I went through the physical therapy, and then I used chiropractic care, as well as crossfit, to kinda get me to that 100% mark. And I haven’t had a problem since, I continue to do crossfit and I use chiropractic care to make sure my body is aligned. It gives me that extra sense of feeling that I’m not gonna injure myself again, that my body is feeling good and 100%. I never have that feeling in the back of my mind, that, you know, I’m gonna injure myself. Sometimes I forget I even had a surgery and I think I can attribute that to a combination of chiropractic care and to the overall training aspect of crossfit. – Andrew Hutchison
There are a variety of causes for both hip pain and knee pain. While the hip joint can withstand a tremendous amount of wear-and-tear, it’s not indestructible. With age and usage, the hip cartilage can begin to degenerate, resulting in hip pain. Tendons and ligaments at the hip may also get excessive overused and can start to demonstrate signs of wear-and-tear over time. The anatomy of the knee, however, is more complex. The knee is collectively made up of bones, pads of cartilage and a joint capsule. Trauma or damage from an injury or degeneration associated with aging may cause knee pain.
Causes of Hip Pain
Hip pain is the general term used to define pain felt in or around the hip joint. Certain injuries and/or conditions may commonly cause hip pain. Arthritis, especially rheumatoid arthritis, are the primary culprits of hip pain in older individuals. Both may result in the breakdown of cartilage in the hip joint and can cause inflammation in the area. Combined with pain and discomfort, there’s generally also reduced range of motion in the hip as well as stiffness. Bursitis may also result in hip pain. The bursae are sacs of fluid which function by helping to reduce friction between the joints. If these become inflamed, however, they can lead to pain. Typically, it’s only repetitive movements that irritate the hip joint and result in pain.
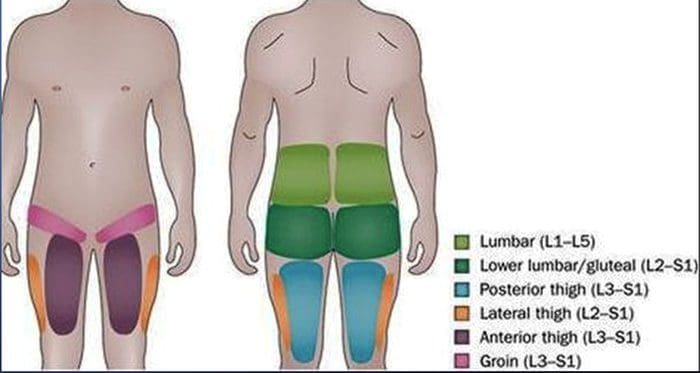
Similar to bursitis, tendinitis can also lead to inflammation and is usually caused by repetitive stress from movements. Muscle or tendon strain can be a result of overuse. Repeated physical activities can additionally place unnecessary amounts of pressure on the ligaments, tendons and joints of the hip, especially in those which support the buttocks. If some of these are inflamed, the hip won’t be able to function normally and there will be painful symptoms as a result. Below, we will describe the various causes of hip pain as well as discuss their effects on the structure of the hip in detail.�Hip pain isn’t always felt in the hip itself as it may also be felt in the groin or thigh.
Tendonitis
The most frequent cause of severe hip pain is inflamed tendons, or tendonitis. This can generally be due to excessive exercise or physical activities. This health issue can be quite debilitating but it usually heals within a couple of days with proper care.
Arthritis
As mentioned above, one of the most common causes of chronic hip pain is arthritis. Arthritis can cause painful, stiff and tender joints, and it can cause walking problems. Various types of arthritis can cause hip pain, including:
Osteoarthritis might be the final result of age-related degeneration in the cartilage that surrounds the joints.
Trauma, damage or injury to a joint, like a fracture, may cause traumatic arthritis similar to atherosclerosis.
Infectious arthritis is a result of an infection in the joint caused by the degeneration of cartilage.
Rheumatoid arthritis is a result of the human body’s immune system attacking its own joints. This type of arthritis can ultimately destroy joint bones and cartilage.
Osteoarthritis is a a lot more commonly diagnosed than rheumatoid arthritis.It’s fundamental to understand the different types of arthritis as these can be powerful diagnostic tools to help effectively treat hip pain.
Trochanteric Bursitis
Another possible cause of hip pain involves a health issue medically referred to as trochanteric bursitis, as previously mentioned. This condition occurs when the bursa, which are liquid-filled sacs near the hip joint, become inflamed. Any number of variables can lead to trochanteric bursitis, such as hip injury, overuse of the joints, underlying health issues, or even the presence of other conditions like rheumatoid arthritis. This condition is reportedly much more common in females than in males.
Hip Fractures
Hip fractures are common causes of hip pain which most frequently occur in older adults and in people who have osteoporosis, which is a weakening of the bones associated with age and various other factors. Hip fractures cause very sudden and extreme hip pain, where they will require immediate medical attention. There are complications that can happen due a fractured hip, like a blood clot in the leg. A hip fracture usually requires surgical interventions to be corrected. Additionally, you may be required to seek further care from a qualified healthcare professional in order to engage in a rehabilitation program.
Less Common Causes of Hip Pain
There are additional, less common conditions that can result in hip pain. These include snapping hip syndrome and osteonecrosis, or avascular necrosis. Below, we will discuss these two health issues in detail.
Snapping Hip Syndrome
Snapping hip syndrome, which most commonly occurs in athletes, especially dancers, is characterized by a snapping noise or feeling from the hip. By way of instance, this snapping may happen when you’re walking or getting up from a chair. The problem is usually painless, but it can cause pain in several cases. Snapping hip with pain is generally an indication of a tear in the hip cartilage or other structure surrounding the hip joint.
Osteonecrosis
Osteonecrosis, also known as avascular necrosis, occurs when blood isn’t able to reach the bones, either permanently or temporarily. This can cause the reduction of bone. The cartilage of individuals with this condition is normal initially, however, it will eventually collapse as the disease evolves. Finally, bones may crack or crumble. It’s not always clear what triggers osteonecrosis. Joint harm, heavy usage of steroid drugs or alcohol, and cancer treatments could put you at greater risk of developing this condition, however, the cause is never determined in many osteonecrosis cases.
Causes of Knee Pain
Similar to hip pain, arthritis, especially rheumatoid arthritis and osteoarthritis, may commonly cause knee pain. With the breakdown of cartilage associated with osteoarthritis in the knee, the bones can begin to rub against one another, causing pain and discomfort which could eventually lead to other painful symptoms. Rheumatoid arthritis is a chronic inflammatory disorder of the joints and it can affect the soft tissue which lines the knee joints. The final result is inflammation, joint damage and joint pain at the knee. The knee joint is very prone to accidents. Typical knee injuries include: meniscal injuries, anterior cruciate ligament injuries and tendon injuries.
The meniscus might be damaged when the knee is bent and twisted in an unnatural way, where ligaments and tendons could also be overstretched and ultimately torn as a result. If it is not repaired, the probability of developing osteoarthritis increases. Any abrupt change in movement can additionally injure the anterior cruciate ligament. Nearly all causes of knee injury and knee pain are the result of a blow to the surface of the knee. Exercises or physical activities which could harm the complex structures of the knee include jogging and jumping. A dislocated kneecap is still another frequent source of knee pain. This occurs when the patella is moved from place and it can be very debilitating.
Temporary knee pain differs from chronic knee pain. Persistent knee pain is not always attributable to one incident. It the result of many causes or conditions.Persistent knee pain is characterized as long-term pain, swelling, or sensitivity in a single or both knees. The reason behind your knee pain can determine the symptoms you develop. Many conditions may cause or lead to chronic knee pain, and lots of treatments exist. Every person’s experience with chronic knee pain will most likely be different. Understanding the causes of knee pain can be a powerful diagnostic tool which can help healthcare professionals properly determine the proper treatment option for your specific health issue.�Common causes of knee pain include:
osteoarthritis: pain, inflammation and joint destruction brought on by degeneration of a joint.
tendinitis: pain in the knee which worsens when climbing, taking stairs, or walking up an incline.
bursitis: inflammation caused by repeated overuse or trauma of the knee.
chondromalacia patella: damaged cartilage under the kneecap.
gout: arthritis brought on by the buildup of uric acid.
Baker’s cyst: a buildup of synovial fluid, fluid which lubricates the joint, supporting the knee.
rheumatoid arthritis, or RA: a chronic autoimmune inflammatory disease that causes painful swelling, joint deformity and bone erosion.
dislocation: dislocation of the kneecap most commonly caused by trauma, damage or injury.
meniscus tear: a rupture in one or more of the soft tissues in the knee.
torn ligament: tear at one of the four ligaments in the knee, the most commonly injured ligament is the anterior cruciate ligament, or the ACL.
bone tumors: osteosarcoma, is the second most common bone cancer, which most commonly occurs in the knee.
Dr. Alex Jimenez’s Insight
While the hip and knee joints are capable of sustaining various degrees of stress when performing physical activities, trauma, damage or injury as well as the degeneration of these complex structures, can ultimately lead to knee and hip pain. The balance of the human body as a whole is fundamental towards overall health and wellness. Therefore, if an individual experiences hip or knee pain, the entire structure and function of their body can be tremendously affected. It’s important for a person with knee or hip pain to seek immediate medical attention from a qualified and experienced healthcare professional, such as a chiropractor or physical therapist, in order to restore the balance of their entire body.
Treatment for Knee and Hip Pain
The treatment of hip pain is based upon the cause. For many instances of trauma, damage or injury, rest is generally enough to enable the hip to heal. By way of instance, exercise-associated hip pain is normally eliminated within a couple of days. When you have arthritis, a healthcare professional may sometimes prescribe drugs and/or medications to help relieve stiffness and pain. Furthermore, your physician will refer you to a doctor who can provide additional information regarding the cause of your hip pain along with recommending an alternative treatment option, such as chiropractic care and physical therapeutics, that will explain to you how you can perform rehabilitation exercises to help maintain joint strength, mobility and flexibility.
For injuries, therapy typically involves bed rest and the use of drugs and/or medications, such as naproxen, to alleviate pain, swelling and stiffness. Hip fractures, malformation of the hip and some injuries may require surgical intervention to repair or replace the hip. In hip replacement surgery, a surgeon will replace a broken hip joint with an artificial one. Although hip replacement surgery will need rehabilitation to become accustomed to the new joint, this type of treatment option is often considered.
Alternative Treatment Options
Some holistic remedies can offer relief from hip pain. Make certain you discuss treatment options with your doctor before considering any treatment option. Potential alternative treatment options include visiting a chiropractor for a spinal adjustment or manual manipulation. Chiropractic care is a well-known treatment approach which focuses on the diagnosis, treatment and prevention of a variety of injuries and/or conditions associated with the musculoskeletal and nervous system. Chiropractic care can help carefully re-align the spine as well as help reduce pain and discomfort, improve swelling and inflammation and even increase strength, flexibility and mobility on other structures of the human body. Physical therapeutics can also help treat both hip and knee pain.
There are many benefits of physical therapeutics, including increased range of motion, reduction of pain, less inflammation and swelling, as well as an overall improvement of quality of life. The first steps a chiropractor or physical therapist will perform if you have hip pain will consist of tests, such as a gait evaluation, range of motion measurement and intensity measurements. Afterwards, the healthcare professional will create a personalized treatment program. Treatment techniques may also include ultrasound and ice. There will also be specific exercises and stretches to help boost hip strength, mobility and flexibility to decrease pain. For knee pain, tests are also done along with active and passive treatments. Chiropractic care and physical therapeutics can help promote healing without the need for drugs and/or medications, and surgical interventions.
Bursitis, a frequent cause of knee pain, can be treated in the following ways:
Ice the knee for 15 minutes once an hour for three of four hours. Do not apply the ice directly to the knee, instead, cover your knee with a cotton towel. Put ice in a plastic zip-close bag, then place the bag on the towel.
Wear cushioned, flat shoes that support your toes and do not worsen your pain.
Avoid sleeping on your side. Use cushions positioned on both sides of your body to keep you from rolling on your side. When lying on the side, keep a pillow between your knees.
Stay seated when possible. Should you need to stand, prevent hard surfaces and maintain your weight evenly distributed on both legs.
Participate or engage in weight loss programs and strategies to lose weight if you are overweight or obese, to reduce the amount of stress that is placed on the knees.
If you are experiencing hip pain, knee pain or some other type of joint pain, make sure to contact a qualified healthcare professional, in order to receive a proper diagnosis to begin the best treatment approach for your specific health issue. Trained and skilled doctors will take you on the path to better healing. Make sure you prepare a one-on-one consultation to acquire a comprehensive examination and say good-bye to your pain. Healthcare professionals are devoted to providing you with a healthy and wholesome lifestyle.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Did you know that inflammation and low back pain can by caused by a low pH balance? Inflammation is believed to be caused by a variety of factors, including injury and/or an underlying condition, however, recent research studies have found a connection between inflammation, chronic back pain and pH balance. The lower your pH balance is, the more acidic your body is. When the human body is acidic, a condition referred to as acidosis, it can cause inflammation and other symptoms throughout the body, even in the lower back. Whether your pH balance or another health issue is causing your low back pain, it’s important to understand how acidity and low pH levels can affect the structure and function of the human body.
Metabolic acidosis is a condition used to describe when there is too much acid in your body fluids. When there is too much acid in your body, your pH balance reading will be low. In other words, your body will be considered acidic. When the human body is acidic, it neutralizes the acid by leaching calcium, magnesium, potassium and sodium from the bones. Over time, the excess acidity of the body can begin to gradually eat away at the bones, causing the progressive degeneration of the bones and eventually even leading to fractures. While a fracture may seem like a severe cause for back pain, the degeneration of the vertebrae of the spine can also cause disc degeneration disease, or DDD, leading to back pain and low back pain. The purpose of the article below is to demonstrate as well as discuss the relationship between low pH balance in intervertebral discs and low back pain.
The Relationship Between Low PH in Intervertebral Discs and Low Back Pain: a Systematic Review
Abstract
Introduction: To systematically review the relationship between low pH in intervertebral discs and low back pain.
Material and methods: Electronic database (PubMed, ISI Web of Science, Cochrane Library, CINAHL, AMED, and China National Knowledge Infrastructure) searches and hand searching of conference proceedings were conducted. Two authors independently evaluated the methodological quality and abstracted relevant data according to standard criteria. Then the experimental methods and samples employed in the finally retrieved articles were assessed.
Results: We first retrieved 136 articles regarding pain and pH, and only 16 of them were mainly about low back pain and pH. Finally, 7 articles met our expectation to focus on the pathogenesis of low back pain caused by pH. In these 7 studies the authors held three opinions to explain the pathogenesis of low back pain in relation to low pH. First, low pH caused by lactate stimulates the muscle and increases the muscle tension, which causes low back pain. Second, low pH stimulates the nerve roots and produces the feeling of pain. Third, low pH changes the matrix metabolism, leading to neuronal death and low back pain.
Conclusions: In this systematic review we propose a new hypothesis that low back pain may be caused by low pH based on the previous literature. Further experimental studies are necessary to verify our hypothesis. This hypothesis will promote our understanding of the pathogenesis of low back pain and the development of novel diagnostic and therapeutic approaches for low back pain.
Keywords:low back pain, pH, acidity, intervertebral disc, systematic review
Introduction
Low back pain is one of the most frequent causes of morbidity and disability. Low back pain affects up to 50% to 80% of the population in developed countries and its recurrence rate amounts to 85%, resulting in an economic loss of approximately 50 to 100 billion dollars per year in the US [1, 2].
Currently, effective treatment of low back pain is severely hampered due to the fact that its pathogenesis remains elusive [3, 4]. In recent years, several hypotheses have been proposed to explain the pathogenesis of low back pain and most of them focus on the dysfunction of the spinal column and its components, such as injury and clinical instability [5�7], spinal column degeneration [8], inferior facet-tip impingement on the lamina [9], and Schmorl’s nodes [10] and facet joint injury [11]. Other hypotheses focus on subfailure injury of the spinal muscles and ligaments and propose that spinal ligaments, disc annulus, facet capsules and thoracolumbar fascia may cause chronic back pain due to muscle control dysfunction [12�16]. In addition, the pain adaptation and pain-spasm-pain hypotheses have been proposed [17�19]. However, these hypotheses are largely speculative and need further experimental investigations.
The intervertebral disc (IVD) is composed of the nucleus pulposus (NP), the annulus fibrosus (AF), and the endplates (EP). The corpora vertebrae lie above and below the discs. The healthy disc is avascular, and its nutrition depends on diffusion via the AF and EP [20, 21]. The discs mainly produce ATP via anaerobic glycolysis; consequently lactate is produced and the pH is lower than other tissues. Low back pain is known to be related to intervertebral disc degeneration, and the pH would decrease in degenerated intervertebral discs [22, 23]. Therefore, low pH in the discs may be related to low back pain. Indeed, Hambly and Mooney [24] reported a close relationship between low back pain and low intradiscal pH in rabbits, while Krapf et al. [25] found that low pH could cause muscle spasm which was related to low back pain.
Based on the previous literature we propose a new hypothesis that low pH may cause low back pain. In this systematic review, we have collected and analysed the relevant literature regarding the relationship between low pH and low back pain to address the following questions: (1) What role does low pH play in low back pain? (2) Is the relationship obvious between low pH and low back pain? And (3), why are low pH and low back pain so relevant?
Material and Methods
Electronic databases (PubMed, ISI Web of Science, Cochrane Library, CINAHL, AMED, and China National Knowledge Infrastructure), which were last updated on 26 Nov. 2011, were searched without limit by two independent investigators. The search used terms and Boolean operators as follows: (low back pain OR lower back pain OR low back ache OR low backaches OR lumbago OR recurrent low back pain OR postural low back pain or mechanical low back pain) AND (low pH OR lactate OR lactate OR hydrogen ion concentration). Reference lists of all the selected articles were hand-searched for any additional trials. Conference abstracts of key pain and orthopaedic journals were hand-searched to identify unpublished data. If necessary, we contacted the authors to get additional information.
In total 136 articles were initially identified by literature search, and 113 articles were excluded after checking the titles and abstracts, which did not reach our expectation. Next we reviewed the full texts of the remaining articles and excluded the following articles: (1) articles not in English; (2) reviews, systematic reviews or letters; (3) pain in other tissues; (4) not related to pH, acidity or protons. As a result, 16 articles were retrieved and the references of these 16 articles were checked to ensure that other pertinent publications would not be missed. Finally, seven articles met our expectation to focus on the pathogenesis of low back pain caused by pH (Figure 1). The literature search was performed by two of the authors (CZL and HL) independently, and any disagreement was resolved by discussion.
We scrutinized the seven articles with the focus on �the mechanisms by which pH causes low back pain�, and then assessed the experimental methods and samples employed in the seven articles.
Results
Seven articles met our expectation [26�32]. Then we evaluated the level of evidence for each article, according to the standard listed in Table I [33]. Five of them were level II, and two were level III. The characteristics of the seven studies are listed in Table II.
Nerve Roots
Three studies involving 32 patients [26, 27, 29] suggested that low pH would stimulate the nerve roots and cause low back pain.
Diamant et al. analysed the correlation between lactate level and pH in discs of patients with lumbar rhizopathy and found that low pH was caused by the increased lactate level due to the enhanced anaerobic glycolysis within the NP, which counteracts the decreased nutritional diffusion. The reaction of nerve roots in cases with low pH is related to increased production and leakage of acid metabolism. Sensitive structures such as the nerve roots could be irritated by the leakage of acid metabolites and it was shown that pain will arise in tissues with low pH [26, 34].
Keshari et al. used HR-MAS NMR spectroscopy to analyse snap frozen samples taken from 9 patients who underwent discectomy for painful disc degeneration [27, 35, 36]. They found that proteoglycan, collagen, and lactate may serve as metabolism markers of discogenic back pain. Therefore, they speculated that low pH was caused by increased lactate and increased lactate stimulated nerve fibres in granulation tissue associated with disc healing, which was correlated with discogenic pain [27, 35, 36].
Baumann et al. examined the responses of cultured adult human dorsal root ganglion (hDRG) neurons to low pH [29]. They found that low pH evoked, sustained depolarizations were due to more than one mechanism, and the inhibition of resting membrane conductance contributes to the responses to low pH in some hDRG neurons, which was related to low back pain [29].
Muscle Tension and Swelling of Connective Tissue
A previous study suggested that low pH would increase muscle tension, which could cause low back pain [30]. The authors examined 20 patients with chronic palpable tension of the erector muscles of the spine, and found that the pH decreased because of the enhanced anaerobic glycolysis in NP. The low pH was caused by the accumulation of lactate. Lactate would stimulate the multifidus muscle and increase the muscle tension. Simultaneously, myogelosis is induced, leading to low back pain [30]. Vormann et al. [31] showed that the simple and safe addition of an alkaline multimineral preparate was able to reduce the pain symptoms in these patients with chronic low back pain. These results suggest that a disturbed acid-base balance may contribute to the symptoms of low back pain.
Metabolism
Bartels et al. measured the oxygen and lactate concentrations in 11 patients with back pain and 13 patients with scoliosis, and found that in each case, the oxygen and lactate concentrations were the highest in the interior of the disc and fell toward the outer annulus [28]. Therefore, they speculated that the microcirculation through the endplate and the rate of cellular metabolism would influence the oxygen and lactate concentrations in the disc. For instance, the oxygen concentration would fall as cellular demand increases; consequently the lactate concentration would increase and the pH would decrease. It was observed that in some discs the concentration of oxygen was less than 40 mm Hg and that of lactate was more than 5 mmol/l, which would lead to cell death.
Another study also indicated that decreased pH, decreased PO2 and increased PCO2 may be related to the mechanisms of pain production in patients with back pain [32]. These abnormalities can be identified by magnetic resonance imaging. Further investigation is needed to determine whether therapeutic manipulation of these variables can be effective in relieving axial spinal pain.
Low pH would lead to a change in the matrix metabolism, which could strongly influence the cell activity and even cause cell death. It is well known that acid-sensing ion channels (ASICs) on the cell surface could be stimulated by protons. After cells die, the protons would increase and activate ASICs, which in turn mediate ischaemic neuronal death [37], and eventually cause low back pain [28, 38�40].
Dr. Alex Jimenez’s Insight
When an individual’s bodily fluids contain too much acid, or they’re too acidic,�a common concern known as acidosis, it can lead to a variety of health issues if not properly addressed. Your lungs and kidneys can generally compensate for slight pH imbalances, however, problems with any of these organs or even an improper nutrition consisting of processed foods high in sugar, can result in excess acid accumulating in the human body. Other risk factors which can contribute to an increased chance of developing acidosis include: a high-fat diet that’s low in carbohydrates, kidney failure, obesity, dehydration, aspirin or methanol poisoning, and diabetes. Furthermore, as mentioned in the article, acidosis has also been associated as a cause of inflammation which may lead to chronic back pain and low back pain. Therefore, maintaining pH balance is believed to be able to help treat low back pain, alongside other alternative treatment options, such as chiropractic care.
Discussion
After careful review of the seven articles we retrieved, we obtained a systematic view with regard to the relationship between low pH and low back pain, although the authors of the individual studies had proposed three different opinions.
If low pH directly stimulates the nerve roots, the pH is very important to the healing of low back pain. Lactate would cause low pH, stimulate the nerve roots, cause depolarization at the surface of the nerves, and modulate the nociceptors to let the patients feel pain. However, in order to establish a relationship between discogenic back pain and lactate, a much larger number of patients need to be studied and the changes in proteoglycans (PG)/collagen (col), PG/lactate peak (Lac), and Lac/col ratios should be correlated with visual pain scores or other pain indexes [27, 29].
The second opinion holds that low pH would act on the muscle but not nerve roots. If the oxygen tension falls below 5 mm Hg, the muscle tension would increase, and even result in myogelosis. Muscle contraction depends solely on the chemical energy of ATP. If the oxygen tension decreased, the cells would undergo anaerobic glycolysis and produce much lactate, leading to decreased pH. However, it remains elusive what level of pH would cause pain [30].
The third opinion claims that disc energy and matrix metabolism are crucially involved in low back pain [38�40]. This provides a valuable insight into the pathogenesis of low back pain. Nevertheless, the detailed cellular and molecular mechanisms by which disc energy and matrix metabolism disruption lead to neuronal death and eventually pain development are not completely understood.
This systematic review had several limitations. First, the heterogeneity between individual studies was substantial. Second, there are only small number patients in several prospective cohort studies of selected articles. Third, there may be some selection bias because the retrieved articles were confined to limited databases.
In conclusion, in this systematic review we propose a new hypothesis that low back pain may be caused by low pH based on previous literature, in which three opinions have been proposed by the authors to explain the pathogenesis of low back pain in relation to low pH. First, low pH caused by lactate stimulates the muscle and increases the muscle tension, which would cause low back pain. Second, low pH stimulates the nerve roots and produces the feeling of pain. Third, low pH changes the matrix metabolism, leading to neuronal death and low back pain. These different opinions are not exclusive but may be complementary. Further experimental studies are necessary to verify our hypothesis that low pH causes low back pain. This hypothesis will promote our understanding of the pathogenesis of low back pain and the development of novel diagnostic and therapeutic approaches for low back pain.
Acknowledgments
This study was partly supported by a grant from the National Nature Science Foundation of China (81171756) and the Science and Technology Planning Project of Zhejiang Province (2012C13G2010083).
In conclusion,�a lower pH balance can mean that your blood is more acidic, while a higher pH balance means that your blood is closer to the levels it should be at. While these numbers may only appear to differentiate slightly, these numerical differences can be serious and may ultimately affect your overall health and wellness. In the article above, researchers proposed that low back pain may be caused by low pH levels. Furthermore, the outcome measures of the systematic review will help support the understanding of the pathogenesis of low back pain, promoting more treatment options for chronic back pain. Information referenced from the National Center for Biotechnology Information (NCBI).�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
4.�Ghahreman A, Bogduk N. Predictors of a favorable response to transforaminal injection of steroids in patients with lumbar radicular pain due to disc herniation.�Pain Med.�2011;12:871�9.�[PubMed]
5.�Panjabi MM. The stabilizing system of the spine. Part II. Neutral zone and instability hypothesis.�J Spinal Disord.�1992;5:390�6.�[PubMed]
6.�Depalma M, Ketchum J, Saullo T, Schofferman J. Structural etiology of chronic low back pain due to motor vehicle collision.�Pain Med.�2011;12:1622�7.�[PubMed]
7.�Raczkowski JW, Daniszewska B, Zolynski K. Functional scoliosis caused by leg length discrepancy.�Arch Med Sci.�2010;6:393�8.�[PMC free article]�[PubMed]
8.�Kirkaldy-Willis WH, Wedge JH, Yong-Hing K, Reilly J. Pathology and pathogenesis of lumbar spondylosis and stenosis.�Spine.�1978;3:319�28.�[PubMed]
9.�Yang KH, King AI. Mechanism of facet load transmission as a hypothesis for low-back pain.�Spine.�1984;9:557�65.�[PubMed]
10.�Lipson SJ, Fox DA, Sosman JL. Symptomatic intravertebral disc herniation (Schmorl’s node) in the cervical spine.�Ann Rheum Dis.�1985;44:857�9.�[PMC free article]�[PubMed]
11.�Farfan HF, Sullivan JD. The relation of facet orientation to intervertebral disc failure.�Can J Surg.�1967;10:179�85.�[PubMed]
12.�Schleip R, Vleeming A, Lehmann-Horn F, Klingler W. Letter to the Editor concerning �A hypothesis of chronic back pain: ligament subfailure injuries lead to muscle control dysfunction� (M. Panjabi)�Eur Spine J.�2007;16:1733�5.�[PMC free article]�[PubMed]
13.�Panjabi MM. A hypothesis of chronic back pain: ligament subfailure injuries lead to muscle control dysfunction.�Eur Spine J.�2006;15:668�76.�[PMC free article]�[PubMed]
14.�DePalma MJ, Ketchum JM, Saullo TR. Etiology of chronic low back pain in patients having undergone lumbar fusion.�Pain Med.�2011;12:732�9.�[PubMed]
15.�Karabekir HS, Yildizhan A, Atar EK, et al. Effect of ligamenta flava hypertrophy on lumbar disc herniation with contralateral symptoms and signs: a clinical and morphometric study.�Arch Med Sci.�2010;6:617�22.�[PMC free article]�[PubMed]
16.�Petronic I, Nikolic D, Cirovic D, et al. Distribution of affected muscles and degree of neurogenic lesion in patients with spina bifida.�Arch Med Sci.�2011;7:1049�54.�[PMC free article]�[PubMed]
17.�van Dieen JH, Selen LP, Cholewicki J. Trunk muscle activation in low-back pain patients, an analysis of the literature.�J Electromyogr Kinesiol.�2003;13:333�51.�[PubMed]
18.�Lund JP, Donga R, Widmer CG, Stohler CS. The pain-adaptation model: a discussion of the relationship between chronic musculoskeletal pain and motor activity.�Can J Physiol Pharmacol.�1991;69:683�94.�[PubMed]
19.�Maigne JY, Vautravers P. Mechanism of action of spinal manipulative therapy.�Joint Bone Spine.�2003;70:336�41.�[PubMed]
20.�Roberts S, Evans H, Trivedi J, Menage J. Histology and pathology of the human intervertebral disc.�J Bone Joint Surg Am.�2006;88(Suppl 2):10�4.�[PubMed]
21.�Raj PP. Intervertebral disc: anatomy-physiology-pathophysiology-treatment.�Pain Pract.�2008;8:18�44.[PubMed]
22.�Kitano T, Zerwekh JE, Usui Y, et al. Biochemical changes associated with the symptomatic human intervertebral disk.�Clin Orthop Relat Res.�1993;293:372�7.�[PubMed]
23.�Wuertz K, Godburn K, Iatridis JC. MSC response to pH levels found in degenerating intervertebral discs.�Biochem Biophys Res Commun.�2009;379:824�9.�[PMC free article]�[PubMed]
24.�Hambly MF, Mooney V. Effect of smoking and pulsed electromagnetic fields on intradiscal pH in rabbits.�Spine.�1992;17:S83�5.�[PubMed]
25.�Krapf MW, Muller S, Mennet P, et al. Recording muscle spasm in the musculus erector spinae using in vivo 31P magnetic resonance spectroscopy in patients with chronic lumbalgia and generalized tendomyopathies.�Z Rheumatol.�1992;51:229�37.�[PubMed]
26.�Diamant B, Karlsson J, Nachemson A. Correlation between lactate levels and pH in discs of patients with lumbar rhizopathies.�Experientia.�1968;24:1195�6.�[PubMed]
27.�Keshari KR, Lotz JC, Link TM, et al. Lactic acid and proteoglycans as metabolic markers for discogenic back pain.�Spine.�2008;33:312�7.�[PubMed]
28.�Bartels EM, Fairbank JC, Winlove CP, Urban JP. Oxygen and lactate concentrations measured in vivo in the intervertebral discs of patients with scoliosis and back pain.�Spine.�1998;23:1�7.�[PubMed]
29.�Baumann TK, Burchiel KJ, Ingram SL, Martenson ME. Responses of adult human dorsal root ganglion neurons in culture to capsaicin and low pH.�Pain.�1996;65:31�8.�[PubMed]
30.�Strobel ES, Krapf M, Suckfull M, et al. Tissue oxygen measurement and 31P magnetic resonance spectroscopy in patients with muscle tension and fibromyalgia.�Rheumatol Int.�1997;16:175�80.�[PubMed]
31.�Vormann J, Worlitschek M, Goedecke T, Silver B. Supplementation with alkaline minerals reduces symptoms in patients with chronic low back pain.�J Trace Elem Med Biol.�2001;15:179�83.�[PubMed]
32.�Moore MR, Brown CW, Brugman JL, et al. Relationship between vertebral intraosseous pressure, pH, PO2, pCO2, and magnetic resonance imaging signal inhomogeneity in patients with back pain. An in vivo study.�Spine.�1991;16:S239�42.�[PubMed]
33.�Prommahachai A, Wittayapirot K, Jirarattanaphochai K, Sae-Jung S. Correction with instrumented fusion versus non-corrective surgery for degenerative lumbar scoliosis: a systematic review.�J Med Assoc Thai.�2010;93:920�9.�[PubMed]
34.�Menkin V. Biochemical mechanisms in inflammation.�Br Med J.�1960;1:1521�8.�[PMC free article][PubMed]
35.�Aoki Y, Akeda K, An H, et al. Nerve fiber ingrowth into scar tissue formed following nucleus pulposus extrusion in the rabbit anular-puncture disc degeneration model: effects of depth of puncture.�Spine.�2006;31:E774�80.�[PubMed]
36.�Ozawa T, Ohtori S, Inoue G, et al. The degenerated lumbar intervertebral disc is innervated primarily by peptide-containing sensory nerve fibers in humans.�Spine.�2006;31:2418�22.�[PubMed]
37.�Wang YZ, Xu TL. Acidosis, acid-sensing ion channels, and neuronal cell death.�Mol Neurobiol.�2011;44:350�8.�[PubMed]
38.�Ohshima H, Urban JP. The effect of lactate and pH on proteoglycan and protein synthesis rates in the intervertebral disc.�Spine.�1992;17:1079�82.�[PubMed]
39.�Ishihara H, Urban JP. Effects of low oxygen concentrations and metabolic inhibitors on proteoglycan and protein synthesis rates in the intervertebral disc.�J Orthop Res.�1999;17:829�35.�[PubMed]
40.�Holm S, Maroudas A, Urban JP, Selstam G, Nachemson A. Nutrition of the intervertebral disc: solute transport and metabolism.�Connect Tissue Res.�1981;8:101�19.�[PubMed]
The spine is made of bones called vertebrae, with the spinal cord running through the spinal canal in the center. The cord is made up of nerves. These nerve roots split from the cord and travel between the vertebrae into various areas of the body. When these nerve roots become pinched or damaged, the symptoms that follow are known as, radiculopathy. El Paso, TX. Chiropractor, Dr. Alexander Jimenez breaks down�radiculopathies,�along with their causes, symptoms and treatment.
The entire length of the spine, at each level, nerves exit through holes in the bone of the spine (foramen) on each side of the spinal column. These nerves are called nerve roots, or radicular nerves and�branch out from the spine and supply different parts of the body.
Nerves exiting the cervical spine travel down through the arms, hands, and fingers. This is where neck problems affecting a cervical nerve root can cause pain, as well as, other symptoms through the arms and hands, one form of (radiculopathy). Another is low back problems that affect a lumbar nerve root. This can radiate through the leg and into the foot, another form of (radiculopathy, or sciatica), which creates leg pain and/or foot pain.
The spinal cord does not go into the lumbar spine and because the spinal canal has space in the lower back, problems in the lumbosacral region often cause nerve root problems and not a spinal cord injury. Serious conditions i.e. disc herniation or fracture in the lower back are also not likely to cause permanent loss of motor function in the legs.
Cervical Spine – This nerve root is named according to the Lower spinal segment that the nerve root runs between.�
Example – The nerve at C5-C6 level is called the C6 nerve root.
It’s named like this because as it exits the spine, it passes Over the C6 pedicle (a piece of bone part of the spinal segment).
Lumbar Spine – These nerve roots are named according to the Upper spinal segment that the nerve runs between.
Example – The nerve at L4-L5 level is called the L4 nerve root.
The nerve root is named this way because as it exits the spine it passes Under the L4 pedicle.
Two Nerve Roots
Two nerves cross each disc level
Only one exits�the spine (through the foramen) at that level.
Exiting Nerve Root –�This is the nerve root exiting the spine at a certain level.
Example: L4 nerve root exits the spine at L4-L5 level.
Traversing Nerve Root –�This nerve root goes across the disc and exits the spine at the level below.
Example: L5 nerve is the traversing nerve root at L4-L5 level, and is the exiting nerve root at L5-S1 level.
There is some confusion when a nerve root is compressed by disc herniation or other cause to refer both to the intervertebral level (where the disc is) and to the nerve root that is affected. This depends on where the disc herniation or protrusion is happening. It could impinge upon either the exiting nerve�or the traversing nerve.
If The Traversing Nerve Is Affected
Lumbar Radiculopathy
In the lumbar spine, there is a weak area in the disc space right in front of the traversing nerve root, so lumbar discs tend to herniate or leak out and impinge on the traversing nerve.
If The Exiting Nerve Is Affected
Cervical Radiculopathy
The opposite is true in the neck. In the cervical spine, the disc tends to herniate to the side, rather than toward the back and the side. If the disc material herniates to the side, it will compress or impinge the exiting nerve root.
Radiculopathy & Sciatica
Nerve root goes by another name Radicular Nerve, and when a herniated or prolapsed disc presses on a radicular nerve, this is referred to as a radiculopathy. A medical physician might say there is herniated disc at L4-L5, which creates an L5 radiculopathy or an L4 radiculopathy. It all depends on where the disc herniation occurs (the side or the back of the disc) and which nerve is affected. And the term for radiculopathy in the low back is the ever famous Sciatica.
Radiculopathy
A pinched nerve can occur at different areas of the spine (cervical, thoracic or lumbar).
Common causes are narrowing of the hole where the� nerve roots exit, which can result from stenosis, bone spurs, disc herniation and other conditions.
Symptoms vary but often include pain, weakness, numbness and tingling.
Symptoms can be managed with nonsurgical treatment, but minimal surgery can also help.
Prevalence & Pathogenesis
A herniated disc can be defined as herniation of the nucleus pulposus through the fibers of the annulus fibrosus.
Most disc ruptures occur during the third and fourth decades of life while the nucleus pulposus is still gelatinous.
The most likely time of day associated with increased force on the disc is the morning.
In the lumbar region, perforations usually arise through a defect just lateral to the posterior midline, where the posterior longitudinal ligament is weakest.
Epidemology
Lumbar Spine:
Symptomatic lumbar disc herniation occurs during the lifetime of approximately 2% of the general population.
Approximately 80% of the population will experience significant back pain during the course of a herniated disc.
The groups at greatest risk for herniation of intervertebral discs are younger individuals (mean age of 35 years)
True sciatica actually develops in only 35% of patients with disc herniation.
Not infrequently, sciatica develops 6 to 10 years after the onset of low back pain.
The period of localized back pain may correspond to repeated damage to annular fibers that irritates the sinuvertebral nerve but does not result in disc herniation.
Epidemology
Cervical Spine:
The average annual incidence of cervical radiculopathies is less than 0.1 per 1000 individuals.
Pure soft disc herniations are less common than hard disc abnormalities (spondylosis) as a cause of radicular arm pain.
In a study of 395 patients with nerve root abnormalities, radiculopathies occurred in the cervical and lumbar spine in 93 (24%) and 302 (76%), respectively.
Pathogenesis
Alterations in intervertebral disc biomechanics and biochemistry over time have a detrimental effect on disc function.
The disc is less able to work as a spacer between vertebral bodies or as a universal joint.
Pathogenesis – LUMBAR SPINE
The two most common levels for disc herniation are L4-L5 and L5-S1, which account for 98% of lesions; pathology can occur at L2-L3 and L3-L4 but is relatively uncommon.
Overall, 90% of disc herniations are at the L4-L5 and L5-S1 levels.
Disc herniations at L5-S1 will usually compromise the first sacral nerve root, a lesion at the L4-L5 level will most often compress the fifth lumbar root, and herniation at L3-L4 more frequently involves the fourth lumbar root.
Disc herniation may also develop in older patients.
Disc tissue that causes compression in elderly patients is composed of the annulus fibrosus and and portions of the cartilaginous endplate (hard disc.)
The cartilage is avulsed from the vertebral body.
Resolution of some of the compressive effects on neural structures requires resorption of the nucleus pulposus.
Disc resorption is part of the natural healing process associated with disc herniation.
The enhanced ability to resorb discs has the potential for resolving clinical symptoms more rapidly.
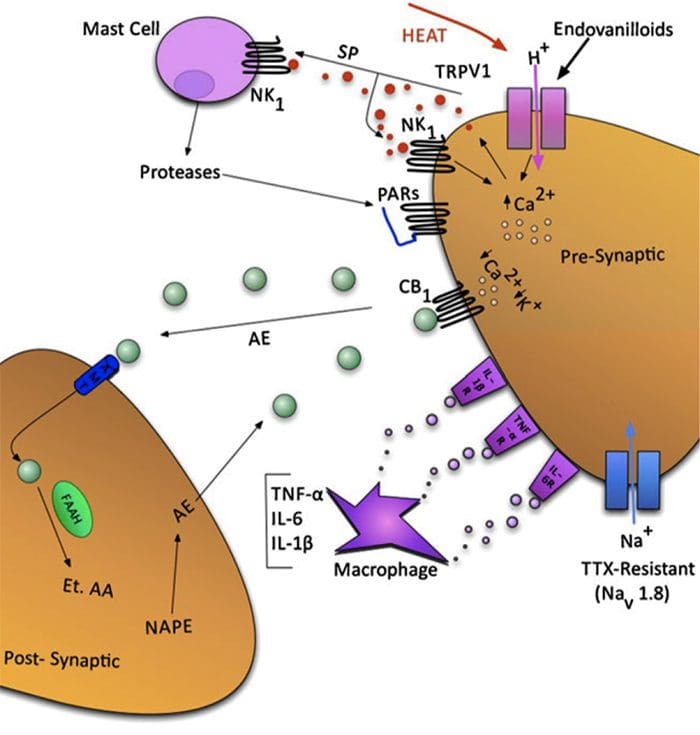
Resorption of herniated disc material is associated with a marked increase in infiltrating macrophages and the production of matrix metalloproteinases (MMPs) 3 and 7.
Nerlich and associates identified the origins of phagocytic cells in degenerated intervertebral discs.
The investigation identified cells that are transformed local cells rather than invaded macrophages.
Degenerative discs contain the cells that add to their continued dissolution.
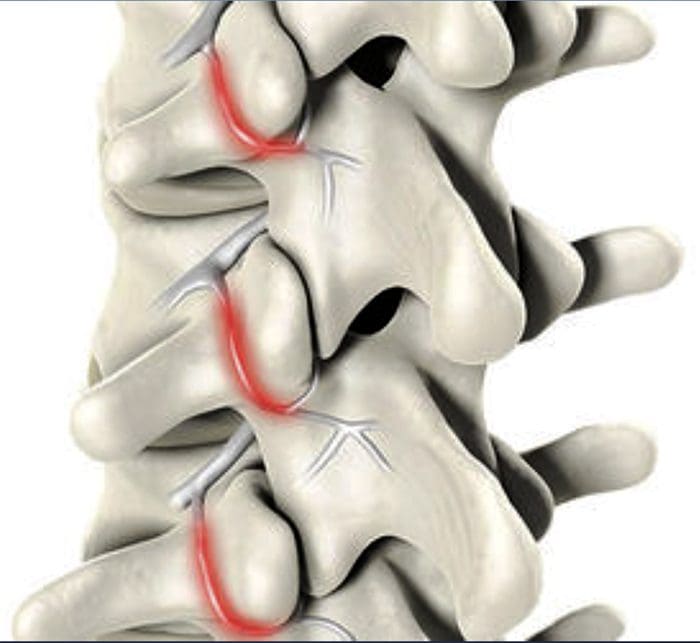
Pathogenesis – CERVICAL SPINE
In the early 1940s, a number of reports appeared in which cervical intervertebral disc herniation with radiculopathies was described.
There is a direct correlation between the anatomy of the cervical spine and the location and pathophysiology of disc lesion.
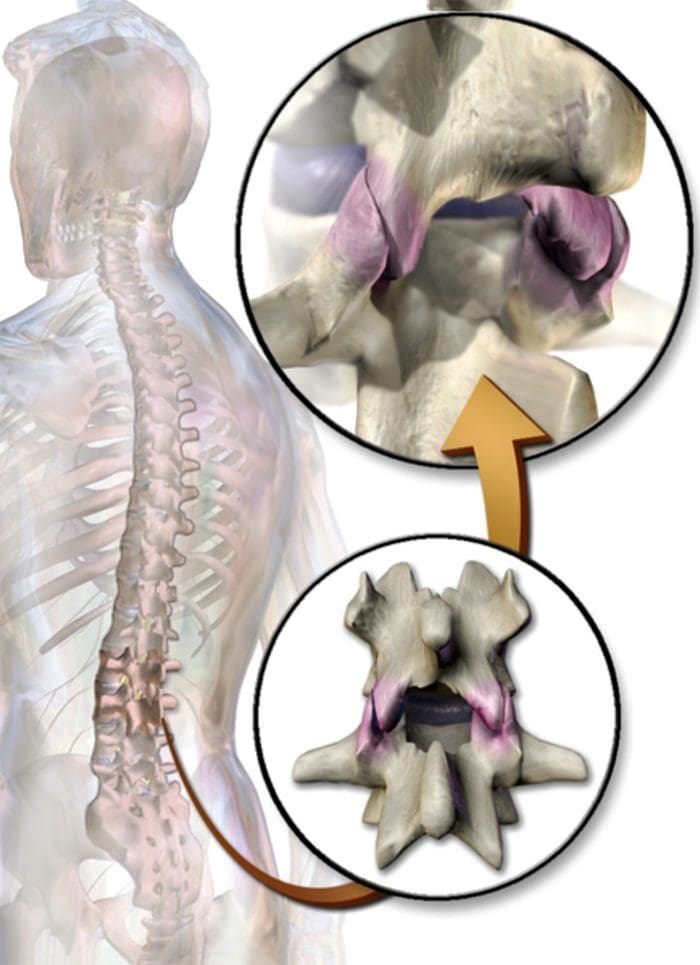
The eight cervical nerve roots exit via intervertebral foramina that are bordered anteromedially by the intervertebral disc and posterolaterally by the zygapophyseal joint.
The foramina are largest at C2-C3 and decrease in size until C6-C7.
The nerve root occupies 25% to 33% of the volume of the foramen.
The C1 root exits between the occiput and the atlas (C1)
All lower roots exit above their corresponding cervical vertebrae (the C6 root at the C5-C6 interspace), except C8, which exits between C7 and T1.
A differential growth rate affects the relationship of the spinal cord and nerve roots and the cervical spine.
Most acute disc herniations occur posterolaterally and in patients around the forth decade of life, when the nucleus is still gelatinous.
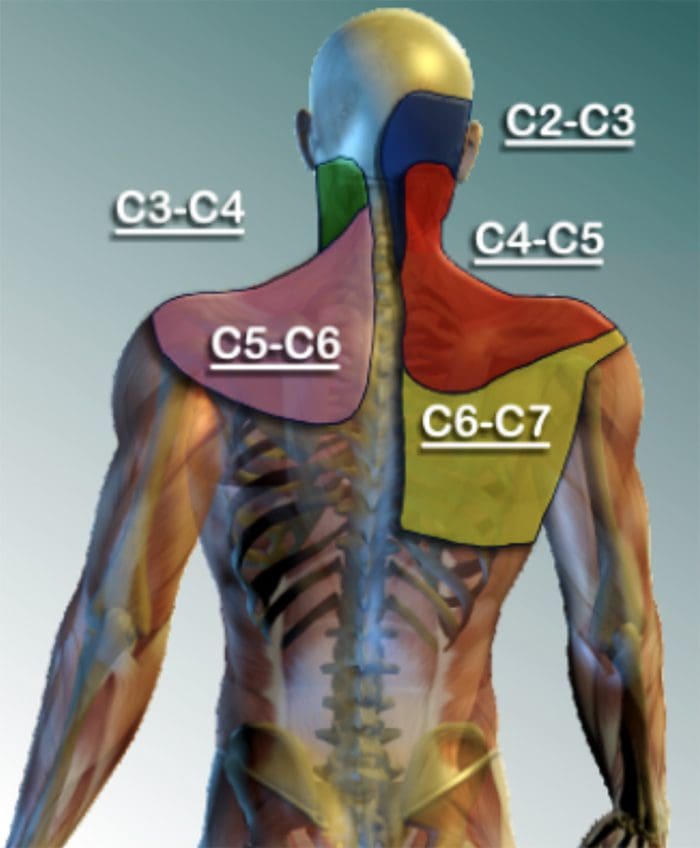
The most common areas of disc herniations are C6-C7 and C5-C6.
C7-T1 and C3-C4 disc herniations are infrequent ( less than 15 %).
Disc herniation of C2-C3 is rare.
Patients with upper cervical disc protrusions in the C2-C3 region have symptoms that include suboccipital pain, loss of hand dexterity, and paresthesias over the face and unilateral arm.
Unlike lumbar herniated discs, cervical herniated discs may cause myelopathy in addition to radicular pain because of the anatomy of the spinal cord in the cervical region.
The uncovertebral prominences play a role in the location of ruptured discs material.
The uncovertebral joint tends to guide extruded disc material medially, where cord compression may also occur.
Disc herniations usually affect the nerve root numbered most caudally for the given disc level; for example, the C3 � C4 disc affects the fourth cervical nerve root; C4- C5, the fifth cervical nerve root; C5 � C6, the sixth cervical nerve root; C6 � C7, the seventh cervical nerve root; and C7 � T1, the eighth cervical nerve root.
Not every herniated disc is symptomatic.
The development of symptoms depends on the reserve capacity of the spinal canal, the presence of inflammation, the size of the herniation, and the presence of concomitant disease such as osteophyte formation.
In disc rupture, protrusion of nuclear material results in tension on the annular fibers and compress?on of the dura or nerve root causing pain.
Also important is the smaller size of the sagittal diameter, the bony cervical spinal canal.
Individuals in whom a cervical herniated disc causes motor dysfunction have a complication of cervical disc herniation if the spinal canal is stenotic.
Clinical History – LUMBAR SPINE
Clinically, the patient�s major complaint is a sharp, lancinating pain.
In many cases there may be a previous history of intermittent episodes of localized low back pain.
The pain not only in the back but also radiates down the leg in the anatomic distribution of the affected nerve root.
It will usually be described as deep and sharp and progressing from above downward in the involved leg.
Its onset may be insidious or sudden and associated with a tearing or snapping sensations of the spine.
Occasionally, when sciatica develops, the back pain may resolve because once the annulus has ruptured, it may no longer be under tension.
Disc herniation occurs with sudden physical effort when the trunk is flexed or rotated.
On occasion, patients with L4-L5 disc herniation have groin pain. In a study of 512 lumbar disc patients, 4.1% had groin pain.
Finally, the sciatica may vary in intensity; it may be so severe that patients will be unable to ambulate and they will feel that their back is “locked”.
On the other hand, the pain may be limited to a dull ache that increases in intensity with ambulation.
Pain is worsened in the flexed position and relieved by extension of the lumbar spine.
Characteristically, patients with herniated discs have increased pain with sitting, driving, walking, couching, sneezing, or straining.
Clinical History – CERVICAL SPINE
Arm pain, not neck pain, is the patient� s major complaint.
The pain is often perceived as starting in the neck area and then radiating from this point down to shoulder, arm and forearm and usually into the hand.
The onset of the radicular pain is often gradual, although it can be sudden and occur in association with a tearing or snapping sensation.
As time passes, the magnitude of the arm pain clearly exceeds that of the neck or shoulder pain.
The arm pain may also be variable in intensity and preclude any use of the arm; it may range from severe pain to a dull, cramping ache in the arm muscles.
The pain is usually severe enough to awaken the patient at night.
Additionally, a patient may complain of associated headaches as well as muscle spasm, which can radiate from the cervical spine to below the scapulae.
The pain may also radiate to the chest and mimic angina (pseudoangina) or to the breast.
Symptoms such as back pain, leg pain, leg weakness, gait disturbance, or incontinence suggest compression of the spinal cord (Myelopathy).
Physical Examination – LUMBAR SPINE
Physical examination will demonstrated a decrease in range of motion of the lumbosacral spine, and patients may list to one side as they try to bend forward.
The side of the disc herniation typically corresponds to the location of the scoliotic list.
However, the specific level or degree of herniation does not correlate with the degree of list.
On ambulation, patients walk with an antalgic gait in which they hold the involved leg flexed so that they put as little weight as possible on the extremity.
Neurologic Examination:
The neurologic examination is very important and may yield objective evidence of nerve root compression (We should evaluate of reflex testing, muscle power, and sensation examination of the patient).
In addition, a nerve deficit may have little temporal relevance because it may be related to a previous attack at a different level.
Compression of individual spinal nerve roots results in alterations in motor, sensory, and reflex function.
When the first sacral root is compressed, the patient may have gastrocnemius-soleus weakness and be unable to repeatedly raise up on the toes of that foot.
Atrophy of the calf may be apperent, and the ankle (Achilles) reflex is often diminished or absent.
Sensory loss, if present, is usually confined to the posterior aspect of the calf and the lateral side of the foot.
Involvement of the fifth lumbar nerve root can lead to weakness in extension of the great toe and, in a few cases, weakness of the everters and dorsiflexors of the foot.
A sensory deficit can appear over the anterior of the leg and the dorsomedial aspect of the foot down to the big toe
With compression of the fourth lumbar nerve root, the quadriceps muscle is affected; the patient may note weakness in knee extension, which is often associated with instability.
Atrophy of the thigh musculature can be marked. Sensory loss may be apparent over the anteromedial aspect of the thigh, and the patellar tendon reflex can be diminished.
Nerve root sensitivity can be elicited by any method that creates tension.
The straight leg-raising (SLR)test is the one most commonly used.
This test is performed with the patient supine.
Physical Examination – CERVICAL SPINE
Neurologic Examination:
A neurologic examination that shows abnormalities is the most helpful aspect of the diagnostic work-up, although the examination may remain normal despite a chronic radicular pattern.
The presence of atrophy helps document the location of the lesion, as well as its chronicity.
The presence of subjective sensory changes is often difficult to interpret and requires a coherent and cooperative patient to be of clinical value.
When the third cervical root is compressed, no reflex change and motor weakness can be identified.
The pain radiates to the back of the neck and toward the mastoid process and pinna of the ear.
Involvement of the fourth cervical nerve root leads to no readily detectable reflex changes or motor weakness.
The pain radiates to the back of the neck and superior aspect of the scapula.
Occasionally, the pain radiates to the anterior chest wall.
The pain is often exacerbated by neck extension.
Unlike the third and the fourth cervical nerve roots, the fifth through eighth cervical nerve roots have motor functions.
Compression of the fifth cervical nerve root is characterized by weakness of shoulder abduction, usually above 90 degree, and weakness of shoulder extension.
The biceps reflexes are often depressed and the pain radiates from the side of the neck to the top of the shoulder.
Decreased sensation is often noted in the lateral aspect of the deltoid, which represents the autonomous area of the axillary nerve.
Involvement of the sixth cervical nerve root produces biceps muscles weakness as well as diminished brachioradial reflex.
The pain again radiates from the neck down the lateral aspect of the arm and forearm to the radial side of hand (index finger, long finger, and thumb).
Numbness occurs occasionally in the tip of the index finger, the autonomous area of the sixth cervical nerve root.
Compression of the seventh cervical nerve root produces reflex changes in the triceps jerk test with associated loss of strength in the triceps muscles, which extend the elbow.
The pain from this lesion radiates from the lateral aspect of the neck down the middle of the area to the middle finger.
Sensory changes occur often in the tip of the middle finger, the autonomous area for the seventh nerve.
Patients should also be tested for scapular winging, which may occur with C6 or C7 radiculopathies.
Finally, involvement of the eighth cervical nerve root by a herniated C7-T1 disc produces significant weakness of the intrinsic musculature of the hand.
Such involvement can lead to rapid atrophy of the interosseous muscles because of the small size of these muscles.
Loss of the interossei leads to significant loss of fine hand motion.
No reflexes are easily found, although the flexor carpi ulnaris reflex may be decreased.
The radicular pain from the eighth cervical nerve root radiates to the ulnar border the hand and the ring and little fingers.
The tip of the little finger often demonstrates diminished sensation.
Radicular pain secondary to a herniated cervical disc may be relieved by abduction of the affected arm.
Although these signs are helpful when present, their absence alone does not rule out a nerve root lesion.
Laboratory Data
Medical screening laboratory test (blood counts, chemistry panels erythrocyte sedimentation rate [ESR]) are normal in patients with a herniated disc.
Electro diagnostic Testing
Electromyography(EMG)is an electronic extension of the physical examination.
The primary use of EMG is to diagnose radiculopathies in cases of questionable neurologic origin.
EMG findings may be positive in patients with nerve root impingement.
Radiographic Evaluation – LUMBAR SPINE
Plain x-rays may be entirely normal in a patient with signs and symptoms of nerve root impingement.
Computed Tomography
Radigraphic evaluation by CT scan may demonstrate disc bulging but may not correlate with the level of nerve damage.
Magnetic Resonance Imaging
MR imaging also allows visualization of soft tissues, including discs in the lumbar spine.
Herniated discs are easily detected with MR evaluation.
MR imaging is a sensitive technique for the detection of far lateral and anterior disc herniations.
Radiographic Evaluation – CERVICAL SPINE
X-rays
Plain x-rays may be entirely normal in patients wit han acute herniated cervical disc.
Conversely,�70% of asymptomatic women and 95% of asymptomatic men between the ages of 60 and 65 years have evidence of degenerative disc disease on plain roentgenograms.
Views to be obtained include anteroposterior, lateral, flexion, and extension.
Computed Tomography
CT permits direct visualization of compression of neural structures and is therefore more precise than myelography.
Advantages of CT over myelography include better visualization of lateral abnormalities such as foraminal stenosis and abnormalities caudal to the myelographic block, less radiation exposure, and no hospitalization.
Magnetic Resonance
MRI allows excellent visualization of soft tissues, including herniated discs in the cervical spine.
The test is noninvasive.
In a study of 34 patients with cervical lesions, MRI predicted 88% of the surgically proven lesions versus 81% for myelography-CT, 58% for myelography, and 50% for CT alone.
Differential Diagnosis – LUMBAR SPINE
The initial diagnosis of a herniated disc is ordinarily made on the basis of the history and physical examination.
Plain radiographs of the lumbosacral spine will rarely add to the diagnosis but should be obtained to help rule out other causes of pain such as infection or tumor.
Other tests such as MR, CT, and myelography are confirmatory by nature and can be misleading when used as screening tests.
Spinal Stenosis
Patient with spinal stenosis may also suffer from back pain that radiates to the lower extremities.
Patients with spinal stenosis tend to be older than those in whom herniated discs develop.
Characteristically, patients with spinal stenosis experience lower extremity pain (pseudoclaudication=neurogenic claudication) after walking for an unspecified distance.
They also complain of pain that is exacerbated by standing or extending the spine.
Radiographic evaluation is usually helpful in differentiating individuals with disc herniation from those with bony hypertrophy associated with spinal stenosis.
In a study of 1,293 patients, lateral spinal stenosis and herniated intervertebral discs coexisted in 17.7% of individuals.
Radicular pain may be caused by more than one pathologic process in an individual.
Facet Syndrome
Facet syndrome is another cause of low back pain that may be associated with radiation of pain to structures outside the confines of the lumbosacral spine.
Degeneration of articular structures in the facet joint causes pain to develop.
In most circumstances, the pain is localized over the area of the affected joint and is aggravated by extension of the spine (standing).
A deep , ill-defined, aching discomfort may also be noted in the sacroiliac joint, the buttocks, and the legs.
The areas of sclerotome affected show the same embryonic origin as the degenerated facet joint.
Patients with pain secondary to facet joint disease may have relief of symptoms with apophyseal injection of a long-acting local anesthetic.
The true role of facet joint disease in the production of back and leg pain remains to be determined.
Other mechanical causes of sciatica include congentenial abnormalites of the lumbar nerve roots, external compression of the sciatic nerve (wallet in a back pants pocket), and muscular compression of the nerve (piriformis syndrome).
In rare circumstances, cervical or thoracic lesion should be considered if the lumbar spine is clear of abnormalities.
Medical causes of sciatica (neural tumors or infections, for example) are usually associated with systemic symptoms in addition to nerve pain in a sciatic distribution.
Differential Diagnosis – CERVICAL SPINE
No diagnostic criteria exist for the clinical diagnosis of a herniated cervical disc.
The provisional diagnosis of a herniated cervical disc is made by the history and physical examination.
The plain x-ray is usually nondiagnostic, although occasionally disc space narrowing at the suspected interspace or foraminal narrowing on oblique films is seen.
The value of x-rays is to exclude other causes of neck and arm pain, such as infection and tumor.
MR imaging and CT-myelography are the best confirmatory examinations for disc herniation.
Cervical disc herniations may affect structures other than nerve roots.
Disc herniation may cause vessel compression (vertebral artery) associated with vertebrobasilar artery insufficiency and be manifested as blurred vision and dizziness.
Other mechanical causes of arm pain should be excluded.
The most common is some form of compression on a peripheral nerve.
Such compression can occur at the elbow, forearm, or wrist. An example is compression of the median nerve by the carpal ligament leading to carpal tunnel syndrome.
The best diagnostic test to rule out these peripheral neuropathies is EMG.
Excessive traction on the arm secondary to heavy weights may cause radicular pain without disc compression of nerve roots.
Spinal cord abnormalities must be considered if signs of myelopathy are present in conjunction with radiculopathies.
Spinal cord lesions such as syringomyelia are identified by MRI, and motor neuron disease is identified by EMG.
Multiple sclerosis should be considered in a patient with radiculopathies if the physical signs indicate lesions above the foramen magnum (optic neuritis).
In very rare circumstances, lesions of the parietal lobe corresponding to the arm can mimic the findings of cervical radiculopathies.
You try to stand up from a seated position and feel a stab of pain in your lower back. It may even shoot through your hip, buttock, or down the back of your thigh. The pain may even get worse then you walk uphill or sit for a long period of time. While these symptoms could mean a pinched nerve, lumbar disc herniation, hip bursitis, or degenerative hip disease, it could also be sacroiliac joint dysfunction.
What Is Sacroiliac Joint Dysfunction?
The sacroiliac (SI) joint is located in the pelvis. It is very strong as it is a weight bearing joint connecting the pelvis to the sacrum. It is surrounded by tough ligaments that reinforce it, providing added support.
There is an SI joint located on each side of the sacrum and they work together, moving as a single unit to act as a shock absorber for the spine and for transmitting force of the upper body. Just like any other joint in the body, the SI joint can be injured or diseased, causing it to become unstable and inflamed, causing pain and limited mobility.
What Causes SI Joint Inflammation?
While doctors have not established how the pain is generated, it is believed that it is due to a change in the normal motion of the joint. This could occur due to:
Hypermobility (Instability or Too Much Movement) � This can cause the pain to reside in the lower back. It can also be felt in the hip or both the hip and lower back and may even radiate into the groin.
Hypomobility (Fixation or Too Little Movement) � This can cause the pain to reside in the lower back or buttocks and may radiate down one leg, usually in the back of the thigh. It usually doesn�t reach the knee, but sometimes can even reach the ankle and foot. In this way, the condition mimics sciatica.
Sacroiliac joint dysfunction typically affects women who are young or middle aged. Older women and men are rarely affected although it does happen.
What Are Treatment Options For Sacroiliac Joint Pain?
When SI joint pain is initially diagnosed the treatment is usually fairly conservative. Medication, physical therapy, and injections are used by doctors for pain management.
NSAIDs and other similar medications decrease inflammation and reduce pain, while physical therapy can readjust the SI joint in cases where it is dislocated or immobilized. It also includes exercises that stabilize the joint for pain management over the long term.
Steroid injections directly into the sacroiliac joint can help with the reduction of inflammation and pain while making physical therapy more effective. When steroid injections are effective but the effects are temporary there is another non-surgical treatment that is sometimes used called RFA, or radiofrequency ablation.
In cases where the conservative methods do not achieve the desired results there are surgical options that provide pain reduction and stabilization on a more permanent scale. SI fusion involves fusing the joint, providing relief.
However, there is a treatment option that is non-invasive, doesn�t involve steroids or medications that could have harmful side effects � chiropractic.
Spinal manipulation � This is the traditional chiropractic adjustment that is also known as high-velocity, low-amplitude (HVLA) thrust.
Spinal mobilization � This is a less forceful, gentle chiropractic adjustment also known as low-velocity, low-amplitude thrust.
Chiropractic is proven to be an effective, non-invasive, gentle method for relieving the pain and inflammation of SI joint dysfunction. No medication, no surgery, just relief.
So if you�ve been suffering from sacroiliac joint dysfunction, give us a call! Our Doctor of Chiropractic is here to help!
Injury Medical Clinic: Sciatica Treatments & Recoveries
Biomarkers (short for biological markers) are biological measurements of a biological condition. By definition, a biomarker is “a characteristic that is objectively measured and evaluated as an indicator of normal biological processes, pathogenic processes or pharmacological responses to a therapeutic intervention” Biomarkers are the measurements utilized to perform a clinical evaluation like blood pressure or cholesterol level and therefore are used to monitor and forecast health conditions in individuals or across populations so that appropriate treatment options could be proposed. Biomarkers may be used by itself or in combination to assess the health or disease state of an individual.
Variety of Biomarkers
A wide selection of biomarkers are used now. Every biological system, such as the cardiovascular system, metabolic system or the immune system, has its own specific biomarkers. Many of these biomarkers are rather easy to quantify and form part of regular medical examinations. By way of instance, a general health check may include assessment of blood pressure, heart rate, cholesterol, triglycerides and fasting glucose levels. Body dimensions such as weight, body mass index, or BMI, and waist-to-hip ratio are routinely used for assessing conditions like obesity and metabolic disorders, among others. These varieties in biomarkers can ultimately be useful in the diagnosis of a variety of health issues.
Attributes of a Perfect Biomarker
An ideal biomarker has particular characteristics that make it suitable for assessing a particular disease or condition. Ideally, an ideal marker should possess the following features, as it should be:
Safe and simple to measure
Cost effective to follow up
Modifiable with treatment
Consistent across gender and cultural groups
Biomarkers as Health and Disease Predictors
Biomarkers are used to predict significant ailments like diabetes and cardiovascular disease, among others. Each individual biomarker indicates whether there’s a disease or health condition and can be combined to offer a thorough demonstration of how healthy an individual is and whether further diagnosis needs to be made. Biomarkers ultimately serve as health and disease predictors, capable of determining a potential onset of disease or illness, such as that of cancer.
Biomarkers in Cancer Detection and Drug Development
The principles of biomarkers in disease have been applied to the discovery, screening, diagnosis, treatment and monitoring of cancer. Traditionally, anti-cancer drugs and/or medications were agents that eliminated both cancer cells and healthy cells. However, more targeted therapies have now been developed that can be instructed to kill cancer cells only, while sparing healthy cells. The evaluation of a typical biomarker in cancer will help in the development of therapies that may target the biomarker. This can minimize the risk of toxicity and reduce the cost of treatment. In cancer research, genetic studies are valuable because genetic abnormalities so often underlie the evolution of cancer. Certain DNA or RNA markers might therefore help in the treatment and detection of specific cancers. The purpose of the following article, however, is to demonstrate the biomarkers involved in low back pain, disc degeneration and other chronic pain health issues, such as neuropathic pain.
Inflammatory Biomarkers of Low Back Pain and Disc Degeneration: a Review
Abstract
Biomarkers are biological characteristics that can be used to indicate health or disease. This paper reviews studies on biomarkers of low back pain (LBP) in human subjects. LBP is the leading cause of disability, caused by various spine-related disorders, including intervertebral disc degeneration, disc herniation, spinal stenosis, and facet arthritis. The focus of these studies is inflammatory mediators, because inflammation contributes to the pathogenesis of disc degeneration and associated pain mechanisms. Increasingly, studies suggest that the presence of inflammatory mediators can be measured systemically in the blood. These biomarkers may serve as novel tools for directing patient care. Currently, patient response to treatment is unpredictable with a significant rate of recurrence, and, while surgical treatments may provide anatomical correction and pain relief, they are invasive and costly. The review covers studies performed on populations with specific diagnoses and undefined origins of LBP. Since the natural history of LBP is progressive, the temporal nature of studies is categorized by duration of symptomology/disease. Related studies on changes in biomarkers with treatment are also reviewed. Ultimately, diagnostic biomarkers of LBP and spinal degeneration have the potential to shepherd an era of individualized spine medicine for personalized therapeutics in the treatment of LBP.
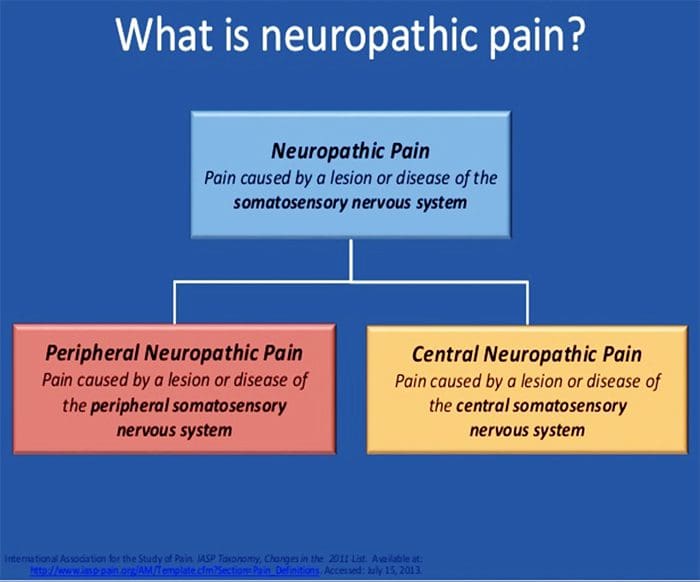
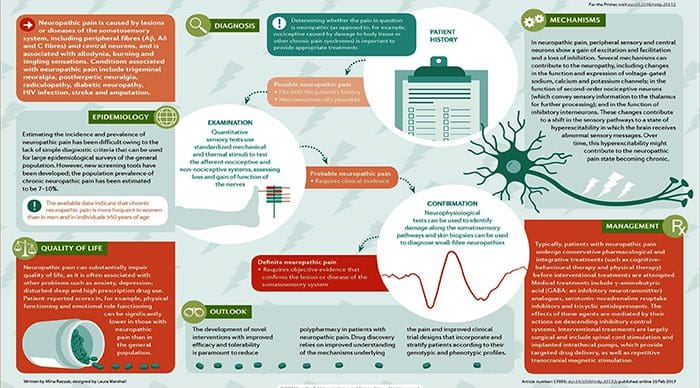
Biomarkers for Chronic Neuropathic Pain and their Potential Application in Spinal Cord Stimulation: a Review
Abstract
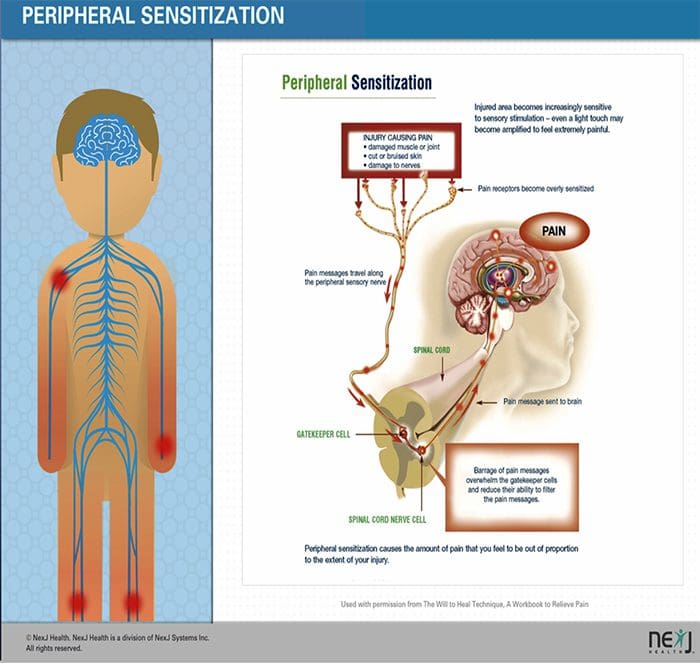
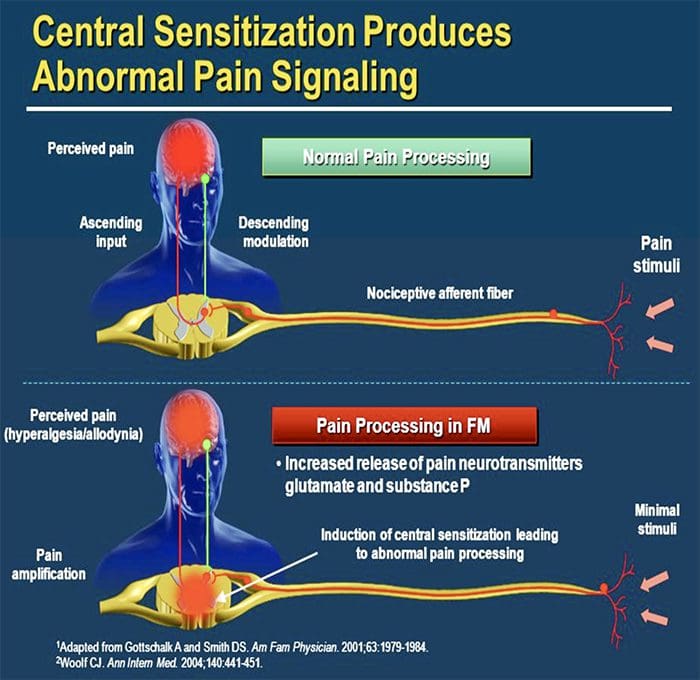
This review was focused on understanding which substances inside the human body increase and decrease with increasing neuropathic pain. We reviewed various studies, and saw correlations between neuropathic pain and components of the immune system (this system defends the body against diseases and infections). Our findings will especially be useful for understanding ways to reduce or eliminate the discomfort, chronic neuropathic pain brings with it. Spinal cord stimulation (SCS) procedure is one of the few fairly efficient remedial treatments for pain. A follow-up study will apply our findings from this review to SCS, in order to understand the mechanism, and further optimize efficaciousness.
Chronic neuropathic pain disorders represent a common long-term disability in the United States, as well as, globally. They affect 1 in 4 Americans. Chronic neuropathic pain treatment has limited success because of poor understanding of the mechanisms that lead to the initiation and maintenance. Additionally, the effectiveness of neuropathic pain management regimens and procedures has been difficult to determine in the past, due to the subjectivity related to pain perception, and a lack of standardized assessment of neuropathic pain. However, one of the most effective management strategies in recent times is spinal cord stimulation (SCS). The main goals of spinal cord stimulation are to improve physical function and quality of life in the patients afflicted with chronic neuropathic pain associated with complex regional pain syndrome (CRPS), failed back syndrome, and other chronic neuropathic pain syndromes [1�2]. Despite limited knowledge of how people benefit from SCS, more than 20,000 stimulators are implanted each year, with more than a half-billion dollars in revenue [3]. While it is generally believed that spinal cord stimulation inhibits pain transmission in the dorsal horn, the exact mechanisms by which SCS relieves neuropathic pain is unknown. Chronic neuropathic pain is caused often by inflammation and/or nerve injury. The advances have shown that inflammation and nerve injury produce changes in the expression of cytokines, neurotransmitters, and structural proteins [4]. It is very likely that there are changes in the body�s serum biomarkers of neuropathic pain before SCS and after SCS. Such a study would contribute greatly to the field of neuromodulation, as objective quantifiers of neuropathic pain control before and after SCS have not yet been investigated. Such definitive data regarding the effectiveness of SCS in relieving neuropathic pain and improving function will be important in future use of SCS.
In preparation for the launching of this study, the authors� goal with this transcript is to provide a review of the literature regarding known biomarkers for chronic neuropathic pain, and then prepare a role for biomarker analysis in the prediction of therapy success in SCS.
Data
The expression of certain genes is altered under chronic pain conditions. This alteration has helped provide an insight into the identification of potential biomarkers [5]. Current advanced research suggests that genetic expression of cytokines, positively or negatively, correlates with the experience of chronic pain. This negative or positive correlation primarily depends on the nature of the cytokine. Cytokines are signaling proteins which mediate the activation, differentiation, and proliferation of immune cells. They can be pro-inflammatory or anti-inflammatory. A misaligned balance between pro-inflammatory and anti-inflammatory cytokines has been common in most of the studies conducted (Table 1). Pro-inflammatory cytokines such as IL-1?, IL-6, IL-2, IL-33, CCL3, CXCL1, CCR5, and TNF-?, have been found to play significant roles in the amplification of chronic pain states. In studies involving discogenic pain, Complete Freund�s adjuvant (CFA)-induced discogenic pain in animal models has been observed to coincide with a sustained up-regulation of the above named cytokines [6]. In a more recent study, chronic constriction injury (CCI)-induced rats (neuropathic pain induction) were shown to have increased serum levels of CCL3 and CCR5. Even more interesting, an intrathecal injection of the anti-inflammatory cytokine, IL-4, and the CCL3-neutralizing antibody, reduced the CCI-induced neuropathic pain, estimated by a plantar test [7]. Other studies have also shown that the selective genetic impairment of the highlighted pro-inflammatory cytokines attenuated nerve-injury induced pain behavior, observed in neuropathic pain models [8]. Particularly, Zarpelon et al. revealed that CCI-induced rats showed reduced mechanical hyperalgesia when the IL-33 receptor gene, IL-33R (ST2), was knocked out, compared to the wild-type mice [9].
On the other hand, one study showed that blood levels of anti-inflammatory cytokines (such as IL-10 and IL-4) of Complex Regional Pain Syndrome (CRPS) patients were lower compared to the control [10]. A recent study also shows a distinction of the significant increases of pro-inflammatory cytokines based on the part of the back affected. There were more significant elevations (p<0.05, student�s t test) of pro-inflammatory cytokines in the plasma of lower back pain patients than in upper back patients, when compared to controls [11]. There has also been a study focusing on the levels of the aforementioned cytokines in patients with painful neuropathy in contrast with painless neuropathy and healthy control subjects. Patients with a painful neuropathy had about double the level of IL-2 expression (p = 0.001), TNF expression (p < 0.0001) and protein levels (p = 0.009) than the controls. The study further indicated there was about double the IL-2 and TNF level expression (p = 0.03; p = 0.001) and protein levels in painful neuropathy (p = 0.04; p = 0.04) than patients with painless neuropathy. On the contrary, levels of mRNA expression of the anti-inflammatory cytokines, IL-10 and IL-4 were considerably lower in patients with painful neuropathy than in patients with painless neuropathy (p =0.001) [12].
Several other studies, focused on the antagonist and agonist effects of some drugs targeting pro-inflammatory and anti-inflammatory cytokines, also have pointed out their significance with pain. Certain known analgesics were seen to reduce the levels of pro-inflammatory cytokines in the studies reviewed. There was a study about (CCI)-induced rats, in which case, this induced injury significantly, elevated the levels of pro-inflammatory cytokines, and decreased the serum levels of anti-inflammatory cytokines. Omeprazole, a known remedy for stomach pain, was observed to reduce the levels of pro-inflammatory cytokines (TNF-?, IL-1?, and IL-6) to normal, compared with the CCI control. It is important to note that this was while curbing the CCI-induced neuropathic pain, measured with the paw withdrawal latency [13]. Zhou et al. also highlighted the significance of certain drugs in determining the correlation between cytokines and neuropathic pain. CCI was again, used to induce neuropathic pain on rat models; and in turn, Paenoflorin, an established analgesic [14] was administered. Once Paenoflorin was introduced, significant decreases in serum levels of pro-inflammatory cytokines of CCI-induced rats (IL-1?, IL-6, TNF-?, and CXCL1) were observed, compared to the CCI-control [15]. The cytokines identified here, are the ones that showed correlation in various studies reviewed.
Even though cytokines are the key chronic pain biomarkers, according to the studies reviewed, there are still other proteins and nucleotides that have been observed to associate with chronic pain disorder. Two studies laid emphasis on regulatory microRNAs (miRNAs), which are small non-coding RNA molecules involved in post-transcriptional gene regulation. miRNAs achieve this by binding to mRNAs and degrading them or repressing their functions. Orlova et al. showed that 60% of CRPS patients in their study showed a significant down-regulation of 18 different miRNAs. The rest of the patients, however, showed variable (contradicting) miRNA levels. miRNA levels show variability, depending on the gene being regulated [5]. Tao et al. revealed that an increased inflammatory stimulation by the cytokine IL-1? in normal and osteoarthritis chondrocytes produced a significant down-regulation of the miRNA, miR-558, and a significant up-regulation of miR-21 in DRG neurons. A connection between IL-1? and miR-21 was attributed to AP-1, which is a transcription factor located in the promoter site of the mRNA, and is activated by IL-1? [4]. siRNAs have the same features as miRNAs, in the sense, that they are regulatory nucleotides. They also show variability, depending on the gene being regulated. SIRT1, a deacetylase, functions in regulating various pathways, including inflammation. It was observed that an intrathecal injection of SRT170, an SIRT1 agonist, reduced serum levels of NF-?B, a transcription factor for pro-inflammatory cytokines, in CCI-induced rat models. When SRT170-siRNA (a regulator of the regulator) was administered before SRT170, there was no agonistic effect [16].
Dr. Alex Jimenez’s Insight
A biomarker is most accurately defined as any measurement which demonstrates an interaction between a biological system and the possibility of a chemical, physical or biological hazard. However, biomarkers are often most commonly associated with medicine. In this setting, these can be utilized to determine the effects a particular treatment may have on a patient as well as for determining the risk a patient may have of developing certain health issues. An example of a diagnostic use of biomarkers includes the measurement of biomarkers in blood to evaluate the severity of a heart attack. In the same manner, blood samples can be analyzed and biomarkers can be measured in the instance of chronic pain.
Discussion
Chronic neuropathic pain affects a tremendous amount of the population. There are few effective therapies. However, outcomes are hard to determine due to the subjective nature of pain. We would like to devise a strategy that would establish objectivity of pain assessment. After review of various studies relating to pain biomarkers, we found that serum levels of pro-inflammatory cytokines and chemokines, such as IL-1?, IL-6, IL-2, IL-33, CCL3, CXCL1, CCR5, and TNF-?, were significantly up-regulated during chronic pain experience. On the other hand, anti-inflammatory cytokines such as IL-10 and IL-4 were found to show significant down-regulation during chronic pain state. Regulatory miRNAs, siRNAs, and deacetylases that coincide with these cytokines, also showed negative correlation, corresponding to the cytokine they were regulating.
The authors would like to apply this knowledge to SCS, a therapy for chronic neuropathic pain, in an attempt to develop a biomarker profile to help predict success. This study will be a prospective study including patients scheduled for SCS. One month before SCS surgery, patients will complete a survey assessing their subjective level of pain on the visual analog scale and subjective level of function. Patients will also have venipuncture performed, and serum will be analyzed for levels of pain biomarkers. After SCS surgery, patients will be followed at 6 more time points: 2 weeks, 1 month, 3 months, 6 months, 1 year, and 2 years. At each time point, the survey will be re-administered and blood work will be repeated. By evaluating patients pre-operatively and post-operatively, we will be able to assess subjective and objective levels of pain, allowing us to analyze trends in pain biomarkers in the context of patient-reported pain measurement. The duration of this study will be 4 years. Each subject will participate in this study for a total period of 25 months, which will allow us to follow these patients for 2 years postoperatively.
Conclusion
The review of various studies relating to inflammation- and/or nerve injury-induced chronic pain disorder led us to hypothesize that the application of the spinal cord stimulation procedure should relatively reduce serum pro-inflammatory cytokines, and relatively increase serum levels of anti-inflammatory cytokines. This should, in turn, help us understand the mechanism of spinal cord stimulation, thereby optimizing the efficaciousness of the procedure, and perhaps allow us to make predictions regarding therapy success. A follow-up prospective study regarding serum biomarker profile in SCS patients is currently being undertaken.
Footnotes
Author Disclosure:The authors declare no conflicts of interest.
Disclosure of Funding:This work was supported by grants from the University of Medicine and Dentistry of New Jersey and the National Institutes of Health, Bethesda, Maryland (grant numbers: NS072206, HL117684, and DA033390).
In conclusion,�diagnostic biomarkers have the potential of leading new personalized therapeutics in the treatment of chronic pain health issues, such as low back pain, disc degeneration and neuropathic pain. Several research studies like the ones above have been established to ultimately help healthcare professionals understand better ways to reduce or eliminate the pain and discomfort associated with these chronic pain problems. Furthermore, biomarkers can be essential diagnostic tools for the evaluation and treatment of a variety of health issues. Information referenced from the National Center for Biotechnology Information (NCBI).�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
2.�Kumar K, Hunter G, Demeria D. Spinal Cord Stimulation in Treatment of Chronic Benign Pain: Challenges in Treatment Planning and Present Status, a 22-year Experience.�Neurosurgery.�2006;58:481�491.�[PubMed]
3.�Vallejo R, Kramer J, Benjamin R. Neuromodulation of the Cervical Spinal Cord in the Treatment of Chronic Intractable Neck and Upper Extremity Pain: A Case Series and Review of the Literature.�Pain Physician.�2007;10:305�311.�[PubMed]
4.�Lutz BM, Bekker A, Tao YX. Non-coding RNAs: New Players in Chronic Pain.�Anesthesiology.�2014 doi: 10.1097/ALN.0000000000000265.�[PMC free article]�[PubMed]�[Cross Ref]
5.�Orlova IA, Alexander GM, Qureshi RA, Sacan A, et al. MicroRNA Modulation in Complex Regional Pain Syndrome.�Journal of Translational Medicine.�2011;9:195.�[PMC free article]�[PubMed]
6.�Jung WW, Kim HS, Shon JR, et al. Intervertebral Disc Degeneration-induced Expression of Pain-Related Molecules: Glial Cell-derived Neurotropic Factor as a Key Factor.�J Neurosurg Anesthesiol.�2011;23:329�334.�[PubMed]
7.�Sun S, Chen D, Lin F, Chen M, Yu H, Hou L, Li C. Role of Interleukin-4, the Chemokine CCL3 and its Receptor CCR5 in Neuropathic Pain.�Mol Immunol.�2016;77:184�192.�[PubMed]
8.�Clark AK, Old EA, Malcangio M. Neuropathic Pain and Cytokines: Current Perspectives.�Journal of Pain Research.�2013;6:803�814.�[PMC free article]�[PubMed]
10.�Parkitny L, McAuley JH, Pietro FD, Stanton TR, O�Connell NE, Marinus J, van Hilten JJ, Moseley GL. Inflammation in Complex Regional Pain Syndrome.�Neurology.�2013;80:106�117.�[PMC free article][PubMed]
11.�Li Y, Liu J, Liu ZZ, Duan DP. Inflammation in Low Back may be detected from the Peripheral Blood: Suggestions for Biomarker.�Bioscience Reports.�2016 doi: 10.1042/BSR20160187.�[PMC free article][PubMed]�[Cross Ref]
12.�Uceyler N, Rogausch JP, Toyka KV, Sommer C. Differential Expression of Cytokines in Painful and Painless Neuropathies.�Neurology.�2007;69:42�49.�[PubMed]
13.�Chanchal SK, Mahajan UB, Siddharth S, Reddy N, Goyal SN, Patil PH, Bommanahalli BP, Kundu CN, Patil CR, Ojha S. In Vivo and In Vitro Protective Effects of Omeprazole against Neuropathic Pain.�Sci Rep.�2016;6:30007.�[PMC free article]�[PubMed]
14.�Yin D, Liu YY, Wang TX, Hu ZZ, Qu WM, Chen JF, Cheng NN, Huang ZL. Paeoniflorin exerts analgesic and hypnotic effects via adenosine A1 receptors in a mouse neuropathic pain model.�Psychopharmacology (Berl)�2016 Jan;233(2):281�93.�[PubMed]
15.�Zhou J, Wang L, Wang J, Wang C, Yang Z, Wang C, Zhu Y, Zhang J. Evid Based Complement.�Alternat Med.�2016;2016:8082753.�[PMC free article]�[PubMed]
16.�Lv C, Hu HY, Zhao L, Zheng H, Luo XZ, Zhang J. Intrathecal SRT1720, a SIRT1 agonist, exerts anti-hyperalgesic and anti-inflammatory effects on chronic constriction injury-induced neuropathic pain in rats.�Int J Clin Exp Med.�2015;8(5):7152�7159.�[PMC free article]�[PubMed]
17.�Kraychete DC, et al. Serum Cytokine Levels in Patients with Chronic Low Back Pain due to Herniated Disc: Analytical Cross-Sectional Study.�Sao Paulo Med J.�2010;128(5):259�292.�[PubMed]
18.�Bazzichi L, et al. Cytokine Patterns in Fibromyalgia and Their Correlation with Clinical Manifestations.�Clinical and Experimental Rheumatology.�2007;25:225�230.�[PubMed]
19.�Iannuccelli C, et al. Pathophysiology of Fibromyalgia: A Comparison with the Tension-Type Headache, a Localized Pain Syndrome.�Ann NY Acad Sci.�2010;1193:78�83.�[PubMed]
20.�Backonja MM, Coe CL, Muller DA, Schell K. Altered Cytokine Levels in the Blood and Cerebrospinal Fluid of Chronic Pain Patients.�Journal of Neuroimmunology.�2008;195:157�163.�[PubMed]
21.�Empl M1, Renaud S, Erne B, Fuhr P, Straube A, Schaeren-Wiemers N, Steck AJ. TNF-Alpha Expression in Painful and Non-painful Neuropathies.�Neurology.�2001;56(10):1371�7.�[PubMed]
22.�Della Vedova C, et al. Peripheral Interleukin-1? Levels are elevated in Chronic Tension-Type Headache Patients.�Pain Res Manag.�2013;18(6):301�306.�[PMC free article]�[PubMed]
23.�Ko�er A, et al. Interleukin-6 Levels in Tension Headache Patients.�Clin J Pain.�2010;26:690�693.[PubMed]
24.�Bekker A, Haile M, Kline R, Didehvar S, Babu R, Martiniuk F, Urban M. The effect of intraoperative infusion of dexmedetomidine on the quality of recovery after major spinal surgery.�J Neurosurg Anesthesiol.�2013;25(1):16�24.�[PMC free article]�[PubMed]
25.�Dominques RB, Duarte H, Rocha NP, Teixeira AL. Increased Serum Levels of Interleukin-8 in Patients with Tension-Type Headache.�Cephalagia.�2014;0(0):1�6.
Arthritis pain is a complex phenomenon involving intricate neurophysiological processing at all levels of the pain pathway. The treatment options available to alleviate joint pain are fairly limited, and most arthritis patients report only modest pain relief with current treatments. A better understanding of the neural mechanisms responsible for musculoskeletal pain and identifying new targets will help develop future pharmacological therapies. This article reviews some of the latest research into factors that contribute to joint pain and covers areas such as cannabinoids, proteinase-activated receptors, sodium channels, cytokines, and transient receptor potential channels. The emerging hypothesis that osteoarthritis may have a neuropathic component is also discussed.
Introduction
The world health organization ranks musculoskeletal disorders as the most frequent cause of disability in the modern world, affecting one in three adults [1]. Even more alarming is that the prevalence of these diseases is rising while our knowledge of their underlying causes is fairly rudimentary.
Fig. 1 A schematic illustrating some of the targets known to modulate joint pain. Neuromodulators can be released from nerve terminals as well as mast cells and macrophages to alter afferent mechanosensitivity. Endovanilloids, acid, and noxious heat can activate transient receptor potential vanilloid type 1 (TRPV1) ion channels leading to the release of algogenic substance P (SP), which subsequently binds to neurokinin-1 (NK1) receptors. Proteases can cleave and stimulate protease-activated receptors (PARs). Thus far, PAR2and PAR4have been shown to sensitize joint primary afferents. The endocannabinoid anandamide (AE) is produced on demand and synthesized from N-arachidonoyl phosphatidylethanolamine (NAPE) under the enzymatic action of phospholipases. A portion of AE then binds to cannabinoid-1 (CB1) receptors leading to neuronal desensitization. Unbound AE is rapidly taken up by an anandamide membrane transporter (AMT)before being broken down by a fatty acid amide hydrolase (FAAH)into ethanolamine (Et) and arachidonic acid (AA). The cytokines tumor necrosis factor-?(TNF-?), interleukin-6 (IL-6) and interleukin1-beta (IL-1?) Can bind to their respective receptors to enhance pain transmission. Finally, tetrodotoxin (TTX)-resistant sodium channels (Nav1.8) are involved in neuronal sensitization.
Patients yearn for their chronic pain to disappear; however, currently prescribed analgesics are largely ineffective and are accompanied by a wide range of unwanted side effects. As such, millions of people worldwide are suffering from the debilitating effects of joint pain, for which there is no satisfactory treatment [2].
More than 100 different forms of arthritis have osteoarthritis (OA) being the most common. OA is a progressively degenerative joint disease that causes chronic pain and loss of function. Commonly, OA is the inability of the joint to repair damage effectively in response to excessive forces being placed on it. The biological and psychosocial factors that comprise chronic OA pain are not well understood, although ongoing research unravels the complex nature of disease symptoms [2]. Current therapeutics, such as non-steroidal anti-inflammatory drugs (NSAIDs), provide some symptomatic relief, reducing the pain for short periods of time, but do not alleviate pain across the patient’s lifespan. Furthermore, high-dose NSAIDs cannot be taken repeatedly over many years, as this can lead to renal toxicity and gastrointestinal bleeding.
Traditionally, arthritis research has focused largely on the articular cartilage as a primary target for the therapeutic development of novel OA drugs for disease modification. This chondrogenic focus has shed new light on the intricate biochemical and biomechanical factors that influence chondrocyte behavior in diseased joints. However, as the articular cartilage is aneural and avascular, this tissue is unlikely to be the source of OA pain. This fact, coupled with the findings that there is no correlation between the damage of articular cartilage and pain in OA patients [3,4] or preclinical models of OA [5], has caused a shift in focus to develop drugs for effective pain control. This article will review the latest findings in joint pain research and highlight some of the emerging targets that may be the future of arthritis pain management (summarized in Fig. 1)
Cytokines
The actions of various cytokines in joint neurophysiology studies have featured quite prominently recently. Interleukin-6 (IL-6), for example, is a cytokine that typically binds to the membrane-bound IL-6 receptor (IL-6R). IL-6 can also signal by binding with a soluble IL-6R (SIL-6R) to produce an IL-6/sIL-6R complex. This IL-6/sIL-6R complex subsequent lybinds to a transmembrane glycoprotein subunit 130(gp130), thereby allowing IL-6 to signal in cells that do not constitutively express membrane-bound IL-6R [25,26]. IL-6 and SIL-6R are key players in systemic inflammation and arthritis, as upregulation of both has been found in RA patients’ serum and synovial fluid [27,29]. Recently, Vazquez et al.observed that co-administration of IL-6/sIL-6R into rat knees caused inflammation-evoked pain, as revealed by an increase in the response of spinal dorsal horn neurons to mechanical stimulation of the knee and other parts of the hindlimb [30]. Spinal neuron hyperexcitability was also seen when IL-6/sIL-6R was applied locally to the spinal cord. Spinal application of soluble gp130 (which would mop up IL-6/sIL-6R complexes, thereby reducing trans-signaling) inhibited IL-6/sIL-6R-induced central sensitization. However, acute application of soluble gp130 alone did not reduce the neuronal responses to already established joint inflammation.
The transient receptor potential (TRP) channels are non-selective cation channels that act as integrators of various physiological and pathophysiological processes. In addition to thermosensation, chemosensation, and mechanosensation, TRP channels are involved in the modulation of pain and inflammation. For example, TRP vanilloid-1 (TRPV1) ion channels have been shown to contribute to joint inflammatory pain as thermal hyperalgesia was not evocable in TRPV1 mono arthritic mice [31]. Similarly, TRP ankyrin-1 (TRPA1)ion channels are involved in arthritic mechano hypersensitivity as blockade of the receptor with selective antagonists attenuated mechanical pain in the Freunds complete adjuvant model inflammation [32,33]. Further evidence thatTRPV1 may be involved in the neurotransmission of OA pain comes from studies in which neuronal TRPV1 expression is elevated in the sodium monoiodoacetate model of OA [34]. In addition, systemic administration of the TRPV1 antagonist A-889425 reduced the evoked and spontaneous activity of spinal-wide dynamic range and nociception-specific neurons in the monoiodoacetate model [35]. These data suggest that endovanilloids could be involved in central sensitization processes associated with OA pain.
There are currently known to be at least four polymorphisms in the gene that encodes TRPV1, leading to an alteration in the structure of the ion channel and impaired function. One particular polymorphism (rs8065080) alters the sensitivity of TRPV1 to capsaicin, and individuals carrying this polymorphism are less sensitive to thermal hyperalgesia [36]. A recent study examined whether OA patients with the rs8065080 polymorphism experienced altered pain perception based on this genetic anomaly. The research team found that patients with asymptomatic knee OA were more likely to carry the rs8065080 gene than patients with painful joints [37]. This observation indicates that OA patients with normal functioning; TRPV1 channels have an increased risk of joint pain and re-affirms the potential involvement of TRPV1 in OA pain perception.
Conclusion
While the hurdle of treating arthritis pain effectively remains, great leaps are being made in our understanding of the neurophysiological processes responsible for the generation of joint pain. New targets are being discovered continually, while the mechanisms behind known pathways are being further defined and refined. Targeting one specific receptor or ion channel is unlikely to be the solution to normalizing joint pain, but rather a polypharmacy approach is indicated in which various mediators are used in combination during specific phases of the disease. Unraveling the functional circuitry at each level of the pain pathway will also improve our knowledge of how joint pain is generated. For example, identifying the peripheral mediators of joint pain will allow us to control nociception within the joint and likely avoid the central side effects of systemically administered pharmacotherapeutics.
FACETOGENIC PAIN
FACET SYNDROME & FACETOGENIC PAIN
Facet syndrome is an articular disorder related to the lumbar facet joints and their innervations and produces both local and radiating facetogenic pain.
Excessive rotation, extension, or flexion of the spine (repeated overuse) can result in degenerative changes to the joint’s cartilage. In addition, itt may involve degenerative changes to other structures, including the intervertebral disc.
CERVICAL FACET SYNDROME & FACETOGENIC PAIN
Axial neck pain (rarely radiating past the shoulders), most common unilaterally.
Pain with and/or limitation of extension and rotation
Tenderness upon palpation
Radiating facetogenic pain locally or into the shoulders or upper back, and rarely radiate in the front or down an arm or into the fingers as a herniated disc might.
LUMBAR FACET SYNDROME & FACETOGENIC PAIN
Pain or tenderness in the lower back.
Local tenderness/stiffness alongside the spine in the lower back.
Pain, stiffness, or difficulty with certain movements (such as standing up straight or getting up from a chair.
Pain upon hyperextension
Referred pain from upper lumbar facet joints can extend into the flank, hip, and upper lateral thigh.
Referred pain from lower lumbar facet joints can penetrate deep into the thigh, laterally and/or posteriorly.
L4-L5 and L5-S1 facet joints can refer to pain extending into the distal lateral leg, and in rare instances, to the foot
EVIDENCE-BASED MEDICINE
Evidence-based Interventional Pain Medicine according to Clinical Diagnoses
12. Pain Originating from the Lumbar Facet Joints
Abstract
Although the existence of a facet syndrome had long been questioned, it is now generally accepted as a clinical entity. Depending on the diagnostic criteria, the zygapophysial joints account for between 5% and 15% of cases of chronic, axial low back pain. Most commonly, facetogenic pain results from repetitive stress and/or cumulative low-level trauma, leading to inflammation and stretching of the joint capsule. The most frequent complaint is axial low back pain with referred pain perceived in the flank, hip, and thigh. No physical examination findings are pathognomonic for diagnosis. The strongest indicator for lumbar facetogenic pain is pain reduction after anesthetic blocks of the rami mediales (medial branches) of the rami dorsales that innervate the facet joints. Because false-positive and, possibly, false-negative results may occur, results must be interpreted carefully. In patients with injection-confirmed zygapophysial joint pain, procedural interventions can be undertaken in the context of a multidisciplinary, multimodal treatment regimen that includes pharmacotherapy, physical therapy, and regular exercise, and, if indicated, psychotherapy. Currently, the gold standard for treating facetogenic pain is radiofrequency treatment (1 B+). The evidence supporting intra-articular corticosteroids is limited; hence, this should be reserved for those who do not respond to radiofrequency treatment (2 B1).
Facetogenic Pain emanating from the lumbar facet joints is a common cause of low back pain in the adult population. Goldthwaite was the first to describe the syndrome in 1911, and Ghormley is generally credited with coining the term �facet syndrome� in 1933. Facetogenic pain is defined as pain that arises from any structure that is part of the facet joints, including the fibrous capsule, synovial membrane, hyaline cartilage, and bone.35
More commonly, it is the result of repetitive stress and/or cumulative low-level trauma. This leads to inflammation, which can cause the facet joint to be filled with fluid and swell, resulting in stretching of the joint capsule and subsequent pain generation.27 Inflammatory changes around the facet joint can also irritate the spinal nerve via foraminal narrowing, resulting in sciatica. In addition, Igarashi et al.28 found that inflammatory cytokines released through the ventral joint capsule in patients with zygapophysial joint degeneration may be partially responsible for the neuropathic symptoms in individuals with spinal stenosis. Predisposing factors for zygapophysial joint pain include spondylolisthesis/lysis, degenerative disc disease, and advanced age.5
I.C ADDITIONAL TESTS
The prevalence rate of pathological changes in the facet joints on radiological examination depends on the mean age of the subjects, the radiological technique used, and the definition of abnormality. Degenerative facet joints can be best visualized via computed tomography (CT) examination.49
NEUROPATHIC PAIN
Pain initiated or caused by a primary lesion or dysfunction in the somatosensory nervous system.
Neuropathic pain is usually chronic, difficult to treat, and often resistant to standard analgesic management.
Abstract
Neuropathic pain is caused by a lesion or disease of the somatosensory system, including peripheral fibers (A?, A? and C fibers) and central neurons, and affects 7-10% of the general population. Multiple causes of neuropathic pain have been described. Its incidence is likely to increase due to the aging global population, increased diabetes mellitus, and improved survival from cancer after chemotherapy. Indeed, imbalances between excitatory and inhibitory somatosensory signaling, alterations in ion channels, and variability in how pain messages are modulated in the central nervous system all have been implicated in neuropathic pain. Furthermore, the burden of chronic neuropathic pain seems to be related to the complexity of neuropathic symptoms, poor outcomes, and difficult treatment decisions. Importantly, quality of life is impaired in patients with neuropathic pain due to increased drug prescriptions and visits to health care providers and the morbidity from the pain itself and the inciting disease. Despite challenges, progress in understanding the pathophysiology of neuropathic pain is spurring the development of new diagnostic procedures and personalized interventions, which emphasize the need for a multidisciplinary approach to the management of neuropathic pain.
PATHOGENESIS OF NEUROPATHIC PAIN
PERIPHERAL MECHANISMS
After a peripheral nerve lesion, neurons become more sensitive and develop abnormal excitability and elevated sensitivity to stimulation.
This is known as…Peripheral Sensitization!
CENTRAL MECHANISMS
As a consequence of ongoing spontaneous activity in the periphery, neurons develop an increased background activity, enlarged receptive fields, and increased responses to afferent impulses, including normal tactile stimuli. This is known as…Central Sensitization!
Chronic neuropathic pain is more frequent in women (8% versus 5.7% in men) and in patients >50 years of age (8.9% versus 5.6% in those <49 years of age), and most commonly affects the lower back and lower limbs, neck and upper limbs24. Lumbar and cervical painful radiculopathies are probably the most frequent cause of chronic neuropathic pain. Consistent with these data, a survey of >12,000 patients with chronic pain with both nociceptive and neuropathic pain types, referred to pain specialists in Germany, revealed that 40% of all patients experienced at least some characteristics of neuropathic pain (such as burning sensations, numbness, and tingling); patients with chronic back pain and radiculopathy were particularly affected25.
The contribution of clinical neurophysiology to the comprehension of the tension-type headache mechanisms.
Abstract
So far, clinical neurophysiological studies on tension-type headache (TTH) have been conducted with two main purposes: (1) to establish whether some neurophysiological parameters may act as markers of TTH, and (2) to investigate the physiopathology of TTH. Regarding the first point, the present results are disappointing since some abnormalities found in TTH patients may also be frequently observed in migraineurs. On the other hand, clinical neurophysiology has played an important role in the debate about the pathogenesis of TTH. Studies on the exteroceptive suppression of the temporalis muscle contraction have detected a dysfunction of the brainstem excitability and suprasegmental control. A similar conclusion has been reached using trigeminocervical reflexes, whose abnormalities in TTH have suggested a reduced inhibitory activity of brainstem interneurons, reflecting abnormal endogenous pain control mechanisms. Interestingly, the neural excitability abnormality in TTH seems to be a generalized phenomenon, not limited to the cranial districts. Defective DNIC-like mechanisms have indeed been evidenced also in somatic districts by nociceptive flexion reflex studies. Unfortunately, most neurophysiological studies on TTH are marred by serious methodological flaws, which should be avoided in future research to clarify the TTH mechanisms better.
References:
Neurophysiology of arthritis pain. McDougall JJ1 Linton P.
Pain originating from the lumbar facet joints. van Kleef M1,Vanelderen P,Cohen SP,Lataster A,Van Zundert J,Mekhail N.
Neuropathic painLuana Colloca,1Taylor Ludman,1Didier Bouhassira,2Ralf Baron,3Anthony H. Dickenson,4David Yarnitsky,5Roy Freeman,6Andrea Truini,7Nadine Attal, Nanna B. Finnerup,9Christopher Eccleston,10,11Eija Kalso,12David L. Bennett,13Robert H. Dworkin,14and Srinivasa N. Raja15
The contribution of clinical neurophysiology to the comprehension of the tension-type headache mechanisms. Rossi P1, Vollono C, Valeriani M, Sandrini G.
Doctor of Chiropractic Near Me: Mike Melgoza is an active individual who engages in a variety of strenuous physical activities on a regular basis, as a result, however, he began to experience chronic pain symptoms due to improper technique and repetitive movements. Although Mike Melgoza works out of town, he visits Dr. Alex Jimenez every time he begins to experience pain to receive chiropractic care. Mike Melgoza recommends Dr. Alex Jimenez as the non-surgical choice for chronic pain. Mike Melgoza trusts Dr. Jimenez to care for his health.
Doctor Of Chiropractic Near Me
Before you go to a chiropractor to deal with your chronic pain symptoms, it’s important to understand what exactly is causing your pain. Your physician will perform a physical exam as well as some tests to help them diagnose the source of the patient’s pain. As soon as you’re diagnosed with a pain illness, your chiropractor will create a treatment program. Your treatment plan may include spinal manipulation, manual therapies, and therapeutic exercises. Work with your chiropractor to develop a treatment plan. Once your pain is fully addressed, you should be able to slowly resume daily activities.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine





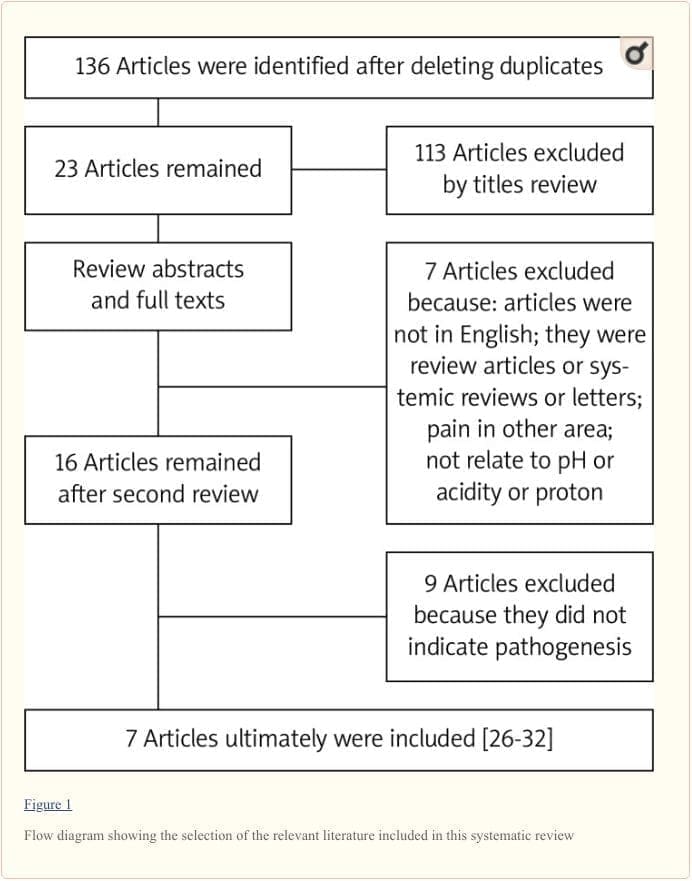

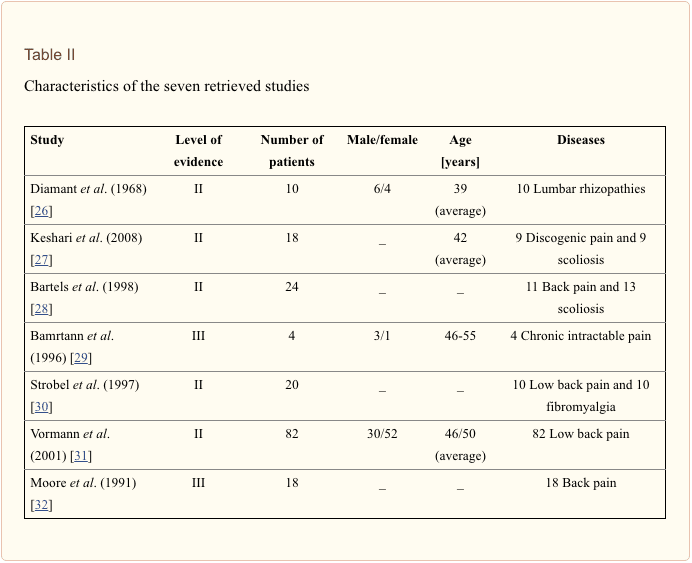


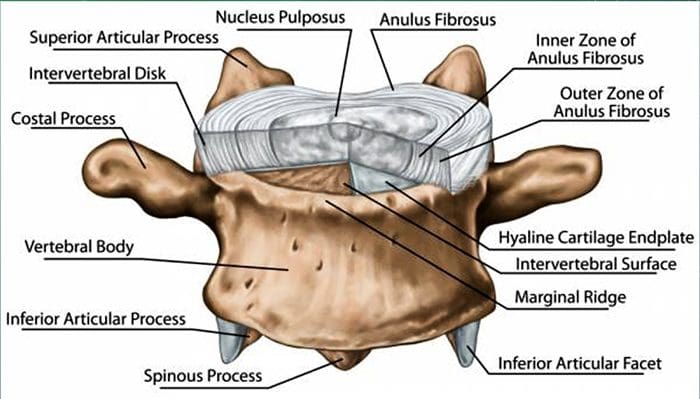
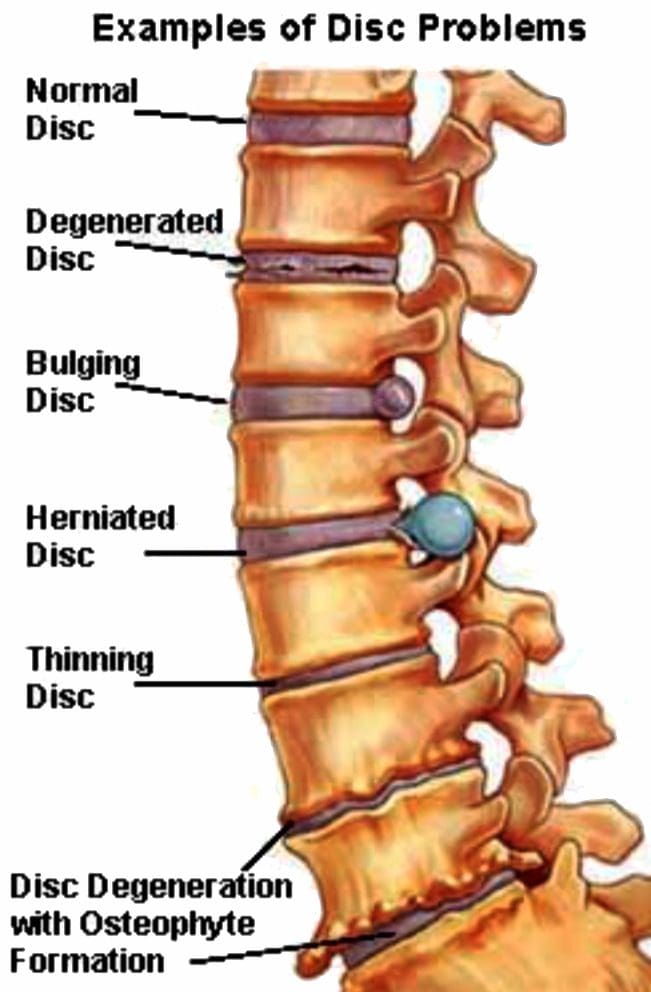 Lumbar Spine:
Lumbar Spine: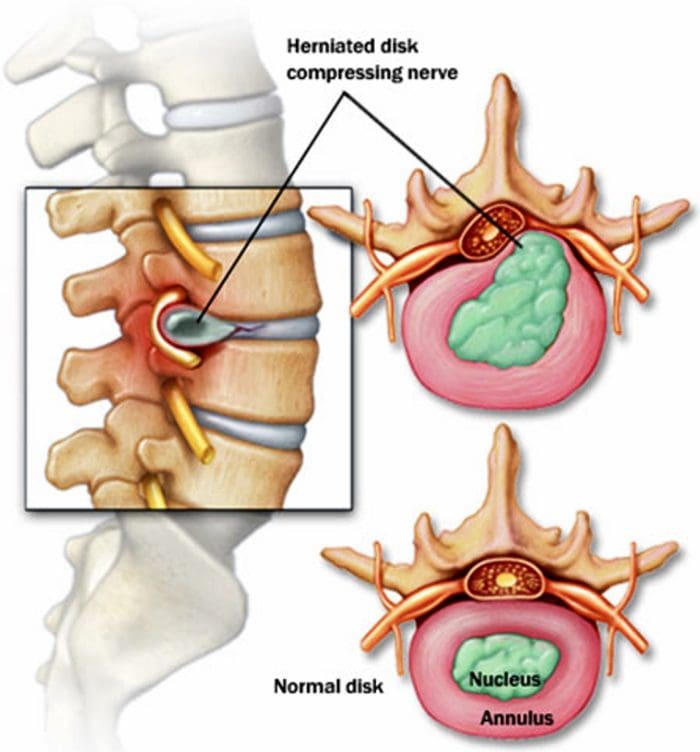
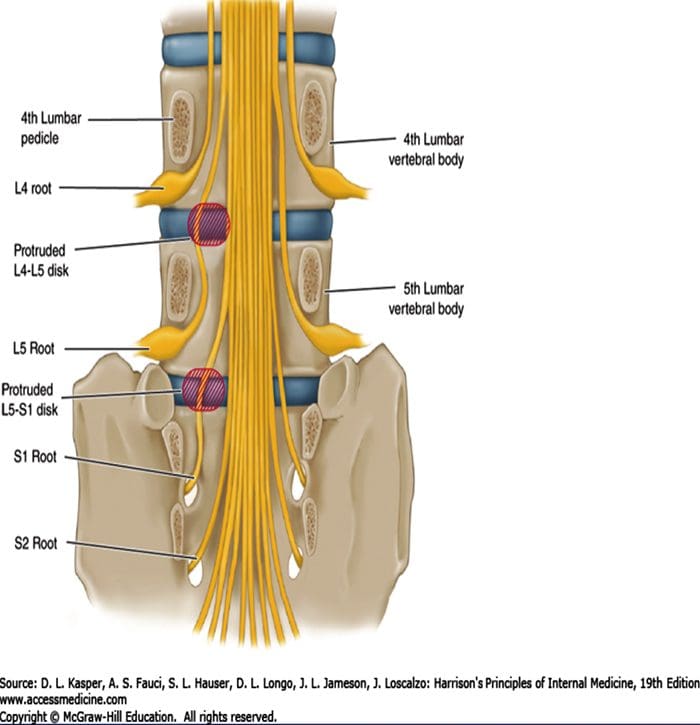
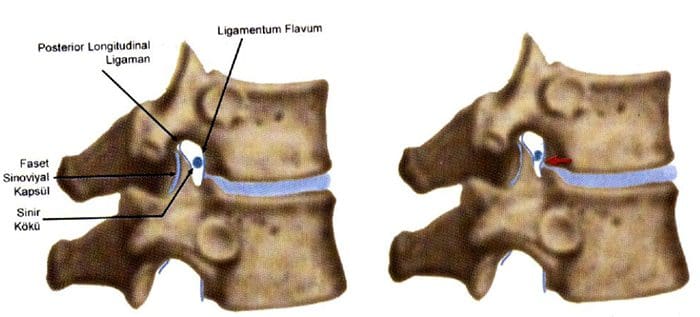
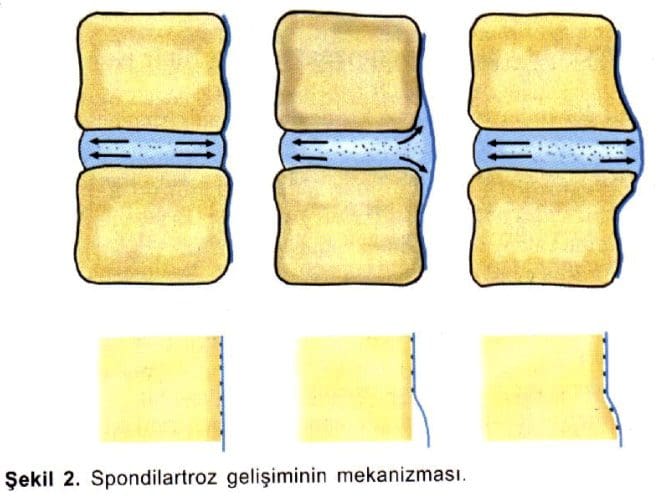
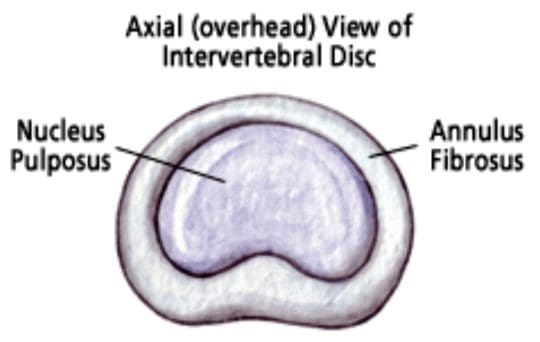
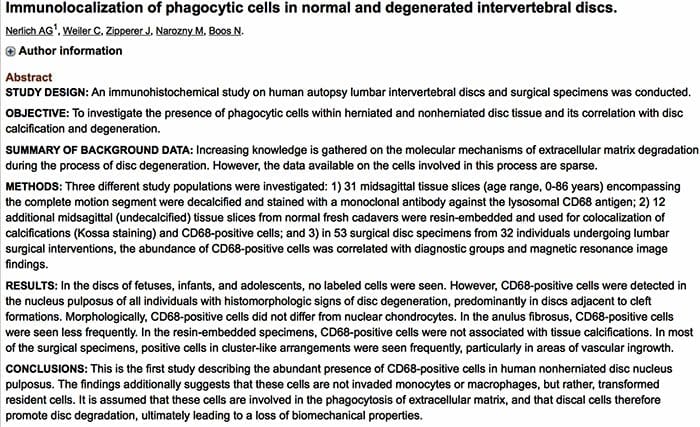
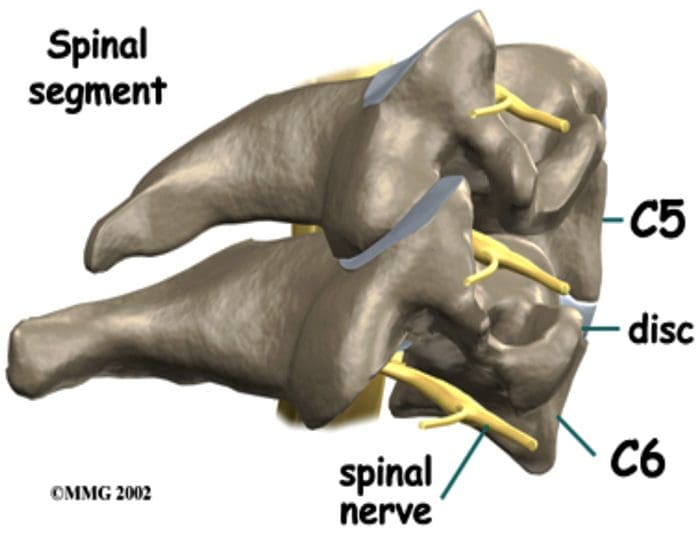

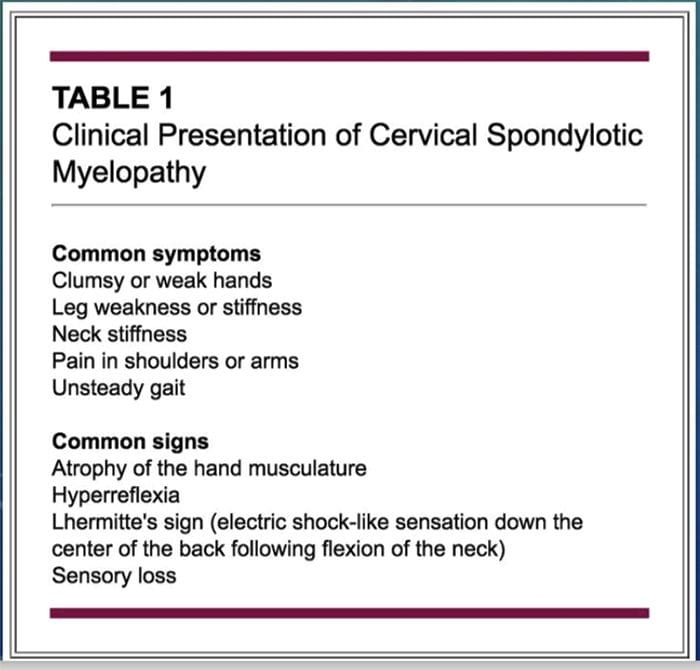
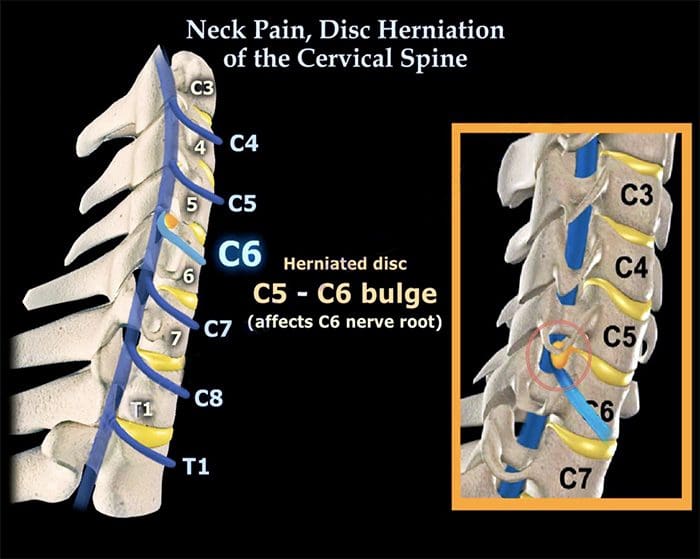
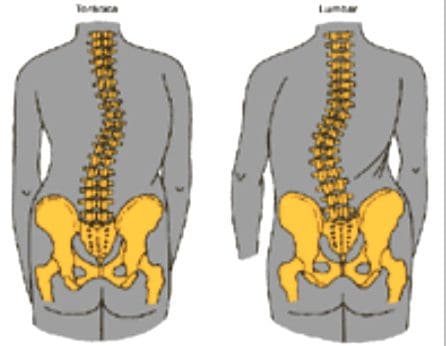
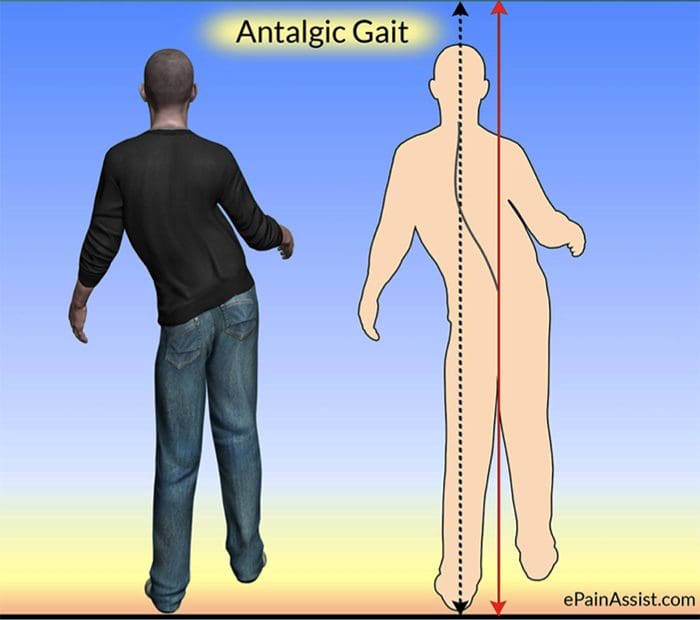
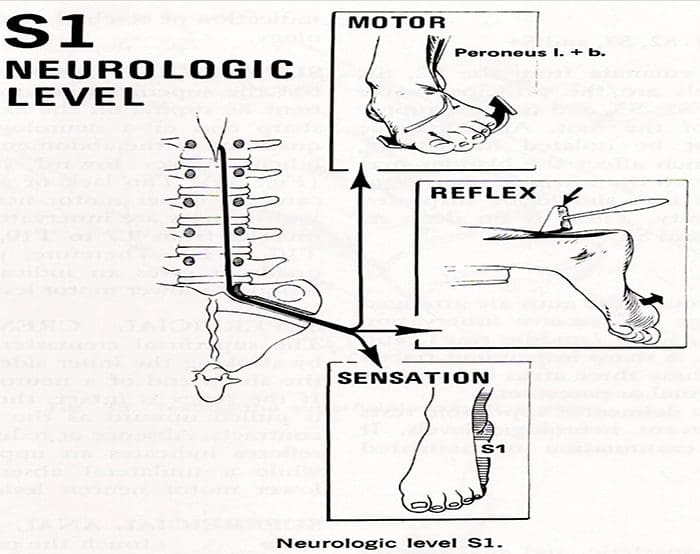
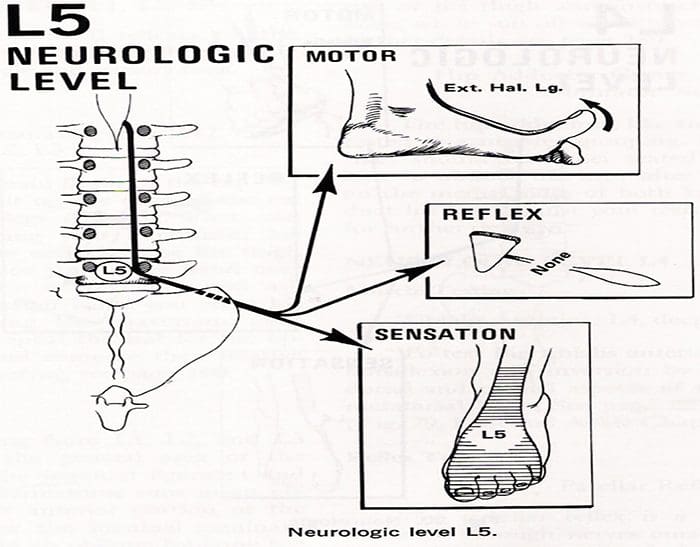
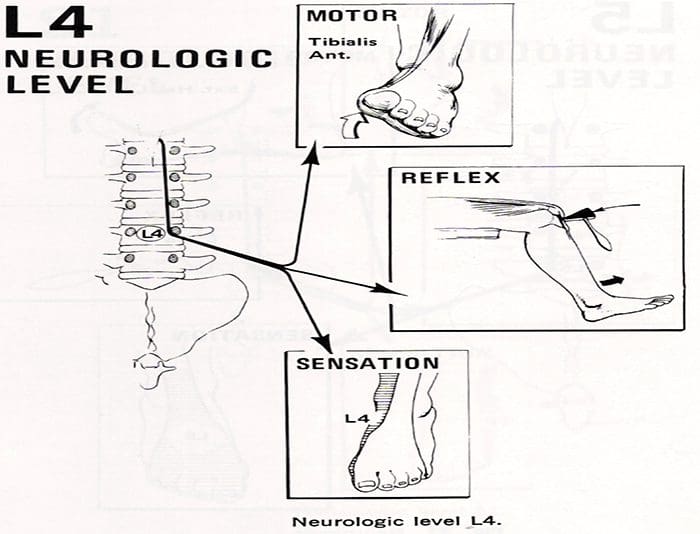
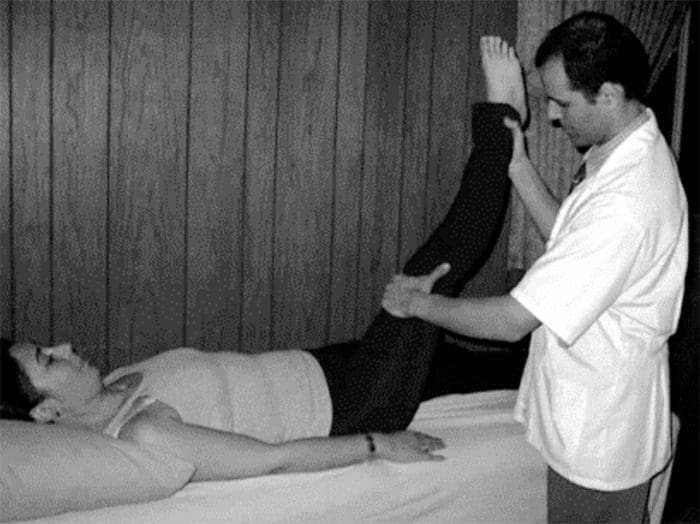
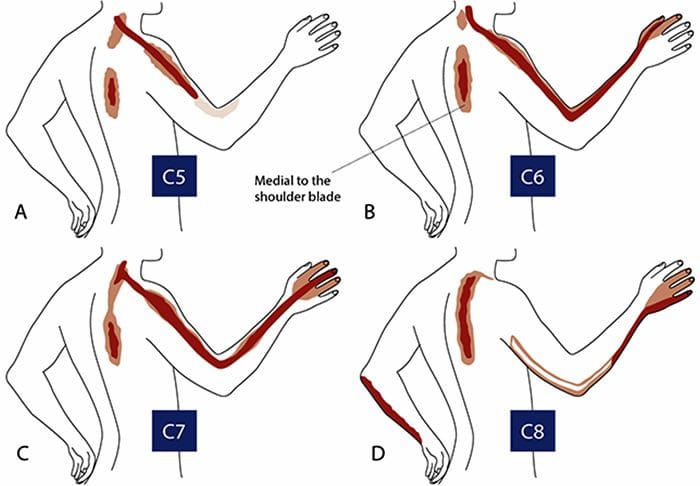
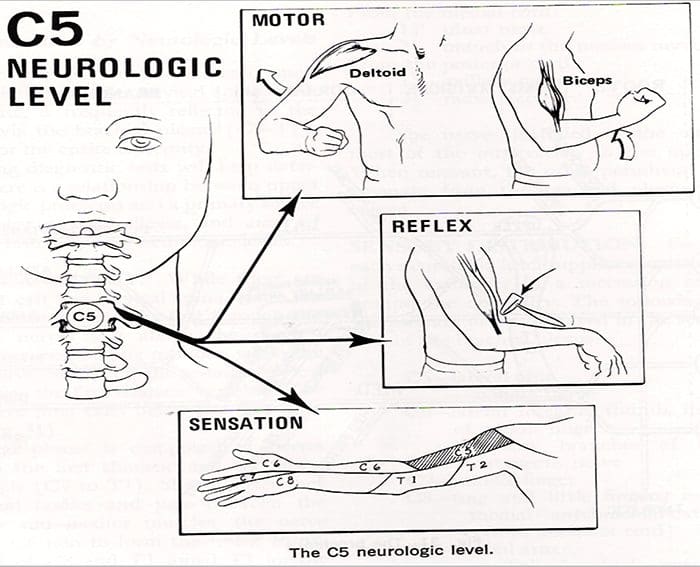
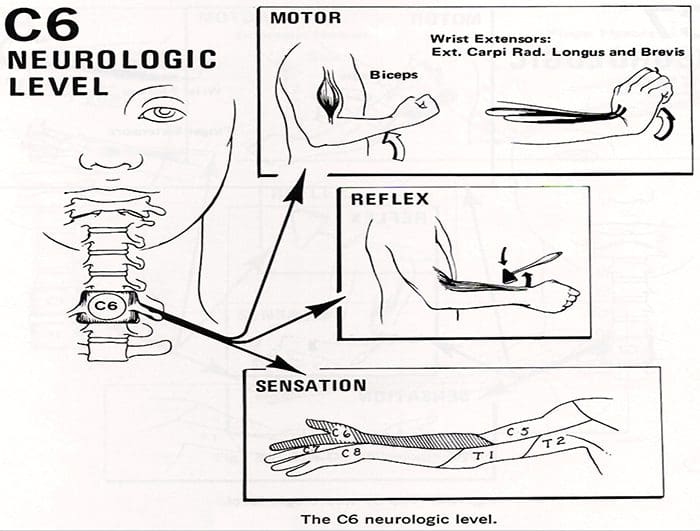
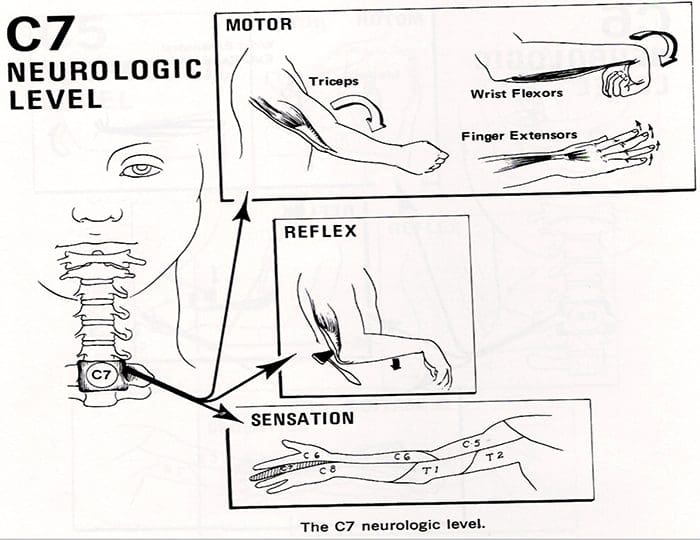
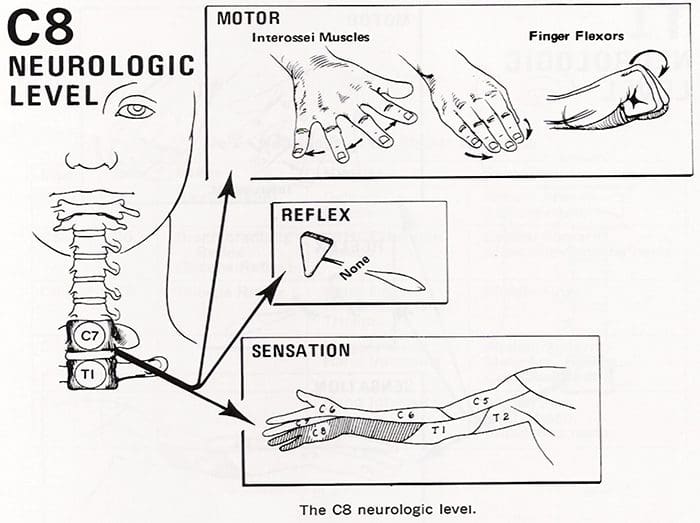



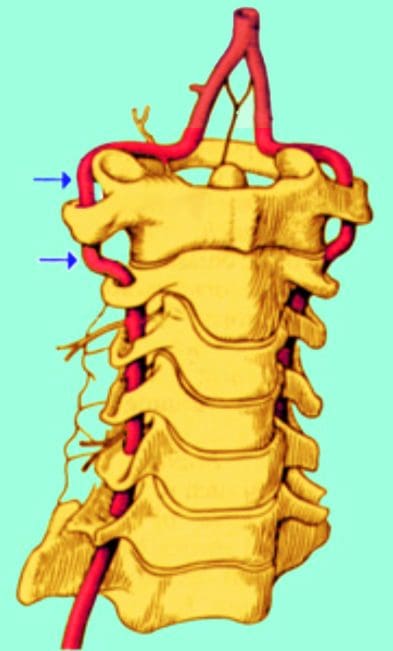
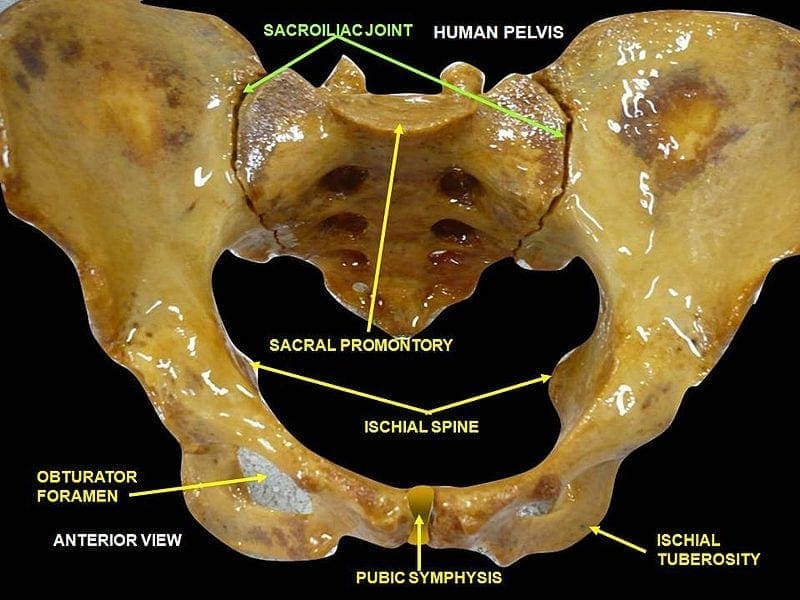

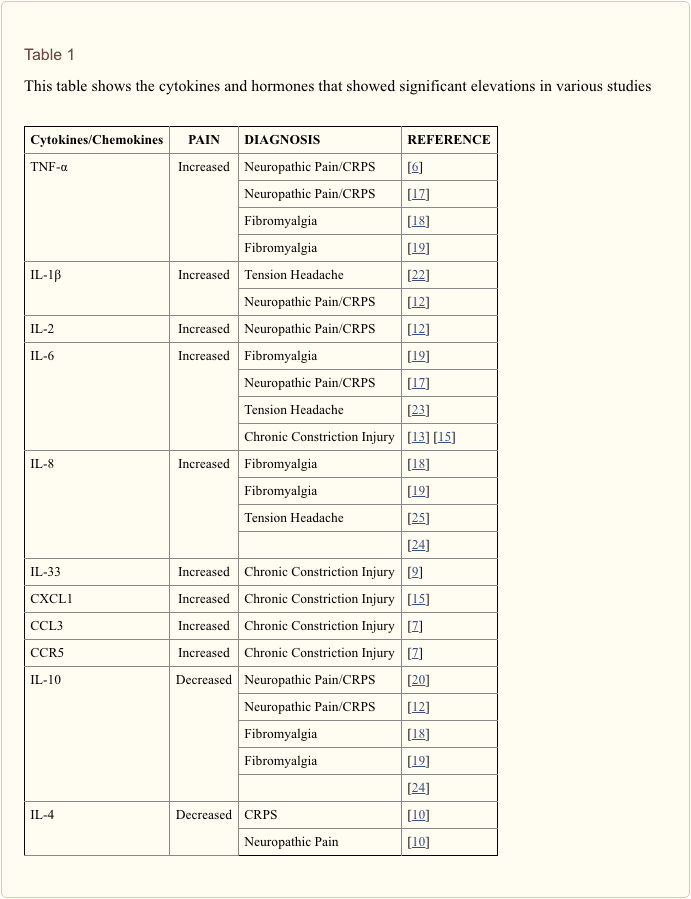


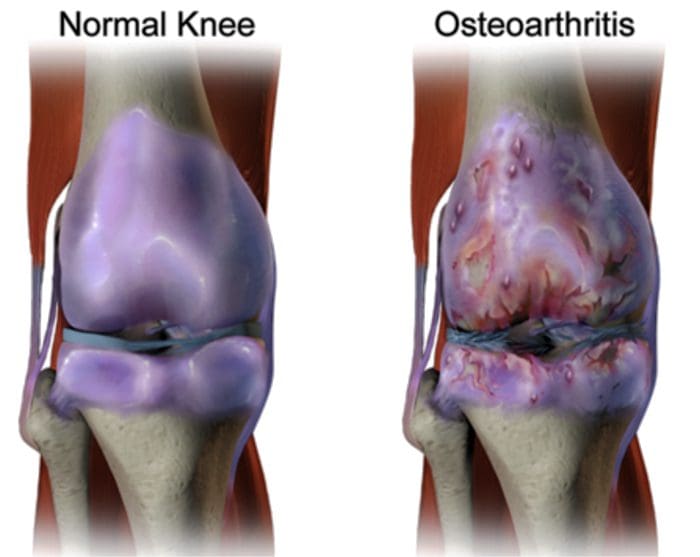
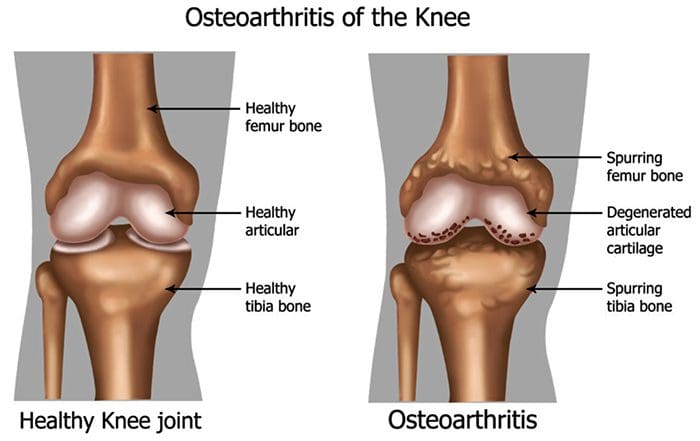
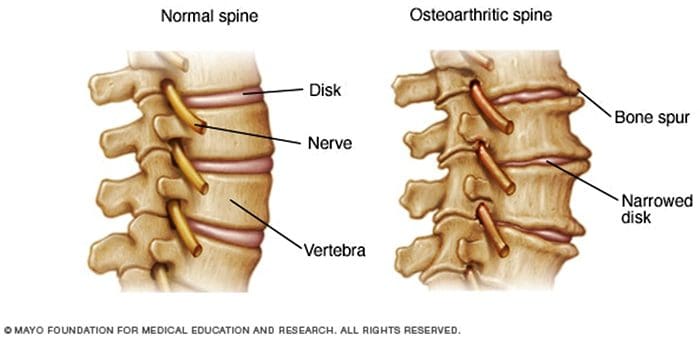
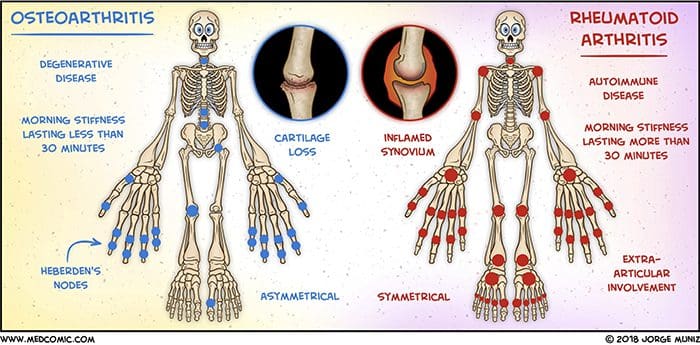 Abstract
Abstract