The body is home to the spine, where it is allowed to move, twist, bend, and run around without being in pain. When a person suffers from a back injury or pulled a muscle, the pain can range from a dull ache to a sudden sharp pain that hinders and affects their quality of life. Luckily many treatments can help manage back pain and possibly reverse the effects. One of the treatments is spinal decompression, and it can help alleviate back pain issues like bulging discs. In this article, we will be looking at what is bulging disc is, its symptoms, and its factors, as well as how spinal decompression can help alleviate bulging disc. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is A Bulging Disc?
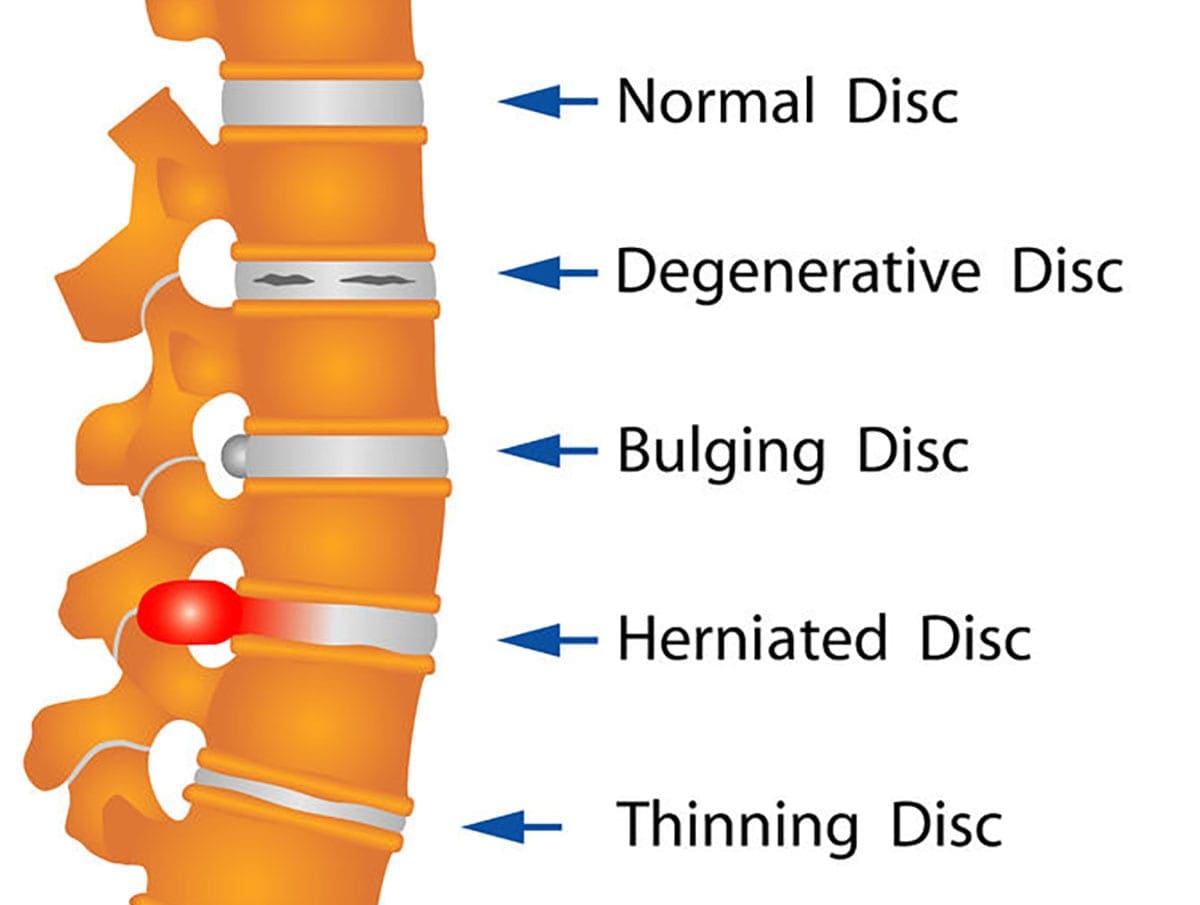
The spinal discs in the spine are flat circular cushions between the spine’s vertebrae and help protect the spine from any injuries. As the body ages naturally, the spinal discs will begin to lose their function through wear and tear. Research studies have shown that when the spinal discs begin to wear and tear with age, it can cause the disc to be dehydrated and cause the cartilage to be stiff. When this happens, the outer layer of the spinal disc will begin to protrude out and will not touch the nerve. If the protruding bulge continues to get worse and starts to crack the outer wall, the inner wall of the spinal disc will begin to come out and touch the spinal nerve root causing pain to the individual. This is known as a herniated disc.
Other research studies have found that when the spine has bulging discs, it is one of the causes of low back pain as about 80% of many individuals suffer from some back pain. Low back pain has many different diagnoses when this happens to the back, and DDD (degenerative disc disease) and disc herniation/bulging are the most common symptoms. These two common symptoms usually go hand in hand and, if not treated, will begin to cause a hindrance to the individual, leaving them with low back pain.
The Symptoms & Factors
The symptoms and factors of disc herniation/bulging vary depending on how severe the pain is. The pain from disc herniation can range from a dull, mild ache on the lower back to a sharp, sudden pain that travels from the lower back down to the leg. Research studies have shown that the primary symptoms of lumbar disc herniation are radicular pain, sensory abnormalities, and weakness in the lumbosacral nerve root. This will increase the pressure on the spinal disc causing the individual to be in pain while sitting. Other research studies have found that other common symptoms and factors that are caused by disc herniation/bulging include:
Excess weight: Can be compressed onto the spinal disc, causing disc herniation
Aging: Can naturally cause wear and tear on the spinal disc
Spinal Decompression Therapy Affecting Bulging Discs- Video
The video above shows how spinal decompression therapy can help alleviate bulging discs by using traction to stretch the spine gently. Spinal decompression is when individuals are lying down on the traction table and are strapped in as their spine is being pulled gently, causing the spinal disc to receive the beneficial nutrients back into the spine and allowing any herniation or bulging disc to go back to normal on the spine. Research studies have shown that utilizing physical therapy and spinal decompression therapy can help many individuals suffering from low back pain, herniated disc, or leg pain. By incorporating spinal decompression therapy into their wellness journey, many individuals will begin to feel relief and be pain-free. If you want to learn more about spinal decompression therapy, this link will explain the benefits of spinal decompression and how it can alleviate low back pain symptoms.
The Effects Of Spinal Decompression On Bulging Disc
Research studies have found that a lumbar herniation/bulging disc on the spine can induce neurological signs that can hinder a person with muscle weakness. One of the many treatments that can help alleviate bulging discs is spinal decompression therapy. Spinal decompression therapy and physical therapy can help stabilize the spine and can help improve muscle strength while providing a gentle stretch on the spine to allow the bulging discs to retreat to the spine, causing instant relief. Other research studies have shown that incorporating the two treatments are effective for many individuals by improving their pain and disability. This will allow their spine to be pain-free and restore their original function in the body.
Conclusion
The spine’s primary function is to make sure that the body is moving around without feeling any pain. As the body naturally ages over time, so does the spine as the spinal disc start to wear and tear, causing them to bulge out of the spine. If they start to press against the spinal nerve root, it can lead to herniation and cause shooting pain down from the lower parts of the body. Luckily some treatments allow the individual to feel relief, which is spinal decompression. Spinal decompression helps the spine by gently stretching it with a traction table, causing the nutrients and fluids to enter the spine and cause instant relief. When spinal decompression is combined with physical therapy, many individuals will notice that they are feeling no pain in their back and can continue their wellness journey.
References
Al Qaraghli, Mustafa I, and Orlando De Jesus. “Lumbar Disc Herniation.” StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 30 Aug. 2021, https://www.ncbi.nlm.nih.gov/books/NBK560878/.
Amin, Raj M, et al. “Lumbar Disc Herniation.” Current Reviews in Musculoskeletal Medicine, Springer US, Dec. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5685963/.
Choi, Jioun, et al. “Influences of Spinal Decompression Therapy and General Traction Therapy on the Pain, Disability, and Straight Leg Raising of Patients with Intervertebral Disc Herniation.” Journal of Physical Therapy Science, U.S. National Library of Medicine, Feb. 2015, https://pubmed.ncbi.nlm.nih.gov/25729196/.
Medical Professionals, Cleveland Clinic. “Herniated Disk: What It Is, Diagnosis, Treatment & Outlook.” Cleveland Clinic, 1 July 2021, https://my.clevelandclinic.org/health/diseases/12768-herniated-disk.
Shelerud, Randy A. “Bulging Disk vs. Herniated Disk: What’s the Difference?” Mayo Clinic, Mayo Foundation for Medical Education and Research, 23 Apr. 2019, https://www.mayoclinic.org/diseases-conditions/herniated-disk/expert-answers/bulging-disk/faq-20058428.
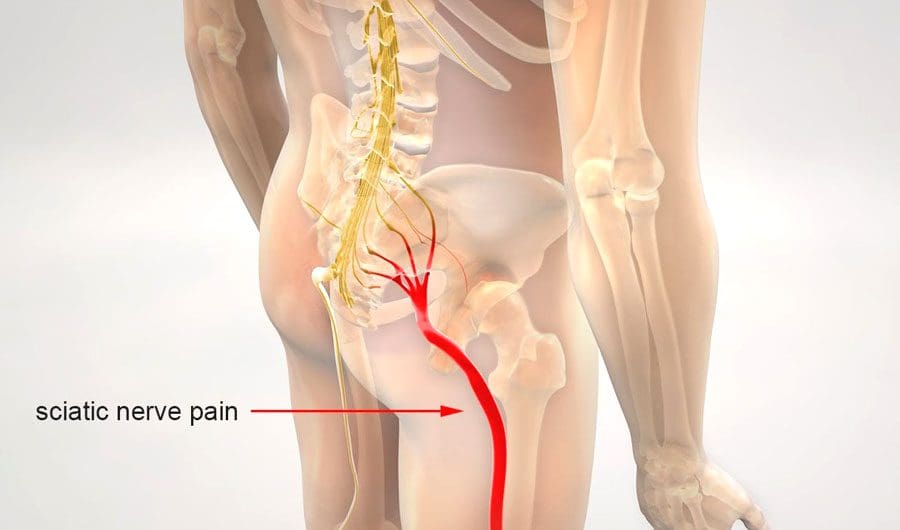
Sciatica is experienced as lower back pain and pain that radiates down the back of the legs. It is pain caused by compression, irritation, or inflammation of the sciatic nerve. It is generally experienced on one side of the body. Body movements like twisting, bending, sitting, or responses like coughing and sneezing can worsen the pain. Individuals with sciatica also experience muscle weakness, numbness, tingling, or electrical shock-like sensations. Injury Medical Chiropractic and Functional Medicine Clinic offer manual and motorized sciatic nerve decompression to stretch/realign the spine, release the compressed nerves, and relieve pain.
Sciatic Nerve Decompression
The spine consists of 23 spinal discs that are shock absorbers for the body during movement. Each disc consists of a soft inner core of a gel substance and a thick outer layer. Wear and tear of the spinal discs from aging, degenerative disc disease, repetitive physical activities like lifting and bending, obesity, and poor posture are some of the factors that can stress the spine, causing the thick outer layer of the spinal disc to crack/breakdown causing the soft inner core to leak out forming a bulging or herniated disc. This type of injury compresses, pinches, or irritates one or more nerve roots that form the sciatic nerve, triggering sciatica.
Spinal stenosis or the narrowing of the spinal canal.
Spondylolisthesis, or the slipping or dislocation of the spinal vertebrae in the lower part of the spine.
Are also known sciatica causes.
Symptoms
Common compressed nerve symptoms include:
Pain or burning sensations radiating down the leg.
Because branches of the sciatic nerve extend from the lumbar spine through the buttocks and down the leg, pain, burning sensations or dull aching can present along the nerve’s pathway if the nerve gets compressed or irritated.
Weakness in the affected leg.
When walking or moving the legs, the nerves transmit information to the brain, stimulating the muscles to react in specific ways.
A pinched sciatic nerve can cause interference with relaying signals, resulting in weakness.
Numbness.
The compression impedes blood circulation and nerve energy transmission.
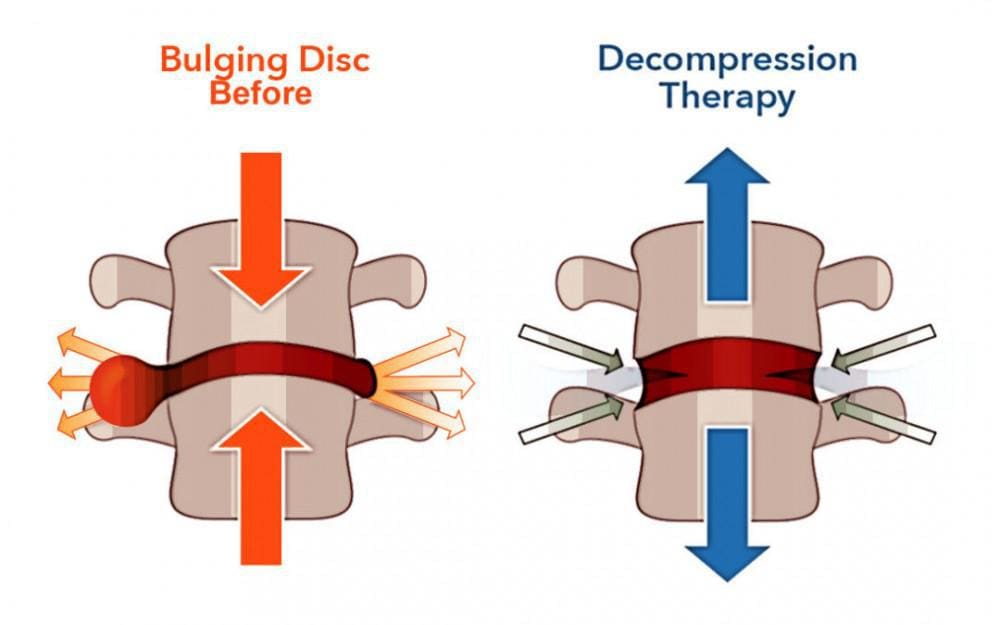
Spinal decompression therapy relieves pressure on the spine by pulling/stretching it in small increments. Non-surgical spinal decompression creates negative pressure within the discs. The negative pressure pulls or vacuums back the disc material that has protruded or herniated and an abundance of nutrients to activate the healing response. The chiropractor, physical therapist, or nurse uses motorized medical equipment with sensors linked to a computer-aided system to perform the procedure. The equipment is designed to adjust the pull force accordingly to prevent muscle resistance. The adjustable table also allows the spine to be stretched at different angles to target the upper or lower back.
The objective of spinal decompression treatment is to relieve the symptoms of sciatica or disc disorders and heal the injured disc. We utilize spinal decompression as an effective tool in treating a vast array of spinal conditions.
DRX9000 Non-Surgical Spinal Decompression
References
Berry, James A et al. “A Review of Lumbar Radiculopathy, Diagnosis, and Treatment.” Cureus vol. 11,10 e5934. 17 Oct. 2019, doi:10.7759/cureus.5934
Davis D, Maini K, Vasudevan A. Sciatica. [Updated 2022 Feb 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507908/
Giuffre BA, Jeanmonod R. Anatomy, Sciatic Nerve. [Updated 2021 Jul 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482431/
National Institutes of Health. (2019.) “Sciatica.” https://medlineplus.gov/sciatica.html
Motorized non-surgical decompression helps relieve pain, removes pressure on the nerves, promotes healing, and increases blood flow to the spine. Spinal discs cannot attain nutrients from the blood without circulation. Decompression opens the spine, flooding the discs with nutrients that result in quicker and optimal healing. This, combined with manual chiropractic adjustments and therapeutic massage, can help get an individual to a pain-free lifestyle.
Spinal Discs
The soft disc material that separates each spinal bone can lose hydration, causing the material to dry out and compress. The discs can also compress from pressure from added weight, trauma from an automobile accident, work, school, and sports injury. Often the soft gel center of the discs spills out, causing a disc herniation. This is usually accompanied by:
Numbness
Tingling
Soreness
Stiffness
Sharp pain
Dull pain
Achiness
Muscle Weakness
Stinging/Burning sensation
Leg pain
Poor balance
These are often indicators of a nerve or nerve bundle, including the sciatic nerve becoming compressed by a herniated disc, bulging disc or slipped disc, stenosis, facet syndrome, or degenerative disc disease. When this happens, the symptoms may be felt in the back or neck area, and/or they may spread out into the arms, hands, legs, or feet.
We focus on providing expert chiropractic treatment that incorporates the most current research and technology into personalized treatment plans. Our goal is to help the individual heal as quickly as possible while educating and training them to use tools to maintain health and wellness.
What Is Spinal Decompression?
References
Andersson, G B, and R A Deyo. “History and physical examination in patients with herniated lumbar discs.” Spine vol. 21,24 Suppl (1996): 10S-18S. doi:10.1097/00007632-199612151-00003
Apfel, Christian C et al. “Restoration of disk height through non-surgical spinal decompression is associated with decreased discogenic low back pain: a retrospective cohort study.” BMC musculoskeletal disorders vol. 11 155. 8 Jul. 2010, doi:10.1186/1471-2474-11-155
Cherkin, DC, and F A MacCornack. “Patient evaluations of low back pain care from family physicians and chiropractors.” The Western journal of medicine vol. 150,3 (1989): 351-5.
Koçak, Fatmanur Aybala et al. “Comparison of the short-term effects of the conventional motorized traction with non-surgical spinal decompression performed with a DRX9000 device on pain, functionality, depression, and quality of life in patients with low back pain associated with lumbar disc herniation: A single-blind randomized controlled trial.” Turkish Journal of physical medicine and rehabilitation vol. 64,1 17-27. 16 Feb. 2017, doi:10.5606/tftrd.2017.154
Urban, Jill PG, and Sally Roberts. “Degeneration of the intervertebral disc.” Arthritis research & therapy vol. 5,3 (2003): 120-30. doi:10.1186/ar629
The body can move, twist, turn and bend due to the spine making sure that the body is upright and functioning without pain. When a person is injured or pulls a muscle that causes pain to the back, it can hinder them from doing their daily activities. The pain can range from a dull, mild ache to a sudden sharp pain affecting a person. Luckily there are ways to treat back pain that can help improve the quality of life of a person while also reducing the pain symptoms. In this article, we will be looking at intradiscal pressure and how disc degeneration can affect it and seeing the effects of vertebral decompression relieving disc degeneration on the spine. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is Intradiscal Pressure?
In the body, the spine is protected by ligaments, the spinal cord, soft tissues, and spinal discs from injuries. When a person stretches and hears the spinal joints pop, the spinal fluid starts to allow the beneficial nutrients to nourish the spine and keep it healthy. This is known as intradiscal pressure, and research studies show that intradiscal pressure is influenced by the fluid flow of the spine, causing intradiscal pressure to be necessary for disc height and axial compliance for the spine for it to be healthy. Other research studies have shown the effects of respiration on intradiscal pressure in a healthy prone individual. However, if the spine has been influenced by disc degeneration, the intradiscal pressure is reduced and can cause spinal issues to develop over time. The spinal load must be healthy for intradiscal pressure because it requires respiratory movement when the body is in motion and in a sitting or standing position.
How Does Disc Degeneration Affect Intradiscal Pressure?
Back pain remains the second most common symptom for many individuals to visit their primary physicians. The spine is protected by soft tissues and spinal discs that allow the body to stay upright and do stuff in its range of motion. When the back gets injured, it can cause a person to be in pain and hinder them, depending on how severe the injury is. Some of the pain sources can include DDD or degenerative disc disease.
Research studies have shown that DDD (degenerative disc disease) can occur when the spine has been injured due to heavy lifting, vibrations, immobilization, and trauma. When these factors start to cause stress to the spinal discs, it can cause the intradiscal pressure to increase and cause low back pain to affect the body, as research shows.
Axial Decompression Therapy-Video
The video above shows how axial decompression therapy is used for individuals suffering from low back pain, herniated disc, or DDD (degenerative disc disease). Research studies have shown that when the body begins to age normally, the spinal disc will wear down and cause the bones to rub together. Utilizing decompression therapy as part of their wellness treatment can help alleviate the painful symptoms that the person was feeling. Decompression therapy uses traction to gently stretch the spine, allowing the beneficial nutrients and oxygen to go back into the spinal disc. This will enable individuals to feel instant relief and get them back on their wellness journey pain-free. If you want to learn more about spinal decompression therapy, this link will explain the benefits of spinal decompression and how it can alleviate low back pain symptoms.
The Effects Of Vertebral Decompression For Disc Degeneration
Many treatments can help the effects of disc degeneration, from elevating to chronic issues on the spine. One of those treatments is vertebral decompression. Research studies have found that when individuals utilize a 6-week treatment on the decompression machine will begin to notice a reduction in pain while an increase in the disc height on the spine. The gentle traction will stretch the spine slowly, alleviate the chronic back symptoms, and repair the spinal discs by allowing nutrients to go in. Other research studies have shown that decompression therapy creates negative pressure on the spine, allowing the intervertebral disc to increase hydration. This negative pressure alleviates the stress of the nerve root that the disc is applying to and causes the person to be in pain. When combined with physical therapy, the individual will begin to feel much better.
Conclusion
The spine is protected by ligaments, soft tissue, the spinal cord, and spinal discs while keeping the body to stay upright while it is in motion. When there is an injury or a pulled muscle that causes the person to be in pain, it can affect the spine and the back. This will cause chronic issues to develop, causing the individual to be in constant pain and making them miserable. Luckily, there are treatments to treat back pain and alleviate the spine, and decompression therapy can help lower the symptoms. Decompression therapy allows the individual to be strapped to a traction table and gets their spine gently pulled to cause instant relief. This will allow the spine to decompress and the nutrients to rehydrate the spinal discs, providing the individual to become pain-free.
References
Apfel, Christian C, et al. “Restoration of Disk Height through Non-Surgical Spinal Decompression Is Associated with Decreased Discogenic Low Back Pain: A Retrospective Cohort Study.” BMC Musculoskeletal Disorders, BioMed Central, 8 July 2010, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2912793/.
Choi, Jioun, et al. “Influences of Spinal Decompression Therapy and General Traction Therapy on the Pain, Disability, and Straight Leg Raising of Patients with Intervertebral Disc Herniation.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Feb. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4339166/.
Li, Jai-Qi, et al. “Comparison of in Vivo Intradiscal Pressure between Sitting and Standing in Human Lumbar Spine: A Systematic Review and Meta-Analysis.” Life (Basel, Switzerland), U.S. National Library of Medicine, 20 Mar. 2022, https://pubmed.ncbi.nlm.nih.gov/35330208/.
Medical Professionals, Cleveland Clinic. “Degenerative Disk Disease: Causes, Symptoms & Treatment.” Cleveland Clinic, 27 May 2021, https://my.clevelandclinic.org/health/diseases/16912-degenerative-disk-disease.
Palepu, V, et al. “Biomechanics of Disc Degeneration.” Advances in Orthopedics, Hindawi Publishing Corporation, 17 June 2012, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3382964/.
Sato, K, et al. “In Vivo Intradiscal Pressure Measurement in Healthy Individuals and in Patients with Ongoing Back Problems.” Spine, U.S. National Library of Medicine, 1 Dec. 1999, https://pubmed.ncbi.nlm.nih.gov/10626309/.
Vergroesen, Pieter-Paul A, et al. “Intradiscal Pressure Depends on Recent Loading and Correlates with Disc Height and Compressive Stiffness.” European Spine Journal : Official Publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, U.S. National Library of Medicine, Nov. 2014, https://pubmed.ncbi.nlm.nih.gov/25031105/.
The spine holds the body together by ensuring that it is kept upright and not in pain when it is in motion. The musculoskeletal system is connected to the spine as the spine makes sure that the body’s center is supported when a person moves, walks, twists, and turns when doing daily activities. When the back gets injured, or the spinal cord gets compressed, it can cause back and spinal pain issues that can hinder a person causing them to be in immense pain and affect their daily lives. Even neck pain can be a nuisance as the cervical discs get compressed and the muscles get stiff. Luckily, many treatments can alleviate back pain and help with neck pain through non-surgical methods. In this article, we will be looking at axial pain and how it affects the neck, and how cervical axial decompression can alleviate neck pain. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is Axial Pain?
The spine is an S-shaped curve protected by ligaments, soft tissues, the spinal cord, and spinal discs from injuries. When the spine gets injured, many back issues start to affect the spine as the spinal discs get compressed, herniated, or even touch the nerve root like the sciatic nerve, causing sharp shooting pain down the leg. However, it is known as axial pain when a person starts to have mixed pain symptoms that begin to affect a person’s quality of life. Research studies have shown that axial pain is considered a syndrome with both nociceptive and neuropathic pain while also being a high socioeconomic impact on people. When individuals have neuropathic pain, it can be due to the result of injured nerves that will contribute to back pain and neck pain.
Neck Pain
As one of the most common musculoskeletal disorders that affect many individuals, research studies have shown that neck pain is a multifactorial disease that causes individuals to be in pain. Some of the risk factors that can cause neck pain can be from:
Other research studies have shown that since the neck is flexible and supports the head’s weight, it is vulnerable to many injuries and conditions that will cause pain and restricted movements like muscle strains, worn-out joints, nerve compression, and whiplash injuries. There are also two types of neck pains that can affect the cervical spine: axial pain, where the pain is felt in the neck mostly, and radical pain, where the pain affects the shoulders.
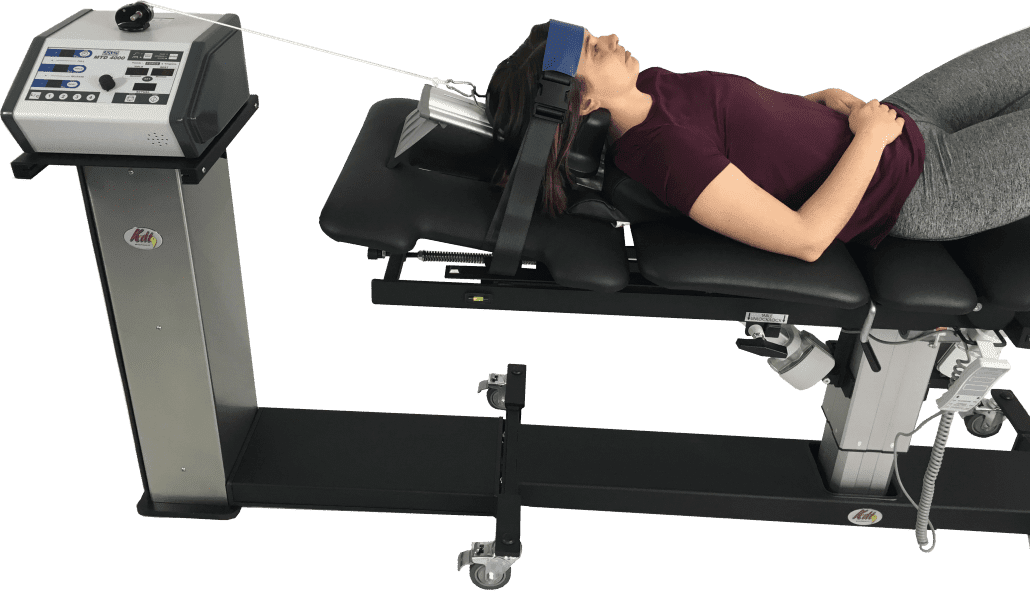
How To Operate The DRX9000-Video
The video above explains how to operate the DXR9000 decompression machine. The DRX9000 is part of spinal decompression therapy. It utilizes traction to gently stretch the spine to all the nutrients that go back into the spine and cause instant relief to many individuals. Many decompression machines allow many decompression treatments to the lumbar spine and provide relief to the cervical spine. With physical therapy, decompression therapy can alleviate the painful symptoms that affect a person’s quality of life and continue on their wellness journey. If you want to learn more about spinal decompression therapy, this link will explain the benefits of spinal decompression and how it can alleviate low back pain symptoms.
How Cervical Axial Decompression Reduces Neck Pain
Since many individuals suffer from neck pain, many treatments can alleviate neck pain. Research studies have shown that treatment for neck pain usually depends on the cause and the best way to reduce neck pain includes:
Gentle stretches
Use heat or ice packs
Traction therapy
Physical therapy
With traction therapy, many individuals are placed in a supine position on a decompression traction table and are strapped in so they won’t slide off. For cervical treatment, individuals are lying on the table as their head is positioned in a cervical cradle unit and strapped in as the traction machine gently stretches the cervical spinal joints to reduce the pressure on the neck. Research studies have shown that cervical decompression can directly reduce the volume of the hernia by creating negative pressure on the intervertebral discs to cause instant relief. Cervical decompression can also increase the intervertebral disc height and decompress the cervical nerve root to diminish the painful symptoms that cause neck pain.
Conclusion
All in all, neck pain is common for many individuals worldwide, caused by stress, injuries, or neuromusculoskeletal disorders. With neck pain, many individuals will feel muscle stiffness and compressed discs that can hinder a person and cause many unwanted issues that they don’t need. Utilizing decompression therapy can help alleviate neck pain and help repair the cervical disc by allowing the nutrients to rehydrate the cervical spine. With physical therapy, many individuals can feel instant relief from decompression and even add small changes to their lifestyle habits that can lower their stress levels and continue on their wellness journey without being in pain.
References
Förster, Matti, et al. “Axial Low Back Pain: One Painful Area–Many Perceptions and Mechanisms.” PloS One, Public Library of Science, 2 July 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3699535/.
Kazeminasab, Somaye, et al. “Neck Pain: Global Epidemiology, Trends and Risk Factors.” BMC Musculoskeletal Disorders, BioMed Central, 3 Jan. 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8725362/.
Staff, Mayo Clinic. “Neck Pain.” Mayo Clinic, Mayo Foundation for Medical Education and Research, 31 July 2020, https://www.mayoclinic.org/diseases-conditions/neck-pain/symptoms-causes/syc-20375581.
Xu, Qing, et al. “Nonsurgical Spinal Decompression System Traction Combined with Electroacupuncture in the Treatment of Multi-Segmental Cervical Disc Herniation: A Case Report.” Medicine, Lippincott Williams & Wilkins, 21 Jan. 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8772752/.
Athletes and fitness enthusiasts work hard to stay in shape, but they are also at an increased risk for a lumbar hyperextension injury. Lumbar hyperextension injuries happen when the low back is bent backward repeatedly or overarches repeatedly. The repetitive stress can lead to severe complications and damage the nerves, vertebrae, and backbones. Motorized decompression therapy could be a treatment option.
Lumbar Hyperextension Injury
Injuries can be caused by overuse, improper mechanics and technique, lack of proper conditioning, insufficient stretching, or trauma. When looking for symptoms of lumbar hyperextension injuries, the first is low back pain that is severe and lasts at least a few days while becoming more intense with time. The lower back pain that worsens when extending, or arching the back, in addition to stiffness, muscle spasms, radiating buttock and thigh pain, tight hamstrings, and difficulty standing or walking, can be indicators of a lumbar hyperextension injury. However, this could be difficult to distinguish from other injuries like muscle strain, disc herniation, and stenosis; this is why a proper examination by a medical professional is recommended.
Treatment
Initial treatment consists of resting, sitting out from the sport, and other activities that could aggravate the back.
A doctor may recommend over-the-counter non-steroidal anti-inflammatory medications.
Heat and ice can also be used to increase circulation and relieve pain.
If hyperextension of the back continues even after rest, it could signify a stress fracture in the vertebrae. This condition is referred to as spondylolysis.Spondylolysis is an overuse injury. It occurs in individuals who participate in sports like gymnastics, diving, volleyball, football, and weight lifting. Spondylolysis and spondylolisthesis are common in adolescent athletes experiencing lower back pain.
A doctor may assign a back brace to prevent movement, allowing the bone to heal back together.
A doctor could also recommend physical therapy for 6-12 weeks after the diagnosis and once the bones have had time to heal.
Rehabilitation exercises focus on improving back flexibility and strength.
Athletes can be cleared to return to their sport within 3-6 months.
Surgery is rarely necessary and only looked into if the individual continues to have persistent pain after 6-12 months of treatment.
This changes the spine’s position, takes the pressure off the nerves and discs, and restores the cushioning.
As the machine pulls the body, a vacuum effect fills the discs with oxygen and nutrients to stimulate healing.
Computer technology controls treatment duration, angle, intensity, and relaxation.
Prevention
Athletes and fitness enthusiasts are recommended to seek professional help to retrain how they perform repetitive and excessive high-impact activities. Specifically, those involving hyperextension movements like kicking, jumping, running, and back bending help minimize the risk of developing a back injury. They are also recommended to maintain body conditioning, back and hamstring flexibility, core muscle strength and endurance, cardiovascular fitness, and properly warming up and stretching before and after the physical activities.
DOC Decompression Table
References
Ball, J.R., Harris, C.B., Lee, J. et al. Lumbar Spine Injuries in Sports: Review of the Literature and Current Treatment Recommendations. Sports Med – Open 5, 26 (2019). https://doi.org/10.1186/s40798-019-0199-7
Carter, D R, and V H Frankel. “Biomechanics of hyperextension injuries to the cervical spine in football.” The American journal of sports medicine vol. 8,5 (1980): 302-9. doi:10.1177/036354658000800502
Goetzinger, Sara, et al. “Spondylolysis in Young Athletes: An Overview Emphasizing Nonoperative Management.” Journal of sports medicine (Hindawi Publishing Corporation) vol. 2020 9235958. 21 Jan. 2020, doi:10.1155/2020/9235958
Lawrence, Kevin J et al. “Lumbar spondylolysis in the adolescent athlete.” Physical therapy in sport: official journal of the Association of Chartered Physiotherapists in Sports Medicine vol. 20 (2016): 56-60. doi:10.1016/j.ptsp.2016.04.003
Low Back Pain: Could it be a Spondy? Nationwide Children’s Hospital. (n.d.). https://www.nationwidechildrens.org/specialties/sports-medicine/sports-medicine-articles/low-back-pain-could-it-be-a-spondy.
Dr. Alex Jimenez DC talks with Dr. Brian Self DC about the beneficial properties of spinal decompression therapy and how it can alleviate many individuals dealing with low back pain. Spinal decompression therapy utilizes traction by gently stretching the spine, allowing the nutrients to go back into the spine. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
[00:01:10] Dr. Alex Jimenez DC: I can. Yes, indeed. We’ve got Rob on. We just have a few other people just kind of pile on in here. And I’ll just keep allowing him to come in as we go. But guys, we’ll get started here now. We’re about one minute past 12:30, but I asked Dr. Self to be on. Many of you have met him already in regards to the doc tables. Dr. Self, we have a couple of offices on this call that runs decompression, not necessarily the DOC table. I’d be in one of them, but I’m ordering a doc table. So we’ve had everybody hop on this call because, the information you can share, you have more clinical and business experience with decompression than any of us and all of us combined. So I wanted to get you on a call with everybody that we have up here in the Midwest now recording some of the docs that could make it so we can make all kind of start off as a good baseline of, you know, some of the teachings that you’ve given to individuals over time and what DOC table you get them rolling with it. We still run into some consistent questions from doctors. Maybe there’s a little confusion, so I wanted to bring you on so so docs can answer or ask you questions so you can answer those. And then we’ll just kind of muddle through probably three or four different topics on this call and then open it up. And I want to open up Q&A the whole time docs, whatever questions you have if there’s anything pressing you’re dealing with right now. Any questions you have will be great for the rest of us to hear. So I gave Dr. Self a little heads up on some of the questions we talked about on our first call and some of the things he’s working on for us, such as the cheat sheet. Or what do we call on that the flow chart? The flow chart, so Dr. Self’s working on that right now, and we’re excited to get that to you here shortly. Still, one of the first topics that we had on the list was the proper diagnosis in diagnosing and what protocol or the appropriate protocol. So, Dr. Brian, if you want to start, maybe there with your experience and share a little bit, and then docs, if you have any questions, unmute and fire away. So it’s going to be an open forum.
[00:03:23] Dr. Brian Self DC: All right. Thanks. Yeah, as far as diagnosis goes, you know, many people always ask, Well, do I need an MRI? I can’t do it without an MRI. I would say starting. They’re just my opinion, as most of these patients don’t need an MRI. As long as you feel like it’s not something weird or more severe, you wouldn’t want to miss multiple myeloma or pathologic aortic aneurysm or something that would be an absolute contraindication to care. So if you feel like it’s pretty straightforward, my own opinion is I tell patients, you know, give me two weeks, let’s treat every day for two weeks. And if we don’t have any results by the end of the second week, maybe let’s get an MRI. The vast majority of patients will see some sort of relief if you do it every day for two weeks. Most patients will feel a little bit of relief to the point where an MRI is probably not necessary. You can keep going and finish out the rest of the protocol. I tell patients that you can spend their time and money on a test that will probably not change how we treat this. Or you can spend your time and money on the actual treatment of the condition itself. So that’s one of the main questions that come up. But like I said, if you feel like it’s anything weird or random or you’re not quite sure, obviously get an MRI at that point; better safe than sorry. But as far as when the patients come in, you know you’re going to check their dermatomes, do their reflexes on everybody, and do muscle testing on everybody. Those are the three annual orthopedic tests. I would say that those are the four things regardless of, you know, even if you’ve seen this a thousand times. Going through those things with the patient shows them that you’re the specialist, you’re the person taking the time, the energy to find out specifically what is wrong and how can we best treat it? You know, I think that a lot of times we think that we get so good at this and maybe we are, maybe we don’t even need to do that stuff, but the patient needs to see that stuff and feel that stuff to qualify you as the specialist ready to treat this specialty type condition. So, you know, again, reflexes, dermatomes, arms, muscle testing, and then your orthopedic test will be the main ones, in my opinion. What I think that you’re looking for is, first and foremost, to make sure it’s not an absolute contraindication that care. Number two is a lot of it comes down to patient positioning. So figuring out, is this patient going to benefit from flexion? Will they benefit from the extension, or will they benefit from some lateral flexion or some lateral flexion with rotation? There have been plenty of patients that I put on a table over the years, and I had no idea what they had, but I knew that if I could find what makes it better, what makes it worse, I could recreate that on the table. Then the vast majority of the time, I could get those patients better. So certain conditions do have certain protocols that you’ll follow. For example, spondylolisthesis will be supine in full flexion with their knees up. That’s just what research has shown to be the best treatment response to spondylolisthesis. So, in general, you’ll start with full supine flexion, bringing the knees up. Grade one and grade two are fine. Grade three and grade four would be technically a contraindication for decompression. Luckily, I’ve never seen a Grade four; I think I’ve seen one grade three. And then, if you’re not sure, you can do some flexion-extension studies to see how much slippage is taking place. And then stenosis will probably be a pretty good amount of flexion, generally supine only because those patients are usually heavier and older. They’re not going to want to lie prone, for they’re not going to be prone comfortably for the entire treatment. So I usually will start those patients off supine. Now, in the rare instance that they can do prone, if you can get them comfortable, prone with your table flex down can be the most effective patient for stenosis. And the reason for that is because this is a question that we get a lot when I treat prone. I would think of when to treat prone if you have a posterior bulging disk and especially a younger patient where flexion makes it worse, and the extension makes it better. OK. There are a couple of reasons for that. Number one is when they’re prone, you have gravity working in the same direction that you want it to go. So if it’s a posterior bulging disk and they’re lying prone, you have gravity in your favor. Number two is you’re simply going to be in more extension; you can get a more true extension in the spine when they’re prone versus anything that you could do supine. One thing that is nice about the DOC table is that it is supine. You can take the table down in some extension. So if you’ve never noticed, this is one of the few tables where you would take your table up into its highest elevated position, but then lumbar flex down so that the bottom of your table is flexed down. So if a patient were supine, this would be a way to get some extension into the spine, although prone is still going to be more extension than you could ever do supine. So this would be my last choice. If a patient needs extension but can’t do prone, then the best that you would be able to do would be supine and hold down your lumbar flexion until the table is basically horizontal and then angles down. OK, so if they were supine, this would be an extension. And then again, if they were prone, this could be a position for a stenosis patient. If they could lie comfortably is the issue; this would be a good position for us to know stenosis because often of stenosis, you have a central bulging disk that’s going to be posterior. And again, any time you have a posterior bulging disk, the gravity working in the same direction, combined with the Mackensie type of protocol, you know, when they’re extended, you’ve got posterior structures, all you’ve got all your structures pushing on the posterior portion of the disk. And that is going to want to push that back into place mechanically. Combined with the negative pressure that’s generated inside the disk, when you’re doing the decompression with any sort of linear traction, you’re going to have that negative one hundred and fifty millimeters of mercury up to negative one hundred and ninety millimeters of mercury generated inside the disk as well. So, in my opinion, prone offers those three benefits, which can be far superior to supine. So it’s this kind of random. We’re going all over the place. But so again, stenosis could be either supine at flexion, what their knees up, or if tolerable, they could be prone with the table flex down. So they’re still in flexion because you want to open up that central canal; you know that full flexion will open up the Central Canal by around 20 percent. So you’re getting the benefit of the flexion combined with the benefit of the negative pressure.
[00:12:51] Dr. Alex Jimenez DC: So Brian, sum up your experience dealing with prone. So you gave us two conditions. The synoptic typically is they’ll respond favorably to that, and I understand their presentation matters as well, but stenosis and your bulging disc. Are there any other just conditions? I hate to say as a general rule, but that you be considering prone become.
[00:13:19] Dr. Brian Self DC: Yeah. And again, I think it would come down to any time extension that makes it better. Then I’m thinking prone. And so I’ll almost always take patients through just a primary range of motion, you know, bend forward and touch your toes. What does that do to the symptoms down your leg? Extend back? What does that do to the symptoms down your leg and your foot? Lean-to the left, you know, put them in the left lateral flexion? What does that do to the symptoms down your leg and your foot having to lean to the right? What does that do? What all you’re doing is just looking for what makes it better. What makes it peripheral is what makes it centralized. And then after that, you could get into some more of your specific orthopedic tests like your slumps is a perfect one. Straight leg raise. You know, all those can be a little bit beneficial sometimes. But I think to start, if you’re not sure about orthopedic tests, just look for generalities and range of motions. Sometimes I’ll even put them on their stomach, have them come up and do a Mackensie protocol, and maybe add some overpressure. OK, what does that do to the symptoms down your leg into your foot? Do you feel like those are going farther down your leg into your foot? Or do you feel like we’re making it worse in your back? And often, the only difference that they know is they say, “Yea, my legs are better, but my back is killing me. What did you do to my back?” And that’s a good thing. You know, you’re getting centralization of symptoms, which we’re always looking for. Everything comes down to what centralizes and what peripheral diseases the symptoms, and so regardless of, you know, I think a lot of times we get caught up in patient comfort, which is essential in the fact that they have to be able to lay there for twenty or twenty-three minutes, do not pull through the pain. I spent years going through the pain, just thinking, OK, if I can get them on the table and pull through that pain. They’re going to get better, and looking back on it, and I think I made a mistake early on because I didn’t have a DOC table. I had a DRX9000, which only treated supine inflection. And I think where I missed a lot of patients was not finding the exact position that centralizes the symptoms because I could only pull in one linear position inflection. And I think where this table separates itself is being able to flex the table and laterally flex with rotation. And again, a lot of that’s just going to be based on how the patient is seated in your waiting room? They’re seated in your waiting room, leaning to the left and left rotated. And that’s what’s bringing them relief. I know I’m putting the table on a left lateral flexion with the left rotation because that’s the position that their body is telling them is taking the pressure off of the nerve. So just because I know we have a wide range of people who have had a table for different times. But again, your lateral flexion will be the button on the left, so I always think l- for left is L for lateral flexion. So if we go to just the left one, we can laterally flex the table left and right. And then R for right is R for rotations. So if I squeeze just the right one, I can rotate the table left and right. I usually do one at a time just because it’s confusing to try to do both simultaneously. But if I have seen a patient walking down the hallway and holding on to the wall and they’re in the left lateral flexion with a bit of left rotation, I know I’m going to go to the left lateral flexion with the left rotation.
[00:17:39] Dr. Alex Jimenez DC: In your email, obviously starting with observation, which should be for all of us. Still, you’re taking all that in consideration of finding their intelligent posture that decreases their pain level in addition to the exam with your range of motions defined, you know whether it’s a centralized player for eyes is all that information that you’re using that to allow you to see how you’re going to set them on this table?
[00:18:02] Dr. Brian Self DC: Absolutely. The way they’re sitting in the waiting room, the way they’re walking down the hall, and then my orthopedic tests range is the motion. And then lastly is, sometimes I still have no idea at that point. Well, I’m just going to put them on a table, take them through the range of the motion on the table and see if they can tell you, OK, yeah, that feels a lot better; that’s way worse at shooting down my leg into my foot right now. Sometimes I have no idea, and I’ll just put the table in left lateral flexion and say, OK, what’s that doing to the pain down your leg? And your foot is way worse? It’s shooting down my leg right now as we speak. OK, then take it in the other direction. What’s that? Yeah, that does seem to be a little bit better. And sometimes, even at that point, patients like I don’t know. Yeah, it’s kind of better. I’m not sure. In that case, I’m just going to do an entire treatment based on what I think I should do. And I’m going to tell them, OK, tomorrow when you come back, tell me, did that seem like it made it better, worse, or the same if they come back and say that was worse, it was shooting worse than it’s ever done. Then tomorrow, during the next treatment, I will do the complete opposite. Now, keep in mind that I would only change one parameter per visit so you can keep track of exactly what’s going on. So, for example, if I’m going to do lateral flexion, I’m going to do left lateral flexion, and that’s the only parameter I’m going to change. And then tomorrow, when they come in, OK, did that make it better? Worse or the same? Oh, it was way worse. OK, today I’m going to do right lateral flexion, and then they come back. That was a little bit better. OK, now I will try some right lateral flexion with right rotation and then return. Yeah, that felt good. OK, then I might try more flexion, and they come back. That was worse than I might have so that I might put them in a more extension. They come back. That was a little bit better. And then I might try, you know, an aggressive treatment. So if I’m doing 50 pounds of force and feel like they’re just not responding the way they should, then I might go up to 70 pounds of force. And then they come back. I was so sore. Yeah, that wasn’t very pleasant. So then I know that may be more force is not the answer. So then I might try a longer treatment, but with less force. So if I was doing 50, I might try 40, but for like 30 minutes or thirty-five minutes or, you know or even like 30 pounds of force, but over like thirty-five minutes and see how they do. Many of your strictly degenerative discs will respond better to more time but less force. If you treat with too much force over too much time, you’re barely going to be able to get the patient off the table, which I’ve done hundreds of times. I just did it last week on a friend of mine. If you overtreat it, the worst-case scenario is that everything locks up and goes into spasm. You have to peel them off the table, and you have to try to get them to walk it out, which can help. But you know, you don’t want to set them back a visit. This isn’t like a lot of treatments where it’s one step backward and two steps forward. If you were doing a shockwave or a technique or something, sometimes, you will make them worse before they get better. With this, I don’t think that’s normally the case. I think you want to be better safe than sorry. Be a little bit more conservative. Less is more.male doctors in particular. Sorry, but we get in the bad habit of pulling too hard. We think that if 50 pounds of force is recommended, if I do 70, they will get better, faster. And that’s not the case with decompression, either. If you look at the research, they showed that they weren’t trying to show this. So you have to extrapolate it. But on the VAX-D, when they were treating prone, they got up to negative one hundred and ninety degrees of negative pressure of mercury generated inside the disk between about sixty-five and seventy-five pounds on their table. And then what happened was the harder they pulled. That negative pressure started going back down in most people, so at like 40 pounds of force is the minimum it took to get any negative pressure generated inside a disc. So, one thing to know is that anything below 40 pounds can still have benefits, but you’re not generating any negative pressure inside a disc. Now you’re still, you know, you’re still doing a lot of good, but you’re not getting any vacuum effect until about 40 to 45 pounds of force. And then once you know, around 50 pounds of force, it was like negative 70 millimeters of mercury. And then again, between negative around 65 to 75 pounds prone, they were at negative one hundred and ninety millimeters of mercury. But then what was interesting is once they got above that, like 85 90 pounds of force, you started to see that go back down a little bit. And again, they didn’t take it far enough. I would have loved to have seen higher amounts of force to see what happened. Would that negative pressure go back down closer to zero at a certain point if we pulled it at one hundred and fifty pounds of force? I don’t know. But I think what you can see from it, and in my opinion, there’s a sweet spot in there. You’re looking for that sweet spot of pulling hard enough to generate the most negative pressure. Still, not pulling so hard that you’re getting guarding, you’re getting spasm, which is, I think, what prevents the most amount of negative pressure from being generated. Does that make sense?
[00:24:27] Dr. Alex Jimenez DC: Yeah, I think some said to bring it back to the user every tool that you have to start with the most appropriate and applicable treatment plan, but there’s going to be some those patients that you’re just not sure. Right. So if you have a patient that you’re just not sure about, you start them on. Are you constantly starting them supine and going from there and then making some tweaks? Or what’s your general?
[00:24:56] Dr. Brian Self DC: Yeah, I do supine. I think about supine is it’s going to be the least likely to make somebody worse is going to be the most comfortable. It’s going to be the least likely to make somebody worse. At least I’ll usually start them off on the legacy one for one cycle and see how they do legacy one on one cycle is going to be about 14 minutes on the lumbar, and it’s going to be way too gentle for most people. And most people will say, I’m not feeling a lot, and that’s perfectly OK. So on supine, start them up on legacy one one cycle. If they come back for the next visit and I didn’t make them worse, I will go up one cycle per visit for the first five visits. So visit number two would be legacy number one for two cycles. Visit number three would be three cycles, and one cycle adds about three minutes per treatment. So visit number four-four cycles, visit number five five cycles. That’s going to put you around twenty-four minutes. That’s the most I would do if you’re trying to maintain 30-minute appointments. So if you’re trying to treat patients at 9:00, 9:30, 10:00, and 10:30, keep it around twenty-three minutes or less. That gives you about seven minutes to take patients on and off the table.
[00:26:27] Dr. Alex Jimenez DC: OK, so docs, any questions about anything thus far. Clarification is needed on any points. Dr. Christian, go ahead.
What To Do Before The Treatment
Dr. Christian DC and Dr. Brian Self DC explain the procedure of getting the individual onto a DOC decompression machine.
[00:26:39] Dr. Christian DC: Quick question. You mentioned briefly the size of the patients and how heavy they are. We have found that with the large patients with big bellies and, like smaller waists, we can’t get them strapped effectively, especially prone; it’s almost like it’s coming down their butt. Is there any way to not create that slippage without cutting off their pelvic circulation?
[00:27:10] Dr. Brian Self DC: So again, on a heavy patient, that’s going to be the drawback as prone is not going to be comfortable, and obviously, you could do supine and take the table all the way down into extension as I showed you. That might be good if you know a couple of things you could do, like your harnessing. And you see this a lot with women who are wearing, like, really slippery silky shirts. You don’t get a lot of slippages. So a lot of times I’ll take my towel. And then drape it over there; it’s the most amount of slippage generally takes place in the thoracic harness. But if you’re treating a problem on a bigger patient, I can see how you could get some of that in the pelvic harness. So but generally, I will take a towel and tuck it around the rib cage, especially if a woman wears a slippery, silky shirt. And then I want to bring this harness over the towel, adding a little bit of grip and a little bit. Also, if it’s tender like if they’re an older lady and have really fragile ribs, that might add just a little bit of comfort; subsequently, you could. And I’ve only done this on a few patients, Dr. Christian, but you could take another towel. And you could drape it over their pelvis. And then bring this around that might help, you know, if they’re not, especially if they’re not wearing jeans, jeans usually make it pretty effective. But even just a towel between the fabric and the harness can help. I’ve had patients that, you know, older people, when you put this on, especially like the buckle from the seat belt, it pinches on their hips or the bone. You know, I’ve taken pads, you know, the towel would be my priority. I’ve taken pads and stuffed them in there, like over the hips or wherever they tend to get, or it puts pressure on. You can put at some, you know, you could take something soft and comfortable and slide it in there as well, that that might help as far as if the harnesses are slipping on the patient.
[00:29:48] Dr. Christian DC: If that person we were doing is doing a flexion, not an extension, should I just put them supine to get a better pull?
[00:29:58] Dr. Brian Self DC: Yeah. Suppose you’re in flexion, and it is better than you would want to go supine because they’re going to be a more flexion; if that’s not working, then I would try prone inflection because it is the one thing that can be the most dramatic game-changer of all the parameters. And I know you probably heard this story about Dr. Tom Shack, but he had done hundreds of visits to the treatment table. He owned one, and I think it was either his office or his house. And he used that hundreds and hundreds of times, but only did it supine. And he said, you know, he felt like it kind of helped. But, you know, after hundreds and hundreds of treatments should have been a lot more effective. And then I got him started prone on the DOC table. And, of course, he liked, doubled the parameters that I told him to do. You guys don’t tell him I told you this, but he got way too aggressive and made him so much worse. And he was like; You can come to pick this table up because I can’t even get out of bed. And I said, Well, what parameters are you doing? And he was like, That’s nothing like what I told you to do. So when he did back it off, doing the prone dramatically made a much more significant difference than supine, even though he was a less force and less time than he was doing supine on the Triton table. He was able to get away with even less force and less time prone because of the dramatic difference it had on his discs in whatever way it was addressing that. So if I’ve tried just about everything and nothing’s seemed to be a big difference, just switching them simply to prone can have a dramatic effect. And a lot of times, it’s not even comfortable while the patients are like this is not comfortable at all. But the results start coming so much faster than they’ll tolerate it. But know that being prone is not a comfortable position, but it can be much more effective. And you can get away with a lot less force prone. So, Dr. Christian, maybe if you like prone and you feel like that’s going to be a good one, if you’re getting some slippage with the harnesses, try less force and see if that helps with the slippage as well because you can get away with less force and get the same results because of the prone versus the supine.
[00:32:36] Dr. Alex Jimenez DC: How long do you wait before you go prone, so if we’re starting somebody supine, you’re like, Man, you commented that I’d tried all these things. Well, what are those other things that you’ve tried? And then determined it’s like, All right, we got to flip them over. We have to go prone.
[00:32:49] Dr. Brian Self DC: I’d say probably by the end of the second week. If I haven’t seen any results, I will get much more aggressive. The first week is just trying to get their body used to the treatments, so I don’t usually switch up anything the first week other than increasing one cycle per visit. And so, after the first week, I’m just trying to get their body used to it. Then the second week, I’m starting to add some different parameters to see if any of those will make a difference. So every day, you’re going to treat for the first two weeks. So I almost always start my patients on a Monday, maybe Tuesday at the latest. Maybe Wednesday. I’m not going to start a patient on a Thursday or Friday because if you set them back a lot of times. So like, if you start a patient on a Thursday and you make them worse and then the Friday, you make them worse. Now they have two days of being in that pain till you can see them again, and you lost all the ground you made. So I’m generally starting on a Monday or Tuesday, ideally on Monday. They’re going to treat every day for that first week. All I’m going to do is go up one cycle per visit for that first week. Then the second week, I might add some flexion. I might add some extensions. I might add some lateral flexion or lateral flexion with rotation. I might experiment with the forces and the times. And then, by the end of the second week, if they haven’t seen any results or feel ready for prone, I’m going to flip them over prone, starting probably in week three, the first visit a week three. Now you’re going to go every day for two weeks or until they’re at least 50 percent improved. So in that rare case that you get to the third week and they’re not 50 percent improved, keep going every day until they’re at least 50 percent approved; then, at that point, you can go three times a week for two weeks and then two times a week for two weeks.
[00:35:02] Dr. Alex Jimenez DC: Cool beans.
[00:35:05] Dr. Brian Self DC: To review quickly on prone, everything will be the same about supine, and let’s just quickly review that to make sure what you’re looking for. So you’re looking for this red line to be right at the bottom of this thoracic cushion on everybody, regardless of how tall or short they are. That red line is going at the thoracic cushion. This harness moves up or down. The thoracic harness moves up or down, depending on how tall the patient is. So your shortest patient, you’re five foot zero female. Those two red tabs are going to be touching each other. So this thoracic will slide down until those two tethers zero-gap there. That’s going to be the shortest patient that you treat. And then five foot four to about five foot 11 is going to be about two to three-inch gap there with again with the thoracic harness moving and then six foot two legs six foot seven. It’s going to be a four to five-inch gap there. OK. What this is equal to is the top of the iliac crest, which always goes at the top of this pelvic harness or the red line is about the ASIS, so that is always on every patient that’s going to be standard regardless of whether they’re supine or prone or taller, shorter, heavier. This red line goes at the bottom of the thoracic cushion. There is always that the red line or the top of the iliac crest is at the top of the pelvic harness. OK. And then what you’re aiming for here is for the harness to come for the lowest rib to be right in the center of this harness. So when you’re bringing this around, you’re going to bring it around and down. So we want our very lowest rib to be right in the center. So half of the harness is above the lowest rib, half of the harness just below the lowest rib. OK, that’s stuck around that rib to prevent the patient from sliding down as we pull. OK. So you know that you did it halfway, correct? If this makes an X pattern, OK, so when you come around and down, this should look like an X, and this lowest rib should be right in the center of that harness. And so, again, the distance between these two harnesses is equal to the distance from the top of the iliac crest to the lowest rib. Now keep in mind that because women have higher hips and a higher iliac crest, this base here will be a little bit shorter on a woman than a similar height on a male, so if you have a five-foot-eight female versus a five foot eight male, the five-foot-eight females that are going to be a little bit higher. And so, keep that in mind as well. But when you’re doing prone, all you’re going to do is take your armrests out of the supine slot, and nobody ever figures these out, but you’re going to take this out of the supine. You’re going to turn it around one hundred and eighty degrees and put it on the opposite side of the table in the lower slot facing forward like a chiropractic table. And so the that’ll give the patient while they’re lying prone to put their arms on, and then I usually get a massage face pillow, put it over the thoracic harness so that they can comfortably put their head straight, just a U-shaped massage pillow is fine on that. And then this is going to be flexed down a little bit. So their neck is not extended. And then so they would be laying prone. But all of this is the same, regardless of whether the patient is supine or prone. All of that’s going to be the same landmarks, same philosophy. You’re either trying to create a vacuum effect and reduce a herniated disc or pumping that disc for a degenerative disc with an intermittent short type of cycle. But all that philosophy will be the same, regardless of whether they’re supine or prone.
During The Treatment
Dr. Denay DC and Dr. Brian Self DC explained their experience when going on the DOC decompression machine.
[00:40:18] Dr. Alex Jimenez DC: Good docs, any other questions? Keep on firing them. Dr. Denay, did you get your answers about your back answered last week?
[00:40:28] Dr. Denay DC: I did, yeah.
[00:40:30] Dr. Alex Jimenez DC: Well, yes, shared; it’s good to hear that you’re a patient affected adversely to decom table.
[00:40:38] Dr. Denay DC: Yeah, it was me. I was the first person I couldn’t get off the decom table, so that was good. It was. I did supine, and then Tom and Jack told me to go prone. And then I went back to supine, and I went not prone first but went supine the next day, legacy one, and I couldn’t get off the table.
[00:41:01] Dr. Brian Self DC: Do you remember your parameters regarding how many pounds?
[00:41:08] Dr. Denay DC: So I did one-third of my body weight, weighing 170. So I think it was like 50 pounds. Right? Yeah.
[00:41:18] Dr. Brian Self DC: Do you remember if you did legacy one or?
[00:41:20] Dr. Denay DC: Legacy one.
[00:41:22] Dr. Brian Self DC: For just how many cycles?
[00:41:23] Dr. Denay DC: I was on there like 20 minutes, so two or three cycles. OK. And I felt fine initially, and then there was just a lot of pressure, and I pushed through that, now knowing I don’t ever pull through pain. I should have stopped it right there, and I think it would have been fine. But yeah.
[00:41:42] Dr. Brian Self DC: And that’s a very common mistake. Like I said, I’ve done it hundreds of times. I’ll continue to do it. It’s just it’s either too much force. So I would back it down in your case, back it down to about 40 pounds. I would put it out one cycle and maybe even stop the treatment earlier. See how you do for too much time. If you feel like that, 14 minutes is even too much. And then also, did you do any stretching before you got off the table?
[00:42:19] Dr. Denay DC: Yes, I did. But I think I couldn’t lift my left leg. It was just like pressure and pinch feel. So that’s when I was like I had pulled it up myself, but it was painful to lift it by myself. So then the next day, I reached out to Casey, and he’s like, I don’t know, ask Tom or Jack. Last night, Jack told me to do K1 the next day. So that night, I was super, super sore. I iced all night, and then I did K1 the next day and felt so much better.
[00:42:51] Dr. Brian Self DC: Yeah, and that’s perfectly normal. And it’s hard for patients to understand, but just know that that is perfectly normal. It doesn’t. You see, maybe 15 percent of the time, it will happen like that. You’re going to make a patient worse before they get better. All that means is that you overtreated it. Like I said, either too much force or too much time or a combination of the two. Maybe the patient position had a little to do with it, but back off; everything starts slow and works your way up. If the next treatment you were around like 40 pounds over, like, let’s say, 13 or 14 minutes, see how you do. If you don’t make anything worse, give it a couple of bases, then go up to forty-five pounds over 16 minutes and then maybe 50 pounds over 17 minutes. I would say at least one or two weeks, basically real gently and slowly ramping yourself up. And what you’ll find is that your body will continue to get used to each treatment. And then you’ll hit a visit where most patients hit one visit, where everything just starts to get better from that point on. Now, sometimes that takes a week, sometimes it takes two weeks. Whatever it is, once they hit that visit or start getting better, it all seems to snowball and go downhill from there. But in that interim, you know, you might make somebody a little bit worse before they get better until you figure it out or overtreat them. And that, honestly, I hate to say it, but that’s perfectly OK. You want to avoid it if you can, and you can prevent it with less force and less time and patient positioning.
[00:44:45] Dr. Alex Jimenez DC: I think the communication piece before starting people on decomp is to make sure that you guys are all prepping for those reactions. It’s no different than the adjustment. So as it does occur, if it does happen in that 10 to 15 percent of your patient base, it’s not an alarming piece to the treatment. It’s normal.
[00:45:04] Dr. Brian Self DC: This is expected. And then again, I know you said you did this, Dr. Denay, but make sure that you’re stretching the patient before getting off the table. So while they’re laying there on their back, have them. I have them put their feet flat on the table with their knees up. Just kind of have them rock side to side. You’re just trying to get everything moving again before they go to put all that pressure back on it and then have them bring their knee up to their chest for a minute. Stretch it in. You could add a little bit of overpressure if you wanted. A worst-case scenario is you have them get up and walk it out. They can always walk around the clinic a little bit, and they will slowly start to walk that out. Another thing you could do is you can take your back brace if the disc is super hot and you’re just not sure. You can always take your back brace and put it under. So undo all their harnesses so that everything’s nice and open. And then take your back brace and slide it under while they’re still laying there. You know, just kind of shimmy it under there and then put their back brace on nice and tight and then come off. Often, on a hot desk, you know, it feels fantastic when you’re decompressing it. And then they go to sit up. And all of that pressure comes down, and it can even be worse than before. Having that back brace on there before they get up can sometimes minimize the amount of downward force on that disk, which can help a little bit. And then, you know, stretching them before they get up is huge. And having them walk around the clinic to kind of walk it out. And then we’ve talked about this before, but getting the back braces with the hot and cold packs, keeping them frozen in the office. And so they come in with their unfrozen ice pack when they’re done with the decompression, take your ice out of the freezer, switch it out, so you’re not losing ice packs. Put the ice packs in their back brace. Have them drive home with 20 minutes of ice, then take the ice out and wear their back brace for a minimum of three to four hours after every treatment. The first week I have them wear it all day, every day. I feel like it’s one of the few things that makes a big therapeutic difference in helping to stabilize that disc, helping to remind them not to do anything silly. And so I have them wear their back brace all day, every day for the first week. I think Dr. Cox of Cox’s flexion and distraction. He said he has them wear it more than 48 hours a day for the first, like three days, or even sleep in it. You know, I think three to four hours minimum after every treatment. Six to eight hours on some of your more acute patients can sleep in it if they feel like that helps. So the back bracing, I think, is one of the few things that does for a low cost; it does make a pretty good therapeutic value there.
[00:48:43] Dr. Alex Jimenez DC: OK, docs, any other like prone versus supine moving doctors through? I think he hit that pretty well, but is there any confusion? Or positioning? I think we’re pretty good on that. I guess remaining questions on that topic.
[00:49:03] Dr. Brian Self DC: One thing, if you can’t see what you have in mind, I know going over K one, I sometimes think how to put in the parameters on a computer that can be a little bit confusing sometimes. But what do you have next?
The Recovery Process
Dr. Brian Self DC explains the after-care protocol that all individuals must do after getting treated with spinal decompression.
[00:49:17] Dr. Alex Jimenex DC: I think just noted contraindications. There’s an average presenting patient. So you talked about a grade three forces on spondylosis, just direct contraindications? Yeah.
[00:49:31] Dr. Brian Self DC: Yeah, I mean, there’s a complete list I’ll send you. You know, my philosophy is if you didn’t adjust it, you probably wouldn’t decompress it. So anything, you know, that’s metastasized to the spine, multiple myeloma cancer that’s affected the vertebra, disk infection, an artificial disk, in my opinion, is an absolute contraindication. I think they’re not that great. I think you wouldn’t want to be blamed for a pretty crappy product in the first place. Pathologic aortic aneurysm. You know, there’s a certain amount of millimeters. I can’t remember what is at the top of my head, but any sort of aortic aneurysm, if you wouldn’t adjust it, you probably wouldn’t decompress it. Pregnancy? You know, screws, rods, cages. I have to tell you guys; technically, it is a contraindication. The only thing I can say is that doctors treat them all the time. They focus on the area above or below, you know, from all the surgeons I’ve talked to, they’re going to tell you that you couldn’t pull a rod or a screw loose with 40 pounds of force or 50 pounds of force or 60 pounds of force. But technically, rods and cages are a contraindication. A discectomy is one that many people ask about in a failed discectomy. The research recommends waiting a year after a failed discectomy or laminectomy. There’s going to be a lot of scar tissue in there. The one patient I treated with a failed discectomy was only about six months old. It was just the treatments were just way too sore. It made him way too sore. I was just pulling on that scar tissue that hadn’t fully healed; you know, pulling on relatively fresh surgical tissue did increase his pain enough that he couldn’t finish the treatments? Now, some people have argued that, you know what? A better thing could you do than to apply some gentle, extended access distraction over time on healing scar tissue to get it, align better, get it, and not, you know, not form as much in the first place. And to improve the motion of that scar tissue, I can see that argument. But technically, you’re supposed to wait a year after a failed surgery or a year after a compression fracture if you have a pretty decent compression fracture. It’s recommended to wait at least a year before you treat that.
[00:52:26] Dr. Alex Jimenez DC: What about adjusting? Are you adjusting all patients right out of the gate? I’ll get that question a lot.
[00:52:36] Dr. Brian Self DC: So that’s a philosophical question. And if you ask ten different specialists, you’re probably going to get at least five other answers. My personal opinion is I don’t adjust these; I don’t adjust the area that you’re treating. If you’re treating a lumbar disc, I’m not going to adjust the lumbar for probably four or five weeks. I might do activator, arthostem, pro adjuster, or maybe some drop. But the last thing I’m going to do is put the table on their side. Put them in the flexion and then rotate a disc that was injured by flexing it and rotating it in the first place. Now I might adjust their thoracic adjust their cervical spine. But I’m the only thing I’m doing to that lumbar disc is warming it up, and then I’m decompressing it, and then I’m calming everything down, and then I’m stabilizing it with the back brace and telling the patient for the first three to four weeks, don’t do anything. You know, no exercising, no gardening, vigorous labor, and nothing for the first three to four weeks. Just let it calm down, let it heal. And then, at that point, you can start rehab, start your stretches, start your, you know what, all the good stuff that you guys do. Just don’t do it too soon. I talked to many patients who say I did six months of physical therapy, which made this worse, or I saw no improvement. You have been decompressing it for a week and a half, and I’m 90 percent improved. How could that possibly be? You know, we did because we left it alone. We’re taking all the pressure off of it and letting it heal. In contrast, your physical therapist had you ride the bike, walk on the treadmill, and massage it. And they were just constantly irritating it, not letting it heal because that’s what they get paid to do. You know, they get paid to move it. And so, by stabilizing it and letting it heal and then eventually getting into your rehab, in my opinion, you’re going to see a lot better results in the long term.
Back Braces
Dr. Brian Self DC explains how after individuals go through a spinal decompression treatment, to use a back brace to help support the back.
[00:55:09] Dr. Alex Jimenez DC: Good. All right, Doctor. Any other questions while we still have Dr. Self on the call? Speak up if you do.
[00:55:19] Dr. Melissa DC: I have one. Melissa. If the patient isn’t able or willing to purchase one of the Aspen braces with high-quality results, we should look for any typical things in a back brace to stabilize?
[00:55:35] Dr. Brian Self DC: No, the the the cheapest one. That’s a suitable brace. This one here. I love the Aspen Braces. They’re super high quality. They can be a little bit more expensive. I don’t know why you guys pay for the Aspen ones, but this one is called Back Max. And if you call Back Max and Dr. Tom, you could probably even get you an excellent price on these, I mean, they’re probably like 30 to 35 dollars, and they worked with them to develop some hot and cold packs for these two. And so, if it’s a price thing, I would go with this one. And you got the Aspen was a great quality brace, and I think they probably have some hot and cold pack options with that. But if you’re looking for a cost-effective one, that’s still a good brace. I would say this Backs Max one. Also, before I forget, I ran across this week. This one is made by a company called G.T. Simulators. I like this one because it’s like two times the size of anything else that I found. And what I found with a lot of these older patients is anything that you can make more significant. You know, it’s going to be good, but this one is just cool because you can flex it forward and show them the herniation that shoots out and hits that nerve. And then, you know, we’ll take them through with some animations and say, OK, so if we’re compressing it and making that worse, then if we decompress, if we take all the pressure off of that, what the decompression, what is that going to do to this desk right here? Oh, well, it looks like it will suck it back in. Exactly. So you sit and make it worse. We decompress it and create a vacuum effect. Suck it back in. Oh, OK. This would be a long-term fix versus a pill or a shot. So anyway, I don’t make anything off of those models. I just saw that one, and I like that it was so large and looks like an excellent quality one. I know there are a lot of cheaper ones on eBay. I have most of those that I bought like they just fall apart after three or four months.
[00:58:03] Dr. Alex Jimenez DC: So we’ll be out working, and Dr. Self will be working on that flowchart, and all that will help answer a lot of questions on basically everything we talked about today. Dr. Nick, do you have a question? You muted for a second there. But yeah, I was just going to say those back braces. We’ve been using those that Dr. Self just showed you guys for a while. And they’ll send you a like a display as well. It’s just a cardboard display, but it’s pretty well done, and it’s just another piece to add more eyes and more questions to decompression. So it’s just a place to put them on display those braces, so that’s another good thing, too.
[00:58:39] Dr. Brian Self DC: Yeah. I like those braces because they’re supportive, but they’re breathable and small roll-up. They’re not super; they’re restrictive, but not super restrictive. So when patients are traveling with them or, you know, not wanting this big, bulky brace to carry around everywhere, I mean, you can stick it inside a purse with no issues that patients like them because they can, you know, you could long term once they are feeling better, they can golf and those they can do stuff.
Conclusion
Dr. Brian Self DC gives a recap on the advanced benefits of spinal decompression on individuals that are dealing with low back pain.
[00:59:15] Dr. Melissa DC: I had one last question. I’m sorry. Do you have just a one-page handle of the people who think of a sheet that we can give patients we think are candidates for decomp? Kind of just a summary of the who, what, when, where, and when?
[00:59:35] Dr. Brian Self DC: The marketing materials so that you guys should all have, or if you don’t, we’ll get them all over to you for free. There’s a one-page promotional sheet explaining decompression. And then there’s a four-page brochure that’s either specific for herniation and bulges or a degenerative disc. So we kind of group all of our patients into those two categories because your consultation will be based on either having a degenerative disc or having a hernia, then bolting. So if it’s degenerative, we’re pumping the disc, pushing out the toxins, drawing in the proteome glycans and the oxygen and the nutrients to restore the hydrostatic mechanism to make it taller and move better. Your consultation is completely different if it’s a herniated or a bulging desk. What we’re doing is we’re adding some extended access distraction to create a vacuum effect based on the negative millimeters of mercury of pressure to suck it back in. So the four-page brochure that you guys get, you’re either going to have one for a degenerative disc, or you’re going to have one for a herniated or bulging disc. So that’s also a good one to hand out to patients. And then we have like an 18-page brochure. So really, what it comes down to is the printing costs. So obviously, to print an 18-page booklet, you’re not going to want to hand those out to every patient that comes in the door. So all the patients usually get the one-page flier because obviously, that’s going to be a lot cheaper to print now if it’s the absolute perfect patient and they’re going home to try to explain to their spouse what’s going on. I’m going to give them the 18-page brochure because, you know, it’s probably going to be worth it. Or, if I’m mailing one out to a patient, I might give them the 18-page one. But if they’re relatively qualified and I might give them the four-page one to take home because, you know, that might be, let’s say, a dollar fifty to print versus a one-page one that may cost you, you know, twenty-five cents or whatever, fifty cents if you do it in color and then the 18 page one, if they’re pretty highly qualified. So you guys should have access to all of those. We customize all those for your clinic. If you don’t have them, let me know, and I’ll make sure. Jeff Thomas, my graphic designer, usually sends out a link. He’ll customize everything for your clinic, then send you a link. You click on the link, download those brochures, make sure they’re perfect, and send them off to your printer. But to answer your question. There’s a one-page brochure, there’s a four-page brochure, and then there’s an 18-page brochure.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine