For individuals experiencing lower back pain and sciatica symptoms, can using a lidocaine patch help?
Lidocaine Patch
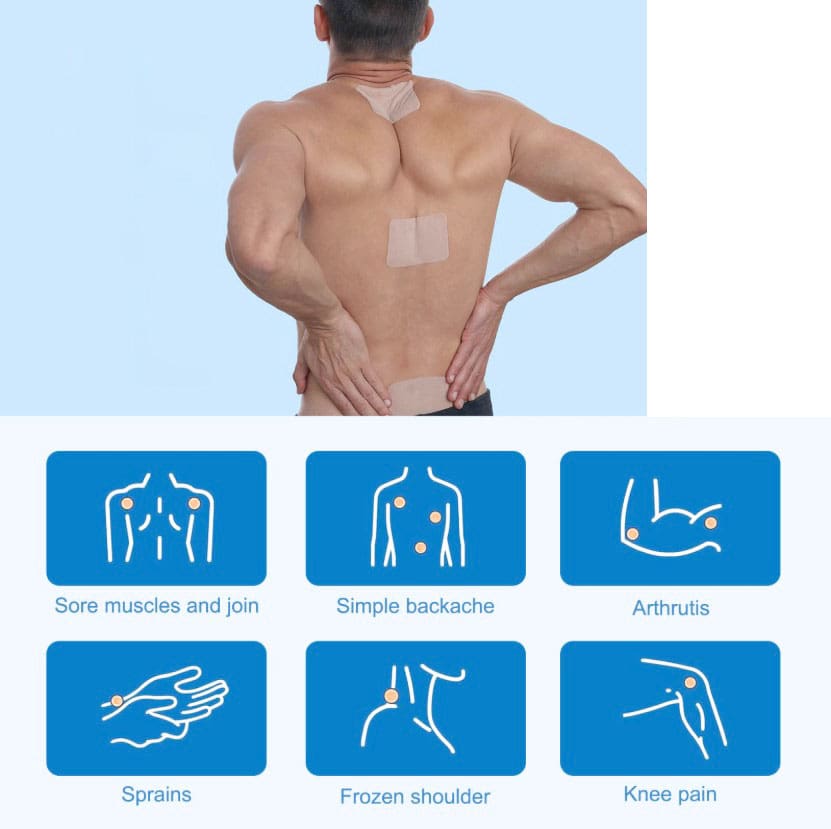
Lidocaine patches are in a drug class called local anesthetics (MedlinePlus, 2025) (Food and Drug Administration, 2022). They relieve pain in small body areas by blocking the nerves from sending pain signals. The Food and Drug Administration approved lidocaine 5% or 1.8% patches for relieving postherpetic neuralgia (PHN) pain. These lidocaine patches are prescription-only (Food and Drug Administration, 2022). They are available either by prescription or over the counter and are commonly used for back pain and other areas. Over-the-counter lidocaine, 4% patches, can be used to relieve minor aches and pains, including back pain. However, further research is needed to recommend the use of lidocaine patches as an effective method of pain relief. (Department of Veterans Affairs/Department of Defense, 2022) (North American Spine Society, 2020)
The Patch
They are available in prescription and over-the-counter forms. Over-the-counter forms come as a 4% patch in various brands, such as (MedlinePlus, 2025)
Aspercreme
Lidocare
Salonpas
Prescription-only patches come in 5% or 1.8% patches and are approved to relieve long-term nerve pain from shingles in adults. Zlido is a brand name for a 1.8% lidocaine patch. Five percent lidocaine patches are available generically. (DailyMed, 2018) (Food and Drug Administration, 2021) The safety and effectiveness in children are unknown. (Food and Drug Administration, 2022)
Other Lidocaine Forms
As a local anesthetic, it is available in several other forms, including:
Spray
Topical cream
Lotion
Liquid
Ear drops
Eye gel
Injection
It is also available as a short-term intravenous infusion for abnormal heart rhythm. (DailyMed, 2025)
Effectiveness
Clinical trials have shown that the patches effectively relieve chronic low back pain. However, these studies were nonrandomized and did not include a control group to compare against the treatment group. (Santana J. A., Klass S., & Felix E. R. 2020) The results may be subject to potential biases. For this reason, further evidence is needed to support lidocaine patches’ effectiveness in reducing low back pain. (North American Spine Society, 2020) High-quality randomized and controlled clinical trials are necessary to study the effectiveness. (North American Spine Society, 2020) (Santana J. A., Klass S., & Felix E. R. 2020)
Clean and dry the affected area before placing the patch.
Apply to the affected body area as directed.
Wash your hands after touching the patch.
Remove the patch after what is usually recommended after eight hours.
How Quickly Does It Work?
The amount of medication absorbed into the blood depends on how long the patch is placed on the body and how much is covered with the patch. In a study, healthy participants wore three lidocaine patches on their backs for 12 hours on and 12 hours off during 24 hours. Lidocaine levels were highest at 11 hours. At the end of the 24 hours, there was still some lidocaine left in the bloodstream. (Food and Drug Administration, 2022)
Individuals with PHN may notice a difference in pain intensity after four hours of using the patch. (Rowbotham, M. C. et al., 1996) (Food and Drug Administration, 2022) Experts may suggest using patches for four weeks for those who experience pain after their shingles rash disappears. However, if there is still pain after these four weeks, it is recommended to see a pain specialist. (Gross, G. E. et al., 2020)
Side Effects
Common side effects are typically mild skin reactions where the patch is. These reactions are usually temporary and will disappear within a few minutes or hours. Examples include: (Food and Drug Administration, 2022)
Severe allergic reactions are rare, but it is possible.
Symptoms include breathing problems, itchiness, and rash.
Methemoglobinemia
Methemoglobinemia is a condition that makes it hard for red blood cells to carry oxygen.
Individuals may experience symptoms of blue-looking skin, headache, lightheadedness, shortness of breath, abnormal heart rhythm, or seizures.
Using too many lidocaine patches to cover large parts of the body or using the patches longer than 12 hours within 24 hours may cause side effects that may include heart-related effects, such as a slow heart rate and low blood pressure. Individuals may also experience the following side effects (Food and Drug Administration, 2022)
Hot or cold sensation
Numbness
Dizziness
Ringing ears
Lightheadedness
Mood changes
Drowsiness to unconsciousness
Vision changes
Seizures
Tremors
Vomiting
Injury Medical Chiropractic & Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Sciatica Causes and Treatments
References
National Library of Medicine. MedlinePlus. (2025). Lidocaine transdermal patch. Retrieved from https://medlineplus.gov/druginfo/meds/a603026.html
Food and Drug Administration. (2022). Lidoderm label. Retrieved from https://www.accessdata.fda.gov/spl/data/eedfe43b-1019-19a0-e053-2995a90a7696/eedfe43b-1019-19a0-e053-2995a90a7696.xml
Department of Veterans Affairs/Department of Defense. (2022). VA/DoD clinical practice guideline for the diagnosis and treatment of low back pain. Retrieved from https://www.healthquality.va.gov/guidelines/Pain/lbp/VADoDLBPCPGFinal508.pdf
North American Spine Society. (2020). Evidence-based clinical guidelines for multidisciplinary spine care: diagnosis and treatment of low back pain. https://www.spine.org/Portals/0/assets/downloads/ResearchClinicalCare/Guidelines/LowBackPain.pdf
National Library of Medicine. DailyMed. (2018). Label: lidocaine patch. Retrieved from https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=5c66f3b9-6e04-47ab-8d94-21e89ceec154
Food and Drug Administration. (2021). Ztlido label. Retrieved from https://www.ztlido.com/wp-content/uploads/2022/12/ZTlido-LABEL.pdf
National Library of Medicine. DailyMed. (2025). Lidocaine-lidocaine hydrochloride injection, solution. Retrieved from https://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=f1b26274-a55e-4321-b96c-ce0df830f205
Santana, J. A., Klass, S., & Felix, E. R. (2020). The Efficacy, Effectiveness and Safety of 5% Transdermal Lidocaine Patch for Chronic Low Back Pain: A Narrative Review. PM & R: the journal of injury, function, and rehabilitation, 12(12), 1260–1267. https://doi.org/10.1002/pmrj.12366
Rowbotham, M. C., Davies, P. S., Verkempinck, C., & Galer, B. S. (1996). Lidocaine patch: double-blind controlled study of a new treatment method for post-herpetic neuralgia. Pain, 65(1), 39–44. https://doi.org/10.1016/0304-3959(95)00146-8
Gross, G. E., Eisert, L., Doerr, H. W., Fickenscher, H., Knuf, M., Maier, P., Maschke, M., Müller, R., Pleyer, U., Schäfer, M., Sunderkötter, C., Werner, R. N., Wutzler, P., & Nast, A. (2020). S2k guidelines for the diagnosis and treatment of herpes zoster and postherpetic neuralgia. Journal der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology: JDDG, 18(1), 55–78. https://doi.org/10.1111/ddg.14013
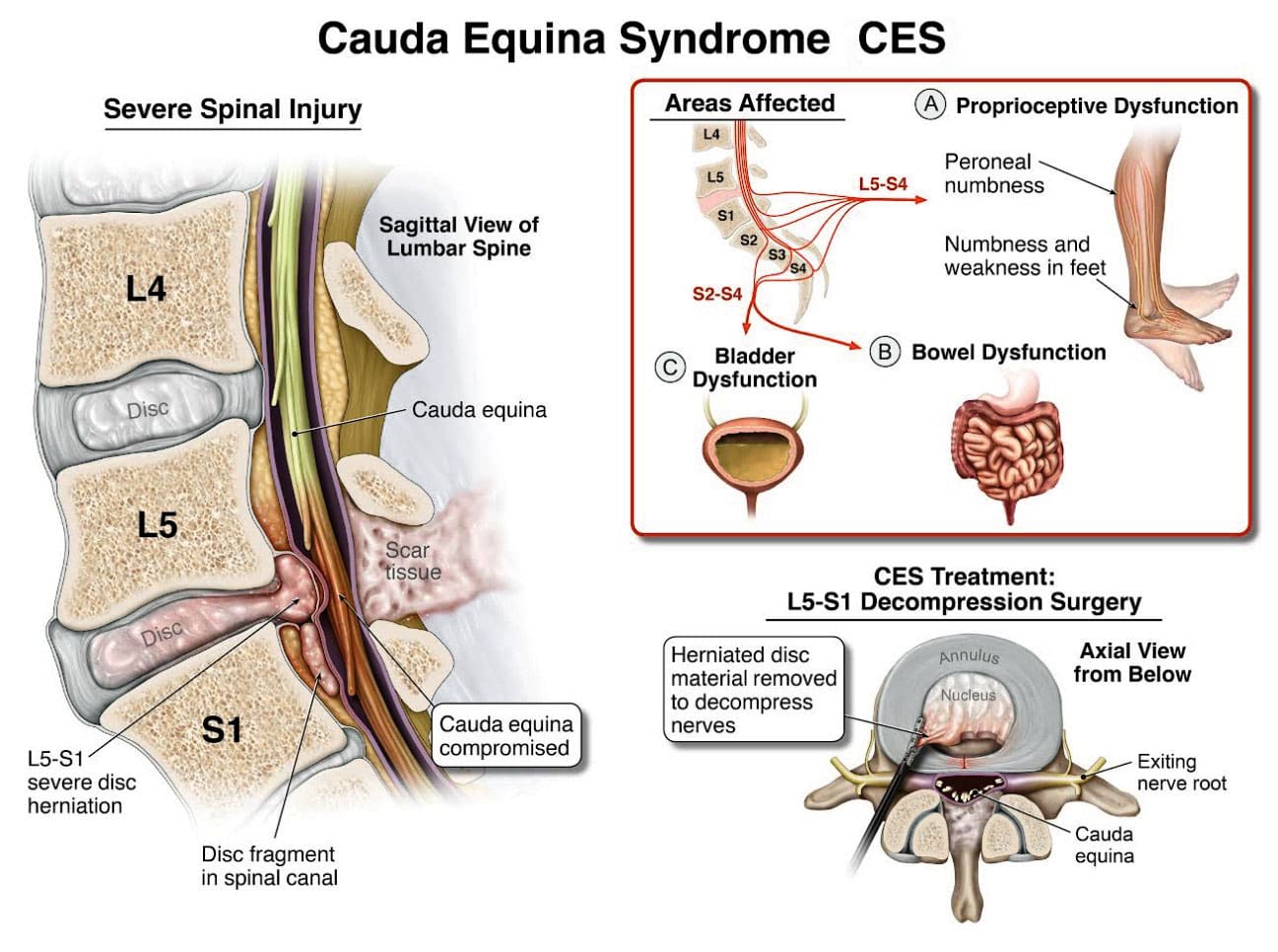
Cauda equina syndrome/CES is a rare condition in which the nerves in the lower back are compressed. It can include sciatica as one of its symptoms. Individuals presenting with symptoms that could be CES are advised to see a healthcare provider as soon as possible, as delaying treatment can lead to permanent damage.
Cauda Equina Syndrome
A cluster of nerve roots called the cauda equina, Latin for horse’s tail, sends and receives messages to the legs, bladder, and other body parts. Cauda equina syndrome is a rare condition in which nerve roots in the lower spinal cord are compressed. This compresses the nerves and disrupts motor and sensory function in the bladder and lower extremities. The most common cause is a ruptured or herniated disc in the lumbar area. This usually occurs when a severe disc herniation compresses the nerve bundle at the base of the spinal cord, causing significant neurological dysfunction like bladder/bowel issues and numbness in the saddle area. If found early, it is treated with surgery within 24 to 48 hours of symptom onset.
This is characterized by symptoms that include unusual urinary sensation, loss of desire to urinate, poor urinary stream, and having to strain to urinate. (Gardner A., Gardner E., & Morley T. 2011)
Pott’s paralysis is a neurological complication of tuberculosis (TB) of the spine.
TB is a bacterial infection that usually affects the lungs but can spread to the spine.
Iatrogenic Side Effects
Injuries or illnesses that result from medical or surgical treatment
Spinal Lesions or Malignant Tumors
A spinal lesion refers to any abnormal growth or damage within the spine.
It can include benign (noncancerous) and malignant (cancerous) tumors.
A malignant tumor is a cancerous growth within the spine; essentially, a malignant tumor is a type of spinal lesion with the potential to spread to other parts of the body.
Spinal Infection, Inflammation, Hemorrhage, or Fracture
A spinal infection refers to a bacterial, fungal, or viral infection that occurs within the bones of the spine (vertebrae) or the surrounding tissues, potentially causing pain, inflammation, and, in severe cases, neurological complications like weakness or paralysis;
Spinal inflammation is a general term for swelling or irritation within the spinal column.
Spinal hemorrhage” indicates bleeding within the spinal canal.
A spinal fracture refers to a break in one or more of the vertebrae in the spine.
Spinal Arteriovenous Malformations (AVMs)
A spinal arteriovenous malformation (AVM) is a rare condition in which the arteries and veins in the spinal cord tangle abnormally.
This can damage the spinal cord over time.
Complications from Lumbar Surgery
Lumbar surgery can have several complications, including infections, blood clots, nerve damage, and spinal fluid leaks.
Spinal Anesthesia
Spinal anesthesia is a regional anesthesia that blocks pain and sensation in the lower body.
It involves injecting a local anesthetic medication into the subarachnoid space surrounding the spinal cord.
The exact cause is not fully understood, but it can involve direct nerve root injury from the needle, inflammation caused by the anesthetic, or a spinal hematoma compressing the nerve roots.
Infection of the tissues (meninges) that cover the cauda equina and spinal cord.
An abscess pressing on the cauda equina.
Diagnosis
Diagnosis requires a medical history of symptoms, general health, activity level, and a physical exam to assess strength, reflexes, sensation, stability, alignment, and motion. (American Association of Neurological Surgeons, 2024) Testing includes:
X-ray or computerized tomography (CT) imaging is enhanced by the injection of contrast material into the cerebrospinal fluid spaces, which can show displacement of the spinal cord or spinal nerves.
Specialized Nerve Testing
This could be nerve conduction velocity tests and testing electrical activity in muscles or electromyography.
Treatment
The extent of urinary problems can determine treatment protocols. A CES diagnosis is usually followed by emergency surgery within 24 to 48 hours to relieve compression of the nerves. Moving quickly is essential to prevent permanent complications such as nerve damage, incontinence, or leg paralysis. (American Association of Neurological Surgeons, 2024)
Depending on the cause, corticosteroids also may be prescribed to reduce swelling.
Antibiotics may be needed if an infection is responsible for CES.
For situations in which a tumor is the cause, surgery to remove it may be necessary, followed by chemotherapy and/or radiation.
The outcome with CES-I during surgery is generally favorable.
Those whose CES has deteriorated to CES-R tend to have a less favorable prognosis.
Post Surgery Therapy
After surgery, CES can be challenging to deal with. If bladder function has been impaired, recovery of control can take time.
Frequent urinary infections are also a potential complication.
Loss of bladder or bowel control can be psychologically distressing, impacting social life, work, and relationships.
Sexual dysfunction can also occur, contributing to relationship difficulties or depression.
Therapy with a mental health professional may be recommended. When damage is permanent, it will be important to include family and friends in the adjustment to living with a chronic condition. Psychological counseling and/or a support group can be helpful. Other specialists who can help include: (American Academy of Orthopaedic Surgeons, 2024)
Occupational therapist
Physical therapist
Physiotherapist
Sex therapist
Social worker
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and mitigate issues through adjustments that help the body realign itself. The clinic can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Disc Herniation
References
American Association of Neurological Surgeons. (2024). Cauda Equina Syndrome. https://www.aans.org/patients/conditions-treatments/cauda-equina-syndrome/
Gardner, A., Gardner, E., & Morley, T. (2011). Cauda equina syndrome: a review of the current clinical and medico-legal position. European Spine Journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 20(5), 690–697. https://doi.org/10.1007/s00586-010-1668-3
Fairbank, J., & Mallen, C. (2014). Cauda equina syndrome: implications for primary care. The British journal of general practice: the journal of the Royal College of General Practitioners, 64(619), 67–68. https://doi.org/10.3399/bjgp14X676988
American Academy of Orthopaedic Surgeons. (2024). Cauda equina syndrome. https://orthoinfo.aaos.org/en/diseases–conditions/cauda-equina-syndrome
Can individuals dealing with sciatica incorporate nonsurgical treatments to reduce thigh pain and restore mobility in the legs and hips?
The Tensor Fascia Latae
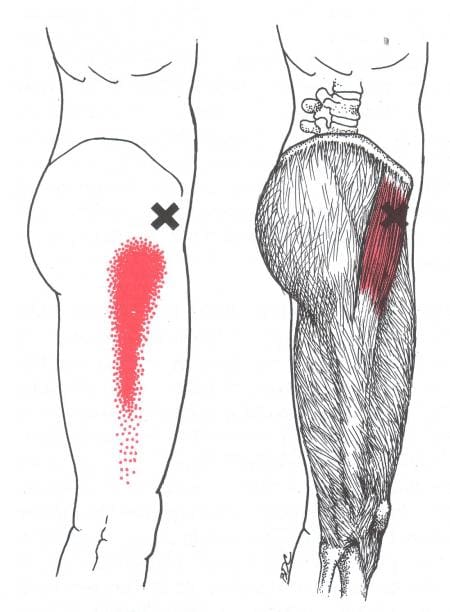
Do you feel stiffness or tightness in your legs, feet, and hips? Have you experienced walking crookedly when running errands? Or have you experienced radiating pain from your gluteal region down to your feet? The hips, thighs, and legs have numerous muscles, tissues, and ligaments surrounding the skeletal bone in the body’s lower extremities. These components allow the lower half of the body to stabilize the upper body’s weight and enable the individual to be mobile throughout the day. One muscle that works together is the tensor fasciae latae (TFL) muscle. The TFL muscle is part of the proximal anterolateral thigh between the deep fibers of the iliotibial (IT) band. It works with the gluteal muscles in various hip movements and assists with the knees. (Trammell et al., 2025) This muscle is poorly misunderstood as it helps with the hips and knee joint and pelvic stability. (Iyengar et al., 2022) At the same time, it has a casual relationship with the IT band.
The Iliotibial Band (ITB)
The iliotibial (IT) band is part of the lower extremities as it is a tough, fibrous fascial tissue that works together with the TFL muscle and has various functional roles that are dependent on posture and allows the individual to be mobile via walking, sprinting, and running. (Hutchinson et al., 2022) However, this muscle’s main function is knee flexion. When environmental factors affect the body, it can cause irritation and inflammation to the IT band, causing knee pain. (Martinez-Velez et al., 2020) When dealing with issues within their lower extremities, they affect the IT band, TFL muscle, and the thighs. Environmental factors can also affect the lower extremities as the surrounding muscles can aggravate the nerve roots, thus leading to sciatica pain. We associate with certified medical providers who inform our patients of how sciatica can negatively impact the lower extremities, especially the thighs. While asking important questions to our associated medical providers, we advise patients to integrate various non-invasive treatments to reduce sciatica and help regain mobility back to the lower body. Dr. Alex Jimenez, D.C., envisions this information as an academic service. Disclaimer.
Reclaim Your Mobility: Chiropractic Care For Sciatica Recovery-Video
Sciatica & Thigh Pain
When the general population hears about sciatica, it is a frequent diagnosis associated with low back pain, which causes discomfort within the lower extremities, especially in the thighs. Sciatica is a debilitating condition where the sciatic nerve is often compressed and irritated, causing pain. (Davis et al., 2025) Many influences cause sciatica to develop, and it can cause the individual to deal with a spinal imbalance, which correlates with walking incorrectly, causing the accessory muscles to work overtime and compressing the sciatic nerve, causing thigh pain. (Wang et al., 2022) With thigh pain correlating with sciatica, many symptoms can range from muscle weakness, absence of tendon reflexes to the knees, and sensory deficit. (Fairag et al., 2022) Luckily, treatments are available to reduce thigh pain associated with sciatica and regain mobility back to the lower extremities.
Treatments For Sciatica-Thigh Pain
When treating the lower extremities, especially when experiencing sciatica-thigh pain, many individuals with thigh pain associated with sciatica can incorporate non-invasive treatments to reduce the pain. Many athletic and non-athletic individuals can utilize PRICE (protection, rest, ice, compression, and elevation) to the affected muscles that can minimize the injuries causing pain. (Lempainen et al., 2022) This can help reduce the inflammatory effects causing issues to the thighs and lower extremities. Many non-surgical treatments like physio-exercise therapy, massages, stretching, and spinal stabilization therapies can improve core strength and posture and help with range of motion to relieve sciatica pain affecting the lower extremities. (Aguilar-Shea et al., 2022) Other non-surgical treatments like yoga, physical therapy, and chiropractic care can help improve joint and lower extremity motions, stretch and strengthen weak muscles surrounding the thighs, and relieve sciatic nerve pain. (Kim & Yim, 2020) When people start thinking about their bodies and how pain is affecting their quality of life, many can incorporate non-surgical treatments to reduce the pain associated with sciatica. Many people can make small positive changes in their routine by becoming more physically active, stretching more, eating healthier, and being more mindful of what they are doing, which can reduce the chances of sciatica returning and affecting the lower extremities. This can help them achieve a healthier, better life.
References
Aguilar-Shea, A. L., Gallardo-Mayo, C., Sanz-Gonzalez, R., & Paredes, I. (2022). Sciatica. Management for family physicians. J Family Med Prim Care, 11(8), 4174-4179. https://doi.org/10.4103/jfmpc.jfmpc_1061_21
Fairag, M., Kurdi, R., Alkathiry, A., Alghamdi, N., Alshehri, R., Alturkistany, F. O., Almutairi, A., Mansory, M., Alhamed, M., Alzahrani, A., & Alhazmi, A. (2022). Risk Factors, Prevention, and Primary and Secondary Management of Sciatica: An Updated Overview. Cureus, 14(11), e31405. https://doi.org/10.7759/cureus.31405
Hutchinson, L. A., Lichtwark, G. A., Willy, R. W., & Kelly, L. A. (2022). The Iliotibial Band: A Complex Structure with Versatile Functions. Sports Med, 52(5), 995-1008. https://doi.org/10.1007/s40279-021-01634-3
Iyengar, K. P., Azzopardi, C., Kiernan, G., & Botchu, R. (2022). Isolated pathologies of Tensor Fasciae Latae: Retrospective cohort analysis from a tertiary referral centre. J Clin Orthop Trauma, 29, 101870. https://doi.org/10.1016/j.jcot.2022.101870
Kim, B., & Yim, J. (2020). Core Stability and Hip Exercises Improve Physical Function and Activity in Patients with Non-Specific Low Back Pain: A Randomized Controlled Trial. Tohoku J Exp Med, 251(3), 193-206. https://doi.org/10.1620/tjem.251.193
Lempainen, L., Mecho, S., Valle, X., Mazzoni, S., Villalon, J., Freschi, M., Stefanini, L., Garcia-Romero-Perez, A., Burova, M., Pleshkov, P., Pruna, R., Pasta, G., & Kosola, J. (2022). Management of anterior thigh injuries in soccer players: practical guide. BMC Sports Sci Med Rehabil, 14(1), 41. https://doi.org/10.1186/s13102-022-00428-y
For individuals who injure their neck or back, the muscles may spasm or seize up, making it difficult to get through the day, exercises, physical activities, etc. Can skeletal muscle relaxers help relieve pain and reduce frequency?
Back Spasms Muscle Relaxers
Back muscle spasms are common back pain that feels like a sudden tightness or contraction in the back muscles. They can range from minor twinges to severe pain.
Causes
Poor posture: Sitting or standing with bad posture can strain the back muscles.
Overuse: Picking something up, bending, or lifting can cause a spasm.
Dehydration: Not drinking enough water can cause electrolyte imbalances, leading to spasms.
Underlying conditions: A herniated disc or degenerative disc disease can cause back spasms.
Muscle imbalances: Weak muscles or muscles that are too tight can cause spasms.
Treatments
Home treatments: You can apply heat or ice, take over-the-counter pain medication, try gentle stretching, or massage the area.
Exercise: Improve your back’s strength and flexibility with exercise or physical therapy.
Hydration and nutrition: Drink enough water and eat foods rich in magnesium and calcium.
Chiropractic Adjustments: These can realign the spine to the correct position and muscles to relax.
Non-surgical Decompression: Decompression of the spine will allow more blood and nutrients to heal painful areas.
Skeletal Muscle Relaxers
A healthcare provider may prescribe skeletal muscle relaxers. These medications are not available over the counter and must be prescribed by a healthcare provider.
Skeletal muscle relaxers will probably cause drowsiness.
Individuals should not drive, operate heavy machinery, or engage in other physical activities while taking back spasm muscle relaxers.
Skeletal muscle relaxers are not recommended for 65 or older because safer, effective alternatives exist.
Also, women who are pregnant or breastfeeding should not take these medications.
Discuss these issues with your healthcare provider.
Carisoprodol
Carisoprodol is available generically and as Soma and Vanadom brands. It works by suppressing nerve impulses located in the brain and spinal cord. Healthcare providers prescribe this medication in combination with physical therapy for the healing release of any muscle spasm and management of musculoskeletal injuries and/or pain. (Witenko C. et al., 2014) It’s not about having to continue taking the medication to feel better but more as a jump start to help with the physical therapy program.
Back muscle spasms are a perfect example of a condition that may benefit from carisoprodol in the short term.
Carisoprodol can be habit-forming.
Be sure to talk to a healthcare provider before suddenly going off this medication.
Carisoprodol can cause side effects that may impair thinking or reactions.
Inform your healthcare provider of any drug allergies, kidney disease, or liver disease, or if you get seizures.
Cyclobenzaprine
Cyclobenzaprine is available as Amrix and in generic form. Like other muscle relaxers, cyclobenzaprine may cause dizziness or drowsiness. The sedation effects are how it works on painful, tension-filled muscles. Cyclobenzaprine is used together with physical therapy to treat skeletal muscle-related conditions and/or injuries, especially when pain or spasm is involved. When used in conjunction with physical therapy, it can help expedite recovery.
Cyclobenzaprine is chemically related to tricyclic antidepressants.
Although it is considered a derivative of the tricyclic antidepressant class, it does not pose the same risk to liver health.
According to the National Institutes of Health, reasons not to take this medication include having a thyroid disorder, heart block, congestive heart failure, a heart rhythm disorder, or having recently had a heart attack. (Witenko C. et al., 2014)
Metaxalone
Skelaxin is the brand name for metaxalone. As with the other muscle relaxers, metaxalone is used in combination with physical therapy and rest when muscles get too tight. (Witenko C. et al., 2014) It works by suppressing nerve impulses in the brain and spinal cord. In addition to older individuals and pregnant women, metaxalone is usually not prescribed for those with kidney disease, liver disease, seizures, or blood disorders.
Injury Medical Chiropractic and Functional Medicine Clinic
Back spasms: Muscle relaxers could help individuals, along with a personalized physical therapy treatment program. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Thoracic Spine Pain
References
Witenko, C., Moorman-Li, R., Motycka, C., Duane, K., Hincapie-Castillo, J., Leonard, P., & Valaer, C. (2014). Considerations for the appropriate use of skeletal muscle relaxants for the management of acute low back pain. P & T: a peer-reviewed journal for formulary management, 39(6), 427–435.
Zacny, J. P., Paice, J. A., & Coalson, D. W. (2012). Subjective and psychomotor effects of carisoprodol in combination with oxycodone in healthy volunteers. Drug and alcohol dependence, 120(1-3), 229–232. https://doi.org/10.1016/j.drugalcdep.2011.07.006
Stress on the lower back during pregnancy often leads to back (upper, middle, lower), sciatica, and leg pain. Can you use a massage gun while pregnant?
Pregnancy Massage Gun Use
Pregnant women often experience back, hip, and leg pain along with symptoms such as swelling (edema), muscle spasms, cramps, and fatigue, which interfere with daily functions and sleep. Pregnancy massage gun use is a safe and helpful form of stress and tension relief, so long as healthcare providers and safety precautions are followed and sensitive areas are avoided. Massage guns use percussion and vibration to create a form of massage that can relieve tension, stiffness, and muscle soreness, break up tissue adhesions, and reduce inflammation. Moreover, pregnancy massage can provide relaxation and pain relief for muscles and joints that are adapting to a growing, changing body. Traditional massage therapy and massage gun therapy have been shown to help reduce muscle soreness and pain. (Imtiyaz S., Veqar Z., & Shareef M. Y. 2014) The benefits of pregnancy massage gun use include:
However, it is essential to discuss massage gun use with a healthcare professional and follow safety precautions when using massage guns during pregnancy.
Benefits
While there is no specific research on the benefits of massage guns for pregnant individuals, studies have demonstrated the general benefits of massage during pregnancy, including deep tissue massage. Therapeutic massage effectively reduces pregnancy discomforts and pain and is a safe and affordable method of pain relief. (El-Hosary EA, Abbas Soliman HF, El-Homosy SM. 2016) Researchers believe this relief helps improve the health of mother and baby in ways that include. (El-Hosary EA, Abbas Soliman HF, El-Homosy SM. 2016) (Mueller S. M., & Grunwald M. 2021)
Improves cardiovascular health
Overall circulation improves
Increases serotonin and dopamine levels
Decreases chronic back pain
Relieves muscle aches and joint pains
Improves sleep patterns
Increases energy
Reduces anxiety
Increases immune response
Enhances sense of well-being and mood
Reduces risk of preterm delivery
Massage Gun Safety
Pregnancy massage gun use is generally safe for those who do not have preexisting conditions. (Mueller S. M., & Grunwald M. 2021) However, there are no studies on the safety of massage guns or other massage tools for pregnant individuals. It is recommended to discuss the use of massage guns with a doctor before use.
Individuals with high-risk factors, such as bleeding, pre-term contractions, and preeclampsia, should avoid using massage guns unless a doctor clears them to do so.
Preeclampsia
This condition causes a rise in blood pressure that can be serious.
It typically develops around 20 weeks of pregnancy or later.
Deep Vein Thrombosis – DVT
Avoid using a massage gun if there is a history of deep vein thrombosis.
Blood volume increases during pregnancy, and leg circulation can be poor.
Certain hormones that prevent hemorrhage during delivery can cause blood to clot more easily.
Using a massage gun on areas with potential blood clots may release the clot, leading to a life-threatening embolism. (Sutham K. et al., 2020)
Compression socks are a better alternative for relieving leg pain and swelling, but follow the healthcare provider’s recommendations.
Placenta Previa, Accrete, or Abruption
These conditions involve the placenta, which can lead to bleeding.
Gestational Diabetes
High blood sugar levels do not necessarily mean individuals cannot use a massage gun during pregnancy.
However, speak to a doctor and monitor blood sugar before use.
How to Use
Although there are no specific expert directions for the use of massage guns during pregnancy, there are guidelines to consider while using the device. This includes:
Never place the massage gun directly over bones, nerves, or joints.
Avoid using the device around injured, swollen, or painful areas.
Avoid using a massage gun directly on the abdomen.
Start by trying a light 10- to 15-second pass over sore or tight areas.
Perform three to five sweeps over the location, then move on to another.
Be careful not to keep the gun on a single area too long, as you could overwork the muscle, leading to bruising and irritation.
The recommended time for leaving the massager in one area is two minutes.
Stop using the massage gun if there is unusual pain, sensations, or discomfort.
Injury Medical Chiropractic and Functional Medicine Clinic
Massage during pregnancy can help relieve symptoms such as anxiety, stress, pain, discomfort, tightness, and poor circulation. Regular massage can help improve sleep and can even benefit the baby. However, it is recommended to consult with a doctor about using a massage gun before trying it out. Injury Medical Chiropractic and Functional Medicine Clinic can help individuals recover and regain the benefits of quality rest through healthy sleep practices and lifestyle accommodations. We build optimal health and wellness solutions with primary healthcare providers and specialists. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Pregnancy and Sciatica: How Chiropractic Helped
References
Imtiyaz, S., Veqar, Z., & Shareef, M. Y. (2014). To Compare the Effect of Vibration Therapy and Massage in Prevention of Delayed Onset Muscle Soreness (DOMS). Journal of clinical and diagnostic research: JCDR, 8(1), 133–136. https://doi.org/10.7860/JCDR/2014/7294.3971
American Massage Therapy Association. (2011). Pregnancy Massage. https://www.amtamassage.org/publications/massage-therapy-journal/massage-and-pregnancy/
El-Hosary EA, Abbas Soliman HF, El-Homosy SM. (2016). Effect of Therapeutic Massage on Relieving Pregnancy Discomforts. IOSR Journal of Nursing and Health Science., 5(4), 57-64. https://doi.org/10.9790/1959-0504025764
Mueller, S. M., & Grunwald, M. (2021). Effects, Side Effects and Contraindications of Relaxation Massage during Pregnancy: A Systematic Review of Randomized Controlled Trials. Journal of Clinical Medicine, 10(16), 3485. https://doi.org/10.3390/jcm10163485
American Massage Therapy Association. (2018). Massage and pregnancy: A powerful combination. https://www.amtamassage.org/publications/massage-therapy-journal/massage-and-pregnancy-a-powerful-combination/
Sutham, K., Na-Nan, S., Paiboonsithiwong, S., Chaksuwat, P., & Tongsong, T. (2020). Leg massage during pregnancy with unrecognized deep vein thrombosis could be life-threatening: a case report. BMC pregnancy and childbirth, 20(1), 237. https://doi.org/10.1186/s12884-020-02924-w
Hospital for Special Surgery. Surgery, H. F. S. (2021). What you should know about using a massage gun. https://www.hss.edu/article_how-to-use-massage-gun.asp
Can non-surgical treatments help individuals with piriformis syndrome reduce referred sciatica pain and help restore hip mobility?
Piriformis Muscle & Piriformis Syndrome
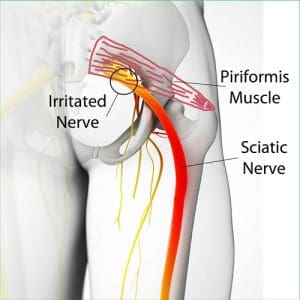
Within the lower extremities, various muscles, ligaments, tendons, and nerve roots allow the legs, hips, and thighs, enabling individuals to be mobile and help with good posture. One of the muscles, known as the piriformis muscle, is located in the gluteal region of the lower body, which helps the major muscles with every movement and allows the individual to walk, run, and rotate at the hips. (Chang et al., 2024) At the same time, the piriformis muscle is over the sciatic nerve, the longest and largest nerve that travels through the lower limbs down to the heel and provides motor-sensory function to the lower limbs. (Giuffre et al., 2024) Environmental factors like physical inactivity, excessive sitting or standing, lifting heavy objects, or improper posture can affect the piriformis muscle and develop musculoskeletal issues in the lower extremities. We associate with certified medical providers who inform our patients of the effects of piriformis syndrome, which affects their lower body extremities and causes pain and discomfort. While asking important questions to our associated medical providers, we advise patients to incorporate various non-surgical therapies to reduce the pain-like symptoms associated with piriformis syndrome. Dr. Alex Jimenez, D.C., envisions this information as an academic service. Disclaimer.
Have you experienced a pins and needles sensation in your hips and thighs that make it unbearable to walk? Do you feel radiating pain that travels down to your feet? Or have you noticed tightness in your hips and glutes region when stretching? When environmental factors impact the body, especially in the upper and lower extremities, they can cause overlapping risk profiles that can develop into chronic conditions. So, environmental factors affecting the piriformis muscle can lead to a musculoskeletal condition called piriformis syndrome. Piriformis syndrome is a somatic and neuropathic musculoskeletal condition caused by excessive or prolonged contraction of the piriformis muscle. (Jankovic et al., 2013) Many individuals who have dealt with piriformis syndrome will begin to report pain in the gluteal region that is causing sensations down the leg that can compress the sciatic nerve. (Hicks et al., 2024)
What Triggers Piriformis Syndrome?
Three causing factors can trigger piriformis syndrome in the lower extremities. Environmental factors like excessive movement, physical inactivity, or musculoskeletal conditions can compress the sciatic nerve over time, entrapping it and causing gradual pain. Additionally, trigger points in the muscles caused by repetitive strain can lead to muscle spasms or inflammation to irritate the sciatic nerve, which may present with a different musculoskeletal condition. (Pfeifer & Fitz, 1989) Finally, many people will begin to think that the pain they are experiencing is sciatica pain instead of piriformis syndrome.
Sciatica-Like Symptoms
Now, sciatica and piriformis syndrome are completely different but have similar symptoms that cause them to correlate. Sciatica is caused by spinal issues affecting the lower back that causes radiating pain down the leg. Piriformis syndrome only involves the piriformis muscle pressing one sciatic nerve area, causing overlapping risk profiles. Some of the common symptoms both sciatica and piriformis are associated with include:
Numbness
Tingling & burning sensations
Inflammation
Muscle spasms & tenderness
Pain & discomfort when sitting or standing
Sciatica: Causes, Symptoms, & Tips- Video
Non-Surgical Treatments For Piriformis
Luckily, numerous treatments are non-surgical and can help many individuals with piriformis syndrome find relief. Non-surgical treatments are affordable and non-invasive, customized to the person’s pain. With piriformis syndrome, non-surgical treatments can help improve pain and functionality back to the lower extremities and provide symptomatic relief from the piriformis muscle. (Vij et al., 2021) Some of the non-surgical treatments that are excellent for reducing pain-like symptoms associated with piriformis include:
Physical Therapy: Physical therapies allow the muscles to be mobilized and stretched and decompress the musculoskeletal structures. (Gandolfi et al., 2023)
Acupuncture: A trained acupuncturist incorporates small needles into the acupoints around the piriformis and provides anti-inflammatory effects. (He et al., 2023)
Chiropractic Adjustments: Chiropractors utilize mechanical and manual spinal manipulation to realign the body, stretch and strengthen the affected muscles, and alleviate pain.
Rest: Avoiding strenuous activities and sleeping on the right mattress can help reduce spinal pain associated with piriformis syndrome and improve sleep quality.
Incorporating these non-surgical treatments to reduce piriformis syndrome can help many individuals be more mindful of their bodies daily. They can be part of a daily routine in a person’s health and wellness journey in managing piriformis syndrome and reducing its pain-like symptoms. Doing so allows the lower extremities to be mobile again and the individual to be pain-free.
Gandolfi, M. G., Zamparini, F., Spinelli, A., & Prati, C. (2023). Asana for Back, Hips and Legs to Prevent Musculoskeletal Disorders among Dental Professionals: In-Office Yoga Protocol. J Funct Morphol Kinesiol, 9(1). https://doi.org/10.3390/jfmk9010006
Jankovic, D., Peng, P., & van Zundert, A. (2013). Brief review: piriformis syndrome: etiology, diagnosis, and management. Can J Anaesth, 60(10), 1003-1012. https://doi.org/10.1007/s12630-013-0009-5
Pfeifer, T., & Fitz, W. F. (1989). [The piriformis syndrome]. Z Orthop Ihre Grenzgeb, 127(6), 691-694. https://doi.org/10.1055/s-2008-1040313 (Das Piriformis-Syndrom.)
Vij, N., Kiernan, H., Bisht, R., Singleton, I., Cornett, E. M., Kaye, A. D., Imani, F., Varrassi, G., Pourbahri, M., Viswanath, O., & Urits, I. (2021). Surgical and Non-surgical Treatment Options for Piriformis Syndrome: A Literature Review. Anesth Pain Med, 11(1), e112825. https://doi.org/10.5812/aapm.112825
Sleeping with lower back pain and sciatica can be difficult and frustrating. What are ways to get more comfortable sleep?
Sleeping With Lower Back Pain and Sciatica
Various factors can affect sleeping with lower back pain and sciatica, including age, injury and medical history, the mattress (e.g., soft vs. firm mattress), and sleep positions. Unfortunately, there’s no one-cure-all solution for this problem, and depending on the underlying cause/s, they can worsen the pain and cause sleep problems. For example, if a herniated disc places added pressure on the nerves in the lower back, twisting the spine can worsen the lower back pain, and sleeping in a fetal position can exacerbate the nerve pain. (UCF Health, N.D.)
Lower-Back Pain
Low-back pain can be activity-related, intermittent, or constant. (American Association of Neurological Surgeons, 2024) For some, it only occurs occasionally, such as when performing specific movements. For others, it can be excruciating, chronic, and disabling. Low-back pain is unique for everybody and can differ depending on the cause. Some low-back pain symptom descriptions include (Förster M. et al., 2013)
Aching pain deep in the back
Shooting pain flare-ups
Pain caused by slight pressure
Burning
Tingling
Sciatica Not Present
For some, low-back pain may be confined to a specific area known as axial back pain. (Förster M. et al., 2013) The pain may be felt in a band along the lower back and does not radiate down the legs or anywhere else.
Sensory changes radiating down the leg – numbness, burning, and or tingling
Sleep Tools
Consider changing the mattress to improve sleeping with lower back pain and sciatica. For the best spinal support, choose a medium to firm mattress. Pillows, wedges, and other tools can also help improve sleep. (UCF Health, N.D.) It is recommended that individuals who sleep on their backs place a small pillow under their knees to reduce pressure on their lower backs. For those who sleep on their side, placing a pillow between the knees can keep the spine in a neutral/straight position. To relieve lower back pain, consider sleeping in a reclined, angled position with the head and shoulders higher than the hips. This can be accomplished with an adjustable bed or a wedge to prop the body in a regular bed.
Back Sleeping
Easing back pain while sleeping involves maintaining the body in a neutral or straight position. Extending the muscles, tendons, and ligaments too far in any one direction while sleeping with lower back pain and sciatica can cause stiffness, muscle spasms, and pain. Sleeping on the back puts the spine in neutral alignment with the least stress on the neck and back. It evenly distributes body weight to avoid exerting pressure on the joints and prevent backaches. In addition, a supine position allows outstretched ligaments to shrink and recover to their normal positions. (Keck Medicine of USC, 2019)
Chiropractic Assessment
Chiropractic care aims to help individuals improve movement with less pain due to condition, after injury, or surgery. A chiropractic physical therapy team may be best for individuals with acute back, neck, and musculoskeletal pain and discomfort symptoms. A chiropractor can quickly assess your condition and develop a customized treatment plan to expedite pain relief and improve mobility. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Sciatica, Causes, Symptoms and Tips
References
UCF Health. (N.D.). The best sleeping position for lower back pain (and the worst). https://ucfhealth.com/our-services/lifestyle-medicine/best-sleeping-position-for-lower-back-pain/
American Association of Neurological Surgeons. (2024). Low back pain. https://www.aans.org/patients/conditions-treatments/low-back-pain/
Förster, M., Mahn, F., Gockel, U., Brosz, M., Freynhagen, R., Tölle, T. R., & Baron, R. (2013). Axial low back pain: one painful area–many perceptions and mechanisms. PloS one, 8(7), e68273. https://doi.org/10.1371/journal.pone.0068273
North American Spine Society. (2020). Evidence-based clinical guidelines for multidisciplinary spine care: Diagnosis and treatment of low back pain. North American Spine Society. https://www.spine.org/Portals/0/assets/downloads/ResearchClinicalCare/Guidelines/LowBackPain.pdf
American Academy of Orthopaedic Surgeons. (2021). Sciatica. https://orthoinfo.aaos.org/en/diseases–conditions/sciatica
Keck Medicine of USC. (2019). The best -and worst – sleep positions for back pain. Keck Medicine of USC Blog. https://www.keckmedicine.org/blog/the-best-and-worst-sleep-positions-for-back-pain/
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine