Manuel Lozano’s ability to participate in his daily responsibilities was lost after he was involved in an auto accident. Mr. Lozano’s symptoms worsened and took hold of his life. He couldn’t take it anymore and sought treatment. Local El Paso chiropractor Dr. Alex Jimenez treated and restored Mr. Lozano’s health to optimal performance, and he recommends El Paso Back Clinic & Dr. Jimenez for auto accident injuries.
El Paso Back Clinic
We are blessed to present El Paso’s Premier Wellness & Injury Care Clinic to you.
At El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we are passionately focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility, and agility programs tailored for all age groups and disabilities.
We were hoping you could live a life filled with more energy, a positive attitude, better sleep, less pain, proper body weight, and education on maintaining this way of life.
Helping You Heal To Optimal Performance!
Please feel free to subscribe and recommend us if you have enjoyed this video and we have helped you.
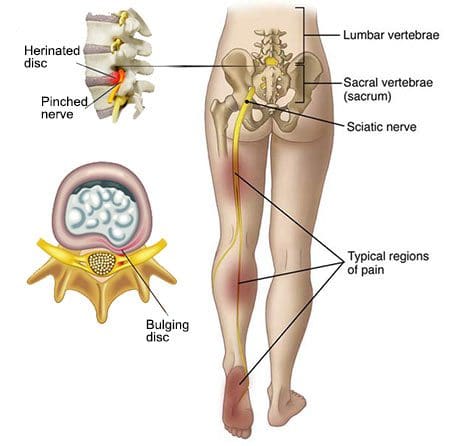
� Sciatica, or sciatic nerve pain, is a collection of symptoms caused by the compression or impingement of the spinal cord and/or nerve roots, due to disk herniation, spinal health issues like osteoarthritis, spondylolisthesis, and spinal stenosis as well as intraspinal tumors and abscesses. Impingement or compression may typically occur along the spinal canal or intervertebral foramen. Health issues associated with the compression or impingement of the spinal cord and/or nerve roots may commonly occur in the lower back, pelvis, or buttocks. � �
Sciatica Symptoms
� The common symptoms of sciatic nerve pain include pain and discomfort which radiates along the lower back, down the buttocks and posterior aspect of the leg, into the knee and foot. The painful symptoms may affect one or both lower extremities and it may occur with or without low back pain. The pain and discomfort are described as burning, lancinating, or stabbing. Other common symptoms of sciatica include tingling sensations and numbness anywhere along the length of the sciatic nerve, particularly in the lower extremities. � Coughing or the Valsalva maneuver, a specific way of breathing which increases pressure in the chest, may worsen sciatic nerve pain symptoms. Moreover, the compression or impingement of the spinal cord and nerve roots can cause sensory, motor, or reflex deficits, among other health issues. Symptoms of sciatica may depend on which nerves are affected based on the segmental level of the spine. By way of instance, an L5 to S1 disk herniation may affect the ankle jerk reflex while an L3 to L4 disk herniation may affect the knee jerk reflex. �
Sciatica, or sciatic nerve pain, is a collection of symptoms rather than a single health issue, characterized by radiating pain, tingling sensations, and/or numbness which extends from the lower back and buttocks, down into the legs and feet. Sciatica is generally diagnosed through its symptoms and depending on the type of painful symptoms, a healthcare professional can safely and effective treat sciatic nerve pain. It’s important for patients to understand the symptoms of sciatica in order to continue with a diagnosis and follow-up with the appropriate treatment option. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
� Healthcare professionals have determined that straight leg raising may aggravate pain and discomfort which radiates down the length of the leg when gradually raised above 60 degrees or less. According to numerous research studies, this outcome measure is sensitive to sciatic nerve pain. Painful symptoms radiating down the affected leg when the contralateral leg is lifted, also known as crossed straight leg raising, is more common for sciatica. Furthermore, sciatica can ultimately be diagnosed through a series of tests and evaluations. � The straight leg raise test can be performed while patients are sitting with their hip joints flexed at 90 degrees. Then, their leg is carefully raised until the knee is fully extended. If the patient has sciatica, the painful symptoms will most often manifest as the leg is extended. The slump test can be performed like the straight leg raise test, but while the patient is slumping with the thoracic and lumbar spine flexed as well as the neck flexed. The slump test is more accurate but less specific, for disk herniation than the straight leg raise test. �
Sciatic Nerve Pain Diagnosis
� Sciatica is commonly diagnosed through its characteristic, painful symptoms. Once sciatic nerve pain is diagnosed, healthcare professionals should test a patient’s strength, sensations, and reflexes to determine any possible health issues. If painful symptoms persist for more than 6 weeks, or if there are neurologic deficits, imaging and electrodiagnostic studies should be performed. Structural and functional abnormalities which result in sciatica, such as spinal stenosis, can most accurately be diagnosed through MRI or CT scans. � Imaging and electrodiagnostic studies can help confirm the segmental level of the spinal cord and/or nerve root compression and/or impingement, which can exclude health issues that may mimic sciatica, such as polyneuropathy. These studies may help determine whether single or multiple regions of the spinal cord and/or nerve roots are being affected and whether the diagnosis correlates with MRI abnormalities. Abnormalities may not be obvious on imaging and electrodiagnostic studies for up to a few weeks after symptoms manifest. �
Sciatica Treatment
� Patients with sciatica, or sciatic nerve pain, can achieve relief from their painful symptoms through bed rest in a recumbent position with the head of the bed elevated about 30 degrees, also known as the semi-Fowler position. Treatment for low back pain can include nonopioid analgesics, such as NSAIDs and acetaminophen. Drugs and/or medications which decrease neuropathic pain, such as gabapentin or other anticonvulsants and low-dose tricyclic antidepressants, may also help relieve sciatic nerve pain, or sciatica, signs and symptoms. � Muscle spasm associated with low back pain or sciatica can be relieved through the utilization of heat or cold, physical therapy, and chiropractic care, among other alternative treatment options. Whether corticosteroids should be used to treat acute radicular pain remains controversial. Epidural corticosteroids can help achieve pain relief, however, these should not be utilized unless the patient’s painful symptoms are severe or persistent. Many healthcare professionals may utilize oral corticosteroids for these special occasions. � Surgery for sciatic nerve pain, or sciatica, is only recommended for cauda equina syndrome or for unequivocal disk herniation along with the presence of muscular weakness, progressive neurologic deficit and/or intolerable, intractable pain which interferes with regular physical activities in an emotionally stable patient which has not decreased after 6 weeks of conservative treatments. The standard procedure for sciatica caused by disk herniation is through classic diskectomy with a limited laminotomy. If the disk herniation is localized, a microdiscectomy may be performed, where the skin incision and laminotomy are smaller. Chemonucleolysis, which uses an intradiscal injection of chymopapain, is no longer utilized to help treat sciatic nerve pain. � Sciatica is a collection of symptoms caused by the compression or impingement of the spinal cord and/or nerve roots. Understanding the symptoms of sciatic nerve pain is essential towards obtaining a diagnosis in order to follow up with the best treatment. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions.
To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
�
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All of the above XYMOGEN policies remain strictly in force.
Approximately 8 out of 10 people will experience sciatica or a sharp electrical surge that painfully runs through the back down to the foot. It can then lead to having numbness in different areas of the back, leg, and foot. Here are two such cases that describe their back pain and their inability to engage in activities. �
Truide discusses how her pregnancy caused her back pain.
Dionicio discusses how truck driving triggered his back pain.
These patients utilized chiropractic care with Dr. Alex Jimenez, DC and are now back on their feet, pain-free and ready to get on with their lives. The El Paso Back Clinic is the place to go for sciatica back pain relief.
El Paso Back Clinic
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities. �
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. �
Only the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us. �
Patients involved in automobile accident injuries discuss how their symptoms affected their well-being. Through the utilization of chiropractic care, these patients describe how Dr. Alex Jimenez, brought them back to their original quality of life.
Chiropractic medicine focuses on the musculoskeletal system, which is what keeps the body in balance. A sudden impact to the body, such as from an auto accident throws the body out of whack. Chiropractic brings it all back together in harmony. These patients give their testimonies and praise Dr. Jimenez as the best injury chiropractor in El Paso TX.
El Paso Back Clinic
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
You may be suffering from sciatica if you have ever experienced a shooting, nerve-like pain down one of your legs. The sciatic nerve can be impacted by a number of different things, including injury and degenerative diseases, that can lead to sciatica. Fortunately, chiropractic can be extremely effective for the treatment of sciatica.
What To Know
The sciatic nerve is a large nerve that travels from the lower back down both of the legs and into the feet. When pressure is placed on the nerve, such as from a herniated disc, it can lead to the symptoms commonly referred to as sciatica.
Shooting pain that travels down from the lower back and through the leg and calf
A feeling of electricity down one leg
Burning pain
Pain from a particular movement, or a jolt � like a sneeze
Numbness
Weakness
Severe symptoms can include trouble controlling the bowels and debilitating pain
Sciatica Causes
Causes of sciatica include:
Vertebrae Misaligned
Misaligned vertebrae, referred to as subluxations in chiropractic, can put pressure on nerves in the spine � including the sciatic nerve.
Herniation
The discs that cushion the vertebrae are made up of a tough outer layer and a softer inner layer. When the outer layer is damaged and the inner layer comes out into the spine, it is referred to as disc herniation.
Often the symptoms of a herniated disc include back pain, as the inner layer of the disc puts pressure on nerves in the spine. A herniated disc can impact the sciatic nerve, leading to sciatica.
Car Accidents
A car accident can easily damage the spine and soft tissues. An auto accident may cause a misalignment of the spine, a herniated disc, or other injuries that cause symptoms of sciatica.
Athletic Injuries
Even the fittest athletes are susceptible to back injuries, which in turn can cause sciatica. The spine and discs can be damaged due to a large impact, repetitive motion injuries, or even twisting the wrong way.
Job Injuries
Many sufferers of sciatica do not realize that their workplace activities � including repetitive motions and sitting in one position for long periods of time � can lead to sciatica.
How Chiropractic Can Help
A study cited by the health magazine Prevention found that sixty percent of sciatica sufferers who failed to get relief from other treatments found their symptoms improved after chiropractic care. In fact, they got the same level of relief as those who went through surgery � without any of the serious side effects that so often come with surgical procedures.
The spinal misalignments that are often the cause of sciatica can be corrected through careful chiropractic adjustments. The chiropractor analyzes the misalignment, then applies specific pressure to the spine to relieve the misalignment. Once the pressure is removed from the sciatic nerve, symptoms improve.
Spine Decompression
For those whose sciatica is caused by a herniated disc, spinal decompression can bring real relief. Using a specially designed table, the chiropractor can gently stretch the spine � creating space for the disc to heal and pull back from the sciatic nerve.
We Give Relief From Sciatica
Please contact our chiropractic team today to schedule an appointment if you are experiencing symptoms of sciatica. We are ready to help you feel better and get back on your feet again.
The sciatic nerve is the largest and longest nerve in the human body. It connects the lower extremities to the central nervous system. Any type of compression or impingement can cause sciatic nerve pain. A herniated disc, misalignment of the spine, and other spinal health issues can cause symptoms of sciatica.
Sciatic nerve pain, or sciatica, is a collection of symptoms characterized by low back pain, tingling sensations, and numbness which radiate down the length of the legs and into the feet. Dr. Alex Jimenez helps many patients from all walks of life find pain relief. Chiropractic medicine specializes in treating sciatica. EP Back Clinic patients give their testimonies, as to how Dr. Jimenez is the best chiropractor for sciatica pain.
EP Back Clinic
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
The sciatic nerve is the largest nerve in the human body and its main function is to connect the feet to the CNS. The painful symptoms associated with sciatic nerve pain, or sciatica, can tremendously affect a person’s quality of life.
Sciatica, or sciatic nerve pain, is caused by the compression of the sciatic nerve, which runs from the low back, down each leg, and into the feet.
Dr. Alex Jimenez focuses on the diagnosis, treatment, and prevention of a variety of health issues associated with the musculoskeletal and nervous systems.
Chiropractic care is an alternative option that utilizes spinal adjustments and manual manipulations to safely and effectively correct any spinal misalignments, or subluxations, which may be causing painful symptoms like sciatic nerve pain or sciatica. Dr. Jimenez is the non-surgical choice.
El Paso Back Clinic
We are blessed to present to you El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend us.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine


 �
�