The body needs protein which is essential in building muscle, repairing tissue, producing enzymes and hormones and is a source of energy. Whey is a complete protein source that provides all the essential amino acids, vitamins, minerals, and other nutrients that increase anabolism, also known as muscle growth. It is used for various reasons. Some individuals want to build muscle mass and gain strength, while others want to lose weight and achieve improved results from working out. Even individuals who don’t exercise can benefit from the supplement as it supports immune function, helps reduce blood pressure, and improves insulin response.
Whey Protein
Whey protein is made from the liquid produced during the cheese-making process.
Milk comprises two forms of protein: casein (80%) and whey (20%).
It contains less than 0.5 g of fat and only 5 mg of cholesterol per serving.
Pure whey does not contain any gluten.
It is referred to as the most nutritious protein available.
It’s easy to digest.
Incorporating whey into a healthy diet can help lower the risk of diabetes.
Types
There are three primary types of whey protein in supplements.
Hydrolysate is a form that has already gone through partial hydrolysis, a process so the body can absorb protein.
It is considered pre-digested, so it gets absorbed quicker.
Concentration is the most popular and least expensive option that retains the most nutrients. However, some individuals can tolerate isolate and hydrolysate a lot better and are ideal for those trying to cut down on carbs and fats.
Benefits
Increased Strength and Muscle
Helps to increase protein consumption.
Most brands contain 80 to 90 percent without added carbs or fats.
Helps to build muscle and increase strength after physical activity/exercise recovery.
Can Help Burn Fat
A study found a group of adults that supplemented their diet with whey protein experienced a decrease in body fat and weight.
Combining whey protein and resistance training, participants found their weight and fat loss were even higher.
Can Help Stabilize Blood Sugar
Consuming whey protein with a high glycemic index before a meal can help stimulate insulin production while preventing spikes in blood sugar levels.
The protein naturally reduces blood sugar levels after meals when consumed before the meal.
Improves Heart Health
It can help reduce blood pressure and arterial stiffness.
It has been linked to improving individual lipid profiles.
Promotes heart health by building muscle and helping with weight loss.
Increased Immunity
It can help encourage glutathione synthesis, which increases immune system function.
It is also rich in vitamins and minerals that promote immune function.
It helps the body recover from oxidative stress and inflammation.
Improves Energy Levels
It helps to increase glycogen, a source of energy during exercise or other physical activities.
It also increases leptin which helps balance the body’s energy levels.
Whey is easily digested, which can be quickly converted to energy.
Factors to Consider When Choosing
Flavor
The flavor is crucial because nobody wants to drink a daily protein shake they cannot enjoy.
Options like chocolate and vanilla are usually safe.
If experimenting, get a small container to start.
Mixability
Not all supplements mix properly or thoroughly.
Find a brand that dissolves quickly and has little clumping.
Container Size
Most protein supplements are available in 1 lb, 2 lb, 5 lb, or 10 lb containers.
Larger sizes are more cost-effective.
One 5 lb package is cheaper than buying five 1 lb containers.
Everything You Need To Know
References
Ebaid, Hossam et al. “Whey protein enhances normal inflammatory responses during cutaneous wound healing in diabetic rats.” Lipids in health and disease vol. 10 235. 14 Dec. 2011, doi:10.1186/1476-511X-10-235
Hashemilar, Mazyar, et al. “Effect of Whey Protein Supplementation on Inflammatory and Antioxidant Markers, and Clinical Prognosis in Acute Ischemic Stroke (TNS Trial): A Randomized, Double-Blind, Controlled, Clinical Trial.” Advanced pharmaceutical bulletin vol. 10,1 (2020): 135-140. doi:10.15171/apb.2020.018
Kim, Jooyoung, et al. “Effect of timing of whey protein supplement on muscle damage markers after eccentric exercise.” Journal of exercise rehabilitation vol. 13,4 436-440. 29 Aug. 2017, doi:10.12965/jer.1735034.517
Marshall K. Therapeutic applications of whey protein. Alternative Medicine Review. 2004;9(2):136-156.
Pradhan, Geetali, et al. “Ghrelin: much more than a hunger hormone.” Current opinion in clinical nutrition and metabolic care vol. 16,6 (2013): 619-24. doi:10.1097/MCO.0b013e328365b9be
Volek, Jeff S et al. “Whey protein supplementation during resistance training augments lean body mass.” Journal of the American College of Nutrition vol. 32,2 (2013): 122-35. doi:10.1080/07315724.2013.793580
Medical experts advise that maintaining body hydration is one of the most important things to do in extreme heat. Individuals out in the heat lose electrolytes like sodium, potassium, and chloride and need added electrolytes to prevent cramping and excessive sweating that can strain the body. Dehydration can be dangerous, leading to heat exhaustion and possible heat stroke. If gulping water all day seems like a lot, remember that not all hydration must come from drinking water; there are hydrating foods that contain enough water that can be incorporated.
Sweating is vital for maintaining body temperature, and electrolytes are essential in maintaining the body’s homeostasis. Electrolytes help coordinate muscle contractions, heart function, and the conductivity of electric signals transmitting to and from the nervous system. The kidneys regulate fluid absorption and excretion to maintain electrolyte balance, but an imbalance can occur when electrolyte levels spike or drop. An electrolyte imbalance is caused by a change in the number of electrolytes in the body. Sodium, potassium, and calcium are the common elements most likely to be affected by an electrolyte imbalance. Other reasons why electrolyte levels can change include:
Unhealthy diet
Medications
Kidney problems
It is recommended that instead of focusing on how many glasses of water have been drunk, concentrate on two biomarkers:
When the body is thoroughly hydrated, an individual should go to the bathroom every two to three hours, and the urine should be a pale yellow. If it looks orange, it indicates that the body is trying to conserve water and needs further hydration.
Hydrating Foods
Consulting a doctor or nutritionist is recommended to help determine what foods are safe for the individual if there are underlying conditions or other health concerns. Here are a few hydrating foods that contain at least 80 percent water that can be eaten throughout the hot day to maintain body hydration.
Apples
Best known for their fiber content (up to 5 grams), they are also more than 80 percent water.
A quick crunchy snack with potassium, vitamin B6, C, and magnesium.
Watermelon
These can be up to 92 percent water.
Contain vitamin A, B6, and C, plus lycopene and antioxidants.
Watermelon can be cubed by itself or with feta cheese, olive oil, salt, pepper, and basil for a sweet-savory salad.
Peaches
These can contain up to 88 percent water, fiber, protein, and vitamin C.
Peaches can be added to salsas or incorporated into a salad.
Carrots
Carrots are around 90 percent water.
Rich in beta carotene, which the body uses to make vitamin A.
Vitamin A helps the eyes convert light into a signal sent to the brain, allowing for better sight in dim to dark light.
Vitamin K
Potassium
Fiber
Cucumbers
Cucumbers have more than 96 percent water.
They also contain potassium, phosphorus, magnesium, and some calcium.
They contain nutrients known as cucurbitacins, which can have an anti-diabetic effect.
Fisetin is an anti-inflammatory substance that helps brain health.
Potatoes
The waxy variety contains more water, as much as 80 percent.
They contain potassium, vitamin C, fiber, and minerals.
Have them baked or roasted with skins to keep as much potassium as possible.
Tomatoes
Tomatoes are almost 95 percent water.
They contain cancer-fighting carotenoid lycopene, vitamin A and C, and potassium.
Sliced onto sandwiches, sauteed into pasta, or blended into a gazpacho.
Cantaloupe
90 percent water.
Contains beta-carotene, fiber, and vitamin C.
It can be eaten by itself, chopped into salads or smoothies.
Plain yogurt
One cup of plain yogurt is around 88 percent water.
It contains protein, gut probiotics, calcium, zinc, magnesium, potassium, and phosphorus.
Top with some berries for extra hydration.
These are a few hydrating foods that can help with the intense heat. Others include zucchini, iceberg lettuce, strawberries, blueberries, celery, broccoli, and cauliflower. Healthy H2O levels benefits include:
Decreased appetite.
Improved physical performance during exercise.
Increased energy levels.
Optimal brain function.
What Are The Most Hydrating Foods?
References
Bergeron, Michael F. “Hydration and thermal strain during tennis in the heat.” British journal of sports medicine vol. 48 Suppl 1, Suppl 1 (2014): i12-7. doi:10.1136/bjsports-2013-093256
Gauer, Robert, and Bryce K Meyers. “Heat-Related Illnesses.” American family physician vol. 99,8 (2019): 482-489.
Karppanen, H et al. “Why and how to implement sodium, potassium, calcium, and magnesium changes in food items and diets?.” Journal of human hypertension vol. 19 Suppl 3 (2005): S10-9. doi:10.1038/sj.jhh.1001955
Schiefermeier-Mach, Natalia, et al. “Electrolyte Intake and Major Food Sources of Sodium, Potassium, Calcium, and Magnesium among a Population in Western Austria.” Nutrients vol. 12,7 1956. 30 Jun. 2020, doi:10.3390/nu12071956
Strimbu, Kyle, and Jorge A Tavel. “What are biomarkers?.” Current opinion in HIV and AIDS vol. 5,6 (2010): 463-6. doi:10.1097/COH.0b013e32833ed177
Nutrition is how the body utilizes consumed food. Nutrition plays a role in chronic pain; lifestyle behaviors can influence how food contributes to illness/diseases. A common cause of chronic pain is chronic systemic inflammation. Inflammation plays a role in many chronic disease conditions, including diabetes, heart disease, and cancer. Reducing inflammation can be achieved by adjusting diet to get individuals back to feeling better quickly and to aid them in maintaining and improving their overall health. Injury Medical Chiropractic and Functional Medicine Clinic offer diet and nutritional supplements guidance as part of a personalized treatment plan.
Inflammation
The purpose of the inflammatory response includes:
Isolate the dangerous bacteria, viruses, or damaged cells.
Flush out the dead cells and other damaging substances.
Reductions of comorbidities like obesity and cardiovascular disease.
Reducing healthcare costs.
Vitamin and Mineral Supplements
Diet and nutritional supplements provide added essential nutrients to a damaged, inflamed, or injured body. Dietary supplements improve overall health and wellness.
Vitamin D and calcium tablets help maintain optimal bone health, as low vitamin D levels can lead to back pain.
Vitamins E and C, combined with copper, help with blood production, tissue repair, and brain and skin health.
Folic acidcan help with joint pain and myofascial pain.
B Vitamins can help with pain and prevent liver dysfunction.
Nutritional supplements support the body until the body and/or organs have correctly healed. Recovery from an injury could cause body stress that can interfere with the healing process. Diet and nutritional supplements expedite the healing and recovery process by:
Helping overcome dietary deficiencies.
Improving immune system function.
Detoxifying toxins.
Contain antioxidants that help the body stay toxin-free.
Chiropractic restores and realigns the body by incorporating supplements to nourish the body tissues and recover optimally from injury.
InBody Nutrition
References
Dragan, Simona, et al. “Dietary Patterns and Interventions to Alleviate Chronic Pain.” Nutrients vol. 12,9 2510. 19 Aug. 2020, doi:10.3390/nu12092510
Lee, Mi Kyung, et al. “The use of nutritional guidance within chiropractic patient management: a survey of 333 chiropractors from the ACORN practice-based research network.” Chiropractic & manual therapies vol. 26 7. 20 Feb. 2018, doi:10.1186/s12998-018-0175-1
Li, Chuan, et al. “Macrophage polarization and meta-inflammation.” Translational research: the journal of laboratory and clinical medicine vol. 191 (2018): 29-44. doi:10.1016/j.trsl.2017.10.004
Nutrition and Chronic Pain https://www.iasp-pain.org/resources/fact-sheets/nutrition-and-chronic-pain/
Pahwa R, Goyal A, Jialal I. Chronic Inflammation. [Updated 2021 Sep 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK493173/
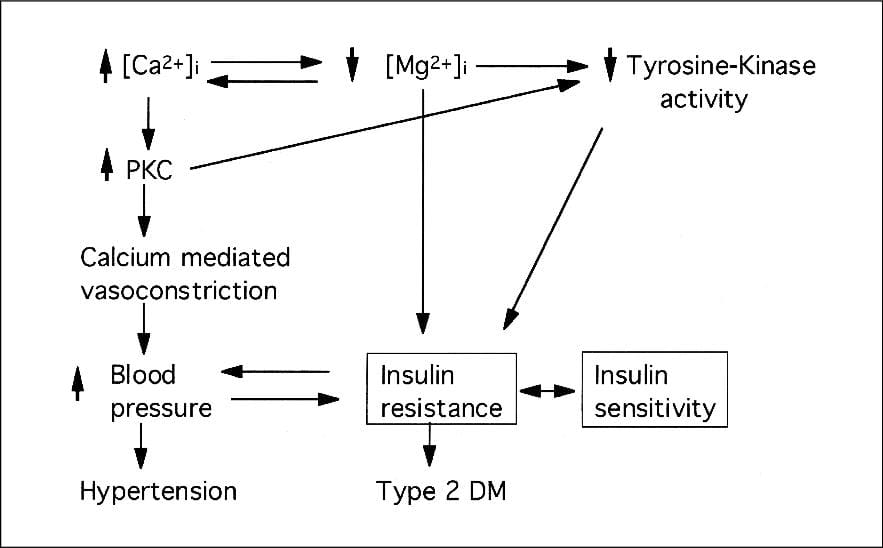
The body requires energy to move around and get to places as fast as possible. The primary energy source is the blood glucose in the body, which helps provide power for the body and the brain, muscle cell tissues, and the blood cells that travel to each body’s organs. When disruptive forces start to affect the body, like chronic stress, endocrine disruptors, or lifestyle choices, it can cause the glucose levels to either increase or decrease depending on the severity. When glucose levels become too high, it can cause hyperglycemia or diabetes to develop. When they are too low, it can cause hypoglycemia. The body also suffers when there aren’t enough nutrients, minerals, or vitamins to provide energy to the body as symptoms of fatigue and insulin resistance begin to rise. Fortunately, there are ways to boost the body’s glucose levels naturally. Today’s article focus on a mineral known as magnesium, its benefits, and how it affects insulin resistance in the body. Refer patients to certified, skilled providers specializing in endocrine treatments for individuals with insulin resistance. We guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is critical for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
What Is Magnesium?
Have you been feeling weird pins and needles sensations in certain parts of your body? Are you suffering from chronic fatigue and muscle cramps? Have you lost your sense of appetite? Or have you felt muscle spasms in your arms or legs? Many of these symptoms are signs that your body is suffering from low levels of magnesium in your body. Research studies have defined magnesium as the fourth most common mineral in the body that provides fundamental functions for regulation. Magnesium can be found in certain foods like leafy greens, chocolate, nuts, fruits, and meats that are riched with this mineral and can be regulated in homeostasis in the intestines, kidneys, and bones in the body. Additional research studies have shown that magnesium is essential for maintaining the body’s normal organ and cellular function. Magnesium also ensures that each organ functions normally and is transported through the entire body by the blood cells. Magnesium also plays a vital role in the body’s energy production as it helps regulate glycemic control.
What Are Its Benefits?
As the fourth common mineral in the body, magnesium helps the body in many ways as it provides energy to other organs and body systems. Some of the benefits that magnesium provides, as research has shown, include:
Reducing insomnia
Prevent metabolic syndrome
Reduce migraines and headaches
Helps with pregnancies
Reduce asthmatic symptoms
Relieve muscle cramps
Additional information has shown that magnesium can help those with anxiety by modulating the HPA (hypothalamic pituitary adrenal) axis and substrating the stress response system in the body. Magnesium also plays a role when it comes to glucose levels in the body and affects insulin resistance.
An Overview Of Magnesium & Insulin Resistance-Video
Are you feeling migraines and headaches popping up out of nowhere? Have your muscles started to ache and cramped? Have you been experiencing asthmatic symptoms more frequently? Or have your blood glucose levels begun to rise? If you have been suffering from any of these symptoms, you could suffer from magnesium deficiency. The video above explains what happens when the body is experiencing insulin resistance due to magnesium deficiency. Research studies have found that magnesium deficiency is not uncommon worldwide, as early signs of magnesium deficiency can cause nausea, vomiting, and weakness in the body while causing metabolic syndrome and type 2 diabetes. Surprisingly, diabetes is one of the most common causes of magnesium deficiency and insulin resistance.
How Does Magnesium Affect Insulin Resistance?
Research studies have found that magnesium deficiency in the body can increase the risk of insulin resistance and cause the body to become dysfunctional. When metabolic imbalances are associated with trending low or alert, low magnesium levels in the body, it can increase the serum CRP-hs, cause headaches, weight gain, and an increased risk for metabolic syndrome, insulin resistance, and type 2 diabetes. The intestines will be impaired in intestinal absorption while the blood glucose levels will increase and cause type 2 diabetes to form. However, additional information has also been provided that when an individual begins to take magnesium regularly, it can help dampen the effects of insulin resistance by regulating the blood glucose levels in the body. Many individuals with pre-existing diabetes can take a bit of magnesium to improve their blood glucose levels and continue on their health journey.
Conclusion
Incorporating supplements and minerals like magnesium could help lower the risk of insulin resistance and manage type 2 diabetes. The body needs the energy to function normally and move around constantly. Magnesium is a common mineral that can help regulate the organ’s functions and helps regulate blood glucose levels. When the body starts to suffer from magnesium deficiency, it can cause various issues that can make a person miserable while the body starts to become dysfunctional. Incorporating magnesium as part of a healthy lifestyle for the body can provide the necessary energy that a person needs to function and help them along their health and wellness journey.
References
Al Alawi, Abdullah M, et al. “Magnesium and Human Health: Perspectives and Research Directions.” International Journal of Endocrinology, Hindawi, 16 Apr. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5926493/.
Boyle, Neil Bernard, et al. “The Effects of Magnesium Supplementation on Subjective Anxiety and Stress-A Systematic Review.” Nutrients, MDPI, 26 Apr. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5452159/.
Gröber, Uwe, et al. “Magnesium in Prevention and Therapy.” Nutrients, MDPI, 23 Sept. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4586582/.
Kostov, Krasimir. “Effects of Magnesium Deficiency on Mechanisms of Insulin Resistance in Type 2 Diabetes: Focusing on the Processes of Insulin Secretion and Signaling.” International Journal of Molecular Sciences, MDPI, 18 Mar. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6470576/.
Razzaque, Mohammed S. “Magnesium: Are We Consuming Enough?” Nutrients, MDPI, 2 Dec. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6316205/.
Schwalfenberg, Gerry K, and Stephen J Genuis. “The Importance of Magnesium in Clinical Healthcare.” Scientifica, Hindawi, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5637834/.
Wang, Jinsong, et al. “Dietary Magnesium Intake Improves Insulin Resistance among Non-Diabetic Individuals with Metabolic Syndrome Participating in a Dietary Trial.” Nutrients, MDPI, 27 Sept. 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3820051/.
The gut system is a massive ecosystem that helps modulate the body’s immune system and metabolic changes that the body itself is going through. The gut system provides the body with the necessary nutrients to function correctly and transports these nutrients to their respective sections like the endocrine system, the nervous system, and the musculoskeletal system to do their jobs. When gut disorders start to affect the intestinal walls, it can cause the inflammatory cytokines to attack the gut walls due to bacteria and nutrients leaking out of the tight junctions. Fortunately, there are therapeutic ways to help the gut system and prevent inflammation from causing more issues in the gut. Today’s article looks at gut metainflammation and how nutraceuticals can help many individuals with gut metainflammation. Referring patients to qualified, skilled providers who specialize in gastroenterology treatments. We provide guidance to our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is critical for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
What Is Gut Metainflammation?
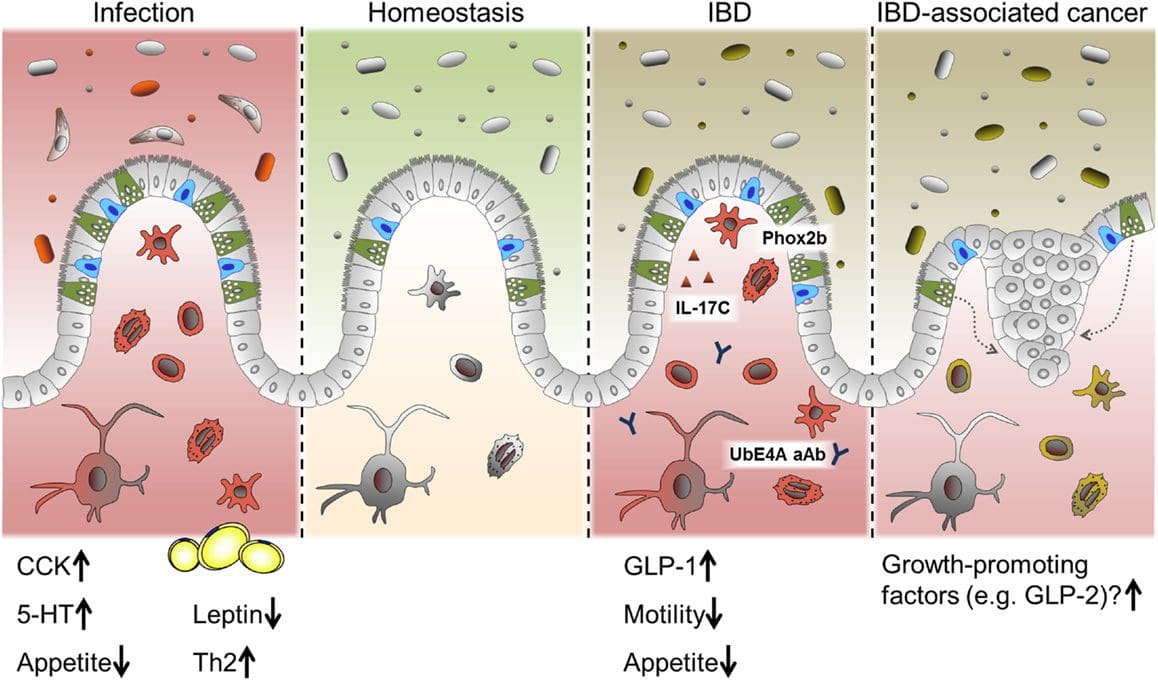
Does your gut system feel sore or tender to the touch? Do ordinary factors like stress, sleep problems, hormone imbalances, and cardiovascular issues affect you more than they should have? Have you experienced inflammatory gut issues like IBS or leaky gut? Having any gut disorder is no laughing matter for your health. When the gut system is experiencing chronic low‐grade inflammatory sequela, this is what gut metainflammation is in the body. Gut metainflammation is defined as an over‐activation of immunity in the gut that leads to increased production of inflammatory cytokines, thus referring to metabolism-induced inflammation. Research studies have shown that when the gut is experiencing metainflammation, it causes a disturbance to the neurometabolic pathways. This causes an increase in the aging processes and metabolic signaling issues the gut is trying to provide for the body. Other research studies have shown that metainflammation is one of the primary markers for metabolic disorders like obesity, type 2 diabetes, and NAFLD (nonalcoholic fatty liver disease). Gut metainflammation also causes an increase in peripheral and central inflammation that can cause gut disorders like leaky gut to allow bacteria and toxins to enter the bloodstream, thus leading to peripheral and central inflammation of the body.
Treatments For GI Disorders-Video
Have you experienced a leaky gut? Do you feel tired throughout the entire day? Have you experienced any food sensitivities in your gut? These gut issues are due to gut metainflammation that can impact a person’s health and quality of life. When this occurs, the body will become dysfunctional, and other issues will arise unless it is treated right away. The video above shows how treatments are available for alleviating motility disorders and GI disorders affecting the gut system. Utilizing treatments beneficial to the gut system can help dampen the effects of metainflammation and other gut disorders from progressing in the body. Some treatments that can help with draining metainflammation in the gut system can be found by changing dietary lifestyles and incorporating nutraceuticals that are beneficial to the gut.
Controlling Gut Metainflammation Through Nutraceuticals
Research studies have shown that since trillions of microbial cells make up the gut microbiota when factors like obesity, metainflammation, and impaired insulin activity affect the gut, it can cause the immune cells to reactivate and reinforce the inflammatory process to attack the gut system. When the gut system becomes dysfunctional, many individuals try to find ways to alleviate gut inflammation. One of the treatments is by incorporating nutraceuticals to provide relief from gut metainflammation. Research studies have mentioned that combined with functional foods can help provide a positive influence on the body’s metabolism and the gut microbiota. Nutraceuticals help give the body the necessary nutrients it deserves and help dampen any effects from disorders affecting the body’s gut, immune, and metabolic components. Two nutraceuticals can help control gut metainflammation: curcumin and peptides.
Curcumin & Peptides For Gut Metainflammaion
From turmeric (Curcuma longa) root/rhizome and used traditionally for dyspeptic conditions, research studies have mentioned that curcumin and its anti-inflammatory metabolites can help influence the gut microbiota. What curcumin does to the gut is that it helps decrease the inflammasome signaling while decreasing oxidative stress via the Nrf2‐keap1 pathway. Curcumin can also help improve flexibility and mobility in the body while inhibiting the activation of a peroxisome proliferator‐activated receptor‐gamma pathway. Additional information has provided that curcumin can help not only reduce oxidative stress and even prevent neurodegeneration.
Peptides or BPC‐157 (Body Protection Compound) are derived from human gastric juice that is cytoprotective and anti‐inflammatory that helps support the gut mucosal lining. Research studies have shown that peptides play a critical role in maintaining intestinal homeostasis while being effective in decreasing metainflammatory signaling in the gut microbiota. When there is metainflammation in the gut, peptides can help improve cell survival under oxidative stress conditions by downregulating TNF‐alpha in the body. Incorporating peptides can help improve GI mucosal integrity from meta inflammation and help the gut function normally.
Conclusion
The gut is home to trillions of microorganisms that help keep the body’s functionality and regulate immunity from various diseases. When unwanted factors like metainflammation start to infiltrate the gut, it can lead to dysbiosis and wreck the intestinal walls. Nutraceuticals like curcumin and peptides have beneficial properties that help repair the intestinal walls while dampening inflammatory effects from progressing further in the gut system. Incorporating nutraceuticals is helpful for many individuals who suffer from gut disorders and improve their health by replenishing their nutrients in the body.
References
Boulangé, Claire L, et al. “Impact of the Gut Microbiota on Inflammation, Obesity, and Metabolic Disease.” Genome Medicine, BioMed Central, 20 Apr. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4839080/.
Di Meo, Francesco, et al. “Curcumin, Gut Microbiota, and Neuroprotection.” Nutrients, MDPI, 11 Oct. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6835970/.
Gubatan, John, et al. “Antimicrobial Peptides and the Gut Microbiome in Inflammatory Bowel Disease.” World Journal of Gastroenterology, Baishideng Publishing Group Inc, 21 Nov. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8613745/.
Laparra, J M, and Y Sanz. “Interactions of Gut Microbiota with Functional Food Components and Nutraceuticals.” Pharmacological Research, U.S. National Library of Medicine, 13 Nov. 2009, https://pubmed.ncbi.nlm.nih.gov/19914380/.
Scazzocchio, Beatrice, et al. “Interaction between Gut Microbiota and Curcumin: A New Key of Understanding for the Health Effects of Curcumin.” Nutrients, MDPI, 19 Aug. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7551052/.
Scheithauer, Torsten P M, et al. “Gut Microbiota as a Trigger for Metabolic Inflammation in Obesity and Type 2 Diabetes.” Frontiers in Immunology, Frontiers Media S.A., 16 Oct. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7596417/.
Tilg, Herbert, et al. “The Intestinal Microbiota Fuelling Metabolic Inflammation.” Nature Reviews. Immunology, U.S. National Library of Medicine, 6 Aug. 2019, https://pubmed.ncbi.nlm.nih.gov/31388093/.
Maintaining a healthy weight is challenging, especially Fridays, Saturdays, Sundays, and extended weekends, increasing the risk of binge eating and weight gain. This is where healthy cheat meals and snacks come into play to help individuals stick to their diet while enjoying healthy junk food. Plus, finding the proper high-calorie carb-packed meal can help optimize the body’s hormones to prevent adverse effects on metabolism and hunger.
Cheat Meals
One way to look at a diet and still have the flexibility for sweet or savory foods is to set up the flexibility. To maintain health, practice portion control and eat healthy foods 80% of the time, allowing a 20% margin for the junk foods. To improve health, eat healthy foods 90% of the time, and allow a 10% margin until a health goal is reached.
Cheeseburger without the Buns and Sweet Potato Fries
They can be made healthy with lean ground beef, beans, peppers, cheese, avocado, tomatoes, and jalapeños for a meal that incorporates quality protein and healthy fats.
It can be made vegetarian by removing the meat and adding more beans and vegetables.
Dark chocolate contains monounsaturated fats that can help improve cholesterol, blood sugar, and insulin levels.
Dark chocolate also supplies vitamins, minerals, and antioxidants for heart and brain health.
Dietician Nutritionist
These are a few examples; the objective is to get individuals to learn to create their healthy cheat meals A diet or adjusting for a more nutritional food plan should always start with a nutritionist, dietician, or health care provider. They can help develop a customized plan that fits an individual’s specific needs. It is about finding the balance and creating a positive relationship with food.
Fibromyalgia Food Choices Nutraceutical Options
References
Coelho de Vale R, et al. (2016). The benefits of behaving badly on occasion: Successful regulation by planned hedonic deviations.
doi.org/10.1016/j.jcps.2015.05.001
Kuijer RG, et al. (2014). Chocolate cake. Guilt or celebration? Associations with healthy eating attitudes, perceived behavioral control, intentions, and weight loss. DOI:
10.1016/j.appet.2013.11.013
Murray SB, et al. (2018). Cheat meals: A benign or ominous variant of binge eating behavior? DOI:
10.1016/j.appet.2018.08.026
Warren JM, et al. (2017). A structured literature review on the role of mindfulness, mindful eating, and intuitive eating in changing eating behaviors: Effectiveness and associated potential mechanisms. DOI:
10.1017/S0954422417000154
Inside the body lies the internal organs that provide the nutrients and energy for the body to stay in motion. The gut system helps the body energy by digesting the consumed food that gets turned into energy and nutrients beneficial for the vital organs, muscles, tissues, and growth that the body needs. The gut system also helps regulate the other body systems like the musculoskeletal system, the immune system, central nervous system, and the endocrine system. The gut system operates by transporting these nutrients to make the body operational, to name a few needs. When unwanted issues start to enter the gut system and cause havoc, it can lead to many chronic problems that will cause the body to be in constant pain while causing other issues that affect the entire body. Today’s article will look at how different gut issues start to affect the body and how an amino acid named glutamine can provide beneficial relief to various gut issues. Referring patients to qualified and skilled providers who specialize in gastroenterology treatments. We guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is essential for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
How Gut Issues Affect The Body
Have you been experiencing pain located in your gut? Does your gut seem to be extra sensitive after consuming food? Have you been anxious or stressed that it has been affecting your body? Experiencing these symptoms are signs that you might have some gut issues that are affecting your body. Research studies have found that gut issues or disorders usually develop when the gut has either underproduced or overproduced the beneficial gut bacteria that can influence harmful bacteria to attack the gut’s intestinal walls. Gut issues can also be influenced due to lifestyle choices or autoimmune disorders that affect the gut and the rest of the body and its systems. Additional information has found that when the microbiome is being challenged with factors that change the physiology of the gut microbiome. These changes will cause an increase in the intestinal permeability, which allows the harmful bacteria to leak out, causing the immune system to attack the exposed bacteria at the intestinal walls leading to inflammatory issues.
Other research studies have found that gut bacteria provides an essential role in the body as it helps supply the vital nutrients beneficial for the body’s health. When abnormal changes affect gut bacteria, the gut ecosystem accelerates dysbiosis, causing many chronic issues. Many individuals will begin to lose their quality of life due to pain. Fortunately, there are ways to alleviate the chronic issues affecting the gut and even help lower the harmful bacteria by replenishing the beneficial bacteria while reducing inflammatory markers.
An Overview About Glutamine-Video
Have you been experiencing issues that are affecting your gut? Has your torso area been feeling tender to the touch? How about random pain spots that are in your abdomen? You could be experiencing gut issues affecting your overall health and wellness. Why not incorporate glutamine into your daily supplementation. Research studies mentioned that glutamine is an amino acid with beneficial properties in replenishing the immune system and metabolizing in the gut and other vital organs that need glutamine to nourish the cellular structure for the body to feel better and provide energy for many individuals. The video above includes information about the benefits of glutamine and how it can help the body.
How Glutamine Helps The Gut
As stated earlier, glutamine is an amino acid with beneficial properties that are utilized to provide energy for the entire body. Research studies have shown that glutamine in the gut system can maintain the intestinal structure and function as the body ages while regulating the tight junction proteins. Glutamine has also helped modulate the gut intestinal permeability effects of HPA-axis stress that affects the gut and protects the cells from apoptosis and cellular stress. Additional research studies have provided that when individuals take glutamine as part of their daily regime, they will have a better inflammatory response and redox balance in the gut with the combination of physical activities. Utilizing glutamine for gut health can help improve the gut function and gastrointestinal permeability function for many athletic individuals.
Conclusion
Overall, the gut system utilizes glutamine for optimal gut health in dampening the effects of gut issues and disorders that will affect the body. The gut provides the transportation of the essential nutrients for the rest of the body systems that need them to function correctly. When unwanted factors or unhealthy lifestyles affect the gut system, it can increase the harmful bacteria in the gut and diminish the beneficial bacteria. This will cause the inflammatory cytokines to attack the intestinal permeability walls and cause more issues that will affect the body. Beneficial supplements and nutrients that help alleviate inflammatory factors or alleviate gut issues are there to provide relief by dampening these harmful effects and repairing the body. Incorporating glutamine into your gut will help the body recover over time and become pain-free.
References
Almeida, Ewin B, et al. “L-Glutamine Supplementation Improves the Benefits of Combined-Exercise Training on Oral Redox Balance and Inflammatory Status in Elderly Individuals.” Oxidative Medicine and Cellular Longevity, Hindawi, 22 Jan. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7204202/.
Clapp, Megan, et al. “Gut Microbiota’s Effect on Mental Health: The Gut-Brain Axis.” Clinics and Practice, PAGEPress Scientific Publications, Pavia, Italy, 15 Sept. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5641835/.
Cruzat, Vinicius, et al. “Glutamine: Metabolism and Immune Function, Supplementation and Clinical Translation.” Nutrients, MDPI, 23 Oct. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6266414/.
Kim, Min-Hyun, and Hyeyoung Kim. “The Roles of Glutamine in the Intestine and Its Implication in Intestinal Diseases.” International Journal of Molecular Sciences, MDPI, 12 May 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5454963/.
Nouvenne, Antonio, et al. “Digestive Disorders and Intestinal Microbiota.” Acta Bio-Medica : Atenei Parmensis, Mattioli 1885, 17 Dec. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6502202/.
Zhang, Yu-Jie, et al. “Impacts of Gut Bacteria on Human Health and Diseases.” International Journal of Molecular Sciences, MDPI, 2 Apr. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4425030/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine