Can individuals utilize chiropractic care to reduce sciatica pain and help restore mobility to their lower back and legs?
Introduction
Many individuals are always on the move and utilize the lower half of the body to go from one location to another. From the lower back to the feet, many individuals do repetitive movement that causes the lower back muscles to be constantly stretched. This, in turn, can lead to overlapping risk profiles that can affect the lower back and a long nerve connected to the lower back, known as the sciatic nerve. When numerous issues affect the sciatic nerve, many individuals experience pain and discomfort over time, which can develop into something chronic without treatment. Luckily, when individuals begin to think about their health and wellness, it reduces the chances of pain and discomfort from returning. Today’s article looks at the causes of sciatica and how non-surgical treatments like chiropractic care can help relieve sciatica pain and restore mobility to the lower back and legs. We discuss with certified medical providers who inform our patients how sciatica pain correlates with the lower back. While asking informed questions to our associated medical providers, we advise patients to incorporate non-surgical treatments like chiropractic care to reduce sciatica pain and help realign the body. Dr. Alex Jimenez, D.C., encompasses this information as an academic service. Disclaimer.
What Causes Sciatica?
Do you feel numbness or tingling sensations in your legs, making walking unbearable? Do you experience pain or discomfort in your lower back after lifting a heavy object? Or how long have you stretched your body after sitting down or standing excessively at work? Many of these scenarios are often correlated with low back pain. However, low back pain is always connected with sciatica and can impact the body. While the sciatic nerve plays a huge role in direct motor function to the hamstrings and lower extremities, sciatica is when environmental factors impact or compress the sciatic nerve, causing pain-like symptoms to the lower extremities. (Davis et al., 2024) Since the sciatic nerve is large and travels down to the feet, it allows mobility to the lower extremities. When many individuals experience low back pain, they will also experience sciatica.
Sciatica also means that pain will always be transmitted along the sciatic nerve root, leading to various impairments and socioeconomic consequences and affecting a person’s quality of life. (Siddiq et al., 2020) Many of the causes of sciatica pain can vary as they are all correlated with low back pain. Some of the various environmental factors that can cause sciatica include:
Physical inactivity
Excessive sitting or standing
Poor posture
Musculoskeletal conditions
Another environmental factor that leads to the development of sciatica is disc degeneration. This can cause the nerves to be irritated due to herniation and cause asymptomatic overlapping risk profiles (Zhou et al., 2021). When people are dealing with the overlapping risk profiles of sciatica, many often seek treatment to reduce the pain and restore mobility to the lower extremities.
Sciatica: Causes, Symptoms, & Tips- Video
How Chiropractic Care Reduces Sciatica
Since sciatica is commonly experienced as a frequent symptom cause of low back and leg pain, the symptoms can range from a mild tingling sensation to a burning sensation, and treatment is needed. Many individuals will seek out non-surgical treatments to reduce the pain caused by sciatica. Non-surgical treatments are non-invasive, affordable, and customizable to the individual. One of the non-surgical treatments is chiropractic care, which can help many individuals dealing with sciatica. A chiropractor can diagnose a person’s sciatica and assess the root cause of the symptoms to provide the most appropriate form of treatment. The main goal for chiropractic care is to restore the natural mobility of the spine and provide progressive relief from pain and stiffness in the lower extremities while improving a person’s daily living. (Kruse et al., 2019)
Chiropractic Care Restores Lower Back & Leg Mobility
Chiropractors utilize manual and mechanical spinal manipulation to increase lumbar spinal mobility and flexibility and improve the legs biomechanically. (Siciliano et al., 2024) Chiropractic treatments can also use various methods like neural mobilization intervention to decrease the pain and restore nerve function in the lower extremities and lower back. (Peacock et al., 2023) This allows individuals to have a reduced disability from sciatica associated with low back pain, and it is possible to prevent sciatica from occurring in the future. As many people begin to become more mindful of what is causing their sciatica, they can find effective ways to improve their spine’s well-being and prevent sciatica symptoms from affecting the lower extremities.
Kruse, R. A., White, B. A., & Gudavalli, S. (2019). Management of Lumbar Radiculopathy Associated With an Extruded L4-L5 Spondylolytic Spondylolisthesis Using Flexion-Distraction Manipulation: A Case Study. J Chiropr Med, 18(4), 311-316. https://doi.org/10.1016/j.jcm.2019.02.001
Peacock, M., Douglas, S., & Nair, P. (2023). Neural mobilization in low back and radicular pain: a systematic review. J Man Manip Ther, 31(1), 4-12. https://doi.org/10.1080/10669817.2022.2065599
Siciliano, T. B., Gudavalli, M. R., & Kruse, R. (2024). Spinal manipulation and mobilization forces delivered treating sciatica: a case report. Front Integr Neurosci, 18, 1356564. https://doi.org/10.3389/fnint.2024.1356564
Siddiq, M. A. B., Clegg, D., Hasan, S. A., & Rasker, J. J. (2020). Extra-spinal sciatica and sciatica mimics: a scoping review. Korean J Pain, 33(4), 305-317. https://doi.org/10.3344/kjp.2020.33.4.305
Zhou, J., Mi, J., Peng, Y., Han, H., & Liu, Z. (2021). Causal Associations of Obesity With the Intervertebral Degeneration, Low Back Pain, and Sciatica: A Two-Sample Mendelian Randomization Study. Front Endocrinol (Lausanne), 12, 740200. https://doi.org/10.3389/fendo.2021.740200
It can be challenging for individuals trying to keep their homes clean with chronic back pain. Can learning and proper body mechanics help manage household responsibilities without aggravating pain symptoms?
Household Chores
Household-related back problems usually occur because we don’t take the time to consider how to move and perform the tasks from a musculoskeletal perspective to avoid and prevent injuries. Most ergonomic tips for household chores revolve around the same ideas for athletes and fitness enthusiasts: maintain a neutral spine, avoid twisting when possible, strengthen the body’s core, take regular breaks, stretch, and don’t overdo it. A healthy body mechanics system works for those who garden as well. Using strategies like cleaning a little here and there instead of taking an entire day whenever possible and organizing tools ahead of time along with training oneself how to perform them in a way that the spine, back muscles, and the entire body are protected from injury, pain, sciatica, or re-injury. However, implementing proper body mechanics requires a willingness to become aware of how each task is performed and to retrain the body where necessary to a healthier method/technique and a happier household.
Vacuuming
Vacuuming is one of those chores that can quickly lead to a habitual bent-over posture. This is not recommended for the spine’s health; slouching, whether from a position held for a sustained period of time or an activity that requires repetition, can lead to problems with the intervertebral discs and pain symptoms. (Nazari J., Pope M. H., and Graveling R. A. 2012) Another posture that individuals tend to engage in is vacuuming with an overly straight back. Like slouching, keeping the spine rigidly over-extended while vacuuming can irritate the spine and cause muscle spasms. It can also increase the normal low back curve, which, in turn, may lead to extra tightness and a painful back.
Vacuuming with healthy body mechanics includes employing a minimal lunge that stays in a pain-free position that does not extend beyond the comfortable position. Individuals should place one foot in front of the other for a short distance. The stance is similar to the way fencers position themselves. This allows a shift forward and back during the vacuuming process instead of bending or rounding over at the spine. For those with sacroiliac joint issues, the forward placement of one leg may be more comfortable than the forward placement of the other. Try out and use the side that feels comfortable, and stick with that. Do not work in pain or through the pain. Switching legs and/or arms can help avoid muscle fatigue or injury triggers. Place the non-vacuuming hand on the thigh in front to help take the weight and pressure off the back. Maintain the pelvis in a level position when working. Another strategy for those who can get up and down from the floor without trouble is to vacuum while kneeling on one knee. This brings the body’s center of mass closer to the floor, reducing the degree to which the body has to deal with the force of gravity. Kneeling while vacuuming may also help prevent rounding over at the spine.
Dusting
When dusting, reduce the load off the back by propping the inactive arm on the item or area being cleaned. Alternatively, prop the arm on the thigh.
Laundry
In a large household, it is very easy to overdo laundry and trying to finish up as much as possible can lead to pain symptoms and injuries. If possible, break up the loads that have to be lifted or carried into smaller bundles that weigh less. This can mean more loads, but the strategy protects the back and spine. Avoid extremes in the spinal position; don’t round over at the spine or keep it rigid and over-extended. Lift with the legs and protect the discs. Adjustments that can be made to the basic lift with the leg and not the back strategy include putting the laundry basket on a table or chair that is preferably the same height as the washer or dryer. This will minimize bending. To relieve pressure on the back, use one hand to load the washer, dryer, or laundry basket while using one of the appliances to prop the other hand.
Dishes
During dishwashing, use a small step stool or box to help prevent injury and/or relieve pain. Place it in the cabinet under the sink and rest one foot on it. This strategy can work well for those with sacroiliac joint problems, especially if the foot on the pain-free side is the one placed on the box or stool. Ensuring foot placement reduces pain and discomfort and does not cause pain. Using a box or stool can also help with core stability. Core stability is one of the best ways, in general, to prevent injury and keep low back pain away. (Coulombe B. J., Games K. E., Neil E. R., and Eberman L. E. 2017) As the box is directly under the sink, the body has to firmly position itself against the counter, providing stability during the task. The box or stool will contract the pelvic and hip muscles and strengthen the core.
Sweeping
Many sweep, mop, and rake with their spines, which can be counterproductive to health, as twisting and bending simultaneously is a known risk factor for a herniated disc. (Shimia, M. et al., 2013) Use the arms and legs instead of overly involving the back during sweeping and raking. The idea is to reach and pull the broom or sweeper with the arms rather than twisting around to reach all the areas working with one leg in front of the other. When needing to change directions, pivot on the back leg, keeping the trunk relaxed, equivalent to a tai chi movement. Or, turn the whole body in different directions by taking small steps. Taking small steps or pivoting on the back leg to change the direction of the trunk and arms protects from overuse and extensive wear and tear.
Adjustments for a new method of household sweeping and raking include:
Sweeping or raking about 1 to 2 feet in front to avoid overreaching and strain.
Maintaining the spine in one long, flexible, but unbroken line.
The head, shoulders, rib cage, pelvis, knees, and feet should always face the same direction and be vertically balanced relative to one another.
This will mean changing directions by pivoting the back leg or moving the whole body around, taking small steps.
Consider using an ergonomically designed broom, sweeper, mop, rake, and other household tools. This will be a bend in the handle or stem to help avoid bending.
Injury Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop personalized treatment programs. We focus on what works for you and use an integrated approach to treating injuries and chronic pain syndromes to improve flexibility, mobility, and agility, relieve pain, and help individuals return to normal activities. Our providers use Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles. Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers if other treatments are needed.
Heel Spurs
References
Nazari, J., Pope, M. H., & Graveling, R. A. (2012). Reality about migration of the nucleus pulposus within the intervertebral disc with changing postures. Clinical biomechanics (Bristol, Avon), 27(3), 213–217. https://doi.org/10.1016/j.clinbiomech.2011.09.011
Coulombe, B. J., Games, K. E., Neil, E. R., & Eberman, L. E. (2017). Core Stability Exercise Versus General Exercise for Chronic Low Back Pain. Journal of athletic training, 52(1), 71–72. https://doi.org/10.4085/1062-6050-51.11.16
Shimia, M., Babaei-Ghazani, A., Sadat, B. E., Habibi, B., & Habibzadeh, A. (2013). Risk factors of recurrent lumbar disk herniation. Asian journal of neurosurgery, 8(2), 93–96. https://doi.org/10.4103/1793-5482.116384
For individuals experiencing piriformis syndrome. Can knowing the causes and what it feels like help in diagnosis and treatment?
Managing Piriformis Syndrome
Piriformis syndrome is where spasms occur in the piriformis muscle located in the buttocks. These muscle spasms can cause pain and numbness in the buttocks and the back of the leg. (Cedars Sinai, 2022)
What Is It?
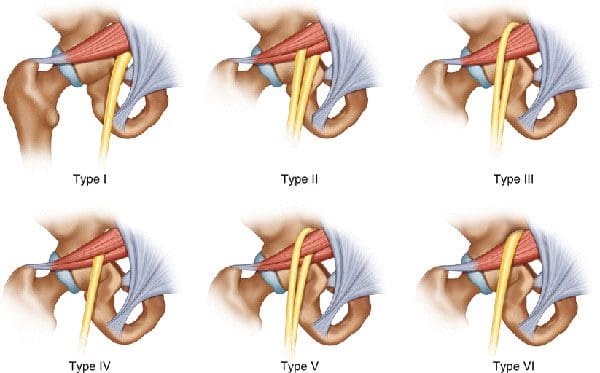
Piriformis syndrome is an irritation of the sciatic nerve from the piriformis muscle. Although the piriformis muscle is small compared to other muscles around the hip and thigh, it supports the hip joint’s external rotation or turning out. The sciatic nerve supplies the lower extremities with motor and sensory functions. The piriformis tendon and sciatic nerve cross each other behind the hip joint in the deep buttock. Both are about one centimeter in diameter. The piriformis muscle spasms can irritate the sciatic nerve, causing sciatica symptoms. (Cedars Sinai, 2022)
Triggers
A piriformis syndrome diagnosis means the piriformis tendon binds or spasms around the sciatic nerve, causing irritation and symptoms. Many doctors and specialists support the theory that when the piriformis muscle and its tendon tighten, this can cause compression and pinch the nerve. This can decrease blood circulation and irritate the nerve due to pressure. (Cass S. P. 2015) Many doctors also believe that piriformis syndrome occurs from anatomic variation of the muscle and tendon. It is thought this muscle-tendon variation irritates the nerve in some, leading to sciatica symptoms.
How It Feels
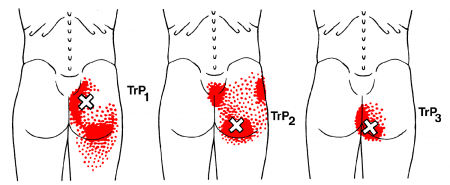
Common signs and symptoms experienced include (Cass S. P. 2015)
Pain in the buttocks.
Pain behind the hip.
Electric shock pains traveling down the back of the lower extremity.
Numbness in the lower extremity.
Tenderness with pressure that often causes pain when sitting.
Some develop symptoms abruptly, while others gradually increase in symptoms in the back of their thighs.
Most who are diagnosed with piriformis syndrome are generally active individuals who experience increasing difficulty with certain types of physical activity.
Testing
There are no specific tests that accurately diagnose piriformis syndrome. Doctors will order tests, including MRI and nerve conduction studies. Because it can be difficult to diagnose, there are likely many misdiagnosis cases. This means that some with the condition don’t have a piriformis diagnosis. In addition, some with vague hip pain may receive this diagnosis even if they don’t have the condition. (Cass S. P. 2015) An injection is often administered into the piriformis muscle when the diagnosis is uncertain. (Jankovic D. et al., 2013) Performing an injection can help determine the specific location of the discomfort. When an injection is given into the piriformis muscle or tendon, it is administered by ultrasound guidance to ensure the needle delivers medication to the correct location. (Bardowski E. A., and Byrd J. W. T. 2019)
Differential Diagnosis
Some other conditions with buttock pain can have similar symptoms. Other causes can include:
Radiculopathy/Sciatica
Herniated discs
Hip bursitis
Spinal stenosis
The diagnosis of piriformis syndrome is given when these diagnoses are eliminated as possible causes of pain.
Treatment
Managing piriformis syndrome is quite general, and it is often difficult to recover from. Common treatment and management suggestions include the following. (Jankovic D. et al., 2013)
Rest
Avoiding activities that cause symptoms for at least a few weeks.
Physical Therapy
Focuses on stretching and strengthening the hip rotator muscles.
Anti-inflammatory Medication
To decrease inflammation around the tendon.
Deep Massage
Used to relax the piriformis muscle and help release the compressed nerve.
Cortisone Injections
It can help decrease inflammation and swelling.
Botulinum Toxin Injection
It can paralyze the piriformis muscle to reduce pain and discomfort.
In severe cases, surgery can be performed to loosen the piriformis tendon, known as a piriformis release (Cass S. P. 2015). This surgical procedure is recommended when conservative treatments have been tried for at least six months and other causes of pain have been evaluated and ruled out. Recovery takes several months.
The goal of managing piriformis syndrome is to improve the range of motion and flexibility around the hip and diminish inflammation around the sciatic nerve. Working with a professional chiropractic team can help relieve pain, return individuals to normal function, and expedite healing. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a customized treatment program through an integrated approach to treating injuries and chronic pain syndromes, improving flexibility, mobility, and agility. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Piriformis Syndrome Treatment Chiropractor
References
Cedars Sinai. Sinai, C. (2022). Piriformis syndrome. https://www.cedars-sinai.org/health-library/diseases-and-conditions/p/piriformis-syndrome.html
Cass S. P. (2015). Piriformis syndrome: a cause of nondiscogenic sciatica. Current sports medicine reports, 14(1), 41–44. https://doi.org/10.1249/JSR.0000000000000110
Jankovic, D., Peng, P., & van Zundert, A. (2013). Brief review: piriformis syndrome: etiology, diagnosis, and management. Canadian journal of anaesthesia = Journal canadien d’anesthesie, 60(10), 1003–1012. https://doi.org/10.1007/s12630-013-0009-5
Bardowski, E. A., & Byrd, J. W. T. (2019). Piriformis Injection: An Ultrasound-Guided Technique. Arthroscopy techniques, 8(12), e1457–e1461. https://doi.org/10.1016/j.eats.2019.07.033
Individuals dealing with pain in the buttocks can make life difficult to sit, walk, or perform simple, everyday tasks. Can understanding the anatomy, location, and function of the gluteus maximus muscle help in muscle rehabilitation and avoid potential injuries?
Gluteus Maximus
The gluteus maximus is the largest human body muscle responsible for hip extension, external rotation, adduction, and abduction, as well as the ability to stand upright. The primary muscle extends laterally and keeps the body upright by supporting the bony pelvis and trunk. (Neto W. K. et al., 2020) When the gluteus maximus is strained, injured, or weak, it can lead to pain and inflammation.
Common symptoms can include:
Stiffness in the buttock
Discomfort while sitting
Difficulty standing up from sitting
Difficulty bending over
Pain when walking, especially upstairs or on a hill
Pain in the lower back and/or tailbone
Anatomy and Structure
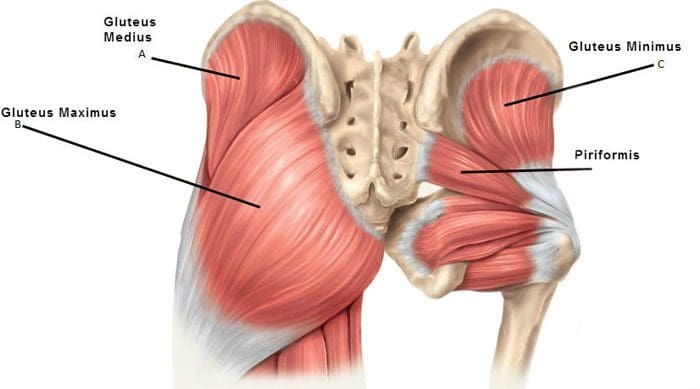
The muscles that comprise the glutes are the gluteus maximus, gluteus medius, and gluteus minimus. The gluteus medius runs underneath the gluteus maximus, and the gluteus minimus is underneath the gluteus medius.
The gluteus maximus is one of the strongest muscles. Fibers from the muscle connect to different body parts, including the femur/thighbone and the iliotibial band, which comprises connective tissue that runs up the thigh. The superior gluteal artery transports blood from the heart to the glutes.
Nerve Supply
The inferior gluteal nerve, part of the sacral plexus branch, innervates the maximus muscle. The sacral plexus nerves support motor and sensory function in the thighs, lower legs, feet, and pelvis. The sciatic nerve runs under the gluteus maximus, from the lower back down to the leg, and is often the cause of nerve pain in and around the area. (Carro L. P. et al., 2016) The main nerve of the perineum is the pudendal nerve, which runs under the gluteus maximus muscle.
Location
The gluteus maximus muscle defines the buttocks. It can be called a superficial muscle, sometimes referred to muscles that help provide shape. The origin of the gluteus maximus connects to the sacrum, the ilium, or the large upper part of the hip bone, the thoracolumbar fascia tissue, and the sacrotuberous ligaments attached to the posterior superior iliac spine. The gluteus maximus has a 45-degree angle from the pelvis to the buttocks and then inserts at the gluteal tuberosity of the femur and the iliotibial tract.
Variations
Sometimes, a duplicate muscle may originate from the gluteus maximus muscle in rare cases. However, it is more common that the gluteus maximus muscle fibers may be inserted into different body parts than where they are typically inserted. (Taylor, V. G., Geoffrey & Reeves, Rustin. 2015) This can cause a condition called greater trochanteric pain syndrome or GTPS. Inflammation of the gluteus medius, minimum tendons, and bursa inflammation can also cause GTPS. Individuals with GTPS will have tenderness or a pulsing feeling on the outer side of the hip and thigh when lying on the side, along with other symptoms.
Function
The gluteus maximus extends and externally rotates the hip joint, stabilizing the body. It is highly engaged during running and hiking activities. Regular walking does not typically target gluteus maximus strength training. However, the gluteus maximus promotes balance when walking and other activities by helping keep the pelvis and posture upright.
Conditions
The most common condition associated with the gluteus maximus is muscle strain, and deep gluteus maximus syndrome is another condition that can cause pain and involves the muscles.
Muscle Strain
A muscle strain can result from stretching and working the muscle too much that it becomes overstretched or tears. (Falótico G. G. et al., 2015) This can happen from not warming up or cooling down properly, repetitive use injury, and over-exercising. Alternatively, not exercising and not utilizing your gluteus maximus can weaken it, leading to lower back pain, hip pain, and stability and posture issues. (Jeong U. C. et al., 2015)
Deep Gluteus Maximus Syndrome
This syndrome causes pain in the buttocks when the sciatic nerve becomes entrapped. (Martin, H. D. et al., 2015) The location of the pain can help healthcare providers determine where the nerve is trapped. Those with deep gluteus maximus syndrome may experience various types of discomfort, including (Martin, H. D. et al., 2015)
Numbness and tingling in the leg
Pain when sitting
Pain when walking
Pain that radiates down the back and hips and into the thigh
To diagnose the condition, a healthcare provider may perform a physical examination and various tests to rule out other conditions that can cause similar symptoms.
Treatment and Rehabilitation
If there is pain in the buttocks and/or lower extremities, it’s important to consult a primary doctor, chiropractor, or physical therapist. They will evaluate the strength of the gluteus muscles to diagnose any strain or weakness. From there, they will develop a personalized treatment plan to help heal the injury, strengthen the muscles, and restore function. Treatment will include stretches once the strain is rested and improves.
Recommendations can include taking a few days off to rest the muscle or, at the very least, stop performing the work or activity that caused the strain.
Ice and over-the-counter medication like ibuprofen can help reduce inflammation.
For weak gluteus maximus, a physical therapist will strengthen and retrain the muscle with a tailored program of exercises. (Jeong U. C. et al., 2015)
Treatment for deep gluteus maximus syndrome may include conservative treatment, such as chiropractic decompression and realignment, physical therapy, medications for pain and inflammation, and injections.
If conservative treatments do not relieve the pain, a primary healthcare provider may recommend surgery. (Martin, H. D. et al., 2015)
Working with a chiropractic physical therapy team can help individuals return to normal function and expedite healing. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a customized treatment program through an integrated approach to treating injuries and chronic pain syndromes, improving flexibility, mobility, and agility to relieve pain and help individuals return to normal activities. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
The Science of Motion and Chiropractic Care
References
Neto, W. K., Soares, E. G., Vieira, T. L., Aguiar, R., Chola, T. A., Sampaio, V. L., & Gama, E. F. (2020). Gluteus Maximus Activation during Common Strength and Hypertrophy Exercises: A Systematic Review. Journal of sports science & medicine, 19(1), 195–203.
Carro, L. P., Hernando, M. F., Cerezal, L., Navarro, I. S., Fernandez, A. A., & Castillo, A. O. (2016). Deep gluteal space problems: piriformis syndrome, ischiofemoral impingement and sciatic nerve release. Muscles, ligaments and tendons journal, 6(3), 384–396. https://doi.org/10.11138/mltj/2016.6.3.384
Taylor, Victor & Guttmann, Geoffrey & Reeves, Rustin. (2015). A variant accessory muscle of the gluteus maximus. International Journal of Anatomical Variations. 8. 10-11.
Falótico, G. G., Torquato, D. F., Roim, T. C., Takata, E. T., de Castro Pochini, A., & Ejnisman, B. (2015). Gluteal pain in athletes: how should it be investigated and treated?. Revista brasileira de ortopedia, 50(4), 462–468. https://doi.org/10.1016/j.rboe.2015.07.002
Jeong, U. C., Sim, J. H., Kim, C. Y., Hwang-Bo, G., & Nam, C. W. (2015). The effects of gluteus muscle strengthening exercise and lumbar stabilization exercise on lumbar muscle strength and balance in chronic low back pain patients. Journal of physical therapy science, 27(12), 3813–3816. https://doi.org/10.1589/jpts.27.3813
Martin, H. D., Reddy, M., & Gómez-Hoyos, J. (2015). Deep gluteal syndrome. Journal of hip preservation surgery, 2(2), 99–107. https://doi.org/10.1093/jhps/hnv029
For individuals living with chronic pain and various diseases like Parkinson’s, arthritis, and diabetes, can water aerobics be beneficial?
Water Aerobics
Water aerobics are low-impact exercises performed commonly in swimming pools. It is a great way to exercise for a full-body, low-impact workout without overworking the body’s joints and muscles. Other names used include:
Aquafitness
Aqua aerobics
Aquarobics
Many types can be tailored to individual needs, injuries, and/or conditions. The exercises have various health benefits, especially for those who cannot perform higher-impact movements.
Individuals participating in water aerobics will need a bathing suit, towel, goggles, and a swim cap to protect their eyes or hair from chlorinated water. Individuals do not need other special equipment while exercising as the water acts as extra resistance. Foam dumbbells or paddles can be used to increase resistance. Other optional equipment includes: (Plunge San Diego, 2024) (Harvard Health Publishing Harvard Medical School, 2023)
Kickboards
Wrist and ankle weights
Water-jogging belts
Swim bar
Pool Exercises
There are many types of pool exercises to help reach health and fitness goals. They include:
Water Walking
The basic act of walking in water is a great way to get a full-body workout.
Start by standing in waist-deep water with the feet planted on the bottom of the pool.
Lengthen the spine by bringing the shoulders up and back and aligning the shoulders with the hips and knees.
Once in a good starting position, walk through the water, putting pressure on the heel first and then the toes, just like walking out of the water, while swinging the arms back and forth through the water.
This exercise can be done for five to 10 minutes.
The muscles that will get the most attention are the arms, core, and the lower body.
Arm Lifts
Stand up to the shoulders in water.
With the palms facing up, draw the elbows into the torso while lifting the forearms in front of the body up to the water’s surface.
Once at the surface, rotate the palms to face down and slowly move the forearms back down to the sides.
For more resistance, this exercise can also be done using foam dumbbells.
Repeat the action 10–15 times for one to three sets.
The muscles targeted are the core and the arm muscles.
Jumping Jacks
Water resistance makes jumping jacks in the water much more difficult than on land.
To perform, start by standing in chest-level water with your feet together and your arms straight down the sides.
Once in position, begin by simultaneously swinging the legs out to the side and arms over the head before returning to the starting position.
Muscles targeted include the entire body and cardiovascular system.
Add wrist or ankle weights for more resistance and to make the exercise more challenging.
High-Knee-Lift Extensions
High-knee-lift extensions are performed while standing in water that is waist deep.
To do the exercise, engage the core and lift one leg in a bent position until it is level with the water’s surface.
Hold the position for a few seconds, then extend the leg out in front and hold again.
After the hold period, move the leg back down through the water to the starting position while keeping it straight and flexing the foot.
Repeat on both legs for two to three sets of 15 reps per leg.
Use weights on the ankles to increase resistance.
The muscles targeted include the core, glutes, and lower body.
Risks
While exercising in water, individuals may not notice how much they sweat. This can make it seem like the workout is not as hard and can lead to dehydration. Individuals should always hydrate before and after a pool workout. Individuals who cannot swim well should avoid exercises that do not require a flotation device. Sometimes pools are heated, so choosing one 90 degrees F or below is recommended so the body doesn’t get overheated while exercising.
Stop Pool Exercises Immediately
Performing pool exercises can often seem easier than they are, leading to overworking. Stop exercising immediately if you feel:
Pain in any area of the body
Shortness of breath
Nauseated
Faint
Dizzy
Pressure in the upper body or chest
Other Health Conditions That Benefit
Water aerobics is recommended for most individuals, completely healthy or with a chronic disease. Those with chronic disease have been shown to benefit from the low-impact exercise. (Faíl, L. B. et al., 2022) One study looked at individuals with various health conditions, with the results showing that the following conditions saw improvements after 12 weeks of regular water exercise (Faíl, L. B. et al., 2022)
Diabetes
Arthritis
Fibromyalgia
Bone diseases
High blood pressure
Coronary artery disease
Stroke
Multiple sclerosis (MS)
Parkinson’s disease
While the benefits of water aerobics have been studied and proven effective, individuals should be cleared by a medical professional before starting any new exercise regimen. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution through an integrated approach to treating injuries and chronic pain syndromes, improving flexibility, mobility, and agility programs to relieve pain and help individuals return to normal. Our providers create personalized care plans for each patient. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Chiropractic and Integrative Healthcare
References
Harvard Health Publishing Harvard Medical School. (2023). Basic types of water-based exercises. HealthBeat. https://www.health.harvard.edu/healthbeat/basic-types-of-water-based-exercise
Pereira Neiva, H., Brandão Faíl, L., Izquierdo, M., Marques, M. C., & Marinho, D. A. (2018). The effect of 12 weeks of water-aerobics on health status and physical fitness: An ecological approach. PloS one, 13(5), e0198319. https://doi.org/10.1371/journal.pone.0198319
Harvard Health Publishing Harvard Medical School. (2024). Advantages of water-based exercise. HealthBeat. https://www.health.harvard.edu/healthbeat/advantages-of-water-based-exercise
Plunge San Diego. (2024). 5 must-have pieces of aquatic exercise equipment for water aerobics. Plunge San Diego. https://plungesandiego.com/what-equipment-needed-water-aerobics-shoes/
Faíl, L. B., Marinho, D. A., Marques, E. A., Costa, M. J., Santos, C. C., Marques, M. C., Izquierdo, M., & Neiva, H. P. (2022). Benefits of aquatic exercise in adults with and without chronic disease-A systematic review with meta-analysis. Scandinavian journal of medicine & science in sports, 32(3), 465–486. https://doi.org/10.1111/sms.14112
For individuals dealing with sciatica, can non-surgical treatments like chiropractic care and acupuncture reduce pain and restore function?
Introduction
The human body is a complex machine that allows the host to be mobile and stable when resting. With various muscle groups in the upper and lower body portions, the surrounding muscles, tendons, nerves, and ligaments serve a purpose for the body as they all have specific jobs in keeping the host functional. However, many individuals have developed various habits that cause strenuous activities that cause repetitive motions to their muscles and nerves and affect their musculoskeletal system. One of the nerves that many individuals have been dealing with pain is the sciatic nerve, which causes many issues in the lower body extremities and, when not treated right away, leads to pain and disability. Luckily, many individuals have sought non-surgical treatments to reduce sciatica and restore body function to the individual. Today’s article focuses on understanding sciatica and how non-surgical therapies like chiropractic care and acupuncture can help reduce the sciatic pain-like effects that are causing overlapping risk profiles in the lower body extremities. We discuss with certified medical providers who consolidate with our patients’ information to assess how sciatica is often correlated with environmental factors that cause dysfunction in the body. We also inform and guide patients on how various non-surgical treatments can help reduce sciatica and its correlating symptoms. We also encourage our patients to ask their associated medical providers many intricate and important questions about incorporating various non-surgical therapies as part of their daily routine to reduce the chances and effects of sciatica from returning. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
Understanding Sciatica
Do you often feel radiating pain that travels down one or both legs when sitting down for a long period? How often have you experienced tingling sensations that cause you to shake your leg to reduce the effect? Or have you noticed that stretching your legs causes temporary relief? While these overlapping pain symptoms can affect the lower extremities, many individuals may think it is low back pain, but in actuality, it is sciatica. Sciatica is a common musculoskeletal condition that affects many people worldwide by causing pain to the sciatic nerve and radiating down to the legs. The sciatic nerve is pivotal in providing direct and indirect motor function to the leg muscles. (Davis et al., 2024) When the sciatic nerve is compressed, many people state that the pain can vary in intensity, accompanied by symptoms like tingling, numbness, and muscle weakness that can affect a person’s ability to walk and function.
However, some of the root causes that lead to the development of sciatica can play into the factor that causes the pain in the lower extremities. Several inherent and environmental factors are often associated with sciatica, causing lumbar nerve root compression on the sciatic nerve. Factors like poor health status, physical stress, and occupational work are correlated with the development of sciatica and can impact a person’s routine. (Gimenez-Campos et al., 2022) Additionally, some of the root causes of sciatica can include musculoskeletal conditions like herniated discs, bone spurs, or spinal stenosis, which can correlate with these inherent and environmental factors that can reduce many individuals’ motility and life quality. (Zhou et al., 2021) This causes many individuals to seek out treatments to relieve sciatica pain and its correlating symptoms. While the pain caused by sciatica can vary, many individuals often seek non-surgical treatments to alleviate their discomfort and pain from sciatica. This allows them to incorporate effective solutions to managing sciatica.
Beyond Adjustments: Chiropractic & Integrative Healthcare- Video
Chiropractic Care For Sciatica
When it comes to seeking non-surgical treatments to reduce sciatica, non-surgical treatments can reduce the pain-like effects while helping restore body function and mobility. At the same time, non-surgical treatments are customized to the individual’s pain and can be incorporated into a person’s routine. Some non-surgical treatments like chiropractic care are excellent in reducing sciatica and its associated pain symptoms. Chiropractic care is a form of non-surgical therapy that focuses on restoring the body’s spinal movement while improving body function. Chiropractic care utilizes mechanical and manual techniques for sciatica to realign the spine and help the body heal naturally without surgery or medication. Chiropractic care can help decrease intradiscal pressure, increase intervertebral disc space height, and improve the range of motion in the lower extremities. (Gudavalli et al., 2016) When dealing with sciatica, chiropractic care can alleviate the unnecessary pressure on the sciatic nerve and help reduce the risk of reoccurrence through consecutive treatments.
The Effects of Chiropractic Care For Sciatica
Some of the effects of chiropractic care for reducing sciatica can provide insight to the person as chiropractors work with associated medical providers to devise a personalized plan to relieve the pain-like symptoms. Many people who utilize chiropractic care to reduce the effects of sciatica can incorporate physical therapy to strengthen the weak muscles that surround the lower back, stretch to improve flexibility and be more mindful of what factors are causing sciatic pain in their lower extremities. Chiropractic care may guide many people on proper poster ergonomics, and various exercises to reduce the chances of sciatica returning while offering positive effects to the lower body.
Acupuncture For Sciatica
Another form of non-surgical treatment that can help reduce the pain-like effects of sciatica is acupuncture. As a key component in traditional Chinese medicine, acupuncture therapy involves professionals placing thin, solid needles at specific points on the body. When it comes to reducing sciatica, acupuncture therapy can exert analgesic effects on the body’s acupoints, regulate the microglia, and modulate certain receptors along the pain pathway to the nervous system. (Zhang et al., 2023) Acupuncture therapy focuses on restoring the body’s natural energy flow or Qi to promote healing.
The Effects of Acupuncture For Sciatica
Regarding the effects of acupuncture therapy on reducing sciatica, acupuncture therapy can help reduce the pain signals that sciatica produces by changing the brain signal and rerouting the corresponding motor or sensory disturbance of the affected area. (Yu et al., 2022) Additionally, acupuncture therapy can help provide pain relief by releasing endorphins, the body’s natural pain reliever, to the specific acupoint that correlates with the sciatic nerve, reducing inflammation around the sciatic nerve, thus alleviating pressure and pain and helping improve nerve function. Both chiropractic care and acupuncture offer valuable non-surgical treatment options that can provide aid in the healing process and reduce pain caused by sciatica. When many people are dealing with sciatica and looking for numerous solutions to reduce the pain-like effects, these two non-surgical treatments can help many people address the underlying causes of sciatica, enhance the body’s natural healing process, and help provide significant relief from the pain.
Gimenez-Campos, M. S., Pimenta-Fermisson-Ramos, P., Diaz-Cambronero, J. I., Carbonell-Sanchis, R., Lopez-Briz, E., & Ruiz-Garcia, V. (2022). A systematic review and meta-analysis of the effectiveness and adverse events of gabapentin and pregabalin for sciatica pain. Aten Primaria, 54(1), 102144. https://doi.org/10.1016/j.aprim.2021.102144
Gudavalli, M. R., Olding, K., Joachim, G., & Cox, J. M. (2016). Chiropractic Distraction Spinal Manipulation on Postsurgical Continued Low Back and Radicular Pain Patients: A Retrospective Case Series. J Chiropr Med, 15(2), 121-128. https://doi.org/10.1016/j.jcm.2016.04.004
Yu, F. T., Liu, C. Z., Ni, G. X., Cai, G. W., Liu, Z. S., Zhou, X. Q., Ma, C. Y., Meng, X. L., Tu, J. F., Li, H. W., Yang, J. W., Yan, S. Y., Fu, H. Y., Xu, W. T., Li, J., Xiang, H. C., Sun, T. H., Zhang, B., Li, M. H., . . . Wang, L. Q. (2022). Acupuncture for chronic sciatica: protocol for a multicenter randomised controlled trial. BMJ Open, 12(5), e054566. https://doi.org/10.1136/bmjopen-2021-054566
Zhang, Z., Hu, T., Huang, P., Yang, M., Huang, Z., Xia, Y., Zhang, X., Zhang, X., & Ni, G. (2023). The efficacy and safety of acupuncture therapy for sciatica: A systematic review and meta-analysis of randomized controlled trails. Front Neurosci, 17, 1097830. https://doi.org/10.3389/fnins.2023.1097830
Zhou, J., Mi, J., Peng, Y., Han, H., & Liu, Z. (2021). Causal Associations of Obesity With the Intervertebral Degeneration, Low Back Pain, and Sciatica: A Two-Sample Mendelian Randomization Study. Front Endocrinol (Lausanne), 12, 740200. https://doi.org/10.3389/fendo.2021.740200
When sciatica or other radiating nerve pain presents, can learning to distinguish between nerve pain and different types of pain help individuals recognize when spinal nerve roots are irritated or compressed or more serious problems that require medical attention?
Spinal Nerve Roots and Dermatomes
Spinal conditions such as herniated discs and stenosis can lead to radiating pain that travels down one arm or leg. Other symptoms include weakness, numbness, and/or shooting or burning electrical sensations. The medical term for pinched nerve symptoms is radiculopathy (National Institutes of Health: National Institute of Neurological Disorders and Stroke. 2020). Dermatomes could contribute to irritation in the spinal cord, where the nerve roots cause symptoms in the back and limbs.
Anatomy
The spinal cord has 31 segments.
Each segment has nerve roots on the right and left that supply motor and sensory functions to the limbs.
The anterior and posterior communicating branches combine to form the spinal nerves that exit the vertebral canal.
The 31 spine segments result in 31 spinal nerves.
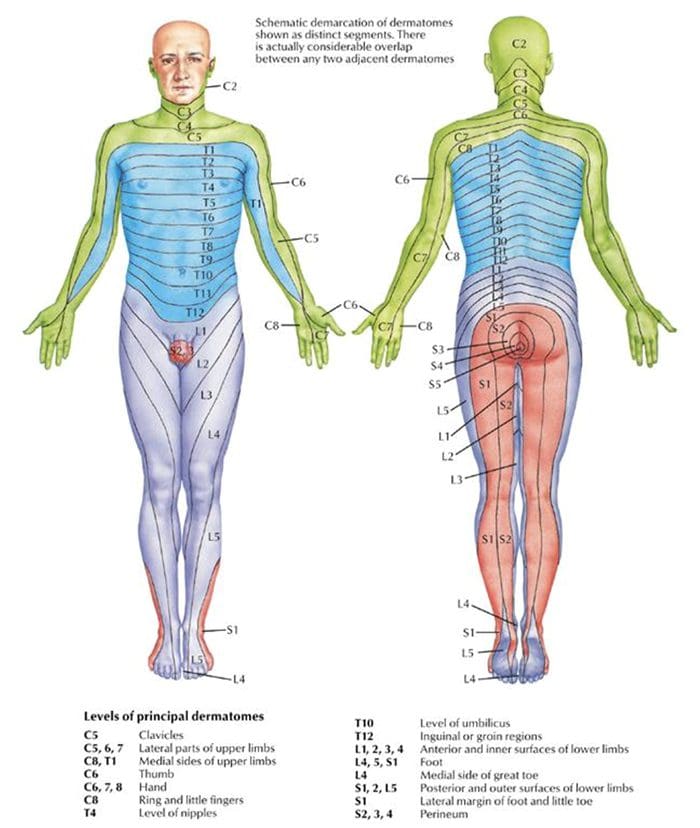
Each one transmits sensory nerve input from a specific skin region on that side and area of the body.
These regions are called dermatomes.
Except for the first cervical spinal nerve, dermatomes exist for each spinal nerve.
The spinal nerves and their associated dermatomes form a network all over the body.
Dermatomes Purpose
Dermatomes are the body/skin areas with sensory input assigned to individual spinal nerves. Each nerve root has an associated dermatome, and various branches supply each dermatome off that single nerve root. Dermatomes are pathways through which sensational information in the skin transmits signals to and from the central nervous system. Sensations that are physically felt, like pressure and temperature, get transmitted to the central nervous system. When a spinal nerve root becomes compressed or irritated, usually because it comes into contact with another structure, it results in radiculopathy. (National Institutes of Health: National Institute of Neurological Disorders and Stroke. 2020).
Radiculopathy
Radiculopathy describes symptoms caused by a pinched nerve along the spine. Symptoms and sensations depend on where the nerve is pinched and the extent of the compression.
Cervical
This is a syndrome of pain and/or sensorimotor deficiencies when nerve roots in the neck are compressed.
It often presents with pain that goes down one arm.
Individuals may also experience electrical sensations like pins and needles, shocks, and burning sensations, as well as motor symptoms like weakness and numbness.
Lumbar
This radiculopathy results from compression, inflammation, or injury to a spinal nerve in the lower back.
Sensations of pain, numbness, tingling, electrical or burning sensations, and motor symptoms like weakness traveling down one leg are common.
Diagnosis
Part of a radiculopathy physical examination is testing the dermatomes for sensation. The practitioner will use specific manual tests to determine the spinal level from which the symptoms originate. Manual exams are often accompanied by diagnostic imaging tests like MRI, which can show abnormalities in the spinal nerve root. A complete physical examination will determine if the spinal nerve root is the source of the symptoms.
Treating Underlying Causes
Many back disorders can be treated with conservative therapies to provide effective pain relief. For a herniated disk, for example, individuals may be recommended to rest and take a nonsteroidal anti-inflammatory medication. Acupuncture, physical therapy, chiropractic, non-surgical traction, or decompression therapies may also be prescribed. For severe pain, individuals may be offered an epidural steroid injection that can provide pain relief by reducing inflammation. (American Academy of Orthopaedic Surgeons: OrthoInfo. 2022) For spinal stenosis, a provider may first focus on physical therapy to improve overall fitness, strengthen the abdominals and back muscles, and preserve motion in the spine. Pain-relieving medications, including NSAIDs and corticosteroid injections, can reduce inflammation and relieve pain. (American College of Rheumatology. 2023) Physical therapists provide various therapies to decrease symptoms, including manual and mechanical decompression and traction. Surgery may be recommended for cases of radiculopathy that don’t respond to conservative treatments.
Injury Medical Chiropractic and Functional Medicine Clinic care plans and clinical services are specialized and focused on injuries and the complete recovery process. Our areas of practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols. We focus on restoring normal body functions after trauma and soft tissue injuries using Specialized Chiropractic Protocols, Wellness Programs, Functional and integrative Nutrition, Agility, and mobility Fitness Training, and Rehabilitation Systems for all ages. If the individual requires other treatment, they will be referred to a clinic or physician best suited for their condition. Dr. Jimenez has teamed with the top surgeons, clinical specialists, medical researchers, therapists, trainers, and premiere rehabilitation providers to bring El Paso, the top clinical treatments, to our community.
Reclaim Your Mobility: Chiropractic Care For Sciatica Recovery
References
National Institutes of Health: National Institute of Neurological Disorders and Stroke. (2020). Low back pain fact sheet. Retrieved from https://www.ninds.nih.gov/sites/default/files/migrate-documents/low_back_pain_20-ns-5161_march_2020_508c.pdf
American Academy of Orthopaedic Surgeons: OrthoInfo. (2022). Herniated disk in the lower back. https://orthoinfo.aaos.org/en/diseases–conditions/herniated-disk-in-the-lower-back/
American College of Rheumatology. (2023). Spinal stenosis. https://rheumatology.org/patients/spinal-stenosis
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine