Dr. Alex Jimenez at El Paso Back Clinic®: Beating Back Pain from Long Desk Hours
Businesswoman experiences worsening back pain while sitting at her desk.
If your back pain gets worse the longer you sit at your desk, you are not alone. Many people in El Paso face this issue due to long hours spent in sedentary jobs. Sitting for extended periods can put pressure on the spine, tighten muscles, and reduce blood flow, leading to stiffness, aches, and, in some cases, chronic problems (Colorado Pain Care, n.d.). The positive news is that you can take simple steps to reduce the pain and prevent it from worsening. At El Paso Back Clinic® in El Paso, TX, the wellness chiropractic care team, led by Dr. Alex Jimenez, DC, APRN, FNP-BC, focuses on helping people just like you find natural, long-term relief through personalized plans.
Prolonged sitting stresses the lower back by increasing disc pressure by up to 90% compared to standing. It flattens the spine’s natural curve, strains muscles, and creates imbalances (Colorado Pain Care, n.d.). Slouching or leaning forward adds extra load to the neck and upper back. Over time, this can lead to tight hips, weak core muscles, and ongoing discomfort that affects daily life.
At El Paso Back Clinic®, our experts understand these issues caused by sedentary work. They use a holistic approach that combines chiropractic adjustments, functional medicine, and rehab to address root causes like poor posture and muscle imbalances from desk jobs (Jimenez, n.d.-a).
Here are practical changes to start today:
Move often: Get up every 30 minutes to stand, walk, or shift positions. Short 1-2 minute breaks improve circulation and ease tension (Huntsville Hospital Health System, n.d.; Sydney West Physio, n.d.).
Use regular breaks: Set a timer for quick walks to get water or to stretch. This habit prevents stiffness from building up throughout the day.
Add dynamic movement: While sitting, shift weight, uncross legs periodically, or use a footrest to change angles. These small actions keep the spine mobile (Colorado Pain Care, n.d.).
A proper ergonomic setup supports optimal posture and reduces strain.
Follow these key tips:
Set your chair so that your feet are flat on the floor, your knees are at 90 degrees, and your hips are level with or above your knees.
Add lumbar support (a small pillow or rolled towel works) to maintain the lower back’s curve.
Place your screen at eye level to avoid looking down or up too much.
Keep the keyboard and mouse close so elbows bend at 90 degrees and shoulders stay relaxed.
Avoid crossing legs for long, as it can tilt the pelvis (Senara Chiropractic & Med Spa, n.d.; Huntsville Hospital Health System, n.d.).
Consider alternating between sitting and standing with a standing desk. Even partial standing reduces spinal pressure.
Stretches help loosen tight spots from sitting, such as the hips, shoulders, and neck.
Try these simple ones:
Hip flexor stretch: Kneel on one knee, gently push hips forward, and hold 20-30 seconds per side.
Chest and shoulder opener: Clasp hands behind your back or use a wall to stretch forward.
Neck tilts: Slowly tilt the head side to side or forward/back; hold for 10-15 seconds.
Upper back extension: Hands behind head, gently arch upper back (Sydney West Physio, n.d.).
Do them hourly or during breaks for better flexibility.
Strengthening the core supports the spine and improves posture long-term.
Include these:
Planks: Hold forearm plank 20-30 seconds.
Cat-camel: On hands and knees, arch and round back slowly.
Bridges: Lie back, lift hips while squeezing glutes.
Walking or gentle yoga: Build overall strength (Huntsville Hospital Health System, n.d.; Sydney West Physio, n.d.).
Aim for 20-30 minutes of activity most days.
For lasting relief, professional care targets alignment, mobility, and personalized fixes. At El Paso Back Clinic®, Dr. Alex Jimenez leads a team offering integrated chiropractic care. This includes spinal adjustments to correct misalignments, non-surgical spinal decompression for disc relief, acupuncture, functional medicine for nutrition and stress, and rehab exercises tailored to desk-related issues.
Dr. Jimenez, with dual expertise as a chiropractor and nurse practitioner, emphasizes posture correction, mobility training, and the prevention of sedentary pain through evidence-based methods. The clinic helps restore function without drugs or surgery, focusing on root causes like imbalances from prolonged sitting (Jimenez, n.d.-a; Jimenez, n.d.-b).
Other options in El Paso exist, but El Paso Back Clinic® stands out for its comprehensive wellness approach, advanced diagnostics, and patient-centered plans that go beyond basic adjustments.
If pain includes numbness, tingling, or weakness in the legs, or persists despite changes, seek evaluation to rule out serious conditions (University of Maryland Medical System, n.d.).
Start small: improve movement, setup, and stretches. If needed, contact El Paso Back Clinic® for expert help. Many in El Paso regain comfort and stay active with this care.
Spinal Hygiene Explained: Daily Habits to Keep Your Spine Strong and Pain-Free
A woman performs spinal hygiene exercises on a fitness ball at home, strengthening her back muscles.
Spinal hygiene is the practice of caring for your spine every day to keep it strong, flexible, and healthy. Just like brushing your teeth helps prevent cavities, spinal hygiene helps avoid back problems and keeps your body moving well. The spine supports your whole body, protects the nervous system, and lets you bend, twist, and stand tall. Good habits can make a big difference in how you feel now and as you get older.
What Spinal Hygiene Means
Spinal hygiene includes simple daily actions to protect the spine’s natural shape and movement. The spine has gentle curves that help absorb shock and allow smooth motion. When these curves stay balanced, and the spine moves freely, you feel better overall.
Proper posture: Sit and stand with your shoulders back, head aligned over your spine, and pelvis in a neutral position to avoid extra strain.
Regular movement and exercise: Stay active with walking, swimming, or stretching to keep joints loose and muscles strong.
Proper body mechanics: Lift things by bending your knees, keeping objects close to your body, and avoiding twists to prevent injury.
Core strength: Build muscles around your midsection for better support and stability.
Hydration and nutrition: Drink plenty of water to keep spinal discs cushioned, and eat foods rich in calcium, vitamin D, magnesium, and omega-3 fatty acids to support bone and tissue health.
Stress management: Use deep breathing, meditation, or yoga to reduce tension that tightens back muscles.
These steps help maintain the spine’s integrity and prevent issues like stiffness or pain (Spinenpain.org, n.d.; Lifemovesmt.com, n.d.).
Neglecting spinal hygiene can lead to problems over time. Poor habits can cause muscle imbalances, joint wear, reduced motion, and conditions such as herniated discs or chronic back pain. This can affect your nervous system, since the spine houses nerves that control body functions. When the spine is out of alignment, it may press on nerves, leading to pain, weakness, or other issues (Servinglifedallas.com, n.d.; Drmmalone.com, n.d.).
Benefits of Good Spinal Hygiene
Taking care of your spine brings many advantages. It reduces the chance of back pain, improves how easily you move, and supports better posture. A healthy spine also helps the nervous system function smoothly, boosting energy, coordination, and overall well-being. Regular care can slow age-related changes, lower injury risk, and help you stay active longer.
Prevents muscle tightness and joint problems
Improves blood flow and nutrient delivery to spinal tissues
Enhances balance and reduces fall risk
Supports better sleep and less daily discomfort
Studies and experts note that these habits promote long-term health and vitality (Illinoisspinalcare.com, n.d.; Spinehealth.org, n.d.).
How Chiropractic Care Fits In
Chiropractic care plays a key role in spinal hygiene. Chiropractors use gentle adjustments to fix misalignments, called subluxations, that can stress the spine and nerves. These adjustments restore proper movement, reduce pain, and improve function. Regular chiropractic visits act as preventive maintenance, catching small issues before they grow.
Many people combine chiropractic with other habits for the best results. Adjustments improve alignment, while daily posture and exercise help maintain gains. This approach helps address common complaints such as neck or low back pain and supports recovery from injuries (Illinoisspinalcare.com, n.d.; Eastportlandchiropractor.com, n.d.).
The Power of Integrative Care with Chiropractors and Nurse Practitioners
An integrative approach brings together diverse experts to achieve stronger results. Chiropractors focus on the spine’s structure, alignment, and movement through adjustments and rehab. Nurse practitioners (NPs), especially those with advanced training, address broader health needs such as nutrition, stress management, hormone balance, and lifestyle changes.
This team effort addresses both the physical spine and daily habits that affect it. For example, a chiropractor might correct alignment after an injury, while an NP guides on anti-inflammatory foods or stress reduction to aid healing. Together, they create personalized plans that work better than one alone, especially for complex pain, chronic issues, or recovery from accidents.
Dr. Alexander Jimenez, DC, APRN, FNP-BC, stands out in this field. As a Doctor of Chiropractic and board-certified Family Nurse Practitioner, he combines spinal adjustments, decompression therapy, and functional medicine. His practice emphasizes root-cause care, using nutrition, lifestyle tweaks, and advanced diagnostics for musculoskeletal problems, personal injuries, and overall wellness. Clinical observations from his work show that integrative methods restore mobility, reduce pain, and improve quality of life by treating the whole person—not just symptoms (Dralexjimenez.com, n.d.; A4m.com, n.d.).
Simple Ways to Start Spinal Hygiene Today
You can begin with easy changes that fit into daily life.
Posture checks: Set reminders to sit tall and take breaks from sitting every 30 minutes.
Daily stretches: Try cat-cow pose, child’s pose, or seated twists for 5-10 minutes.
Safe lifting: Always bend at the knees and use your legs.
Stay hydrated: Drink water throughout the day to keep your discs healthy.
Eat spine-friendly foods: Include leafy greens, fish, nuts, and dairy or alternatives for key nutrients.
Move often: Walk or do low-impact activity for at least 30 minutes most days.
Manage stress: Practice deep breathing or short meditation sessions.
Adding regular chiropractic check-ups can help monitor and maintain progress (Lifemovesmt.com, n.d.; Newlifefamilychiropractic.net, n.d.).
Final Thoughts
Spinal hygiene is a smart, everyday way to protect one of your body’s most important parts. By focusing on posture, movement, nutrition, and professional care when needed, you support a strong spine, healthy nerves, and a better quality of life. Small habits add up to big benefits, helping you stay active and pain-free for years.
Innovations in Sciatica Treatment in 2026: A Shift Toward Targeted, Minimally Invasive, and Integrative Care
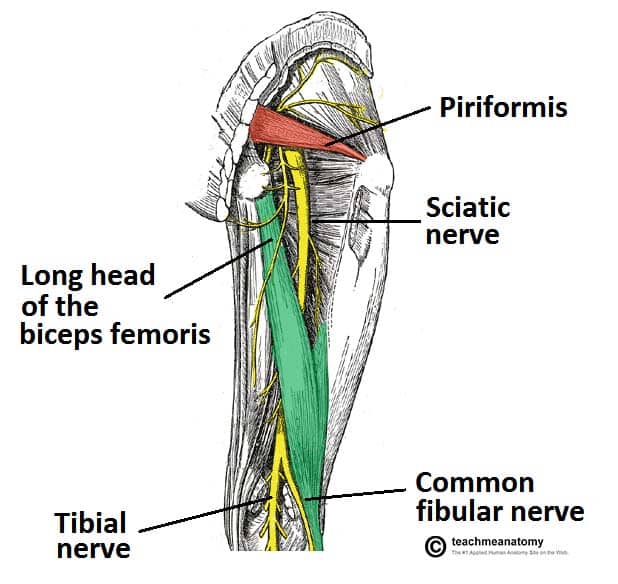
Sciatica is one of the most common causes of chronic lower back and leg pain. It occurs when the sciatic nerve—the longest nerve in the body—is irritated or compressed, often due to disc herniation, spinal degeneration, inflammation, or biomechanical imbalance. For years, treatment options focused mainly on pain medications, steroid injections, or surgery when symptoms became severe.
In 2026, sciatica care has entered a new phase. Treatment is no longer just about “blocking pain.” Instead, the focus is on precision diagnosis, nerve healing, inflammation reduction, and functional recovery, with fewer complications and faster healing times. These advances also emphasize integrated, interdisciplinary care, combining chiropractic treatment with the diagnostic and clinical oversight of nurse practitioners (NPs).
This article explains the most important innovations shaping sciatica treatment in 2026, using easy-to-understand language while staying grounded in current clinical research and real-world outcomes.
Understanding Sciatica: Why Better Solutions Were Needed
Sciatica is not a single disease. It is a symptom caused by pressure or irritation along the sciatic nerve, usually beginning in the lower spine and traveling into the buttock and leg. Pain can feel sharp, burning, electric, or aching and may include numbness or weakness.
Common contributors include:
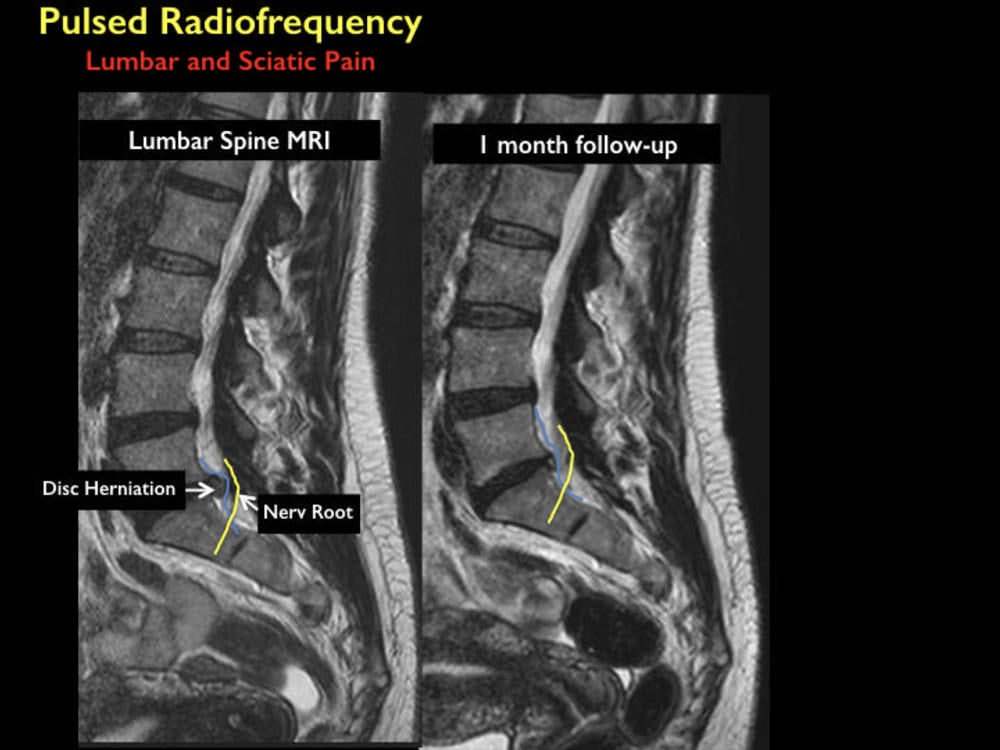
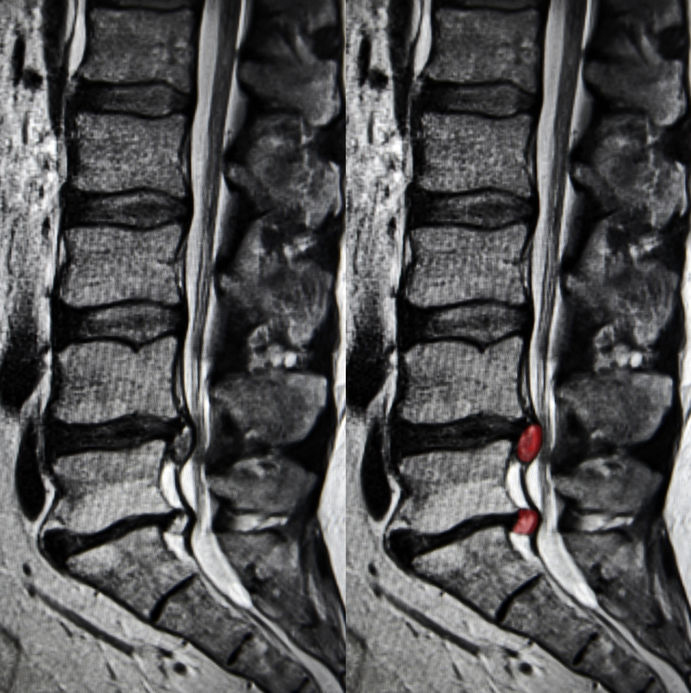
Herniated or bulging lumbar discs
Spinal stenosis
Degenerative disc disease
Muscle imbalance or pelvic instability
Inflammation around nerve roots
Traditional treatments often relied on:
Long-term anti-inflammatory or pain medications
Opioids for severe cases
Epidural steroid injections
Surgery as a last resort
While these approaches helped some patients, they did not always address the underlying cause, and many carried risks such as dependency, complications, or prolonged recovery (Stanford Health Care, n.d.).
What Has Changed in 2026?
By 2026, sciatica treatment emphasizes early, targeted, and minimally invasive care. Research and clinical experience now show that addressing nerve irritation early and restoring healthy movement patterns can prevent chronic pain and disability (BioSpace, 2025).
Key changes include:
Improved imaging and diagnostics
Precision-guided nerve procedures
Regenerative medicine options
Advanced neuromodulation technologies
Integrated chiropractic and NP-led care models
Advanced Diagnostic Imaging: Seeing the True Source of Pain
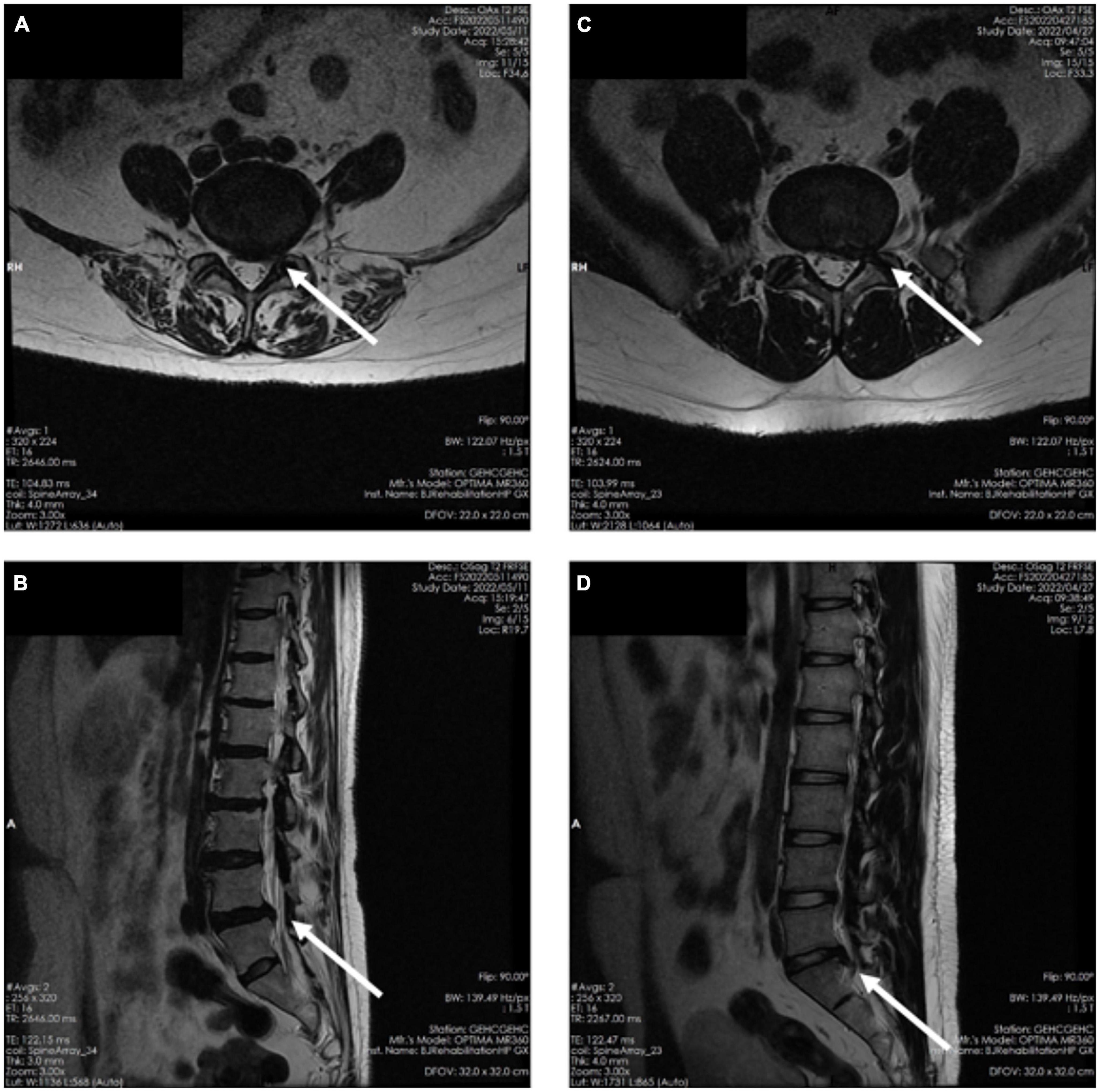
One of the biggest improvements in sciatica care is high-resolution MRI technology. Modern imaging allows clinicians to:
Identify the exact nerve root involvement
Distinguish disc-related pain from muscular or inflammatory causes
Detect subtle nerve inflammation missed in earlier imaging methods
Enhanced MRI protocols now guide treatment decisions more accurately, reducing unnecessary procedures and improving outcomes (Stanford Health Care, n.d.).
Nurse practitioners play a critical role here by:
Ordering and interpreting imaging
Correlating findings with physical symptoms
Coordinating referrals and follow-up care
Minimally Invasive Pain Procedures: Precision Without Surgery
Improved Nerve Blocks
Modern nerve blocks are no longer “blind injections.” In 2026, they are image-guided and highly targeted, delivering medication exactly where inflammation and irritation occur.
Benefits include:
Faster pain relief
Reduced medication dosage
Improved diagnostic clarity
Lower complication risk
Nerve blocks are now often used as diagnostic tools to help clinicians determine whether pain is mechanical, inflammatory, or neuropathic in origin (Apollo Spine & Pain, 2026a).
Radiofrequency Ablation (RFA)
Radiofrequency ablation uses controlled heat to disrupt pain signals traveling through irritated nerves. Newer RFA systems are more precise and selective than earlier versions.
Key advantages:
Long-lasting pain relief
Minimal tissue damage
Short recovery time
Reduced reliance on medications
RFA is especially helpful for chronic sciatica that does not respond to conservative care (Apollo Spine & Pain, 2026b).
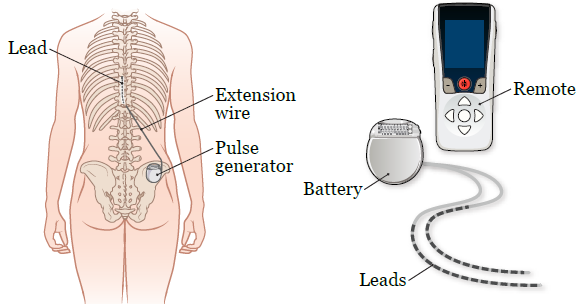
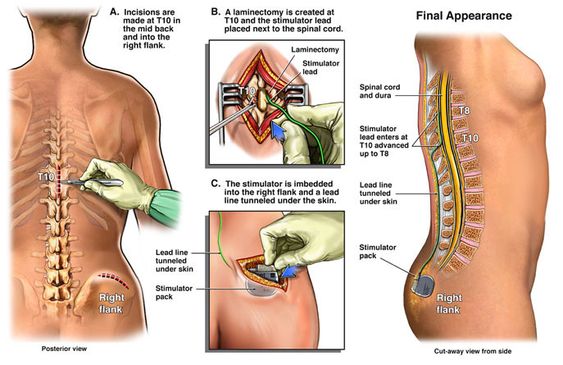
Spinal Cord Stimulation: Rewiring Pain Perception
Spinal cord stimulation (SCS) has evolved significantly. New devices are smaller, smarter, and more adaptive. They deliver gentle electrical signals that change how the brain interprets pain signals from the sciatic nerve.
Modern SCS systems offer:
Personalized stimulation patterns
Adjustable settings via external controllers
Reduced side effects compared to older models
SCS is now used earlier in care for select patients, helping many avoid surgery altogether (Pain and Spine Specialists, n.d.).
Regenerative Medicine: Supporting Nerve Healing
Platelet-Rich Plasma (PRP)
PRP therapy uses a patient’s own blood components to promote healing and reduce inflammation. In sciatica care, PRP is increasingly used around:
Inflamed nerve roots
Degenerative disc structures
Surrounding soft tissues
Research suggests PRP may:
Reduce inflammation
Support tissue repair
Improve long-term outcomes
While still evolving, regenerative therapies are driving growth in the global sciatica treatment market (Grand View Research, n.d.; PMC, 2024).
Therapeutic Exercise Innovations: Movement as Medicine
Nerve Flossing and Targeted Rehab
Exercise therapy in 2026 is more specific and personalized. One standout approach is nerve flossing, which involves controlled movements designed to improve nerve mobility and reduce irritation.
Benefits include:
Improved nerve glide
Reduced stiffness
Decreased pain during daily activities
Programs are now customized using imaging findings and functional testing, ensuring exercises match the patient’s specific condition (Goodman Campbell, 2026).
Chiropractic Care: A Drug-Free Foundation
Chiropractic care remains central to non-surgical sciatica treatment. Modern chiropractic approaches focus on restoring spinal alignment, reducing nerve compression, and improving movement patterns.
Common techniques include:
Spinal adjustments
Flexion-distraction therapy
Soft tissue mobilization
Low-level laser therapy
Research continues to associate chiropractic care with reduced opioid use and improved pain outcomes (ReachMD, 2024; UH Hospitals, 2025).
Integrated Care: Chiropractors and Nurse Practitioners Working Together
One of the most important shifts in 2026 is the collaborative care model. Instead of isolated treatment, patients benefit from coordinated care involving chiropractors and nurse practitioners.
This model allows for:
Accurate diagnosis and imaging oversight
Conservative, drug-free pain management
Monitoring of neurological symptoms
Reduced opioid exposure
Clinical observations from Dr. Alexander Jimenez, DC, APRN, FNP-BC, highlight that patients receiving coordinated chiropractic and NP care often experience:
Faster recovery
Better functional improvement
Fewer invasive interventions
Greater long-term pain control
His integrative approach emphasizes treating the cause of nerve irritation, not just the symptoms (Jimenez, n.d.).
Why These Innovations Matter
Together, these advances represent a major shift in sciatica care:
From surgery-first to conservative-first
From symptom masking to root-cause resolution
From isolated care to interdisciplinary teamwork
Patients now have more options, fewer risks, and better long-term outcomes.
Conclusion: The Future of Sciatica Care Is Personalized and Precise
By 2026, sciatica treatment has become more effective, safer, and patient-centered. Innovations in diagnostics, minimally invasive procedures, regenerative medicine, and integrative chiropractic-NP–NP care are reducing the need for surgery and long-term medication use.
The focus is no longer just pain relief—it is nerve health, mobility restoration, and sustainable recovery. As research and technology continue to evolve, patients suffering from sciatica can expect even more targeted, evidence-based solutions in the years ahead.
Relieve Lower Back and Hip Pain with Squats, Core Exercises, and Chiropractic Care at El Paso Back Clinic®
Many people in El Paso suffer from lower back pain and hip discomfort due to daily activities, work demands, injuries, or long-term issues. These problems often stem from muscle strains, poor posture, tight hips or glutes, and weak supporting muscles. At El Paso Back Clinic® in El Paso, TX, we specialize in helping patients overcome these challenges through personalized chiropractic care, rehabilitation, and safe exercises.
Squats and core exercises, performed correctly, strengthen the muscles that support the spine, improve alignment, and enhance hip mobility. This reduces stress on the back during movement. They are effective for chronic low back pain, mild sciatica, and general aches from weak muscles. Proper form is essential—sharp pain, numbness, or weakness means you should seek professional evaluation first.
Strong Core + Chiropractic for Lower Back and Hip Pain Relief
The lower back and hips are closely connected through shared muscles, joints, and nerves. Tight hips or glutes can tug on the back, leading to strain. Weak core muscles cause spinal instability and poor posture, leading to chronic pain.
Muscle imbalances force the back to overcompensate in everyday tasks.
Reduced hip mobility leads to excessive forward leaning, stressing the lower back.
Problems in ankle or upper back mobility contribute further.
These factors can result in lumbar instability or pain radiating from the hips to the back.
How Squats Benefit Lower Back and Hip Conditions
Squats strengthen the legs, glutes, and core. With proper technique, they relieve pressure from the lower back.
Proper squats maintain a neutral spine and engaged core, providing stability and minimizing lumbar strain. Activating core and hip muscles during squats supports the spine, preventing excessive arching or rounding.
Squats also increase hip mobility. Tight hip flexors are a common cause of back pain during deeper squats. Improved flexibility allows the hips to function better, sparing the back from overload.
Builds glutes and legs for stronger spinal support.
Enhances blood flow and reduces inflammation in the area.
Aids mild pain that improves with gentle activity.
Research supports that the correct form reduces risks associated with squats.
Core Exercises: A Key to Back and Hip Relief
Core exercises focus on deep muscles in the abdomen, back, and pelvis, acting as a natural spinal brace.
Strong core muscles enhance posture and balance, easing the load on spinal discs and preventing persistent pain from inadequate support. Studies show core stability exercises effectively reduce non-specific low back pain and improve function.
Core training also supports hip pain by stabilizing the pelvis, which is beneficial for conditions like arthritis or glute tightness.
Planks and bird-dogs develop endurance in stabilizing muscles.
Pelvic tilts and bridges safely activate deep muscles.
Standing core activities help relieve pain from prolonged sitting.
Evidence indicates that core exercises often outperform general workouts in reducing pain.
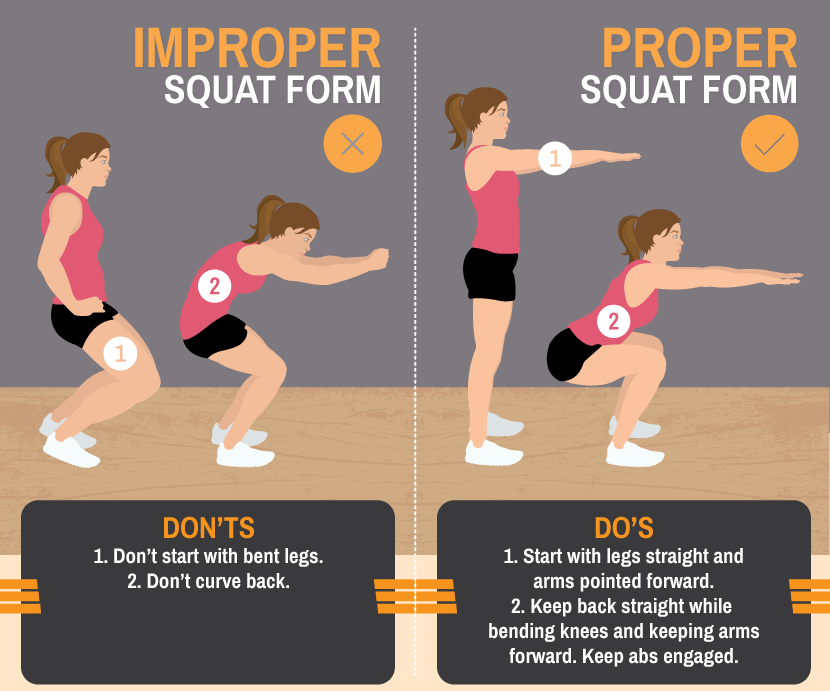
Mastering Proper Form for Safe Squats and Core Work
Incorrect squat form is a leading cause of lower back pain. Frequent mistakes include back rounding, knee collapse, or excessive weight.
Safe squat guidelines:
Position feet shoulder-width apart, toes slightly turned out.
Engage your core as if bracing for impact.
Hinge at the hips, keep the chest high, and descend until the thighs are parallel to the ground.
Drive up through heels, maintaining a neutral spine.
For core exercises, prioritize controlled movement. Hold planks straight with tight abs—avoid dipping or arching.
Begin with bodyweight versions and always warm up to boost circulation and lower injury risk.
Pain during squats typically indicates a weak core, tight hips, or mobility deficits. Address these with targeted stretches and progressive loading.
When Exercises Are Helpful and When to Get Professional Care
Squats and core exercises support:
Chronic low back pain from muscle weakness.
Mild sciatica by decreasing nerve pressure.
Hip tightness referring pain to the back.
Posture-related daily discomfort.
They foster long-term resilience and prevent compensatory back strain. Halt immediately if experiencing severe pain, numbness, weakness, or loss of balance—these may indicate serious conditions such as a disc herniation.
Consult a provider before beginning, especially if you have pre-existing injuries.
Integrative Care at El Paso Back Clinic®
At El Paso Back Clinic®, Dr. Alexander Jimenez, DC, APRN, FNP-BC, leads a team that delivers comprehensive, integrative chiropractic and wellness care for lower back and hip pain. Our approach combines squats and core exercises with chiropractic adjustments, spinal decompression, physical therapy, functional medicine, and rehabilitation programs.
Chiropractic adjustments correct misalignments and joint dysfunctions. A reinforced core helps maintain these corrections by enhancing spinal stability.
Dr. Jimenez creates tailored plans that address root causes through evidence-based protocols, drawing on over 30 years of experience in complex injuries, sciatica, and chronic pain. This multidisciplinary method often yields superior, sustained results compared to isolated treatments.
Visit our main location at 11860 Vista Del Sol, Suite 128, El Paso, TX 79936, or call (915) 850-0900 to schedule your consultation.
Beginner Exercises to Try Under Guidance
Start with these fundamentals, supervised by our team:
Bodyweight Squats: 3 sets of 10-15 repetitions, emphasizing technique.
Glute Bridges: Lie on your back, and elevate your hips by engaging your glutes.
Bird-Dog: On hands and knees, extend opposite arm and leg while bracing core.
Planks: Maintain position for 20-30 seconds, gradually increasing duration.
Pelvic Tilts: On the back, press the lower back into the floor via a pelvic tilt.
Incorporate 2-3 sessions weekly. Include hip mobility work and advance gradually.
Regain Comfort and Mobility Today
At El Paso Back Clinic®, squats and core exercises form integral components of our rehabilitation strategies for lower back and hip pain. They fortify stabilizing muscles, correct alignment, and promote mobility to manage strains, poor posture, instability, and tightness.
Combined with expert chiropractic and integrative care under Dr. Alexander Jimenez, they deliver lasting strength and relief.
Reach out to El Paso Back Clinic® today. Our team will assess your needs and develop a customized plan for optimal recovery.
When You Don’t Stretch: Why Muscles Get Stiff, Movement Gets Harder, and Injuries Become More Likely
A patient with chronic back pain does targeted stretches.
If you rarely stretch, your body can start to feel “tight,” which can change how you move. Many people notice they can’t bend, twist, squat, reach overhead, or turn their head as easily as they used to. Over time, this can affect your flexibility, your range of motion (how far a joint can move), and how smooth and efficient your daily movements feel.
At El Paso Back Clinic, Dr. Alexander Jimenez, DC, APRN, FNP-BC, often explains this: when mobility decreases, the body starts to “compensate.” That means you move around a stiff area instead of through it, and those workarounds can build up stress in nearby joints and muscles (Jimenez, n.d.-a). This is one reason people can develop recurring back pain, neck stiffness, hip tightness, or shoulder irritation even without a single big injury.
What “Muscle Stiffness” Really Means
Muscle stiffness usually feels like tightness, soreness, or difficulty moving. It can happen after overuse, after you’ve been still for a long time, or when your muscles stay “stuck” in a more contracted state (Tarantino, 2025). Osmosis
Osmosis notes that stiffness can appear after a long period of minimal motion (such as bed rest or inactivity) or after new exercise that causes temporary muscle cell damage (Tarantino, 2025). Osmosis
Key idea: When your body doesn’t move a joint through its normal range often enough, the muscles and tissues around it can start to feel restricted. That restriction can make normal tasks think harder than they should.
Do Muscles Actually “Shorten” If You Don’t Stretch?
You’ll hear people say, “If you don’t stretch, your muscles will shorten.” That statement is partly true, but it needs context.
Adidas explains that the word “shorten” can be misleading: for most people, it feels like shortening because mobility and flexibility decrease when stretching is skipped, even if the muscle is not literally shrinking in everyday life (Adidas, 2025). adidas
Harvard Health adds an important clarification: without regular stretching, muscles can become tight, and when you need them for activity, they may not extend fully, increasing the risk of joint pain, strains, and muscle damage (Harvard Health Publishing, 2024). Harvard Health
So the practical takeaway is simple:
Skipping stretching often leads to less mobility and flexibility
Tight muscles can reduce how far joints can move
Tight muscles can make injuries more likely when you suddenly “ask more” of your body
How Tight Muscles Reduce Range of Motion
Range of motion (ROM) is the movement around a joint or body part. When ROM is limited, you can’t move that body part through its usual, healthy motion (Jimenez, n.d.-b). El Paso Back Clinic® • 915-850-0900
El Paso Back Clinic explains how tightness—especially in areas like the hips and ankles—can reduce ROM and limit potential for form and strength. When posture and form are compromised, pain and injury risk can rise (Jimenez, n.d.-b). El Paso Back Clinic® • 915-850-0900
What limited ROM can look like in real life
You might notice:
You can’t turn your head fully when driving
You bend from your lower back instead of your hips
You can’t squat without your heels lifting
Your shoulders feel “pinched” when reaching into a cabinet
Your hamstrings feel tight when you try to walk fast
And here’s the tricky part: your body still gets the job done—just with more strain.
Why Stiffness Can Raise Injury Risk
Harvard Health explains that tight muscles may be more easily damaged when they are suddenly stretched during strenuous activity (Harvard Health Publishing, 2024). Harvard Health
That’s why injuries often show up in moments like:
A weekend game after sitting all week
A sudden sprint to catch something
Lifting a heavy box with “cold” hips and hamstrings
A long drive followed by quick unloading or bending
Mayo Clinic also notes that better flexibility can help joints move through full ROM and may decrease injury risk, while emphasizing that stretching must be done correctly (Mayo Clinic Staff, n.d.). Mayo Clinic
Common Reasons People Stop Stretching (And How to Fix Them)
Most people don’t skip stretching because they don’t care. They skip it because it feels confusing, time-consuming, or uncomfortable.
Common barriers
“I don’t have time.”
“Stretching hurts.”
“I’m not flexible, so it doesn’t work for me.”
“I only need stretching if I work out.”
Better, more realistic reframes
You only need 5–10 minutes a few times a week to start seeing benefits (Mayo Clinic Staff, n.d.). Mayo Clinic
Stretching should create tension, not pain (Mayo Clinic Staff, n.d.). Mayo Clinic
Flexibility improves over weeks to months, not days (Harvard Health Publishing, 2024). Harvard Health
Stretching supports everyday movement, not just workouts (Harvard Health Publishing, 2024). Harvard Health
Safe Stretching Basics (So You Don’t Make Things Worse)
This matters: stretching done poorly can backfire.
Mayo Clinic recommends:
Don’t stretch cold muscles—warm up 5–10 minutes first
Don’t bounce
Hold stretches about 30 seconds (longer for problem areas)
Don’t stretch into pain (Mayo Clinic Staff, n.d.). Mayo Clinic
The American Heart Association adds:
Stretch when muscles are warm
Hold 10–30 seconds and repeat 3–5 times
Stretch slowly and smoothly (American Heart Association, 2024). www.heart.org
Quick safety checklist
Warm up first (easy walk, gentle movement)
Move slowly
Breathe
No bouncing
Stop if you feel sharp pain, numbness, or joint pain
A Simple 10-Minute Daily Stretch Routine for Real Life
This is designed for normal adults: busy schedules, stiff hips, tight neck, and lots of sitting.
Step 1: Warm up (1–2 minutes)
Walk around the house
March in place
Gentle arm circles
Step 2: Do these 6 stretches (about 8 minutes total)
1) Hip flexor stretch (1 minute each side) Helps if you sit a lot and feel tight in the front of your hips.
2) Hamstring stretch (1 minute each side) Harvard points out that tight hamstrings from sitting can limit how well you extend your leg and support walking mechanics (Harvard Health Publishing, 2024). Harvard Health
3) Calf stretch (45 seconds each side) Helpful for ankle mobility, walking, and squatting mechanics.
4) Chest opener (45 seconds) Stand in a doorway and gently open the chest to reduce rounded-shoulder posture.
5) Upper back reach (45 seconds) Hug yourself and gently pull your shoulder blades apart.
6) Neck side stretch (30 seconds each side) Gentle only—never crank your neck.
Step 3: Add “micro-mobility” during your day (optional but powerful)
Stand up every hour for 30–60 seconds
Do 5 bodyweight squats to a chair
Do 10 shoulder rolls
Take a 3-minute walk after meals
These small habits often matter as much as one long stretch session.
Stretching After Workouts: What You Should Know
Adidas explains the difference clearly:
Dynamic movement is best before workouts (prepares your body)
Static stretching is typically better after workouts, when you’re warm (Adidas, 2025). adidas
Mayo Clinic also cautions that stretching cold muscles can increase injury risk and notes that some intense activities may not benefit from heavy stretching right before performance (Mayo Clinic Staff, n.d.). Mayo Clinic
A balanced approach
Before exercise: warm up + dynamic mobility
After exercise: gentle static stretching + breathing
On rest days: short, consistent flexibility routine
When Stiffness Is a Sign You Need More Than Stretching
Sometimes the problem is not just “tight muscles.” You may have:
Joint restrictions that block movement
Spine or pelvis alignment issues affecting mechanics
Inflammation around a joint
Pain patterns that keep muscles “guarded”
A nerve-related problem (numbness, tingling, weakness)
El Paso Back Clinic notes that limited ROM in areas like the back, neck, or shoulders can be linked to the body being out of natural alignment, repetitive motions, or wear and tear (Jimenez, n.d.-b). El Paso Back Clinic® • 915-850-0900
If stretching doesn’t help—or makes symptoms worse—it’s smart to get assessed.
The El Paso Back Clinic Approach: Integrative Chiropractic + Nurse Practitioner Support
This is where integrative care can be a game-changer: you’re not only “stretching more,” you’re also finding out why you’re tight and building a plan that fits your body.
What chiropractic care can add
El Paso Back Clinic describes a “restoration” approach that may include:
Soft tissue work (to reduce tightness and improve circulation)
Adjustments (to address misalignments and support mobility)
Nurse practitioners are advanced practice clinicians who assess, diagnose, and treat illnesses and injuries and support chronic condition management (American Nurses Association, n.d.). ANA Healthgrades also describes NPs performing screenings and physical exams, ordering lab work, documenting care, and diagnosing certain conditions (Prosser, 2025). Healthgrades Resources
Why the combo helps stiffness and pain
Together, a chiropractor + NP team can:
Screen for red flags (nerve symptoms, systemic issues)
Decide when imaging or labs are appropriate
Build a movement plan that matches your pain level
Address sleep, stress, inflammation, and recovery habits
Track progress using measurable goals (like ROM improvements)
Dr. Jimenez’s Mobility & Flexibility materials emphasize that “great mobility” supports functional movement without ROM restrictions and that people who don’t stretch often may experience stiffened muscles that reduce effective movement (Jimenez, n.d.-a). El Paso Back Clinic® • 915-850-0900
Red Flags: When to Stop Stretching and Get Checked
Call a clinician promptly if you have:
Numbness, tingling, or weakness in an arm/leg
Loss of balance, clumsiness, or trouble walking
Severe pain that doesn’t improve
Pain after trauma (car accident, fall, sports collision)
Fever, unexplained swelling, or sudden intense stiffness
Muscle stiffness can sometimes be related to underlying medical issues, and diagnosis may require an exam and follow-up testing, depending on the cause (Tarantino, 2025). Osmosis
The Bottom Line
If you don’t stretch regularly, it’s common to feel tighter and less mobile over time. That stiffness can reduce range of motion, make daily tasks harder, and increase your risk of injury when you suddenly push your body. The good news is that you don’t need extreme flexibility. You need consistent, safe mobility work—and when required, professional support to restore movement and reduce pain.
A practical plan usually includes:
Small daily stretching habits
Better warm-ups and recovery routines
Strength + mobility (not stretching alone)
Integrative evaluation when pain, ROM loss, or repeated flare-ups keep returning
Real-Life Posture Rehab: How El Paso Back Clinic Helps You Move Better Every Day
Move around and change posture positions throughout the day.
Improving posture is one of the fastest ways to feel stronger, breathe easier, and protect your spine—especially if you live with long commutes, heavy work, or hours at a desk, like many people in El Paso. At El Paso Back Clinic, Dr. Alexander Jimenez, DC, APRN, FNP-BC, and his team see every day how targeted physical activity, along with integrative chiropractic and nurse practitioner (NP) care, can turn slouching and stiffness into confident, upright movement. El Paso, TX Doctor Of Chiropractic+1
This article explains, in simple language:
What good posture really is
Recommended physical activities and exercises to enhance posture
How yoga, Pilates, and mind-body practices improve alignment
Easy desk and “tech neck” fixes
How integrative chiropractic care supports posture
How nurse practitioners help with medical, ergonomic, and lifestyle support
How the El Paso Back Clinic combines all of this in real-world care
What “Good Posture” Means (and Why It Matters in Daily Life)
Good posture means your body is stacked in a natural, balanced way:
Ears over shoulders
Shoulders over hips
Hips over knees and ankles
Spine holding its natural curves (neck, mid-back, low back)
When posture is poor—like slouching over a phone or leaning forward at a desk—stress builds up in your neck, shoulders, and back. Over time, this can lead to:
Chronic neck and back pain
Tension headaches
Fatigue and shallow breathing
Tight hip flexors and weak glutes
Early joint wear and tear
Research and clinical guides show that specific exercises and posture-friendly habits can reduce pain and improve alignment by strengthening postural muscles and keeping you moving throughout the day. Healthline+2Harvard Health+2
At El Paso Back Clinic, Dr. Jimenez often reminds patients that posture is not about “standing stiff.” It is about a strong, relaxed, and mobile spine that can handle work, sports, and life in the desert heat. El Paso, TX Doctor Of Chiropractic+1
Core Principles of Posture-Focused Exercise
Most effective posture plans share the same core goals:
Strengthen the core and back—so your spine has solid support
Activate glutes and shoulders—to counter slumping and hip stress
Improve flexibility—especially in chest, hip flexors, and hamstrings
Train body awareness—so you notice and correct slouching
Add low-impact cardio—to boost circulation and recovery
Think of Your Program in Simple Pieces
Try to include each week:
2–3 days of core and back strengthening
2–3 days of mobility and stretching
2–4 days of low-impact cardio like walking or swimming
Daily micro-breaks from sitting or driving
That may sound like a lot, but many of these can be done in 10–20 minute blocks and woven into your normal day.
Foundational Strength Exercises for Better Posture
Many posture programs start with bodyweight moves you can do at home—no machines, no fancy equipment. Sources on physical therapy and spine health support these exercises. Healthline+2Primal Physical Therapy+2
Planks (Front and Side Planks)
Why they help: Planks strengthen your deep core, shoulders, and glutes. A strong core keeps your spine from sagging or arching too much.
Basic front plank:
Start on your forearms and toes
Keep your body in a straight line from head to heels
Gently pull your belly toward your spine
Hold 20–30 seconds, rest, repeat 2–3 times
Side planks add extra stability for your sides and hips, which support upright posture. Woodlands Sports Medicine
Bird-Dog
Why it helps: Bird-dog builds core and back strength while training balance and control.
How to do it:
Start on hands and knees
Extend your right arm forward and left leg back
Keep your hips level; don’t twist
Hold 3–5 seconds, then switch sides
Do 8–10 reps per side
Physical therapists often use this exercise to improve posture and relieve back pain. Primal Physical Therapy+1
Glute Bridges
Why they help: Bridges work the glutes and hamstrings and relieve stress on the lower back.
Lie on your back, knees bent, feet flat
Press through your heels and lift your hips
Squeeze your glutes at the top
Hold 3–5 seconds, then lower
Repeat 10–15 times
Strong glutes help balance tight hip flexors from long periods of sitting, which is very common among drivers and office workers in El Paso. Primal Physical Therapy+1
Superman Exercise
Why it helps: The Superman move targets the “posterior chain,” the muscles along the back of your body that help prevent slouching. Woman & Home
Lie face down
Lift your chest, arms, and legs slightly off the floor
Hold briefly and lower with control
Start with 5–8 reps
This move is especially useful if you sit a lot or look down at screens, as it helps your back muscles stay active.
Rowing Movements (Bands or Dumbbells)
Why they help: Rowing exercises strengthen the upper back and shoulder stabilizers that pull your shoulders back.
Use a resistance band or light dumbbells
Pull your elbows back and squeeze your shoulder blades together
Mobility and Stretching: Releasing the “Posture Brakes”
If strength is the “engine,” tight muscles are the “brakes.” You need both to work well. Stretching and mobility exercises help open areas that tend to tighten up, such as the chest, neck, hips, and upper back. Illinois Back Institute+1
Key Posture Stretches
Chest Opens / Doorway Stretch
Stand in a doorway with your forearms on the frame
Gently lean forward until you feel a stretch across your chest
Gently slide your chin straight back (like a mini “double chin”)
Hold 3–5 seconds
Repeat 10 times
Cat-Cow
On hands and knees
Slowly round your back toward the ceiling, then gently arch it
Move with your breath for 8–10 cycles
Hip Flexor Stretch
In a half-kneeling position, gently shift your hips forward
Keep your torso upright; avoid over-arching your back
Hold 20–30 seconds on each side
These stretches are simple but powerful when done daily—especially if you spend long hours driving I-10 or sitting at a workstation in El Paso. Illinois Back Institute+1
Mind-Body Practices: Yoga, Pilates, and Tai Chi
Mind-body exercises are excellent for posture because they combine strength, flexibility, and body awareness.
Yoga for Alignment and Awareness
Yoga routines often include:
Mountain Pose (Tadasana)—teaches what upright alignment feels like
Child’s Pose and Cat-Cow – gently move and decompress the spine
Bridge Pose – strengthens glutes and back
Chest opener poses—counter phone and computer hunching
Research-based guides show yoga can improve postural muscle endurance and help people become more aware of how they carry themselves. Healthline+1
Pilates for Core Control
Pilates focuses on:
Deep core strength
Controlled breathing
Smooth, precise movements
Many physical therapy and rehab programs use Pilates-style exercises to support spinal alignment and postural stability. Primal Physical Therapy+1
Tai Chi for Balance and Relaxed Upright Posture
Tai chi uses slow, flowing movements with calm breathing. It helps:
Improve balance and coordination
Encourage relaxed, upright posture
Reduce stress and muscle guarding
Chiropractic resources often recommend swimming, walking, yoga, and tai chi as ideal companions to chiropractic care. Muscle and Joint Chiropractic+1
Everyday Physical Activities That Support Posture
You don’t have to become a gym athlete to help your posture. Many everyday activities, done with good form, support a healthier spine.
Helpful posture-friendly options include:
Walking:
Encourages natural spinal motion
Easy to fit into breaks or evenings
Swimming:
Full-body, low-impact workout
Strengthens back and shoulder muscles with less joint stress
Dancing:
Builds coordination and body awareness
Helps you practice an upright chest and an active core
Cycling (with proper bike fit):
Strengthens hips and legs
Supports overall fitness and endurance
Clinics that treat back pain often highlight walking and swimming as key activities for long-term spinal health. Illinois Pain & Spine Institute+1
Desk, Phone, and “Tech Neck”: Quick Fixes You Can Actually Use
Long hours on a computer or phone are a major reason posture has become such a problem. Harvard Health and orthopedic clinics stress the importance of frequent movement breaks and simple desk exercises. Harvard Health+2barringtonortho.com+2
Desk-Friendly Posture Break Routine
Try this mini-routine a few times each day:
Chin tucks – 10 reps
Shoulder blade squeezes – hold 5 seconds × 10 reps
Seated Cat-Cow – 5–10 slow breaths
Forward fold stretch next to your desk—hold 20–30 seconds
Simple Ergonomic Tips
Keep feet flat on the floor
Hips and knees are near 90 degrees
Screen at or just below eye level
Use a small lumbar support or rolled towel behind your low back
Stand and walk at least every 30–60 minutes
Recent expert tips also support using standing desks, wireless headphones for “walking meetings,” and light resistance bands at your station to keep postural muscles awake. Harvard Health+1
How Integrative Chiropractic Care at El Paso Back Clinic Supports Posture
Chiropractic care focuses on the spine, joints, and nervous system. Integrative chiropractic care goes further, combining adjustments with corrective exercises, lifestyle coaching, and medical input from NPs. Advanced Spine & Posture+1
What a Posture-Focused Chiropractic Visit Often Includes
The Nurse Practitioner’s Role in Supporting Posture
At El Paso Back Clinic, Dr. Jimenez works not only as a chiropractor but also as a board-certified family nurse practitioner, which provides a broader, medically informed perspective on posture-related problems. El Paso, TX Doctor Of Chiropractic+1
A nurse practitioner can:
Review your full medical history
Identify arthritis, osteoporosis, nerve issues, or autoimmune conditions that affect posture.
Order and interpret imaging and labs
X-rays, MRIs, and blood work when appropriate
Prescribe or adjust medications
Short-term pain or muscle-relaxant use when necessary
Coordinate referrals
Physical therapy, pain management, and surgical consults if needed
Give lifestyle and ergonomic counseling
Weight management, sleep, stress, and work setup
Use telemedicine for follow-up
To keep you on track with your exercise and pain management plan
This integrative model makes it easier to catch red flags early, adjust plans safely, and provide each patient with a personalized path rather than a one-size-fits-all list of exercises.
How Dr. Alexander Jimenez Combines Physical Activity, Chiropractic Care, and NP Expertise
With decades of experience in personal injury, sports, and functional medicine, Dr. Jimenez has seen the same pattern again and again: posture improves the most when hands-on care, smart exercise, and patient education are combined. El Paso, TX Doctor Of Chiropractic+2El Paso, TX Doctor Of Chiropractic+2
In his clinical observations at El Paso Back Clinic:
Agility and functional training (such as controlled squats, lunges, and balance drills) help patients return to sports, warehouse work, or family life with greater resilience.
Posture work is often integrated with nutrition, sleep, and stress management, because tired, inflamed bodies struggle to maintain good alignment. El Paso, TX Doctor Of Chiropractic+1
This dual license (DC + APRN, FNP-BC) allows Dr. Jimenez to move comfortably between spine mechanics and whole-person health, which is ideal for complex posture and pain cases.
Sample Weekly Posture-Boosting Plan (General Example)
This is a general example for educational purposes, not a personal prescription. Always consult your provider—especially if you have pain, injuries, or medical conditions.
Posture check around your home and car: adjust chairs, pillows, and monitor height
Patients at El Paso Back Clinic often have a plan customized to their injury type (auto accident, work injury, or sports strain) and their job or sport. El Paso Back Clinic® • 915-850-0900+1
Safety Tips: When to Get Help
Stop and get professional care if posture exercises cause:
Sharp or stabbing pain
Numbness or tingling in arms or legs
New weakness or loss of coordination
Trouble walking or standing
Loss of bladder or bowel control (emergency—seek urgent care)
A chiropractor can evaluate your spine and joints; a nurse practitioner can check for underlying medical causes. At El Paso Back Clinic, the team works together to decide whether you need imaging, medication, rehab, or a referral to another specialist. El Paso, TX Doctor Of Chiropractic+1
Bringing It All Together
To enhance posture and protect your spine:
Strengthen your core, back, and glutes with planks, bridges, bird-dogs, rows, and Supermans
Stretch your chest, neck, and hips to release tight, “slouching” muscles
Use mind-body practices like yoga, Pilates, and tai chi to build body awareness
Add low-impact activities like walking and swimming to support overall spine health
Fix your desk and phone habits with regular movement breaks and better ergonomics
At El Paso Back Clinic, integrative chiropractic care and nurse practitioner support bring all of these pieces together. With Dr. Alexander Jimenez’s dual training, patients receive:
Spinal and joint adjustments
Corrective exercise and posture coaching
Medical evaluation, imaging, and medication management when needed
Telemedicine and follow-up plans that fit real life in El Paso
The goal is simple: help you stand taller, move with less pain, and feel stronger in everything you do—from lifting kids or boxes at work to walking the trails of the Franklin Mountains.
Faster Recovery After Spine Surgery: Enhanced Surgical Recovery (ESR) Programs at El Paso Back Clinic® in El Paso, TX
The doctor administers a local anesthetic into the patient’s affected area, using ultrasound to visualize the spine’s anatomical components.
Spine surgery can help treat serious back problems, such as pain from injuries, disc issues, or aging. At El Paso Back Clinic® in El Paso, TX, we focus on helping patients recover faster and more safely through modern methods. Enhanced Surgical Recovery (ESR), also called Enhanced Recovery After Surgery (ERAS), is a team-based plan that reduces the need for strong pain medications, shortens hospital stays, and lowers the risk of readmission. Led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, our clinic combines chiropractic care, nurse practitioner expertise, and new tools to support healing. This article explains the main parts of ESR for spine surgery, how it cuts opioid use, shortens hospital stays, and reduces readmissions. We also cover the big roles of integrative chiropractic care and nurse practitioners, plus exciting new tech like virtual reality (VR) for building strength after surgery.
Many people in El Paso face back pain from work, accidents, or daily life. Surgery may be necessary, but traditional methods can make recovery challenging. ESR improves this process by planning care before, during, and after the operation. It uses simple steps, such as teaching patients, eating better, and moving early. Studies show these measures can cut opioid use a lot and help people go home sooner (Dagal et al., 2023). At El Paso Back Clinic®, we work with surgeons to add non-drug options for even better results.
What Is Enhanced Surgical Recovery (ESR)?
ESR is a proven plan to make surgery recovery easier and quicker. It started in other surgeries, but now helps a lot with spine operations, such as fusions or disc repairs. The idea is to lower body stress and speed natural healing. Instead of staying in bed and taking many pain pills, patients move soon and use gentler pain control.
Key parts of ESR include:
Team Approach — Doctors, nurses, chiropractors, and therapists all work together.
Step-by-Step Care — Planning starts before surgery and continues at home.
Personal Plans — Care fits each person’s health needs.
Research shows ESR helps with many spine issues, from small fixes to big ones (Zaed et al., 2023). Reviews find that most programs use around 12 key steps, such as better pain management and early walking (Berk et al., 2025).
Main Components of ESR for Spine Surgery
ESR has steps before, during, and after surgery to make things smoother.
Before Surgery (Pre-Op)
Getting ready early helps avoid problems.
Teaching Patients: Learn what to expect, how to manage pain, and why moving matters. This lowers worry and helps follow the plan (Zaed et al., 2023).
Better Nutrition: Check for low energy or anemia. Eat protein and carbs to build strength. Nutritious food helps healing (Soffin et al., 2022).
Pain Prep: Start gentle meds like acetaminophen. Quit smoking to lower risks (American Association of Nurse Anesthesiology, n.d.).
Prehab Exercises: Build strength with walks or stretches.
These make surgery safer.
During Surgery (Intra-Op)
The team uses ways to protect the body.
Better Anesthesia: Short drugs to wake up fast. Add non-opioid options (Dagal et al., 2023).
Careful Fluids: Just the right amount to avoid issues.
Small Cuts: Less muscle damage for quicker recovery (Dietz et al., 2019).
Pain Blocks: Numb the area for hours after.
Patients feel better right away.
After Surgery (Post-Op)
Focus on rapid healing.
Early Walking: Get up soon and walk daily (Zaed et al., 2023).
Mixed Pain Control: Use non-opioids, ice, and movement.
Quick Eating: Start foods and drinks early.
Checks for Safety: Watch for clots or other issues.
These steps lower risks.
How ESR Reduces Opioid Use
Strong pain drugs like opioids help, but can lead to problems like addiction. ESR cuts its use by at least half (Dagal et al., 2023). At El Paso Back Clinic®, we add chiropractic methods for even less need.
Mixed Pain Options: Non-opioids first, like NSAIDs and nerve meds. Some programs use almost no IV opioids (HCA Healthcare, n.d.).
Teaching Non-Drug Ways: Ice, breathing, and adjustments.
Blocks and Early Move: Numb areas and walk to ease pain.
In fusions, opioids dropped considerably without worse pain (Dagal et al., 2023). This helps avoid side effects and promotes natural healing.
Shortening Hospital Stays with ESR
Long hospital time raises costs and risks. ESR cuts stay by 1-2 days (HCA Healthcare Today, 2022).
Early Movement: Prevents issues and builds strength.
Fast Nutrition: Energy for recovery.
Good Pain Control: Less bedtime.
Team Reviews: Go home when ready.
One example shows noticeable shortened stays (Dagal et al., 2023). Patients heal better at home.
Lowering Readmission Rates
Going back to the hospital is tough. ESR lowers this risk (HCA Healthcare Today, 2022).
Home Care Teaching: Know warning signs.
Follow-Ups: Calls from our team at El Paso Back Clinic®.
Fewer Problems: Better prep means fewer infections.
Full Care: Controls swelling early.
Fewer complications overall (Berk et al., 2025).
Integrative Chiropractic Care at El Paso Back Clinic®
Chiropractic care fits perfectly with ESR. At our clinic, Dr. Jimenez uses hands-on adjustments to align and relieve symptoms.
Before Surgery: Improve posture and movement.
Pain Without Drugs: Soft tissue work eases tension.
After Surgery: Reduce scar tissue and build mobility (New York City Spine, n.d.).
Nerve Help: Better signals for less pain.
We complement therapy for smoother recovery (Active Health Center, n.d.).
Role of Nurse Practitioners
Nurse practitioners (NPs) like Dr. Jimenez coordinate care.
Team Links: Connect everyone.
Teaching and Meds: Focus on safe, non-opioid options.
Tracking Progress: Adjust plans.
NPs help stick to ESR paths (American Association of Nurse Anesthesiology, n.d.).
New Tech: Virtual Reality (VR) for Recovery
VR uses games and guides to make rehab more enjoyable. It helps spine patients build strength.
Fun Exercises: Improves engagement and movement.
Less Pain Feel: Distraction helps.
Strength Gains: Tailored for muscles and focus.
Home Options: Practice alone.
Recent studies show VR speeds recovery after spine issues, like in cervical cases or general neurorehab (Bolton et al., 2025; various 2025 trials).
Insights from Dr. Alexander Jimenez at El Paso Back Clinic®
Dr. Alexander Jimenez, DC, APRN, FNP-BC, leads El Paso Back Clinic® with dual expertise in chiropractic and nursing. He uses team care for pain management and rehab after injuries or surgery. His plans include adjustments, nutrition, and integrative methods for better mobility without heavy drugs. He stresses whole-body healing for lasting results (Dr. Alex Jimenez, n.d.; LinkedIn, n.d.).
Conclusion
ESR programs accelerate spine surgery recovery and make it safer. With education, nutrition, movement, and team support, they reduce opioids, shorten stays, and lower readmissions. At El Paso Back Clinic® in El Paso, TX, we add chiropractic care and NP guidance for full support. New VR tech adds exciting ways to build strength. If facing spine surgery, ask about ESR and our integrative options. Contact us at 915-850-0900 for help.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine