
Neuropathic pain is a complex, chronic pain condition that is generally accompanied by soft tissue injury. Neuropathic pain is common in clinical practice and also poses a challenge to patients and clinicians alike. With neuropathic pain, the nerve fibers themselves may be either damaged, dysfunctional or injured. Neuropathic pain is the result of damage from trauma or disease to the peripheral or central nervous system, where the lesion may occur at any site. As a result, these damaged nerve fibers can send incorrect signals to other pain centers. The effect of a nerve fiber injury consists of a change in neural function, both at the region of the injury and also around the injury. Clinical signs of neuropathic pain normally include sensory phenomena, such as spontaneous pain, paresthesias and hyperalgesia.
Neuropathic pain, as defined by the International Association of the Study of Pain or the IASP, is pain initiated or caused by a primary lesion or dysfunction of the nervous system. It could result from damage anywhere along the neuraxis: peripheral nervous system, spinal or supraspinal nervous system. Traits that distinguish neuropathic pain from other kinds of pain include pain and sensory signs lasting beyond the recovery period. It’s characterized in humans by spontaneous pain, allodynia, or the experience of non-noxious stimulation as painful, and causalgia, or persistent burning pain. Spontaneous pain includes sensations of “pins and needles”, burning, shooting, stabbing and paroxysmal pain, or electric-shock like pain, often associated with dysesthesias and paresthesias. These sensations not only alter the patient’s sensory apparatus, but also the patient’s well-being, mood, attention and thinking. Neuropathic pain is made up of both “negative” symptoms, such as sensory loss and tingling sensations, and “positive” symptoms, such as paresthesias, spontaneous pain and increased feeling of pain.
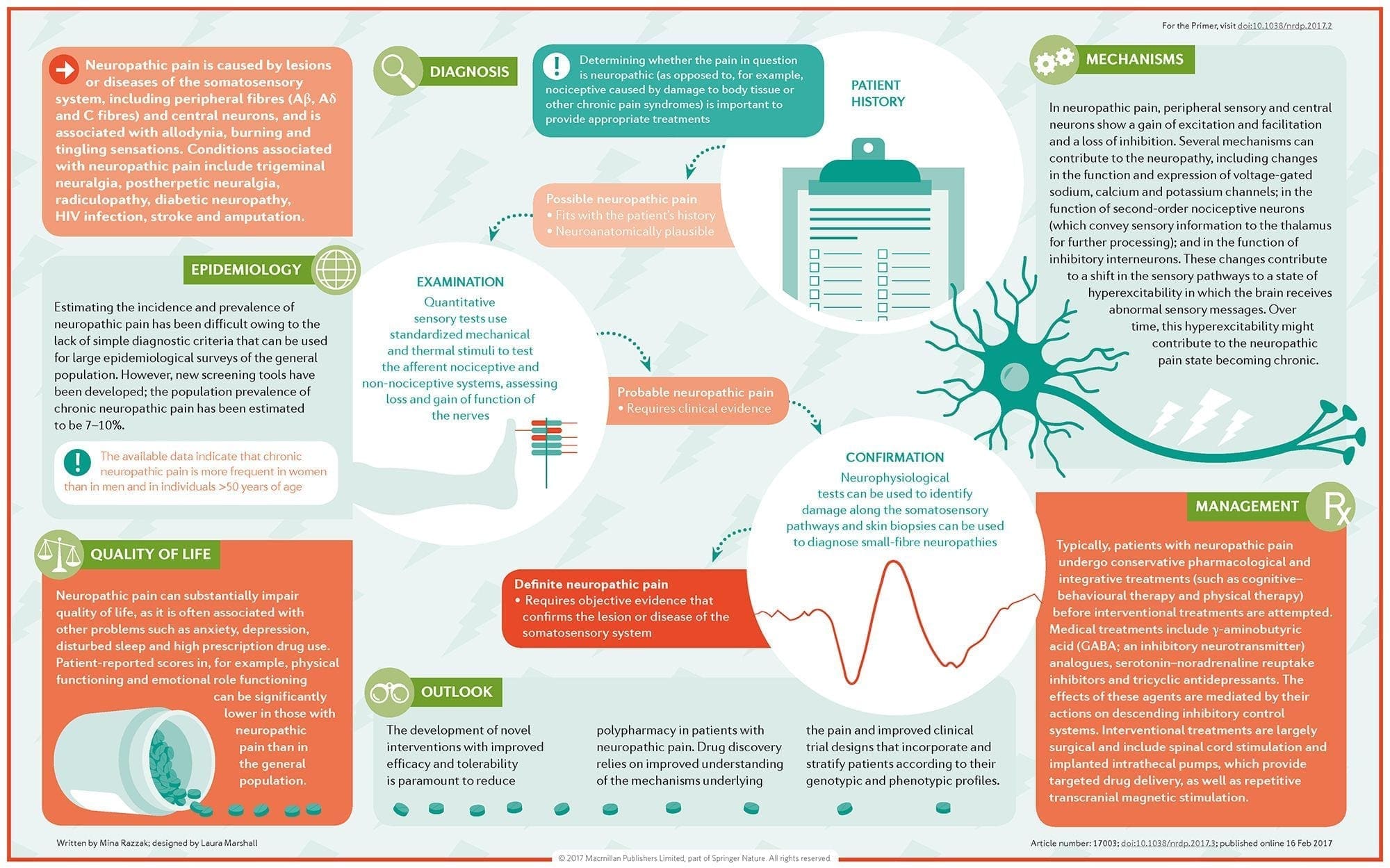
Conditions frequently related to neuropathic pain can be classified into two major groups: pain due to damage in the central nervous system and pain because of damage to the peripheral nervous system. Cortical and sub-cortical strokes, traumatic spinal cord injuries, syringo-myelia and syringobulbia, trigeminal and glossopharyngeal neuralgias, neoplastic and other space-occupying lesions are clinical conditions that belong to the former group. Nerve compression or entrapment neuropathies, ischemic neuropathy, peripheral polyneuropathies, plexopathies, nerve root compression, post-amputation stump and phantom limb pain, postherpetic neuralgia and cancer-related neuropathies are clinical conditions that belong to the latter group.
Contents
Pathophysiology of Neuropathic Pain
The pathophysiologic processes and concepts underlying neuropathic pain are multiple. Prior to covering these processes, a review of ordinary pain circuitry is critical. Regular pain circuitries involve activation of a nociceptor, also known as the pain receptor, in response to a painful stimulation. A wave of depolarization is delivered to the first-order neurons, together with sodium rushing in via sodium channels and potassium rushing out. Neurons end in the brain stem in the trigeminal nucleus or in the dorsal horn of the spinal cord. It is here where the sign opens voltage-gated calcium channels in the pre-synaptic terminal, allowing calcium to enter. Calcium allows glutamate, an excitatory neurotransmitter, to be released into the synaptic area. Glutamate binds to NMDA receptors on the second-order neurons, causing depolarization.
These neurons cross through the spinal cord and travel until the thalamus, where they synapse with third-order neurons. These then connect to the limbic system and cerebral cortex. There is also an inhibitory pathway that prevents pain signal transmission from the dorsal horn. Anti-nociceptive neurons originate in the brain stem and travel down the spinal cord where they synapse with short interneurons in the dorsal horn by releasing dopamine and norepinephrine. The interneurons modulate the synapse between the first-order neuron as well as the second-order neuron by releasing gamma amino butyric acid, or GABA, an inhibitory neurotransmitter. Consequently, pain cessation is the result of inhibition of synapses between first and second order neurons, while pain enhancement might be the result of suppression of inhibitory synaptic connections.

The mechanism underlying neuropathic pain, however, aren’t as clear. Several animal studies have revealed that lots of mechanisms may be involved. However, one has to remember that what applies to creatures may not always apply to people. First order neurons may increase their firing if they’re partially damaged and increase the amount of sodium channels. Ectopic discharges are a consequence of enhanced depolarization at certain sites in the fiber, resulting in spontaneous pain and movement-related pain. Inhibitory circuits might be diminished in the level of the dorsal horn or brain stem cells, as well as both, allowing pain impulses to travel unopposed.
In addition, there might be alterations in the central processing of pain when, because of chronic pain and the use of some drug and/or medications, second- and third-order neurons can create a “memory” of pain and become sensitized. There’s then heightened sensitivity of spinal neurons and reduced activation thresholds. Another theory demonstrates the concept of sympathetically-maintained neuropathic pain. This notion was demonstrated by analgesia following sympathectomy from animals and people. However, a mix of mechanics can be involved in many chronic neuropathic or mixed somatic and neuropathic pain conditions. Among those challenges in the pain field, and much more so as it pertains to neuropathic pain, is the capability to check it. There is a dual component to this: first, assessing quality, intensity and advancement; and second, correctly diagnosing neuropathic pain.
There are, however, some diagnostic tools that may assist clinicians in evaluating neuropathic pain. For starters, nerve conduction studies and sensory-evoked potentials may identify and quantify the extent of damage to sensory, but not nociceptive, pathways by monitoring neurophysiological responses to electrical stimuli. Additionally, quantitative sensory testing steps perception in reaction to external stimuli of varying intensities by applying stimulation to the skin. Mechanical sensitivity to tactile stimuli is measured with specialized tools, such as von Frey hairs, pinprick with interlocking needles, as well as vibration sensitivity together with vibrameters and thermal pain with thermodes.
It is also extremely important to perform a comprehensive neurological evaluation to identify motor, sensory and autonomic dysfunctions. Ultimately, there are numerous questionnaires used to distinguish neuropathic pain in nociceptive pain. Some of them include only interview queries (e.g., the Neuropathic Questionnaire and ID Pain), while others contain both interview questions and physical tests (e.g., the Leeds Assessment of Neuropathic Symptoms and Signs scale) and the exact novel tool, the Standardized Evaluation of Pain, which combines six interview questions and ten physiological evaluations.
Treatment Modalities for Neuropathic Pain
Pharmacological regimens aim at the mechanisms of neuropathic pain. However, both pharmacologic and non-pharmacologic treatments deliver complete or partial relief in just about half of patients. Many evidence-based testimonials suggest using mixtures of drugs and/or medications to function for as many mechanisms as possible. The majority of studies have researched mostly post-herpetic neuralgia and painful diabetic neuropathies but the results may not apply to all neuropathic pain conditions.
Antidepressants
Antidepressants increase synaptic serotonin and norepinephrine levels, thereby enhancing the effect of the descending analgesic system associated with neuropathic pain. They’ve been the mainstay of neuropathic pain therapy. Analgesic actions might be attributable to nor-adrenaline and dopamine reuptake blockade, which presumably enhance descending inhibition, NMDA-receptor antagonism and sodium-channel blockade. Tricyclic antidepressants, such as TCAs; e.g., amitriptyline, imipramine, nortriptyline and doxepine, are powerful against continuous aching or burning pain along with spontaneous pain.
Tricyclic antidepressants have been proven significantly more effective for neuropathic pain than the specific serotonin reuptake inhibitors, or SSRIs, such as fluoxetine, paroxetine, sertraline and citalopram. The reason may be that they inhibit reuptake of serotonin and nor-epinephrine, while SSRIs only inhibit serotonin reuptake. Tricyclic antidepressants can have unpleasant side effects, including nausea, confusion, cardiac conduction blocks, tachycardia and ventricular arrhythmias. They can also cause weight gain, a reduced seizure threshold and orthostatic hypotension. Tricyclics have to be used with care in the elderly, who are particularly vulnerable to their acute side effects. The drug concentration in the blood should be monitored to avoid toxicity in patients who are slow medication metabolizers.
Serotonin-norepinephrine reuptake inhibitors, or SNRIs, are a new class of antidepressants. Like TCAs, they seem to be more effective than SSRIs for treating neuropathic pain because they also inhibit reuptake of both nor-epinephrine and dopamine. Venlafaxine is as effective against debilitating polyneuropathies, such as painful diabetic neuropathy, as imipramine, in the mention of TCA, and the two are significantly greater than placebo. Like the TCAs, the SNRIs seem to confer benefits independent of their antidepressant effects. Side effects include sedation, confusion, hypertension and withdrawal syndrome.
Antiepileptic Drugs
Antiepileptic drugs can be utilized as first-line treatment especially for certain types of neuropathic pain. They act by modulating voltage-gated calcium and sodium channels, by improving the inhibitory effects of GABA and by inhibiting excitatory glutaminergic transmission. Anti-epileptic medications have not been demonstrated to be effective for acute pain. In chronic pain cases, antiepileptic drugs seem to be effective only in trigeminal neuralgia. Carbamazepine is routinely employed for this condition. Gabapentin, which functions by inhibiting calcium channel function through agonist actions at the alpha-2 delta subunit of the calcium channel, is also known to be effective for neuropathic pain. However, gabapentin acts centrally and it might cause fatigue, confusion and somnolence.
Non-Opioid Analgesics
There is a lack of strong data supporting using non-steroidal anti inflammatory medications, or NSAIDs, in the relief of neuropathic pain. This may be due to the lack of an inflammatory component in relieving pain. But they have been utilized interchangeably with opioids as adjuvants in treating cancer pain. There have been reported complications, though, especially in severely debilitated patients.
Opioid Analgesics
Opioid analgesics are a subject of much debate in relieving neuropathic pain. They act by inhibiting central ascending pain impulses. Traditionally, neuropathic pain has been previously observed to be opioid-resistant, in which opioids are more suitable methods for coronary and somatic nociceptive types of pain. Many doctors prevent using opioids to treat neuropathic pain, in large part because of concerns about drug abuse, addiction and regulatory issues. But, there are many trials that have found opioid analgesics to succeed. Oxycodone was superior to placebo for relieving pain, allodynia, improving sleep and handicap. Controlled-release opioids, according to a scheduled basis, are recommended for patients with constant pain to encourage constant levels of analgesia, prevent fluctuations in blood glucose and prevent adverse events associated with higher dosing. Most commonly, oral preparations are used because of their greater ease of use and cost-effectiveness. Trans-dermal, parenteral and rectal preparations are generally used in patients who cannot tolerate oral drugs.
Local Anesthetics
Nearby acting anesthetics are appealing because, thanks to their regional action, they have minimal side effects. They act by stabilizing sodium channels at the axons of peripheral first-order neurons. They work best if there is only partial nerve injury and excess sodium channels have collected. Topical lidocaine is the best-studied representative of the course for neuropathic pain. Specifically, the use of this 5 percent lidocaine patch for post-herpetic neuralgia has caused its approval by the FDA. The patch seems to work best when there is damaged, but maintained, peripheral nervous system nociceptor function from the involved dermatome demonstrating as allodynia. It needs to be set directly on the symptomatic area for 12 hours and eliminated for another 12 hours and may be used for years this way. Besides local skin reactions, it is often well tolerated by many patients with neuropathic pain.
Miscellaneous Drugs
Clonidine, an alpha-2-agonist, was shown to be effective in a subset of patients with diabetic peripheral neuropathy. Cannabinoids have been found to play a role in experimental pain modulation in animal models and evidence of the efficacy is accumulating. CB2-selective agonists suppress hyperalgesia and allodynia and normalize nociceptive thresholds without inducing analgesia.
Interventional Pain Management
Invasive treatments might be considered for patients who have intractable neuropathic pain. These treatments include epidural or perineural injections of local anesthetics or corticosteroids, implantation of epidural and intrathecal drug delivery methods and insertion of spinal cord stimulators. These approaches are reserved for patients with intractable chronic neuropathic pain who have failed conservative medical management and also have experienced thorough psychological evaluation. In a study by Kim et al, it was shown that a spinal cord stimulator was effective in treating neuropathic pain of nerve root origin.

Dr. Alex Jimenez’s Insight
With neuropathic pain, chronic pain symptoms occur due to the nerve fibers themselves being damaged, dysfunctional or injured, generally accompanied by tissue damage or injury. As a result, these nerve fibers can begin to send incorrect pain signals to other areas of the body. The effects of neuropathic pain caused by nerve fiber injuries includes modifications in nerve function both at the site of injury and at areas around the injury. Understanding the pathophysiology of neuropathic pain has been a goal for many healthcare professionals, in order to effectively determine the best treatment approach to help manage and improve its symptoms. From the use of drugs and/or medications, to chiropractic care, exercise, physical activity and nutrition, a variety of treatment approaches may be used to help ease neuropathic pain for each individual’s needs.
Additional Interventions for Neuropathic Pain
Lots of patients with neuropathic pain pursue complementary and alternative treatment options to treat neuropathic pain. Other well-known regimens used to treat neuropathic pain include acupuncture, percutaneous electrical nerve stimulation, transcutaneous electrical nerve stimulation, cognitive behavioral treatment, graded motor imagery and supportive treatment, and exercise. Among these however, chiropractic care is a well-known alternative treatment approach commonly utilized to help treat neuropathic pain. Chiropractic care, along with physical therapy, exercise, nutrition and lifestyle modifications can ultimately offer relief for neuropathic pain symptoms.
Chiropractic Care
What is known is that a comprehensive management application is crucial to combat the effects of neuropathic pain. In this manner, chiropractic care is a holistic treatment program that could be effective in preventing health issues associated with nerve damage. Chiropractic care provides assistance to patients with many different conditions, including those with neuropathic pain. Sufferers of neuropathic pain often utilize non-steroidal-anti-inflammatory medications, or NSAIDs, such as ibuprofen, or heavy prescription painkillers to help ease neuropathic pain. These may provide a temporary fix but need constant use to manage the pain. This invariably contributes to harmful side effects and in extreme situations, prescription drug dependence.
Chiropractic care can help improve symptoms of neuropathic pain and enhance stability without these downsides. An approach such as chiropractic care offers an individualized program designed to pinpoint the root cause of the issue. Through the use of spinal adjustments and manual manipulations, a chiropractor can carefully correct any spinal misalignments, or subluxations, found along the length of the spine, which could lower the consequences of nerve wracking via the realigning of the backbone. Restoring spinal integrity is essential to keeping a high-functioning central nervous system.
A chiropractor can also be a long-term treatment towards enhancing your overall well-being. Besides spinal adjustments and manual manipulations, a chiropractor may offer nutritional advice, such as prescribing a diet rich in antioxidants, or they may design a physical therapy or exercise program to fight nerve pain flair-ups. A long-term condition demands a long-term remedy, and in this capacity, a healthcare professional who specializes in injuries and/or conditions affecting the musculoskeletal and nervous system, such as a doctor of chiropractic or chiropractor, may be invaluable as they work to gauge favorable change over time.
Physical therapy, exercise and movement representation techniques have been demonstrated to be beneficial for neuropathic pain treatment. Chiropractic care also offers other treatment modalities which may be helpful towards the management or improvement of neuropathic pain. Low level laser therapy, or LLLT, for instance, has gained tremendous prominence as a treatment for neuropathic pain. According to a variety of research studies, it was concluded that LLLT had positive effects on the control of analgesia for neuropathic pain, however, further research studies are required to define treatment protocols that summarize the effects of low level laser therapy in neuropathic pain treatments.
Chiropractic care also includes nutritional advice, which can help control symptoms associated with diabetic neuropathy. During a research study, a low fat plant-based diet was demonstrated to improve glycemic control in patients with type 2 diabetes. After about 20 weeks of the pilot study, the individuals involved reported changes in their body weight and electrochemical skin conductance in the foot was reported to have improved with the intervention. The research study suggested a potential value in the low-fat plant-based diet intervention for diabetic neuropathy. Moreover, clinical studies found that the oral application of magnesium L-threonate is capable of preventing as well as restoring memory deficits associated with neuropathic pain.
Chiropractic care can also offer additional treatment strategies to promote nerve regeneration. By way of instance, enhancing the regeneration of axons has been suggested to help improve functional recovery after peripheral nerve injury. Electrical stimulation, together with exercise or physical activities, was found to promote nerve regeneration after delayed nerve repair in humans and rats, according to recent research studies. Both electrical stimulation and exercise were ultimately determined to be promising experimental treatments for peripheral nerve injury which seem ready to be transferred to clinical use. Further research studies may be needed to fully determine the effects of these in patients with neuropathic pain.
Conclusion
Neuropathic pain is a multifaceted entity with no particular guidelines to take care of. It’s best managed using a multidisciplinary approach. Pain management requires ongoing evaluation, patient education, ensuring patient follow-up and reassurance. Neuropathic pain is a chronic condition that makes the option for the best treatment challenging. Individualizing treatment involves consideration of the impact of the pain on the individual’s well-being, depression and disabilities together with continuing education and evaluation. Neuropathic pain studies, both on the molecular level and in animal models, is relatively new but very promising. Many improvements are anticipated in the basic and clinical fields of neuropathic pain hence opening the doorways to improved or new treatment modalities for this disabling condition. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez

Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.

EXTRA IMPORTANT TOPIC: Low Back Pain Management
MORE TOPICS: EXTRA EXTRA:�Chronic Pain & Treatments
General Disclaimer, Licenses and Board Certifications *
Professional Scope of Practice *
The information herein on "Overview of the Pathophysiology of Neuropathic Pain" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a Multi-State board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our multidisciplinary team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those on this site and on our family practice-based chiromed.com site, focusing on naturally restoring health for patients of all ages.
Our areas of multidisciplinary practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is multidisciplinary, focusing on musculoskeletal and physical medicine; wellness; contributing etiological viscerosomatic disturbances within clinical presentations; associated somato-visceral reflex clinical dynamics; subluxation complexes; sensitive health issues; and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and licensure jurisdiction. We use functional health & wellness protocols to treat and support care for musculoskeletal injuries or disorders.
Our videos, posts, topics, and insights address clinical matters and issues that directly or indirectly relate to our clinical scope of practice.
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies upon request to regulatory boards and the public.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez, DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Multidisciplinary Licensing & Board Certifications:
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License #: TX5807, Verified: TX5807
New Mexico DC License #: NM-DC2182, Verified: NM-DC2182
Multi-State Advanced Practice Registered Nurse (APRN*) in Texas & Multi-States
Multi-state Compact APRN License by Endorsement (42 States)
Texas APRN License #: 1191402, Verified: 1191402 *
Florida APRN License #: 11043890, Verified: APRN11043890 *
Colorado License #: C-APN.0105610-C-NP, Verified: C-APN.0105610-C-NP
New York License #: N25929, Verified N25929
License Verification Link: Nursys License Verifier
* Prescriptive Authority Authorized
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)
(Licensed Medical Doctor)
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Licenses and Board Certifications:
MD: Medical Doctor
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)*
(Licensed Medical Doctor)*
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933






