El Paso, TX. Chiropractor Dr. Alexander Jimenez takes a look at seizures, epilepsy, and treatment options. Seizures are defined as abnormal movements or behavior from unusual electrical activity in the brain. Seizures are a symptom of epilepsy, but not all who have epileptic fits have epilepsy. There is a group of related disorders characterized by recurrent seizures. Epilepsy is a group of disorders that are related and characterized by recurrent seizures. There are different types of epilepsy and seizures. There are medications for epilepsy that are prescribed to control seizures, and surgery is rarely needed if medication is ineffective.
Seizures & Epilepsy
Seizures occur when there is spontaneous depolarization and synchronized firing of groups of neurons, often in response to a trigger such as metabolic compromise
Any brain can have a seizure if the conditions are right
Epilepsy or seizure disorder, is the pathologically increased likelihood of seizure activity occurring in a person’s brain
Seizure Categories
General/Global onset seizures
Generalized motor seizure (Grand mal)
Absence seizure (Petite mal)
Focal onset seizures
Simple partial seizure
Motor cortex (Jacksonian)
Sensory cortex
Somatosensory
Auditory-vestibular
Visual
Olfactory-gustatory (uncinate)
Complex partial seizure (limbic)
Continuous/Ongoing seizures
Generalized (status epilepticus)
Focal (epilepticus partialis continua)
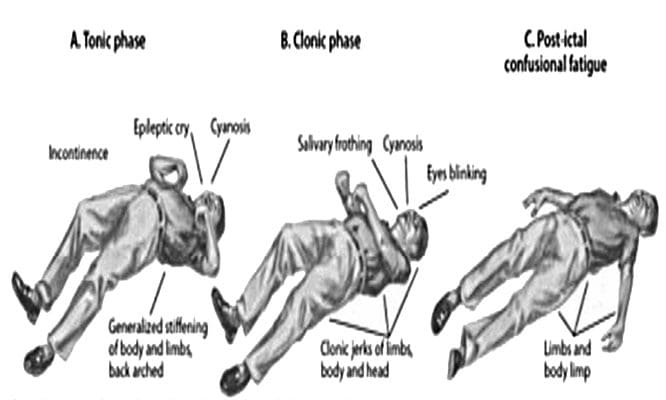
Generalized Motor Seizure
Electrical depolarization of neurons in the entire cerebral cortex simultaneously
Triggers are assumed to be outside of the cerebral cortex, such as in thalamus or brainstem
Episodes begin with loss of consciousness followed by tonic contraction (extension)
Respiration is halted, and air is expelled past the closed glottis (“cry”)
Elevated blood pressure, dilated pupils
Intermittent contraction and relaxation (clonic activity)
Usually lasts a few minutes, but for some patients can last hours or even days (status epilepticus)
Sedative withdrawal in addicts (alcohol, barbiturates, benzodiazepines)
Hypoglycemia
Hypoxia
Hyperthermia (especially patients under 4 years old)
Toxin exposure
Genetic abnormal sensitivity of neurons (rarely)
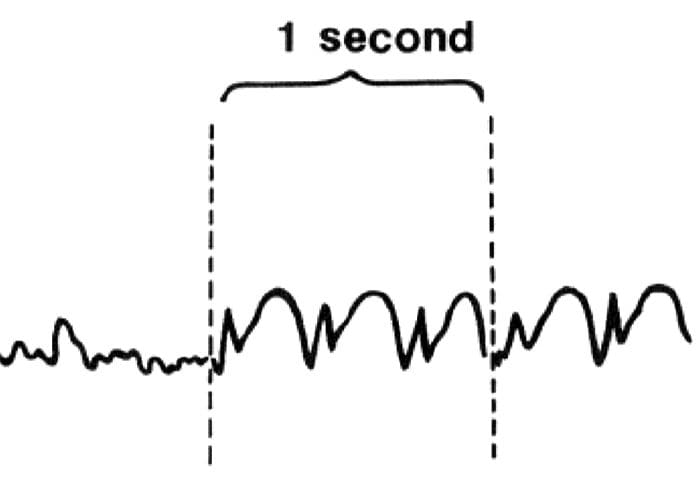
EEG Of Grand Mal Seizure
Tonic phase
Clonic phase
Postictal phase
Swenson, R. Epilepsy. 2010
Absence (Petit Mal) Seizures
Most often occur in children
Originate in the upper brainstem
Often look like losing train of thought or staring off into space
These children may go on to develop focal seizures later in life
Spontaneous remission possible as neurons mature
Absence Seizure Caught On Camera
EEG Of Petit Mal Seizure
3 spike-waves/second
Can be elicited by hyperventilation
Spike = excitation
Wave = inhibition
Swenson, R. Epilepsy. 2010
Simple Focal/Partial Seizures
May be with or without secondary generalization
Patient generally retains consciousness
Begin in a localized primary functional area of the cortex
Different symptoms and classifications depending on where in the brain the epileptiform activity originates
Sensory areas usually produce positive phenomenon (seeing lights, smelling something, etc., as opposed to lack of sensation)
Motor areas may produce positive or negative symptomology
Function of area of involvement may be reduced during the postictal phase
We refer to it as “Todd paralysis” if the primary motor cortex is involved.
Partial (Focal Seizure), 12-Year-Old Boy
Partial Seizure In The Motor Cortex
May begin as a jerking of one body area, on the side contralateral to the epileptiform activity, but may spread through the body in a homuncular pattern (Jacksonian seizure/march)
Produces paresthesia on the contralateral side to the epileptiform activity and can also spread in a homuncular pattern (march) similar to the motor type
May produce hallucinations in the contralateral visual field
Visual cortex (calcarine cortex) produced flashes, spots, and/or zig-zags of light
Visual association cortex produces more complete hallucinations, such as floating balloons, stars, and polygons
Partial Seizure in the Olfactory-Gustatory Cortex
May produce olfactory hallucinations
Likely area to spread to more generalized seizure
Complex Partial Seizures
Involves the association cortices of the frontal, temporal or parietal lobes
Similar to simple partial seizures but there may be more confusion/reduced consciousness
Limbic Cortex (hippocampus, parahippocampal temporal cortex, retro-splenial-cingulate-subcallosal cortex, orbito- frontal cortex, and insula) is the most susceptible to metabolic injury
Therefore this is the most common type of epilepsy
May produce visceral and affective symptoms (most likely), peculiar and unpleasant smells and tastes, bizarre abdominal sensations, fear, anxiety, rarely rage, and excessive sexual appetite; visceral and behavioral phenomena such as sniffing, chewing, lip smacking, salivation, excessive bowel sounds, belching, penile erection, feeding, or running
Clips Of Different Seizures In Same Child
Continuous/Ongoing Seizures
2 Types
Generalized (status epilepticus)
Focal (epilepticus partialis continua)
Continuous or recurrent seizures over 30 minutes without return to normal over the period
Prolonged seizure activity or multiple seizures occurring close together without full recovery in between
Most often seen as the result of acute cessation of anticonvulsive medications due to rebound hyperexcitability
Emotional excess, fever, or other hypermetabolic states; hypoglycemia; hypocalcemia; hypomagnesemia; hypoxemia; toxic states (e.g., tetanus, uremia, exogenous, excitatory agents such as amphetamine, aminophylline, lidocaine, penicillin), and sedative withdrawal may also predispose to ongoing seizure
Status Epilepticus
Ongoing grand mal seizure is a medical emergency because it may result in brain damage or death if the seizure is not stopped
Elevated temperature due to sustained muscle activity, hypoxia due to inadequate ventilation, and severe lactic acidosis can damage neurons
Death can result from shock and overtaxation of the cardiopulmonary system
Epilepsia Partialis Continua
Less life-threatening than status epilepticus, but seizure activity must be terminated as it may progress to generalized seizure form if allowed to go on for prolonged periods
May be a result of neoplasm, ischemia-infarction, stimulant toxicity or hyperglycemia
Treatment Of Seizures
If the seizures are the result of an underlying condition, such as infection, disorders of fluid and electrolyte balance, exogenous and endogenous toxicities, or renal failure, treatment of the underlying condition should ameliorate seizure activity
Most antiepileptic medications treat multiple seizure types—not perfect though
Some are slightly more effective (phenytoin, carbamazepine, valproic acid and phenobarbital)
Some have fewer side effects (gabapentin, lamotrigine and topiramate)
Certain medications only treat one seizure type (such as ethosuximide for absence seizures)
Sources
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
Swenson, R. Epilepsy. 2010.
Difficulty making eye contact, gestures and words at the same time
Little imitation of others
No longer uses words they used to use
Uses another person�s hand as a tool
Social Interaction
Difficulty making eye contact
Lack of joyful expression
Lack of responsiveness to name
Does not try to show you things they�re interested in
Repetitive Behaviors & Restricted Interests
Unusual way of moving their hands, fingers or body
Develops rituals, such as lining up objects or repeating things
Focuses on unusual objects
Excessive interest in a particular object or activity which interferes with social interaction
Unusual sensory interests
Under or over reaction to sensory input
ASD Diagnostic Criteria (DSM-5)
Persistent deficits in social communication and social interaction across multiple contexts, as manifested by the following, currently or by history (examples are illustrative, not exhaustive; see text):
Deficits in social-emotional reciprocity, ranging, for example, from abnormal social approach and failure of normal back-and-forth conversation; to reduced sharing of interests, emotions, or affect; to failure to initiate or respond to social interactions.
Deficits in nonverbal communicative behaviors used for social interaction, ranging, for example, from poorly integrated verbal and nonverbal communication; to abnormalities in eye contact and body language or deficits in understanding and use of gestures; to a total lack of facial expressions and nonverbal communication.
Deficits in developing, maintaining, and understand relationships, ranging, for example, from difficulties adjusting behavior to suit various social contexts; to difficulties in sharing imaginative play or in making friends; to absence of interest in peers.
ASD Diagnostic Criteria
Restricted, repetitive patterns of behavior, interests, or activities, as manifested by at least two of the following, currently or by history (examples are illustrative, not exhaustive; see text):
Stereotyped or repetitive motor movements, use of objects, or speech (e.g., simple motor stereotypes, lining up toys or flipping objects, echolalia, idiosyncratic phrases).
Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior (e.g., extreme distress at small changes, difficulties with transitions, rigid thinking patterns, greeting rituals, need to take same route or eat same food every day).
Highly restricted, fixated interests that are abnormal in intensity or focus (e.g., strong attachment to or preoccupation with unusual objects, excessively circumscribed or perseverative interests).
Hyper – or Hyporeactivity to sensory input or unusual interest in sensory aspects of the environment (e.g. apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive smelling or touching of objects, visual fascination with lights or movement).
ASD Diagnostic Criteria
Symptoms must be present in the early developmental period (but may not become fully manifest until social demands exceed limited capacities, or may be masked by learned strategies in later life).
Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning.
These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay. Intellectual disability and autism spectrum disorder frequently co-occur; to make comorbid diagnoses of autism spectrum disorder and intellectual disability, social communication should be below that expected for general developmental level.
ASD Diagnostic Criteria (ICD- 10)
A. Abnormal or impaired development is evident before the age of 3 years in at least one of the following areas:
Receptive or expressive language as used in social communication;
The development of selective social attachments or of reciprocal social interaction;
Functional or symbolic play.
B. A total of at least six symptoms from (1), (2) and (3) must be present, with at least two from (1) and at least one from each of (2) and (3)
1. Qualitative impairment in social interaction are manifest in at least two of the following areas:
a. failure adequately to use eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction;
b. failure to develop (in a manner appropriate to mental age, and despite ample opportunities) peer relationships that involve a mutual sharing of interests, activities and emotions;
c. lack of socio-emotional reciprocity as shown by an impaired or deviant response to other people�s emotions; or lack of modulation of behavior according to
social context; or a weak integration of social, emotional, and communicative behaviors;
d. lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (e.g. a lack of showing, bringing, or pointing out to other people objects of interest to the individual).
2. Qualitative abnormalities in communication as manifest in at least one of the following areas:
a. delay in or total lack of, development of spoken language that is not accompanied by an attempt to compensate through the use of gestures or mime as an alternative mode of communication (often preceded by a lack of communicative babbling);
b. relative failure to initiate or sustain conversational interchange (at whatever level of language skill is present), in which there is reciprocal responsiveness to the communications of the other person;
c. stereotyped and repetitive use of language or idiosyncratic use of words or phrases;
d. lack of varied spontaneous make-believe play or (when young) social imitative play
3. Restricted, repetitive, and stereotyped patterns of behavior, interests, and activities are manifested in at least one of the following:
a. An encompassing preoccupation with one or more stereotyped and restricted patterns of interest that are abnormal in content or focus; or one or more interests that are abnormal in their intensity and circumscribed nature though not in their content or focus;
b. Apparently compulsive adherence to specific, nonfunctional routines or rituals;
c. Stereotyped and repetitive motor mannerisms that involve either hand or finger flapping or twisting or complex whole body movements;
d. Preoccupations with part-objects of non-functional elements of play materials (such as their oder, the feel of their surface, or the noise or vibration they
generate).
C. The clinical picture is not attributable to the other varieties of pervasive developmental disorders; specific development disorder of receptive language (F80.2) with secondary socio-emotional problems, reactive attachment disorder (F94.1) or disinhibited attachment disorder (F94.2); mental retardation (F70-F72) with some associated emotional or behavioral disorders; schizophrenia (F20.-) of unusually early onset; and Rett�s Syndrome (F84.12).
Asperger�s Syndrome Diagnostic Criteria (ICD-10)
A. Qualitative impairment in social interaction, as manifested by at least two of the following:
marked impairments in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction.
failure to develop peer relationships appropriate to developmental level.
a lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (e.g. by a lack of showing, bringing, or pointing out objects of interest to other people).
lack of social or emotional reciprocity.
B. Restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by at least one of the following:
encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus.
apparently inflexible adherence to specific, nonfunctional routines or rituals.
stereotyped and repetitive motor mannerisms (e.g., hand or finger flapping or twisting, or complex whole-body movements).
persistent preoccupation with parts of objects.
C. The disturbance causes clinically significant impairment in social, occupational, or other important areas of functioning
D. There is no clinically significant general delay in language (e.g., single words used by age 2 years, communicative phrases used by age 3 years).
E. There is no clinically significant delay in cognitive development or in the development of age-appropriate self- help skills, adaptive behavior (other than social interaction), and curiosity about the environment in childhood.
F. Criteria are not met for another specific Pervasive Developmental Disorder or Schizophrenia.
Attention-Deficit/Hyperactivity Disorder (ADHD)
Inattention – gets off task easily
Hyperactivity – seems to move about constantly
Impulsivity – makes hasty actions that occur in the moment without first thinking about them
ADHD Risk Factors
Genetics
Cigarette smoking, alcohol use, or drug use during pregnancy
Exposure to environmental toxins during pregnancy
Exposure to environmental toxins, such as high levels of lead, at a young age
Somatic signs including sleep disturbances, enuresis or urinary frequency
*The onset of PANS may start with infectious agents other than strep. It also includes onset from environmental triggers or immune dysfunction
Pediatric Autoimmune Disorders Associated With Streptococcus
(PANDAS)
Presence of significant obsessions, compulsions and/or tics
Abrupt onset of symptoms or a relapsing-remitting course of symptom severity
Pre-pubertal onset
Association with streptococcal infection
Association with other neuropsychiatric symptoms (including any of the PANS �accompanying� symptoms)
PANS/PANDAS Tests
Swab/Strep culture
Blood tests for strep
Strep ASO
Anti-DNase B Titer
Streptozyme
Test for other infectious agents
MRI preferred but PET can be used if necessary
EEG
False Negatives
Not all children who have strep have elevated labs
Only 54% of children with strep showed a significant increase in ASO.
Only 45% showed an increase in anti�DNase B.
Only 63% showed an increase in either ASO and/or anti�DNase B.
Treatment Of PANS/PANDAS
Antibiotics
IVIG
Plasmaphoresis
Anti-Inflammatory protocols
Steroid medications
Omega-3’s
NSAIDS
Probiotics
Injury Medical Clinic: Chiropractor (Recommended)
Sources
�Attention Deficit Hyperactivity Disorder.� National Institute of Mental Health, U.S. Department of Health and Human Services, www.nimh.nih.gov/health/topics/attention-deficit-hyperactivity-disorder-adhd/index.shtml.
Autism Navigator, www.autismnavigator.com/.
�Autism Spectrum Disorder (ASD).� Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 29 May 2018, www.cdc.gov/ncbddd/autism/index.html.
�Introduction to Autism.� Interactive Autism Network, iancommunity.org/introduction-autism.
Shet, Anita, et al. �Immune Response to Group A Streptococcal C5a Peptidase in Children: Implications for Vaccine Development.� The Journal of Infectious Diseases, vol. 188, no. 6, 2003, pp. 809�817., doi:10.1086/377700.
�What Is PANDAS?� PANDAS Network, www.pandasnetwork.org/understanding-pandaspans/what-is-pandas/.
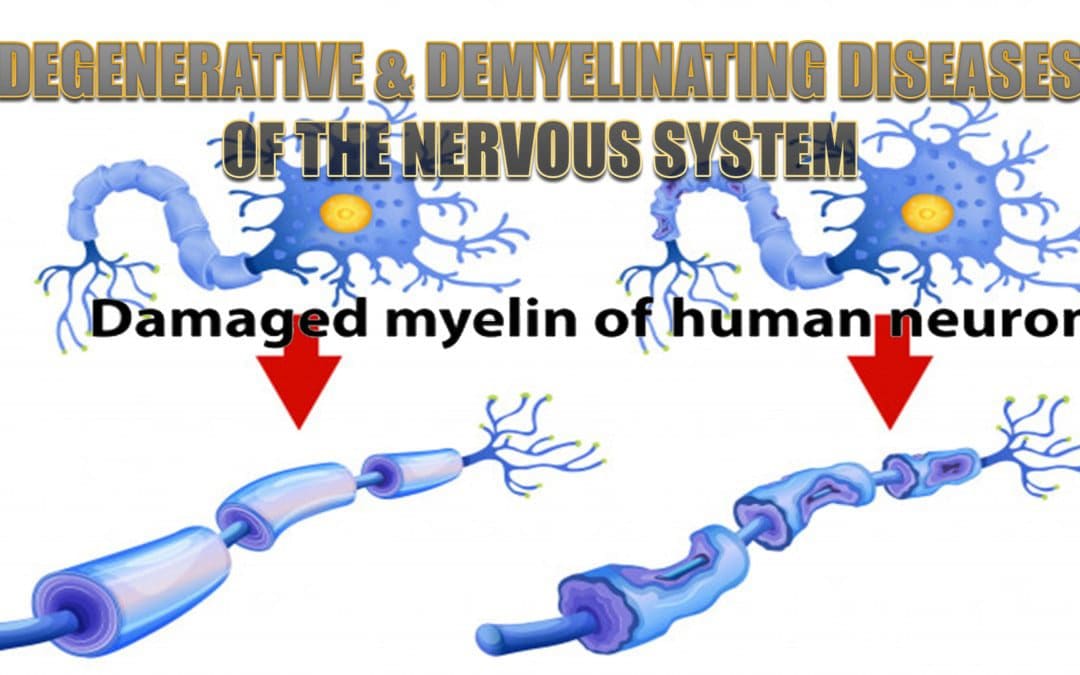
El Paso, TX. Chiropractor, Dr. Alexander Jimenez focuses on degenerative and demyelinating diseases of the nervous system, their symptoms, causes and treatment.
Degenerative & Demyelinating Diseases
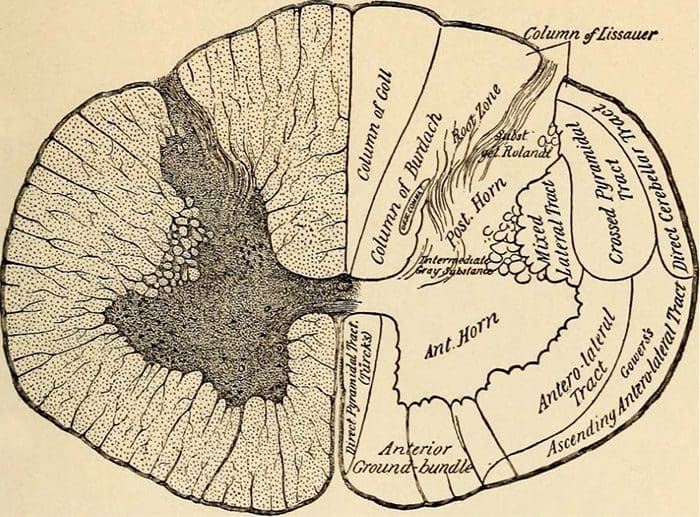
Motor Neuron Diseases
Motor weakness without sensory changes
Amyotrophic lateral sclerosis (ALS)
ALS Variants
Primary lateral sclerosis
Progressive bulbar palsy
Inherited conditions that cause anterior horn cell degeneration
Werdnig-Hoffmann disease in infants
Kugelberg-Welander disease in children and young adults
Amyotrophic Lateral Sclerosis (ALS)
Affects patients 40-60 years of age
Damage to:
Anterior horn cells
Cranial nerve motor nuclei
Corticobulbar and corticospinal tracts
Lower motor neuron findings (atrophy, fasciculations) AND upper motor neuron findings (spasticity, hyperreflexia)
Survival ~three years
Death results from weakness of the bulbar and respiratory musculature and resultant superimposed infection
ALS Variants
Usually eventually evolve into typical ALS pattern
Primary Lateral Sclerosis
Upper motor neuron signs begin first, but patients do eventually have lower motor neuron signs as well
Survival can be ten years or longer
Progressive Bulbar Palsy
Selectively involves the head and neck musculature
As more and more cortical areas become involved, the patient will develop more severe cognitive deficits, however paresis, sensory loss, or visual field defects are features.
Treatment Options
Medications that inhibit central nervous system acetylcholinesterase
Donepezil
Galantamine
Rivastigmine
Aerobic Exercise, 30 minutes daily
PT/OT care to maintain activities of daily living
Antioxidant and anti-inflammatory therapies
In advanced stages, may require full time, in home care
Vascular Dementia
Cerebral arteriosclerosis leading to stroke
Patient will have documented stroke history or signs of prior stroke (spasticity, paresis, pseudobulbar palsies, aphasia)
May be associated with Alzheimer Disease if due to amyloid angiopathy
Frontotemporal Dementia (Pick�s Disease)
Familial
Affects the frontal and temporal lobes
May be seen on imaging if advanced degeneration in these areas
Inability to compensate for perturbations, resulting in retropulsion
Mask-like facies
Mild to moderate dementia
Later in progression, due to lewy body accumulation
Pathology
Deficiency of dopamine in the striatum (caudate and putamen) of the basal ganglia
Dopamine normally has the effect of stimulating the direct circuit through the basal ganglia, while inhibiting the indirect pathway
Carbidopa/Levodopa
Most common treatment is a combination drug
Levodopa
A dopamine precursor that crosses the blood-brain barrier
Carbidopa
Dopamine decarboxylase inhibitor that does not cross the BBB
Amino acids will reduce effectiveness (competition) and so medication should be taken away from protein
Prolonged Treatment With Carbidopa/Levodopa
The patient�s capacity to store dopamine declines with medication use and therefore the improvements from the medications will last for shorter and shorter periods the longer the medication is used
Over time can result in proliferation of dopamine receptors
Peak-dose dyskinesia
Long term use puts stress on the liver
Other side effects can include nausea, hypotension and hallucinations
Other Treatment Options
Medications
Anticholinergics
Dopamine agonists
Dopanime breakdown inhibitors (Monoamine oxidase or catechol-O-methyl transferase inhibitors)
High dose glutathione
Brain balancing functional neuro-rehab exercises
Vibration
Retropulsive stimulation
Repeated reflex stimulation
Targeted CMT/OMT
Multiple System Atrophy
Symptoms of Parkinson Disease paired with one or more of the following:
Pyramidal signs (Striatonigral degeneration)
Autonomic dysfunction (ShyDrager syndrome)
Cerebellar finding (Olivopontocerebellar atrophy)
Generally not responsive to standard Parkinson Disease treatments
Progressive Supranuclear Palsy
Fast progressing degeneration involving tau proteins in many areas including the rostral midbrain
Symptoms usually start around ages 50-60
Gait difficulty
Significant dysarthria
Voluntary vertical gaze difficulty
Retrocollis (dystonic extension of the neck)
Severe dysphagia
Emotional lability
Personality changes
Cognitive difficulty
Does not respond well to standard PD treatment
Diffuse Lewy Body Disease
Progressive dementia
Severe hallucinations and possible paranoid delusions
Confusion
Parkinsonian symptoms
Multiple Sclerosis
Multiple white matter lesions (plaques of demyelination) in the CNS
Variable in size
Well-circumscribed
Visible on MRI
Optic nerve lesions are common
Peripheral nerves are not involved
Uncommon in children under 10, but usually presents before age 55
Viral infection may trigger an inappropriate immune response with antibodies to a common virus-myelin antigen
Infectious and immune mechanisms contribute
Types Of MS
Primary progressive MS (PPMS)
Secondary progressive MS (SPMS)
Relapsingremitting multiple sclerasis (RRMS)
Most common type
Can develop acutely, spontaneous appear to resolve and return
Eventually becomes like SPMS
Optic Nerve Involvement
In 40% of MS cases
Pain with eye movements
Visual field defect (central or paracentral scotoma)
Funduscopic examination
May reveal papilledema if the plaque involves the optic disk
May not appear unusual if plaques are behind the optic disk (retrobulbar neuritis)
Medial Longitudinal Fasciculus Involvement
Demyelination of the MLF results in internuclear ophthalmoplegia
During lateral gaze there is paresis of the medial rectus and nystagmus of the contralateral eye
Cerebrovascular disease is a designated group of conditions that can lead to cerebrovascular event/s, i.e. stroke. These events affect the blood supply and vessels to the brain. With a�blockage, malformation, or hemorrhage�happens,�this�prevents brain cells from getting enough oxygen, which can cause brain damage. Cerebrovascular diseases can develop in different ways. These include deep vein thrombosis (DVT) and atherosclerosis.
Types of cerebrovascular disease: Stroke, transient ischemic attack, aneurysms, and vascular malformations
In the U.S. cerebrovascular disease is the fifth most common cause of death.
Cerebrovascular Disorders
The Brain
Makes up ~2% of the body weight
Accounts for ~10% of the body�s oxygen use
Accounts for ~20% of the body�s glucose use
Receives ~20% of the cardiac output
Per minute, requires ~50-80cc of blood per 100g of grey matter brain tissue and ~17-40cc of blood per 100g of white matter
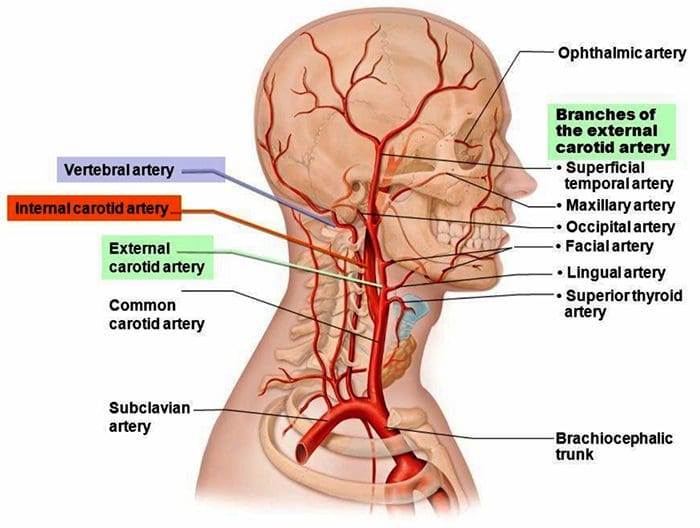
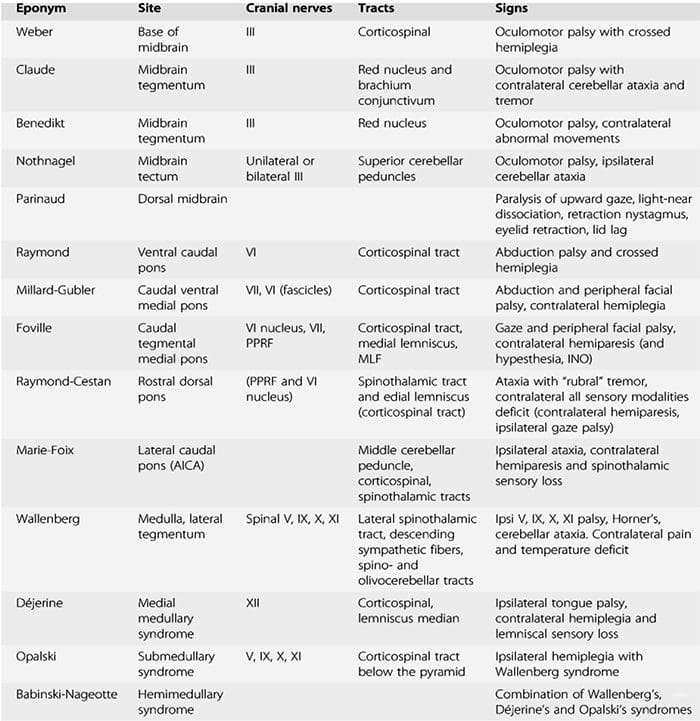
Bilateral or unilateral sensory and motor deficits
Syncope
Weakness in the distribution of a motor cranial nerve one side of the head with a contralateral hemiparesis (medial brainstem damage)
Damage to a sensory cranial nerve & Horner�s syndrome on one side of the head and loss of contralateral pain and temperature sensation in the body (lateral brainstem damage)
Long-Term Symptoms Depend On Area Affected
Monocular visual obscuration (amaurosis fugax) that is due to retinal ischemia
Rehab needs depend upon the area of brain tissue that was affected by the stroke
Speech therapy
Restriction of functioning limbs
Balance and gait exercises
Encourages neuroplastic restructuring
Symptoms may improve within the first 5 days due to reduction in edema
Edema may cause herniation through the foramen magnum which can cause brainstem compression and death � patients with this problem may require craniectomy (last resort)
Sources
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
Swenson, R. Cerebrovascular Disorders. 2010
After a neurological exam, physical exam, patient history, x-rays and any previous screening tests, a doctor may order one or more of the following diagnostic tests to determine the root of a possible/suspected neurological disorder or injury. These diagnostics generally involve neuroradiology, which uses small amounts of radioactive material to study organ function and structure and ordiagnostic imaging, which use magnets and electrical charges to study organ function.
Neurological Studies
Neuroradiology
MRI
MRA
MRS
fMRI
CT scans
Myelograms
PET scans
Many others
Magnetic Resonance Imaging (MRI)
Shows organs or soft tissue well
No ionizing radiation
Variations on MRI
Magnetic resonance angiography (MRA)
Evaluate blood flow through arteries
Detect intracranial aneurysms and vascular malformations
Magnetic resonance spectroscopy (MRS)
Assess chemical abnormalities in HIV, stroke, head injury, coma, Alzheimer’s disease, tumors, and multiple sclerosis
Functional magnetic resonance imaging (fMRI)
Determine the specific location of the brain where activity occurs
Computed Tomography (CT or CAT Scan)
Uses a combination of X-rays and computer technology to produce horizontal, or axial, images
Shows bones especially well
Used when assessment of the brain needed quickly such as in suspected bleeds and fractures
Myelogram
Contrast dye combined with CT or Xray
Most useful in assessing spinal cord
Stenosis
Tumors
Nerve root injury
Positron Emission Tomography (PET Scan)
Radiotracer is used to evaluate the metabolism of tissue to detect biochemical changes earlier than other study types
Used to assess
Alzheimer’s disease
Parkinson’s disease
Huntington’s disease
Epilepsy
Cerebrovascular accident
Electrodiagnostic Studies
Electromyography (EMG)
Nerve Conduction Velocity (NCV) Studies
Evoked Potential Studies
Electromyography (EMG)
Detection of signals arising from the depolarization of skeletal muscle
May be measured via:
Skin surface electrodes
Not used for diagnostic purposes, more for rehab and biofeedback
Needles placed directly within the muscle
Common for clinical/diagnostic EMG
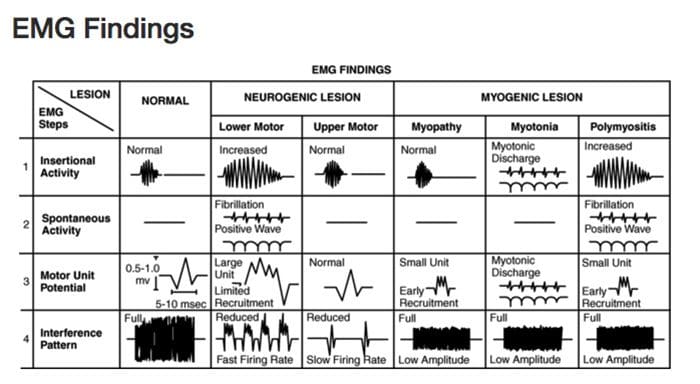
Diagnostic Needle EMG
Recorded depolarizations may be:
Spontaneous
Insertional activity
Result of voluntary muscle contraction
Muscles should be electrically silent at rest, except at the motor end-plate
Practitioner must avoid insertion in motor end-plate
At least 10 different points in the muscle are measured for proper interpretation
Procedure
Needle is inserted into the muscle
Insertional activity recorded
Electrical silence recorded
Voluntary muscle contraction recorded
Electrical silence recorded
Maximal contraction effort recorded
Samples Collected
Muscles
Innervated by the same nerve but different nerve roots
Innervated by the same nerve root but different nerves
Different locations along the course of the nerves
Helps to distinguish the level of the lesion
Motor Unit Potential (MUP)
Amplitude
Density of the muscle fibers attached to that one motor neuron
Proximity of the MUP
Recruitment pattern can also be assessed
Delayed recruitment can indicated loss of motor units within the muscle
Early recruitment is seen in myopathy, where the MUPs tend to be of low amplitude short duration
Polyphasic MUPS
Increased amplitude and duration can be the result of reinnervation after chronic denervation
Complete Potential Blocks
Demyelination of multiple segments in a row can result in a complete block of nerve conduction and therefore no resulting MUP reading, however generally changes in MUPs are only seen with damage to the axons, not the myelin
Damage to the central nervous system above the level of the motor neuron (such as by cervical spinal cord trauma or stroke) can result in complete paralysis little abnormality on needle EMG
Denervated Muscle Fibers
Detected as abnormal electrical signals
Increased insertional activity will be read in the first couple of weeks, as it becomes more mechanically irritable
As muscle fibers become more chemically sensitive they will begin to produce spontaneous depolarization activity
Fibrillation potentials
Fibrillation Potentials
DO NOT occur in normal muscle fibers
Fibrillations cannot be seen with the naked eye but are detectable on EMG
Often caused by nerve disease, but can be produced by severe muscle diseases if there is damage to the motor axons
Positive Sharp Waves
DO NOT occur in normally functioning fibers
Spontaneous depolarization due to increased resting membrane potential
Abnormal Findings
Findings of fibrillations and positive sharp waves are the most reliable indicator of damage to motor axons to the muscle after one week up to 12 months after the damage
Often termed �acute� in reports, despite possibly being visible months after onset
Will disappear if there is complete degeneration or denervation of nerve fibers
Nerve Conduction Velocity (NCV) Studies
Motor
Measures compound muscle action potentials (CMAP)
Sensory
Measures sensory nerve action potentials (SNAP)
Nerve Conduction Studies
Velocity (Speed)
Terminal latency
Amplitude
Tables of normal, adjusted for age, height and other factors are available for practitioners to make comparison
Terminal Latency
Time between stimulus and the appearance of a response
Useful in assessing demyelinative peripheral neuropathies
Sources
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
Day, Jo Ann. �Neuroradiology | Johns Hopkins Radiology.� Johns Hopkins Medicine Health Library, 13 Oct. 2016, www.hopkinsmedicine.org/radiology/specialties/ne uroradiology/index.html.
Concussions are traumatic brain injuries that affect brain function. Effects from these injuries are often temporary but can include headaches, problems with concentration, memory, balance and coordination. Concussions are usually caused by a blow to the head or violent shaking of the head and upper body. Some concussions cause loss of consciousness, but most do not. And it is possible to have a concussion and not realize it. Concussions are common in contact sports, such as football. However, most people gain a full recovery after a concussion.
Can also happen due to excessive shaking of the head or acceleration/deceleration
Mild injuries (mTBI/concussions) are the most common type of brain injury
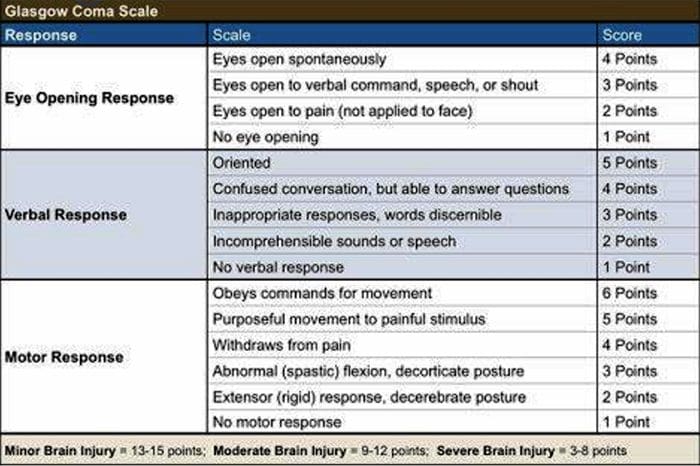
Glasgow Coma Scale
Common Causes Of Concussion
Motor vehicle collisions
Falls
Sports injuries
Assault
Accidental or intentional discharge of weapons
Impact with objects
Prevention
Prevention of concussive injuries can be paramount
Encourage Patients To Wear Helmets
Competitive sports, especially boxing, hokey, football and baseball
Horseback riding
Riding bicycles, motorcycles, ATVs, etc.
High elevation activates such as rock climbing, zip lining
Skiing, snowboarding
Encourage Patients To Wear Seatbelts
Discuss the importance of wearing seatbelts at all times in vehicles with all of your patients
Also encourage use of appropriate booster or car seats for children to ensure adequate fit and function of seat belts.
Driving Safely
Patients should never drive while under the influence of drugs, including certain medications or alcohol
Never text and drive
Make Spaces Safer For Children
Install baby gates and window latches in the home
May in areas with shock-absorbing material, such as hardwood mulch or sand
Supervise children carefully, especially when they�re near water
Prevent Falls
Clearing tripping hazards such as loose rugs, uneven flooring or walkway clutter
Using nonslip mats in the bathtub and on shower floors, and installing grab bars next to the toilet, tub and shower
Ensure appropriate footwear
Installing handrails on both sides of stairways
Improving lighting throughout the home
Balance training exercises
Balance Training
Single leg balance
Bosu ball training
Core strengthening
Brain balancing exercises
Concussion Verbiage
Concussion vs. mTBI (mild traumatic brain injury)
mTBI is the term being used more commonly in medical settings, but concussion is a more largely recognized term in the community by sports coaches, etc.
The two terms describe the same basic thing, mTBI is a better term to use in your charting
Evaluating Concussion
Remember that there does not always have to be loss of consciousness for there to be a concussion
Post-Concussion Syndrome can occur without LOC as well
Symptoms of concussion may not be immediate and could take days to develop
Monitor for 48 post head injury watching for red flags
Blurred eyesight or other vision problems, such as dilated or uneven pupils
Confusion
Dizziness
Ringing in the ears
Nausea or vomiting
Slurred speech
Delayed response to questions
Memory loss
Fatigue
Trouble concentrating
Continued or persistent memory loss
Irritability and other personality changes
Sensitivity to light and noise
Sleep problems
Mood swings, stress, anxiety or depression
Disorders of taste and smell
Mental/Behavioral Changes
Verbal outbursts
Physical outbursts
Poor judgment
Impulsive behavior
Negativity
Intolerance
Apathy
Egocentricity
Rigidity and inflexibility
Risky behavior
Lack of empathy
Lack of motivation or initiative
Depression or anxiety
Symptoms In Children
Concussions can present differently in children
Excessive crying
Loss of appetite
Loss of interest in favorite toys or activities
Sleep issues
Vomiting
Irritability
Unsteadiness while standing
Amnesia
Memory loss and failure to form new memories
Retrograde Amnesia
Inability to remember things that happened before the injury
Due to failure in recall
Anterograde Amnesia
Inability to remember things that happened after the injury
Due to failure to formulate new memories
Even short memory losses can be predictive of outcome
Amnesia may be up to 4-10 times more predictive of symptoms and cognitive deficits following concussion than is LOC (less than 1 minute)
Return To Play Progression
Baseline: No Symptoms
As the baseline step of the Return to Play Progression, the athlete needs to have completed physical and cognitive rest and not be experiencing concussion symptoms for a minimum of 48 hours. Keep in mind, the younger the athlete, the more conservative the treatment.
Step 1: Light Aerobic Activity
The Goal: Only to increase an athlete�s heart rate.
The Time: 5 to 10 minutes.
The Activities: Exercise bike, walking, or light jogging.
Absolutely no weight lifting, jumping or hard running.
Step 2: Moderate activity
The Goal: Limited body and head movement.
The Time: Reduced from typical routine.
The Activities: Moderate jogging, brief running, moderate-intensity stationary biking, and moderate-intensity weightlifting
Step 3: Heavy, non-contact activity
The Goal: More intense but non-contact
The Time: Close to typical routine
The Activities: Running, high-intensity stationary biking, the player�s regular weightlifting routine, and non- contact sport-specific drills. This stage may add some cognitive component to practice in addition to the aerobic and movement components introduced in Steps 1 and 2.
Step 4: Practice & full contact
The Goal: Reintegrate in full contact practice.
Step 5: Competition
The Goal: Return to competition.
Microglial Priming
After head trauma microglial cells are primed and can become over active
To combat this, you must mediate the inflammation cascade
Prevent repeated head trauma
Due to priming of the foam cells, response to follow-up trauma may be far more severe and damaging
What Is Post-Concussion Syndrome (PCS)?
Symptoms following head trauma or mild traumatic brain injury, that can last weeks, months or years after injury
Symptoms persist longer than expected after initial concussion
More common in women and persons of advanced age who suffer head trauma
Severity of PCS often does not correlate to severity of head injury
PCS Symptoms
Headaches
Dizziness
Fatigue
Irritability
Anxiety
Insomnia
Loss of concentration and memory
Ringing in the ears
Blurry vision
Noise and light sensitivity
Rarely, decreases in taste and smell
Concussion Associated Risk Factors
Early symptoms of headache after injury
Mental changes such as amnesia or fogginess
Fatigue
Prior history of headaches
Evaluation Of PCS
PCS is a diagnosis of exclusion
If patient presents with symptoms after head injury, and other possible causes have been ruled out => PCS
Use appropriate testing and imaging studies to rule out other causes of symptoms
Headaches In PCS
Often �tension� type headache
Treat as you would for tension headache
Reduce stress
Improve stress coping skills
MSK treatment of the cervical and thoracic regions
Constitutional hydrotherapy
Adrenal supportive/adaptogenic herbs
Can be migraine, especially in people who had pre-existing migraine conditions prior to injury
Reduce inflammatory load
Consider management with supplements and or medications
Reduce light and sound exposure if there is sensitivity
Dizziness In PCS
After head trauma, always assess for BPPV, as this is the most common type of vertigo after trauma
Dix-Hallpike maneuver to diagnose
Epley�s maneuver for treatment
Light & Sound Sensitivity
Hypersensitivity to light and sound is common in PCS and typically exacerbates other symptoms such as headache and anxiety
Management of excess mesencephalon stimulation is crucial in such cases
Sunglasses
Other light blocking glasses
Earplugs
Cotton in ears
Treatment Of PCS
Manage each symptom individually as you otherwise would
Manage CNS inflammation
Curcumin
Boswelia
Fish oil/Omega-3s � (***after r/o bleed)
Cognitive behavioral therapy
Mindfulness & relaxation training
Acupuncture
Brain balancing physical therapy exercises
Refer for psychological evaluation/treatment
Refer to mTBI specialist
mTBI Specialists
mTBI is difficult to treat and is an entire specialty both in the allopathic and complementary medicine
Primary objective is to recognize and refer for appropriate care
Pursue training in mTBI or plan to refer to TBI specialists
Sources
�A Head for the Future.� DVBIC, 4 Apr. 2017, dvbic.dcoe.mil/aheadforthefuture.
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
�Heads Up to Health Care Providers.� Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 16 Feb. 2015, www.cdc.gov/headsup/providers/.
�Post-Concussion Syndrome.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 28 July 2017, www.mayoclinic.org/diseases-conditions/post- concussion-syndrome/symptoms-causes/syc-20353352.
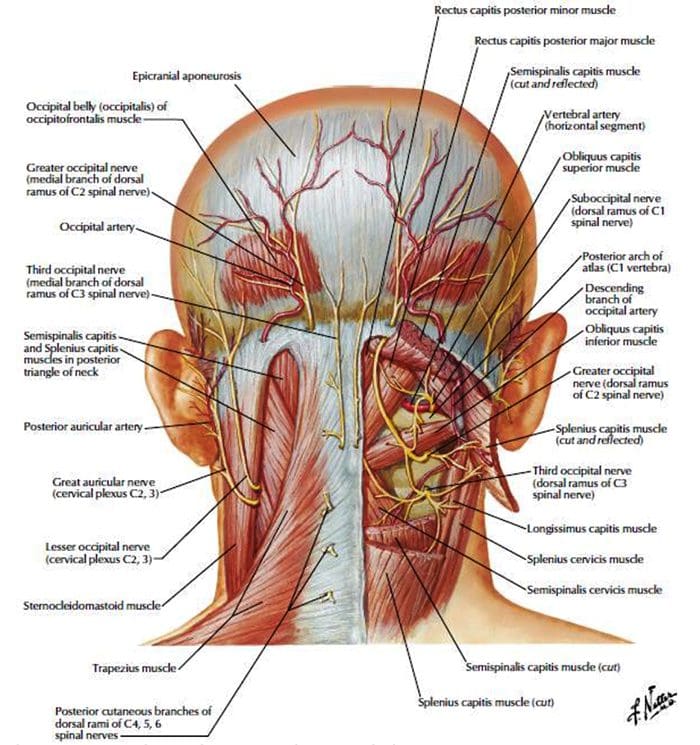
Origin: The most common cause of�migraines/headaches�can relate to neck complications. From spending excessive time looking down at a laptop, desktop, iPad, and even from constant texting, an incorrect posture for extended periods of time can begin to place pressure on the neck and upper back leading to problems that can cause headaches. The majority of these type of headaches occurs as a result of tightness between the shoulder blades, which in turn causes the muscles on the top of the shoulders to also tighten and radiate pain into the head.
Arteriovenous malformations and expanding aneurysms
Lupus cerebritis
Venous sinus thrombosis
Cervical fracture or malformation
Fracture or dislocation
Occipital neuralgia
Vertebral artery dissection
Chiari malformation
Metabolic
Hypoglycemia
Hypercapnea
Carbon monoxide
Anoxia
Anemia
Vitamin A toxicity
Glaucoma
Subarachnoid Hemorrhage
Usually due to ruptured aneurysm
Sudden onset of severe pain
Often vomiting
Patient appears ill
Often nuchal rigidity
Refer for CT and possibly lumbar puncture
Meningitis
Patient appears ill
Fever
Nuchal rigidity (except in elderly and young children)
Refer for lumbar puncture – diagnostic
Neoplasms
Unlikely cause of HA in average patient population
Mild and nonspecific head pain
Worse in the morning
May be elicited by vigorous head shaking
If focal symptoms, seizures, focal neurologic signs, or evidence of increased intracranial pressure are present rule our neoplasm
Subdural Or Epidural Hemorrhage
Due to hypertension, trauma or defects in coagulation
Most often occurs in the context of acute head trauma
Onset of symptoms may be weeks or months after an injury
Differentiate from the common post-concussion headache
Post-Concussive HA may persist for weeks or months after an injury and be accompanied by dizziness or vertigo and mild mental changes, which will all subside
Exquisite tenderness and/or swelling over the temporal or occipital arteries
Evidence of arterial insufficiency in the distribution of branches of the cranial vessels
High ESR
Cervical Region HA
Neck trauma or with symptoms or signs of cervical root or cord compression
Order MR or CT cord compression due to fracture or dislocation
Cervical instability
Order cervical spine x-rays lateral flexion and extension views
Ruling Out Dangerous HA
Rule our history of serious head or neck injury, seizures or focal neurologic symptoms, and infections that may predispose to meningitis or brain abscess
Check for fever
Measure blood pressure (concern if diastolic >120)
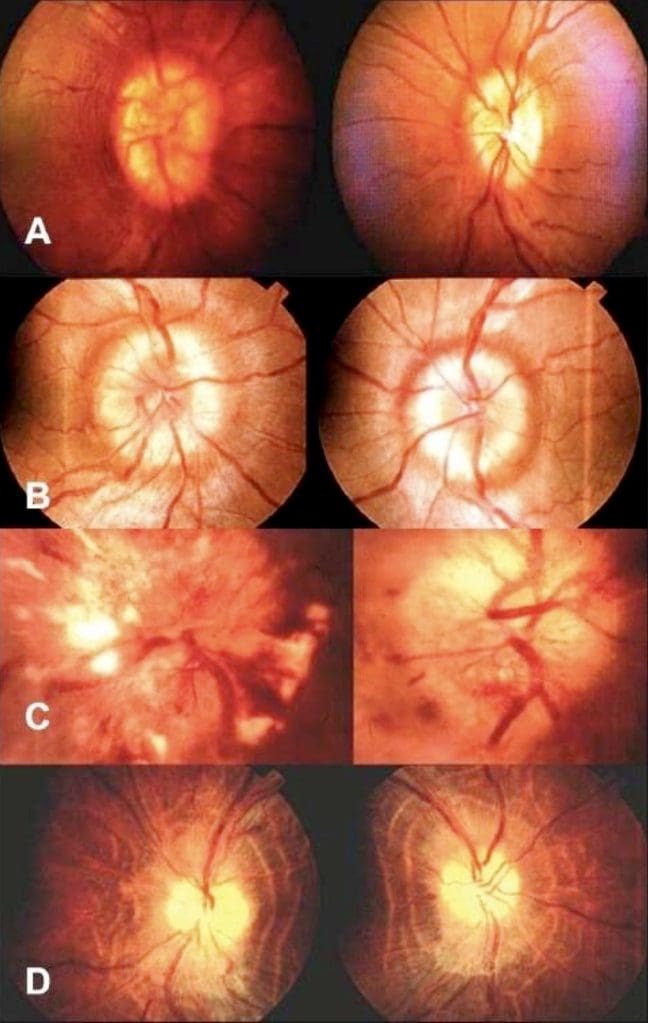
Ophthalmoscopic exam
Check neck for rigidity
Auscultate for cranial bruits.
Complete neurologic examination
If needed order complete blood cell count, ESR, cranial or cervical imaging
Episodic Or Chronic?
<15 days per month = Episodic
>15 days per month = Chronic
Migraine HA
Generally due to dilation or distension of cerebral vasculature
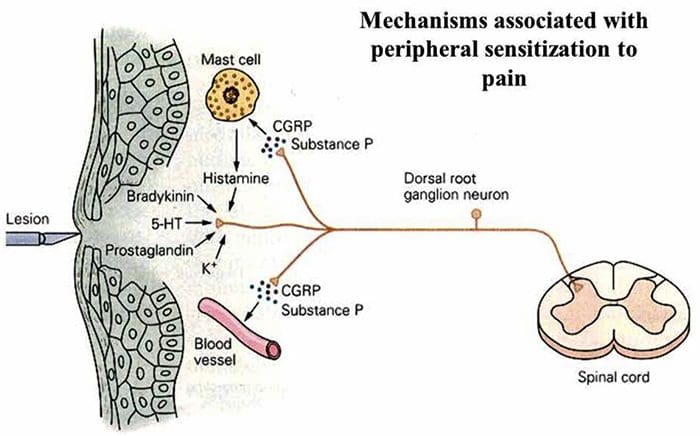
Serotonin In Migraine
AKA 5-hydroxytryptamine (5-HT)
Serotonin becomes depleted in migraine episodes
IV 5-HT can stop or reduce severity
Migraine With Aura
History of at least 2 attacks fulfilling the following criteria
One of the following fully reversible aura symptoms:
Visual
Somatic sensory
Speech or language difficulty
Motor
Brain stem
2 of the following 4 characteristics:
1 aura symptom spreads gradually over ?5 min, and/or 2 symptoms occur in succession
Each individual aura symptom lasts 5-60 min
1 aura symptom is unilateral
Aura accompanied or followed in <60 min by headache
Not better accounted for by another ICHD-3 diagnosis, and TIA excluded
Migraine Without Aura
History of at least 5 attacks fulfilling the following criteria:
Headache attacks lasting 4-72 h (untreated or unsuccessfully treated)
Unilateral pain
Pulsing/pounding quality
Moderate to severe pain intensity
Aggravation by or causing avoidance of routine physical activity
During headache nausea and/or sensitivity to light and sound
Not better accounted for by another ICHD-3 diagnosis
Cluster Headache
Severe unilateral orbital, supraorbital and/or temporal pain
�Like an ice pick stabbing me the eye�
Pain lasts 15-180 minutes
At least one of the following on the side of headache:
Conjunctival injection
Facial sweating
Lacrimation
Miosis
Nasal congestion
Ptosis
Rhinorrhea
Eyelid edema
History of similar headaches in the past
Tension Headache
Headache pain accompanied by two of the following:
Pressing/tightening (non-pulsing) quality
�Feels like a band around my head�
Bilateral location
Not aggravated by routine physical activity
Headache should be lacking:
Nausea or vomiting
Photophobia and phonophobia (one or the other may be present)
History of similar headaches in the past
Rebound Headache
Headache occurring on ?15 days a month in a patient with a pre-existing headache disorder
Regular overuse for >3 months of one or more drugs that can be taken for acute and/or symptomatic treatment of headache
Due to medication overuse/withdrawal
Not better accounted for by another ICHD-3 diagnosis
Sources
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine
 http://nanfoundation.org/neurologic-disorders/epilepsy/what-is-epilepsy
http://nanfoundation.org/neurologic-disorders/epilepsy/what-is-epilepsy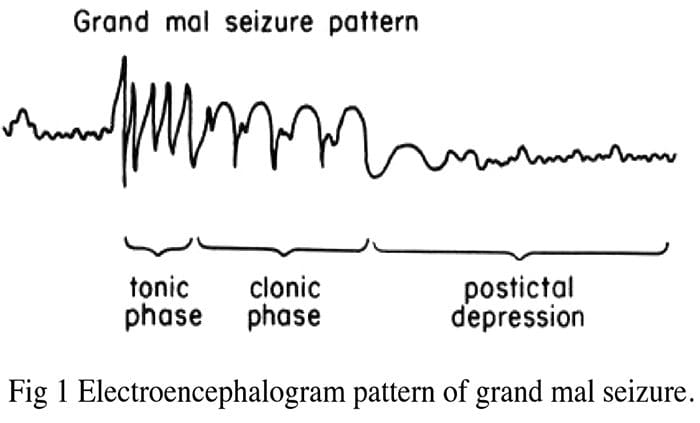
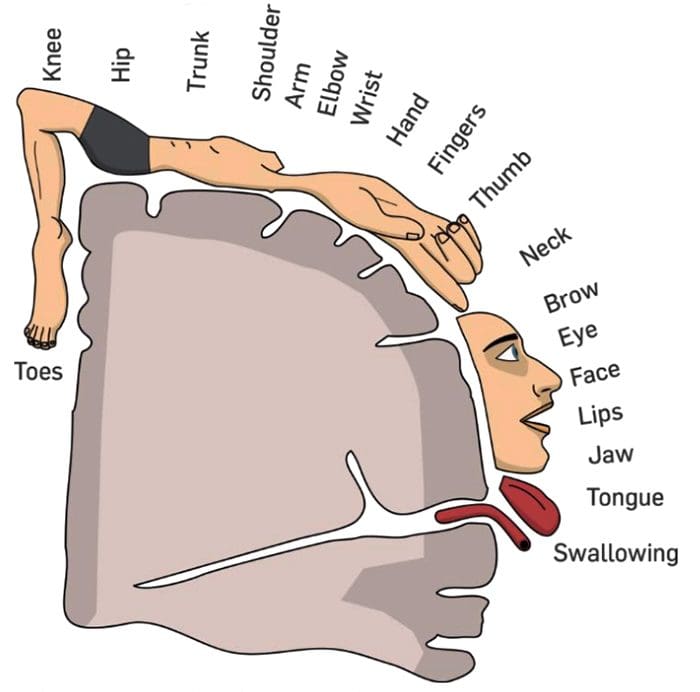
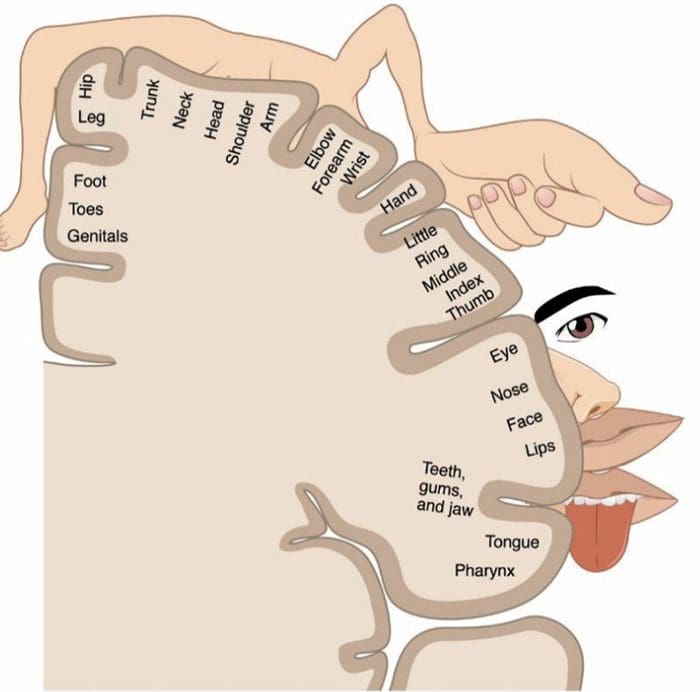 https://en.wikipedia.org/wiki/Cortical_homunculus
https://en.wikipedia.org/wiki/Cortical_homunculus
 Church, Archibald. Nervous and Mental Diseases. W.B. Saunders Co., 1923.
Church, Archibald. Nervous and Mental Diseases. W.B. Saunders Co., 1923.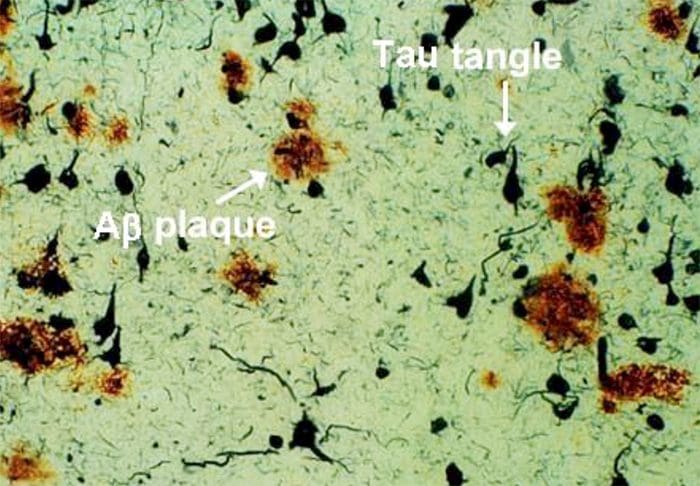 http://sage.buckinstitute.org/wp-content/uploads/2015/01/plaque-tanglesRNO.jpg
http://sage.buckinstitute.org/wp-content/uploads/2015/01/plaque-tanglesRNO.jpg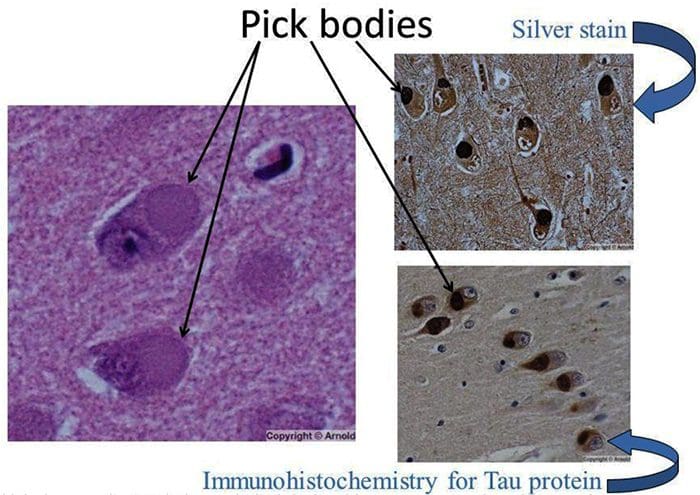 http://slideplayer.com/9467158/29/images/57/Pick+bodies+Silver+stain+Immunohistochemistry+for+Tau+protein.jpg
http://slideplayer.com/9467158/29/images/57/Pick+bodies+Silver+stain+Immunohistochemistry+for+Tau+protein.jpg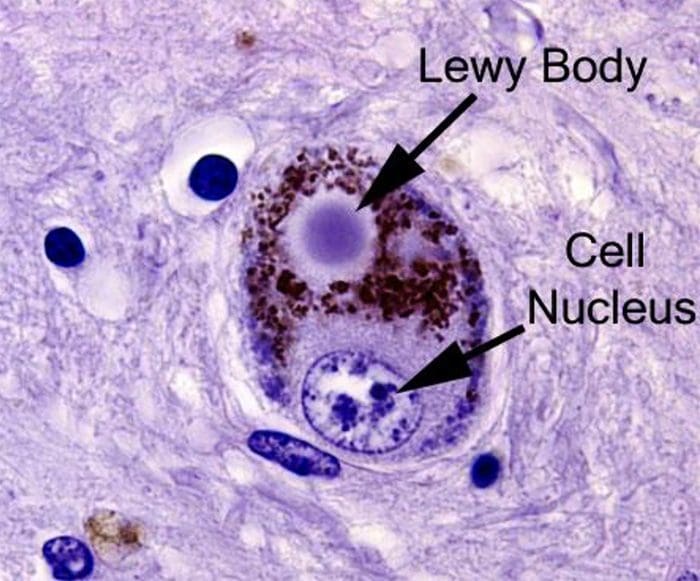 https://scienceofpd.files.wordpress.com/2017/05/9-lb2.jpg
https://scienceofpd.files.wordpress.com/2017/05/9-lb2.jpg
 http://madeinkibera.com/lingual-arterie-anatomie
http://madeinkibera.com/lingual-arterie-anatomie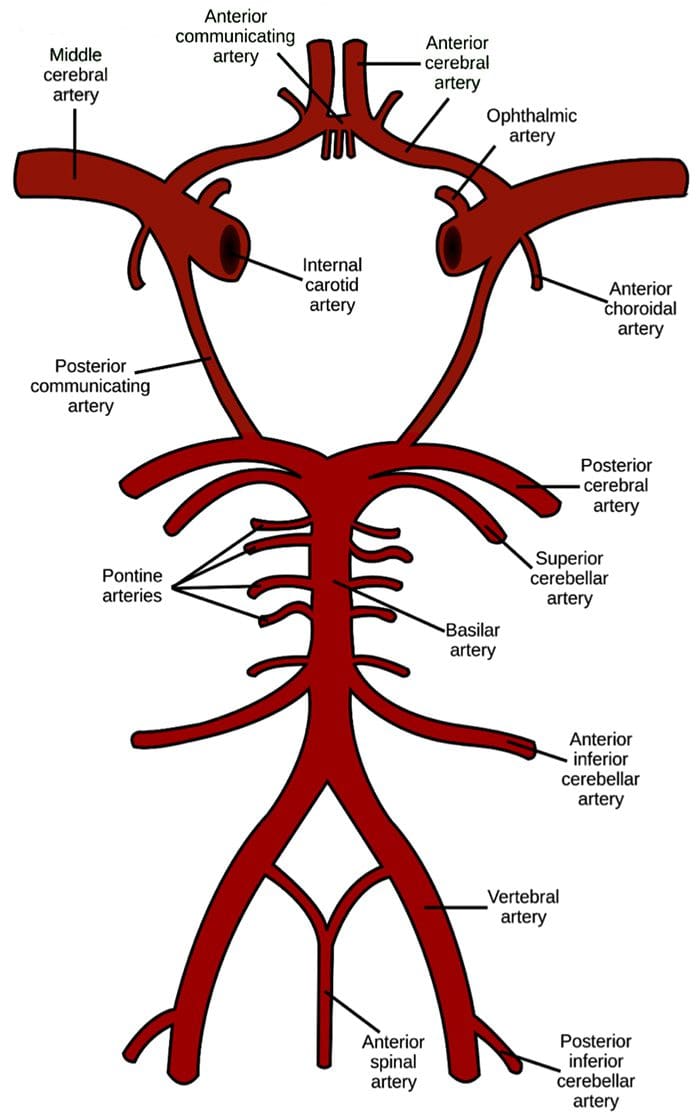 https://en.wikipedia.org/wiki/Circle_of_Willis
https://en.wikipedia.org/wiki/Circle_of_Willis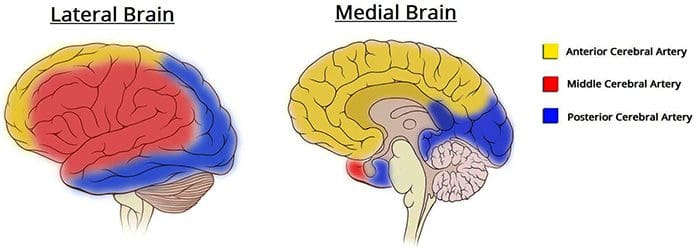 http://teachmeanatomy.info/neuro/vessels/arterial-supply/
http://teachmeanatomy.info/neuro/vessels/arterial-supply/

 http://roho.4senses.co/stroke- syndromes/common-stroke- syndromes-chapter-9-textbook-of- stroke-medicine.html
http://roho.4senses.co/stroke- syndromes/common-stroke- syndromes-chapter-9-textbook-of- stroke-medicine.html
 Diagnostic Needle EMG
Diagnostic Needle EMG Polyphasic MUPS
Polyphasic MUPS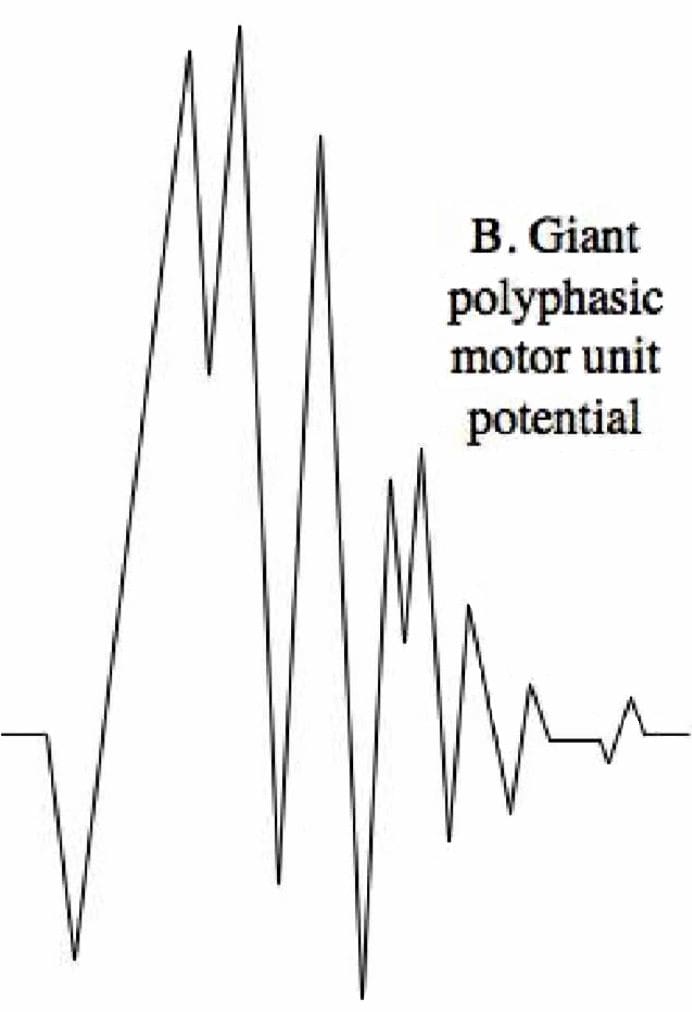 Complete Potential Blocks
Complete Potential Blocks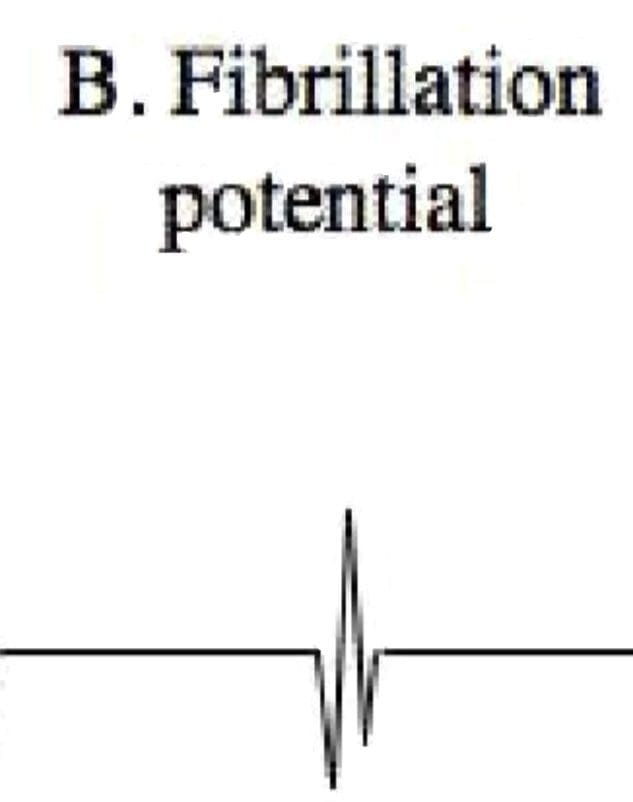 Positive Sharp Waves
Positive Sharp Waves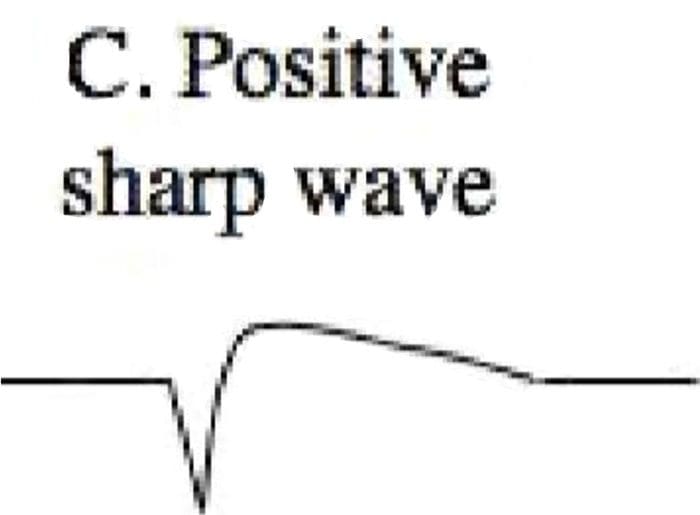 Abnormal Findings
Abnormal Findings