Neck aches, soreness, and pain symptoms are not always neck-related. Tight thoracic or mid-back muscles can pull on the neck muscles causing various symptoms. Upper back tightness occurs anywhere from the neck’s base to the bottom of the rib cage. The bones in the upper area don’t move or flex as much as the neck and low back. This can lead individuals to believe there is nothing wrong with the mid-back, as there are no pain symptoms or signs of discomfort. However, individuals don’t realize how tight the muscles are, which can go on for years, causing neck issues. Injury Medical Chiropractic and Functional Medicine Clinic can relieve symptoms, release, and relax tight muscles, increase circulation, and restore optimal function.
Mid-Back Muscle Tightness
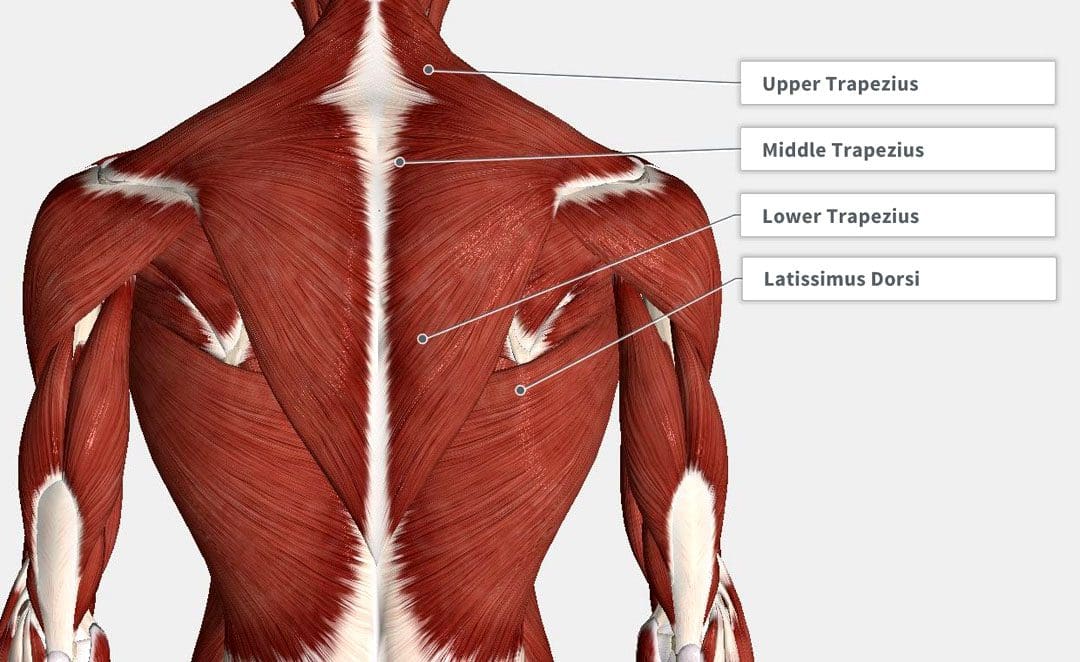
The upper and middle back is the thoracic spine. The thoracic spine has twelve small bones called vertebrae. Each vertebra on the thoracic spine is connected to a pair of ribs. The ribs wrap around the body and attach to a long, flat sternum bone. This forms the rib cage. The bones in the upper back work with the ribs to stabilize the back and protect vital organs, including the heart and lungs. The tightening and pulling eventually cause neck aches that can come out of nowhere; even when not moving and looking straight ahead, there can be persistent dull achiness or stinging sensations.
Causes
Unhealthy posture, disc problems, injuries, fractures, or other issues or conditions can cause mid-back muscle tightness.
Posture
Constant sitting or standing combined with unhealthy posture and being hunched over can cause the muscles to tighten, limiting mobility.
Holding Onto Stress
Chronic stress can cause muscle tightening, whether it is in the low back, mid-back, neck, or elsewhere.
Hereditary
Individual genetic makeup may make the body more susceptible to muscle tightness.
For example, individuals with a lot of muscle tone vs. individuals with less muscle tone may experience muscle tightness more often.
Adequate Hydration
Being properly hydrated is important for muscle and joint lubrication.
Water provides nutrients to contracting muscles.
This keeps the body loose and ready for movement.
Muscle Imbalance and Underlying Weakness
Individuals that tend to work one side of the body more than the other or have repeatedly been moving in a certain way for years can cause muscle imbalances and trigger points to develop.
If muscle tightness continues, even after stretching, it could be an underlying weakness.
The muscles can sometimes seize up and guard, so they feel tight when they have become chronically weak and not strong enough to meet the physical demands.
Chiropractic Care
Chiropractic care involves various therapies to address the root cause fully and relieve neck aches. These include:
Massage therapies to break up compacted muscle tissue.
Remove trigger points.
Relax the muscles to a pliable state.
Perform chiropractic adjustments to realign the spine.
Stretching and strengthening.
Posture training that includes stretches/exercises.
Nutritional plans to help strengthen muscles.
Thoracic Tension Release
References
Gatt, Adrianna, et al. “Anatomy, Fascia Layers.” StatPearls, StatPearls Publishing, Jul 25, 2022.
Liebsch, Christian, and Hans-Joachim Wilke. “How Does the Rib Cage Affect the Biomechanical Properties of the Thoracic Spine? A Systematic Literature Review.” Frontiers in bioengineering and biotechnology vol. 10 904539. Jun 15, 2022, doi:10.3389/fbioe.2022.904539
Maciejewska-Skrendo, Agnieszka et al. “Genetics of Muscle Stiffness, Muscle Elasticity and Explosive Strength.” Journal of human kinetics vol. 74 143-159. 31 Aug. 2020, doi:10.2478/hukin-2020-0027
Modes RJ, Lafci Fahrioglu S. Anatomy, Back. [Updated 2022 Feb 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539746/
Page, Phil. “Current concepts in muscle stretching for exercise and rehabilitation.” International journal of sports physical therapy vol. 7,1 (2012): 109-19.
Petrofsky, Jerrold et al. “The Efficacy of Sustained Heat Treatment on Delayed-Onset Muscle Soreness.” Clinical journal of sports medicine: official journal of the Canadian Academy of Sports Medicine vol. 27,4 (2017): 329-337. doi:10.1097/JSM.0000000000000375
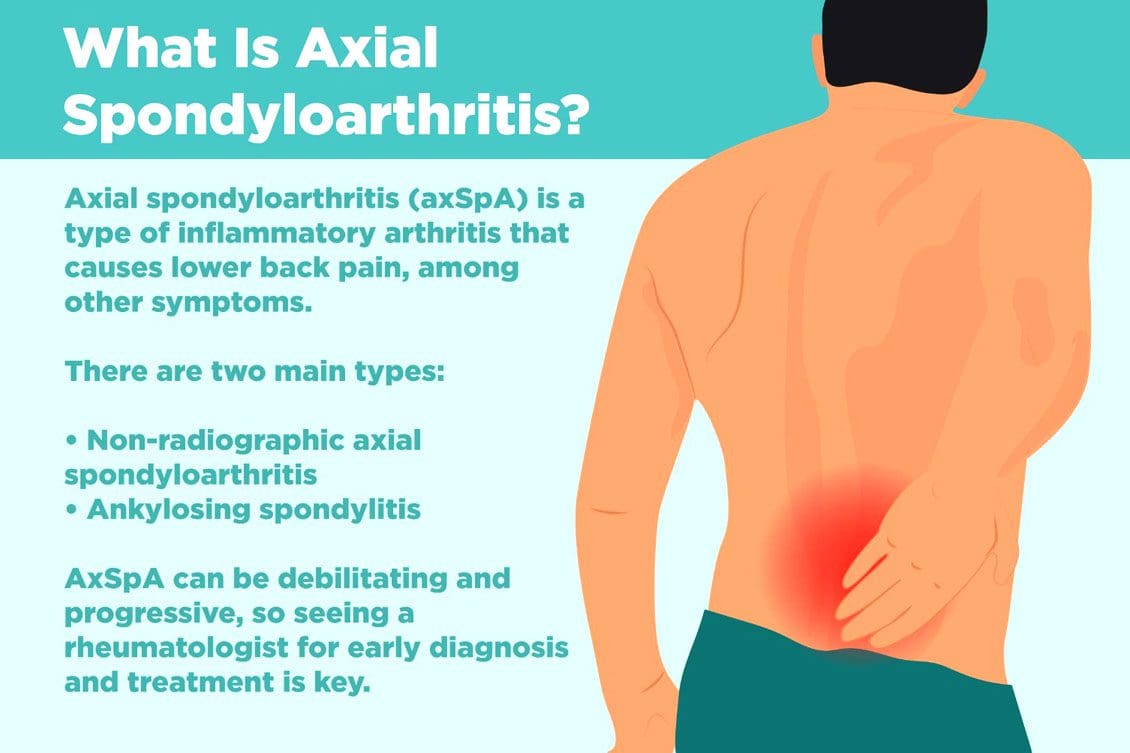
Non-radiographic axial spondyloarthritis or nr-axSpA and non-radiographic ankylosing spondylitis/AS are related. However, non-radiographic axial spondyloarthritis can present AS symptoms with active inflammation of the spine and sacroiliac/SI joints, causing back and hip pain but does not reveal joint damage on X-rays or MRIs. Injury Medical Chiropractic and Functional Medicine Clinic can explain what it means to have non-radiographic axial spondyloarthritis, how it can be managed, and what to do to prevent it from turning into ankylosing spondylitis.
Non-Radiographic Axial Spondyloarthritis
Non-radiographic axial spondyloarthritis means there are early AS symptoms but have not developed enough joint inflammation or damage to show up on an X-ray or other form of imaging. Early evidence of joint inflammation includes blurring of the joint edges and localized regions of joint erosion. It can be difficult for physicians to see these subtle changes on an x-ray.
Ankylosing Spondylitis
Ankylosing spondylitis, or AS, is a form of inflammatory arthritis that affects joints in the spine and elsewhere.
It is a chronic, inflammatory, autoimmune disease.
Medical research is still ongoing to determine the exact cause, but a genetic component is believed to be contributing factor.
Around 85% of individuals with ankylosing spondylitis have inherited the HLA-B27 gene, which is associated with multiple autoimmune conditions.
In the early stages, individuals will present lower back pain around the sacroiliac joints or the joints that connect the spine to the pelvis.
Later stages have more obvious X-ray findings, like the fusing of the sacroiliac joints and the lower spine that takes place over time.
Joint inflammation can progress, causing permanent joint damage and spine rigidity.
Most individuals with the condition can manage their symptoms with NSAIDs, chiropractic care, physical and massage therapy, and range of motion exercises.
Stage 1
There is no evidence of spinal inflammation on x-rays.
MRI provides more detailed images of bones and may reveal bone marrow edema or accumulation of fluid in the structures of the spinal bones and joints.
Individuals with non-radiographic axial spondyloarthritis, you are here.
Stage 2
There is visible inflammation of the spinal joints on the x-ray.
The sacroiliac joints between the spine and the pelvis are the most affected.
Stage 3
Chronic inflammation of the joints has caused bone loss and permanent joint damage, resulting in spine rigidity.
Symptoms of Non-Radiographic Axial Spondyloarthritis
There are differences between back pain associated with muscle strain and arthritis. Back pain symptoms include:
Starts to present before age 40.
It has a gradual onset and can go unnoticed for years.
Improves with movement or activity.
Eases up throughout the day.
Starts up in the evening when resting.
Other symptoms include:
Joint stiffness
Swollen fingers
Heel pain
Bilateral buttock discomfort and pain
Slowing Progression
Progression from non-radiographic axial spondyloarthritis to ankylosing spondylitis occurs in 10% – 20% of individuals over a two-year period. Progression factors include genetics, gender, degree of joint damage, and level of inflammatory markers at the time of diagnosis.
Early diagnosis and treatment can slow the progression before significant joint damage with anti-inflammatory therapy, rheumatological therapy, and targeted exercise.
Work with a specialist like an orthopedic spine specialist and rheumatologist that understands the disorder and is up to date on the most recent treatment modalities.
Individuals with non-radiographic axial spondyloarthritis should expect to have serial X-rays to gauge the progression of the disease.
Staying healthy and active is recommended to slow the progression of nr-AxSpA and AS.
Recent medical advances and lifestyle adjustments can slow the progression in most cases.
axSpA
References
Six tips for living well with ankylosing spondylitis. Available at https://www.mayoclinic.org/diseases-conditions/ankylosing-spondylitis/in-depth/6-tips-for-living-well-with-ankylosing-spondylitis/art-20478753. Accessed 11/07/2022.
Ankylosing spondylitis. Mayo Clinic. Available at https://www.mayoclinic.org/diseases-conditions/ankylosing-spondylitis/symptoms-causes/syc-20354808. Accessed 11/05/2022.
D. J. Pradeep, A. Keat, K. Gaffney, Predicting outcome in ankylosing spondylitis, Rheumatology, Volume 47, Issue 7, July 2008, Pages 942–945, https://doi.org/10.1093/rheumatology/ken195
Kucybała, Iwona, et al. “Radiologic approach to axial spondyloarthritis: where are we now and where are we heading?.” Rheumatology international vol. 38,10 (2018): 1753-1762. doi:10.1007/s00296-018-4130-1
Michelena, Xabier, López-Medina, Clementina, and Helena Marzo-Ortega. “Non-radiographic versus radiographic axSpA: what’s in a name?”.” National Center for Biotechnology Information. October 14, 2020. https://doi.org/10.1093/rheumatology/keaa422
Swift D. Ankylosing spondylitis: disease progression varies widely. Medpage Today. Accessed 11/05/2022.Available at https://www.medpagetoday.com/rheumatology/arthritis/49096
Ankylosing spondylitis, or AS, is a type of inflammatory arthritis that usually impacts the spine, causing back stiffness and pain, pain in the hips, and decreased range of motion. Brain fog can also be a symptom of AS and other chronic inflammatory conditions. Brain fog can affect memory, concentration, decision-making, learning, and problem-solving. Injury Medical Chiropractic and Functional Medicine Clinic can educate on the causes of ankylosing spondylitis brain fog and how to reduce its effects.
Brain Fog
Experts do not fully understand how conditions like AS cause brain fog and how it affects the brain and central nervous system. However, they believe brain fog is linked to chronic inflammation and pain associated with the condition, along with certain factors.
Chronic Inflammation
Inflammation occurs when the body’s immune system attacks healthy cells.
This triggers the release of inflammation-causing cytokines.
Cytokines can interfere with normal brain function.
Ankylosing Spondylitis Chronic Pain
Chronic pain can cause fatigue and unhealthy sleep quality.
Fatigue and poor sleep can worsen chronic pain, leading to intense fatigue and extreme sleep issues, becoming a vicious cycle.
Corticosteroids
Doctors typically treat ankylosing spondylitis with corticosteroids.
Individuals with cardiovascular risk factors have an increased risk of brain fog from the medications.
Depression
Individuals with AS can present symptoms of depression, which has been linked to cognitive impairment.
Depression can contribute to the development of brain fog.
Cornelson, Stacey M et al. “Chiropractic Care in the Management of Inactive Ankylosing Spondylitis: A Case Series.” Journal of chiropractic medicine vol. 16,4 (2017): 300-307. doi:10.1016/j.jcm.2017.10.002
Creaky Joints. (September 17, 2018) “You can ease inflammatory arthritis brain fog with these 12 tips for a sharper mind.” https://creakyjoints.org/living-with-arthritis/arthritis-brain-fog/
Vitturi, Bruno Kusznir et al. “Cognitive Impairment in Patients with Ankylosing Spondylitis.” The Canadian journal of neurological sciences. Le journal canadien des sciences neurologiques vol. 47,2 (2020): 219-225. doi:10.1017/cjn.2020.14
Zhang, Jun-Ming, and Jianxiong An. “Cytokines, inflammation, and pain.” International anesthesiology clinics vol. 45,2 (2007): 27-37. doi:10.1097/AIA.0b013e318034194e
After a car accident, you may notice neck pain. It could be a slight soreness you think is nothing but take care of. More than likely, you have whiplash. And that little soreness can turn into a lifetime of chronic neck pain if only treated with pain meds and not treated at the source.
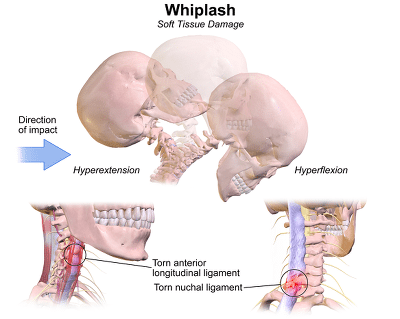
Whiplash trauma, aka neck sprain or neck strain, is an injury to the soft tissues around the neck.
Whiplash can be described as a sudden extension or backward movement of the neck and flexion or forward movement of the neck.
Severe whiplash can also include injury to the following:
Intervertebral joints
Discs
Ligaments
Cervical muscles
Nerve roots
Symptoms of Whiplash
Most people experience neck pain either immediately after the injury or several days later.
Other symptoms of whiplash trauma can include:
Neck stiffness
Injuries to the muscles and ligaments around the neck
Headache and dizziness
Symptoms & possible concussion
Difficulty swallowing and chewing
Hoarseness (possible injury to the esophagus and larynx)
The sensation of burning or prickling
Shoulder pain
Back pain
Diagnosis of Whiplash Trauma
Whiplash trauma usually causes damage to the soft tissues; a doctor will take x-rays of the cervical spine in case of delayed symptoms and rule out other problems or injuries.
Treatment
Fortunately, whiplash is treatable, and most symptoms resolve completely.
Most often, whiplash is treated with a soft cervical collar.
This collar may need to be worn for 2 to 3 weeks.
Other treatments for individuals with whiplash may include the following:
Heat treatment for relaxing muscle tension and pain
Pain meds such as analgesics and non-steroidal anti-inflammatory
Some people will tell you that whiplash is a made-up injury that people use to get more money in a settlement stemming from an accident. They do not believe it is possible in a low-speed rear-end accident and see it as a legitimate injury claim, mainly because there are no visible marks.
Some insurance experts claim that about a third of whiplash cases are fraudulent, leaving two-thirds of the cases legitimate. Much research also supports the claim that low-speed accidents can indeed cause whiplash, which is very real. Some patients suffer from pain and immobility for the rest of their lives.
NCBI Resources
Chiropractors will use different techniques to relieve the pain of whiplash and help with healing.
Chiropractic Adjustment The chiropractor performs spinal manipulation to move the joints into alignment gently. This will help to align the body to relieve pain and encourage healing.
Muscle Stimulation and Relaxation This involves stretching the affected muscles, relieving tension, and helping them relax. Finger pressure techniques may also be combined with trying to alleviate pain.
McKenzie Exercises These exercises help with disc derangement that whiplash causes. They are first performed in the chiropractor’s office, but the patient can be taught how to do them at home. This helps the patient have some degree of control over their healing.
Each whiplash case is different. A chiropractor will evaluate the patient and determine the appropriate treatment case-by-case basis. The chiropractor will determine the best course of treatment that will relieve your pain and restore your mobility and flexibility.
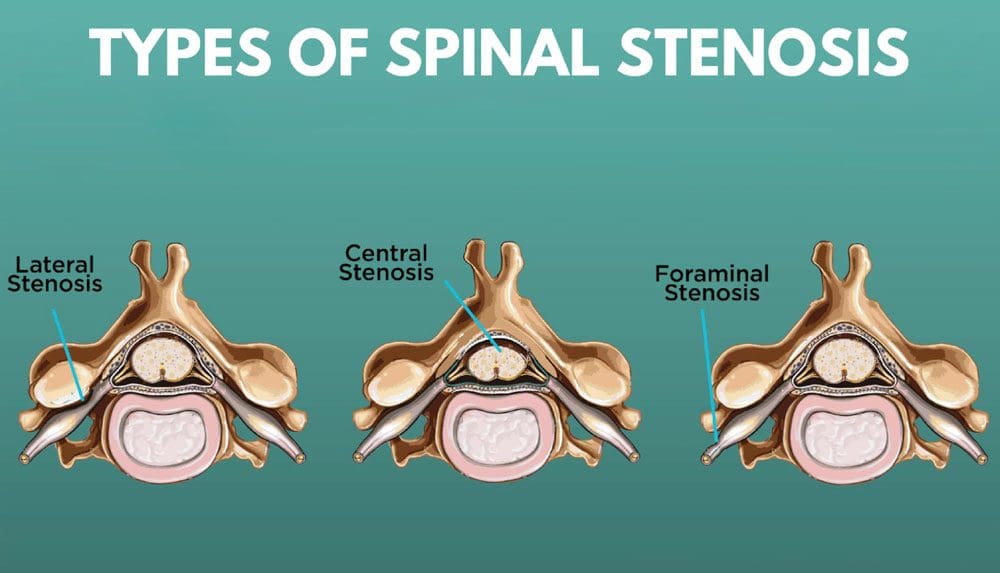
The spine is the body’s central highway, with the spinal canal as the main lane that handles all the traffic. There are entrances and exits, or spinal cavities, that allow the nerves to branch off the spinal cord and run throughout the body. A traffic jam develops during lane closures, accidents, or construction at an entrance or exit. Lateral recess stenosis causes the narrowing of the spine’s lateral recess/Lee’s entrance, which can compress nerves, impede nerve circulation, and cause painful symptoms.
Lateral Recess Stenosis
The spinal column provides a strong and flexible structure for the spinal cord. The nerves travel from the spinal cord through various openings and passageways to the rest of the body. One of the openings is known as the lateral recess. Stenosis means narrowing. When a lateral recess in a vertebra develops stenosis, the nerve in that area can get jammed/pinched with no room to move, causing varying symptoms and sensations.
Symptoms
Depending on where the stenosis is taking place (neck, middle or low back), common symptoms of lateral recess stenosis can include:
Back pain that can spread out to other areas.
Cramping that can spread out to other sites.
Radiating pain that worsens with movement and eases with rest.
Numbness or weakness of the legs or arms.
Electrical tingling sensations down the leg or arm.
Muscle groups around the stenosis area are built up to take the pressure off of the area, alleviating symptoms.
Medications
A doctor or spine specialist may recommend or prescribe medication to ease symptoms. These include:
Tylenol – acetaminophen.
NSAIDS – Advil/ibuprofen or Aleve/naproxen.
Muscle relaxers
Steroid Injections
According to a study, neurogenic claudication is the main reason for disability and loss of independence in the elderly.
Neurogenic claudication describes pain and weakness in the buttocks and legs during physical activity that originates from the nerves, not the vessels.
This can happen from inflammation and swelling around a compressed nerve.
A steroid injection can decrease inflammation for several months.
Surgery
If activity modification, NSAIDs, bracing, and physical therapy don’t work or provide adequate relief, a doctor or specialist could recommend surgery.
Fusion is reserved when there is instability combined with the condition.
Back Problems Chiropractor
References
American College of Rheumatology (n.d.) “Spinal Stenosis” https://www.rheumatology.org/I-Am-A/Patient-Caregiver/Diseases-Conditions/Spinal-Stenosis
Arthritis Foundation (n.d.) “Corticosteroids” https://www.arthritis.org/drug-guide/corticosteroids/corticosteroids
Drug Design, Development and Therapy (2014) “Steroid for epidural injection in spinal stenosis: a systematic review and meta-analysis” https://doi.org/10.2147/DDDT.S78070
Lee, Seung Yeop, et al. “Lumbar Stenosis: A Recent Update by Review of Literature.” Asian spine journal vol. 9,5 (2015): 818-28. doi:10.4184/asj.2015.9.5.818
Liu, Kuan, et al. “Steroid for epidural injection in spinal stenosis: a systematic review and meta-analysis.” Drug design, development, and therapy vol. 9 707-16. Jan 30, 2015, doi:10.2147/DDDT.S78070
Medline Plus (n.d.) “Achondroplasia” https://medlineplus.gov/genetics/condition/achondroplasia/
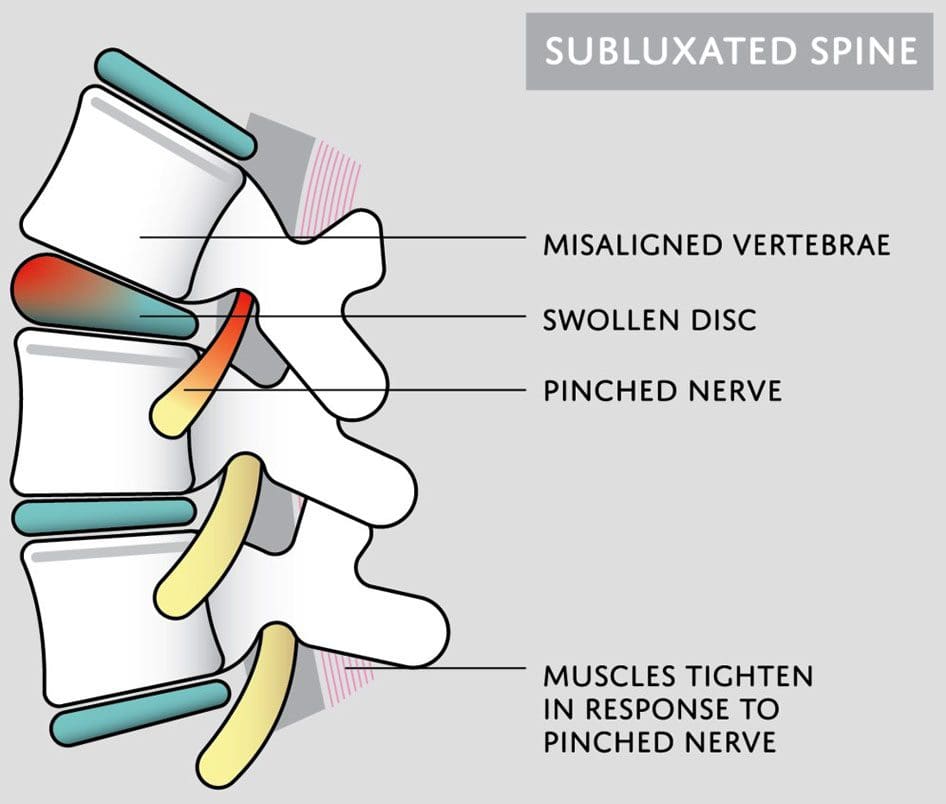
Subluxation is when a joint shifts out of alignment, which can happen to any joint in the body. Spinal subluxation indicates a misalignment of one or more portions of the spinal vertebrae. It is common in the spine from all the reaching, bending, twisting, and flexing the body goes through. Spinal subluxations, if left untreated, can cause disc degeneration, permanent nerve damage, neurological conditions, and chronic pain symptoms. A subluxation chiropractor will realign and decompress the spine combined with massage therapy to relax the muscles and restore mobility and function.
Subluxation Chiropractor
Some subluxations don’t cause any problems or pain, but that doesn’t mean they aren’t affecting the back and body. A spinal subluxation can cause long-term problems by:
Research shows that spinal subluxations can affect many facets of the body. Long-term effects may include:
Sleep problems
Low energy
Brain fog
Mood swings
Anxiety and depression
Digestive issues
Respiratory problems
Bone spurs
Spinal arthritis
Chiropractic Care
When the spine is out of alignment, it can cause issues throughout the body. Changes in one area affect the rest of the body. A subluxation chiropractor looks at the spine’s neurological and mechanical components and aims to reset everything back into its proper position. Similar to the way a massage helps the mind and body relax and de-stress, a spinal adjustment helps by:
Increasing circulation
Relieving discomfort and pain
Releasing tension
Improving mood
Reducing stress levels
Improving sleep function
Increasing energy levels
When the spine is properly aligned, the body can operate at its full potential.
Adrenal Dysfunction
References
Brian S. Budgell, Reflex effects of subluxation: the autonomic nervous system, Journal of Manipulative and Physiological Therapeutics, Volume 23, Issue 2,
2000, Pages 104-106, ISSN 0161-4754, https://doi.org/10.1016/S0161-4754(00)90076-9. (https://www.sciencedirect.com/science/article/pii/S0161475400900769)
Green, J D et al. “Anterior subluxation of the cervical spine: hyperflexion sprain.” AJNR. American journal of neuroradiology vol. 2,3 (1981): 243-50.
Meyer, S. “Thoracic spine trauma.” Seminars in roentgenology vol. 27,4 (1992): 254-61. doi:10.1016/0037-198x(92)90004-l
Neva MH, Häkkinen A, Mäkinen H, et al. High prevalence of asymptomatic cervical spine subluxation in patients with rheumatoid arthritis waiting for orthopedic surgeryAnnals of the Rheumatic Diseases 2006;65:884-888.
Nourollahi, Maryam, et al. “Awkward trunk postures and their relationship with low back pain in hospital nurses.” Work (Reading, Mass.) vol. 59,3 (2018): 317-323. doi:10.3233/WOR-182683
Vernon, Howard. “Historical overview and update on subluxation theories().” Journal of chiropractic humanities vol. 17,1 (2010): 22-32. doi:10.1016/j.echu.2010.07.001
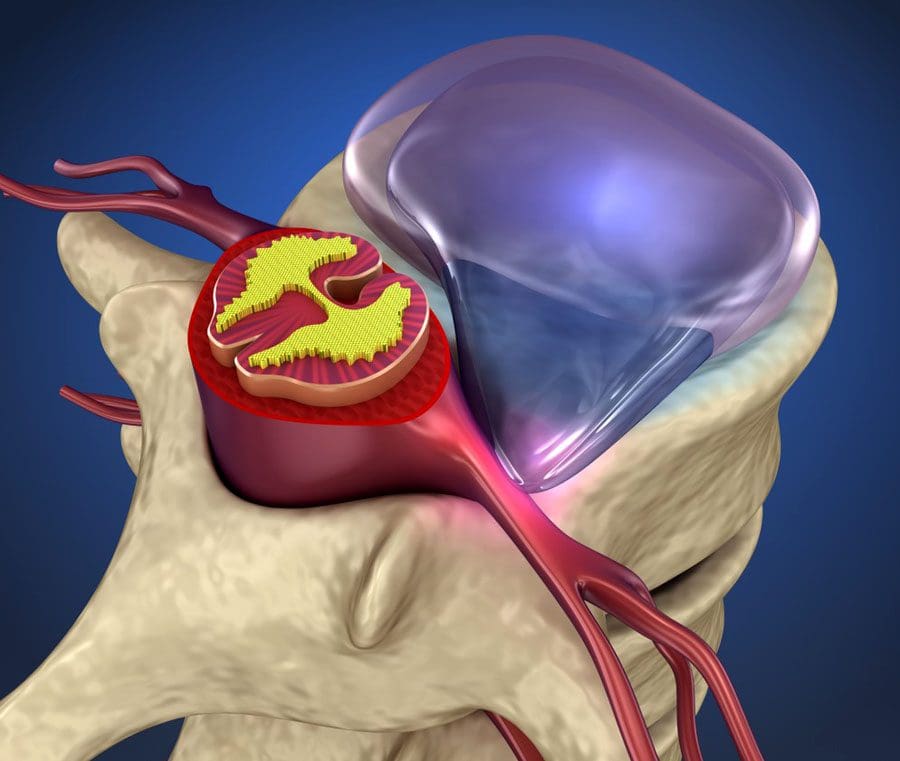
Herniated disc injuries and the time it takes to heal depend on the injury’s cause, the severity, and where it occurred along the spine. Symptoms can last a few days to months. Chiropractic treatment, massage therapy, and decompression realign the spine and return the disc to its correct position. Still, the herniated disc signs it is returning to normal can take time as the rest of the spine and body adjust to the realignment.
Herniated Disc Signs It Is Returning To Normal
Most cases take a few weeks with healing time depending on health conditions, physical activity level, and age. However, in severe cases, a herniated disc can take up to several months to fully heal, but discomfort symptoms usually resolve sooner.
Expectations From a Healing Disc
Resting the spine and taking it easy after the injury is recommended.
Too much rest is not recommended as it can cause muscle stiffness.
While the herniated disc is healing, a primary doctor may prescribe anti-inflammatories or muscle relaxants to help ease discomfort.
A chiropractor and/or physical therapist can teach exercises and stretches to relieve pressure on nerves, loosen tight muscles, and improve circulation.
Signs The Herniated Disc Is Healing
Most herniated discs cause significant pain in the back and neck from the nervous system, causing some of the muscles of the low back or neck to spasm to protect the area from further damage.
Usually, the muscle spasms relax within the first days of the injury.
After spinal decompression, neurological symptoms like the sharp, shooting pain down a nerve in the arm or leg are the first symptoms to go away.
Then muscle weakness along the path of the nerve goes away.
Numbness in the extremities can linger around longer.
Length of Time
The wear and tear of adult spinal discs, combined with unhealthy posture habits, job occupation, previous injuries, etc., decrease blood circulation.
This is why it can take some time to heal completely, as the entire blood supply needs to reset to optimal circulation.
Nerve compression causing aches and pain sensations down the nerves can also take time.
Regular Activity
Returning to regular activities depends on the individual’s case and condition. It is essential not to overdo things that can cause excessive loading of the spine before the disc has fully healed, which increases the risk of re-herniation and other injuries.
Inactivity can slow the healing process and cause inflammation.
Patients are encouraged to return to activities that generate gentle motion to stimulate the stabilizing muscles to function properly and increase blood circulation to the injured area.
Individuals are recommended to:
Learn posture improvement when walking, sitting, standing, and sleeping.
Adjust sleep patterns.
Incorporate anti-inflammatory nutrition during the healing process.
This provides a mechanical and biological environment that eventually becomes a personalized exercise physical therapy program.
DOC Spinal Decompression
References
Díez Ulloa, Máximo Alberto. “Role of Microangiogenensis in Disc Herniation Healing.” Journal of investigative surgery: the official journal of the Academy of Surgical Research vol. 34,6 (2021): 685. doi:10.1080/08941939.2019.1682725
Factors that influence recovery: Mayo Clinic. February 8, 2022. “Herniated disk.” https://www.mayoclinic.org/diseases-conditions/herniated-disk/symptoms-causes/syc-20354095
Factors that influence recovery: NHS. March 22, 2021. “Slipped Disc.” https://www.nhs.uk/conditions/slipped-disc/
How to speed up healing time: American Academy of Orthopaedic Surgeons. January 2022. “Herniated Disk in the Lower Back” https://orthoinfo.aaos.org/en/diseases–conditions/herniated-disk-in-the-lower-back/
Keramat, Keramat Ullah, and Aisling Gaughran. “Safe physiotherapy interventions in large cervical disc herniations.” BMJ case reports vol. 2012 bcr2012006864. 18 Aug. 2012, doi:10.1136/bcr-2012-006864
Stoll, T et al. “Physiotherapie bei lumbaler Diskushernie” [Physiotherapy in lumbar disc herniation ]. Therapeutische Umschau. Revue therapeutique vol. 58,8 (2001): 487-92. doi:10.1024/0040-5930.58.8.487
Swartz, Karin R, and Gregory R Trost. “Recurrent lumbar disc herniation.” Neurosurgical focus vol. 15,3 E10. 15 Sep. 2003, doi:10.3171/foc.2003.15.3.10
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine



 Brain Fog
Brain Fog