Spinal decompression surgery could be a treatment option discussion with a doctor to relieve nerve pain brought on by a spinal condition or disorder. Everything to know about the procedures straight from the experts.
Spinal Decompression Surgery Types: Laminectomy or Laminotomy
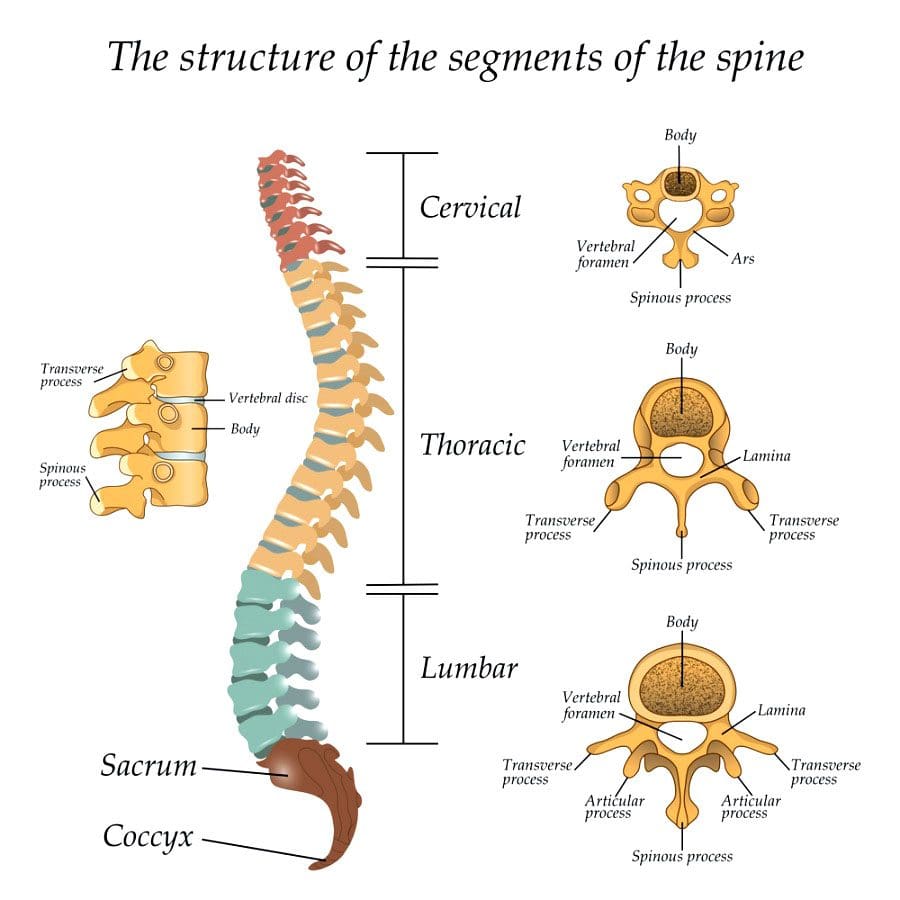
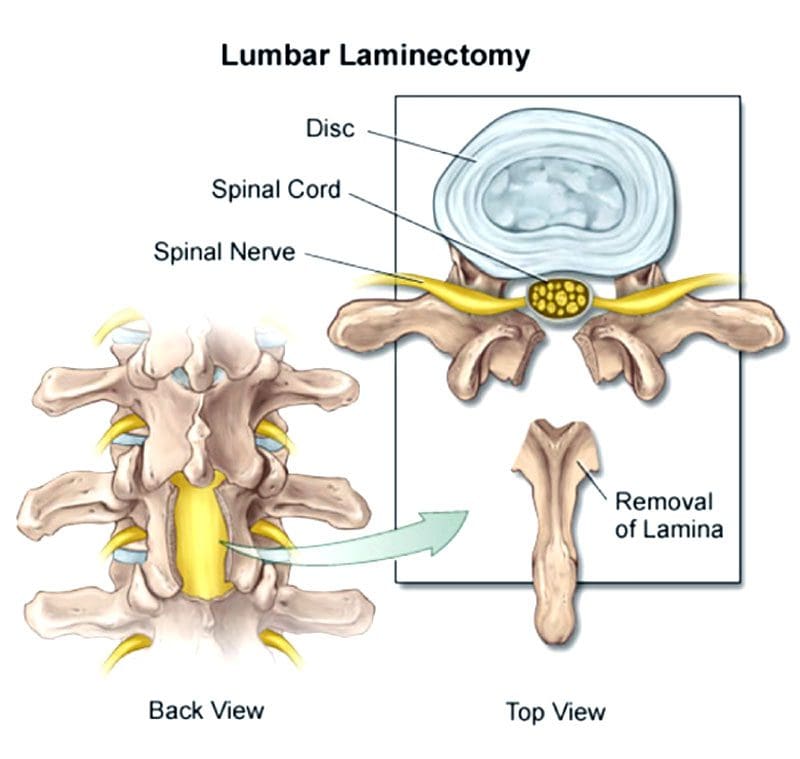
Both procedures involve the vertebrae�s lamina, which is an arch of bone that protects the spinal canal.
In a laminectomy, the lamina is removed almost entirely.
In a laminotomy, it is a partial removal.
Despite the removal, the large muscles of the back provide sustained protection for the nerves below. Therefore, the spinal nerves are still safe and secure following the procedures. Which one is right depends on the situation.
A laminectomy is usually performed to treat an arthritic condition of the spinal canal like spinal stenosis.
Laminotomy is used almost exclusively to remove a herniated disc.
A laminectomy removes more bone and sometimes the inner edge of the facet joint.
Ultimately, a surgeon will determine which of the two procedures is best for the individual’s needs and condition.
Decompression Surgery
Spinal stenosis or the narrowing of the spinal canal is usually caused by arthritis and overgrowth of the discs and joints. Similar compression issues respond well to non-surgical treatment. But sometimes surgery is necessary to treat uncommon but potentially severe cases. These include patients with:
Bowel or bladder problems caused by the pressure on the spinal nerves
Leg weakness that gets worse
Inability to walk or move for long periods and distance
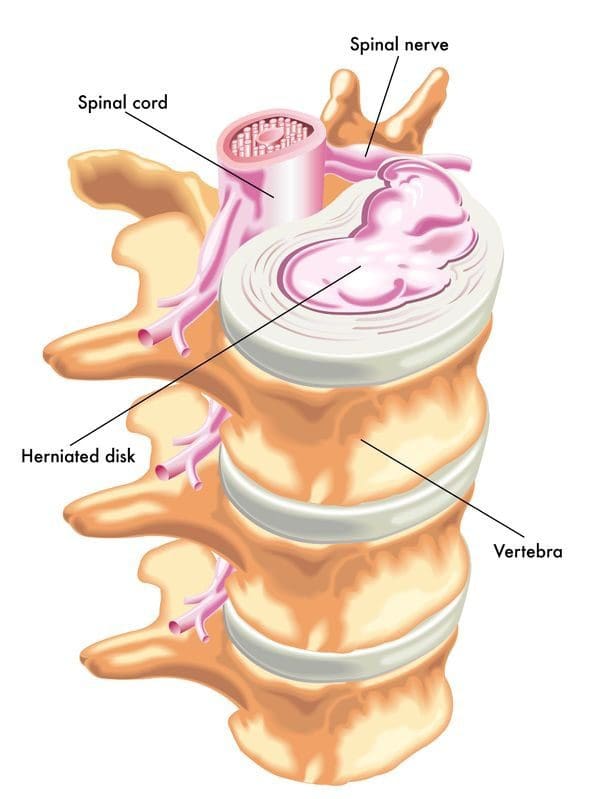
The objective of spinal decompression surgery is to create space around the spinal cord and surrounding nerves by removing the compressing structure/s. When the cord and/or nerve/s are compressed, physical and neurological symptoms are experienced down the nerve�s pathway. This includes:
Tingling
Numbness
Electric shock sensations
Radiating/spreading pain
Weakness
Once the compressed nerves have space to relax and move around symptoms subside.
Laminectomy process
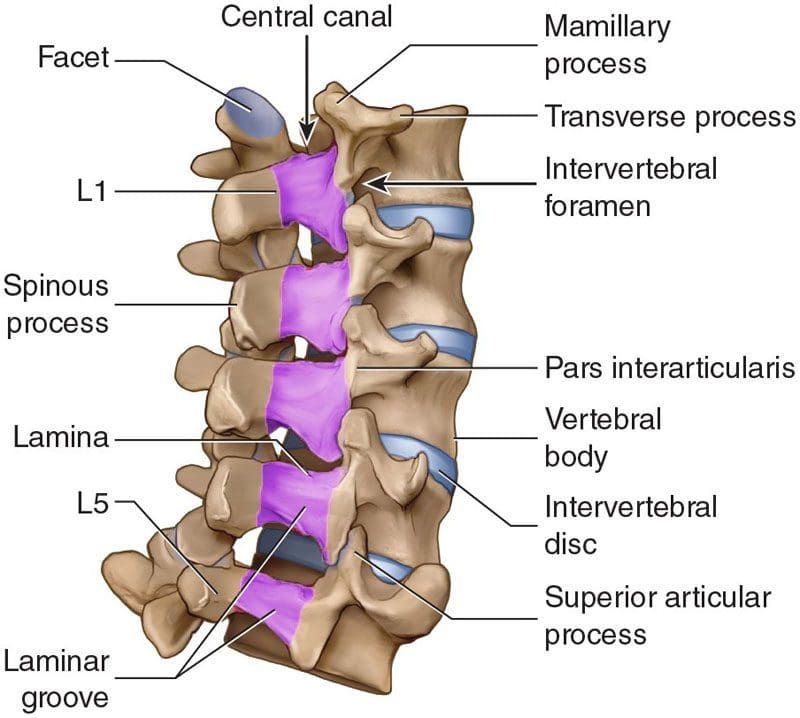
Lumbar laminectomy is the most common procedure to treat spinal stenosis in the low back.
It also helps treat herniated discs by allowing the surgeon to easily access the discs to repair any damage.
The surgeon removes the lamina and ligaments that have thickened and are causing problems to create more space in the canal.
The surgery enlarges the spinal canal so that pressure is relieved.
By removing the source of the pressure, the pain caused by the compressed nerves is alleviated.
An open laminectomy creates an incision of a couple of inches and exposes the spine.
The muscles of the spine and back are cut through to expose the bone.
Another technique that surgeons utilize is operating through a tube.
They’ve adapted these techniques to be able to decompress both the right and the left sides although they are only operating on one side.
Both procedures, minimal and traditional accomplish the same goals.
The difference is the minimally invasive approach involves one or more tiny incisions also known as skin punctures and small instruments designed to separate muscles and soft tissues instead of cutting through them.
The traditional approach requires a larger incision and instruments that retract, separate and cut tissues.
Laminectomy surgery
Laminectomies are performed under general anesthesia using a posterior approach/lying face down during the procedure.
It can be open or minimally invasive sometimes called a microlaminectomy.
In an open laminectomy, the surgeon makes an incision near the affected spinal area.
Once the incision is made, a retractor will move the skin, fat, and muscles to the side so the surgeon can access the spine.
Next, they remove or trim the lamina and thickened ligaments to enlarge the space surrounding the compressed nerves.
Once done, the retractor is removed and the incision is closed with sutures.
Minimally invasive surgery or MIS is performed using special instruments like endoscopes and tubular retractors.
These instruments allow for smaller incisions and less cutting.
They will also use special eyewear to have a detailed view of the surgical field.
Sometimes, the surgeon uses an endoscope or a microscope focused down the tube to perform the surgery.
The portion of the lamina is removed, along with any bone overgrowths/osteophytes and ligament tissue.
The tubular retractors are taken out so the soft tissue moves back into place, and the incision is closed with dissolving sutures.
Other spinal procedures performed alongside
Laminectomies and laminotomies are typically not performed together. However, a surgeon could perform both if the surgery affects multiple levels of the spine. They can also be combined with other spinal surgeries, that include:
Foraminotomy
A foraminotomy is also a decompression procedure. But instead of removing part or all the lamina, the surgeon accesses the nerves through the spine�s foramen or the passageway that nerves pass through on both sides.
Discectomy
This decompression surgery involves the removal of all or part of the damaged intervertebral disc and is utilized for herniated discs.
Spinal fusion
Fusion is often performed after spinal decompression surgery, as the space that was created by removing spinal structure/s can cause instability to the spine.
Candidates for spinal decompression surgery
Both are common procedures performed by neurosurgeons and orthopedic spine surgeons. Laminectomies are considered one of the most effective treatments for spinal stenosis and spinal canal issues like:
Tumors
Certain types of infections and abscesses
Spinal issues involving bowel/bladder dysfunction
The primary reason for laminectomy is spinal stenosis, most common in individuals over the age of 60.
Other considerations and conditions include:
Non-invasive treatments that don’t improve the condition that includes medication, massage, and physical therapy
Ask questions about the procedure to ensure you are comfortable with the operation. Here are some questions:
What are the risks associated?
Will the surgery relieve all symptoms?
Not having the surgery risks?
What is recovery like?
Recovery
Open or micro, recovery does take time. Following the doctor�s instructions carefully are essential to make a full, healthy recovery.
Individuals should be careful for about a month following the surgery. But does not mean laying down or being sedentary. Movement is crucial to recovery.
The patient should not stay in bed or lie on the sofa.
Wait a week or two before beginning physical therapy if necessary.
Most will have a weak core, poor posture, and poor body mechanics, the goal is to help develop and strengthen these areas.
Things to help with recovery include:
Ice/cold packs will help reduce swelling and pain.
Try not to sit for too long, as sitting is the least comfortable position after back surgery.
Body mechanic awareness means avoiding too much bending or lifting and using the right body mechanics when bending or lifting.
Especially before surgery. Quitting entirely or at least for at least six weeks before surgery will make recovery easier and healthier.
Losing weight
Speak with a doctor about weight. Just 5 pounds can make a significant difference during recovery.
Blood sugar
For individuals with diabetes, having an A1C under eight before surgery is ideal.
Every patient�s recovery is different. Recovery time depends on:
The complexity of the surgery
Personal medical history
Health issues
Recovery typically takes about two to four weeks after the surgery. However, it depends on the reason/s for the surgery.
Questions
Post-laminectomy syndrome
Post-laminectomy syndrome PLS also known as failed back surgery syndrome is a condition where an individual continues to have pain after surgery. Individuals still having symptoms after should speak with their doctor to determine the next phase of treatment.
How long before exercise?
Returning to the gym or getting into an exercise routine will take some time. It is important to follow the doctor�s recommendations and complete the full course of physical therapy before regular exercise activity can resume. Discuss workout plans with the doctor to determine the best timeline for the spine.
Full recovery?
Returning to some activity is possible around four weeks after surgery. Full recovery takes longer as each patient�s recovery is unique. Depending on the complexity of the surgery, most return to all activities within 6 to 9 months.
Body Composition Spotlight
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Whiplash is one of the most devastating cervical/neck spinal injuries. Rapid acceleration and deceleration can be so powerful that it bruises, tears the muscles, ligaments, soft tissue, and herniates the neck’s discs. Chiropractic relief can take care of initial and late-onset symptoms. As symptoms develop, they typically take the form of radiculopathy pain. Depending on the severity of the whiplash the types of symptoms that can occur include:
Swelling of the face
Neck pain
Shoulder and arms aching and pain
Hands can swell and ache
Loss of mobility
Numbness or complete loss of feeling
Symptoms can get worse indicating progressive nerve damage
If left untreated the individual can face long-term, chronic spine problems. Injury Medical Chiropractic Relief focuses on treating the whiplash, radiculopathy, and herniated discs at the source. After assessing the symptoms and the severity we can develop the most optimal treatment plan for the individual.
Radiculopathy
Radiculopathy is the result of a pinched nerve. This sends pain signals throughout the entire length of the nerve. With the neck’s nerve bundles, this means the pain travels as far as the face and hands. Tracing the extent of the radiculopathy informs the chiropractor as to which specific vertebrae have been affected. For example, if the nerve bundle in C7, which is the lowest neck vertebrae gets pinched, it can present in the arms. Another example, if chronic and persistent headaches or cheek pain are presenting, then C3-C4 will be the focus. The key is to look past the site of the pain and find its point of origin. Tracing referred pain quickly will allow the chiropractor to get a handle on the symptoms, even after the accident.
Herniated discs
A major factor in radiculopathy is a herniated disc. Displaced discs are how nerve compression and signal disruption begins. Until the disc/s are realigned, corrected, and reset, the affected nerves will continue to suffer.
The Connection
Make mention of any vehicle accidents throughout life. This can help the chiropractor immensely in diagnosis. A severe case of whiplash can occur even if the airbag does not deploy. The rocking motion of the cervical spine is strong, meaning whiplash can happen at collisions as slow as 5 miles per hour. Whether a minor car accident, a roller coaster ride, or sports, the condition frequently presents long after the accident.
Chiropractic Relief and Realignment
A chiropractor must put together the clues of a condition to hypothesize the cause. If experiencing pain symptomatic with recent neck trauma, it is essential to get checked. Injury Medical Chiropractic Clinic will address the condition before symptoms progress to a chronic condition.
Body Composition
The Function of Skeletal Muscle
Skeletal muscle is one of three major types of muscles in the body. The others are smooth and cardiac muscle. These muscles are attached to the bone by tendons. Skeletal muscles consist of nerves and blood vessels along with connective tissue to operate properly. These muscles consist of cells that come together and form bundles of skeletal muscle fibers.
Strength training stimulates the muscle fibers and combined with proper nutrition causes the muscles to grow. Muscles contract and shorten pulling on the bone and joints. This is what causes body movement. The nervous system sends signals to the nerves in the muscle and trigger contractions. Besides movement, skeletal muscle helps maintain posture, generate body heat, and stabilizes the bones and joints.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Rodriquez, Arthur A et al. �Whiplash: pathophysiology, diagnosis, treatment, and prognosis.��Muscle & nerve�vol. 29,6 (2004): 768-81. doi:10.1002/mus.20060
Back or disc pain is becoming increasingly common for individuals of all ages. The spinal discs are prone to injury because of the extreme amount of pressure/stress placed on the lower back and neck. Fortunately, most cases of back pain heal on their own, while others can cause long-term chronic pain that can be difficult to manage, without proper treatment.
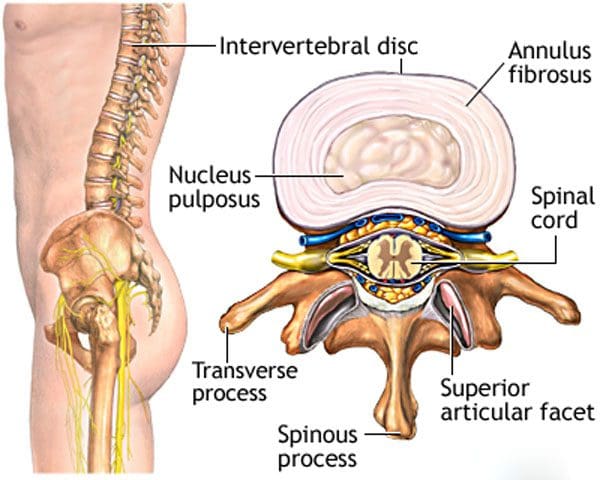
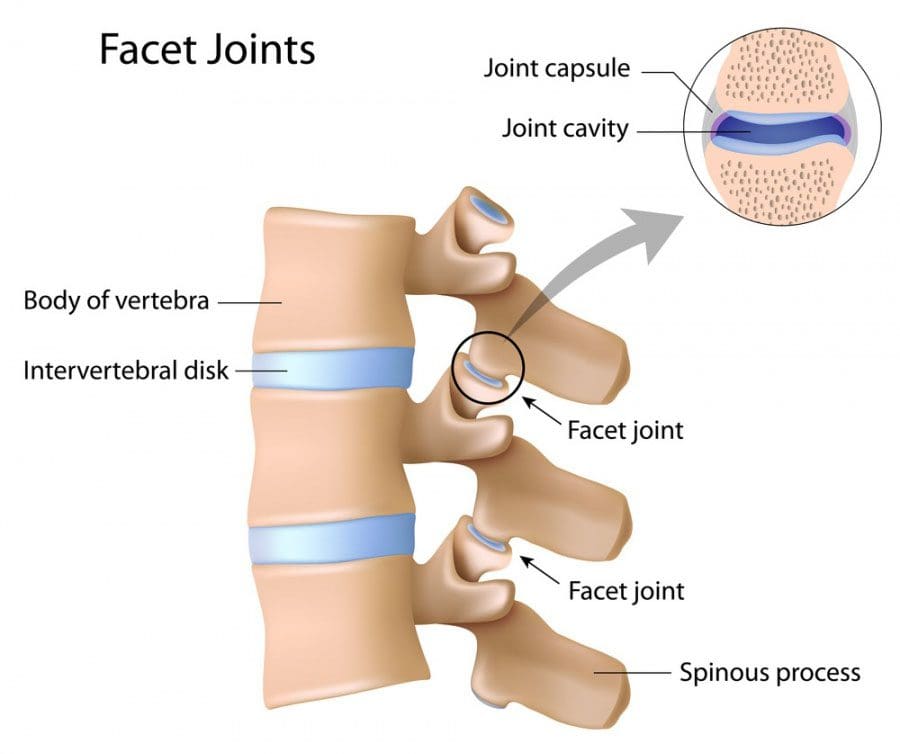
Different types of pain can be caused by problems with the spinal discs. The spinal discs are elastic sections of the spine that sit between the vertebrae. They are made up of materials called annulus fibrosus on the outside and a gel-like material called nucleus pulposus on the inside.
These discs are flexible, which allows for a range of motion to the spine and body shock absorption to increase comfort when in motion. When an individual visits a chiropractor, the practitioner will not know the exact cause of the pain, but only that it hurts around a certain area. Our spinal experts will help individuals understand the different types of ailments or conditions that could be affecting the spine. Then a customized treatment plan can be developed.
Disc problems
Spinal disc pain has two major sources of pain related to spinal discs: They are disc degeneration and nerve root pain. They are most common in the neck and the lower back. Individuals need to be informed of the difference to understand what is happening with the spine and potential treatment options to alleviate the pain and heal the problem.
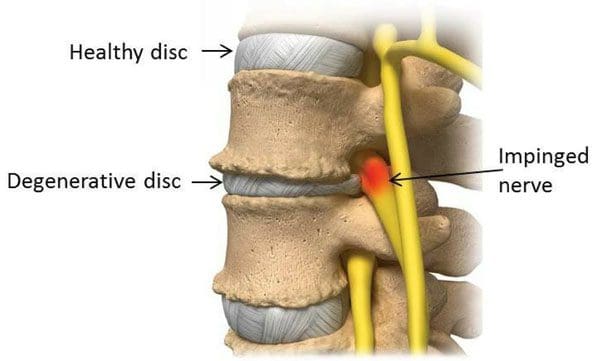
Degenerative disc disease
Degenerative disc disease is when the spinal discs begin to dry out and deteriorate. The discs start to shrink and can tear, which leaves that segment with little or no cushioning. This can cause pain, as well as inflammation of the surrounding muscles and joints. Disc degeneration usually presents with low levels of consistent pain and occasional severe flare-ups.
A chiropractor can utilize spinal manipulation to restore alignment, function, and mobility of the affected joint. Massages stretches and exercises will help alleviate the tension in the surrounding muscles along with strengthening them for better support.
Nerve root pain
Nerve root pain does not take place within the disc but is usually caused by a bulging or herniated disc. This condition can be called a slipped disc or pinched nerve, affect the nerves that are in close proximity to the neck and lower vertebrae.
The pain can lead to numbness, tingling, and weakness along the path of the nerve, and radiate out to the arms and legs. A bulging disc is when the spinal disc progressively protrudes through a narrow opening.
This can irritate any nearby nerve roots causing inflammation and pain. If the disc herniates or breaks through then the outer protective material tears, letting the cushion/gel leak out and come in contact with the nerve root/s, which could also cause pinching and inflammation. Treatment for a bulging or herniated disc includes:
Spinal manipulation
Corrective exercises
Physical therapy
Massage
Diet adjustments
These treatments can help realign the disc/s, moving them away from any nerves, and minimizing inflammation.
Proper Identification and Diagnosis
Spinal disc problems can be similar in their pain and symptoms. For example, degenerative disc disease can weaken the spinal discs to such a degree that nerve root pain follows creating a dual combination of pain. The conditions require various approaches and treatment methods often done in combination. However, they require a proper diagnosis to create a proper and custom treatment program for every individual. This will ensure the root cause of the disc pain is properly identified and handled. Call us to learn more.
Skateboarding Injury Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Browning, J E. �Chiropractic distractive decompression in the treatment of pelvic pain and organic dysfunction in patients with evidence of lower sacral nerve root compression.��Journal of manipulative and physiological therapeutics�vol. 11,5 (1988): 426-32.
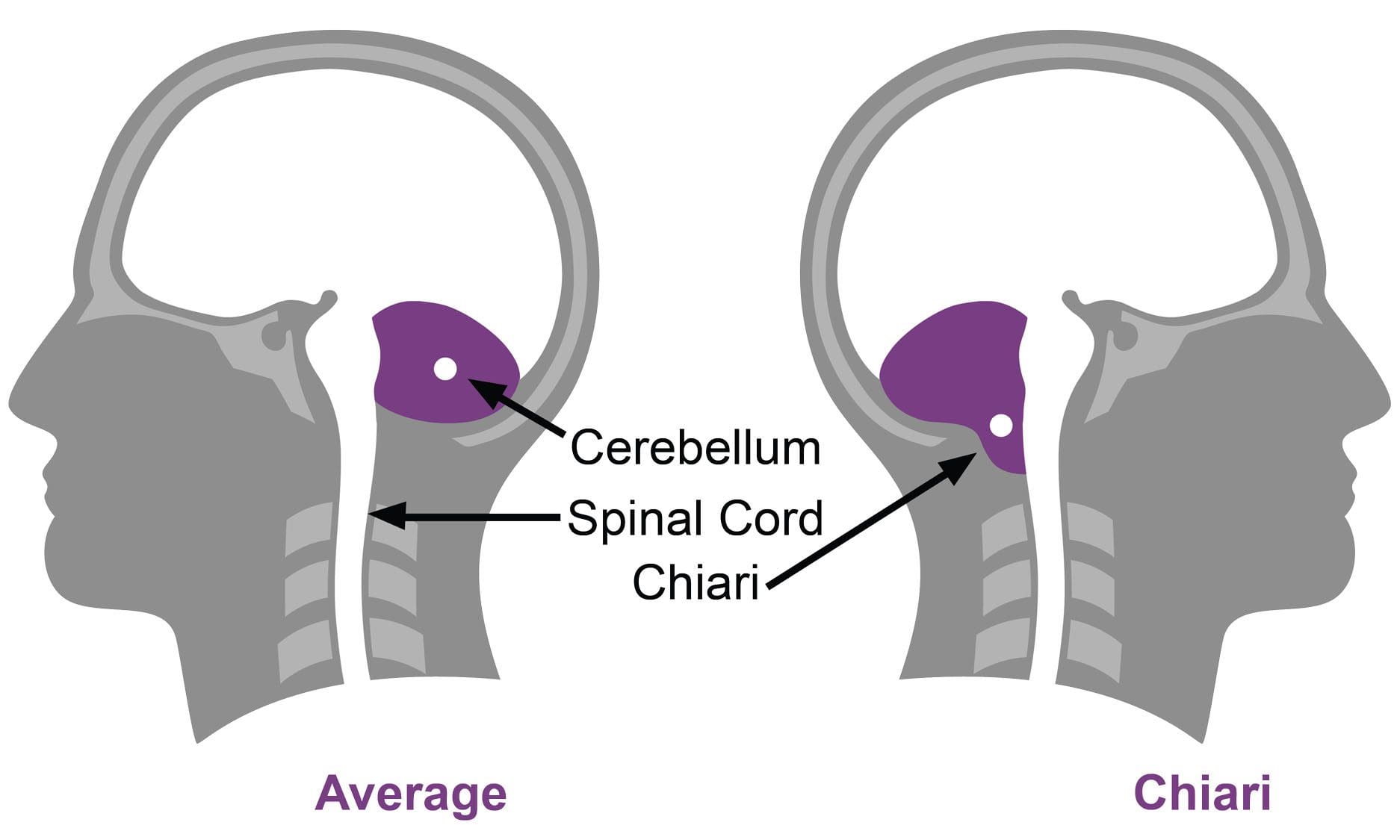
Chiari malformation is a condition that causes brain tissue to extend out and settle into the spinal canal. It protrudes out where the skull and neck meet. It occurs because part of the skull is too small or shaped in a unique way that allows part of the brain to settle into the foramen magnum. The foramen magnum is a large opening at the bottom of the skull. The brain’s nerves go through into the spinal canal and join the spinal cord. However, only the nerves should be present. The brain should not be able to push/press/leak through. When it does this is Chiari malformation.
Causes
Chiari malformation can be caused by structural problem/s with the:
Brain
Skull
Spinal canal
Structural conditions/issues can be present at birth, which are congenital defects. This is also called primary Chiari malformation and is not caused by any other condition. Secondary Chiari malformations are caused by something else, most often through surgery. This is extremely rare, but it is possible to develop after having surgery to remove a tumor in the skull or neck region. A surgeon could have removed too much bone while removing the tumor. This allowed the brain to settle into the open space.
Types
There are 4 types and are categorized by how much brain tissue protrudes into the spinal canal.
Type I
This is the adult version and is also the most common.
It is usually first noticed and discovered from an examination for something else. Most individuals don’t realize that they have Chiari malformation unless the symptoms are severe. With Type I a part of the brain, specifically the cerebellar tonsils settle into the foramen magnum.
Type II
Type II is also known as Arnold-Chiari malformation. This is the pediatric version. Symptoms are more severe with Type II because more brain tissue comes through. With this type, the cerebellar tonsils and some of the brainstem protrude. With Type II myelomeningocele, which is a form of spina bifida is a concern. What happens is the vertebrae and spinal canal do not close correctly before birth, so the spinal cord has no protection.
Type III
This type also affects children and is more severe than types 1 or 2. Here a significant portion of the brain, including the cerebellum and the brainstem protrude all the way through the foramen into the spinal canal.
The symptoms vary based on the type and severity. The most common symptom is a headache. Individuals with a Chiari malformation usually have headaches in the occipital region of the brain. This is the back of the head, right where the skull joins the cervical spine/neck. The headaches can be aggravated being in certain positions and actions, tilting the head back, and coughing. Typical symptoms include:
However, Chiari malformation can interrupt the flow of cerebrospinal fluid. Cerebrospinal fluid is necessary to protect the brain and spinal cord. If the normal flow is disrupted it becomes more difficult for the brain and spinal cord to send/receive nerve messages. The pressure built up can also cause nerve issues/problems. For some individuals, symptoms can come and go. This depends on how much cerebrospinal fluid has built up. Individuals with Type I sometimes don’t have any symptoms. It all depends on the severity.
Diagnosis
Diagnosis is done with a magnetic resonance imaging test or MRI. The MRI will show the various parts of the brain, skull, spinal cord, and spinal canal. They will be able to see abnormalities that could point to Chiari malformation.
Treatment
The recommended treatment depends on the severity. If pain is presenting a doctor could recommend pain medications to help manage the pain. Non-steroidal anti-inflammatory meds could also be recommended to reduce inflammation. Analgesics or pain killers can be recommended. Often both non-steroidal anti-inflammatories and analgesics are available in over-the-counter and prescription. The doctor will figure out the best medication treatment plan.
Surgery can be used to relieve symptoms and is the only way to relieve the pressure on the spinal cord and nerves. The goal is to stop the malformation from worsening. Surgeons use a posterior fossa decompression procedure. The surgeon removes part of the skull to make more room for the brain to sit in. This takes the pressure off the brain and spinal cord, and should reduce the neurological symptoms and problems. The surgeon may increase the size of the dura or the sac around the brain.
Laminectomies at C1 and C2, which are the first and second levels of the neck and are utilized to make more room for the brain. The surgeon will place a patch that is made from animal or synthetic tissue that will grow into the dura. The patch makes the dura bigger, which allows more room for the brain. Not all surgeries involve the dural patch.
Neck Pain Chiropractic Care
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
A bone graft is defined as using bone-in spine fusion surgery. Spinal fusion’s purpose is to link or weld bones together, in this case, the spinal bones. There are a variety of spinal conditions cause instability and pain:
Degenerative disc disease
Scoliosis
Trauma from an auto accident, sports injury, slip, and fall accident
Spine surgeons use a bone graft to:
Stop motion between two or more vertebrae
Stabilize a spinal deformity
Repair fractures of the spine
�
�
Spinal Fusion Stimulates New Bone Growth
A bone graft does not heal or fuse the spine instantly. Rather a bone graft sets up a foundational frame for the individual’s body to generate and grow new bone. A bone graft stimulates new bone production. It is when this new bone begins to grow and solidify, that fusion takes place.
With these types of surgeries, instrumentation like screws, and rods are typically used for the beginning stabilization. But it is the actual healing of the bone that welds the vertebrae together creating long-term stability.
A bone graft can be used for structural purposes for supporting the spine, usually this is done in place of a disc or bone that was removed. Or it can be an onlay, this means that a mass of bone fragments will grow together to stabilize the spine bridging the joint.
There are two generalized bone graft types:
Real bone
Substituted bone graft
Real bone can come from the patient, which is called an auto-graft or from a donor’s bone, called an allograft.
�
The Individual’s Bone or Auto-graft
An auto-graft is bone taken or harvested from the individual’s body and transplanted to a specific area, in this case, the spine. An auto-graft is considered the gold standard because it is the individual’s own bone, which contains:
These all help to stimulate the healing of the fusion. There are advantages for an auto-graft, which include a higher probability for fusion success and a lower risk for disease transmission. The only real setback for individuals of an auto-graft is the post-operative pain that usually comes with the procedure when harvesting an individuals’ bone. Bone can be harvested from one of the individual’s:
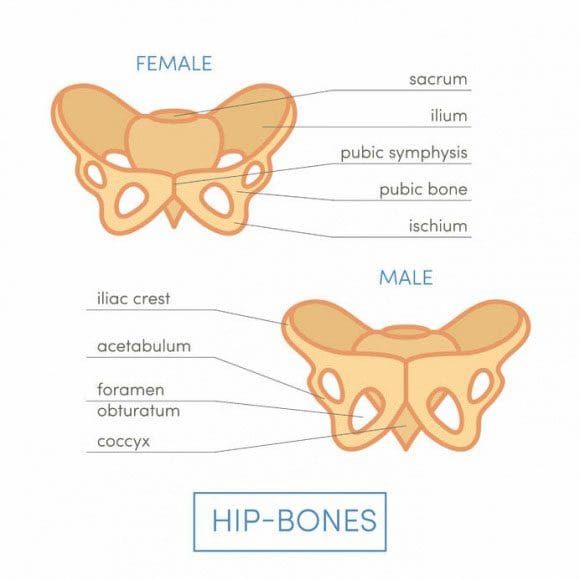
Iliac crests
Pelvic bones
Ribs
Spine
� Bone graft harvesting creates a new set of risks. These include:
Because of these risks and the possibility that the bone could be poor quality, a surgeon could decide to use another type of bone graft. When this happens a surgeon could go with what is known as a local auto-graft. This is bone harvested from the decompression itself.
These are the parts that are removed to decompress the nerves. They usually consist of bone spurs, lamina, and portions of the spinous process. These same bone pieces can be reused to assist with the fusion of the decompressed areas.
�
Donor Bone or Allograft
An allograft is a bone harvested from another person, usually from a tissue bank. Tissue banks harvest bone and other tissues from cadavers for medical purposes. An allograft is prepared by freezing or freeze-drying the bone or tissues. This helps limit the risk of graft rejection. Bone from an allograft does not have living bone cells and is not as effective at fusion stimulation when compared to an autograft. However, it still does work. Tissue banks:
Screen all their donors
Supervise bone recovery
Test donations
Sterilize donations
Store for use
Look for tissue banks that are accredited by the American Association of Tissue Banks. US Food and Drug Administration has strict regulations when it comes to human cell and tissue processing. These include rules about the eligibility of donors. These guidelines/protocols help reduce the risk of tissue contamination and the spread of disease.
�
Bone Graft Substitute
These substitutes are man-made or are made from a manipulated version of a natural product. These alternatives are safe and can provide a solid foundation for the individual’s body to grow bone. Substitutes have similar properties of human bone, which include a porous structure and proteins that stimulate healing.
�
Demineralized Bone Matrix – DBM
A demineralized bone matrix is an allograft that has gone through a process where the mineral content has been removed. This demineralization helps reveal bone-forming proteins like collagen, and growth factors hidden within the bone that can stimulate healing.
This procedure is often considered a bone graft extender. It is not considered a replacement. This is because its ability to fuse the human spine on its own has not been proven. DBM can be combined with the regular bone for more volume and is available in these forms:
Chip
Granule
Gel
Powder
Putty
�
Ceramic-based Extenders
Ceramic-based extenders are mixed in combination with other sources of bone. This is because they consist of calcium matrix for fusion, but there are no cells or proteins to stimulate the healing process. These include:
Ceramic-based extenders do not present a risk for disease transfer but can cause inflammation. They are available in porous and mesh forms.
�
Morphogenetic Protein – BMP
Different types of bone morphogenetic proteins or BMP’s are used to stimulate new bone growth. These proteins are found in human bone, however, they are trace amounts. They are then produced in larger amounts through genetic engineering.
This all depends on the type of spine surgery an individual undergoes. Bone morphogenetic protein could be considered an option in promoting new bone growth along with healing fusion.
Individuals can develop a herniated, slipped or bulging disc in the neck or back.�Too much stress on the disc/s whether from poor posture, being overweight, injury, aging, and an unhealthy lifestyle can increase the risk for disc problems. Herniation can be caused by a combination of factors or physical injury. Several common questions about disc problems are answered.
Can Discs Slip
A slipped disc can mean a ruptured or herniated disc. We use the term slipped disc, however, the discs do not slip. Each disc is sandwiched between two vertebrae that are supported by a system of ligaments that hold the spine together. A bulging or herniated disc is the proper term.
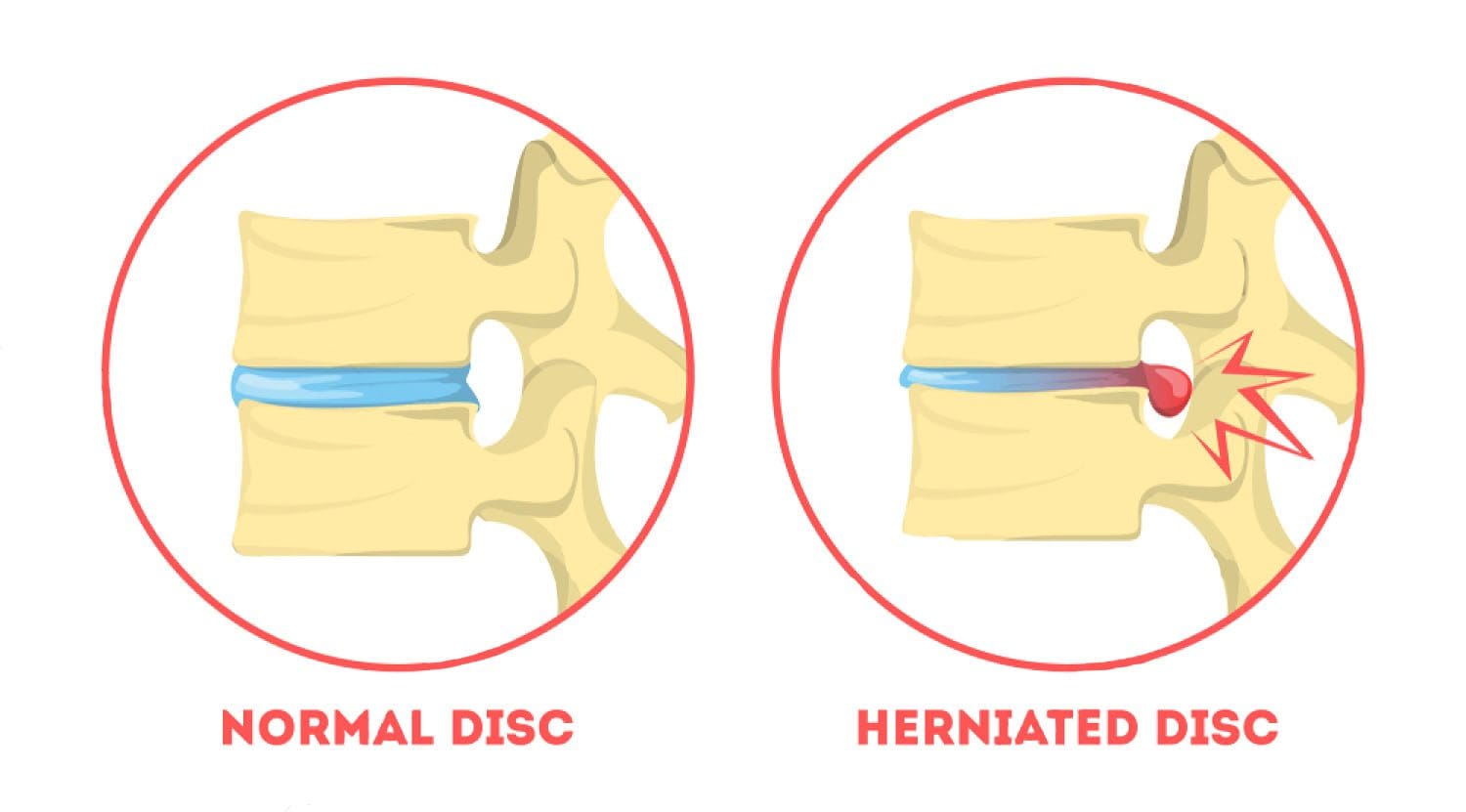
Difference Between a Bulging and Herniated Disc
Disc disorders are categorized as contained or non-contained. Bulging disc is an example of a contained disc disorder.
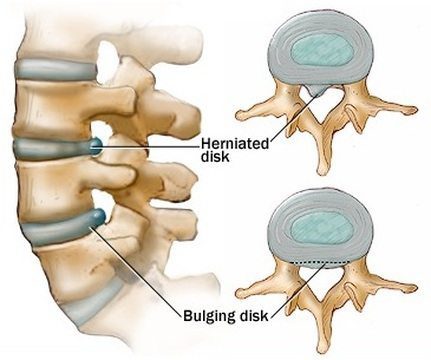
Bulging
A bulging disc has not broken open meaning the nucleus is still contained inside the annulus fibrosus. The disc could protrude into the spinal canal without breaking open. The gel, the jelly interior does not leak out. The disc stays intact except a small bubble pops out.
Herniated/Ruptured
A non-contained disc has either partially or completely broken open, and that is a herniated/ruptured disc. Imagine a closed tube�being squeezed placed under pressure, which causes the contents to move wherever they can. If a portion of the tube is weak or there is too much pressure, the contents could leak or burst out. When a disc herniates the gel-like contents could spread out to the spinal cord and nerves.
Herniation Can Cause Pain
The disc’s gel-like nucleus has a chemical that irritates the nerves and causes them to become inflamed and swell. The chemical stays and continues to press on the irritated nerves. Sometimes fragments from the disc wall or the tube break off from the disc and drift into the spinal canal causing other nerves to inflame and swell. Based on the type of injury and condition of the discs, more than one disc could herniate, rupture, or bulge. Sometimes injury causes a combination of disc disorders.
Symptoms
Symptoms of a herniated disc can include:
Dull
Shooting pain
Muscle spasms
Cramping
Weakness
Tingling
Referred or radiating/traveling pain
Sometimes, however, a herniated disc does not cause any symptoms at all. When this happens it is called an asymptomatic herniated disc. Disc/s could be bulging or herniated, but if it or they are not applying pressure on the spinal nerve/sor the cord, symptoms like pain may not present. This makes a point about herniated disc symptoms that they are dependent on where you have a herniated disc.
Cervical Herniation Symptoms
With a herniated or bulging disc in the neck, then you could experience:
Neck soreness/pain
Muscle tightness
Cramping in the neck
Pain that travels down the arm/s
Tingling in the arm/s or hand/s
Weakness in the arm/s or hand/s
Lumbar Herniation Symptoms
With a herniated disc in the low back the following symptoms could happen:
Low back pain
Muscle tightness
Cramping in and around the low back
Radiating pain that travels down the leg/s
Tingling in your leg/s or foot/feet
Weakness in the leg/s or foot/feet
Referred Pain
Referred pain means that you have pain in another part of the body from the disc problem. An individual could have a bulging or herniated slipped disc in the low back and have pain in the leg. This is lumbar radiculopathy or sciatica. Usually, just one leg is affected. If you have a herniated disc in the neck, there could be referred pain going down the arm and into the hand.
Chiropractic Cares
A chiropractor can help relieve back pain and other herniated disc symptoms. A chiropractor will go through your medical history, do a physical exam, and perform orthopedic and neurological tests. They are looking at several things. Orthopedic and neurological exams can help the chiropractor figure out what’s going on.
Are reflexes functioning properly?�Meaning are your nerves sending messages correctly. An example is a reflex test is when a doctor taps the knee with a hammer and the leg kicks.
Is there a loss of muscle strength?
Signs of muscle/s wasting away?
Is there a loss of sensation, tingling or numbness along the nerve/s path?
They will carefully look at posture, and will probably order an X-ray or MRI to help with the diagnosis.
Chiropractors evaluate the entire spine. Even if you only have lower back pain, your chiropractor will examine your neck, too. They want to see how well your spine is functioning overall. Remember what happens to one area of your spine can influence another part of the spine and/or body.
Pain from a herniated disc can make it difficult to enjoy daily life. Walking, sitting, and sleeping normally/comfortably can become a nightmare. You should make an appointment with a doctor or chiropractor if your herniated slipped disc symptoms last for more than two weeks.
Herniated Disc Treatment
NCBI Resources
In the United States alone, acute cases of lower back pain are the fifth most frequent reason for doctor visits and cause 40% of missed days off work. What�s more, it is the leading cause of disability worldwide.
Q: My primary healthcare provider recently diagnosed me with a herniated disc in the lumbar spine. They referred me to get chiropractic treatment, but I�m nervous because it’s new to me and I’m afraid of being adjusted wrong, paralyzed, etc. Can I trust chiropractic treatment to work?
A: It�s normal to be nervous about going to a chiropractic clinic.
If you’re not sure whether chiropractic is for you, there is scientific evidence that shows how chiropractic techniques like spinal manipulation/spinal adjustment and forms of manual/mechanical therapy are safe and effective for relieving pain and other musculoskeletal pain, conditions, and symptoms.
I encourage everyone to try chiropractic treatment as a non-surgical treatment option for a herniated disc.
It Is Your Decision
At the first appointment, a chiropractor will take a medical history and perform a thorough exam to determine the nature of the symptoms and their possible causes, which include a herniated disc.
Sometimes with a herniated disc, there may be no symptoms at all.
But usually a herniated disc causes:
Back pain
Referred pain or pain that is felt in other parts of the body like the legs, feet, etc.
An irritated spinal nerve can cause symptoms in the legs
This can lead to neurological symptoms like:
Tingling
Numbness
Weakness in the legs
Once the chiropractor determines your symptoms, they may use one or several techniques to relieve the back pain and other symptoms.
Techniques used by chiropractors for disc-related problems include:
Specific self-treatment exercises to improve motion & decrease back pain
Cox technique like spinal traction using special tables
Spinal manipulation
Hands-on techniques that relieve pain and restore movement to the spine and body
These techniques have been proven to be very safe. There are other techniques a chiropractor can recommend for various conditions, as each has their own style and method.
A chiropractic treatment plan will also include:
Education
Self-management instructions
This is to teach you how to control/eliminate pain with proper posture and proper body mechanics.
Whichever treatment the chiropractor recommends, he or she will discuss it with you, including the benefits and risks.
Although the treatments listed above will most likely be a part of your treatment plan, your chiropractor will answer your questions and work with you to select a treatment that meets your specific goals and preferences.
Don’t Be Nervous A Chiropractor Monitors Treatment Progress
If symptoms do not improve within a reasonable time frame, then a chiropractor may refer the patient to other treatments to manage disc-related pain, including:
Physical therapy
Acupuncture
Spinal injections
Surgery
Fortunately, self-management and time can be the best treatment. Allowing the body to heal itself is the way to go. But if rest is not enough then chiropractic treatment may be just what is needed to kick in the body’s self-healing function.
If you decide to give chiropractic treatment a try, don’t be nervous, as a chiropractor will monitor progress throughout the treatment.
In any case, chiropractors are qualified to discuss the benefits and risks of other treatments, depending on the condition.
Hopefully, this article has given you the basics of chiropractic medicine and how it works so you can make the best choice for your herniated disc/s.
Low Back Pain Management El Paso, TX Chiropractor
Denise suffered an auto accident injury which resulted in back pain. When she realized she could not sit, walk or sleep for lengthy periods of time without having painful symptoms, Denise found chiropractic care with Dr. Alex Jimenez at El Paso, TX. Once she received therapy for her automobile accident injuries, Denise experienced relief from her symptoms and she was able to execute her regular tasks once again. Thanks to the education and maintenance Dr. Alex Jimenez supplied, Denise regained her initial health and health.
Back pain is more most common, with roughly nine out of ten adults undergoing it at some time in their lifetime, and five functioning adults developing it annually. Some quote around 95 percent of Americans will experience back pain at some time in their lifetime. It is undoubtedly the typical cause of chronic pain since it’s also a substantial contributor to missed work and handicap. In the United States alone, acute cases of lower back pain are the fifth most frequent reason for doctor visits and cause 40% of missed days off work. What’s more, it is the leading cause of disability worldwide.
NCBI Resources
A herniated disc is a common spinal condition that typically affects the cervical spine (neck region) or the lumbar spine (lower back), although it can occur in any part of the spine. Most often, a herniated disc happens at the L4 � L5 and the L5 � S1.� This is because this portion of the spine, the lumbar region, bears the bulk of the body�s weight.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine