Cyrex Laboratories is an advanced clinical laboratory that specializes in the functional approach in environmentally induced autoimmunity.� Cyrex works with the leading experts in medical research and provides arrays that address the cross-connections throughout the body systems. In addition to this, Cyrex�strives to deliver the best quality for the patients by always improving and using the most accurate and advanced technology.
Arrays
Cyrex has multiple arrays they use to test patients depending on their symptoms. These arrays range from Alzheimer�s to Joint auto-immune reactivity screenings. Often times, patients who have issues with their joints or headaches and pain, can be traced back to an underlying issue. When a patient comes to a doctor, the practitioner will evaluate and assess the patient based on the symptoms they bring.� From here, the practitioner can go to Cyrex and order the arrays that best suit their patient�s needs. The Cyrex system revolves around immune function and measures the identifiers that can affect multiple tissues in the body, including the brain, heart, pancreas, nervous system, liver, gastrointestinal system, bones, and joints.� The turn around time for these labs is fairly quick and helps highlight the underlying route of the patient�s symptoms.
Cyrex arrays use serum (a blood draw) as their main form of testing. No matter the array the doctor orders, the patient will receive the same kit. The requisition form that is inside the kit is what matters to the phlebotomist and lab as this is where the array ordered will be marked.
The kit is a small box labeled Cyrex Laboratories, Serum Collection Kit. On top of the kit held in place by a rubber band will be a shipping label and bag for the sample to go in once collected. Inside the kit is a smaller styrofoam box that includes a serum separator tube, a serum transport tube, tube labels, a biohazard bag, and collection instructions.
As one can see from the above photo, the different arrays test for different reactions/conditions. A doctor may order one or multiple arrays depending on the patient.
Array 2 is one of the most popular, as leaky gut is a condition that affects most Americans. This test screens for IgG, IgA, and IgM of Lipopolysaccharides and Occludin/Zonulin.
Integrative Testing
Often times, practitioners will use multiple lab companies on one patient. This is not because one is superior to the other, but rather because they specialize in different areas. Even though the doctor may order labs from different companies, it is in the patient�s best interest because it allows the practitioner to view multiple areas to truly understand the underlying issue.
Patients who come in with symptoms like aching joints, headaches, trouble falling asleep, difficulty staying asleep, leaky gut, and brain fog will certainly benefit from using multiple lab companies.
Using Cyrex array 2 and DUTCH + CAR the patient will get extremely accurate information in regards to what is occurring in their body. The Cyrex array test will show the practitioner if the patient has a leaky gut and how severe. While the DUTCH + CAR allows the doctor to determine the cortisol patterns in the individual�s body. Sometimes, these levels are not rising and falling at the right times, causing the patient to be tired or having trouble staying asleep.
The patient�s health should always come first, and when doctors are knowledgable enough to use more than one lab, the patient benefits are outstanding. By using the companies together, the doctor is able to check multiple areas, leaving no guesswork when it comes to a treatment protocol. However, it is important to remember that labs vary on patient needs. Some patients are able to use the same company for all labs and obtain the accurate results they need.
Cyrex tests for many conditions and has multiple arrays. Although many
Cyrex labs are a great tool for practitioners and health coaches to use! By using these arrays, it helps the practitioner not only treat the symptoms, but it allows them the insight they need to treat the problem at the route source. The tools that Cyrex provides go a long way in evaluating the complex disorders the human body may have. By using Cyrex and coupling it with other tests from DUTCH or labrix, the patient is able to get proper treatment and get back to the hobbies they used to love and enjoy. These companies are all fantastic and provide specialities in different areas. By using more than one company, the pateint truly gets the best results and the doctors are able to construct a solid treatment protocol with all of the information obtained.�� Kenna Vaughn, Senior Health Coach�
*All information was obtained from Cyrex.com
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Physical therapists or PT’s are healthcare professionals that help treat/rehabilitate patients of all ages with various types of injuries.
Personal
Work
Sports
Auto Accidents
A primary care physician, physiatrist, orthopaedist, spine surgeon, or neurosurgeon may refer an individual to a physical therapist as part of a non-surgical�treatment plan.
A physical therapy program may be an integral part of your after-care following surgery.
Some treatments are done prior to active therapeutic exercise.
Conditions therapists treat
Sciatica
Whiplash
Rheumatoid arthritis
Degenerative disc disease
Spondylosis (spinal arthritis)
Post spine surgery therapy
Therapists want to help patients rebuild strength, flexibility, and endurance after any type of intense surgery, as well as help with any specific physical necessities related to post-surgery.
Team Care
Therapists often work directly for or with a doctor/chiropractor to coordinate a treatment plan.
A doctor may send the therapist:
Diagnosis
Current medications
Imaging/scan results
During the consultation, the physical therapist talks about medical history, diagnosis, and symptoms.
This can include:
Conditions
Medications being taken
Diet
Supplements
Type of Pain like:
Acute
Chronic
Episodic
The location of the pain that will also include:
Severity
Type
Factors that decrease or increase pain
Training
Physical therapists have completed an accredited physical therapy program and passed a required state licensing examination.
Therapists graduate with a Doctor of Physical Therapy (DPT) degree.
The American Board of Physical Therapy Specialties through a series of classes/tests therapists can become board-certified specialists in specific areas like:
Orthopedics
Pediatrics
Geriatrics
Sports
These are just a few, but there are many areas of specialization.
Physical Therapist
Many states allow individuals to go to a physical therapist without a referral from a doctor.
Definitely ask your doctor for a recommendation, but also think about what you want in a therapist.
Male or female physical therapist, which is right for you
Take Charge
Physical therapists are valuable healthcare professionals and members of the medical community.
Physical therapy can be challenging but don’t let that get you down, because they will help get you back to optimal health, along with building a stronger, healthier body.
Whiplash Massage Therapy El Paso, TX Chiropractor
Physical therapist Sandra Rubio describes how whiplash-associated disorders resulting from an automobile accident can cause symptoms of neck pain.
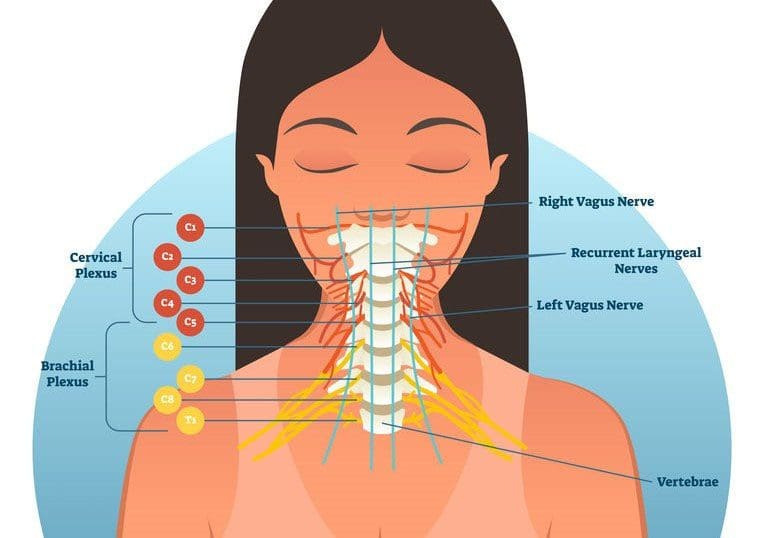
An injury to the cervical spine can damage the complex structures of the neck, including:
Vertebrae
Intervertebral discs
Soft tissues
Tendons
Ligaments
Muscles
Neck pain can come from various structures in the neck including vascular, nerve, airway, digestive, and musculature or it can originate from other areas of the human body.
Most cases can be treated with assistance or using self-help suggestions and techniques.
NCBI Resources
Physical therapy includes both active and passive treatments. Passive treatments help to unwind the body and the physique. As an individual does not need to actively participate, they�re known as passive. A physical treatment program may begin with treatments that are passive, but the goal is to get into treatments that are more active.
A look at what a stinger or burner injury is and what they can do to the neck and shoulders. We will look at:
Symptoms
Treatment
Prevention
Contact sports, like:
Football
Hockey
Soccer
Basketball
This is a very common cervical injury that affects the neck and upper body. This is known as a stinger.
A stinger can also be called a burner and is an injury that happens when the head or neck gets hit to one side, which causes the shoulder to be pulled in the opposite direction.
Stingers/burners often happen at the high school level but can occur at all levels of play.
Stinger/Burner neck injury cause
A stinger is caused by stretching the brachial plexus nerves.
These peripheral nerves that come out of:
Spinal cord
Run across the shoulders
Under the collarbone
Into the arms
The brachial plexus nerves give the arms their strength and sensation.
When a sideways hit to the head or hit to the shoulder occurs, the nerves can become:
Compressed
Stretched
Irritated
Symptoms of a cervical stinger
This type of sideways collision causes immediate and intense pain, tingling or burning sensations that can run down the arm into the fingers.
Weakness in the affected arm or hand is common.
The weakness, numbness, and tingling sensations can last a few minutes or for a few weeks.
Stinger/burner injury treatment
Fortunately, most stinger injuries heal on their own with rest and relaxation of the neck muscles.
Athletes are placed on the disabled list until symptoms are gone and a doctor has cleared the athlete.
Players can return to sport once the pain is gone and they’ve regained:
Full range of motion
Strength
Normal sensation in neck and arms
Constant or recurring symptoms could indicate a more serious injury.
Cervical x-rays, a CT scan, or MRI could be used to rule out other conditions with similar symptoms.
Can stinger/burner injuries be prevented?
Strengthening exercises for the neck muscles are an important way for athletes and beginners to help prevent these injuries.
Using the proper and correct technique in contact sports to avoid spearing/spear tackles and head down tackling.
Safety equipment, like neck rolls, can help limit the backward movement of the neck.
Players who experience stinger symptoms should immediately report it to their coaches or team/personal physician.
Ignoring or playing through a stinger injury can lead to more severe injuries.
*Neck* Pain Chiropractic Care | El Paso, Tx
Following a balanced diet along with healthy lifestyle habits can help promote optimal health and wellness.
People with neck pain realize how much their symptoms affect their ability to engage in everyday activities.
Dr. Alex Jimenez helps patients achieve neck pain relief through chiropractic care, an alternative treatment option that carefully corrects any spinal misalignments or subluxations.�
NCBI Resources
Stretching is an outstanding complement to chiropractic care.
Blood flow to the muscles is increased, helps lower the risk of injury and improves performance.
Stretching is good for the joints, it helps them function through their full range of motion.
The discs that cushion the vertebrae are made up of a tough outer layer and a softer inner layer. When the outer layer is damaged and the inner layer comes out into the spine, it is referred to as�disc herniation.
Often the symptoms of a herniated disc include back pain, as the inner layer of the disc puts pressure on nerves in the spine. A herniated disc can impact the sciatic nerve, leading to sciatica.
If you know that your sciatica was caused by a herniated disc then try these exercises and stretches to help reduce back and leg pain.
Exercises that help relieve sciatica from a herniated disc
If your spine specialist or chiropractor informed you that a herniated disc is what caused the pain also known as lumbar radiculopathy they may recommend� three sciatica exercises:
Prone on elbows into Press-up
Upper back extension
Opposite arm and leg extension
These stretches can help provide relief when the root cause of sciatica from herniated or bulging disc.
Prone Elbows/Press-Up
This exercise is to ease sciatica from herniated disc pain and pressure in the lumbar spine/low back.
How to:
Lay on stomach
Slowly push up until rested on forearms
Beginners hold for 30 seconds
Once strength is gained and you feel comfortable then hold for 3 to 5 minutes
Gently lower to the floor
Repeat 10 times
Once comfortable holding for 5 minutes then perform an extended arms version, which is like push-ups raising your arms to the point where your elbows lock
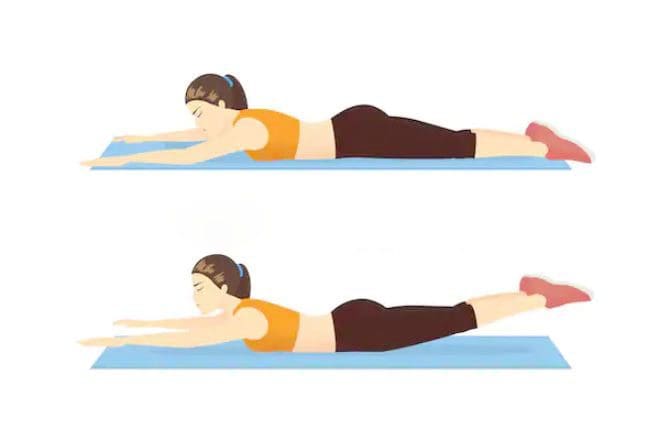
Upper Back Extension
This exercise is to strengthen and stabilize the low back muscles.
How to:
Lay on your stomach with a small pillow or rolled towel under your hips
Rest your arms at your sides
Slowly lift your upper body up off the floor, contracting your low back muscles as you rise
Hold the lifted position for 3 seconds
Slowly lower your body to the ground
Repeat 10 times
Throughout this exercise, keep movements fluid and controlled.
Opposite Arm and Leg Extension
This exercise is to stabilize your spine and strengthen your low back, hamstring and gluteus muscles.
How to:
Lay on your stomach with a small pillow or rolled towel under your abdomen
Extend both arms in front of you
Contract your abdominal muscles as you slowly lift both your right arm and left leg
Hold for 3 seconds. Lower your leg and arm down
Repeat with your left arm and right leg
Hold for 3 seconds
Repeat the exercise 5 to 10 times on each side
As you alternate the lifts, make sure to keep abdominal muscles contracted to get the full benefit.
How do these exercises relieve sciatica from herniated disc
These exercises and stretches are designed to move the pain from the leg and into the low back.
This is centralization/localization.
This is a good thing, as the goal is to get the pain centralized and back at the source.
When the leg pain goes away, it means the pressure on the sciatic nerve and related nerves has been removed.
If sciatic pain stretches down to the foot, you will feel these exercises, meaning that the pain and electrical sensations will move through the ankle and knee. Which means you’re doing it correctly.
This does not mean that the pain is immediately going to centralize to the low back, it does take time because you are trying to stretch and straighten out this long nerve.
But you will notice sciatica pain does not go as far down the leg.
Therefore�these exercises need to be done consistently and be made a part of your routine.
What to know before exercising
Before starting these stretches, consider three recommendations:
Get a doctor�s approval
A spine specialist should clear you to perform these stretches and exercises before you start.
While these exercises are safe, get a doctor�s permission before starting physical activity.
Know the cause so your exercise program helps and not makes the condition worse
Sciatica from herniated disc means a different type of exercise than sciatica caused by piriformis syndrome.
Knowing this information will help you choose an exercise plan that provides maximum relief.
Don�t push too hard
Don’t aggravate sciatica, listen to your body and go slow.
Experience any pain or symptoms:
Weakness
Tingling
Numbness
Contact a spine specialist immediately!
Sciatic nerve pain caused by a herniated or bulging disc is a common problem.
But incorporating these exercises and stretches can provide sustained relief.
The sciatic nerve is a large nerve that travels from the lower back down both of the legs and into the feet. When pressure is placed on the nerve, such as from a herniated disc, it can lead to the symptoms commonly referred to as sciatica.
The sciatic nerve can be impacted by a number of different things, including injury and degenerative diseases.
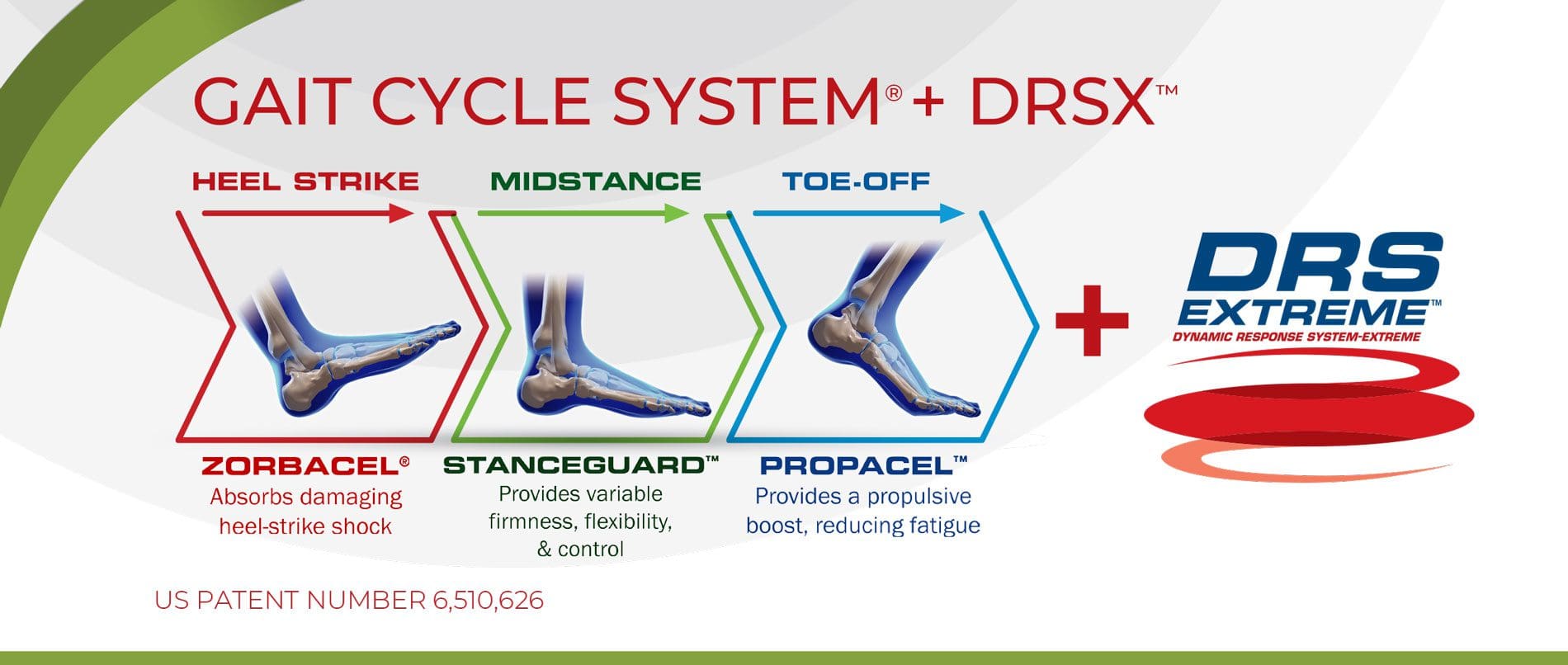
Difference Foot Orthotics Make to *REDUCE FOOT PAIN* & Correct Posture | El Paso, TX (2019)
Custom made foot orthotics can help control foot motion and posture. Healthcare professionals prescribe custom foot orthotics to help patients focus on their foot posture and mobility control. Research studies have ascertained that using custom foot orthotics for posture and mobility control can help fix excessive foot pronation and supination to prevent a variety of foot health problems. The subsequent video describes how custom foot orthotics will help control foot posture and mobility to improve health and wellness.
NCBI Resources
Sciatica is a common back ailment that affects approximately 1 in 10 adults in the United States. It is most prevalent in people between the ages of 25 and 45. Sciatica is characterized by a shooting pain that originates in the lower back and travels down through the hip, buttock, and back of the leg.
The pain can be so severe that it inhibits mobility and can prevent people from working, taking care of their homes, or just enjoying their life. Traditionally, doctors have treated the condition with medications and some invasive therapies, but chiropractic treatments have been found to be extremely effective in alleviating the pain and curing the condition.
Pilates or yoga can work wonders and always stretch before physical exercise.
Get fit – no regular physical activity can lead to serious conditions and possibly chronic pain.
Exercise benefits all, even some light walking around the neighborhood is enough. Just get moving!
Playing a sport could be a way to keep active. Remember, in order for any exercise to work is that it is done regularly.
Strength training is important, just as its name implies strength training builds muscle and reduces muscle imbalances.
It�s never too late to increase strength and flexibility.
Look at activities that you and your friends/family can enjoy and make doing them a regular thing.
A�chiropractor�is the ideal�medical professional to consult with for any unexplained pain in the musculoskeletal system. They are highly qualified professionals that their specialty is treating conditions like lower back pain and they are very affordable. If you or a loved one have pain in the lower back, give us a call. We�re here to help!
Understand *FOOT PRONATION* & How to Correct it with Orthotics | El Paso, TX (2019)
Foot pronation is the natural movement that occurs during foot landing while walking or running. Foot pronation also occurs while standing, and in this instance, it is the amount in which the foot rolls inward toward the arch. Foot pronation is normal, however, excessive foot pronation can cause a variety of health issues, including bad posture. The following video describes the 5 red flags of excessive foot pronation, which can ultimately affect a person’s overall health and wellness. Dr. Alex Jimenez can help diagnose and treat excessive foot pronation. Patients recommend Dr. Alex Jimenez and his staff as the non-surgical choice for excessive foot pronation health issues.
Back pain and everything that comes with it can really take you out of it. It, being life, that you don’t get to participate in, because you have to anticipate how, whatever the activity may be, is going to affect your back. So you just skip activities altogether. No more! You have options and chiropractic care is one of them. Because back pain can occur due to a variety of health issues, diagnosis is essential to create the correct treatment plan.
Doctor of chiropractic Alexander Jimenez specializes in treating back pain. A few patients share their back pain experiences and how it affected their lives. They describe how Dr. Jimenez has helped them improve their overall health and wellness with chiropractic care. Patients highly recommend Dr. Jimenez and his staff as the back pain specialist.
El Paso Back Clinic
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
We Are Ready To Get You Back To Normal Life!
Low Back Pain & Your Feet
The feet are the foundation of the body; they support its weight. If there is not enough support, various parts of the body, especially the spine become exposed to added stress, this can lead to:
Back, hip, knee and foot pain
Poor posture and abnormal foot movement
Sports performance compromised
Greater risk of injury
An abnormal walk leads to imbalances throughout the knees, ankles, and feet, and can eventually cause pain throughout the body, and yes you guessed it the back.
Foot Levelers Kiosk
The Kiosk helps guide patients in selecting the best custom-made orthotics for their condition and lifestyle. It’s�
Fast:�Push the Start button and the scanner begins.
Easy to use:�User-friendly easy touch screen.
Engaging:�Videos explain the importance of healthy feet and the benefits of custom-made orthotics.
Cloud-based:�Results can be securely accessed from anywhere.
Comprehensive:�Easily retrieve previous scans to compare them to new scans and see the difference.
The Foot Levelers Kiosk helps you. It saves time so you can spend more time living your life.
Intake Form
This is the intake form that is used to set up a custom orthotics treatment plan.
Low Back Pain
When there are problems with the feet, it can cause problems through the legs and all the way to the spine. This can cause the ankle to pronate, meaning it rolls inward. This alters the way the�bones of the foot�line up which extends through the tibia, or shin bone.
The spine is the foundation for the body, supporting the spinal cord and the limbs. When there is a problem with any of the limbs it can affect the spine and vice versa. The intricate network of tendons, ligaments, and nerves work together within the incredible machine that is the human body.
When you visit a doctor office for a medical concern, the healthcare professional will perform a variety of diagnostic procedures to determine the source of your symptoms. The doctor will review the patient’s current symptoms and medical history as well as the patient’s results from a physical evaluation to diagnose an injury and/or underlying condition. �
Once the healthcare professional has reviewed the patient’s current symptoms, medical history, and results from the physical evaluation, the doctor will make a list of the probable injuries and/or underlying conditions which may be causing the patient’s symptoms. This is the differential diagnosis. A differential diagnosis refers to the process of differentiating between two or more health issues which share similar signs and symptoms. The doctor will perform additional tests or assessments to rule out specific injuries and/or underlying conditions in order to reach a final diagnosis and follow-up with treatment. �
The differential diagnosis generally varies depending on the health issue. A variety of health issues can cause common symptoms which may make it challenging to determine the source of the pain and discomfort. Sciatica is a collection of symptoms rather than a single condition which can be a frequent symptom for many health issues. Sciatica is characterized as pain, tingling sensations, and numbness, due to compression or impingement along the length of the sciatic nerve. �
Sciatica
The characteristic symptoms of sciatica can range from mild to severe where the sciatic nerve pain is described as a dull ache to pain or as a sharp, searing, or electric-like pain. Symptoms differ from one person to another. By way of instance, some people may experience shooting pain while some people may only experience tingling sensations and/or numbness. � The common symptoms of sciatica, also known as sciatic nerve pain, include: �
Radiating pain along the length of the sciatic nerve
Discomfort, tingling sensations, and numbness
Muscle weakness in the lower back, hips, legs, and feet
A combination of pain, discomfort, tingling sensations and numbness
Painful sensations on one or both sides of the human body
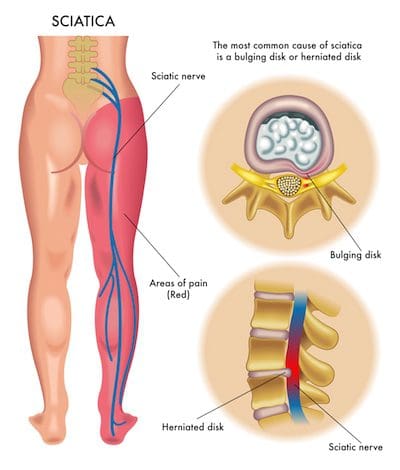
Sciatica commonly occurs when an underlying health issue results in the compression or impingement of the sciatic nerve in the lower back. A bulging or herniated disk is one of the most common causes of sciatica. However, a variety of other underlying health issues can cause sciatica and determining what causes sciatica is necessary for proper treatment. In part 1 of this article, we will demonstrate the differences between sciatica and other health issues with similar painful symptoms. �
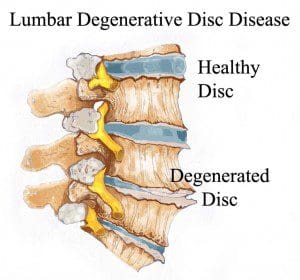
Degenerative Disc Disease
The intervertebral discs also referred to as spinal discs or intervertebral fibrocartilage, provide the padding required between the vertebrae of the spine. The intervertebral discs are an elastic structure made from fibrocartilage tissue. The intervertebral discs cushion the stress of the spine, bears weight, and also helps the spine bend and flex. �
As people age, repeated daily stresses on the backbone and occasional trauma and/or injuries, including minor, undetected health issues, may ultimately damage the intervertebral discs in the back. Changes caused by damage may include: �
Decreased fluid: The intervertebral disks of a healthy young adult are made up of around 90 percent fluid. With age, the fluid material decreases, causing the disc to become thinner. The distance between each vertebra, in turn, becomes smaller and it makes them even less effective to function as a cushion or shock-absorber.
Disc structure: Small tears or cracks can become larger in the outer layer of the disc. The soft and gelatinous material from the inner part may push through the disc, causing a bulging or ruptured disc. The disc may break into fragments.
If the vertebrae have less padding between them, the backbone also becomes less stable. To compensate, the human body builds osteophytes, or bone spurs, small bony structures which develop along the edge of bones. These structures can compress or impinge the spinal cord or nerve roots. These changes can cause painful symptoms and lead to fatigue. �
The pain and discomfort can range from mild to severe and it may often be debilitating. It may result in osteoarthritis along with pain and stiffness. When degenerative disc disease affects the low back or the lumbar spine, the pain may radiate down the buttocks, hips, and thighs, into the knees and feet. There might also be tingling sensations and numbness, the collection of symptoms known as sciatica, caused due to the compression or impingement of the sciatic nerve. �
Radiculopathy
The spine consists of 33 bones, best known as vertebrae, which shield the spinal cord from experiencing injury or trauma. Each vertebra is cushioned from each other with an intervertebral disk. This shields the vertebrae from rubbing over each other. When trauma or injury does occur, these intervertebral discs can become damaged and cause the compression or impingement of a nerve. Depending on which nerve is compressed, an individual can experience a variety of painful symptoms, including sciatica or sciatic nerve pain. Individuals can also develop radiculopathy seemingly without a cause. � Radiculopathy can ultimately develop due to a variety of injuries and/or aggravated conditions, including: �
Herniated discs, or when a disc protrudes, irritating the nerve root
Sciatica
Degenerative disc disease
Bone spurs
Tumors in the spine
Osteoarthritis or spinal arthritis
Spinal stenosis, or the narrowing of the spinal canal
Compression fractures
Spondylolisthesis, or when a vertebra slides over the vertebra beneath it
Scoliosis brought on by an abnormal curve in the backbone
Diabetes, caused by altered nerve blood flow
Cauda equine syndrome, or a condition where nerve root compression affects the pelvic organs and lower extremities
� Additional risk factors for developing radiculopathy include: � �
Aging
Being overweight or obese
Poor posture
Improper lifting methods and techniques
Repetitive movements
A family history of degenerative bone health issues
Individuals may experience painful symptoms in the low back, hips, and legs when nerve compression or impingement occurs in the lumbar spine or low back region of the spine. Lumbar radiculopathy is also commonly referred to as sciatica or sciatic nerve pain. Sciatica symptoms include pain, tingling sensations, and numbness along the length of the sciatic nerve. Occasionally, the nerve roots in charge of controlling the bowel and bladder may become irritated, resulting in bowel or bladder incontinence as well as loss of control. Other generalized symptoms associated with lumbar radiculopathy include: �
Sharp pain extending from the low back to the foot
Sharp pain with sitting or coughing
Weakness or numbness in the lower extremities
Tingling sensations and numbness in the lower extremities
Hypersensitivity, or sensitivity and reflex alterations
Sharp pain radiating into the upper extremities
Intense pain and discomfort with movements of the head and/or neck
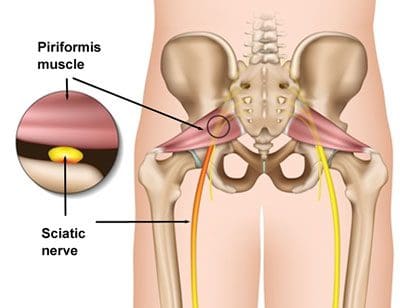
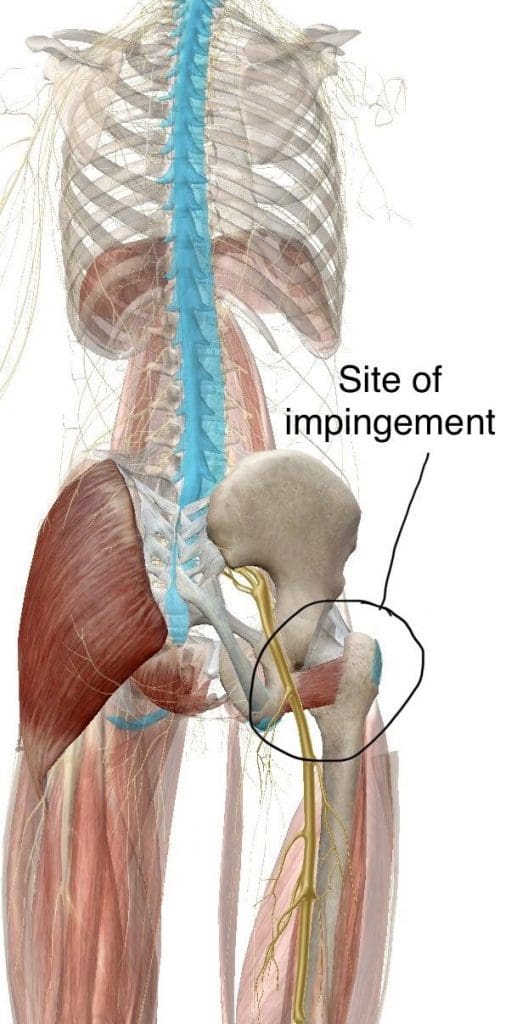
Piriformis Syndrome
People with sciatic nerve pain, or sciatica, will often report experiencing pain and discomfort, tingling sensations, and numbness anywhere along the length of the sciatic nerve. The sciatic nerve is the longest and largest nerve in the human body, which travels from the lower back into the hip and buttocks, down into the thighs, knees, legs, and feet. People with sciatica, or sciatic nerve pain, may also experience another common health issue known as piriformis syndrome. � �
Piriformis syndrome can cause sciatica when a piriformis muscle spasm irritates the sciatic nerve. The piriformis is a muscle which extends from the front of the sacrum, the triangle-shaped bone between the two hipbones in the pelvis, across the sciatic nerve and into the top of the femur, the large bone in the upper leg. When an injury or underlying condition causes the piriformis muscle to compress or impinge the sciatic nerve due to inflammation, the end result is piriformis syndrome. �
Sciatica is the most common symptom associated with piriformis syndrome. Other common symptoms associated with piriformis syndrome include tingling sensations and numbness, muscle tenderness, pain and discomfort while sitting or engaging in physical activities, and difficulty sitting comfortably. The pain and discomfort will generally manifest on one or both sides of the hips, buttocks, and thighs, where it will then radiate down the back of the leg, knees, and feet. �
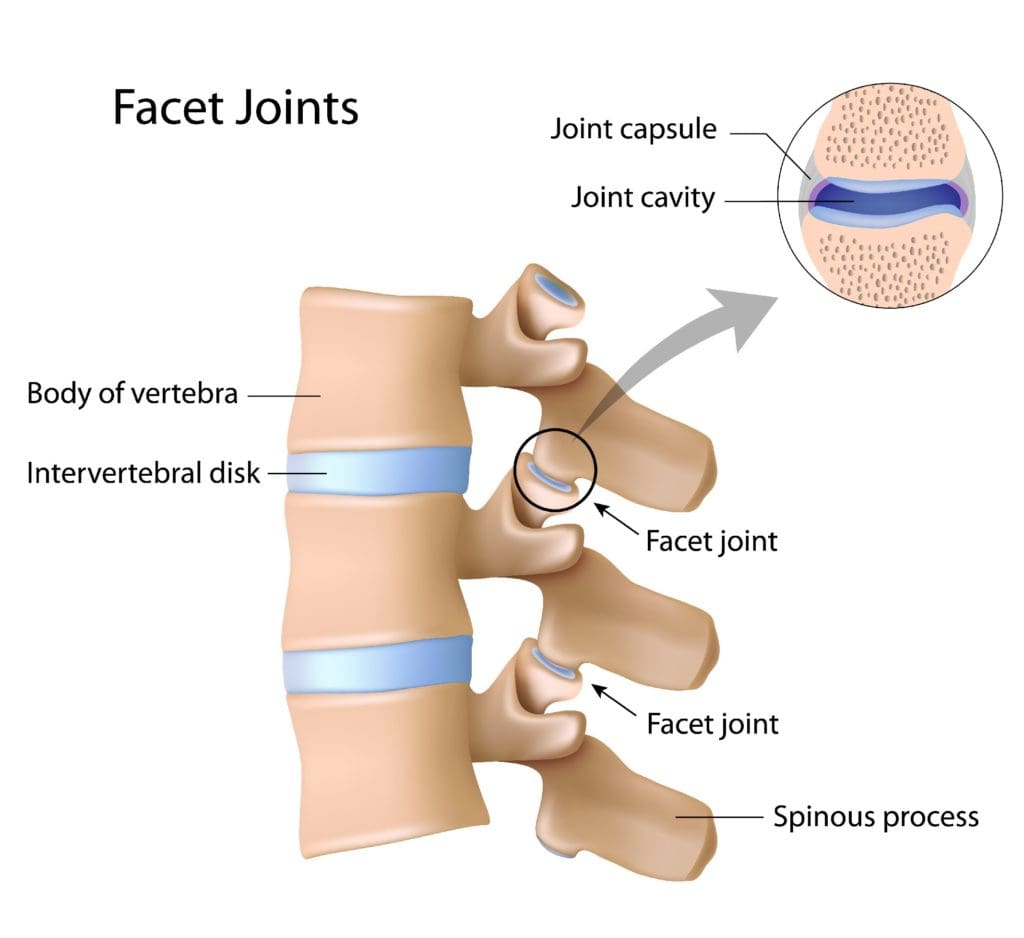
Facet Arthropathy
The facet joints are the joints which are found behind the spine to counterbalance the intervertebral discs found between the vertebrae of the spine. Over time, the natural aging process can cause the facet joints to deteriorate or wear down, causing facet joint arthritis or facet arthropathy. Individuals with facet arthropathy will experience low back pain as a dull ache on one or both sides of the lower back or lumbar spine which can worsen with standing, twisting, or bending backward. �
However, unlike the well-known signs and symptoms of sciatica, caused by the compression or impingement of the sciatic nerve in the lower back, facet arthropathy signs and symptoms generally don’t radiate down the buttocks, hips, and thighs, or into the legs and feet. However, the facet joint, in the same way as any other joint which has arthritis, can also become enlarged and add pressure on nerve roots, causing pain and discomfort to radiate down into the lower extremities. �
Facet arthropathy may cause bone spurs, tiny bone outgrowths. Bone spurs can decrease the distance available between nerve roots, causing a health issue known as spinal stenosis. Spinal stenosis may cause pain, weakness, and numbness on the buttocks, hips, and thighs. It’s frequently associated with other health issues which could lead to facet arthropathy. The natural aging process is frequently considered to be one of the most common indirect sources of facet arthropathy. Other health issues which can ultimately affect the facet joints and cause facet arthropathy include: � �
Osteoarthritis: Degeneration of joint cartilage and underlying bone, generally during middle age
Facet joint degeneration: Wear and tear on the facet joint brought on over time due to aging
Facet joint injury: Trauma to the facet joints caused by an impact, such as a fall or automobile accident
Synovial cyst: A fluid-filled sac which develops in the spine, generally as a result of aging
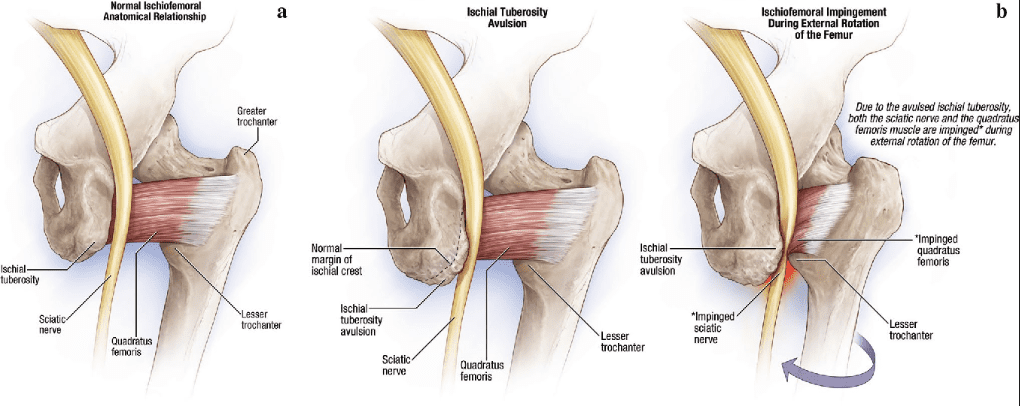
Ischiofemoral Impingement
Ischiofemoral impingement syndrome is a condition which occurs when the ischium and the head of the femur experience excessive amounts of pressure, generally due to trauma, overuse, or surgery. The trauma, overuse, or surgery, can also cause bone spurs to grow along the ischium. This gives the bones an abnormal shape which makes them no longer fit together. �
Because these don�t fit properly together anymore, the bones may then start to rub against each other during movement causing friction which can damage the joint and cause painful symptoms. As friction worsens, the pain may also increase and restrict movements. The symptoms for ischiofemoral impingement may vary and treatment can also depend on symptoms. �
�
The main symptom of ischiofemoral impingement syndrome is hip pain. The pain from this underlying health issue may start off as mild, however, it can often worsen as the rubbing of the bones causes more damage and inflammation. Ischiofemoral impingement syndrome can feel similar to a pulled hamstring but the pain is generally closer to the buttocks like sciatica. �
Ischiofemoral impingement occurs due to excess friction between the top of the thighbone, or the femur, and the hip bone, or the ischium. These two bones generally touch in a way which allows them to move without causing pain, however, trauma, overuse, and surgery can ultimately damage the bone. Moreover, if the damage causes a bone spur to grow on the hip or femur, as described above, the extra piece of bone�can cause more damage and make the condition worse.
When you seek medical attention for a medical concern, it’s fundamental for the healthcare professional to accurately diagnose your health issue in order to follow-up with the proper treatment. A differential diagnosis is a list of possible injuries and/or underlying conditions which may be causing symptoms. Sciatica, a collection of symptoms commonly characterized by pain, discomfort, tingling sensations, and numbness, is a well-known health issue which can have many differential diagnosis. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Fibromyalgia Magazine
The purpose of the article was to discuss the differential diagnosis in sciatica with a variety of other health issues. Accurate diagnosis and proper treatment are important for sciatic nerve pain management. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine