing it in a way where the exercise is still enjoyable and not a chore is recommended.
Individuals who work out too hard and need to rest for a few days risk losing motivation.
Daily Activities
Becoming more active throughout the day outside of the workout regimen is recommended to increase physical activity levels and build and reinforce healthy habits. If exercising is too strenuous for the individual, start with increasing physical daily activities. This is an effective way to ease into regular exercise. Examples of physical activities include:
Developing healthy habits, physical and nutritional are the goals, which is why it is essential to find an exercise approach that doesn’t lose its appeal and continues to develop. One study found that working out with friends or joining group sports can generate greater enjoyment. There are a variety of activities that can include:
Structured workouts
HIIT
Yoga
Pilates
Strength training
Cycling
Running
Biking
Hiking
Organized sports leagues:
Soccer
Basketball
Softball
Volleyball
Tennis
Golf
Low-impact options:
Walking
Stretching
Water aerobics
What is essential is to find something that you will want to continue to do.
Personalized Training and Rehabilitation
References
Barranco-Ruiz, Yaira et al. “Dance Fitness Classes Improve the Health-Related Quality of Life in Sedentary Women.” International journal of environmental research and public health vol. 17,11 3771. 26 May. 2020, doi:10.3390/ijerph17113771
Dalle Grave, Riccardo. “Nutrition and Fitness: Mental Health.” Nutrients vol. 12,6 1804. 17 Jun. 2020, doi:10.3390/nu12061804
Higgins, John P. “Smartphone Applications for Patients’ Health and Fitness.” The American journal of medicine vol. 129,1 (2016): 11-9. doi:10.1016/j.amjmed.2015.05.038
Yang, Yun Jun. “An Overview of Current Physical Activity Recommendations in Primary Care.” Korean journal of family medicine vol. 40,3 (2019): 135-142. doi:10.4082/kjfm.19.0038
The muscles, tissues, and ligaments help stabilize the joints and structure of the spine so that the body can function. These muscles are layered and interwoven in the spine and joints that help facilitate movement. When the body suffers from injuries or traumatic events, the muscles, tissues, and ligaments become affected, causing muscle pain and discomfort. This causes the muscles to be tender to the touch and sensitive. This is known as myofascial pain syndrome. Today’s article looks at myofascial pain syndrome, how it is linked with central sensitization, and ways to manage myofascial pain syndrome. We refer patients to certified providers specializing in musculoskeletal treatments to help many individuals with myofascial pain syndrome associated with central sensitization. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Myofascial Pain Syndrome?
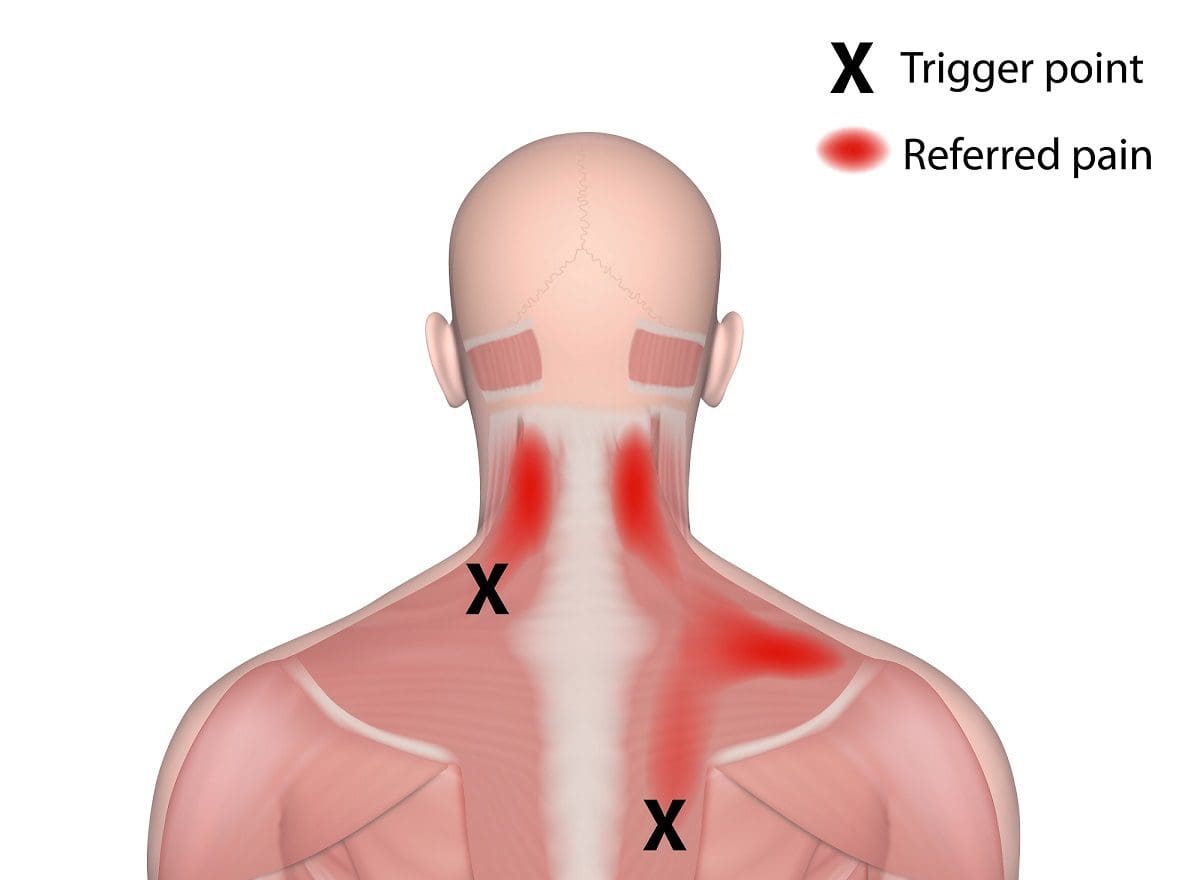
Have you been experiencing muscle tightness in different areas of your body? Have you felt your muscles tender to the touch? Or have you been having trouble sleeping? Many of these overlapping risk factors are signs that you might have myofascial pain syndrome. The term “myofascial” is split into two parts. “Myo” refers to the muscles, while “fascia” refers to the connective tissues found throughout the body. So myofascial pain syndrome is where there is muscle pain in various forms, which includes the muscle tissues, connective tissues, or both. Studies reveal that myofascial pain syndrome originates from trigger points in the skeletal muscle, causing the affected muscle to be in pain. The trigger points in the body’s skeletal muscles are the “knots” people feel when their muscles feel tight. These trigger points are challenging to identify because they occur in different areas causing referred pain (pain in one place but in another body area).
How Central Sensitization Link To Myofascial Pain Syndrome?
Studies reveal that central sensitization in the body is represented as an enhancement in neuron function and circuits in the nociceptive pathways that increases membrane excitability and synaptic efficacy. To that point, it reduces inhibition and manifests the remarkable plasticity of the somatosensory nervous system. The nociceptor inputs can trigger and manifest central sensitization as pain hypersensitivity when the body suffers from an injury. So how is central sensitization linked to myofascial pain syndrome? Let’s use fibromyalgia as an example. Many individuals dealing with myofascial pain may be potentially involved with fibromyalgia. This is due to fibromyalgia being a chronic condition that features widespread pain, and this causes the body to be more sensitive to pain. Central sensitization linked to myofascial pain syndrome can mimic fibromyalgia symptoms in the body, causing muscle pain and discomfort.
An Overview Of Myofascial Pain Syndrome-Video
Are you experiencing muscle weakness or soreness in some regions of your body? Have you dealt with chronic fatigue or poor sleep quality? Or have you been dealing with headaches constantly throughout the entire day? Many of these symptoms are signs that you might be at risk of developing myofascial pain syndrome. The video above explains myofascial pain syndrome, the symptoms, and the causes that affect the body. Studies reveal that myofascial pain has two types of trigger points:
Active trigger points associated with muscle pain without movement
Latent trigger points associated with muscle pain with movement
Myofascial pain syndrome can vary in acute or chronic forms and can range from mild to severe while being in different locations, making it very difficult to pinpoint where the pain is localized. Fortunately, there are ways to manage myofascial pain syndrome in the body that can help with the pain.
Ways To Manage Myofascial Pain Syndrome
When managing myofascial pain syndrome, many individuals dealing with muscle pain will take pain medication to alleviate it; however, that only minimizes the pain for a short period. One way to manage myofascial pain syndrome is by utilizing chiropractic care as part of treatment. Chiropractic care is non-invasive and often the preferred treatment for individuals with myofascial pain syndrome due to its effectiveness and drug-free approach. Chiropractors are not only good at finding the trigger points, but they are good when it comes to treating them using various techniques. Studies reveal that chiropractors use direct pressure on the trigger points to relieve the pain with their hands or specific tools. Incorporating chiropractic care provides the body with an increase in muscle strength, flexibility, and range of motion. Since chiropractic care is a whole-body approach, it allows many people with myofascial pain syndrome to have a better quality of life and learn healthy habits, which include diet, exercise, and mental health, while living with less or no pain at all.
Conclusion
The body has muscles, tissues, and ligaments that help stabilize the joints and structure of the body, so there is functionality. These muscles help facilitate movement since the muscles are interwoven in the spine and joints. When the body suffers from a traumatic event or an injury, the muscles, tissues, and ligaments become affected. This causes muscle pain and discomfort, known as myofascial pain, where the trigger points cause pain in the body and can occur in different areas. Myofascial pain can be challenging to diagnose since it can be on one side of the body but affects a different section, known as referred pain. Fortunately, treatments like chiropractic care can help manage myofascial pain by treating the pain and using direct pressure to alleviate the pain. Incorporating chiropractic care to manage myofascial pain can help many individuals be pain-free on their health and wellness journey.
References
Bordoni, Bruno, et al. “Myofascial Pain – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 18 July 2022, https://www.ncbi.nlm.nih.gov/books/NBK535344/.
Desai, Mehul J, et al. “Myofascial Pain Syndrome: A Treatment Review.” Pain and Therapy, Springer Healthcare, June 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4107879/.
Latremoliere, Alban, and Clifford J Woolf. “Central Sensitization: A Generator of Pain Hypersensitivity by Central Neural Plasticity.” The Journal of Pain, U.S. National Library of Medicine, Sept. 2009, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2750819/.
The brain sends neuron signals to the body to function for everyday movements like walking, running, or resting. These signals travel from the spinal cord through the numerous nerve roots connected to the muscles, tissue, and ligaments that support the joints and organs from multiple factors. However, these factors do affect the body over time, triggering issues that cause pain and discomfort to the body. When this happens, it disrupts the signals from traveling to and forth in the brain, causing dysfunction in the body and leading to neurological disorders associated with neuroinflammation. Today’s article looks at neuroinflammation, how it affects the body, and what is the link between neuroinflammation and neurodegenerative diseases. We refer patients to certified providers specializing in neurological treatments to help many individuals dealing with neuroinflammation associated with neurodegenerative diseases. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Neuroinflammation?
Are you experiencing fatigue and losing focus from your brain? Do you constantly feel stressed or overworked? Or how about developing the risk of Alzheimer’s or other neurological diseases? Many of these symptoms are correlated with neuroinflammation in the brain. Neuroinflammation is defined as an inflammatory response that affects either the brain or the spinal cord. The body has an extensive network known as the immune system, which produces cytokines, antibodies, white blood cells, and other chemicals that protect the body from foreign invaders. Producing cytokines triggers inflammation in the body where the alien invaders are eliminated. The brain surprisingly has its immune system, which provides maintenance and plasticity. When traumatic factors begin to affect the brain’s immune system, the nociceptors become hypersensitive and overexcited due to the results of tissue injuries and inflammation in the peripheral nervous system. Studies reveal that inflammation in the peripheral nervous system results from hyperactivity in the nervous system, which implicates either a positive or negative outcome for the brain.
How Does Neuroinflammation Affect The Body?
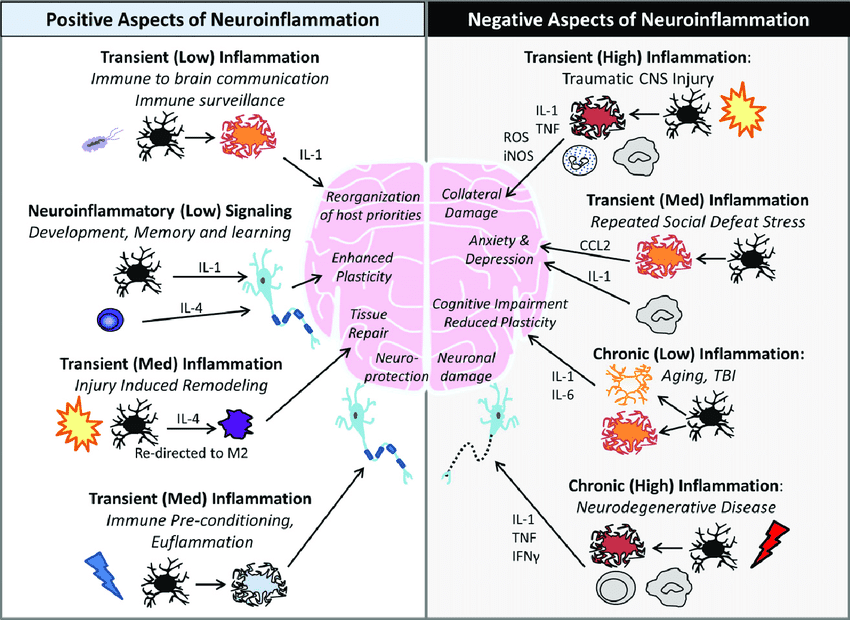
Since neuroinflammation has positive or negative outcomes in the nervous system, it can also trigger the body, making it dysfunctional. Studies reveal that neuroinflammation is mediated by the production of cytokines, ROS (reactive oxygen species), and secondary messengers that becomes the consequences of neuroinflammatory responses. This means that the inflammatory effects are taken into account depending on the intensity and duration of the immune signals in the nervous system, which can be either negative or positive. The positive aspects of neuroinflammation include:
Reorganization of host priorities (immune-brain communication)
While the negative aspects of neuroinflammation include:
Cognitive impairment (aging)
Collateral damage( traumatic injuries)
Neuronal damage (neurodegenerative diseases)
Repeated social defeat stress (anxiety, depression)
Simplified Explanation On Neuroinflammation-Video
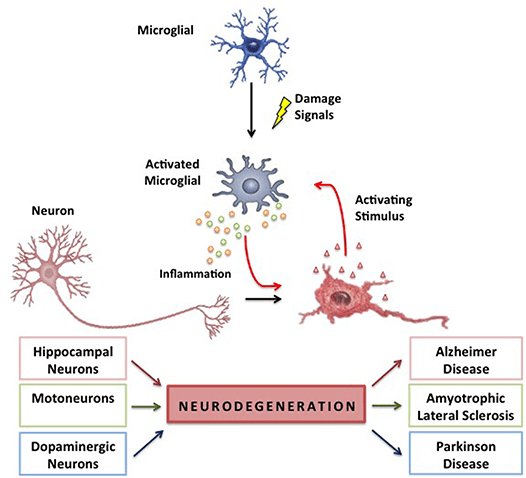
Have you been feeling anxious or depressed? Have you been forgetful as of late? Are you experiencing inflammatory effects in your brain? Many of these symptoms are signs that you could suffer from neuroinflammation in the brain. The video above explains neuroinflammation and how it is linked to the immune system affecting the body. Since neuroinflammation may cause various health issues such as anxiety, stress, depression, and other well-known symptoms, studies reveal that neuroinflammation is a common feature of neurodegenerative diseases. To that point, the relationship between neuroinflammation and neurodegenerative diseases shows that neuroinflammation has been responsible for the abnormal secretion of proinflammatory cytokines to trigger the signaling pathways to the brain, making it dysfunctional.
The Link Between Neuroinflammation & Neurodegenerative Diseases
Since the brain is the primary command center for the body, the link between neurodegenerative diseases and neuroinflammation overlap and cause havoc in the body. Studies reveal that inflammatory and neurotoxic mediators are released in the brain, thus viciously triggering neuroinflammation and neurodegeneration in the body. When the body is dealing with neuroinflammation, one of the symptoms that are prominent in the body is chronic oxidative stress. Research studies have revealed that neuroinflammation has been associated with chronic oxidative stress, a vital feature of all neurodegenerative diseases causing genetic structural alterations. To that point, it results in neurodegeneration. Fortunately, there are ways to lower neuroinflammation associated with neurodegenerative diseases. Some of the ways that many people utilize to reduce neuroinflammation include:
All these small changes are remarkable in reducing neuroinflammation and managing neurodegenerative diseases in the body. This will help many individuals dealing with neuroinflammation associated with neurodegenerative diseases and can regain their health and wellness by managing it.
Conclusion
The brain is the primary command center that sends neuron signals to the body to function in everyday movement. The neuron signals travel from the brain to the spinal cord through the numerous nerve roots connected to the muscles, tissues, and ligaments to support the organs and joints. When environmental factors affect the body over time, it risks developing neuroinflammation associated with neurodegenerative diseases. Neuroinflammation is when the inflammatory mediators start to affect the brain, it can make the brain disrupt the neuron signals from traveling to the body and cause issues associated with neurodegeneration. Fortunately, incorporating different ways to reduce neuroinflammation can help manage neurodegenerative diseases and benefit the body.
References
Chen, Wei-Wei, et al. “Role of Neuroinflammation in Neurodegenerative Diseases (Review).” Molecular Medicine Reports, D.A. Spandidos, Apr. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4805095.
DiSabato, Damon J, et al. “Neuroinflammation: The Devil Is in the Details.” Journal of Neurochemistry, U.S. National Library of Medicine, Oct. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5025335/.
Guzman-Martinez, Leonardo, et al. “Neuroinflammation as a Common Feature of Neurodegenerative Disorders.” Frontiers in Pharmacology, Frontiers Media S.A., 12 Sept. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6751310/.
Kempuraj, D, et al. “Neuroinflammation Induces Neurodegeneration.” Journal of Neurology, Neurosurgery and Spine, U.S. National Library of Medicine, 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5260818/.
Matsuda, Megumi, et al. “Roles of Inflammation, Neurogenic Inflammation, and Neuroinflammation in Pain.” Journal of Anesthesia, U.S. National Library of Medicine, Feb. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6813778/.
Around 60% of individuals have a condition caused by or complicated by chronic inflammation. The body reacts with acute inflammation, which is beneficial as the immune system fights off bacteria that could infect the injury. Examples could be getting a cut on the finger that swells for a day or so to repair the wound or catching a cold and coughing up mucus to expel the germs. However, acute inflammation only lasts as long as necessary; chronic inflammation can last for weeks, months, and years. Individuals can have chronic inflammation and not know the damage being done to arteries and organs until pain or other issues begin to present. There are a few anti-inflammatory diets, which are nutrition plans that can help reduce inflammation.
Anti-Inflammatory Diets
Health-promoting substances include vitamins, minerals, fiber, omega-3 fatty acids, flavan-3-ols in tea and cocoa, and anthocyanins in blueberries, strawberries, raspberries, and other red and purple plant foods. Certain chemicals in the body cause inflammation, and naturally-occurring chemicals in foods, can prevent and combat inflammation by providing essential nutrients.
Nordic Diet
This includes Denmark, Sweden, and Finland, which each have different cuisines, but traditionally, they share healthy foods that provide anti-inflammatory benefits, including:
Rye is a grain shown to help reduce blood sugar, the inflammatory marker C-reactive protein. Individuals that follow this way of eating have lower blood levels of C-reactive protein and other inflammation markers. A randomized study was done in various Nordic countries and lasted six to 24 weeks. One group was assigned a healthy Nordic diet while the other stayed on the country’s modern, less healthy diet. The studies found that individuals that practiced a healthy Nordic diet even for a short while improved inflammatory markers and lost weight.
Mexican Diet
Research has linked a traditional Mexican diet to lower inflammation. Staple foods of a traditional Mexican diet include:
Cheese
Corn tortillas
Fruits and vegetables, including hot peppers
Rice – brown and white
Legumes/Beans
Legumes/beans are linked to protection from inflammatory-related conditions that include:
Obesity
High blood pressure
High blood cholesterol
Type 2 diabetes
Cardiovascular disease
Legumes are high in fiber, which helps:
Reduce inflammation
Reduce unhealthy cholesterol
Reduce blood sugar spikes after a meal, which helps prevent type 2 diabetes and inflammation.
A National Cancer Institute study of post-menopausal women of Mexican descent living in the U.S. found that those following a more traditional Mexican diet averaged 23% lower C-reactive protein levels.
Nutritionist Health Coach and Chiropractic
In some instances, chronic inflammation can come from acute inflammation that does not turn off, which can happen when the body does not make enough chemical substances responsible for turning off the immune response. Blood tests for inflammation can include tests that detect the C-reactive protein and the erythrocyte sedimentation rate, which measures the speed red blood cells settle in a test tube that shows if more inflammatory compounds are present. A combined approach and team of medical professionals, including chiropractic, massage therapy, health coaching, and nutrition, can help relieve and prevent inflammation.
Nutritionist
Consulting a nutritionist is recommended to figure out and determine the best diet/nutrition plan for the individual.
A nutritionist may also suggest supplementation like vitamin D, magnesium, and fish oil supplements.
Body composition analysis breaks down the body elements of water, protein, minerals, and fat that can also discover inflammation markers.
Chiropractic
Chiropractic adjustments help reduce the production of cytokines or proteins that regulate the cells of the immune system. Overproduction of cytokines can cause a severe inflammatory response. Chiropractic’s purpose is to rebalance the body by realigning the vertebrae to reduce pressure on the nerves and promote a healthy nervous system. When the spine and other joints are correctly aligned, the nerves function correctly, returning the body’s biomechanics to normal.
InBody Results
References
Galbete C, Kröger J, Jannasch F, et al. Nordic diet, Mediterranean diet, and the risk of chronic diseases: the EPIC-Potsdam study. BMC Med. 2018;16(1):99.
Lankinen M, Uusitupa M, Schwab U. Nordic Diet and Inflammation-A Review of Observational and Intervention Studies. Nutrients. 2019;11(6):1369.
Ricker MA, Haas WC. Anti-Inflammatory Diet in Clinical Practice: A Review. Nutrition in Clinical Practice. 2017;32(3):318-325.
Santiago-Torres M, Tinker LF, Allison MA, et al. Development and Use of a Traditional Mexican Diet Score in Relation to Systemic Inflammation and Insulin Resistance among Women of Mexican Descent. J Nutr. 2015;145(12):2732-2740.
Valerino-Perea, Selene, et al. “Definition of the Traditional Mexican Diet and Its Role in Health: A Systematic Review.” Nutrients vol. 11,11 2803. 17 Nov. 2019, doi:10.3390/nu11112803
Yang, Yoon Jung, et al. “Dietary flavan-3-ols intake and metabolic syndrome risk in Korean adults.” Nutrition research and practice vol. 6,1 (2012): 68-77. doi:10.4162/nrp.2012.6.1.68
Many people worldwide know that exercising has impressive benefits that help improve the body’s overall wellness. The body has different muscle groups that have a casual relationship with the vital organs inside the body. Organs like the heart, lungs, gut, and bladder correlate with the different muscles through the nerve roots that connect them. When the body suffers from various factors that affect it, it causes referred pain to the body where one pain is at one location but radiates from the other side. Exercising can help the body recover through physical rehabilitation by reducing inflammation and scarring on the muscle tissues. One of the many exercises that helps strengthen the muscles, increase flexibility, and even improve posture is Pilates. Today’s article looks at Pilates, its benefits, and how it can help alleviate back pain. We refer patients to certified providers specializing in musculoskeletal treatments to help many individuals with low back pain issues affecting their bodies. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Pilates?
Have you been feeling sluggish or having low energy throughout the entire day? What about experiencing pain in your lower back? Have you experienced muscle stiffness in certain areas around your body? Many of these symptoms are associated with musculoskeletal issues that correlate with different factors that affect the body; why not try an exercise regime like Pilates? Pilates is a system of exercises that uses a particular machine or body to improve a person’s physical strength and posture while increasing the body’s flexibility and enhancing mental awareness. Joseph Pilates developed Pilates in the early 20th century as an exercise program to help World War I soldiers improve their physical fitness levels. Pilates was used as rehabilitation therapy for injured individuals by incorporating resistance, stretching, and target muscle strengthening. Pilates is now utilized for all individuals with different bodies and fitness levels and can provide tremendous benefits.
What Are The Benefits?
Pilates, like any other form of exercise, has many beneficial properties that help improve a person’s health and wellness. Studies reveal that Pilates helps many individuals, including older adults, by improving their posture by decreasing thoracic flexion while increasing lumbar extension for pain relief. Some of the beneficial properties that Pilates offer to the body include:
Increasing core strength: The deep muscles in the abdomen, back, and pelvic regions become stronger and help stabilize the body more.
Strengthen muscle groups: Pilates helps make the muscles not only strong but also helps stretch them so that they can look long and lean. This makes the individual look toned.
It’s a whole body workout: As many exercises work on specific body parts, Pilates focuses on each muscle part of the body and helps muscle development.
Posture Improvement: Pilates help keep the spine aligned while strengthening the body and core. Over time a person’s posture will improve naturally, making them stand taller, stronger, and even more graceful.
Increases energy: Like all exercises, Pilates will give a person the energy boost they need. This is due to the focused breathing and increased blood circulation that stimulates the muscles and the spine.
Pilates Exercises For Back Pain-Video
Are you looking for a new exercise to tone your muscles? Have you been dealing with pain in your lower back? Do you have muscle weakness in some regions of your body? If you have been experiencing pain-related issues, why not try Pilates? The video above goes through a 10-minute Pilates workout for back pain. Studies reveal that non-specific low back pain is a highly prevalent condition many individuals associate with disability and work absence worldwide. Many environmental factors affect many individuals, causing them to suffer back issues. Pilates can help encourage many individuals to regain their health and wellness by incorporating core strength and stability while improving their posture.
Pilates Alleviate Back Pain
Many people don’t realize that some low back pain symptoms are related to poor posture. Poor posture can lead to associated symptoms of headaches, back pain, improper balance, and pelvic issues. What Pilates does is that it creates body awareness and helps improve the lower back muscles by strengthening them and relaxing the stiff muscles. Studies reveal that incorporating Pilates as physical therapy for individuals suffering from low back pain can help address the mental and physical pain aspects with core strengthening, flexibility, and relaxing the tense muscles. Many individuals should never put off exercising when it comes to back pain. Incorporating an exercise routine can benefit the body and prevent future injuries.
Conclusion
An exercise regime can provide many beneficial results for those looking for ways to be healthy, those suffering from injuries, or those who want to add something else to their workout routine. Pilates is one of those exercises that incorporates resistance, stretching, and muscle targeting as it is a full-body workout. Pilates is used in rehabilitation therapy for injured individuals and can provide tremendous benefits. Pilates can help many individuals with back issues associated with environmental factors like poor posture. Many individuals that utilize Pilates as part of their exercise regime will begin to feel stronger and healthier as their backs will thank them.
References
Baker, Sara. “Pilates Exercise for a Healthy Spine – Spineuniverse.” Spineuniverse, 28 Dec. 2019, https://www.spineuniverse.com/wellness/exercise/pilates-exercise-healthy-spine.
Kuo, Yi-Liang, et al. “Sagittal Spinal Posture after Pilates-Based Exercise in Healthy Older Adults.” Spine, U.S. National Library of Medicine, 1 May 2009, https://pubmed.ncbi.nlm.nih.gov/19404180/.
Sorosky, Susan, et al. “Yoga and Pilates in the Management of Low Back Pain.” Current Reviews in Musculoskeletal Medicine, Humana Press Inc, Mar. 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2684152/.
Yamato, Tiê P, et al. “Pilates for Low Back Pain.” The Cochrane Database of Systematic Reviews, John Wiley & Sons, Ltd, 2 July 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8078578/.
When many individuals look for ways to relax after a stressful event in their daily lives, many people have an exercise regime that allows them to take their minds off of their hectic lives. When finding the proper exercise, it is best to consider that everybody is different and has different fitness levels. Many individuals could be dealing with chronic issues that affect them drastically and with so much pain in their bodies. When these chronic issues overlap with muscle and joint pain, it can make the body dysfunctional while potentially being involved in environmental factors. Yoga is a low-impact exercise that helps tone muscles, relax tension in the body, and focus on deep breathing. Today’s article looks at the benefits of yoga for the body, how chiropractic care works together with yoga, and different yoga poses can help manage various chronic issues. We refer patients to certified providers specializing in musculoskeletal treatments to help many individuals with musculoskeletal problems affecting their bodies. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
The Benefits of Yoga For The Body
Have you been dealing with chronic stress affecting your quality of life? Have you been dealing with bladder or gut issues constantly? What about feeling muscle stiffness in your back, neck, shoulders, or pelvic regions? Some of these symptoms are signs that you could risk developing musculoskeletal problems associated with pain. Dealing with musculoskeletal issues related to pain can make a person feel miserable and have stress affecting their bodies. Yoga is a low-impact exercise that doesn’t put pressure on the joints and will provide a full-body workout through strengthening and stretching weak muscles. Yoga has many benefits for many individuals that are dealing with the following:
Studies reveal that environmental factors are involved in non-specified chronic pain in the spine, overlapping musculoskeletal disorders causing many individuals to try to find relief. Many individuals incorporate yoga because it is a safe and effective way to alleviate various forms of back, neck, or pelvic pain causing issues to the body. Yoga utilizes gentle stretching and strengthening of weak, injured muscles while increasing blood circulation to promote healing in the body.
Chiropractic Care & Yoga
When people are dealing with health conditions or injuries that have affected their bodies, it can make them feel frustrated and think their injuries are taking forever to heal. Many individuals don’t realize that incorporating yoga practices provides impressive health benefits while mirroring the similar foundations of chiropractic care. Both chiropractic care and yoga provide many beneficial results to an aching body that needs a good stretch and ready the body to heal itself naturally. Chiropractic care includes spinal manipulation to the spinal joints while reducing inflammation and strengthening weak muscles. Yoga allows the body to increase its flexibility and stamina, reduces stress and blood pressure, and provides a better sense of breathing and balance.
Yoga For Chronic Pain-Video
Have you felt muscle stiffness in your neck, back, or body? Have you felt sluggish or overly stressed from your day-to-day lives? Do you want to improve your balance? If you have been experiencing these issues affecting your quality of life, why not incorporate yoga as part of your exercise regime? The video above shows that yoga poses for chronic pain affect the body, including the neck, back, and pelvic regions. Studies reveal that yoga can help relieve intense neck pain while improving pain-related function disability. Yoga allows the muscles to not only relax but strengthen them as well. Yoga can also help improve the body’s range of motion through deep breathing and give more awareness of how the body holds tension in places a person hasn’t realized they were holding onto.
Yoga Poses For Different Issues
When a person does yoga, they will go through various poses and repeat them constantly as their body begins to get used to the movements. This allows the body to challenge itself and helps the individual focus more on deep breathing. A good example would be an individual taking a yoga class due to experiencing pelvic pain. By going through each yoga pose, many individuals suffering from pelvic pain will reduce the pain intensity while improving their quality of life. Below are some yoga poses that anyone can do to reduce pain associated with their back, neck, or pelvis.
Bridge Pose
Lie on your back
Bend both knees while placing the feet on the floor at hip-width apart
Arm on the sides with palms facing down
Press feet to the floor and lift the hips as you inhale
Engage the legs and buttock
Hold 4-8 breaths and exhale to lower the hips back to the ground slowly
Cobra Pose
Lie on your stomach with hands near the chest just under the shoulders and fingers facing forward
Keep elbows close to sides
Press hands on the floor and slowly lift your head, chest, and shoulders while slightly bending the elbows by inhaling
Exhale to go back down slow and rest your head
Cat-Cow
Be on all fours, hands under the shoulders and knees under hips (Think like a table)
Inhale to lower your core to the floor as your head looks up to the sky
Exhale slowly to lower your chin to the chest as you round your back
Continue fluid motion for a minute
Forward Bend
Be in a standing position, and feet are at a hip distance apart
Lengthen the body as you lean forward while keeping the knees slightly bended
Place hands on either legs, yoga block, or the floor (Whichever makes you comfortable)
Tuck the chin into the chest, letting the neck and head relax
Gently rock your head side to side to relieve tension in the neck and shoulders
Slowly roll up to a standing position allowing the arms and head to be the last to rise
Supine Spinal Twist
Lie on your back while your knees bent and feet flat on the floor
Extend arms out of the side and place palms down on the floor
As you inhale, breathe into the gut and lower limbs
Exhale to lower knees on the left side (Look at the opposite way to slowly stretch the neck and shoulder muscles)
Pay attention to the stretches for 5 breathes as well as the lengthening sensations on the ribs
Return the knees to the middle and repeat on the right side
Child’s Pose
Sit back on the heels with the knees together (For added support, you can use a rolled-up blanket under your knees)
Bend forward and walk hands in front of you
Gently rest your forehead on the floor
Keep arms extended in the front while focusing on relieving tension in the back as the upper body falls to the knees
Stay in that pose for 5 minutes
Conclusion
Incorporating yoga as part of an exercise regime allows the individual to focus on deep breathing while calming the mind. Yoga is a low-impact exercise that helps strengthen weak muscles associated with pain and inflammation. Yoga provides a full-body workout that benefits many people dealing with chronic pain. Utilizing yoga as part of a daily practice might help individuals learn to be calm and practice mindfulness.
Crow, Edith Meszaros, et al. “Effectiveness of Iyengar Yoga in Treating Spinal (Back and Neck) Pain: A Systematic Review.” International Journal of Yoga, Medknow Publications & Media Pvt Ltd, Jan. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4278133/.
Li, Yunxia, et al. “Effects of Yoga on Patients with Chronic Nonspecific Neck Pain: A Prisma Systematic Review and Meta-Analysis.” Medicine, Wolters Kluwer Health, Feb. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6407933/.
Saxena, Rahul, et al. “Effects of Yogic Intervention on Pain Scores and Quality of Life in Females with Chronic Pelvic Pain.” International Journal of Yoga, Medknow Publications & Media Pvt Ltd, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5225749/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine