Dr. Alex Jimenez Explains Methylation Status, Inflammation and Oxidative Stress
As previously mentioned in the past series of articles, doctors can use a variety of clinical assessments to evaluate the methylation status of their patients. Although no assessment method or technique can accurately determine a patient’s methylation activity, current assessments can provide a better understanding of methylation-related genetic polymorphisms, nutrient status, methylation-related neurotransmitters and neurotransmitter metabolites, amino acids, hormones and metabolites, oxidative stress, and detoxification load. Each of these processes and substances can help doctors and patients understand their methylation status.
Understanding Methylation Status
Various assessment methods and techniques, including measures utilized to determine DNA methylation status, are usually exclusive to research studies and are not yet readily available to doctors. Until methylation status assessments become more widely available, further diagnosis is still required to understand diseases, especially since conflicting outcome measures have been found in research studies on the various methodologies. Although methods and techniques from research studies have rapidly started to evolve, patterns of DNA methylation status in humans across cells, tissues, age, populations, environmental factors like nutrition and lifestyle modifications, as well as disease, have only just started to become more widely recognized by researchers and doctors.
It is fundamental that we focus on a variety of these indicators and that we become aware of the restrictions of our interpretations and their misunderstood factors. Plasma homocysteine, by way of instance, can decrease as methylation activity increases, but, it can also decrease when oxidative stress levels increase, regardless if methylation activity increases. However, as we�ve previously mentioned, only several SNPs have known, quantifiable alterations in enzymatic function and their overall outcome measures on methylation remain unknown. Doctors must rely on a variety of clinical assessments to evaluate the methylation status of their patients. In the following articles, we will continue to discuss methylation status assessment options available to doctors for patients.
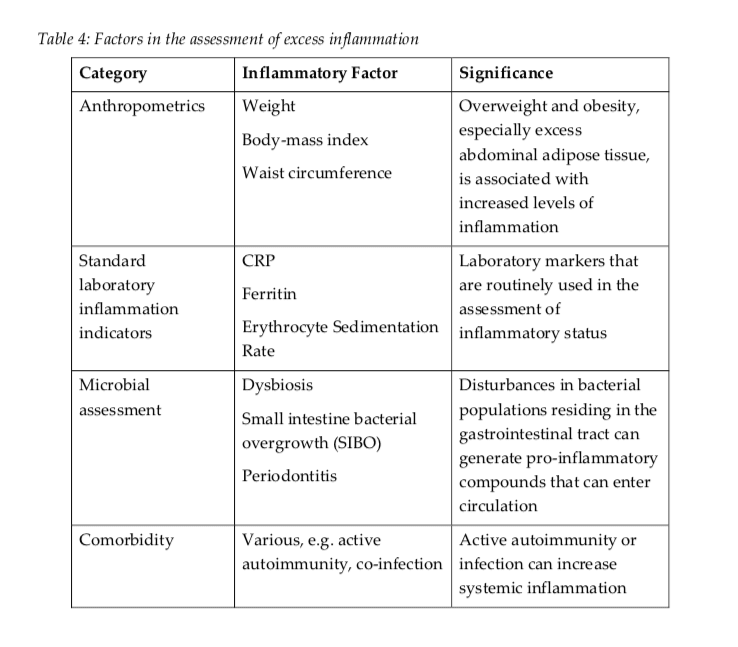
Understanding Inflammation
Inflammation increases the production of cytokine which can alter a patient’s methylation status in a variety of ways. DNA methylation activity is also tremendously affected by inflammation-related signaling molecules. Cytokines, chemokines, free radicals, prostaglandins, growth factors, and matrix metalloproteinases, are produced during inflammation, altering epigenetic changes in DNA methylation activity. IL-1?, by way of instance, suppresses p53 expression, creating a more favorable environment for tumorigenesis. NF?B is a central transcription factor triggered by inflammation which also regulates the expression of more than 400 genes.
Moreover, it directly regulates NK?B-dependent histone demethylase which in turn regulates the fate and transdifferentiation of tumor cells. IL-6, another inflammatory signaling molecule, regulates the activity of DNMTs, microRNAs and histone methyltransferases which affect the epigenetics of p53 tumor suppressor genes by reducing expression. TNF-alpha increases in mitotically-preserved and region-specific DNA methylation activity in a way that seems to include impaired cellular differentiation and renewal. In vitro outcome measures suggest that inflammation may also promote the production of methyl radicals which trigger DNA methylation activity in normal, unmethylated tumor suppressor genes, causing gene silencing and carcinogenesis.
Inflammation can also cause a metabolic milieu that drains methylation resources, by way of instance, through the dysregulation of glucose homeostasis. Pro-inflammatory molecules can also alter insulin signaling in peripheral tissues, reducing inflammatory mediators that promote insulin signaling. Insulin dysfunction and hyperglycemia promote elevated levels of oxidative stress which triggers increased utilization of glutathione and depleted homocysteine, methionine and SAMe. Furthermore, DNA methylation patterns affecting metabolism and inflammation were identified in adipose tissue from subjects with type 2 diabetes.
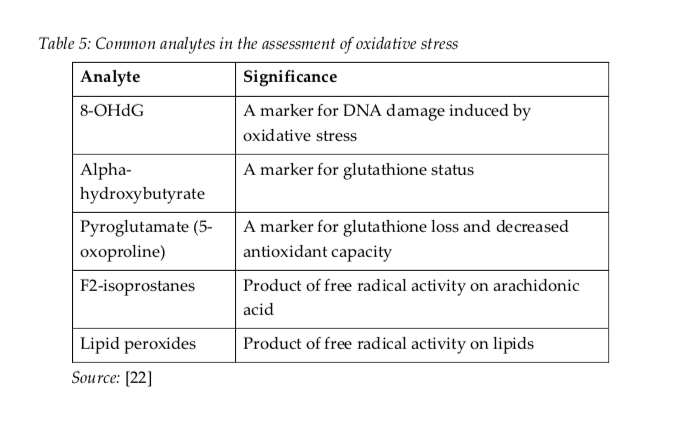
Understanding Oxidative Stress
Oxidative stress is closely associated with inflammation. States of elevated, or chronic, oxidative stress can negatively alter DNA methylation through two mechanisms. First, oxidative stress increases the demand for glutathione synthesis, which pulls homocysteine towards transulfuration pathways, at the expense of methylation pathways and SAMe formation. Second, oxidative stress and increased hydroxyl radical formation can damage DNA and change the ability of DNA methyltransferase enzymes to appropriately methylate DNA. This is one of the most common causes of global DNA hypomethylation and specific areas of hypermethylation.
DNA guanine nucleotides are main regions of DNA damage caused by oxidative stress, which is why they are frequently utilized as a biomarker for DNA-level oxidative stress, or 8OHdG. Generally, guanine functions as a hydrogen bond acceptor to promote the creation of methyl binding protein, or MBP, DNA complexes. However, oxidation of guanine considerably decreases MBP binding when combined to the 5- methylcytosine nucleotide. Additionally, 5-methylcytosine, or 5-mC, may also experience oxidation or hydroxylation, forming 5-hydroxymethylcytosine, or 5-hmC, through oxidative stress. This can tremendously affect interactions with DNA-proteins that can prevent their binding affinity to MBPs, leading to potentially heritable epigenetic alterations.
The methods and techniques commonly utilized to determine DNA methylation can’t distinguish between 5-mC and 5-hmC, which may prove to be an essential distinction, especially in the brain, where most DNA hydroxymethylation can be found. There is outcome measures which demonstrate that acute psychological stress can increase DNA hydroxymethylation in the hippocampal glucocorticoid receptor gene. This epigenetic alteration can lead to the development of neuropsychiatric and neurodegenerative disorders. Aging is also associated with increases in 5-hmC in the brain which may be prevented by caloric restriction and antioxidant upregulation.
A variety of research studies have found that DNA methylation can be affected by inflammation, most commonly caused due to oxidative stress. Increasing outcome measures have also demonstrated that methylation activity may become affected in response to both nutritional and environmental influences. Alterations in DNA methylation caused by inflammation and oxidative stress can lead to problems in gene expression, increasing the potential risk of disease. Understanding the effects of inflammation due to oxidative stress is fundamental when investigating epigenetic mechanisms. DNA methylation assessments based on inflammation and oxidative stress can help patients regulate their overall health and wellness.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many doctors and functional medicine practitioners may recommend higher doses of methyl donors in several patients, however, further research studies are needed to determine the proper amount of methylation supplementation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Fred Foreman is a basketball coach who depends on his overall health and wellness to be able to engage in his everyday responsibilities. As a result, coach Foreman started the 6 Day Detox Program from Xymogen, designed to help renew and enhance the human body’s cleansing and detoxification capabilities.
Fred Foreman discusses his experience with the 6 Day Detox Program, describing the benefits he developed as well as the effort he had to implement, to support his overall health and wellness through the detox. Fred Foreman feels a great sense of fulfillment with the 6 Day Detox Program and he encourages other people, who also wish to improve their well-being, to detox their body. Coach Foreman highly recommends the 6 Day Detox Program as an alternative treatment choice for overall health and wellness.
Injury Medical & Chiropractic Clinic
We are blessed to present to you El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend us.
Healthcare professionals can utilize a variety of clinical assessments to evaluate the methylation status of patients. However, there is no single assessment method or technique which can accurately demonstrate the complexity of methylation in the human body. Current assessments can help provide an understanding into methylation-related genetic polymorphisms, nutrient status, methylation-related neurotransmitters and neurotransmitter metabolites, amino acids, hormones and metabolites, oxidative stress, and detoxification load, all of which can also help provide the understanding of a patient’s methylation status.
Understanding Methylation Status
Some assessment methods and techniques, including measures to determine DNA methylation status, are generally limited to research studies and are not yet available to healthcare professionals. As DNA methylation status assessments become available, healthcare is necessary to understand data because conflicting outcome measures have been demonstrated in research studies based on a variety of methodologies while methylation is further evaluated. Moreover, although methods and techniques, as well as research studies, are quickly evolving, patterns of DNA methylation status in humans across cells, tissues, age, populations, environmental factors like nutrition and lifestyle modifications, and disease, are only just being characterized by healthcare professionals.
It is essential that we emphasize a variety of indicators and be mindful of the restrictions of our interpretations as well as their misunderstood factors. Plasma homocysteine, by way of instance, can decrease as methylation activity improves, however, it can also decrease when oxidative stress levels increase, independently of methylation activity improvements. But, as we�ve previously discussed, only a few SNPs have known, quantifiable changes in enzymatic function, and even then, their overall outcome measures on methylation are unknown. Healthcare professionals must depend on multiple clinical assessments to determine methylation health. In the following articles, we will discuss methylation status assessment options available to healthcare professionals.
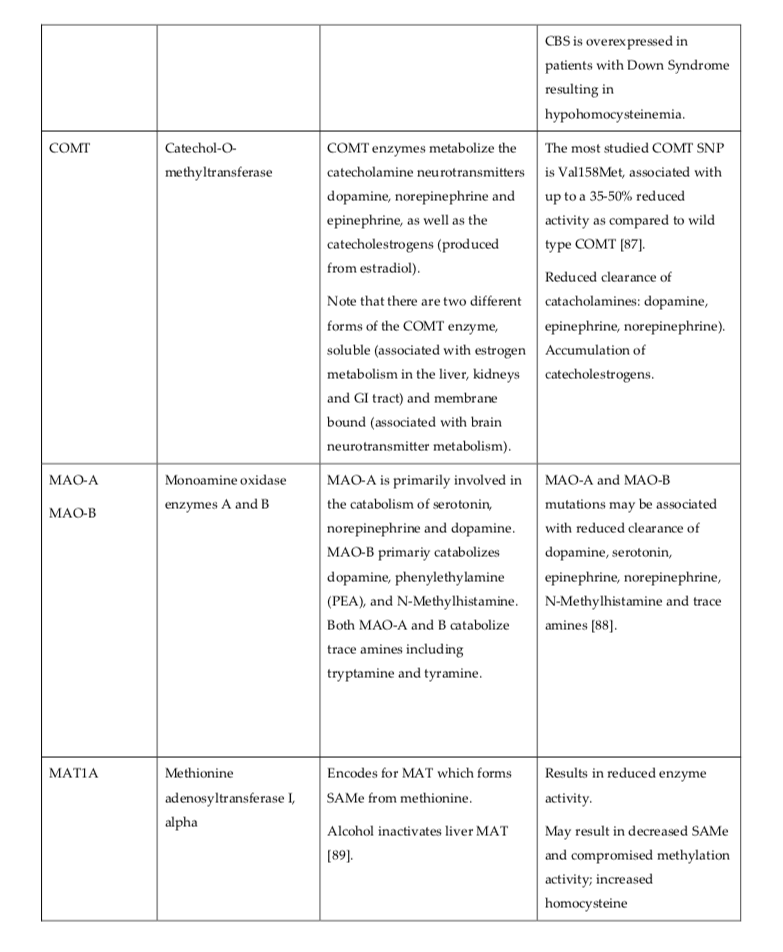
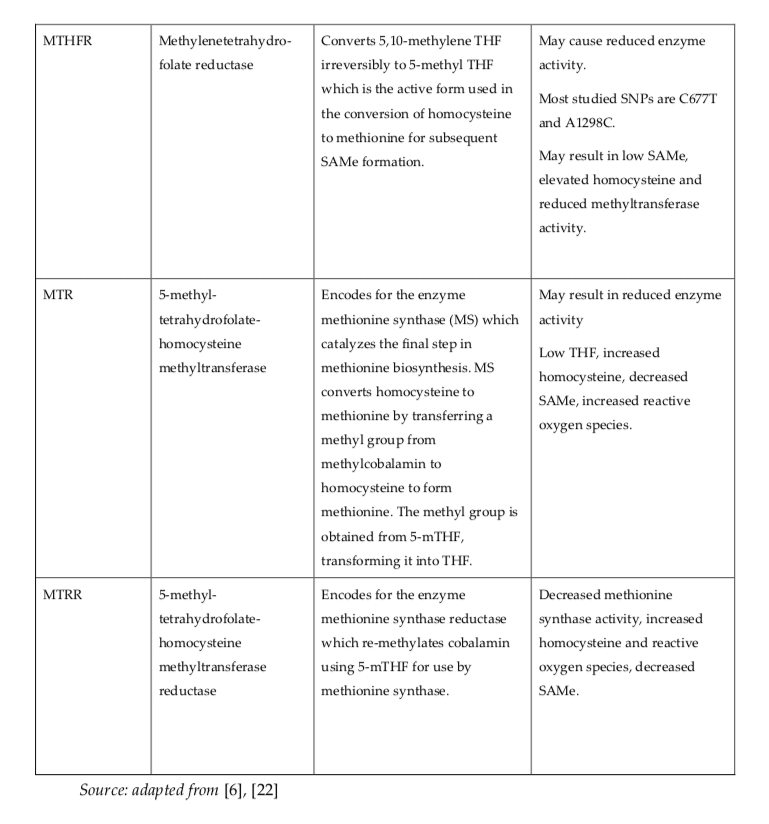
Understanding Genetic Profiling
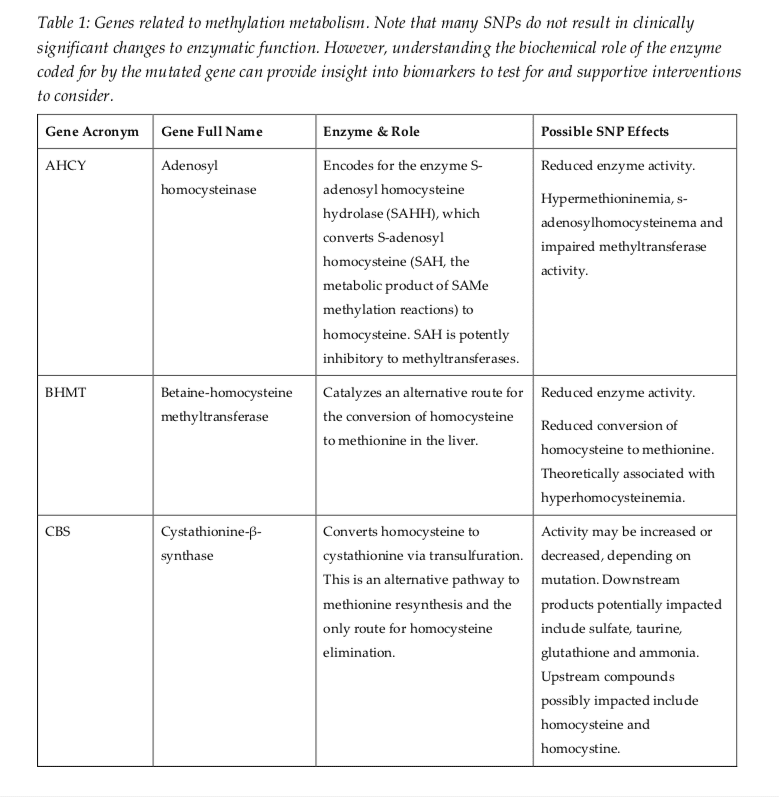
Genetic profiling can help provide some evidence of potential methylation status and risk of developing diseases. Several gene SNPs increase methylation activity, such as CBS, and several other gene SNPs may decrease methylation activity, such as MTHFR, BNMT, MTR, MTRR, and AHCY. However, understanding the overall outcome measures of gene SNPs is complicated to determine through polymorphisms and environmental factors. By way of instance, research studies have demonstrated that the MTHFR C677T polymorphism is associated with an increased risk of autism spectrum disorder, (with an odds ratio = 1.42, 95% CI 1.09-1.85), however, similar research studies have also demonstrated that this risk can decrease through periconceptional folate or folic acid intake.
Furthermore, if a maternal MTHFR C677T polymorphism is combined with a CBS polymorphism, a lack of prenatal supplementation with B vitamins, and a fetal COMT polymorphism, the odds ratio for autism spectrum disorder can increase tremendously, (7.2, CI = 2.3�22.4; P=0.05). The risk of diseases associated with genotype is unfortunately rare because research studies on the combined outcome measures of gene SNPs are still very much in their early stages. In many circumstances, healthcare professionals will need to use careful clinical assessments to evaluate as well as to guide their treatments. The methylation-related genes presented in Table 1 below are frequently evaluated for SNPs. The outcome measures can help doctors understand patient methylation status.
A variety of methods and techniques are available to determine the methylation status of patients. However, the assessment of methylation status can still be challenging for many healthcare professionals. DNA methylation is characterized by the addition of a methyl group to DNA. Healthcare professionals must first understand the pros and cons of the variety of methods and techniques available to determine methylation status to allow them to make an informed choice when deciding which assessment will best suit their research study needs.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many doctors and functional medicine practitioners may recommend higher doses of methyl donors in several patients, however, further research studies are needed to determine the proper amount of methylation supplementation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Can nutritional epigenetics influence how we age and our longevity? El Paso, Tx. Dr. Jimenez presents data on how nutrition can influence longevity and how we age.
Longevity or our length of life is dictated by complex factors which include our genetic blueprint, age, health, and environment. This includes nutrition.
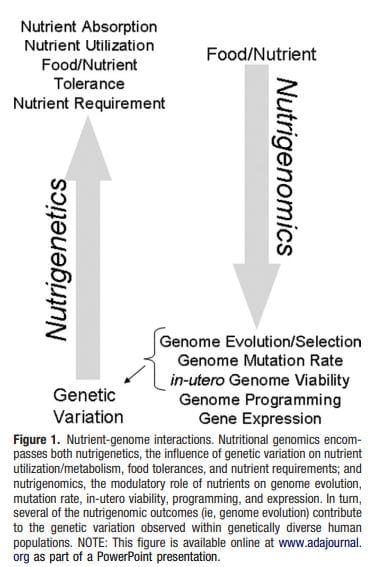
Gene-nutrient interactions are, partly responsible for regulating metabolic processes that begin and develop conditions like obesity, metabolic syndrome, cardiovascular disease, and cancer.
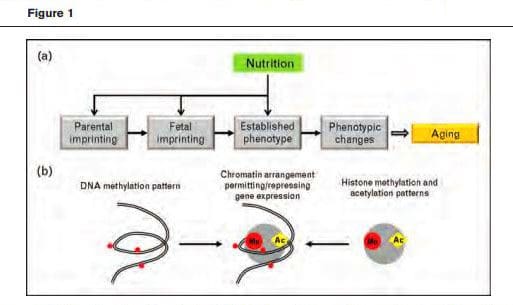
A mechanism of nutrient-gene interaction is the epigenetic involvement of inherited patterns of changes, that are maintained by other mechanisms in DNA, Fig. 1a
Although still not fully proven but on the right track was that the availability of folate improved the regeneration of the adult central nervous system after injury through an epigenetic mechanism.
Epigenetic Aging
During the last couple of years, we witnessed a remarkable increase in the number of studies addressing the relationship between epigenetic alterations and aging. Still in its infancy, and still focusing mainly on brain aging, this research clearly indicated that epigenetic mechanisms are not only responsible, in part, for the aging process but they are also dynamically related with memory formation and maintenance.
Penner MR, Roth TL, Barnes CA, Sweatt JD. An epigenetic hypothesis of aging-related cognitive dysfunction. Front Aging Neurosci 2010; 2:9.
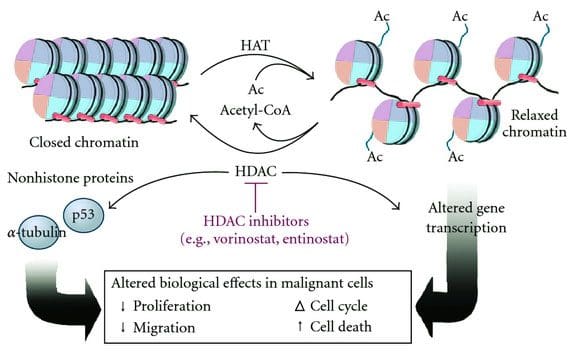
The manipulation of the epigenome for memory improvement became possible through changes in histone acetylation.
The Link: Nutrition & Longevity
Research to complete the chain of nutrition to epigenetic changes to how we age is still ongoing.
Present knowledge of the epigenetic roles in nutrition having to do with longevity/aging relies on the structure of three components:
Nutritionally guided epigenetic modification
Age-related epigenetic changes
Comprehensive knowledge of both of these components
The first two are being developed quickly, but the third is the most demanding in terms of design, time, allocation, and cost. This takes more time. But technology/humanity is moving along at a quick pace, as well, because at the end of the day we all want to be healthy.
Therefore, Nutritional intervention, when applied at critical periods (e.g., embryonic and fetal development) is having a profound effect as to how the epigenome gets shaped.
When considering the beginning of chronic disease/s, being able to fight disease/s with food sounds like a win-win. If epigenetic/genomic nutrition can help in figuring out what we need to beat disease/s, then let’s go!
Family In Kitchen Making Morning Breakfast Together
How does epigenetic and personalized nutrition contribute to optimal health?
Most of us know about unhealthy food how it affects our bodies. They
Slow Down Metabolism
Add Weight
Clog and harden arteries etc.
But now there are foods and food elements that can help us in a way and comes from a place we might not of thought of, and that is our DNA.
Nutriepigenomics examines connections between diet and biomarkers that can be attached or removed from our DNA. This turns our genes on or off.
New studies are showing that certain foods or supplements can adjust the expression of our genes, which can influence our health.
Nutritional genomics is revolutionizing both clinical and public health nutritional practices:
Diet, exercise, and environmental exposure are all elements that have shown a role in switching genes on and off through epigenetics. Adjusting lifestyle factors can control the potential to reduce disease and have a positive impact on our health.
Health professionals from all over are beginning to incorporate epigenetics into their practice aiming to provide more specialized and individualized treatment plans.
�Layering information such as diet, lifestyle, environmental factors, family history, symptoms, and diagnoses along with epigenetics can help guide someone to a state of optimized health,� said Kristy Hall, MS, RNCP, ROHP, a board certified functional nutritionist and founder of Living Well Nutrition who uses epigenetic testing, nutrition counseling, and a multifaceted approach to better provide for her clients.
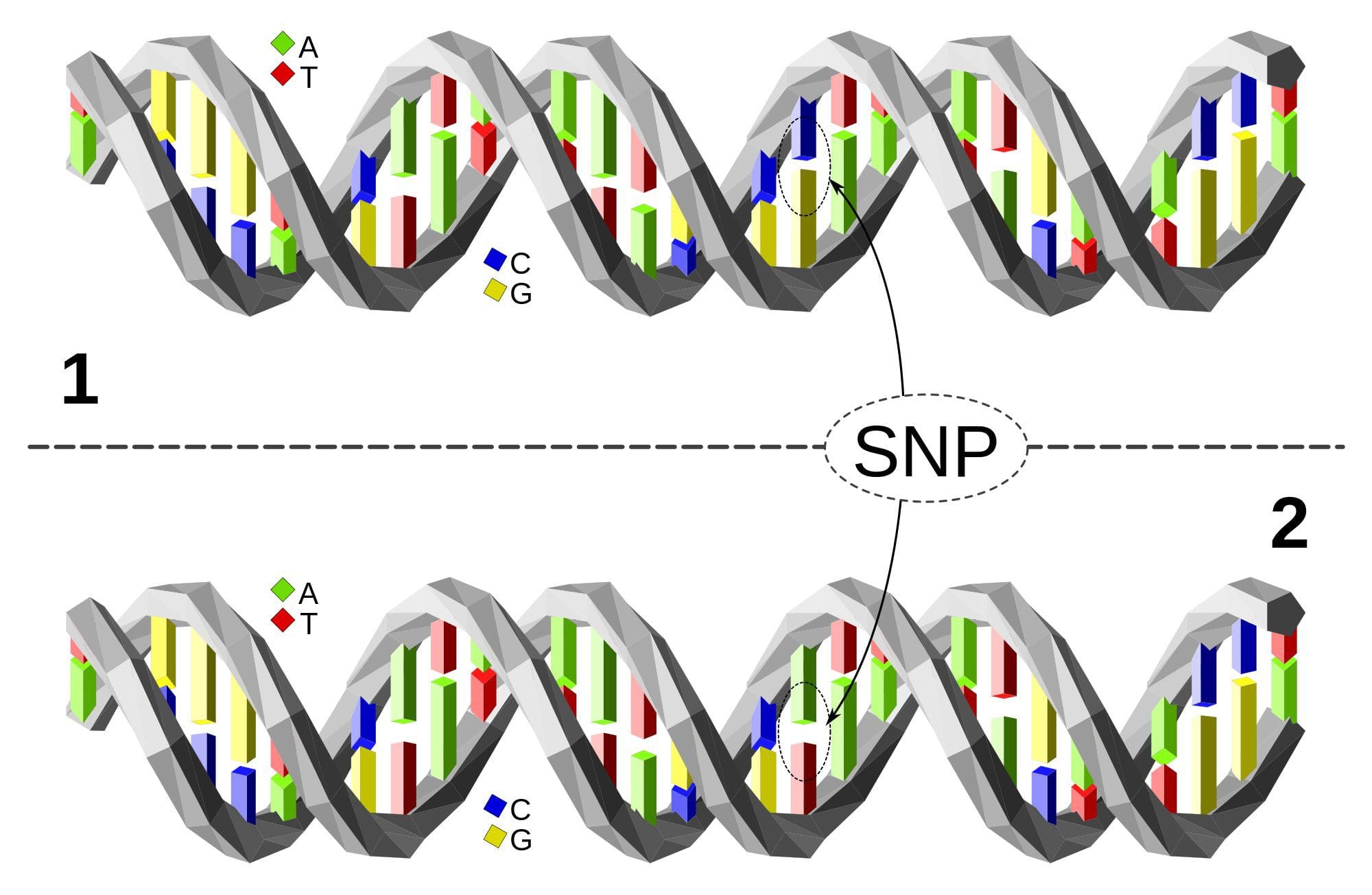
The upper DNA molecule differs from the lower DNA molecule at a single base-pair location (a C/A polymorphism)
Nutritional genetics or nutrigenetics involves the identification, classification, and characterization of human genetic variation that modifies nutrient metabolism/ utilization and food tolerances Fig1.
IOM. Nutrigenomics and beyond: Informing the future. Washington, DC: The National Academies Press; 2007.
Application: Genetic & Epigenetics
Nutrients, for example, pharmaceuticals, are powerful effectors of genome expression and stability, and these gene-nutrient interactions can be optimized for disease prevention.
Individualized Nutrition
The promise of nutritional engineering for optimal health through diet is still ongoing, but the public is holding positive expectations, as is evidenced by the use of dietary supplements.
Scientific research is showing that nutrients in different foods and supplements we eat may be able to adjust or reverse heritable changes. This evidence can be used in making better lifestyle choices.
Blueberries are incredibly high in antioxidants and it�s thought that this �superfood� can epigenetically reduce DNA damage, thereby protecting humans against cancer and possibly even slow aging. Blueberry juice and vitamin C have been shown to be potential methylation inhibitors for the MTHFR gene and the DNMT1 gene in humans.
Kim, M., Na, H., Kasai, H., Kawai, K., Li, Y.-S., & Yang, M. (2017). Comparison of Blueberry (Vaccinium spp.) and Vitamin C via Antioxidative and Epigenetic Effects in Human. Journal of Cancer Prevention, 22(3), 174�181.
Learning about what we eat and what it does to our bodies, especially potential epigenetic impact, is just one step closer to optimal health.
Can methylation donors help promote a balanced methylation support?
Many doctors and functional medicine practitioners generally recommend higher doses of methyl donors, such as 5-methyltetrahydrofolate, or 5-MTHF, and methylcobalamin, in several patients. By way of instance, people with genetic polymorphisms and people with out-of-range methylation-related biomarkers, such as in hyperhomocysteinemia, may often develop health issues which may affect the function of specific enzymes, such as methylenetetrahydrofolate reductase, or MTHFR, among others.
Nutrient deficiencies associated with methyl donors are a prevalent finding in laboratory evaluations, and depending on your population, these may be closely associated with vitamin B12 deficiency-related neuropathy, which is relatively common. Many doctors and functional medicine practitioners also understand the importance of methylation support to help improve hereditary or environmental epigenetic health issues. Improving methylation status and avoiding the pathways of disease and dysfunction associated with potential nutritional deficits in methylation activity is the goal of many healthcare professionals.
However, as with any other biochemical process, methylation activity occurs through the balance of homeodynamics, or the dynamic form of homeostasis. An imbalance in these biochemical processes can ultimately lead to dysfunction and disease. Therefore, although we can be confident that making sure we have enough methyl donors available for use in the human body is essential, we have to question whether �pushing� reaction rates utilizing supraphysiological doses are safe and effective. Instead of forcing reaction rates, perhaps the goal of healthcare professionals should ultimately be to allow the human body to function correctly.
Methylation Supplementation
Numerous health issues associated with long-term, high-dose supplementation for methylation donors include:
According to research studies, the effects of these genetic alterations remains unclear. In comparison to the altered function of MTHFR C677T and A1298C single nucleotide polymorphisms, or SNPs, which have been moderately evaluated, the diagnosis of other SNPs can demonstrate the overall function of these specific enzymes. The effect of these SNPs on methylation activity depends on enzymes working together in the circumstance of a person’s internal and external environment. These outcome measures have been demonstrated in a variety of genome research studies. As a result, researchers are unable to determine the effects which these alterations, including that of MTHFR C677T, can develop on a patient’s overall methylation status.
The correct supplementation dose for methylation donors remains mostly unknown, as it may vary tremendously between patients. No research studies have currently demonstrated what the correct dosage or duration of methyl-donor supplementation is required to balance biochemical and epigenetic methylation status. Various side effects of high-dose 5-methyltetrahydrofolate, or 5-MTHF, supplementation have been demonstrated in clinical practice, including anxiety and worsening of symptoms.
Hypermethylation may be detrimental to an individual’s overall health and wellness. The following series of articles contain many examples of region-specific DNA hypermethylation health issues, including immune dysfunction, Downs Syndrome, and cancer. Both DNA hyper- and hypomethylation can develop due to deficiencies in methylation donors. Folic acid has been associated with increased immune hypersensitivity and cancer. The bottom line is that we don�t understand what effect long-term, high-dose methylation donors and supplementation can have on DNA methylation support. Further research studies are still required to show this effect.
Methylation is a biochemical process which involves the conversion of methylation activity for the function of a variety of processes in the human body. Methylation imbalances, however, can cause a variety of health issues. Methylation donors are a form of supplementation for methylation support. But, research studies have demonstrated that supplementation for methylation support may not be right for everyone. The best way to improve methylation is through proper nutrition, physical activity, and exercise, among other dietary and lifestyle modifications. The nutritional guidelines below can help safely and effectively improve methylation support, promoting overall health and wellness.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Nutrition for Methylation Support
Methylation status can often depend on a patient’s dietary and lifestyle factors. Dietary and lifestyle factors, including physical activity and exercise, stress, sleep, medicines, and toxin exposure, plays a role in methylation. Single interventions with high-dose nutrient supplementation may lack long-term effectiveness or these may not achieve the desired methylation support.
Dietary and lifestyle modifications are safe and effective, alternative treatment options for most individuals with methylation imbalances. This may be fundamental for certain vulnerable individuals, such as patients with active cancers. Aging is also known to be associated with decreased methylation activity, therefore, the Methylation Diet and Lifestyle, or MDL, program can be utilized as an anti-aging tool. Methylation status diagnosis and treatment is essential during preconception, pregnancy and the postnatal period.
The MDL program and supplementation can help promote overall health and wellness. A dietary and lifestyle treatment approach can also be utilized as a follow-up plan for people who need high-dose nutraceutical support. A variety of foods can promote methylation support. Dietary and lifestyle modifications have also been demonstrated to considerably improve methylation activity.
In the following articles, we will discuss dietary and lifestyle factors which can help support methylation. We will also discuss the basic biochemistry of methylation, the roles of methylation in the human body, how to evaluate methylation status, and the risks and benefits of methyl donor supplementation as well as the health issues associated with too little or too much methylation activity.
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications, there are several alternative treatment options you can try for yourself at home. As described above, however, supplementation for methylation support should be correctly determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support in a single serving. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
alanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many doctors and functional medicine practitioners may recommend higher doses of methyl donors in several patients, however, further research studies are needed to determine the proper amount of methylation supplementation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Some people find it easier to engage in certain healthy activities during different times of the year. For instance, they may enjoy the fresh produce of summer or going for a run during the cooler days of fall. However, there are some things you can do to stay healthy regardless of the season. These are some good habits you can cultivate and develop for good health, rain or shine, cool weather or warm. By incorporating these four practices into your daily routine, you are very likely to see much less of your doctor and enjoy your life a whole lot more.
See a Chiropractor Regularly
Visiting a chiropractor regularly will keep your body balanced and your spine aligned. Chiropractic care has several significant benefits including decreased pain, faster healing from injuries, increased mobility, and better flexibility.
What makes it even more preferable is that chiropractic takes a whole-body approach to health issues. This means that when you have a problem such as pain or a medical condition, your chiropractor will work to get to the root of it and treat the condition where it starts while traditional medicine typically focuses on symptoms. Chiropractic care is non-invasive and drug-free, a truly natural approach to health care.
Maintain a Balanced Diet
A healthy diet is the cornerstone of good health. You should maintain a diet that includes lean meats, fresh fruits and vegetables, and whole grains. The key is choosing fresh, seasonal foods that are local to your area. Foods grown in their season have certain vitamins and minerals that the body needs for the time of year in which they are ripe and ready.
It is also worth noting that several small studies have found that animal protein can exacerbate pain, specifically osteoarthritis. It does not mean you should stop eating meat altogether because certain types of meat offer significant health benefits. Salmon is a good example. It is loaded with heart-healthy Omega 3 Fatty Acids � which, incidentally, also help to reduce inflammation in the body.
Find an Exercise Routing that Works
If you want to be able to move, then you have to start moving. Exercise is crucial for maintaining a healthy lifestyle. The problem is, many people believe that the only way they can exercise is by joining the gym or going for a run which has to be done in good weather. This isn�t so.
There are plenty of things you can do indoors, even in small spaces or while on vacation, to get some exercise. If you have problems with mobility, walking is an excellent option, but even gardening is great.
Also, women over 40 should do weight-bearing exercises several times a week to ward off osteoporosis. Furthermore, exercise is a great complement to chiropractic. It helps to keep your body flexible and increases your range of motion. Three to five times a week for 20 to 30 minutes is all you need.
Get Good Sleep
Good sleep is one of the most underrated keys to good health. When you sleep, it gives your brain and body an opportunity to refresh and heal. The discs in your spine are rehydrated, your body relaxes, and you less susceptible to stress when you are well rested.
On average, adults need anywhere from seven to nine hours of sleep a night in order to reap the full benefits. Take time to set up your bedroom for good rest: a comfortable mattress, a good pillow (they can wear out so change them regularly), a cool, dark, quiet room, and a relaxing environment that may include white noise or lavender scent. Make your bedroom as comfortable and sleep-inducing as possible.
Good health practices don�t have to be complicated or difficult. Start with small steps and let those behaviors become habits. Good health habits will help you have a long, full life.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine