With the last article, we talk about how our gut system actually works. With the many microbes that inhabit our intestines, we do try to our best to lead a healthier lifestyle. Here at Injury Medical, local chiropractors and health coaches inform our patients about functional medicine as well as helping them to prevent a leaky gut. Here we will talk more about what the microbiomes in our intestines do when we are exposed to harsh environments.
The Microbiome
The significant role of the microbiome in the epithelial barrier integrity and breakdown. However, we can�t have a conversation with patients about intestinal permeability and food sensitivities without telling them about the role the microbiome plays.
The Wheat zoomer is rich with data but adds the Gut zoomer with the patients; the results are more accurate.
Microbial Influence on our Intestines
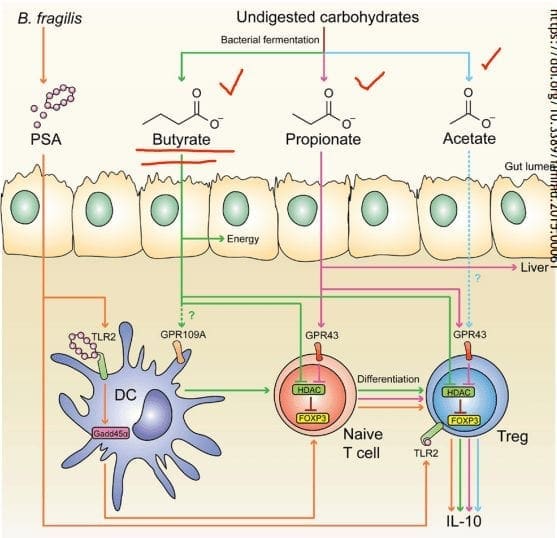
Immune influence: One of the leading roles that microbiomes play in the immune system is that it generates byproducts of carbohydrates/fiber fermentation that will influence T-cell differentiation. Without the distinction, we will see an increase of being at high risk of autoimmune diseases, allergies, autism, and asthma.
SCFAs (Short Chain Fatty Acids): The food we consume gets fermented for good bacteria to feed on. SCFAs creates fermented fibers by commensal microbes into Butyrate, Propionate, Acetate. These three are essential to the intestinal immune system. These SCFAs can influence T-cells differentiation differently, but it still gets the same results.
T-cell Differentiation: na�ve T-cells that activate the immune response to T-regs (police cells) to signal B-cells, and it can be a good thing. But if the T-cells activate and differentiate the wrong cells, it will cause inflammation.
When T-cells differentiation is less abundant, there will be a higher incidence of food sensitivities, autoimmune disease, asthma, and allergies. But when there is an abundance of butyrate, the patients have lower rates of colon cancer and colitis.
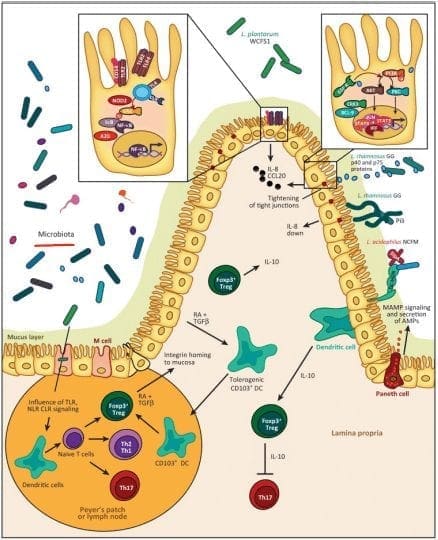
Tight Junction: Lactobacillus plantarum and Lactobacillus rhamnosus are the reinforcers for the tight junction while inducing TLR (toll-like receptors) outside the intestinal epithelial walls, as well as increasing the abundance of zonulin-occludin into the tight junction.
SCFAs also play a vital role in the tight junction by lessening the extent propionate, inducing LOX (lipoxygenase) activity and increasing tight junction�s stability while reducing permeability.
Pathogens/Pathobionts: Can be an influence in the epithelial barriers as they can be opportunistic or conditionally pathogenic. Various pathogens like enteropathogenic E.coli can alternate the tight junction�s system. However, if there is a low abundance of L. plantarum, then it will lead to infections and disruption as well as disorganization of the actin cytoskeletons. This can be reversed by incubating the epithelial cells with L. plantarum to create a high density of actin filaments to the tight junction and repair itself.
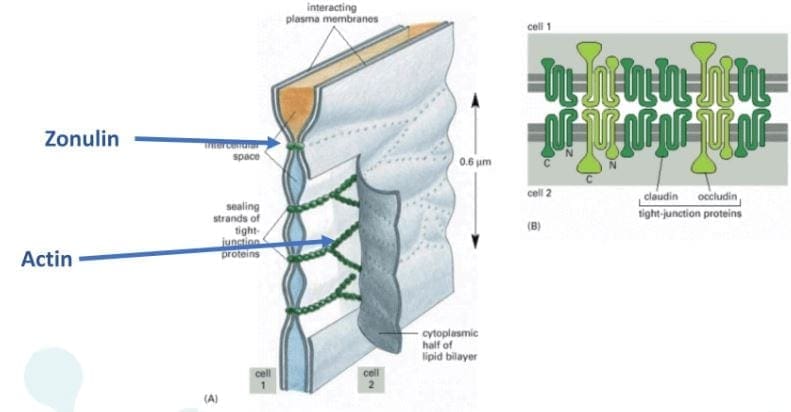
Zonulin, actin, and LPS: In the previous article, zonulin is the �gatekeeper� proteins that are responsible for opening and closing the tight junction. We talked about how if there is a low count of zonulin, it can cause inflammation, but if the zonulins are high, they can increase the IP and may facilitate enteric translocation by disassembling the tight junction. With less zonulin, it can be an overgrowth of b bacteria cells, thus causing more inflammation.
Actins are the structural and functional cells in the tight junction. However, if bacteria enter the actin cell walls, the bacteria will release toxins to the cell walls, it not only damages it but causes it to leak as well. This will make the damage actin cells not only paracellular but also intracellular to the damage actin cell walls.
Actin walls can also be affected when surfactants are involved. Surfactants are food agents and are known to affect the absorption of food substances in the gastrointestinal tract. They are not problematic, but when there is a low count on TEER, it can increase permeability and disband the tight junction.
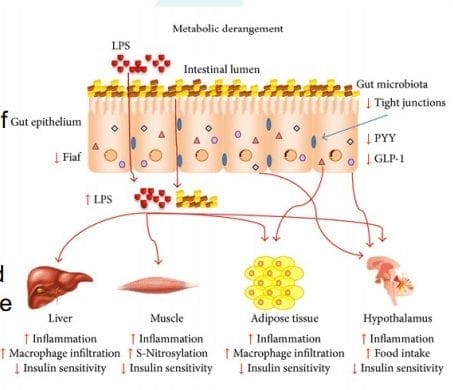
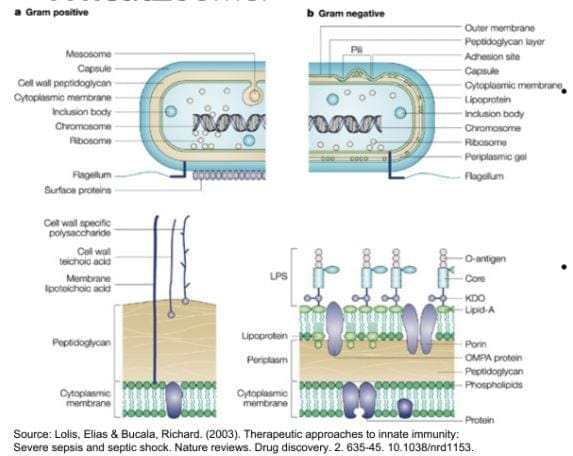
LPS (Lipopolysaccharide) acts as a barrier and is recognized by the immune system as a marker for detecting bacterial pathogen invasion. It�s responsible for the development of inflammatory response in our gut.
Diet and Lifestyle
Diet and lifestyle contributions to the epithelial barrier integrity and breakdown. With the Wheat and Gut Zoomer helping out our intestinal barriers. Specific diets and lifestyles can also play effect to what is causing discomfort to our gut. These factors can cause our gut to be an imbalance, gastro discomfort, inflammation on our intestinal epithelial barriers.
Gluten: Gliadin is the main peptide that can cause gluten sensitivity. The gliadin protein can bind with many microbes, causing discomfort to our intestines and gut. Plus giving us an autoimmune disease, skin allergens, and chronic illnesses.
Keto/High Fat Intake: Increase fat meals cause an increase of permeability, and if a patient has a high gram-negative, it will cause problems. But it can be beneficial, to those who don�t have the gram-negative bacteria in their system but, certain microbes like SCFAs do cling onto these fatty substances. In order to give patients an accurate result use both the Gut Zoomer and Wheat Zoomer to better the chances. Higher fat meals suppress beneficial bacteria. Causing a double risk of toxins in the bloodstream as well as inflammation.
Alcohol: Patients are more willing to give up alcohol than gluten. Alcohol can be a stress reliever but can lead to addiction. It can be one of the causes of redistribution of the junctional proteins. One glass of wine a day is ok, but some patients don�t see alcohol as a mediator for reducing problems.
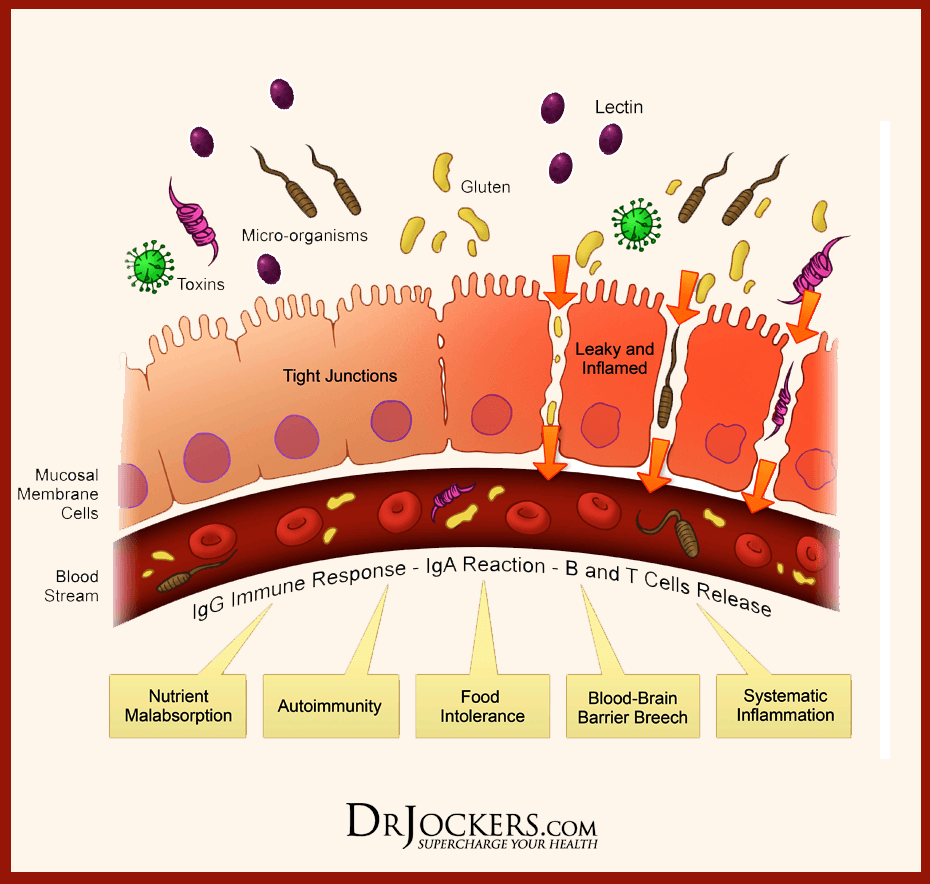
Lectins: Lectins are contributors to permeability and impair the integrity of the intestinal epithelial layer, allowing passage through. Antibiotics for WGA can help lower the permeability of the intestinal wall barriers.
Stress: Stress can cause discomfort and permeability in the intestinal epithelial barrier from high levels of cortisol.
Conclusion
Yes, gluten can cause inflammation in the intestinal epithelial barriers, but many factors that we discussed are also factors that can cause physiological assaults on the barrier�s integrity and stability of the intestinal ecosystem. Dr. Alexander Jimenez informs our patients about the importance of how functional medicine works with the combination of the Gut Zoomer and the Wheat Zoomer. This is not only protecting our gut but by giving us the information on what we can do to prevent a leaky gut.
Today local chiropractors will be giving a description of the wheat zoomer. We will be giving a brief description of each panel, its markers, and the basic interpretations of the test. We will also be discussing the considerations for the patients and providers before we take The Wheat Zoomer test.
What is a Wheat Zoomer test?
The Vibrant wheat zoomer has 6 test in one to identify if the patient has wheat and gluten sensitivity. The Vibrant wheat zoomer does give our patients a thorough evaluation and we ask our patients if they started to be gluten-free or was gluten-free, either from birth or not and how much gluten-contained food did they eat. One of the best ways to ensure that our patients may have a gluten sensitivity is that if they have a food diary for us to look over and that way we can determine how severe of the wheat zoomer.
IgA vs IgG
In order for us to know about the wheat zoomer in our patient�s body, we must know about the immunoglobulins. The first one is IgA. IgA immunoglobulins are mucosal and are found primarily in the epithelial lining of the body: intestinal tract, lungs esophagus, blood-brain barrier and around internal organs. They are:
The first line of defense.
More accurate to our gut.
IgG immunoglobulins found in the blood system and are numerous in the body They are considered �systemic� and are non-specific to any one location. Not all IgG antibodies are sensitive though, some of them can indicate that an antigen has �leaked� into the blood and the immune system tagged that antigen as a �non-self�. And they are not diagnostic as IgG+IgA, but if IgA is absent, the antibodies are more relevant.
If the patient is recently gluten-free, the antibodies will tell us that the antigen hasn�t cleared out in the patient�s system from past weeks of eating gluten.
Celiac
Celiac is a growing autoimmune disease, about 1% of the population is affective and 1 in 7 Americans have a reaction to wheat or wheat gluten disorder. The Vibrant test can determine a 99% sensitivity and 100% specify on the celiac antibodies.
Total IgA and Total IgG measure both the IgA and IgG to determine the patient�s reactivity to gluten
Cut off for IgA is 160 as well as a bottom 1/3rd
Not all traditional markers for celiac disease doesn�t need to be elevated if tTg2 is elevated.
Intestinal Permeability
Zonulin is the gatekeeper for the intestines and controls nutrient flows and molecules across the membrane. It is a protein complex inside the intestinal tight junctions and can be increased by either gluten and high-fat meals.
Anti-Actin, especially f-Actin is in the smooth muscle of the intestines. Actin is part of the actomyosin complex. Vibrant can isolate f-Actin to get a more accurate picture of the patient�s immune response to the intestines. While antibodies in actin can identify intestinal destruction and indicate autoimmune diseases like connective tissue disease and autoimmune hepatitis.
Lipopolysaccharide (LPS) is produced by gram-negative enterobacteria. It is very potent and can cause inflammation. Plus it�s one of the indications of a leaky gut. Practitioners can draw additional lab test for cardiovascular, inflammatory markers, and diabetes/insulin resistance.
Here at Injury Medical Clinic, we suggest to our patients to try a Vibrant GutZoomer to identify the source of their ailments before we add the Vibrant WheatZoomer.
Gluten-mediated Autoimmunity
Fusion Peptide is the new addition to Wheat Zoomer in 2017. It is cross-linked to tTg and can identified celiac progression from 14 months to 4 years.
Differential Transglutaminases can detect autoimmune reactions to gluten that are not celiac or are becoming celiac. However, gluten is still a trigger but react differently in the celiac autoimmune disease such as:
Transglutaminase 3= skin manifestations of autoimmunity like dermatitis herpetiformis, eczema, and psoriasis.
Transglutaminases 6= neurological manifestations of autoimmunity in the cerebellum like gluten ataxia, gate abnormalities, balance and coordination issues.
Wheat Germ Agglutinin
Wheat Germ Agglutinin is the lectin component of wheat but, it is not a component to gluten. Dr. Jimenez can detect a patient’s low level of Vitamin D absorption from the patient�s results. And Wheat Germ Agglutinin is commonly used as an additive in supplements and the supplement can still be called gluten-free due to the different protein structure.
Gliadin, Glutenin, and Prodynorphin
Gliadin and glutenin are what makes up the super protein in gluten. Most people are reacting to the Gliadin portion of gluten and gliadin binds with tTg2 in celiac and binds zonulin to a leaky gut in patients. Gliadin reacts to any antigens can indicate a sensitivity to gluten in patients and gluteomorphin are peptides in wheat and react as a euphoria receptor to the brain. Prodynorphins antibodies can indicate that gluten reacts to signaling hormones and affect the patient’s mood.
Sadly though, patients do have a hard time withdrawing gluten in their diet since their antibodies are used to the compound and it up to us, here at Injury Medical Clinic to gently push our patients to have the will power to fix what is causing them to have ailments.
Wheat Allergin
Wheat Allergen is the true allergen body. Some patients that already know that they are allergic to wheat from a young age but it doesn�t decrease when wheat is eliminated and can remain long term after the allergic response happens.
Glutenin
Glutenin is the other part of the gluten compound. However it is less common to some people, but some individuals do show reactivity to glutenin, thus still have a gluten sensitivity. But there is no clinical difference to the reactivity to glutenin from high to low molecular weight.
Non-Gluten Wheat Proteins
Surprisingly Vibrant has an advantage to their test as they have a panel for patients that don�t have a gluten sensitivity but a wheat sensitivity. The Vibrant advantage to the unique non-gluten wheat panel shows us that:
Proteins in wheat unrelated to gluten but relevant to immune reactions.
It is 30% of the protein molecular weight of wheat.
Some individuals are more reactive to wheat proteins than gluten itself.
If they are trying to be gluten-free, patients still have to read the labels to see if any hidden wheat starches are in the ingredients. But not all food products are gluten-free if they have the wheat protein in them.
Conclusion
If the patient is trying to be gluten-free but previously ate gluten compound food. They can still feel the reaction if they discovered that they have a sensitivity to gluten by their practitioner. And must take precautions when they are reading the labels of the products they are going to buy and consume. In the next four articles, we will discuss what the Wheat Zoomer can provide as well as, discussing about what causes leaky gut, what actually goes on in our patient�s intestines, and wrapping up on what to do after the Wheat Zoomer heals and restores the gut barrier.
Mostly everyone in the world has a gluten allergy or gluten sensitivity when they consume food. When it comes to food that has the gluten compound, most people read the labels on the products that contain it and have cut the compound out of their diets completely. However, did you know that different foods and products have hidden gluten in them? Even though now and days we read labels from products, as well as, cutting off the source of the problem that is making us ill. Hidden additives like gluten, even in small amounts, can cause problems to those that are allergic or sensitive to the compound. Especially when it comes to the product itself, some regulations may or may not be required to label products that contain gluten.
What is Gluten?
Gluten is the main protein that is found in many grains such as wheat, rye, and barley. It is formed by two proteins which are glutenin and gliadin. And the word �gluten� is Latin for �glue� and when mixed with water, it rises and stretches. Most gluten can be found in some bread, pasta, cereal, and beer.
But in this article, we are going to inform you 8 products that have hidden gluten. Because here at Injury Medical Clinic, we take the time to talk with our patients on what ails their bodies and work on discovering what kind of food allergen or food sensitivity they may have. As well as, finding alternatives to prevent inflammation in their bodies.
8 Products with Hidden Gluten
Medications: Yes, you�ve read that correctly, there is gluten in medication. Surprisingly though, a lot of prescription medicine contains excipients (containing gluten) that actually binds the pills together. This is mostly found in generic over the counter medications but the labeling for the ingredients are not always there.
However, labeling standards are changing due to the Gluten in Medicine Disclosure Act of 2019. This was proposed on April 3, 2019, and introduced by Representatives Tim Ryan (D-OH) and Tom Cole (R-OK). The bill�s intent was to make it easier to identify gluten in prescription medicine and it is telling drug manufacturers that it is required to label medications with the list of their ingredients, their sources and whether the gluten compound is present.
Hopefully with enough signatures and votes that the bill will be passed, however, if you are taking medication and the labels look different; always verify with a pharmacist to see if it is correct. Plus, you can always talk with your pharmacist to confirm that your medicine is gluten-free, so that way you won�t get a bad reaction from it.
Sauces and gravy: Everybody loves any sauces and gravies in the meals they prepared and are excellent in mash potatoes and Thanksgiving dinners. But sauces like soy or teriyaki do contain wheat protein, hydrolyzed wheat starch or wheat flour. While others sometimes contain soy sauce or malt vinegar.
In any recipe that contains a type of sauce for the food you are preparing, especially in creamy sauces and gravies, mostly requires a roux; which is wheat flour mixed with butter. So, whenever you are at your favorite restaurant or have a favorite meal to prepare, get familiar with the sauces, so that way you can know that if they are gluten-free or not.
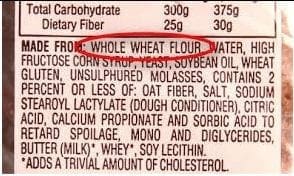
Starches: When we think of starches, our minds go to the potatoes. However, wheat can also be found in starches and starch derivatives. So, whenever you are looking at products that are starchy, look at the ingredient labels and for terms like �wheat starch�, �hydrolyzed wheat starch�, or �contains wheat.�
In order for starches that contain wheat starch to be gluten-free, the wheat compound must remove to less than 20 ppm. And especially in FDA regulated food labels, if the product says �contain wheat�, it is not safe. But food labels don�t apply to barley, rye, or oats, still continue to read the ingredient labels in the case for the wheat compound and if it is not there then the product is safe. For gluten-free starches for those who don�t want to miss out, tapioca starch, rice starch, and potato starch are perfect for frying.
Brown Rice Syrup: This type of sweetener is made from fermented brown rice with enzymes or from barley, which breaks down the starch and transforms it into sugar. Sadly though, this sweetener is not gluten-free and it can be used on its own or be used as an ingredient in a multi-ingredient product. Some companies use brown rice syrup in their products by listing it as �barley� or �barley malt.� And it is a bit problematic for those who have a gluten allergen to this sweetener.
Soups: Who doesn�t love soups. Soup is there for us when we are sick and for comfort when it gets really cold in the fall and winter seasons. But companies use wheat flour or wheat starch as a thickener for those creamier soups that we love in a can and those thickeners can be hidden in the ingredients label. So, if you want pre-packaged soup bases and canned soups for those colder seasons, be sure to read the labels carefully, especially for those creamed-based soup bases and bouillons because they might contain gluten.
Salad dressings: Did you know that many standard salad dressings can wheat flour, soy, or malt vinegar? Not only that but it can contain wheat or gluten-containing additives as a thickener. Plus salad dressings often have artificial colors, flavorings and many other additives that can contain gluten as a sub ingredient. However, if you want to be safe and not have gluten in your salad dressings, simply put in olive oil, lemon, salt, and pepper, and you got yourself a gluten-free salad dressing.
Chips and fries: Chips and fries are the staples for a good burger or hot dog on every barbeque events and parties. Yes, the potato that makes the chips and fries are gluten-free; but the seasonings like malt vinegar and wheat starch do contain gluten. And when we are frying cut potatoes into French fries and chips; the oil that is used to make them can be cross-contaminated with gluten-containing fried foods.
Processed meats: Meat is most likely to be the last place you think that has gluten. However, processed hamburger patties, meatballs, meatloaf, sausages, and deli meats contain gluten. Wheat-based fillers are used to either improve the texture of the meat or bind the meat together. Plus, seasoned or marinated eats can sometimes contain hydrolyzed wheat protein or soy sauce with breadcrumbs are added to bulk up the product.
Conclusion
So if you are at the grocery store getting some food for dinner or meal prepping, it is important to actually read the labeling of the products that you are buying. Whether you have a food allergy or food sensitivity to gluten or any food products, we here at Injury Medical Clinic, listen to what is causing our patients pain to their bodies and offer solutions to fix whatever ailments that the problem is causing.
Functional neurology primarily focuses on the fundamentals of neuron health and it is mainly based on neuroplasticity theories. It’s believed that the brain and the nervous system are capable of changing, and can become malleable, due to a reaction to certain stimulation. The brain can be shaped by sensory, motor, cognitive, or emotional experiences. �
The creation of synapses in the nervous system depends on the stimulation they receive. Neurons which receive too much stimulation are the ones which become stronger and those which don’t receive stimulation become weaker and eventually diminish. It is believed that it is possible to create new neurons even after there has been damage to the nervous system. �
The Role of Functional Neurology
Functional neurology evaluates changes in the nervous system before these become severe health issues. The practice of functional neurology has been adopted by several modalities of practice, such as chiropractic, psychology, occupational therapy and even by conventional healthcare professionals. Functional neurology is commonly practiced by chiropractors. �
The practice of neurology involves applying neuroscience research from laboratory studies to determine how it can be practically applied in health care. The brain is protected by supporting the nervous system. The ultimate goal of functional neurology is to treat brain and nervous system health issues without the utilization of drugs or together with conventional treatment approaches. Functional neurologists can help treat a wide variety of neurological health issues, including: �
Neurodegenerative disorders: Alzheimer�s disease, Parkinson�s disease, dementia, and multiple system atrophy.
Demyelinating conditions: Multiple sclerosis, transverse myelitis, and leukodystrophies.
Trauma and brain injuries: Concussions and whiplash-associated disorders.
Vestibular conditions: Motion sickness, dizziness/disequilibrium, labyrinthitis, vertigo, and Meniere’s disease.
Movement disorders: Tics, restless leg syndrome, myoclonus, and dystonia.
Neuro-developmental conditions: Autism spectrum disorders, ADHD, Asperger’s syndrome, Tourette syndrome, dyslexia, processing disorders, and global developmental delay.
Headaches and pain syndromes: Cluster headaches, complex regional pain syndrome, migraines, and fibromyalgia
Functional neurological disorders which are best referred to as a group of physical, sensory and cognitive symptoms which do not seem to have an identifiable organic etiology.
Functional Neurology Treatment
The primary goal of functional neurology is to promote, support, and restore the optimal function of the brain and the nervous system, as opposed to the absence of pathology. Sometimes it’s not always possible to determine the natural source of a person’s neurological disease and its symptoms. Functional neurology can be particularly beneficial in these instances. �
The patient’s medical history and a non-invasive evaluation are required for diagnosis. Treatment is determined based on the patient’s current and targeted well-being. Any blood tests, x-rays, MRIs and/or other tests are also evaluated. During the evaluation, the healthcare professional will observe all aspects of the patient, including eye movements and posture, which can demonstrate the function of the brain and the nervous system. Blood pressure, pulse, and reflexes are also evaluated. �
Neuro-developmental conditions and behavioral disorders are generally treated with functional neurology. Anxiety is commonly increased in patients with these type of health issues, therefore, it is recommended that the non-invasive evaluation is performed in a way which does not trigger anxiety in the patient. Functional neurology treatment is individualized and every part of the treatment approach is customized to the individual’s treatment requirements. �
Functional neurology emphasizes on encouraging patients to practice self-care so that face-to-face treatment with a healthcare professional does not continue for months or years without end. Home exercise programs are developed to treat the associated health issues, meaning that functional neurology treatment is incorporated into the patient’s daily activities. �
Biochemistry and Nutrition in Functional Neurology
Functional neurology treatment focuses on retraining the brain. Neurons need energy and stimulation to survive and thrive, therefore, functional neurology treatment may involve exercises, such as eye exercises, cognitive activities, balancing activities, and joint adjustments. Different stimulation can affect different regions and pathways in the human brain. �
Moreover, functional neurology treatment may also involve a nutritional and biochemical approach by eliminating several factors which may potentially affect neurons. These can ultimately include toxins, chemicals, and infection, among other factors. Dietary modifications and supplementation may also be included to provide optimal energy for neurons. �
An individualized treatment approach is applied to each individual otherwise there exists the risk of over-stimulating and exceeding the capacity of a patient’s nervous system. The goal of functional neurology treatment is to improve brain and nervous system health, neural processing, communication, and all signaling involving the brain and the entire human body. �
Functional neurology focuses on the diagnosis and treatment of the human brain and the nervous system utilizing sensory and cognitive based treatment methods and techniques to promote, support, and restore neuroplasticity, integrity, and functional optimization. Functional neurology can be utilized to help improve a variety of neurological diseases and health issues, including Alzheimer’s disease. Functional neurology is frequently practiced by chiropractors. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article above is to discuss the purpose of functional neurology in the treatment of neurological disease. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
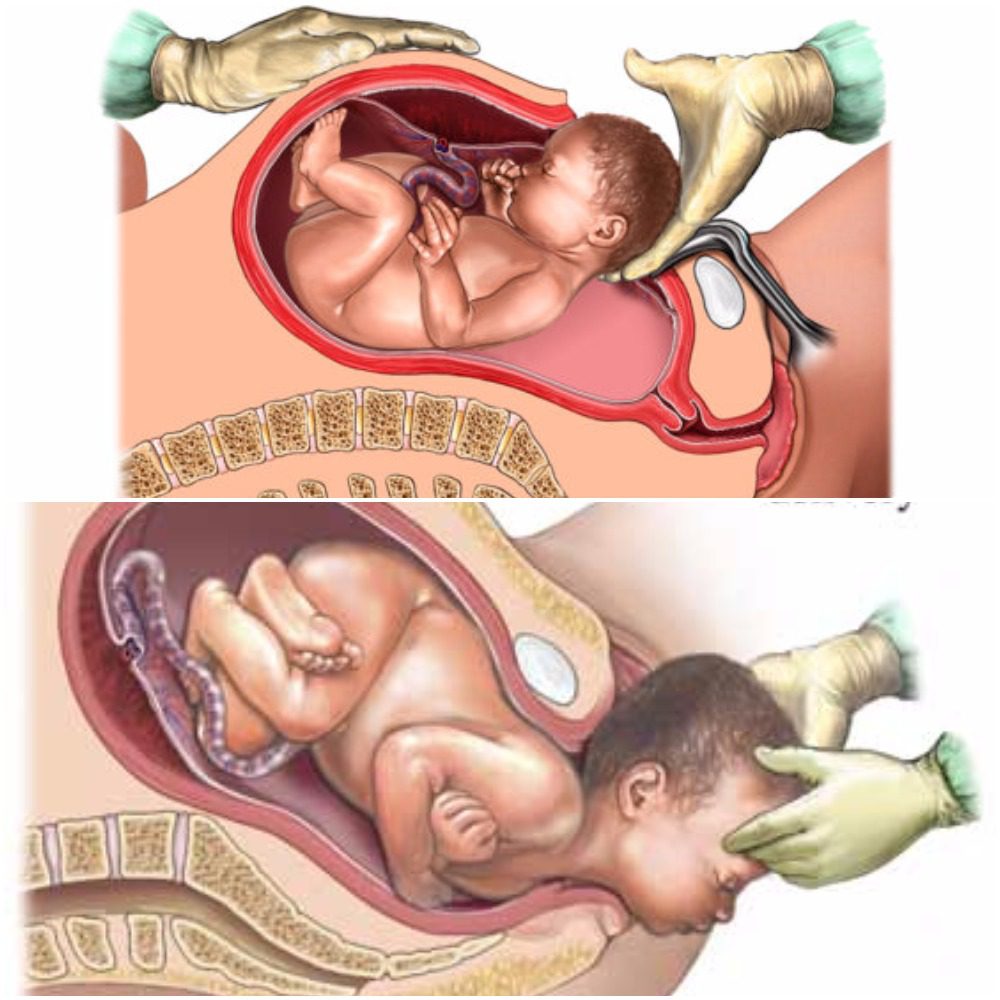
As humans, we depend on microbiomes to stay alive. Microbiomes are essential in fighting off germs and maintaining health. The development of microbiomes begins in utero where the microbes have been isolated to the placenta, fetal membranes, amniotic fluid, and umbilical cord blood, but are mainly transferred from mother to child during birth in a process referred to as “seeding” (1,2). “Seeding”� occurs as the child passes through the mothers vaginal canal and becomes coated in her microbiome. In addition to this, small amounts of microbiomes get transferred to the child as the mother breastfeeds. This early introduction from mother to infant serves as an inoculation process with long term health outcomes for the newborn (2). With the number of cesarean births being higher this decade than in the past, you may find yourself asking, “How does a cesarean birth affect my child’s microbiomes?”
Vaginal
With vaginal births still being the most common way of delivery (68%), these children are seen to have overall better health throughout their lifetime than those born via cesarian (2). Vaginal birth is the most effective way to spread the microbiomes to the child’s skin, but studies have found that microbiomes do differ between ethnic groups. Microbiomes are made up of multiple bacterias and specifically, women with a higher pH have a smaller community of protective biomes. It has also been seen that the gut microbiota in pregnant women with gestational diabetes, tend to have an increased abundance of disease-associated microbes (2). That being said, the pH and mothers gut microbes play a significant role in the types of microbiomes that get transferred to their child.
Cesarean
There are generally two ways a child ends up being born via cesarean, labor ending in a cesarean, or a planned cesarean with no labor attempted. Children who are born via cesarean with labor attempted first, have a slightly higher number of microbiomes due to the vaginal fluids exposed to them during labor than that born elective cesarean. The most effective way a mother can transfer microbiomes to their newborn via cesarean is to “incubate” a cloth for 1 hour in their vaginal canal. When the infant is born,� the doctors rub the child’s mouth, eyes, and skin with the cloth that was previously incubated within minutes after birth (2). This process ensures that the child will have microbiomes more closely related to those born vaginally. Children born elective cesarean without using the incubation method, show fewer gut microbiomes related to their mother, but rather have more skin and oral microbes, and bacteria due to the operating room (2).
Children who are born via cesarean, whether labor was attempted first or not, are more likely to develop immune-related disorders such as asthma, allergies,� inflammatory bowel disease, and obesity (2). This is directly linked to not being “seeded” by the mother. Furthermore, adults who were born via cesarean contain a fecal microbiota that is drastically different than adults who were born vaginally (2).
The purpose of the female reproductive system is to reproduce and birth. Therefore, the best route will always be vaginal if it is safe for baby and mom. This being said, a cesarean is not a bad way to bring a child into the world. The child will just face more skin irritability and have a greater risk of developing health issues due to not receiving the same microbiomes as a child born vaginally. – Kenna Vaughn, Health Coach Insight
References:
(1) Aagaard, Kjersti, et al. �The Placenta Harbors a Unique Microbiome.� Science Translational Medicine, U.S. National Library of Medicine, 21 May 2014, www.ncbi.nlm.nih.gov/pmc/articles/PMC4929217.
(2) Dunn, Alexis B, et al. �The Maternal Infant Microbiome: Considerations for Labor and Birth.� MCN. The American Journal of Maternal Child Nursing, U.S. National Library of Medicine, 2017, www.ncbi.nlm.nih.gov/pmc/articles/PMC5648605/.
Neurological diseases are characterized as health issues associated with the brain, the spine, and the nerves which connect them. Neurological disease is considered to be one of the most prevalent health issues with a high burden to the patients, their families, and society. However, there are now estimates of the burden of neurological diseases in the United States. �
Neurological Disease Prevalence and Costs
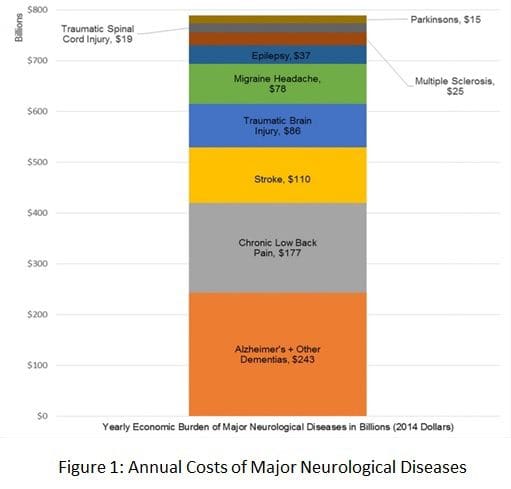
The most prevalent and costly neurological diseases, according to several recent research studies, include Alzheimer disease and other dementias, chronic low back pain, stroke, traumatic brain injury, migraine headaches, epilepsy, multiple sclerosis, spinal cord injury, and Parkinson’s disease. Many other neurological diseases were excluded due to their mixed etiologies. �
The most common neurological disorders described above cost the United States approximately $789 billion in 2014, which may increase as the elderly population increases between 2011 and 2050, according to a research study published in the Annals of Neurology. The research study demonstrates the price of the serious annual financial burden in the US and has been demonstrated as healthcare professionals have suggested budget reductions for federally-funded research studies. �
According to these demographic statistics, the American Neurological Association, or the ANA, commissioned a research study by former ANA marketing committee and public advocacy committee chair Clifton L. Gooch, MD, currently professor and chair of the Department of Neurology in the University of South Florida’s Morsani College of Medicine in Tampa. �
The research study, the Burden of Neurological Disease in the United States: A Summary Report and Call to Action, demonstrated the annual cost of the most prevalent neurological diseases, including Alzheimer’s disease and other dementias, chronic low back pain, stroke, traumatic brain injury, migraine headaches, epilepsy, multiple sclerosis, spinal cord injury, and Parkinson’s disease. Neurological disease ultimately affects an estimated 100 million people in the United States every year and, together with the costs of stroke and dementia alone, these are estimated to total over $600 billion by 2030. �
Funding for Neurology in the United States
The tremendous and sustained capital investments made in cardiovascular and cancer research studies beginning in the 1970s have considerably increased lifespan. Ironically, however, the number of older adults who have a higher chance of developing neurological diseases have increased, which has developed a growing outbreak among healthcare professionals. �
“Preliminary research studies, including those of cancer, focus considerable research study investment to the neurological diseases which are impacting the quality of life and mortality of more and more people in the United States every year,” stated Gooch, referring to the $1.8 billion in funding for cancer and neurology research approved by Congress in 2016. �
“We hope the findings of the report will serve as a wake-up call to Congress to improve much needed clinical and basic research funding necessary to discover treatments which can mitigate, and finally cure, the considerable amount of neurological diseases which have developed profound consequences in our patients as well as for the national economy.” �
“The future of funding for neurological research studies was an issue in 2012 when the ANA voted to support this particular research study,” stated ANA President Barbara G. Vickrey, MD, MPH. “With the reductions now being suggested to the NIH funding from the President of the United States, this has become of even greater concern today. As representatives of the scholars working to eradicate these health issues, we feel we must raise our collective perceptions, armed with the facts.” �
Annual Cost of Neurological Disease Overview
Researchers gathered the information from the research study through a complete review of the world literature among the most prevalent and costly neurological diseases in the United States. To be conservative, researchers focused on the prevalence and cost estimates they considered to be the most comprehensive and accurate, excluding neurological diseases, such as depression and chronic pain, which frequently have mixed etiologies beyond primary nervous system injury. �
“A complete accounting of all neurological diseases would considerably increase price tag estimates,” wrote the authors of the research study. Indirect and direct costs for the most common neurological diseases previously mentioned above, have been demonstrated in the research study and were estimated according to maintenance standards for each health issue. �
Alzheimer’s disease and other dementias accounted for $243 billion of their $789 billion total, while chronic lower back pain represented $177 billion, and stroke represented $110 billion.�As well as documenting the fiscal costs of neurological disease, Gooch and his USF colleagues ultimately recommend an action plan for reducing the burden of these health issues through infrastructure investment in neurological research and enhanced clinical management of neurological disorders. �
Many research studies have demonstrated how several of the most common neurological diseases pose a serious annual financial burden in the United States. The most prevalent and costly neurological health issues, such as Alzheimer’s disease and other dementias, chronic low back pain or sciatica, as well as stroke, among other common neurological diseases mentioned above, have been estimated to have an annual cost totalling $789 billion in 2014, according to research studies. These annual costs have also been demonstrated to considerable increase further over time.� – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article is to demonstrate the annual cost of several of the most prevalent neurological diseases. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Magnesium is an essential mineral, yet it tends to be overlooked as a health concern. To illustrate, a study shows that up to 75% of individuals are not intaking the recommended daily amount (2). This stems from the fact that most foods have steadily decreased the amount of magnesium they provide. Thus leaving many consumers with the need to supplement. Different magnesium supplements have been shown to facilitate the body in different ways.� Magnesium citrate can help to lower blood pressure whereas Magnesium L-Threonate can help with memory loss. So, which magnesium supplement should you be taking?��� �
Magnesium Citrate Overview
Magnesium Citrate is one of the most bioavailable forms of magnesium out there, meaning it’s ready and easily absorbed by the body’s digestive tract (5). In addition to this, Magnesium Citrate has been shown to improve arterial stiffness, lower blood pressure, and in turn, help to prevent cardiovascular disease in patients who are slightly obese (3). However, be aware that magnesium citrate is also used to treat constipation, therefore it can act as a laxative by helping to absorb water in the intestines (1). �
Magnesium L-Threonate Overview
Magnesium L-Threonate is a newer form of magnesium, therefore there are fewer studies showing its full capabilities. However, Magnesium L-Threonate is the only form of magnesium to cross the blood-brain barrier more readily. The blood-brain barrier is extremely selective in order to reduce the amount of toxins entered into the CNS (central nervous system). Due to this, it has been proven to increase synapse density and aid in memory loss, cognitive decline, as well as help to improve short term memory (4). In a long term study of 17 years performed with Magnesium L-Threonate, the results manifested that subjects were 37% less likely to get dementia (4). �
If you are looking for something to assist in relaxation, sleep, and memory; Magnesium L-Threonate is the supplement for you. Although, if you are looking for something to relieve occasional constipation and something to aid in blood pressure that mixes well with water and has little to no taste, magnesium citrate is the route you should consider. Getting started on the right magnesium supplement today could set you up with a better tomorrow. – Kenna Vaughn, Health Coach Insight
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
References
(1)Cisar�, Fabio, et al. �Bowel Preparation for Gastrointestinal Endoscopic Procedures With Sodium Picosulphate-Magnesium Citrate Is an Effective, Safe, and Well-Tolerated Option in Pediatric Patients: A Single-Center Experience.� Gastroenterology Nursing : the Official Journal of the Society of Gastroenterology Nurses and Associates, U.S. National Library of Medicine, 2018, www.ncbi.nlm.nih.gov/pubmed/30063687.
(2)Guerrera, Mary P, et al. �Therapeutic Uses of Magnesium.� American Family Physician, U.S. National Library of Medicine, 15 July 2009, www.ncbi.nlm.nih.gov/pubmed/19621856.
(3)Schutten, Jo�lle C, et al. �Effects of Magnesium Citrate, Magnesium Oxide and Magnesium Sulfate Supplementation on Arterial Stiffness in Healthy Overweight Individuals: a Study Protocol for a Randomized Controlled Trial.� Trials, BioMed Central, 28 May 2019, www.ncbi.nlm.nih.gov/pubmed/31138315.
(4)”Science Review: Magnesium L-Threonate.” Metagenics Institute. 01 Aug. 2019 .
(5)Walker, Ann F, et al. �Mg Citrate Found More Bioavailable than Other Mg Preparations in a Randomised, Double-Blind Study.� Magnesium Research, U.S. National Library of Medicine, Sept. 2003, www.ncbi.nlm.nih.gov/pubmed/14596323. �
Orthotics Treat Other Areas Than the Feet
�
�
Additional Topic Discussion: Xymogen� Supplements
The average adult in the United States takes one or more dietary supplements on a regular basis. Dietary supplements include vitamins, minerals, herbals and botanicals, amino acids, enzymes, and a variety of other products. Several of the most common dietary supplements include vitamin D and vitamin E, minerals such as calcium and iron, herbs such as echinacea and garlic, and products such as glucosamine, probiotics, and fish oils. For people who don’t have balanced nutrition, taking dietary supplements can help them get necessary amounts of essential nutrients and can help improve overall well-being.
Formulas for Methylation Support
�
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
� Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
� Please call our office in order for us to assign a doctor consultation for immediate access.
� If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download � * All of the above XYMOGEN policies remain strictly in force. �
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine