Can a knee brace relieve discomfort, provide support, and expedite recovery for individuals recovering from an injury or surgery?
Knee Brace
A knee brace is a medical device that supports and stabilizes the knee joint to help with pain and recovery after an injury or surgery. Many knee braces are made of various materials and offer a range of support levels. A healthcare provider or physical therapist can recommend the appropriate one for your condition and suggest the best one. Ask a healthcare provider if you’re unsure, as wearing a knee brace correctly and for the recommended time is important for healing. They are generally safe. However, individuals with health conditions such as poor circulation should be cautious when using them and consult their healthcare provider.
What They Do
The knee joint comprises bones, cartilage, ligaments, tendons, and muscles. A knee brace stabilizes these structures, preventing them from moving too much or too fast. Some braces redistribute the knee joint’s weight, decreasing the force the knee absorbs. (American Academy of Family Physicians, 2020)
Conditions
A knee brace is used after surgery to aid in healing and following an injury. This can be:
Knee braces differ in function and support level. Some stabilize the knee, while others completely immobilize the joint. A healthcare provider and/or physical therapist will explain what support is needed and how to use it. They can also check the brace’s fit and determine if adjustments or a different size are required.
Most Commonly Used
Prophylactic Brace
This is a protective knee pad that shields the kneecap from direct impact.
A knee unloader is typically used to control discomfort due to inflammatory conditions like tendonitis and osteoarthritis.
Functional
This brace limits motion in the joint after an injury or prevents dislocation.
Bledsoe Brace
This brace has straps to wrap around the thigh and shin and support brackets on the inside and outside of the knee joint.
A small mechanism locks the knee into full extension or allows the knee to bend a specific amount.
Knee Immobilizer
A knee immobilizer keeps the knee in one position.
It is a long cloth brace that runs the length of the shin and thigh.
Knee Brace vs Knee Support
A knee support or sleeve is usually a tight-fitting fabric garment. It provides compression to help reduce swelling and discomfort. A knee brace offers more support and can also be set to limit mobility.
Wearing The Brace
Individuals may need to wear a knee brace all day or only when performing specific tasks and operations. It depends on the individual and the condition the brace is being used for. Some may only need to wear a knee brace during certain activities or a flare-up of pain. (Mayo Clinic, 2022) Wearing a brace for unnecessarily long periods can cause skin abrasion, joint stiffness, and muscle atrophy. (American Academy of Family Physicians, 2020) Conversely, neglecting to wear it can cause more susceptibility to injury or extend and or impair healing time. Ask a healthcare provider when you should and should not wear the brace. This could be when:
Sitting
Walking
Driving
Sleeping
Stretching
Contraindications
Some medical conditions can make an individual susceptible to injury and adverse effects from wearing a knee brace. These include: (Holden, M. A. et al., 2021)
Poor circulation
Superficial wounds on the knee
Psoriasis
Eczema
Arterial insufficiency
Severe varicose veins
A history of thrombophlebitis
Injury Medical Chiropractic and Functional Medicine Clinic
If you have one of these conditions, a healthcare provider will decide if a knee brace is safe. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Best Knee Injury Chiropractor
References
American Academy of Family Physicians. (2020). Knee Bracing: What Works? https://familydoctor.org/knee-bracing-what-works/
Sprouse, R. A., McLaughlin, A. M., & Harris, G. D. (2018). Braces and Splints for Common Musculoskeletal Conditions. American family physician, 98(10), 570–576.
American Academy of Pediatrics. (2019). Knee pain: how to choose the right knee brace for your child. https://www.healthychildren.org/English/health-issues/injuries-emergencies/sports-injuries/Pages/Knee-Pain-and-braces.aspx
Mayo Clinic. (2022). To brace or not to brace: What’s the best answer? https://www.mayoclinichealthsystem.org/hometown-health/speaking-of-health/to-brace-or-not-to-brace#:~:text=If%20you%20have%20early%20onset%2C%20mild%20arthritis,below%20the%20knee%20for%20compression%20and%20comfort.
Holden, M. A., Callaghan, M., Felson, D., Birrell, F., Nicholls, E., Jowett, S., Kigozi, J., McBeth, J., Borrelli, B., Jinks, C., Foster, N. E., Dziedzic, K., Mallen, C., Ingram, C., Sutton, A., Lawton, S., Halliday, N., Hartshorne, L., Williams, H., Browell, R., … Peat, G. (2021). Clinical and cost-effectiveness of bracing in symptomatic knee osteoarthritis management: protocol for a multicentre, primary care, randomised, parallel-group, superiority trial. BMJ open, 11(3), e048196. https://doi.org/10.1136/bmjopen-2020-048196
Can incorporating an exercise program like the Alfredson Protocol help athletes and individuals who have hurt their Achilles tendon find pain relief and healing so they can return to regular physical activities?
Exercise Protocol Achilles Tendonitis
Achilles tendonitis occurs when the tendon at the back of the ankle gets injured. It is common in runners. For individuals who have Achilles tendonitis, walking and running can be painful. You might have to stop engaging in exercise and physical activities like sports. Depending on your job, having the condition may make working harder. Here are a few of the signs and symptoms of the condition:
Pain in the back of the lower leg, just above the heel.
Pain with running, jumping, or pointing the toes.
A small lump on the Achilles tendon just above the heel.
The first line of treatment is to rest and ice the tendon. Anti-inflammatory medications can help reduce pain. (American Academy of Orthopaedic Surgeons, 2022) Physical therapy can include strengthening exercises, ultrasound heat therapy, and deep massage. Exercises stretching the nearby muscles will help gradually increase the stress the tendon can handle, eventually reducing inflammation and swelling. Stretching and flexibility exercises will help an Achilles tendon heal. (University of Michigan, 2023)
The only way to determine if an individual has injured their Achilles tendon is to see a doctor. If the injury is Achilles tendonitis, a physical therapist may be recommended. A physical therapist can train individuals on the Alfredson protocol, an exercise protocol program for those with Achilles tendonitis (tendinopathy) that research has shown is helpful for those with the condition. The therapist will train on how to exercise to strengthen the tendon. The exercises stretch the Achilles tendon to help it handle forces and stress, known as eccentric loading. (Stevens M., & Tan C. W. 2014)
Inflammation
Tendonitis is inflammation of a tendon. However, studies have shown that the tendon might not be inflamed in those with the condition. When an area of the body is inflamed, inflammatory cells are present. Individuals usually feel pain in the inflamed area. For those with Achilles tendonitis, the tendon will present with pain, but not necessarily because the tendon is inflamed. Under a microscope, researchers examined tissue from the tendons of those with Achilles tendonitis. They did not find inflammatory cells in the tissue. (Stevens M., & Tan C. W. 2014) This means that although individuals felt pain, they were not inflamed. If there are no inflammatory cells in the tendon, this could explain why those with Achilles tendonitis often do not find relief from the anti-inflammatory treatment of non-steroidal anti-inflammatory drugs (NSAIDs). Studies have shown that gentle exercise protocols for the tendon are more helpful. However, researchers are not sure why these exercises are so beneficial. (O’Neill S., Watson P. J., & Barry S. 2015)
Eccentric Exercise
A chiropractic physical therapy team can help individuals heal the injury with eccentric loading exercises. Eccentric loading exercises work the muscles and tendons to help them get stronger. Once healing has begun, they can help strengthen the tendon. Individuals start slowly with easy exercises and then work up to harder ones. They will have the patient lengthen or stretch out the muscle. As the patient moves, the muscles and tendons contract or shorten. The Alfredson protocol consists of eccentric loading exercises for the Achilles and the muscles that support it.
Alfredson Protocol
Before exercising, talk to a doctor or physical therapist to know if it’s safe. How to do the Alfredson protocol:
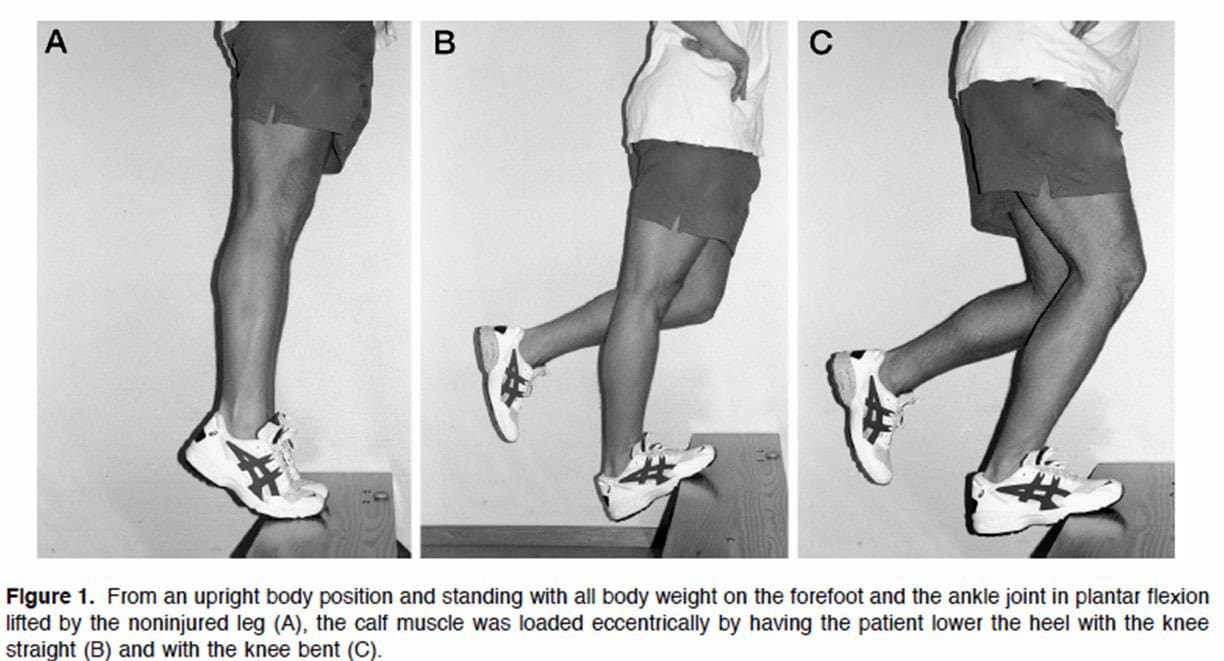
First, stand on a small step or curb.
Stand with the balls of your feet on the edge.
Your heels should hang over the edge.
Hold onto something for balance.
Keep the knees straight.
This will load a muscle part of the Achilles tendon called the gastrocnemius.
Using both feet, lift the heels and rise onto the balls of the feet.
Keep the foot with the painful Achilles tendon on the step.
Lift the non-injured foot off the step.
Slowly lower down using the injured ankle.
The heel should move towards the floor.
The ball of the foot should remain in contact with the edge of the step.
Return the non-injured foot to the step.
Repeat the exercise.
Do three sets of 15 reps with the knees straight. Then, do the Alfredson protocol again with the knees slightly bent. This will work a muscle called the soleus, which connects to the gastrocnemius. Perform three sets of 15 repetitions. Perform both exercises twice a day. This could be in the morning and the evening. The Alfredson protocol is most beneficial when done for about 12 weeks. (Stevens M., & Tan C. W. 2014)
Injury Medical Chiropractic and Functional Medicine Clinic
The Alfredson exercise protocol can be done at home with a step or raised platform to put the feet on safely. Individuals should consider working with a personal trainer to ensure safety and get the most out of the workouts. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
American Academy of Orthopaedic Surgeons. OrthoInfo. (2022). Achilles Tendinitis. https://orthoinfo.aaos.org/en/diseases–conditions/achilles-tendinitis/
University of Michigan. (2023). Achilles Tendon Injury: Physical Therapy and Rehab. https://www.uofmhealth.org/health-library/tr2261
Stevens, M., & Tan, C. W. (2014). Effectiveness of the Alfredson protocol compared with a lower repetition-volume protocol for midportion Achilles tendinopathy: a randomized controlled trial. The Journal of orthopaedic and sports physical therapy, 44(2), 59–67. https://doi.org/10.2519/jospt.2014.4720
O’Neill, S., Watson, P. J., & Barry, S. (2015). WHY ARE ECCENTRIC EXERCISES EFFECTIVE FOR ACHILLES TENDINOPATHY?. International journal of sports physical therapy, 10(4), 552–562.
The vastus lateralis is a muscle on the outside part of the thigh. Injuries to the muscle include strains, tendinitis, femoral nerve compression, and others. Can rehabilitation like heat and ice, massage, and strength and mobility exercises help individuals return to normal activities and function?
Vastus Lateralis Muscle
The vastus lateralis is the largest of the four quadriceps muscles on the thigh’s outer portion. The vastus lateralis helps extend the knee joint and maintain the knee position when walking or running. The vastus lateralis functions to work with the other quad muscles to help extend the knee joint.
Anatomy
Most muscles are attached to bone points of attachment, called the origin and insertion points. The vastus lateralis origin and insertion points are as follows (Vieira, EPL. 2017)
Origin
The origin is on the upper inter-trochanteric line of the femur or thigh bone.
It also arises from the base of the greater trochanter and the linea aspera, the supracondylar ridge, and the lateral intermuscular septum.
Insertion
From its origin, the muscle courses down the lateral thigh and inserts as part of the lateral quadriceps tendon on the tibial tubercle, an elevated portion of the upper shin.
The muscle is a large, flat structure with different attachments and a flat aponeurosis or sheath of connective tissue on the outer thigh.
The femoral nerve from lower back levels two, three, and four controls or innervates the muscle.
Blood supply to the muscle goes through the lateral circumflex femoral artery of the upper thigh.
Function
The muscle works with the other quadriceps muscles to extend or straighten the knee. The quads are responsible for functional activities like walking, running, climbing stairs, and getting up from a seated position. The vastus lateralis and the iliotibial band, which courses down the lateral thigh next to this muscle, form the lateral wall of the thigh. The vastus lateralis is on the opposite side of the vastus medialis muscle on the inner portion of the thigh. These muscles work together to maintain the appropriate position of the patella/kneecap in the femoral groove of the thigh bone. Malfunctioning these muscles properly can lead to knee pain from patellofemoral stress syndrome. (American Academy of Orthopaedic Surgeons, 2024)
Conditions
Many different injuries and conditions can affect the vastus lateralis and quad muscles, especially in athletes or active individuals. These injuries can cause vastus lateralis pain and other problems. (Timothy J. Von Fange, 2024) Some of the injuries and conditions include:
Patellofemoral Stress Syndrome – PFSS
This occurs when the kneecap tracks improperly in the femoral groove of the knee joint.
This leads to pain and difficulty when walking and running.
Vastus Lateralis Strain
A sudden force on the thigh can cause the quad muscle to be strained.
If the vastus lateralis suffers a pull injury, individuals may have pain, muscle swelling, thigh bruising, and walking difficulties.
Patellar Tendinitis
Irritation of the quad tendon that courses over the kneecap can cause patellar tendinitis.
Femoral Nerve Compression Weakness
The femoral nerve may become pinched or irritated from a herniated disc, lumbar stenosis, or arthritis.
Pain, numbness, tingling, or weakness in the thigh may result.
Iliotibial Band Friction Syndrome
Tight or weak muscles can irritate the IT band, and the vastus lateralis muscle can be affected.
Injury Rehabilitation
Injury to the vastus lateralis or quad muscles can cause pain, swelling of the thigh, or limited walking ability. Various treatments are available to help expedite recovery. A primary healthcare provider may recommend working with a physical therapy team. Self-care techniques can include:
Heat and Ice
Ice may be applied to the lateral thigh the first few days after injury to control pain and decrease swelling and inflammation.
Ice should be applied for 10 to 15 minutes.
Individuals may switch to heat two to three days after to promote circulation and improve tissue mobility.
Heat should be applied for 10 to 15 minutes.
Massage
Massage can help decrease pain and promote circulation.
Massage techniques can improve tissue mobility before stretching to help improve quadriceps motion.
Exercises and Stretching
A physical therapy team will prescribe certain exercises and stretches to help regain strength and range of motion. After an injury, quad stretching can improve the mobility and function of the muscle group.
Prone Towel Quad Stretch
Lie on your stomach and place a towel or strap around the ankle.
Bend the knee up, and gently pull on the towel to bend the knee fully.
A pulling sensation should be felt in the front of the thigh.
Hold the stretch for 30 seconds and release.
Repeat three times.
Half-kneeling Quad and Hip Flexor Stretch
Kneel on one knee.
Slowly move forward until a stretch is felt in the front of the hip and thigh.
Hold this position for 30 seconds.
Relax back to the starting position.
Repeat three times.
Back Exercises
If femoral nerve irritation coming from the lower back is causing thigh pain or weakness, exercises to release the nerve may be helpful and can include:
Prone press-ups
Supine lumbar flexion
Lumbar side glides
The exercises are designed to relieve pressure on the lumbar nerve, and postural correction exercises may be performed to maintain decompression.
Strengthening
Weakness to the vastus laterals and quads may be causing injury, and strengthening exercises may be prescribed during rehabilitation and can include:
Hip-strengthening exercises
Straight leg raises
Leg extension exercises
Lunges
Squats
Strengthening exercises should be done two to four times weekly with appropriate rest between sessions.
Balance exercises and sport-specific plyometric training may be recommended to ensure the quad functions normally.
Most quadriceps and vastus lateralis muscle injuries heal within six to eight weeks.
Recovery may be shorter or longer depending on the nature of the injury.
Injury Medical Chiropractic and Functional Medicine Clinic
By understanding the anatomy and function of the vastus lateralis muscle, a healthcare provider can help individuals understand their specific injury and develop a treatment program to rehabilitate the muscle properly. At Injury Medical Chiropractic and Functional Medicine Clinic, we focus on what works for you and strive to develop fitness and better the body through research methods and total wellness programs. These natural programs use the body’s ability to achieve improvement goals, and athletes can condition themselves to excel in their sport through proper fitness and nutrition. Our providers use an integrated approach to create personalized programs, often including Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles.
Knee Injury Chiropractor
References
Vieira EPL. (2017). Anatomic study of the portions long and oblique of the vastus lateralis and vastus medialis muscles. J Morphol Sci., 28(4), 0-. http://www.jms.periodikos.com.br/article/587cb49f7f8c9d0d058b47a1/pdf/jms-28-4-587cb49f7f8c9d0d058b47a1.pdf
American Academy of Orthopaedic Surgeons. (2024). Patellofemoral pain syndrome. https://orthoinfo.aaos.org/en/diseases–conditions/patellofemoral-pain-syndrome/
Timothy J Von Fange. (2024). Quadriceps muscle and tendon injuries. UpToDate. https://www.uptodate.com/contents/quadriceps-muscle-and-tendon-injuries/print
Ramírez-delaCruz, M., Bravo-Sánchez, A., Esteban-García, P., Jiménez, F., & Abián-Vicén, J. (2022). Effects of Plyometric Training on Lower Body Muscle Architecture, Tendon Structure, Stiffness, and Physical Performance: A Systematic Review and Meta-analysis. Sports medicine – open, 8(1), 40. https://doi.org/10.1186/s40798-022-00431-0
Elbow pain from lifting is a common symptom among individuals who lift weights, heavy objects, children, grocery bags, etc. Depending on the underlying cause, can conservative treatments relieve and heal elbow pain?
Elbow Pain Caused By Lifting
Elbow pain from lifting can result from weight training, repetitive daily tasks, or job duties like lifting small children or heavy objects. Pain can manifest at the sides or the front of the elbow. Most minor injury cases can be treated with ice, rest, and medications at home. However, pain after lifting can also be a sign of a serious injury, such as a tendon rupture/tear.
Minor Pain From Lifting
Lifting puts pressure on the tendons connecting the wrist and upper arm to the bones in the elbow joint. Minor elbow pain can occur from temporary inflammation in any of these structures after lifting an object. Tendonitis occurs when a tendon becomes inflamed, often from overuse or lifting something too heavy, and ranges from mild to severe. Mild tendonitis typically causes pain during the activity and improves with rest. (American Academy of Orthopaedic Surgeons, 2020) Common forms of tendonitis include:
Tennis elbow – tendonitis on the outside of the elbow
Golfer’s elbow – tendonitis on the inside of the elbow.
Add ice to the affected area for up to 20 minutes daily to decrease elbow pain.
Rest
Avoid lifting heavy objects as much as possible when pain is present.
Wearing A Brace
If the pain is at the tendons on the inside or outside of your elbow, try wearing a wrist brace to limit the use of your wrist muscles that connect to this area.
Stretching
Gently stretching the wrist flexors and extensors can help reduce elbow pain after lifting. Stretches can be performed several times daily, even after symptoms have resolved. (American Academy of Orthopaedic Surgeons, 2024)
Hold the arm out in front with the palm down. Keep the elbow straight.
Bend the wrist down so that the fingers are pointing toward the ground.
With the other hand, gently pull the wrist further down until a stretch is felt along the back of the forearm.
Hold this position for 15 seconds.
Repeat five times.
Next, bend the wrist upward so the fingers point toward the ceiling.
Using the other hand, gently pull the hand backward until the stretch is felt along the front of the forearm.
Mild cases can improve after a few days of self-care, whereas more pronounced elbow symptoms can take several weeks, months, or even a year. (Kheiran A. Pandey, A. & Pandey R. 2021) If self-care doesn’t work, physical therapy may be recommended. A physical therapy team can use various modalities and treatments to help reduce pain and inflammation from elbow injuries. The therapy can include targeted exercises to strengthen weak muscles and stretch tight muscles that might contribute to the condition. In addition, the therapy team will help individuals modify their lifting technique to help prevent further injury.
A biceps tendon rupture is a rare but serious injury usually caused from lifting. In addition to other visible signs of the injury, there will be a bulge at the top of the upper arm because the muscle bunches up as it is no longer attached to the elbow. (American Academy of Orthopaedic Surgeons, 2022) Individuals may hear an audible popping sound if an elbow ligament or tendon gets torn while lifting. (Johns Hopkins Medicine, 2024)
Treatment
Treatment depends on the severity of the injury, but most cases resolve on their own with rest and, if necessary, physical therapy. Conditions that cause severe pain require orthopedic surgeon expertise. These physicians specialize in treating musculoskeletal system injuries. Imaging such as X-rays, MRIs, or CT scans are often used to determine the extent of damage. Individuals with tendon or ligament tears in the elbow may need surgery to regain full range of motion and strength in their arm. After surgery, physical therapy will help restore function.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other associated medical professionals to integrate a treatment plan to improve the body’s flexibility and mobility and resolve musculoskeletal issues.
Shoulder Pain Chiropractic Treatment
References
American Academy of Orthopaedic Surgeons. (2020). Sprains, strains, and other soft-tissue injuries. https://orthoinfo.aaos.org/en/diseases–conditions/sprains-strains-and-other-soft-tissue-injuries/
Kheiran, A., Pandey, A., & Pandey, R. (2021). Common tendinopathies around the elbow; what does current evidence say?. Journal of clinical orthopaedics and trauma, 19, 216–223. https://doi.org/10.1016/j.jcot.2021.05.021
American Academy of Orthopaedic Surgeons. (2024). Therapeutic exercise program for epicondylitis (tennis elbow/golfer’s elbow). https://orthoinfo.aaos.org/globalassets/pdfs/2024-therapeutic-exercise-program-for-lateral-and-medial-epicondylitis.pdf
American Academy of Orthopaedic Surgeons. (2023). What are NSAIDs? https://orthoinfo.aaos.org/en/treatment/what-are-nsaids/
American Academy of Orthopaedic Surgeons. (2022). Biceps tendon tear at the elbow. https://orthoinfo.aaos.org/en/diseases–conditions/biceps-tendon-tear-at-the-elbow
Can healthcare professionals implement H.E.A.R.T. protocols for trafficked individuals while providing a safe space?
Introduction
Across the world, many local media and organizations are paying close attention to a phenomenon that many people should be aware of. This phenomenon is known as trafficking, and it can be associated with numerous activities, from forced labor to sex labor, and can affect a person’s sense of self-worth. While many people will correlate that trafficking affects many women and children, it can affect many individuals regardless of age, gender, and background. While many survivors of trafficking are dealing with the psychological and physical injuries that they obtain from their traffickers, many medical professionals can implement protocols and roles through the implementation of H.E.A.R.T. to provide a safe space for individuals suffering from trafficking. Today’s article focuses on the definition of trafficking, what H.E.A.R.T. is, and how it is used in a clinical setting. We discuss with certified associated medical providers who consolidate our patients’ information to assess and identify trafficking in a clinical approach while providing a safe space. We also inform and guide patients while asking their associated medical provider intricate questions to formulate customized treatment plans for their pain and provide them with a safe space and positive experience. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
The Definition Of Trafficking
When it comes to defining trafficking, it can be challenging as it is frequently associated with other issues. However, the main definition for trafficking is “recruiting, transporting, transferring, or harboring many individuals or a person that are threatened or forced to achieve the consent of a person having control of the individuals for exploitation.” With human trafficking being a pressing public concern that affects all races, social classes, demographics, and genders, it can impact society and the individual who is being trafficked. (Toney-Butler et al., 2024) Additionally, many people often mistake trafficking and smuggling as they are completely different. Smuggling requires a person to be transported into a nation through voluntary illicit means. While trafficking can come in two forms, which are labor and commercial sex, it can happen within the person’s own home. (Rambhatla et al., 2021) This is because many survivors who are going to get healthcare services will feel various emotions of fear or shame that can prevent them from asking for help due to what they have been through with their trafficker. However, when many individuals who are trafficking survivors are suffering from significant physical, mental, and social health problems and are seeking healthcare services, many healthcare professionals play an important role by creating a safe and responsive space for them. (The Lancet Regional Health-Western, 2022)
Beyond the Surface: Understanding the Effects of Personal Injury- Video
What is H.E.A.R.T In A Clinical Setting
When it comes to creating a safe and positive space in a clinical setting, many healthcare professionals often miss the signs of trafficking due to a lack of training or confidence to identify and treat patients who are trafficking victims. (Lee et al., 2021) However, healthcare protocols should be implemented, and H.E.A.R.T. should be incorporated into a clinical approach to assess and develop a customized treatment plan for the patient. Healthcare professionals can engage with the patient in a one-on-one discussion away from their trafficker and can offer important medical and psychological care resources. (Exeni McAmis et al., 2022) By incorporating H.E.A.R.T. protocols in a healthcare clinic, many doctors and medical professionals can help many patients be in a safe environment. Below is what H.E.A.R.T. stands for.
H-Hearing
The “H” in H.E.A.R.T. is for hearing as many medical professionals not only to hear but to see what is going on in the clinic and to establish environmental awareness. This is due to looking at the patient and who is accompanied by them. With healthcare providers being at the front, they interact with patients and may not know what health concerns are affecting them. This could be due to the following:
By incorporating the hearing aspect in H.E.A.R.T., many healthcare professionals can provide a safe, thoughtful, and engaging approach to the patient and know what to look for when a patient is coming in for treatment.
E-Evaluating
The “E“ in H.E.A.R.T. is used to evaluate its importance in enhancing patient interactions in a trauma-informed care facility. This is highly important because the individual is seeking health care. For the patients being trafficked, it is important to notice the red flags the individual is experiencing. Some of the red flags that many healthcare providers should look for are:
Physical health
Behavioral Health
The patient is with a controlling person
The patient does not have possession of their I.D.
Additionally, it is always important to show compassion, be sensitive to the individual while addressing their needs and concerns, and use a non-judgmental approach during the interview process. This helps the individual ensure they are in a safe environment when discussing sensitive topics. At the same time, it is important not to let the patient be re-traumatized while avoiding the impulse to rescue and overpromise the patient to mental health as we want them to have their self-worth. At the same time, it is best to remember the four “Rs“ when doing a trauma-informed approach; they are:
Realize: Understanding how trauma can affect people.
Recognize: Recognizing the signs of trauma.
Respond: Have all staff trained, use evidence-based practices, and provide a safe environment.
Resist Re-trauma: Recognizing how some practices may trigger painful memories while avoiding re-traumatizing the patient.
By implementing the four “Rs“ and the “E“ in H.E.A.R.T., many healthcare professionals can provide valuable resources to trafficking survivors with a strong support system.
A-Activating
The “A“ in H.E.A.R.T. stands for activating, where healthcare professionals must have proper protocols to engage all employees. This allows the healthcare providers to understand how beneficial it is to develop a protocol for a person who is being trafficked, understand their state and federal reporting laws, and list key elements of effective trauma-informed screening procedures when assessing the patient. This allows a foundational structure to support a response for suspected patients who are being trafficked. At the same time, by following HIPAA laws and organization policies, many healthcare providers must explain the reporting process to the right officials. Additionally, the benefits of developing a protocol for trafficking are by:
Clarifying procedures
Enhance staff training
Optimize the interactions with the trafficking patients
Improve staff confidence
Prepare for any threatening situations
Maximizing preparedness to aid trafficking patients
Optimize support for patients
Develop collaborative outside resources
R-Resourcing
The “R“ in H.E.A.R.T. stands for resourcing, as many healthcare providers must identify the referral systems. This allows healthcare professionals to understand the important message to convey when assessing trafficking victims and the importance of responding to safety, emergency, and reporting requirements. When assessing and interviewing the patient, many will have to recognize that their patient may be a possible victim of trafficking, what their immediate needs are, and what long-term resources can help.
T-Training
The “T” in H.E.A.R.T. stands for training, as it is important that many healthcare providers continuously train to spot trafficking; this provides confidence to many healthcare workers and can help save a person’s life. By implementing H.E.A.R.T. protocols, the “T” allows the doctor to respect the individual’s decision to want help, providing a positive support system while encouraging them to come back, offering to help with a safety plan, and building a resource network. This is because if the patient is accompanied by someone who is controlling and answering for the patient, handing out information discreetly can provide a bit of hope to the individual to make the move. At the same time, providing local and immediate assistance resources can help the individual in the long run. This allows healthcare providers to build a trusting relationship and even help individuals to have a safe and positive experience on their health and wellness journey.
References
Exeni McAmis, N. E., Mirabella, A. C., McCarthy, E. M., Cama, C. A., Fogarasi, M. C., Thomas, L. A., Feinn, R. S., & Rivera-Godreau, I. (2022). Assessing healthcare provider knowledge of human trafficking. PLOS ONE, 17(3), e0264338. https://doi.org/10.1371/journal.pone.0264338
Gutfraind, A., Yagci Sokat, K., Muscioni, G., Alahmadi, S., Hudlow, J., Hershow, R., & Norgeot, B. (2023). Victims of human trafficking and exploitation in the healthcare system: a retrospective study using a large multi-state dataset and ICD-10 codes. Front Public Health, 11, 1243413. https://doi.org/10.3389/fpubh.2023.1243413
Lee, H., Geynisman-Tan, J., Hofer, S., Anderson, E., Caravan, S., & Titchen, K. (2021). The Impact of Human Trafficking Training on Healthcare Professionals’ Knowledge and Attitudes. J Med Educ Curric Dev, 8, 23821205211016523. https://doi.org/10.1177/23821205211016523
Rambhatla, R., Jamgochian, M., Ricco, C., Shah, R., Ghani, H., Silence, C., Rao, B., & Kourosh, A. S. (2021). Identification of skin signs in human-trafficking survivors. Int J Womens Dermatol, 7(5Part B), 677-682. https://doi.org/10.1016/j.ijwd.2021.09.011
For individuals and athletes with a gluteal contusion with severe bruising, can a healthcare provider determine if there are any other injuries to underlying structures, including muscle or tendon tears?
Gluteal Contusion
A gluteal contusion is an injury, in this case, a bruise to the buttocks’ gluteal muscles caused by damage to muscle fibers and blood vessels. A buttock bruise is caused by direct bodily impact, typically from falls, automobile collisions, accidents, bumping into something, or being struck by an object or person. Like all bruises, a gluteal bruise most often results in pain and visible discoloration of the skin at the injury site, varying in severity from grade I to grade III, with higher-graded bruises requiring more time to heal. Most butt bruises can heal on their own with time and rest, but if bruising is severe, individuals may require physical therapy to restore full muscle function.
Symptoms
A contusion is a muscle injury that can affect the body’s skeletal muscles. A gluteal contusion can be painful, with a black and blue mark that changes color over time. Other symptoms may include: (Mount Sinai, 2024)
Tenderness to touch over the injury site
Increased pain with contraction of the glutes
Swelling
Discomfort with sitting
Causes
A contusion occurs from direct trauma and forceful impact on the gluteal muscles, causing damage to underlying blood vessels, muscle fibers, and sometimes bone, resulting in bleeding under the skin. (MedlinePlus, 2016) Direct impacts to the gluteal muscles that can cause a contusion include:
Falls
Car accidents
Direct hits to the buttocks from a piece of sports equipment or person.
Bumping into furniture, a door, or a counter.
Intramuscular injections into the gluteal muscles.
Individuals who take blood thinners or anticoagulant medication have an increased risk of bruising from direct contact injuries.
Diagnosis
A gluteal contusion is usually diagnosed through a physical examination and is generally straightforward to diagnose based on physical appearance, symptoms, and type of injury. Contusions can be graded based on the severity according to the following criteria (Fernandes, T. L. et al., 2015)
Grade I
An injury that affects only a small amount of muscle fibers, resulting in minimal pain, tenderness, and possible swelling.
Causes minimal or no loss of strength in the affected muscle or range of motion limitations.
Muscle use is typically unaffected.
Grade II
An injury that causes significant damage to muscle fibers, resulting in increased pain and impaired muscle contraction.
A small muscle defect can be felt to the touch.
Discoloration increases over the first few days after injury.
Grade III
An injury that involves extensive muscle fiber damage and bleeding across an entire area of a muscle that results in severe, and sometimes total, loss of muscle function.
Causes severe pain and significant discoloration of the skin.
When contusions are larger, deeper, and involve significant blood pooling and swelling, they are called hematomas.
If the bruising is severe, a diagnostic ultrasound, CT scan, or MRI may be used to determine whether any underlying structures are damaged.
Treatment
Contusions are generally mild injuries. Treatment typically involves rest to allow the muscles to heal from the bleeding and the bruising to dissipate.
Applying ice to the injury site can help relieve pain and inflammation.
If the bruising is severe, significant physical activity like sports, dancing, running, jumping, and weight lifting should be avoided until the muscles heal. (Mount Sinai, 2024)
With more severe bruising, contraction and stretching of the glutes are painful and can require longer healing and recovery time.
Physical therapy rehabilitation may be needed for more significant injuries to restore muscle function.
Prognosis
A mild injury usually heals on its own with time and rest. More significant injuries take longer to heal and may require physical therapy to build strength and range of motion if muscle function is affected.
Healing Time and Recovery
Healing and recovery times for gluteal contusions vary depending on the severity of the injury (Fernandes T. L. et al., 2015)
Grade I
Minor injuries that cause minimal discomfort typically heal fully in five days to two weeks.
Grade II
During the first two to three days, contusions develop, increasing discoloration under the skin, and complete healing can take two to three weeks.
Return to sport is typically resumed after a month.
Grade III
Contusions can take up to four to six weeks to heal, often requiring rehabilitation to restore muscle strength and range of motion.
Injury Medical Chiropractic and Functional Medicine Clinic
At Injury Medical Chiropractic and Functional Medicine Clinic, we passionately focus on treating patients’ injuries and chronic pain syndromes. We focus on improving ability through flexibility, mobility, and agility programs tailored to the individual. We use in-person and virtual health coaching and comprehensive care plans to ensure every patient’s personalized care and wellness outcomes. Our providers use an integrated approach to create personalized care plans that include Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles. Our goal is to relieve pain naturally by restoring health and function to the body. If he feels the individual needs other treatment, they will be referred to a clinic or physician best suited for them as Dr. Jimenez has teamed up with the top surgeons, clinical specialists, medical researchers, and premier rehabilitation providers to provide our community with the best clinical treatments.
Building a Stronger Body
References
Mount Sinai. (2024). Bruise. https://www.mountsinai.org/health-library/injury/bruise
MedlinePlus. (2016). Bruises. Retrieved from https://medlineplus.gov/bruises.html
Fernandes, T. L., Pedrinelli, A., & Hernandez, A. J. (2015). MUSCLE INJURY – PHYSIOPATHOLOGY, DIAGNOSIS, TREATMENT AND CLINICAL PRESENTATION. Revista brasileira de ortopedia, 46(3), 247–255. https://doi.org/10.1016/S2255-4971(15)30190-7
Individuals dealing with symptoms like sudden pain, weakness, and tenderness in the back of the knee could have a hamstring injury. Can knowing the symptoms and performing self-care help bring relief?
Hamstring Pain Behind The Knee
The hamstrings consist of three long muscles that run down the back of the thigh, cross over the back of the knee, and connect to bones in that area. A hamstring injury, such as a strain or tear, tendonitis, or biceps femoris tendinopathy, can cause pain in the back of the knee, difficulty bending the knee, swelling, and bruising. A hamstring strain occurs when the muscle is stretched too far or torn completely. This can happen from sudden, forceful movements or overstretching. Hamstring tendonitis develops over time, usually after a sudden increase in activity, when the hamstring tissue cannot recover from too much loading. Pain is often felt after physical activity and exercise and, in severe cases, during the activity or throughout the day. Biceps femoris tendinopathy can also cause pain in the back of the knee. Strains, tendonitis, bursitis, and muscle tears are all possible explanations for a hamstring injury that leads to pain behind the knee. Discussing pain symptoms with a healthcare provider is recommended, especially if it occurs suddenly during physical activity or exercise. They can help identify the exact cause and offer guidance for rehabilitation, including physical therapy referrals.
Causes and Triggers
Individuals may experience hamstring pain behind the knee when the muscles in that area are overworked, inflamed, or injured, such as from activities like running, walking, dancing, soccer, or basketball. Possible types of injuries and their causes.
A primary cause of muscle strain occurs when the muscle is stretched too far or has to handle a sudden force like sprinting or kicking. (American Academy of Orthopaedic Surgeons, 2021)
Severe Cases
Most causes of pain behind the knee are easily treatable at home with self-care and rest. However, it can be more severe, signaling a blood clot, infection, torn muscle or tendon/ligament. Hamstring knee pain may be serious if any of the following is experienced (American Academy of Orthopaedic Surgeons, 2021)
Sudden pain during physical activity, often during a full stride.
Feeling a pop or sharp pain that causes falling or limping.
Pain that worsens over time and prevents or hinders walking or exercising as normal.
If pain is severe and does not improve with rest and anti-inflammatory medications, evaluation by a healthcare professional is necessary.
Assesses Hamstring Pain
A healthcare provider will ask about symptoms and injury, including what happened when the pain began. They will perform a physical examination, which may include pressing on the back of the thigh to look for swelling, bruising, tenderness, or bunched-up muscles. (American Academy of Orthopaedic Surgeons, 2021) The healthcare provider will ask the patient to perform specific resisted movements, such as the manual muscle test, and measure the range of motion. Diagnostic testing includes an X-ray or MRI to determine the degree of the injury and which soft tissues or bones may be involved.
Self-Care
The first line of treating hamstring knee pain is the RICE protocol, which includes: (Mount Siani, 2024)
Rest
Stop any activity that causes symptoms and pain.
A healthcare provider may recommend crutches or a knee scooter in severe cases.
Ice
Apply cold packs to the swollen or painful area for 20 minutes throughout the day.
Compression
A knee brace, wrap, or bandage that applies gentle pressure to the injured area can help reduce and prevent swelling.
Elevation
Lifting the leg higher than the heart will help reduce swelling and blood accumulation.
Individuals may need to lie on a bed or sofa and elevate their legs with pillows.
Individuals can use at-home pain relievers like acetaminophen or NSAIDs like ibuprofen or naproxen. Over time, and depending on the severity of the injury, a healthcare provider will advise on gentle hamstring stretches and how to ease back into physical activity.
A healthcare provider will advise immobilizing the knee to help with muscle healing, which could involve wearing a knee brace or using crutches.
Physical therapy
A healthcare provider may refer the patient to a physical therapist, who will perform a personalized evaluation and prescribe targeted exercises to heal the injury and regain strength, flexibility, and movement.
Surgery
Tendon avulsion injuries are when the hamstring tendon completely tears away from the bone, and surgery is required to reattach the tendon.
Platelet-rich plasma – PRP
Platelet-rich plasma has become an additional treatment for hamstring muscle strain or tendonitis. (Seow D. et al., 2021)
The treatment involves injecting a solution from the patient’s blood into the muscle to heal the injury.
Recovery
Predicting how long a hamstring injury takes to heal and how long the pain will linger depends on the type, location, and severity. The most severe type is the hamstring coming unattached around the knee. This surgical repair and rehabilitation take at least three months before returning to sports and exercise (American Academy of Orthopaedic Surgeons, 2021). Lesser injuries like tendonitis or a mild strain can take less time to heal. However, it’s essential to avoid reinjuring the area so the condition does not become chronic. This includes: (American Academy of Orthopaedic Surgeons, 2021)
Stretching to encourage and maintain flexibility.
Fixing muscle imbalances between the quadriceps and hamstring.
Endurance and conditioning.
Avoiding overuse.
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop personalized treatment programs. We focus on what works for you and use an integrated approach to treating injuries and chronic pain syndromes to improve flexibility, mobility, and agility, relieving pain and helping individuals return to normal activities. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers. Our providers use Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles.
Chiropractic Care for Leg Instability
References
National Library of Medicine. (2017). Tendinitis Also called: Tendonitis. Retrieved from https://medlineplus.gov/tendinitis.html
American Academy of Orthopaedic Surgeons. OrthoInfo. (2020). Sprains, strains, and other soft tissue injuries. https://orthoinfo.aaos.org/en/diseases–conditions/sprains-strains-and-other-soft-tissue-injuries/
American Academy of Orthopaedic Surgeons. OrthoInfo. (2021). Hamstring muscle injuries. https://orthoinfo.aaos.org/en/diseases–conditions/hamstring-muscle-injuries/
American Academy of Orthopaedic Surgeons. OrthoInfo. (2021). Pes aserine (knee tendon) bursitis. https://orthoinfo.aaos.org/en/diseases–conditions/pes-anserine-knee-tendon-bursitis/
Mount Siani. (2024). Hamstring strain – aftercare. https://www.mountsinai.org/health-library/selfcare-instructions/hamstring-strain-aftercare
Seow, D., Shimozono, Y., Tengku Yusof, T. N. B., Yasui, Y., Massey, A., & Kennedy, J. G. (2021). Platelet-Rich Plasma Injection for the Treatment of Hamstring Injuries: A Systematic Review and Meta-analysis With Best-Worst Case Analysis. The American journal of sports medicine, 49(2), 529–537. https://doi.org/10.1177/0363546520916729
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine