Sciatica Relief for Teachers: El Paso Back Clinic’s Chiropractic Solutions
A teacher helping an elementary school girl using a tablet computer
Introduction: Supporting Teachers’ Health in El Paso
Teaching is a rewarding yet demanding profession, especially in vibrant communities like El Paso, Texas. Teachers spend long hours standing, sitting, and moving in ways that strain their bodies. These daily tasks can lead to sciatica, a painful condition caused by irritation of the sciatic nerve, which runs from the lower back down the legs. Symptoms like sharp leg pain, numbness, or tingling can disrupt lesson plans and classroom energy.
At El Paso Back Clinic®, led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, we understand the unique challenges educators face. Prolonged sitting during grading, standing for lessons, poor posture over desks, and the physical demands of managing classrooms increase sciatica risks. Our clinic specializes in chiropractic care, integrative medicine, and functional rehabilitation to help teachers manage pain and prevent flare-ups. Using manual adjustments, ergonomic advice, and targeted exercises, we aim to restore spinal health and enhance quality of life.
This article examines why teachers are prone to sciatica, how our clinic’s chiropractic and integrative approaches can provide relief, and offers practical steps for achieving lasting wellness. Drawing on Dr. Jimenez’s 30+ years of expertise, we’ll share clinical insights and real-world solutions tailored for El Paso’s educators.
What Is Sciatica and Why Does It Affect Teachers?
Sciatica occurs when the sciatic nerve, the body’s longest nerve, becomes compressed or irritated. This nerve starts in the lower spine, travels through the hips, and extends down each leg. Common symptoms include burning pain, tingling, or weakness in one leg, often worsening with sitting or standing. For teachers, this can mean discomfort during classes or while grading at home.
The teaching environment in El Paso schools, from bustling elementary classrooms to high school lecture halls, creates perfect conditions for sciatica. Standing for long periods during lessons or playground duty fatigues back muscles, pressing on spinal discs (Bomberg Chiropractic, 2023). Sitting at desks or in cramped staff rooms can shorten hip muscles, tilt the pelvis, and pinch the nerve (East Bay Chiropractic Office, 2023). Poor posture, like slouching over lesson plans, further irritates the nerve roots (Scoliosis Center of Utah, n.d.).
Dr. Jimenez sees this often at El Paso Back Clinic. His advanced neuromusculoskeletal imaging, such as X-rays and MRIs, pinpoints disc bulges or muscle imbalances that cause sciatica in teachers. By addressing these root causes, our clinic helps educators stay active without pain.
How Teachers’ Daily Routines Trigger Sciatica
Teachers’ days are a mix of physical and mental demands. Standing to deliver lessons or monitor halls strains the lower back, increasing nerve pressure (Boyne Ergonomics, n.d.). Sitting for hours on outdated chairs compresses the spinal discs, a key factor in triggering sciatica (Bomberg Chiropractic, 2023). Bending to assist students or lifting heavy teaching materials—such as projectors or book boxes—can strain the piriformis muscle, which is located near the sciatic nerve.
Poor posture is a major culprit. Leaning over desks or hunching at computers curves the spine unnaturally, squeezing nerve roots (Scoliosis Center of Utah, n.d.). Stress from managing classrooms or meeting tight deadlines can cause muscle tension, leading to inflammation (Paragon Chiropractic, n.d.). In El Paso, where teachers often juggle bilingual classes and extracurricular duties, these risks accumulate.
Dr. Jimenez’s clinic frequently treats educators with sciatica from these habits. His dual-scope approach—combining chiropractic exams with diagnostic imaging—reveals how daily tasks, such as carrying heavy bags, can lead to spinal misalignment. Our tailored treatments at El Paso Back Clinic, including adjustments and massage, address these issues directly, helping teachers move freely.
The Impact of Prolonged Sitting and Standing
Teachers switch between sitting and standing constantly—standing for morning assemblies, sitting for parent-teacher meetings, then standing again for labs. Prolonged sitting, especially on hard classroom chairs, increases disc pressure by up to 30%, irritating the sciatic nerve (Bomberg Chiropractic, 2023). Standing too long without breaks tightens hip flexors, pulling the spine out of alignment (Boyne Ergonomics, n.d.).
This back-and-forth strains stabilizing muscles, risking micro-tears in discs that pinch nerves. In El Paso’s active school settings, teachers may stand for over four hours daily, increasing the odds of back pain by 50% (Abundant Life Chiropractor, 2023). At El Paso Back Clinic, Dr. Jimenez utilizes advanced imaging to identify these strains, which are often seen in teachers following minor classroom injuries or slips. Our spinal decompression therapy gently stretches the spine, relieving nerve pressure and promoting healing.
Simple fixes can help: switch positions every 20 minutes, use cushioned mats for standing, or adjust your desk height to a comfortable level. These small changes, guided by our clinic’s ergonomic coaching, significantly reduce the risk of sciatica.
Poor Posture: A Hidden Cause of Nerve Pain
Posture shapes spinal health. Teachers often slouch over their desks or lean forward to engage students, curving their spines into a “C” shape. This compresses the lumbar vertebrae, irritating sciatic nerve roots (Scoliosis Center of Utah, n.d.). Low computer screens can cause neck craning, which can lead to lower back strain.
In El Paso classrooms, crouching to help young students or writing on low boards exacerbates this issue. Over time, uneven muscle pull misaligns the spine, trapping the nerve. At El Paso Back Clinic, Dr. Jimenez uses posture assessments to spot these habits early. His chiropractic adjustments realign the vertebrae, while acupuncture relaxes tight muscles, such as the piriformis, easing nerve pressure (Jimenez, n.d.a).
Posture tips: Keep your ears over your shoulders, use a lumbar-support chair, and raise screens to eye level. Our clinic offers workshops for El Paso teachers to build these habits, preventing chronic pain.
Physical Demands: The Active Side of Teaching
Teaching isn’t just standing or sitting—it’s dynamic. Lifting stacks of textbooks, bending to pick up dropped items, or dashing to manage recess chaos strains the back. These motions can herniate discs or inflame muscles near the sciatic nerve (East Bay Chiropractic Office, 2023). In El Paso, where teachers may handle heavy bilingual materials or sports equipment, risks grow.
Sudden twists, such as grabbing a falling projector, mimic sports injuries that Dr. Jimenez treats. His clinic documents these as work-related injuries for insurance purposes, utilizing massage and exercise to aid in tissue healing. Advanced imaging ensures an accurate diagnosis, detecting layered issues such as sprains and nerve compression (Jimenez, n.d.b).
Safe habits reduce risks: Lift with bent knees, use carts for supplies, and stretch before engaging in active duties. El Paso Back Clinic’s tailored plans help teachers stay strong and pain-free.
Chiropractic Care at El Paso Back Clinic: Targeted Relief
Chiropractic care is a cornerstone for sciatica relief. At El Paso Back Clinic, our manual adjustments realign the spine, reducing nerve irritation and inflammation (Active Health Center, n.d.). Teachers notice less leg pain and better mobility after sessions. Our spinal decompression therapy gently stretches the spine, retracting bulging discs that pinch nerves (Bomberg Chiropractic, 2023).
Dr. Jimenez’s expertise shines here. With over 30 years of experience treating patients in El Paso, including educators, Dr. [Last Name] combines chiropractic care with integrative methods, such as acupuncture, to provide natural pain relief. Advanced imaging ensures precise adjustments, targeting the exact cause of sciatica (Jimenez, n.d.a). Regular visits prevent flare-ups, letting teachers focus on students, not pain.
Restoring Spinal Alignment and Nerve Function
Adjustments are quick, targeted thrusts that realign vertebrae, freeing the sciatic nerve. This boosts blood flow and reduces inflammation, key for teachers battling daily strain (AFC Adherence, n.d.). At our clinic, Dr. Jimenez pairs adjustments with soft tissue work to release tight hips, a common issue among educators.
Our approach restores function holistically. Teachers regain flexibility for classroom tasks, and consistent care prevents future issues. Jimenez’s diagnostic tools, such as MRIs, ensure that treatments match each patient’s needs, offering El Paso educators reliable relief (Jimenez, n.d.b).
Reducing Inflammation Naturally
Inflammation fuels sciatica pain and swelling of the tissues around the nerve. Our adjustments improve spinal motion, reducing this swelling (Active Health Center, n.d.). We add ice or heat therapy to speed relief, tailored to each teacher’s symptoms.
Dr. Jimenez enhances this approach with nutrigenomics, recommending anti-inflammatory foods, such as salmon, to support the healing process. For El Paso teachers, this integrative approach means less pain and faster recovery from classroom strains (Jimenez, n.d.a).
Lifestyle Changes: Ergonomics and Exercises for Teachers
El Paso Back Clinic goes beyond adjustments, offering practical advice. Ergonomic tips include adjustable chairs, footrests, and raised monitors to reduce strain (Boyne Ergonomics, n.d.). For teachers, we recommend lumbar pillows and standing desks for grading.
Exercises are key: planks strengthen the core, and piriformis stretches loosen the hips (Alliance Orthopedics, n.d.). Dr. Jimenez designs home routines, such as knee-to-chest stretches, to accommodate busy schedules. Our massage therapy supports recovery, ensuring El Paso educators stay active.
Preventing Flare-Ups: Daily Habits for Long-Term Relief
Preventing sciatica means tracking triggers. Long sits or heavy lifts? Take breaks or use carts. Heat eases tight muscles; cold calms acute pain (Abundant Life Chiropractor, 2023). Weekly core workouts and posture apps help maintain proper alignment.
Dr. Jimenez’s clinic emphasizes prevention. Our exercise plans, paired with stress-reducing yoga, help teachers avoid chronic issues. Legal documentation supports work-injury claims, ensuring access to care (Jimenez, n.d.b).
Integrative Care: A Team Approach at El Paso Back Clinic
We combine chiropractic care with physical therapy, acupuncture, and massage to facilitate a comprehensive recovery. Physical therapy builds strength with moves like bridges (Active Health Center, n.d.). Acupuncture calms the nerves, making it ideal for reducing teachers’ stress (Jimenez, n.d.a). Short movement breaks, such as stretching during class, boost circulation.
Our clinic’s integrative model, led by Dr. Jimenez, treats sciatica holistically, addressing work or personal injuries with detailed records for insurance.
Dr. Alexander Jimenez’s Expertise: A Beacon for El Paso Teachers
Dr. Jimenez, with dual credentials as a chiropractor and nurse practitioner, brings unmatched care to El Paso. His clinic treats sciatica from classroom strains, sports injuries, or accidents, using imaging to diagnose precisely. Treatments such as adjustments, massage, and tailored exercises can help the body heal naturally, thereby preventing long-term issues.
For teachers, Jimenez’s legal documentation supports work claims, ensuring coverage. His functional medicine approach, including nutrition and acupuncture, empowers educators to thrive (Jimenez, n.d.a; Jimenez, n.d.b).
Practical Tips for El Paso Teachers
Morning Stretch: Try cat-cow (10 reps) to loosen the spine.
Classroom Ergonomics: Use lumbar-support chairs; raise boards to waist height.
Breaks: March in place every 30 minutes to ease nerve pressure.
Nutrition: Eat berries and fish to combat inflammation, according to Jimenez’s advice.
Conclusion: Empowering El Paso Educators
Sciatica doesn’t have to slow down El Paso’s teachers. At El Paso Back Clinic, Dr. Jimenez and our team offer chiropractic care, integrative therapies, and practical tips to relieve pain and prevent issues. From adjustments to ergonomic tweaks, we help educators stay healthy and focused on inspiring students.
Visit us at 11860 Vista Del Sol Dr, Suite 128, El Paso, TX, or call 915-850-0900 to start your pain-free journey.
Uncover important information on sciatica correlated with a herniated disc resulting from an auto accident and how to manage your symptoms.
Managing Sciatica Pain from Herniated Discs After Auto Accidents: A Comprehensive Guide to Chiropractic and Holistic Care
Sciatica pain resulting from herniated discs, particularly following an auto accident, can profoundly impact daily life, causing discomfort and limiting mobility. This condition, marked by radiating pain, numbness, or weakness along the sciatic nerve, is a frequent consequence of spinal injuries sustained in motor vehicle accidents (MVAs). Nonsurgical treatments such as chiropractic care, targeted exercises, massage therapy, acupuncture, and integrative medicine offer effective solutions to alleviate pain, promote healing, and prevent long-term complications. Drawing on clinical expertise and supported by peer-reviewed research, this comprehensive guide explores the causes, risk factors, and treatment options for sciatica associated with herniated discs. It emphasizes the role of patient-centered care, clear communication, and holistic approaches in supporting the body’s natural recovery processes.
Understanding Herniated Discs and Sciatica
What Is a Herniated Disc?
The spine is a complex structure composed of vertebrae, muscles, ligaments, and intervertebral discs that act as cushions between the vertebrae. Each disc consists of a tough outer layer, the annulus fibrosus, and a gel-like inner core, the nucleus pulposus (Nedresky et al., 2025). A herniated disc occurs when the nucleus pulposus protrudes through a tear in the annulus fibrosus, often due to trauma such as an MVA. This protrusion can compress nearby nerves, leading to pain, numbness, or weakness in the back, legs, or arms, depending on the herniation’s location (Stretanski et al., 2025).
MVAs are a leading cause of spinal injuries, contributing to over 40% of spinal complications annually (El Paso Back Clinic, 2016). The sudden, high-impact forces from a collision can strain or rupture the spinal discs, resulting in herniation and nerve irritation.
What Is Sciatica?
Sciatica is not a standalone condition but a set of symptoms caused by irritation or compression of the sciatic nerve, the body’s largest nerve, formed by nerve roots from L4 to S3 (Davis et al., 2025). It is characterized by radiating pain that travels from the lower back through the buttocks and down one or both legs, often accompanied by numbness, tingling, or weakness in the affected areas. Symptoms can range from mild to severe and are often exacerbated by movements such as bending, twisting, or coughing.
A common cause of sciatica is a herniated disc in the lumbar spine, particularly at the L4-L5 or L5-S1 levels, where the disc material compresses the sciatic nerve roots (Blamoutier, 2019). MVAs can trigger this condition by causing acute trauma to the spine, leading to disc herniation and subsequent nerve irritation.
Causes of Herniated Discs and Sciatica in Motor Vehicle Accidents
How MVAs Lead to Herniated Discs
The spine is designed to support the body’s weight and facilitate movement, but it is not built to withstand the intense forces of an MVA. The sudden jolt from a collision can cause various injuries to the spine, including:
Whiplash: The rapid back-and-forth motion of the neck and upper spine during a crash can strain the cervical and thoracic discs, potentially leading to herniation.
Direct Trauma: The force of impact can rupture the annulus fibrosus, allowing the nucleus pulposus to protrude and compress nearby nerves.
Facet Joint Damage: The facet joints, which connect the vertebrae, can be injured, contributing to spinal instability and increasing the risk of disc herniation (El Paso Back Clinic, 2016).
These injuries disrupt the spine’s structural integrity, making herniated discs a common outcome of MVAs, particularly in rear-end or high-speed collisions.
Factors Contributing to Herniated Discs and Sciatica
Several factors increase the likelihood of developing herniated discs and sciatica following an MVA:
Age: As individuals age, intervertebral discs lose water content, becoming less flexible and more prone to rupture. This risk increases significantly after age 30, as disc degeneration accelerates (Nosikova et al., 2012).
Obesity: Excess body weight places additional stress on the spine, increasing the risk of disc herniation, particularly in women with higher body mass indices (Sonntag, 2010).
Sedentary Lifestyle: Weak core and back muscles from lack of physical activity reduce spinal support, making discs more susceptible to injury during trauma.
Poor Posture: Chronic poor posture, such as slouching while driving, can exacerbate spinal stress during an accident.
Pre-existing Spinal Conditions: Conditions like degenerative disc disease or scoliosis heighten the risk of herniation following trauma (Hincapié et al., 2025).
Accident Severity: The intensity of the collision, including speed and angle, directly correlates with the likelihood and severity of spinal injuries.
Overlapping Risk Profiles of Herniated Discs and Sciatica
Herniated discs and sciatica share interconnected risk profiles due to their closely related pathophysiology. A herniated disc can directly cause sciatica by compressing the sciatic nerve roots, but additional factors amplify the risks and complications for both conditions:
Inflammatory Response: When a disc herniates, the nucleus pulposus releases proinflammatory cytokines, such as interleukin-1, interleukin-6, interleukin-8, and tumor necrosis factor-alpha, which irritate the surrounding nerves and exacerbate sciatica symptoms (Cosamalón-Gan et al., 2021). This inflammation can prolong pain and delay recovery.
Autoimmune Reaction: The nucleus pulposus is immunologically privileged, meaning it is typically shielded from the immune system. When exposed due to a herniation, it can trigger an autoimmune response, further increasing inflammation and nerve irritation (Cosamalón-Gan et al., 2021).
Neurological Complications: Severe disc herniation can lead to serious conditions like cauda equina syndrome, characterized by bowel or bladder dysfunction, requiring immediate surgical intervention (Tang et al., 2019).
Motor Dysfunction: Compression of the sciatic nerve or its roots can cause weakness in the hamstrings, calf muscles, or foot muscles, impairing mobility and increasing the risk of falls (Davis et al., 2025).
Chronic Pain Development: Untreated sciatica or herniated discs can contribute to chronic pain syndromes, such as fibromyalgia, due to prolonged nerve irritation and central sensitization (El Paso Back Clinic, 2016).
These overlapping risks underscore the need for early intervention to address both the mechanical and inflammatory components of sciatica and herniated discs, preventing long-term complications.
Clinical Rationale for Chiropractic Care in Managing Sciatica
Chiropractic care is a cornerstone of nonsurgical treatment for sciatica caused by herniated discs, offering a safe, effective, and evidence-based approach to pain relief and functional restoration. Experts in musculoskeletal health emphasize the importance of personalized, patient-centered care to address the root causes of sciatica and promote long-term healing. Below is the clinical rationale for why chiropractic care is effective for sciatica associated with herniated discs:
1. Restoring Spinal Alignment and Reducing Nerve Compression
Chiropractic adjustments, or spinal manipulations, aim to realign the spine, reducing pressure on compressed nerve roots. By correcting vertebral subluxations (misalignments), chiropractors alleviate nerve irritation and improve spinal mobility. For sciatica caused by herniated discs, techniques such as the flexion-distraction technique utilize specialized tables to gently stretch the spine, thereby moving the disc material away from the nerve root and reducing inflammation and pain (El Paso Back Clinic, 2016).
Clinical Evidence: A randomized controlled trial demonstrated that nonsurgical spinal decompression therapy, similar to flexion-distraction, significantly reduced leg pain and disability in patients with subacute lumbar disc herniation, with a 26.9% reduction in herniation volume compared to controls (Choi et al., 2022).
2. Mitigating Inflammation
The inflammatory response triggered by a herniated disc is a major contributor to sciatica pain. Chiropractic adjustments improve blood flow and stimulate the release of anti-inflammatory mediators, helping to reduce inflammation around the affected nerve. Manual therapies also disrupt the cycle of inflammation caused by proinflammatory cytokines (Cosamalón-Gan et al., 2021).
Expert Insight: Chiropractic care addresses both the mechanical and chemical aspects of sciatica, supporting the body’s natural anti-inflammatory processes to alleviate pain and promote healing.
3. Enhancing Spinal Mobility and Function
Herniated discs and sciatica often restrict spinal mobility, exacerbating pain and dysfunction. Chiropractic adjustments restore range of motion by mobilizing stiff joints and relaxing tense muscles, which is particularly beneficial after an MVA, where muscle spasms and joint stiffness can worsen symptoms.
Clinical Evidence: A systematic review found that spinal manipulative therapy significantly reduced pain and improved function in patients with low back pain and radiculopathy, supporting its use in sciatica management (Alrwaily et al., 2018).
4. Drug-Free Pain Management
Chiropractic care provides a non-pharmacological approach to pain relief, avoiding the risks associated with long-term medication use, such as opioid dependency or gastrointestinal side effects from nonsteroidal anti-inflammatory drugs (NSAIDs). By targeting the underlying cause of sciatica, chiropractic care offers sustainable pain relief.
Expert Approach: Chiropractic care combines spinal adjustments with patient education to empower individuals to manage their pain through lifestyle modifications, thereby reducing their reliance on medications.
5. Preventing Chronic Conditions
Untreated sciatica or herniated discs can lead to chronic pain, neurological deficits, or permanent nerve damage. Chiropractic care focuses on early intervention to prevent these complications by addressing the root cause and promoting natural healing processes.
Clinical Evidence: A meta-analysis revealed that discectomy offers short-term relief for sciatica but yields negligible long-term benefits compared to nonsurgical treatments, such as chiropractic care, which can be equally effective with fewer risks (Liu et al., 2023).
Holistic Approaches to Managing Sciatica Pain
In addition to chiropractic care, holistic approaches enhance recovery, reduce pain, and support the body’s natural healing processes. These methods address physical, emotional, and lifestyle factors to provide comprehensive care for sciatica and herniated discs.
1. Targeted Exercises and Physical Therapy
Therapeutic exercises strengthen the muscles supporting the spine, improve flexibility, and reduce pressure on the sciatic nerve. Programs combining strength training, agility exercises, and biomechanical assessments create personalized rehabilitation plans that optimize recovery (El Paso Back Clinic, 2016).
Recommended Exercises:
Piriformis Stretch: Targets the piriformis muscle, which can compress the sciatic nerve when tight (Hicks et al., 2023).
Cat-Cow Stretch: Enhances spinal flexibility and reduces lower back stiffness.
Core Strengthening: Exercises such as planks and bridges strengthen the abdominal and back muscles, providing better spinal support.
Hamstring Stretches: Reduces tension in the posterior chain, alleviating sciatic nerve irritation.
Clinical Evidence: A systematic review confirmed that targeted exercises and physical therapy significantly reduced pain and disability in patients with lumbar radiculopathy (Vanti et al., 2021).
2. Massage Therapy
Massage therapy relieves muscle tension, improves circulation, and reduces inflammation, all of which contribute to sciatica pain relief. Techniques like deep tissue massage and myofascial release target tight muscles and fascia that may compress the sciatic nerve (El Paso Back Clinic, n.d.).
Expert Insight: Massage therapy complements chiropractic adjustments by enhancing muscle relaxation and the effectiveness of spinal manipulations.
3. Acupuncture
Acupuncture involves inserting thin needles into specific points on the body to stimulate healing and reduce pain. It modulates pain signals and reduces inflammation, making it an effective adjunctive therapy for sciatica.
Clinical Evidence: A network meta-analysis found that acupuncture provided significant pain relief for lumbar disc herniation, comparable to other nonsurgical treatments (Huang et al., 2019).
4. Integrative Medicine
Integrative medicine combines conventional and alternative therapies to address the root causes of sciatica and promote overall wellness. Key components include:
Nutrition: An anti-inflammatory diet rich in omega-3 fatty acids, antioxidants, and whole foods can reduce systemic inflammation and support disc healing (Cosamalón-Gan et al., 2021).
Stress Management: Techniques such as mindfulness meditation and yoga help reduce muscle tension and improve pain tolerance, addressing the emotional aspects of chronic pain.
Weight Management: Maintaining a healthy weight helps reduce spinal stress, thereby lowering the risk of recurrent disc herniation.
Expert Approach: Integrative care combines chiropractic adjustments with nutritional counseling and stress reduction techniques to create a comprehensive treatment plan.
5. Postural Correction and Ergonomics
Poor posture and improper ergonomics can exacerbate sciatica symptoms, particularly after an MVA. Educating patients on proper posture and ergonomic adjustments reduces spinal stress (El Paso Back Clinic, 2016).
Practical Tips:
Use a chair with lumbar support to maintain the spine’s natural curve.
Take breaks every 30 minutes to stand and stretch, avoiding prolonged sitting.
Sleep on a medium-firm mattress with a pillow under the knees to reduce lower back strain.
Feeling Better Than Ever After a Semi-Truck Accident- Video Testimonial
The Importance of Clear Communication in Treatment Success
Clear communication between healthcare providers and patients is critical for successful outcomes in managing sciatica and herniated discs. Patient education empowers individuals to take an active role in their recovery (El Paso Back Clinic, n.d.).
Key Communication Strategies
Explaining the Diagnosis: Patients should understand that sciatica is a symptom of an underlying issue, such as a herniated disc, and that treatment targets the root cause.
Setting Realistic Expectations: Chiropractic care and holistic treatments require time and consistency. Patients should be informed about the expected timeline for pain relief and functional improvement.
Encouraging Active Participation: Patients who engage in prescribed exercises and lifestyle changes tend to have better outcomes.
Addressing Concerns: Open dialogue about risks, benefits, and alternative treatments builds trust and ensures patients feel confident in their care.
Clinical Evidence: Studies show that patient-centered communication improves adherence to treatment plans and enhances outcomes in musculoskeletal conditions (Alrwaily et al., 2018).
Preventing Long-Term Complications
Untreated sciatica or herniated discs can lead to chronic pain, neurological deficits, or permanent disability. Nonsurgical treatments like chiropractic care, targeted exercises, and holistic therapies help prevent these complications by:
Reducing Nerve Compression: Early intervention prevents prolonged nerve irritation, which could lead to permanent damage.
Promoting Tissue Healing: Therapies like spinal decompression and acupuncture enhance blood flow and nutrient delivery to the injured disc (Choi et al., 2022).
Strengthening Supporting Structures: Exercises strengthen muscles and ligaments around the spine, reducing the risk of recurrent injuries.
Addressing Inflammation: Integrative approaches, such as anti-inflammatory diets and acupuncture, help manage the inflammatory response, thereby preventing chronic pain syndromes (Cosamalón-Gan et al., 2021).
Expert Insight: Proactive, nonsurgical interventions are crucial in preventing long-term complications, allowing patients to return to normal activities more quickly and with greater resilience.
Case Study: A Patient’s Journey to Recovery
A patient involved in an MVA experienced sciatica symptoms due to a herniated disc. Initially struggling with pain and limited mobility, they underwent a comprehensive treatment plan including chiropractic adjustments, targeted exercises, and nutritional guidance. This integrative approach, combining spinal decompression, core strengthening, and an anti-inflammatory diet, resulted in significant pain relief and restored function, demonstrating the effectiveness of nonsurgical, patient-centered care (El Paso Back Clinic, 2016).
Conclusion
Sciatica pain caused by herniated discs from MVAs is a complex condition driven by mechanical, inflammatory, and neurological factors. Chiropractic care offers a clinically supported, nonsurgical solution to alleviate pain, restore function, and prevent long-term complications. By integrating targeted exercises, massage therapy, acupuncture, and holistic approaches like nutrition and stress management, patients can achieve lasting relief and support their body’s natural healing processes. Clear communication and patient education are crucial for ensuring adherence and achieving optimal outcomes. For those experiencing sciatica after an MVA, seeking nonsurgical care from qualified professionals can be a critical step toward recovery and improved quality of life.
References
Alrwaily, M., Almutiri, M., & Schneider, M. (2018). Assessment of variability in traction interventions for patients with low back pain: A systematic review. Chiropractic & Manual Therapies, 26(35). https://pubmed.ncbi.nlm.nih.gov/30237870/
Blamoutier, A. (2019). Nerve root compression by lumbar disc herniation: A French discovery? Orthopaedics & Traumatology: Surgery & Research, 105(2), 335–338. https://pubmed.ncbi.nlm.nih.gov/30799172/
Choi, E., Gil, H. Y., Ju, J., Han, W. K., Nahm, F. S., & Lee, P.-B. (2022). Effect of nonsurgical spinal decompression on intensity of pain and herniated disc volume in subacute lumbar herniated disc. International Journal of Clinical Practice, 2022, 6343837. https://pubmed.ncbi.nlm.nih.gov/36263240/
Cosamalón-Gan, I., Cosamalón-Gan, T., Mattos-Piaggio, G., Villar-Suárez, V., García-Cosamalón, J., & Vega-Álvarez, J. A. (2021). Inflammation in the intervertebral disc herniation. Neurocirugia (English Edition), 32(1), 21–35. https://pubmed.ncbi.nlm.nih.gov/32169419/
Hincapié, C. A., Kroismayr, D., Hofstetter, L., Kurmann, A., Cancelliere, C., Raja Rampersaud, Y., Boyle, E., Tomlinson, G. A., Jadad, A. R., Hartvigsen, J., Côté, P., & Cassidy, J. D. (2025). Incidence of and risk factors for lumbar disc herniation with radiculopathy in adults: A systematic review. European Spine Journal, 34(1), 263–294. https://pubmed.ncbi.nlm.nih.gov/39453541/
Huang, R., Meng, Z., Cao, Y., Yu, J., Wang, S., Luo, C., Yu, L., Xu, Y., Sun, Y., & Jiang, L. (2019). Nonsurgical medical treatment in the management of pain due to lumbar disc prolapse: A network meta-analysis. Seminars in Arthritis and Rheumatism, 49(2), 303–313. https://pubmed.ncbi.nlm.nih.gov/30940466/
Liu, C., Ferreira, G. E., Abdel Shaheed, C., Chen, Q., Harris, I. A., Bailey, C. S., Peul, W. C., Koes, B., & Lin, C.-W. C. (2023). Surgical versus non-surgical treatment for sciatica: Systematic review and meta-analysis of randomised controlled trials. BMJ, 381, e070730. https://pubmed.ncbi.nlm.nih.gov/37076169/
Nosikova, Y. S., Santerre, J. P., Grynpas, M., Gibson, G., & Kandel, R. A. (2012). Characterization of the annulus fibrosus-vertebral body interface: Identification of new structural features. Journal of Anatomy, 221(6), 577–589. https://pubmed.ncbi.nlm.nih.gov/22747710/
Sciatic Nerve Health at El Paso Back Clinic: Holistic Healing Solutions
The sciatic nerve is essential for movement and sensation, stretching from the lower back through the legs as the body’s largest nerve. When irritated or compressed, it can cause sciatica—sharp pain, numbness, or tingling that radiates down the leg. At El Paso Back Clinic® in El Paso, TX, we specialize in helping patients overcome sciatic nerve issues through expert chiropractic care and integrative therapies.
This article explores the sciatic nerve’s structure, made of axon bundles wrapped in protective connective tissue, and how El Paso Back Clinic’s chiropractic techniques relieve nerve pressure. We’ll also highlight our integrative approach, combining massage, physical therapy, acupuncture, and nutrition to promote natural healing. Led by Dr. Alexander Jimenez, DC, APRN, FNP-C, our clinic addresses injuries from work, sports, personal accidents, and motor vehicle accidents (MVAs) with personalized, evidence-based care.
Whether you’re managing sciatica or aiming to prevent nerve problems, El Paso Back Clinic offers solutions to help you regain mobility and live pain-free.
Understanding the Sciatic Nerve
The sciatic nerve originates from the L4 to S3 nerve roots in the lower back, runs through the buttocks, and extends down each leg, controlling muscles and sending sensations from the thighs, calves, and feet. Compression from a herniated disk, tight muscles, or injury can trigger sciatica, disrupting daily activities like walking or sitting.
At El Paso Back Clinic, we focus on addressing the root causes of sciatica using non-invasive methods to support the body’s natural healing process, helping patients return to an active lifestyle.
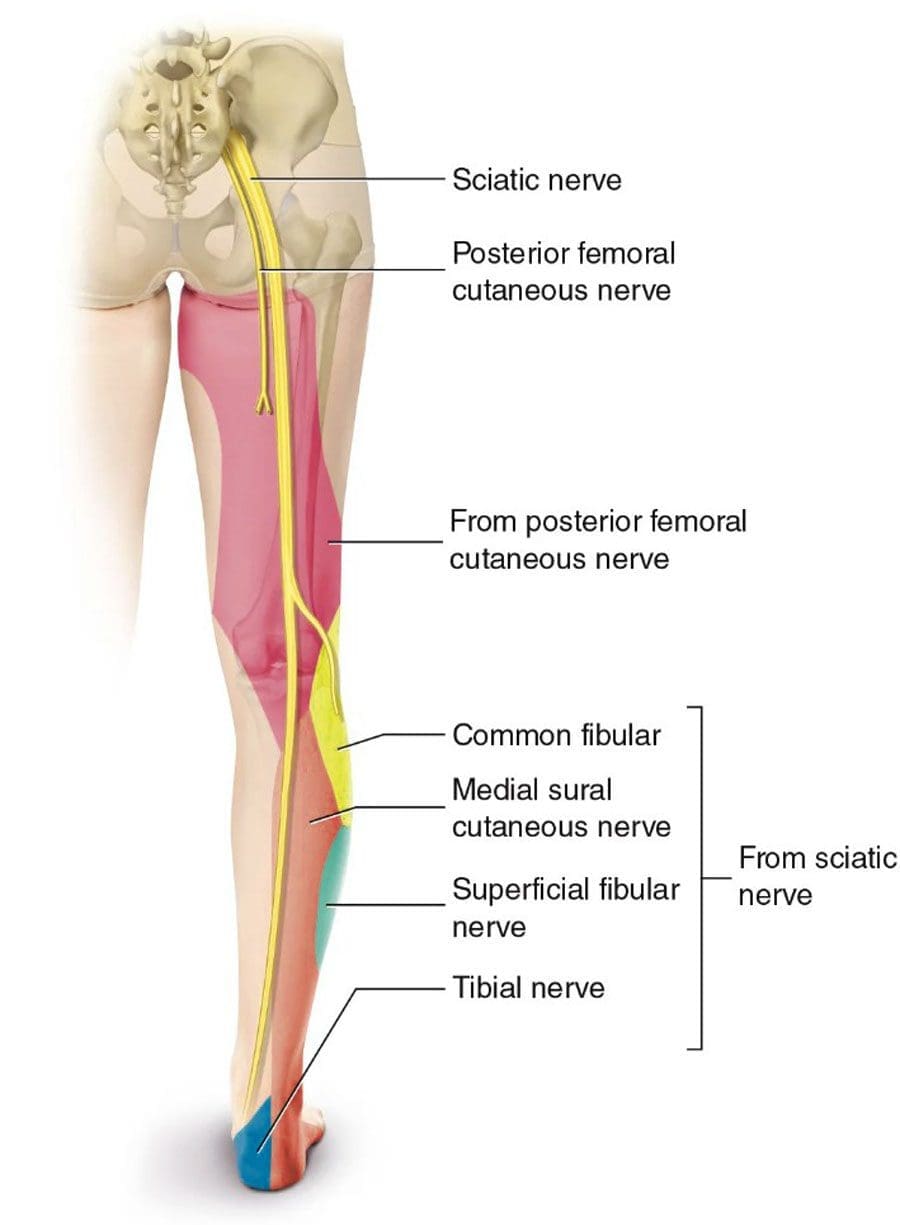
Sciatic Nerve Structure: Axons and Protective Layers
The sciatic nerve is a complex network of neurons, each with a long fiber called an axon that transmits electrical signals. These axons are organized into bundles called fascicles, supported by layers of connective tissue:
Endoneurium: Wraps each axon and its myelin sheath, which speeds up signals and protects the nerve fiber.
Perineurium: Encases each fascicle, regulating the environment to maintain signal efficiency.
Epineurium: The outer layer surrounds the entire nerve, providing strength and flexibility.
These layers, which can comprise up to half of the nerve’s volume, ensure durability but can cause issues if they become inflamed or scarred, trapping axons and triggering pain. El Paso Back Clinic’s treatments aim to reduce inflammation and restore nerve function.
Causes of Sciatic Nerve Issues
Sciatica often results from nerve compression due to:
Herniated disks: Bulging spinal disks pressing on nerve roots.
Spinal stenosis: Narrowed spinal canals crowd the nerves.
Piriformis syndrome: A Tight piriformis muscle pinching the nerve.
Injuries: Trauma from work, sports, falls, or MVAs.
Our clinic sees these issues in patients with repetitive job strains, athletic injuries, or car accidents. Accurate diagnosis is key to effective treatment.
Chiropractic Care at El Paso Back Clinic: Relieving Nerve Pressure
Chiropractic care is at the heart of our approach at El Paso Back Clinic. Dr. Alexander Jimenez and our team use precise spinal adjustments to realign vertebrae and reduce pressure on the sciatic nerve. The procedure alleviates pain and improves mobility by addressing misalignments that cause disc bulging or muscle tension.
For example, a patient with sciatica from a slipped disk may receive lumbar adjustments to create space for the nerve. Dr. Jimenez uses advanced imaging like X-rays and MRIs to identify the issue, ensuring targeted care. His dual expertise as a chiropractor and nurse practitioner allows for comprehensive assessments, combining spinal exams with neurological testing.
Research supports the effectiveness of chiropractic care for chronic pain over medications alone (Ideal Spine, n.d.). For a delivery driver with sciatica from heavy lifting, Dr. Jimenez might use spinal decompression to gently stretch the spine, paired with rehab exercises to prevent recurrence.
Integrative Care: A Holistic Approach to Nerve Health
El Paso Back Clinic embraces integrative medicine, combining chiropractic care with massage therapy, physical therapy, acupuncture, and nutrition for optimal results. Our team, including chiropractors, therapists, and nutritionists, collaborates to create personalized treatment plans.
Massage Therapy: Techniques like deep tissue and trigger point massage relax tight muscles, such as the piriformis, reducing nerve compression. Patients often report less numbness and better movement.
Physical Therapy: Exercises like the McKenzie method or core strengthening stabilize the spine and improve flexibility, guided by our skilled therapists.
Acupuncture: Needle placements reduce inflammation and stimulate the body’s natural pain relief mechanisms, thereby enhancing chiropractic outcomes.
Nutrition Counseling: We recommend nerve-supporting nutrients like vitamin B12 (found in fish and eggs) for myelin repair and alpha-lipoic acid (in spinach) to reduce inflammation (RxWellness, n.d.; Verywell Health, n.d.).
This approach aligns with evidence-based principles of integrative care (NCCIH, n.d.), promoting healing while minimizing reliance on medications.
Dr. Jimenez’s Expertise: Healing Diverse Injuries
With over 25 years of experience, Dr. Alexander Jimenez leads El Paso Back Clinic with a dual perspective as a DC and APRN. His clinic uses advanced tools like EMG, MRI, and functional assessments to diagnose sciatica and related injuries.
Work Injuries: For a construction worker with sciatica from repetitive bending, Dr. Jimenez combines adjustments with B-vitamin supplements and ergonomic advice to prevent further strain.
Sports Injuries: A soccer player experiencing leg pain receives decompression therapy and acupuncture, supplemented by balance exercises to help restore function.
Personal Injuries: A fall victim benefits from massage and PT to reduce swelling, with detailed documentation for insurance claims.
MVAs: Car accident patients get full-body scans to connect whiplash to sciatica, with legal reports to support recovery and claims.
Dr. Jimenez’s approach, detailed on dralexjimenez.com, focuses on root-cause treatment and patient empowerment through holistic care.
Supporting Legal and Medical Needs
Injury cases often require legal or insurance documentation to support claims. El Paso Back Clinic provides thorough records, from initial X-rays to recovery progress, using pain scales and range-of-motion tests. For MVA patients, we collaborate with attorneys to streamline paperwork, ensuring patients focus on healing.
Preventing Long-Term Nerve Issues
Our integrative care promotes natural healing by improving blood flow to axons, strengthening supporting muscles, and reducing inflammation through nutrition. Regular checkups and personalized therapy goals help prevent chronic pain or arthritis, keeping patients active.
Choose El Paso Back Clinic for Sciatic Nerve Care
Located in El Paso, TX, El Paso Back Clinic® offers a welcoming environment where licensed professionals deliver tailored care. Our services—chiropractic, physical therapy, acupuncture, and nutrition—work together to relieve sciatica and boost wellness. Contact us at 915-850-0900 or visit our blog for more insights.
With El Paso Back Clinic, you’re investing in a healthier, pain-free future.
Holistic Wellness at El Paso Back Clinic: Premier Chiropractic Care
Welcome to El Paso Back Clinic, your trusted destination for injury rehabilitation and functional medicine in El Paso, TX. Led by Dr. Alex Jimenez, D.C., APRN, FNP-BC, our clinic specializes in treating sciatica, neck and back pain, whiplash, headaches, joint injuries, sports injuries, and degenerative arthritis. Our team of chiropractors, nurse practitioners, nutritionists, and acupuncturists uses advanced therapies to restore mobility, flexibility, and overall health. We focus on holistic sciatic nerve care, addressing root causes through chiropractic care, nutrition, and integrative medicine to help you achieve optimal wellness.
Comprehensive Chiropractic Care for Musculoskeletal Health
At El Paso Back Clinic, we provide a holistic approach to managing musculoskeletal issues, including sciatica, back pain, and joint injuries. Our treatments focus on restoring biomechanical function and promoting natural healing, helping patients regain their quality of life.
Chiropractic Techniques for Joint and Biomechanical Restoration
Chiropractic care is central to our approach, using gentle spinal adjustments to correct misalignments that cause nerve compression, such as sciatica. These adjustments relieve pressure on the sciatic nerve, improve mobility, and reduce pain (Dr. Leitman, 2023). By restoring proper alignment, we help the body heal naturally, whether the issue stems from a car accident, sports injury, or chronic condition.
Managing Musculoskeletal Inflammation
Inflammation often contributes to sciatica and other musculoskeletal pain. Our clinic utilizes functional medicine to address inflammation through dietary modifications, such as incorporating anti-inflammatory foods like omega-3 fatty acids, and targeted supplements like vitamin B12 (Therapy Organics, 2023). This approach reduces nerve irritation and supports long-term health.
Trigger Point and Massage Therapy
Massage therapy, including trigger point techniques, enhances circulation and relaxes tense muscles, which is crucial for sciatica relief. Improved blood flow delivers nutrients to the sciatic nerve, aiding recovery (Zama Massage, 2018). Our therapists tailor sessions to address specific injuries, from whiplash to sports-related strains.
Recovery and Rehabilitation After Motor Vehicle Accidents
Motor vehicle accidents (MVAs) can cause a range of injuries, from whiplash to gastrointestinal issues, impacting overall health. At El Paso Back Clinic, we offer comprehensive recovery plans tailored to each patient’s needs.
Whiplash and Spinal Injury Recovery
Whiplash-associated disorders (WAD) are common after MVAs, causing neck pain and stiffness. Our chiropractic care and durable medical equipment, such as cervical collars, support recovery by stabilizing the spine and reducing strain (Jimenez, 2023a). We also incorporate regenerative medicine, like platelet-rich plasma (PRP), to promote tissue repair (Family Integrative Medicine, 2023).
Gastrointestinal Injuries Post-Accident
MVAs can lead to gastrointestinal issues due to trauma or stress. Our integrative approach includes nutritional guidance to support gut health, emphasizing foods that reduce inflammation and promote healing (Asuta Health, 2023). This holistic care helps patients recover fully from internal injuries.
Nutrition for Injury Recovery
A tailored diet is vital for healing after an MVA. We recommend nutrient-dense foods and supplements to support tissue repair and reduce inflammation, aiding recovery from musculoskeletal and spinal injuries (Therapy Organics, 2023). Our nutritionists work with patients to create personalized plans.
Sciatica, characterized by pain radiating from the lower back through the buttocks and legs, is often caused by compression of the sciatic nerve. At El Paso Back Clinic, we address sciatica and other injuries with a focus on prevention and long-term wellness.
Sciatica Symptoms and Causes
Symptoms: Pain ranging from mild to severe, numbness, tingling, or muscle weakness in the leg or foot. Pain may worsen with activities such as sitting, coughing, or sneezing (WebMD, 2023a).
Causes: Herniated discs, bone spurs, or spinal misalignments (subluxations) due to poor posture, trauma, or pregnancy. Rarely, tumors or diabetes may contribute (Wilmington Chiropractic, 2023).
Risk Factors: Age-related spinal changes, obesity, sedentary lifestyles, occupations involving heavy lifting or prolonged driving, and diabetes increase the risk of sciatica.
Bicycle and 18-Wheeler Accident Risks
Bicycle collisions and 18-wheeler accidents pose significant risks for musculoskeletal injuries. Wet roads or heavy vehicles can exacerbate these risks, leading to spinal trauma or sciatica (National Center for Biotechnology Information, 2016). Our clinic uses chiropractic care and integrative medicine to address these injuries, promoting recovery and preventing recurrence.
Dr. Alex Jimenez’s Expertise in Diagnosis and Treatment
Dr. Alex Jimenez brings a unique dual perspective as a chiropractor and nurse practitioner, specializing in work, sports, personal, and motor vehicle injuries. His expertise ensures precise diagnoses and effective treatment plans.
Diagnostic Approach
Dr. Jimenez conducts thorough medical exams, using advanced imaging like X-rays and MRIs to identify issues such as herniated discs or nerve compression. Functional health assessments further reveal lifestyle factors that contribute to sciatica or other injuries (Jimenez, 2023b). This comprehensive approach ensures targeted treatments.
Medical and Legal Support
For personal injury cases, Dr. Jimenez provides detailed medical reports that support insurance claims or legal proceedings, easing the burden on patients. His dual qualifications allow him to seamlessly integrate medical care with legal documentation, particularly for MVA-related injuries (Jimenez, 2023c).
Preventing sciatica and other injuries requires proactive measures. Our clinic emphasizes sustainable strategies to maintain spinal health and overall wellness.
Prevention Strategies
Core Strengthening: Exercises targeting the abdomen and lower back support proper posture and spinal alignment (Thrive Cedar Falls, 2023).
Proper Posture: Use ergonomic chairs with lumbar support and maintain a level position with your knees and hips when sitting. A rolled towel can support the spine’s natural curve.
Body Mechanics: Lift with your legs, keep your back straight, and avoid twisting while lifting heavy objects.
An Active Lifestyle: Regular physical activity, such as walking or yoga, reduces the risk of sciatica compared to a sedentary lifestyle.
When to Seek Care
Seek immediate medical attention if you experience:
Severe pain with numbness or weakness in the leg.
Loss of bowel or bladder control.
Pain following a significant injury, such as an MVA.
Mild sciatica may resolve with self-care, but persistent or worsening pain requires professional intervention.
Our clinic combines advanced technology, proven therapies, and a patient-centered approach to deliver exceptional care. Dr. Jimenez’s expertise in chiropractic and integrative medicine ensures comprehensive treatment for sciatica, sports injuries, and MVA-related conditions. We prioritize natural healing and long-term wellness, helping patients return to their active lives.
Discover effective chiropractic care options for sports injuries & sciatica to support your healing journey.
Sciatica Pain and Sports Injuries: A Comprehensive Guide to Chiropractic Care and Recovery
Introduction: The Sciatica Struggle and the Sports Connection
Imagine this: you’re sprinting down the soccer field, weaving through defenders like a pro, when suddenly a sharp, electric jolt shoots down your leg. Or maybe you’re just sitting at your desk, minding your own business, and a nagging pain in your lower back decides to throw a party that radiates all the way to your toes. Welcome to the world of sciatica—a condition that can make even the toughest athletes feel like they’ve been tackled by an invisible linebacker. Sciatica isn’t just a pain in the… well, you know where. It’s a complex musculoskeletal issue that can stem from various causes, including sports injuries, and it affects millions of people worldwide.
At El Paso Back Clinic, led by the esteemed Dr. Alexander Jimenez, DC, APRN, FNP-BC, patients find hope through advanced chiropractic care and integrative treatments tailored to alleviate sciatica pain and restore mobility. Whether you’re an athlete sidelined by a sports injury or someone dealing with the aftermath of a car accident, understanding sciatica and its connection to the musculoskeletal system is key to recovery. In this comprehensive guide, we’ll dive into the causes of sciatica, explore how sports injuries contribute to it, and highlight how chiropractic care, combined with non-surgical treatments, can help you get back on your feet. Plus, we’ll sprinkle in a bit of humor to keep things light—because nobody likes a blog post that’s as stiff as a bad back!
What Is Sciatica? Understanding the Basics
Sciatica isn’t just one thing—it’s a symptom of an underlying issue affecting the sciatic nerve, the longest nerve in your body, which runs from your lower back through your hips, buttocks, and down each leg. When this nerve gets irritated or compressed, it can cause pain, numbness, tingling, or weakness that radiates along its path. Think of it like a garden hose with a kink: the water (or in this case, nerve signals) can’t flow properly, and the result is discomfort that can range from mildly annoying to downright debilitating.
Common Symptoms of Sciatica
Pain: A sharp, burning, or aching sensation that starts in the lower back or buttocks and travels down one leg.
Numbness or Tingling: That “pins and needles” feeling, like your leg fell asleep but decided to stay that way.
Weakness: Difficulty moving your leg or foot, making you feel like you’re auditioning for a role as a wobbly penguin.
One-Sided Symptoms: Sciatica typically affects only one side of the body, though it can occasionally be bilateral (both sides).
Causes of Sciatica
Sciatica can be triggered by various conditions, many of which involve the musculoskeletal system. Some of the most common culprits include:
Lumbar Disc Herniation: When the soft inner material of a spinal disc bulges or ruptures, it can press on the sciatic nerve roots (Wang et al., 2022).
Piriformis Syndrome: The piriformis muscle in the buttocks can irritate the sciatic nerve if it becomes tight or inflamed (Hicks et al., 2021).
Spinal Stenosis: Narrowing of the spinal canal can compress nerve roots, leading to sciatica symptoms.
Degenerative Arthritis: Wear and tear on the spine can cause bone spurs or disc degeneration, irritating the nerve.
Trauma or Injury: Sports injuries, car accidents, or even a bad fall can damage the spine or surrounding tissues, contributing to sciatica (El Paso Back Clinic, n.d.).
Hicks, B. L., Lam, J. C., & Varacallo, M. (2021). Piriformis syndrome: A cause of nondiscogenic sciatica. Current Sports Medicine Reports, 20(2), 97–102. https://pubmed.ncbi.nlm.nih.gov/33560090/
Wang, Y., Chen, J., & Chen, L. (2022). Association between chiropractic spinal manipulation and lumbar discectomy in adults with lumbar disc herniation and radiculopathy: Retrospective cohort study using United States’ data. BMJ Open, 12(12), e068262. https://pubmed.ncbi.nlm.nih.gov/36523295/
The Musculoskeletal System and Sciatica: A Complex Relationship
The musculoskeletal system—your bones, muscles, ligaments, and tendons—works together like a well-oiled machine to keep you moving. But when one part of this system gets out of whack, it can throw everything off balance, including the sciatic nerve. Let’s break down how the musculoskeletal system plays a role in sciatica and why sports injuries can be a major contributing factor.
How the Musculoskeletal System Contributes to Sciatica
The sciatic nerve is surrounded by muscles, bones, and connective tissues, all of which can influence its function. Here’s how:
Spinal Misalignment: When vertebrae in the lumbar spine are misaligned, they can compress nerve roots, leading to sciatica. This is often seen in conditions like spondylolisthesis, where one vertebra slips over another.
Muscle Imbalances: Tight or weak muscles, such as the piriformis or hamstrings, can put pressure on the sciatic nerve or alter spinal alignment.
Joint Dysfunction: Stiff or hypermobile joints in the spine or pelvis can disrupt normal biomechanics, irritating the nerve.
Inflammation: Injuries or overuse can cause inflammation in surrounding tissues, which can compress or irritate the sciatic nerve (Jensen et al., 2023).
Sports Injuries and Sciatica: The Connection
Athletes, whether weekend warriors or seasoned pros, are no strangers to musculoskeletal injuries. Sports like football, soccer, running, or even yoga can put significant stress on the body, leading to injuries that may trigger or exacerbate sciatica. Here’s how sports injuries can contribute:
Direct Trauma: A hard tackle in football or a fall during a basketball game can cause pelvic fractures or spinal injuries, which may compress the sciatic nerve (El Paso Back Clinic, n.d.).
Overuse Injuries: Repetitive motions, like running or cycling, can lead to muscle tightness or inflammation, such as piriformis syndrome, which irritates the sciatic nerve (Hicks et al., 2021).
Poor Biomechanics: Improper form during weightlifting or running can strain the spine or pelvis, leading to disc herniation or misalignment.
Pelvic Injuries: A broken pelvis, as discussed in El Paso Back Clinic’s article, can directly affect the sciatic nerve due to its proximity to the nerve’s path (El Paso Back Clinic, n.d.).
For example, imagine a runner who pushes through a tight hamstring without stretching properly. Over time, this tightness can pull on the pelvis, misalign the spine, and irritate the sciatic nerve. Or picture a soccer player who takes a hard fall, bruising their lower back and causing inflammation that pinches the nerve. These scenarios highlight how sports injuries can set the stage for sciatica.
Hicks, B. L., Lam, J. C., & Varacallo, M. (2021). Piriformis syndrome: A cause of nondiscogenic sciatica. Current Sports Medicine Reports, 20(2), 97–102. https://pubmed.ncbi.nlm.nih.gov/33560090/
Jensen, R. K., Kongsted, A., Kjaer, P., & Koes, B. (2023). Surgical versus non-surgical treatment for sciatica: Systematic review and meta-analysis of randomised controlled trials. BMJ, 381, e070730. https://pubmed.ncbi.nlm.nih.gov/37019468/
Sports Injury Rehabilitation- Video
Risk Factors for Sciatica: Why Athletes Are at Risk
Sciatica doesn’t discriminate—it can affect anyone, from desk jockeys to elite athletes. However, certain factors increase the likelihood of developing sciatica, particularly in those who engage in sports. Let’s explore these risk factors and why athletes might be more susceptible.
Key Risk Factors
Obesity: Excess weight puts extra pressure on the spine, increasing the risk of disc herniation and sciatica (Cao et al., 2021).
Sedentary Lifestyle: Prolonged sitting or inactivity weakens core muscles, leading to poor spinal support and nerve compression.
Age: As we age, degenerative changes in the spine, like arthritis or disc wear, become more common, increasing sciatica risk.
Occupational Hazards: Jobs or activities involving heavy lifting, twisting, or prolonged sitting can strain the spine.
Sports Injuries: High-impact or repetitive sports activities can cause trauma or overuse injuries, leading to sciatica (El Paso Back Clinic, n.d.).
Poor Posture: Slouching or improper body mechanics during sports or daily activities can misalign the spine, irritating the sciatic nerve.
Why Athletes Are Vulnerable
Athletes often push their bodies to the limit, which can lead to musculoskeletal issues that trigger sciatica. For instance:
High-Impact Sports: Football, rugby, or gymnastics involve jarring movements that can stress the spine or pelvis.
Repetitive Motions: Runners or cyclists may develop muscle imbalances or overuse injuries that affect the sciatic nerve.
Inadequate Recovery: Skipping rest days or neglecting proper warm-ups and cool-downs can lead to chronic inflammation or injury.
Improper Equipment: Worn-out running shoes or an ill-fitting bike saddle can alter biomechanics, contributing to sciatica.
Think of an athlete’s body like a finely tuned race car: it performs beautifully until a single misaligned part causes the whole system to sputter. That’s where chiropractic care comes in to realign the wheels and get you back on the track.
References
Cao, H., Zhang, Z., & Lu, T. (2021). Causal associations of obesity with the intervertebral degeneration, low back pain, and sciatica: A two-sample Mendelian randomization study. Frontiers in Endocrinology, 12, 740746. https://pubmed.ncbi.nlm.nih.gov/34956081/
Chiropractic Care: A Non-Surgical Solution for Sciatica
Chiropractic care is like the superhero of non-surgical treatments for sciatica—it swoops in to save the day without the need for scalpels or long recovery times. At El Paso Back Clinic, Dr. Alexander Jimenez and his team use a variety of chiropractic techniques to address the root causes of sciatica, helping patients regain mobility and reduce pain.
How Chiropractic Care Helps
Chiropractic care focuses on restoring proper alignment and function to the musculoskeletal system, which can alleviate pressure on the sciatic nerve. Here’s how it works:
Spinal Adjustments: Gentle manipulations correct misalignments in the spine, reducing nerve compression and improving biomechanics (Wang et al., 2022).
Soft Tissue Therapy: Techniques like myofascial release or trigger point therapy relax tight muscles, such as the piriformis, that may be irritating the nerve (Hicks et al., 2021).
Joint Mobilization: Restoring mobility to stiff joints in the spine or pelvis can reduce strain on the sciatic nerve.
Postural Correction: Chiropractors assess and correct posture issues that contribute to sciatica, ensuring long-term relief.
Benefits of Chiropractic Care for Sciatica
Pain Reduction: By addressing the root cause, chiropractic care can significantly reduce sciatica pain without relying on medications.
Improved Mobility: Restoring joint and muscle function helps patients move more freely, whether they’re athletes or office workers.
Non-Invasive: Unlike surgery, chiropractic care avoids the risks and recovery time associated with invasive procedures (Jensen et al., 2023).
Holistic Approach: Chiropractors often combine adjustments with lifestyle advice, exercises, and nutrition to support overall health.
Dr. Jimenez’s approach at El Paso Back Clinic is particularly effective because it integrates advanced diagnostic tools, like imaging and biomechanical assessments, to pinpoint the exact cause of sciatica. This precision ensures that treatments are tailored to each patient’s unique needs, whether their sciatica stems from a sports injury, a car accident, or a broken pelvis.
References
Hicks, B. L., Lam, J. C., & Varacallo, M. (2021). Piriformis syndrome: A cause of nondiscogenic sciatica. Current Sports Medicine Reports, 20(2), 97–102. https://pubmed.ncbi.nlm.nih.gov/33560090/
Jensen, R. K., Kongsted, A., Kjaer, P., & Koes, B. (2023). Surgical versus non-surgical treatment for sciatica: Systematic review and meta-analysis of randomised controlled trials. BMJ, 381, e070730. https://pubmed.ncbi.nlm.nih.gov/37019468/
Wang, Y., Chen, J., & Chen, L. (2022). Association between chiropractic spinal manipulation and lumbar discectomy in adults with lumbar disc herniation and radiculopathy: Retrospective cohort study using United States’ data. BMJ Open, 12(12), e068262. https://pubmed.ncbi.nlm.nih.gov/36523295/
Integrative Non-Surgical Treatments for Sciatica
While chiropractic care is a cornerstone of sciatica treatment, combining it with other non-surgical therapies can enhance outcomes, especially for athletes recovering from sports injuries. Dr. Jimenez and his team at El Paso Back Clinic incorporate a variety of integrative approaches to address sciatica and its overlapping symptoms.
Complementary Therapies
Acupuncture: This ancient practice involves inserting thin needles into specific points to reduce pain and inflammation. Studies show acupuncture can be effective for sciatica, particularly when tailored to neuropathic pain mechanisms (Li et al., 2020; Zhang et al., 2019).
Massage Therapy: Therapeutic massage can relax tight muscles, improve circulation, and reduce inflammation, complementing chiropractic adjustments.
Nutritional Support: A diet rich in anti-inflammatory foods, like omega-3s and antioxidants, can support recovery by reducing systemic inflammation (El Paso Back Clinic, n.d.).
Durable Medical Equipment: Braces or supports can stabilize the spine or pelvis during recovery, especially after injuries like a broken pelvis.
Acupuncture for Sciatica: A Closer Look
Acupuncture deserves a special mention because of its growing evidence base. Research suggests that acupuncture can modulate pain pathways and reduce inflammation, making it a valuable tool for sciatica management. For example, a randomized controlled pilot study found that acupuncture provided significant pain relief for sciatica patients, with effects varying based on the “dose” of treatment (Zhang et al., 2019). By combining acupuncture with chiropractic care, patients can address both the structural and neurological components of sciatica.
The Role of Nutrition
Nutrition plays a critical role in musculoskeletal recovery. After a sports injury or accident, inflammation can exacerbate sciatica symptoms. Dr. Jimenez emphasizes a diet that includes:
Anti-Inflammatory Foods: Fish, nuts, leafy greens, and berries to reduce inflammation.
Hydration: Proper fluid intake to support tissue repair and disc health.
Supplements: Omega-3 fatty acids or turmeric may help manage inflammation, though patients should consult a professional before starting supplements.
By integrating these therapies, El Paso Back Clinic creates a comprehensive treatment plan that addresses the multifaceted nature of sciatica, helping patients recover faster and more effectively.
Li, Q., Liu, R., & Zhao, J. (2020). The management of sciatica by acupuncture: An expert consensus using the improved Delphi survey. Evidence-Based Complementary and Alternative Medicine, 2020, 8565987. https://pubmed.ncbi.nlm.nih.gov/32595769/
Zhang, W., Liu, Y., & Yu, L. (2019). Therapeutic efficacy and the impact of the “dose” effect of acupuncture to treat sciatica: A randomized controlled pilot study. Journal of Pain Research, 12, 351–360. https://pubmed.ncbi.nlm.nih.gov/30666157/
Dr. Alexander Jimenez: A Leader in Personal Injury Care in El Paso
In El Paso, Dr. Alexander Jimenez stands out as a distinguished practitioner for victims of personal injuries, including those with sciatica caused by sports injuries or motor vehicle accidents. With his credentials as a Doctor of Chiropractic (DC), Advanced Practice Registered Nurse (APRN), and Family Nurse Practitioner-Board Certified (FNP-BC), Dr. Jimenez brings a unique blend of expertise to patient care. His practice at El Paso Back Clinic is renowned for its integrative approach, combining advanced diagnostics with holistic treatments.
Dr. Jimenez’s Approach to Personal Injury Cases
Personal injury cases, such as those involving car accidents or sports injuries, often require meticulous documentation and medical expertise to ensure patients receive proper care and legal support. Dr. Jimenez excels in this area by:
Advanced Imaging: Using X-rays, MRIs, or CT scans to identify structural issues like disc herniation or pelvic fractures that may cause sciatica (El Paso Back Clinic, n.d.).
Diagnostic Evaluations: Conducting thorough physical exams and biomechanical assessments to pinpoint the root cause of pain.
Dual-Scope Procedures: Combining chiropractic adjustments with medical interventions, such as injections or referrals to specialists, when needed.
Legal Liaison: Providing detailed medical reports and collaborating with legal teams to document injuries accurately, ensuring patients receive fair compensation.
Dr. Jimenez’s ability to bridge medical and legal needs makes him a trusted advocate for personal injury victims in El Paso. His work ensures that patients not only recover physically but also have the documentation needed to navigate insurance claims or legal proceedings.
Small Changes, Big Impact: Lifestyle Tips for Sciatica Prevention
Preventing sciatica or managing its symptoms doesn’t always require major interventions. Dr. Jimenez emphasizes that small, intentional changes in daily routines can make a significant difference. Here are some practical tips, infused with a touch of humor to keep you smiling:
Stay Active, But Smart: Regular exercise strengthens core muscles, but don’t go full Hulk mode without warming up. Gentle stretches before and after workouts can prevent muscle tightness.
Mind Your Posture: Slouching is the sciatic nerve’s archenemy. Sit up straight, like you’re trying to impress your high school crush at a reunion.
Ergonomic Workspace: Adjust your chair and desk to support your spine. Think of your office chair as a throne, not a torture device.
Stretch Like a Cat: Incorporate daily stretches for your hamstrings, piriformis, and lower back. Channel your inner feline and make stretching a ritual.
Stay Hydrated: Your spinal discs love water like a plant loves sunlight. Drink up to keep them plump and healthy.
Proper Footwear: Athletes, ditch those worn-out sneakers. Good shoes are like loyal friends—they support you through every step.
By making these small tweaks, you can reduce the risk of sciatica and support your musculoskeletal health, whether you’re hitting the gym or just navigating daily life.
The Role of Advanced Diagnostics in Sciatica Treatment
One of Dr. Jimenez’s strengths is his use of advanced diagnostics to create personalized treatment plans. Sciatica can have multiple causes, and pinpointing the exact source is crucial for effective treatment. At El Paso Back Clinic, patients benefit from:
Imaging Studies: X-rays, MRIs, or CT scans to visualize disc herniation, spinal stenosis, or pelvic injuries.
Electromyography (EMG): Tests to assess nerve function and identify compression sites.
Biomechanical Assessments: Evaluating posture, gait, and joint mobility to identify underlying dysfunctions.
These tools allow Dr. Jimenez to develop targeted interventions, whether it’s chiropractic adjustments, acupuncture, or physical therapy, ensuring that patients receive the most effective care for their specific condition.
To bring this all together, let’s consider a hypothetical case study inspired by real-world scenarios at El Paso Back Clinic. Meet Sarah, a 30-year-old avid runner who developed sciatica after a minor fall during a trail race. The impact caused a pelvic misalignment, which irritated her sciatic nerve, leading to burning pain down her left leg. Initially, Sarah thought it was just a pulled muscle, but the pain persisted, affecting her ability to run or even sit comfortably.
Sarah visited El Paso Back Clinic, where Dr. Jimenez conducted a thorough evaluation. An X-ray revealed a subtle pelvic tilt, and a physical exam confirmed piriformis tightness. Dr. Jimenez developed a treatment plan that included:
Chiropractic Adjustments: To correct pelvic and spinal alignment.
Acupuncture: To reduce inflammation and modulate pain signals.
Physical Therapy: To strengthen core muscles and improve running form.
Nutritional Counseling: To support tissue repair with an anti-inflammatory diet.
Within weeks, Sarah’s pain decreased significantly, and she was back to running with proper form and better shoes. Her case highlights how sports injuries can trigger sciatica and how an integrative approach can lead to lasting recovery.
Sciatica can be a challenging condition, but with the right care, recovery is within reach. At El Paso Back Clinic, Dr. Alexander Jimenez and his team offer a beacon of hope for those struggling with sciatica, whether it’s caused by sports injuries, car accidents, or other musculoskeletal issues. By combining chiropractic care, acupuncture, physical therapy, and nutritional support, patients can address the root causes of their pain and regain their quality of life. Dr. Jimenez’s expertise in personal injury cases also ensures that patients receive the medical and legal support they need to navigate complex situations.
Disclaimer: This blog post is intended for informational purposes only and should not be considered medical advice. Always consult a qualified healthcare professional, such as Dr. Alexander Jimenez at El Paso Back Clinic, for a proper diagnosis and treatment plan tailored to your specific condition. Sciatica and musculoskeletal injuries require individualized care, and self-treatment without professional guidance may worsen symptoms.
References
Cao, H., Zhang, Z., & Lu, T. (2021). Causal associations of obesity with the intervertebral degeneration, low back pain, and sciatica: A two-sample Mendelian randomization study. Frontiers in Endocrinology, 12, 740746. https://pubmed.ncbi.nlm.nih.gov/34956081/
Hicks, B. L., Lam, J. C., & Varacallo, M. (2021). Piriformis syndrome: A cause of nondiscogenic sciatica. Current Sports Medicine Reports, 20(2), 97–102. https://pubmed.ncbi.nlm.nih.gov/33560090/
Jensen, R. K., Kongsted, A., Kjaer, P., & Koes, B. (2023). Surgical versus non-surgical treatment for sciatica: Systematic review and meta-analysis of randomised controlled trials. BMJ, 381, e070730. https://pubmed.ncbi.nlm.nih.gov/37019468/
Li, Q., Liu, R., & Zhao, J. (2020). The management of sciatica by acupuncture: An expert consensus using the improved Delphi survey. Evidence-Based Complementary and Alternative Medicine, 2020, 8565987. https://pubmed.ncbi.nlm.nih.gov/32595769/
Vickers, A. J., & Vertosick, E. A. (2021). Extra-spinal sciatica and sciatica mimics: A scoping review. Pain Medicine, 22(1), 70–81. https://pubmed.ncbi.nlm.nih.gov/32951055/
Wang, Y., Chen, J., & Chen, L. (2022). Association between chiropractic spinal manipulation and lumbar discectomy in adults with lumbar disc herniation and radiculopathy: Retrospective cohort study using United States’ data. BMJ Open, 12(12), e068262. https://pubmed.ncbi.nlm.nih.gov/36523295/
Zhang, W., Liu, Y., & Yu, L. (2019). Therapeutic efficacy and the impact of the “dose” effect of acupuncture to treat sciatica: A randomized controlled pilot study. Journal of Pain Research, 12, 351–360. https://pubmed.ncbi.nlm.nih.gov/30666157/
Find relief from piriformis syndrome through specialized chiropractic care tailored to your needs and well-being.
Chiropractic Care for Piriformis Syndrome and Sciatica Relief: A Comprehensive Guide
Introduction: When Your Butt Hurts (Literally)
Picture this: you’re sitting at your desk, trying to focus on that Zoom meeting, but your backside is staging a full-on rebellion. Every shift in your chair feels like a tiny lightning bolt zapping your hip or leg. Sound familiar? You might be dealing with piriformis syndrome, a sneaky condition that can mimic sciatica and turn your daily routine into a literal pain in the butt. But don’t worry—help is on the way, and it doesn’t involve giving up your favorite chair or resorting to a life of standing desks (unless that’s your thing).
In this comprehensive guide, we’ll dive deep into piriformis syndrome, its overlap with sciatica, and how chiropractic care, led by experts like Dr. Alexander Jimenez, DC, APRN, FNP-BC, at El Paso Back Clinic, can help you reclaim your comfort. We’ll explore the science behind musculoskeletal pain, the role of chiropractic adjustments, and why Dr. Jimenez is a trusted name for personal injury victims in El Paso. Plus, we’ll sprinkle in a bit of humor to keep things light—because nobody wants to read a 5,000-word medical textbook without a chuckle or two.
What Is Piriformis Syndrome? The Muscle That’s a Real Pain
Piriformis syndrome occurs when the piriformis muscle—a small, pear-shaped muscle deep in your buttocks—gets irritated or inflamed, often compressing the sciatic nerve and causing pain that radiates down your leg. Think of the piriformis as that one coworker who’s always taking up too much space and causing drama. This muscle’s job is to help rotate your hip and keep your leg moving properly, but when it’s unhappy, it can make sitting, walking, or even standing feel like a chore.
According to Dr. Alexander Jimenez, piriformis syndrome is a common cause of buttock and leg pain, often mistaken for sciatica caused by a herniated disc (Jimenez, n.d.). The piriformis muscle runs from your sacrum (the base of your spine) to the top of your femur, sitting right next to the sciatic nerve. When it tightens or spasms, it can pinch the nerve, leading to symptoms like:
Pain or tenderness in the buttocks
Radiating pain down the back of the thigh or leg
Numbness or tingling in the leg or foot
Discomfort when sitting for long periods
Worsening pain during activities like climbing stairs or running
Unlike sciatica caused by spinal issues, piriformis syndrome is considered “nondiscogenic,” meaning it doesn’t stem from a problem with your spinal discs (Benzon et al., 2016). Instead, it’s all about that pesky piriformis muscle acting like it owns the place.
References
Benzon, H. T., Katz, J. A., Benzon, H. A., & Iqbal, M. S. (2016). Piriformis syndrome: A cause of nondiscogenic sciatica. Current Pain and Headache Reports, 20(2), 10. https://pubmed.ncbi.nlm.nih.gov/26919222/
Sciatica vs. Piriformis Syndrome: Same Pain, Different Culprit
If piriformis syndrome and sciatica were siblings, they’d be the kind who borrow each other’s clothes and get mistaken for one another at family reunions. Both conditions can cause pain, numbness, or tingling that shoots down your leg, but their causes are different, and knowing the difference is key to getting the right treatment.
Sciatica: The Nerve’s Cry for Help
Sciatica refers to pain caused by irritation or compression of the sciatic nerve, often due to a herniated disc, spinal stenosis, or other spinal issues. The sciatic nerve is the longest nerve in your body, running from your lower back through your buttocks and down your legs. When it’s compressed at the spine, it can cause symptoms like:
Sharp, burning pain in the lower back or buttocks
Pain that radiates down one leg
Weakness or difficulty moving the leg or foot
Piriformis Syndrome: The Muscle’s Revenge
Piriformis syndrome, on the other hand, happens when the piriformis muscle itself irritates or compresses the sciatic nerve. This can occur due to muscle tightness, spasms, or anatomical quirks where the sciatic nerve runs through or under the piriformis muscle (Hicks et al., 2020). Symptoms are similar to sciatica but often include:
Localized pain in the buttocks
Pain that worsens with prolonged sitting or hip rotation
Tenderness when pressing on the piriformis muscle
How to Tell Them Apart
Distinguishing between the two can be tricky, but a skilled practitioner like Dr. Jimenez uses advanced diagnostic tools to pinpoint the cause. For example, imaging like MRI or CT scans can reveal spinal issues causing sciatica, while physical exams, such as the FAIR test (flexion, adduction, and internal rotation of the hip), can identify piriformis syndrome (Fishman et al., 2002). If your pain is more buttock-focused and worsens with specific hip movements, piriformis syndrome might be the culprit. If it’s more about lower back pain radiating down, sciatica from a spinal issue could be to blame.
References
Fishman, L. M., Dombi, G. W., Michaelsen, C., Ringel, S., Rozbruch, J., Rosner, B., & Weber, C. (2002). Piriformis syndrome: Diagnosis, treatment, and outcome—a 10-year study. Archives of Physical Medicine and Rehabilitation, 83(3), 295–301. https://pubmed.ncbi.nlm.nih.gov/12394910/
Why Does Piriformis Syndrome Happen? The Risk Factors
So, why does the piriformis muscle decide to throw a tantrum? Several factors can contribute, and they’re often tied to lifestyle, injury, or biomechanics. Here are the main culprits:
Overuse or Repetitive Strain: Runners, cyclists, or anyone who spends hours pounding the pavement (or the spin bike) can overwork the piriformis muscle, leading to tightness or spasms (Cass, 2015).
Prolonged Sitting: If your job has you glued to a chair all day, your piriformis might get cranky from being squished for too long. Think of it as the muscle’s way of saying, “Get up and move!” (Jimenez, n.d.).
Trauma or Injury: A fall, car accident, or sports injury can inflame the piriformis muscle, especially in personal injury cases common in El Paso (El Paso Back Clinic, n.d.).
Anatomical Variations: In some people, the sciatic nerve runs through the piriformis muscle, making it more likely to get pinched (Smoll, 2010).
Muscle Imbalances: Weak core or hip muscles can put extra strain on the piriformis, leading to overuse and pain (Tonley et al., 2010).
These risk factors often overlap with those for general musculoskeletal pain, such as poor posture, lack of exercise, or improper movement patterns. The good news? Chiropractic care can address both the symptoms and underlying causes, helping you get back to your daily routine without wincing.
References
Cass, S. P. (2015). Piriformis syndrome: A cause of nondiscogenic sciatica. Current Sports Medicine Reports, 14(1), 41–44. https://pubmed.ncbi.nlm.nih.gov/25642660/
Smoll, N. R. (2010). Sciatic nerve variants and the piriformis muscle: A systematic review and meta-analysis. Clinical Anatomy, 23(1), 8–17. https://pubmed.ncbi.nlm.nih.gov/32914702/
Tonley, J. C., Yun, S. M., Kochevar, R. J., Dye, J. A., Farrokhi, S., & Powers, C. M. (2010). Core stability and hip exercises improve physical function and activity in patients with non-specific low back pain: A randomized controlled trial. PM&R, 2(8), 745–752. https://pubmed.ncbi.nlm.nih.gov/32714785/
Piriformis Syndrome Treatment- Video
Chiropractic Care: Your Ticket to Piriformis Pain Relief
Now that we know the piriformis muscle can be a real troublemaker, let’s talk about how chiropractic care can calm it down. Chiropractic adjustments, as practiced by Dr. Alexander Jimenez at El Paso Back Clinic, focus on restoring proper alignment and function to your spine and joints, which can relieve pressure on the piriformis muscle and sciatic nerve. It’s like giving your body a tune-up, but instead of wrenches, Dr. Jimenez uses precise, hands-on techniques.
How Chiropractic Care Helps
Chiropractic care takes a holistic approach to piriformis syndrome by addressing both the symptoms and the root causes. Here’s how it works:
Spinal and Pelvic Adjustments: Misalignments in your spine or pelvis can put extra stress on the piriformis muscle. Chiropractic adjustments realign these structures, reducing muscle tension and nerve irritation (Jimenez, n.d.).
Soft Tissue Therapy: Techniques like trigger point therapy or myofascial release can relax the piriformis muscle, reducing spasms and improving blood flow (El Paso Back Clinic, n.d.).
Sciatic Nerve Mobilization: Specific stretches or manipulations can free up the sciatic nerve, relieving that pesky radiating pain (Siddiq et al., 2020).
Correcting Biomechanics: Chiropractors assess your posture and movement patterns to identify imbalances (like weak glutes or tight hip flexors) that contribute to piriformis syndrome. They’ll prescribe exercises to strengthen weak areas and improve flexibility (Tonley et al., 2010).
Lifestyle Advice: Dr. Jimenez often incorporates nutrition and wellness tips to reduce inflammation and support recovery, ensuring your body heals from the inside out (El Paso Back Clinic, n.d.).
Why It Works
The beauty of chiropractic care is that it’s non-invasive and drug-free, making it a safe option for most people. By addressing misalignments and muscle imbalances, chiropractic adjustments reduce the pressure on the sciatic nerve, allowing the piriformis muscle to relax and heal. Studies show that manual therapies, including chiropractic care, can significantly reduce pain and improve function in patients with piriformis syndrome (Fishman et al., 2002).
References
Fishman, L. M., Dombi, G. W., Michaelsen, C., Ringel, S., Rozbruch, J., Rosner, B., & Weber, C. (2002). Piriformis syndrome: Diagnosis, treatment, and outcome—a 10-year study. Archives of Physical Medicine and Rehabilitation, 83(3), 295–301. https://pubmed.ncbi.nlm.nih.gov/12394910/
Siddiq, M. A. B., Hossain, M. S., & Uddin, M. M. (2020). Physiotherapy for piriformis syndrome using sciatic nerve mobilization and piriformis release. Journal of Bodywork and Movement Therapies, 24(4), 190–196. https://pubmed.ncbi.nlm.nih.gov/32685352/
Dr. Alexander Jimenez: El Paso’s Personal Injury Expert
In El Paso, personal injury cases—especially those involving motor vehicle accidents (MVAs)—are all too common. Whether it’s a fender-bender or a more serious collision, injuries like piriformis syndrome can arise from the trauma of an accident. That’s where Dr. Alexander Jimenez shines. With his extensive credentials (DC, APRN, FNP-BC) and decades of experience, Dr. Jimenez is a trusted practitioner for accident victims seeking recovery (Jimenez, n.d., LinkedIn).
Why Dr. Jimenez Stands Out
Dr. Jimenez doesn’t just treat symptoms—he digs deeper to understand the full scope of your injury. His approach includes:
Advanced Imaging: Using MRI, CT scans, or X-rays to identify structural issues like pelvic misalignments or nerve compression (El Paso Back Clinic, n.d.).
Diagnostic Evaluations: Thorough physical exams, including tests like the FAIR test, to confirm piriformis syndrome or rule out other causes (Fishman et al., 2002).
Dual-Scope Procedures: Combining chiropractic adjustments with integrative therapies like massage or acupuncture to address both musculoskeletal and soft tissue damage.
Legal Liaison: Dr. Jimenez works closely with legal teams to document injuries accurately, ensuring victims receive the medical and legal support they need for personal injury claims.
His expertise makes him a go-to for El Pasoans dealing with the aftermath of MVAs, slip-and-falls, or workplace injuries. Whether it’s piriformis syndrome or whiplash, Dr. Jimenez’s comprehensive approach helps patients regain their quality of life while supporting their legal cases.
References
Fishman, L. M., Dombi, G. W., Michaelsen, C., Ringel, S., Rozbruch, J., Rosner, B., & Weber, C. (2002). Piriformis syndrome: Diagnosis, treatment, and outcome—a 10-year study. Archives of Physical Medicine and Rehabilitation, 83(3), 295–301. https://pubmed.ncbi.nlm.nih.gov/12394910/
Jimenez, A. (n.d.). Professional profile. LinkedIn. https://www.linkedin.com/in/dralexjimenez/
Changing Your Daily Routine: Practical Tips for Relief
Piriformis syndrome doesn’t have to run your life. With chiropractic care and some simple lifestyle changes, you can keep that pesky muscle in check. Here are some tips inspired by Dr. Jimenez’s clinical insights:
Stretch It Out: Gentle stretches like the piriformis stretch (lying on your back, crossing one ankle over the opposite knee, and pulling the knee toward your chest) can loosen the muscle (Siddiq et al., 2020).
Strengthen Your Core and Hips: Exercises like bridges or clamshells strengthen the glutes and core, reducing strain on the piriformis (Tonley et al., 2010).
Mind Your Posture: Avoid slouching or crossing your legs for long periods. A lumbar support pillow can help when sitting (El Paso Back Clinic, n.d.).
Stay Active: Low-impact activities like walking or swimming keep your hips mobile without overworking the piriformis.
Nutrition for Healing: Anti-inflammatory foods like berries, fatty fish, and leafy greens can reduce muscle inflammation and support recovery (El Paso Back Clinic, n.d.).
For those with a desk job, try setting a timer to stand and stretch every 30 minutes. Your piriformis will thank you, and you might even avoid those awkward “my leg’s asleep” moments during meetings.
References
Siddiq, M. A. B., Hossain, M. S., & Uddin, M. M. (2020). Physiotherapy for piriformis syndrome using sciatic nerve mobilization and piriformis release. Journal of Bodywork and Movement Therapies, 24(4), 190–196. https://pubmed.ncbi.nlm.nih.gov/32685352/
Tonley, J. C., Yun, S. M., Kochevar, R. J., Dye, J. A., Farrokhi, S., & Powers, C. M. (2010). Core stability and hip exercises improve physical function and activity in patients with non-specific low back pain: A randomized controlled trial. PM&R, 2(8), 745–752. https://pubmed.ncbi.nlm.nih.gov/32714785/
The Bigger Picture: Musculoskeletal Pain and Overlapping Risks
Piriformis syndrome doesn’t exist in a vacuum—it’s part of the broader world of musculoskeletal pain, which includes conditions like lower back pain, sciatica, and joint inflammation. These conditions often share risk factors like poor posture, sedentary lifestyles, or previous injuries, which can amplify each other’s effects. For example, a weak core can lead to pelvic misalignment, which can tighten the piriformis muscle and irritate the sciatic nerve (Tonley et al., 2010).
Chiropractic care excels at breaking this cycle by addressing the root causes of musculoskeletal pain. By realigning the spine, relaxing tight muscles, and improving biomechanics, chiropractors like Dr. Jimenez help patients avoid the domino effect of one injury leading to another. Plus, their integrative approach—combining adjustments, therapy, and lifestyle changes—ensures long-term relief, not just a quick fix.
References
Tonley, J. C., Yun, S. M., Kochevar, R. J., Dye, J. A., Farrokhi, S., & Powers, C. M. (2010). Core stability and hip exercises improve physical function and activity in patients with non-specific low back pain: A randomized controlled trial. PM&R, 2(8), 745–752. https://pubmed.ncbi.nlm.nih.gov/32714785/
Conclusion: A Serious Note on Your Path to Recovery
While we’ve had some fun comparing the piriformis muscle to an overzealous coworker, piriformis syndrome and sciatica are serious conditions that can significantly impact your quality of life. Chiropractic care, as offered by Dr. Alexander Jimenez at El Paso Back Clinic, provides a proven, non-invasive solution to relieve pain, restore function, and prevent future issues. Whether you’re dealing with the aftermath of a car accident or chronic buttock pain from sitting too long, Dr. Jimenez’s expertise in advanced diagnostics and integrative therapies can help you get back on track.
Disclaimer: This blog post is for informational purposes only and should not be considered medical advice. Always consult a qualified healthcare provider, such as a chiropractor or physician, before starting any treatment for piriformis syndrome or sciatica. For personalized care in El Paso, contact Dr. Alexander Jimenez at El Paso Back Clinic or call 915-850-0900 to schedule a consultation.
Get insights into handling sciatica associated with low back & hip pain and regain your active lifestyle with essential care techniques.
Chiropractic Care for Sciatica: Unraveling the Pain in Your Hips and Lower Back
Picture this: you’re trudging through your day, minding your own grim business, when a sharp, electric jolt shoots from your lower back down to your toes, like a lightning bolt with a personal vendetta. Welcome to the world of sciatica, where your sciatic nerve decides it’s the star of a horror show, and your hips and lower back are the unwilling stage. If life were a gothic novel, sciatica would be the brooding villain, lurking in the shadows of your spine, ready to ruin your day with a sinister cackle. But fear not—Dr. Alexander Jimenez, El Paso’s own maestro of musculoskeletal mayhem, is here to banish this pain with the precision of a chiropractic sorcerer.
This blog post is your guide to understanding sciatica, its connection to low back and hip pain, and how chiropractic care, under the expert hands of Dr. Jimenez, can help you reclaim your life from this nerve-wracking nuisance. We’ll dissect the sciatic nerve’s role, explore how its tantrums disrupt your daily routine, and highlight why personal injury cases in El Paso turn to Dr. Jimenez for his diagnostic wizardry. With a touch of dark humor to keep things delightfully grim, let’s dive into the spine-chilling world of sciatica and its remedies.
The Sciatic Nerve: The Body’s Longest Drama Queen
The sciatic nerve is the rockstar of your nervous system, stretching from your lower back through your hips, buttocks, and down each leg like a diva demanding attention. It’s the longest nerve in your body, and when it’s irritated, it throws a tantrum that rivals a toddler in a haunted house. According to Dr. Alexander Jimenez, a chiropractor and functional medicine expert, sciatica occurs when this nerve gets compressed or irritated, often by a herniated disc, spinal stenosis, or even a rogue muscle like the piriformis playing the villain (Jimenez, n.d., dralexjimenez.com).
Anatomy of a Meltdown
The sciatic nerve originates from the L4-S3 nerve roots in the lumbar spine, weaving through the pelvis and branching out to innervate your legs. Think of it as the body’s electrical wiring, transmitting signals for movement and sensation. When something—like a bulging disc or a tight piriformis muscle—pinches this nerve, it’s like short-circuiting a haunted mansion’s lights. The result? Pain, numbness, tingling, or weakness that can radiate from your lower back to your toes, making every step feel like a dance with a skeleton.
Piriformis syndrome, for instance, is a sneaky culprit. This small muscle in your buttocks can clamp down on the sciatic nerve like a gothic clamp, causing nondiscogenic sciatica (Khalili et al., 2020). Lumbar disc degeneration or herniation is another common offender, pressing on nerve roots and sending pain shooting down your leg like a ghostly arrow (Valat et al., 2010). Even asymptomatic disc abnormalities, as seen in MRI scans, can set the stage for sciatica’s grand entrance (Jensen et al., 1994).
Why Your Hips and Lower Back Are the Stage
The hips and lower back are the sciatic nerve’s favorite performance venues. The lumbar spine bears the weight of your upper body, making it prone to wear and tear, like an old crypt crumbling under centuries of neglect. Disc degeneration, spinal misalignment, or muscle imbalances in the hips can compress the nerve, turning your daily routine into a tragic opera. Dr. Jimenez explains that poor posture, prolonged sitting, or trauma from motor vehicle accidents (MVAs) can exacerbate this, as the spine and pelvis lose their structural harmony (Jimenez, n.d., elpasobackclinic.com).
How Sciatica Ruins Your Day (and Your Goth Aesthetic)
Sciatica doesn’t just cause pain; it’s a full-blown saboteur of your daily routine. Imagine trying to enjoy a moonlit stroll, only to be halted by a stabbing pain that makes you wince like you’ve seen a cheerful puppy. Sciatica can make sitting, standing, walking, or even lying down feel like a punishment straight out of a medieval dungeon.
Daily Routine Disruptions
Sitting: Prolonged sitting, like binge-watching a horror series, compresses the sciatic nerve, especially if your posture resembles a slouched gargoyle. This can lead to numbness or a burning sensation that makes your office chair feel like a torture device.
Walking: Each step can trigger a jolt of pain, turning a simple grocery run into a grim pilgrimage. You might limp like a zombie, favoring one leg to avoid aggravating the nerve.
Sleeping: Finding a comfortable position is like solving a cursed puzzle. The pain might keep you awake, leaving you as sleepless as a vampire in daylight.
Exercise: Your usual workout routine—whether it’s yoga or lifting weights—becomes a battle against your own body. The nerve’s irritation can limit mobility, making you feel like a marionette with tangled strings.
Overlapping Risk Profiles
Sciatica doesn’t work alone; it’s got a whole cast of musculoskeletal minions. Low back pain and hip issues often tag along, creating a trifecta of torment. According to Dr. Jimenez, injuries from MVAs, poor ergonomics, or degenerative conditions like arthritis can weaken the spine and pelvis, increasing the risk of sciatic nerve compression (Jimenez, n.d., linkedin.com). For example:
Herniated Discs: A disc bulging out like a ghoul from a crypt can press on the nerve roots, causing sciatica and low back pain (Valat et al., 2010).
Spinal Stenosis: Narrowing of the spinal canal, like a haunted hallway closing in, can squeeze the nerve, leading to pain and weakness.
Hip Muscle Imbalances: Tight hip flexors or a grumpy piriformis can pull your pelvis out of alignment, irritating the sciatic nerve like an annoying poltergeist.
These overlapping issues create a vicious cycle: pain limits movement, reduced movement weakens muscles, and weak muscles exacerbate misalignment, making sciatica a persistent guest at your misery banquet.
Chiropractic Care: The Antidote to Sciatica’s Curse
If sciatica is the villain, chiropractic care is the hero wielding a spine-cracking sword. Dr. Alexander Jimenez and his team at El Paso Back Clinic use a holistic, non-invasive approach to tame the sciatic beast. Chiropractic care focuses on restoring spinal and pelvic alignment, reducing nerve compression, and promoting healing—without the need for potions or invasive surgeries.
Why Chiropractic Care Works
Chiropractic adjustments target the root causes of sciatica, not just the symptoms. Here’s the clinical rationale, straight from the crypt:
Spinal Alignment: Misaligned vertebrae, or subluxations, can compress the sciatic nerve. Adjustments realign the spine, reducing pressure and restoring nerve function (Chou et al., 2007). It’s like straightening a crooked portrait to stop it from haunting your dreams.
Disc Decompression: Techniques like spinal decompression therapy gently stretch the spine, creating space for herniated discs to retreat, easing nerve irritation (Jimenez, n.d., dralexjimenez.com).
Muscle Relaxation: Chiropractors use soft tissue therapies, like myofascial release, to loosen tight muscles (e.g., the piriformis), reducing nerve compression (Khalili et al., 2020).
Improved Biomechanics: By correcting posture and pelvic alignment, chiropractic care prevents future nerve irritation, ensuring your spine doesn’t turn into a haunted house again.
Studies support this approach. A systematic review found nonpharmacologic therapies, including chiropractic care, effective for acute and chronic low back pain, with benefits for sciatica (Chou et al., 2007). Another meta-analysis showed that spinal manipulation provides significant pain relief for sciatica compared to placebo (Li et al., 2023).
Dr. Jimenez’s Approach
Dr. Jimenez doesn’t just crack spines; he’s a detective of discomfort. Using advanced imaging (like MRI or X-rays) and diagnostic evaluations, he pinpoints the exact source of sciatica, whether it’s a herniated disc, spinal stenosis, or a piriformis tantrum. His dual-scope procedures—combining chiropractic adjustments with functional medicine—address inflammation, muscle imbalances, and biomechanical issues. For example, he might pair spinal adjustments with nutritional counseling to reduce systemic inflammation, speeding up recovery (Jimenez, n.d., elpasobackclinic.com).
References
Chou, R., et al. (2007). Nonpharmacologic therapies for acute and chronic low back pain: A review of the evidence. PubMed. https://pubmed.ncbi.nlm.nih.gov/17909210/
Personal Injury Cases in El Paso: Dr. Jimenez’s Expertise
In El Paso, where car accidents are as common as tumbleweeds, personal injury cases often involve sciatica and related musculoskeletal woes. Motor vehicle accidents (MVAs) can jolt the spine like a skeleton on a rollercoaster, causing whiplash, disc herniations, or pelvic misalignments that trigger sciatica. Dr. Jimenez stands out as a beacon for victims, bridging the gap between medical recovery and legal documentation.
The Role of MVAs in Sciatica
MVAs are a leading cause of sciatica, as the sudden impact can misalign the spine or pelvis, compressing the sciatic nerve. Whiplash-associated disorders (WAD) from rear-end collisions, for instance, can strain the lower back and hips, setting the stage for nerve irritation (Jimenez, n.d., elpasobackclinic.com). Even minor fender-benders can cause microtraumas, leading to chronic pain if left untreated.
Dr. Jimenez: The Legal-Medical Liaison
Dr. Jimenez’s expertise goes beyond the chiropractic table. As a distinguished practitioner, he uses advanced imaging (MRI, CT) and diagnostic tools to document injuries with forensic precision, crucial for personal injury claims. His reports detail how trauma from an MVA correlates with sciatica, providing clear evidence for legal cases. His dual-scope approach—combining chiropractic adjustments with therapies like massage or acupuncture—ensures patients recover while building a robust medical record for attorneys (Jimenez, n.d., linkedin.com).
For example, a patient with sciatica from an 18-wheeler crash might receive spinal decompression, trigger point therapy, and nutritional guidance to reduce inflammation. Dr. Jimenez’s documentation ties these treatments to the accident, strengthening the patient’s case while promoting healing. His clinic’s use of durable medical equipment, like braces or TENS units, further supports recovery and legal claims.
Sciatica isn’t just a spine problem; it’s a whole-body conspiracy. Dr. Jimenez’s integrative approach at El Paso Back Clinic combines chiropractic care with complementary therapies to banish pain and restore function.
Key Therapies
Massage Therapy: Trigger point therapy targets tight muscles, like the piriformis, to release nerve compression. It’s like exorcising a demon from your buttocks (Khalili et al., 2020).
Nutritional Counseling: A diet rich in anti-inflammatory foods (e.g., omega-3s, turmeric) reduces systemic inflammation, easing nerve irritation (Jimenez, n.d., dralexjimenez.com).
Exercise Rehabilitation: Targeted stretches and strengthening exercises restore hip and core stability, preventing future sciatica flare-ups. Think of it as training your body to fend off ghosts.
Patient Education: Educating patients on posture, ergonomics, and movement prevents recurrence. Knowledge is power, even against a nerve with a grudge (Cote et al., 2022).
The Role of Patient Education
Patient education is key to long-term relief. Studies show that informed patients are more likely to adhere to treatment plans and avoid behaviors that worsen sciatica, like sitting on a wallet thicker than a gothic novel (Cote et al., 2022). Dr. Jimenez empowers patients with practical tips, like using lumbar supports or avoiding high heels, to keep sciatica at bay.
Cote, P., et al. (2022). Patient education materials for non-specific low back pain and sciatica: A systematic review and meta-analysis. PubMed. https://pubmed.ncbi.nlm.nih.gov/36265509/
Ignoring sciatica is like ignoring a creaking floorboard in a haunted house—it only gets worse. Chronic nerve compression can lead to:
Permanent Nerve Damage: Prolonged irritation may cause numbness or weakness that doesn’t fade, like a ghost that never leaves.
Chronic Pain: Untreated sciatica can evolve into a constant companion, making every day feel like a funeral procession.
Reduced Mobility: Limited movement can weaken muscles, increasing the risk of falls or further injuries, as if life needed more plot twists.
Emotional Toll: Chronic pain can lead to depression or anxiety, turning your psyche into a gothic novel’s protagonist (Valat et al., 2010).
Dr. Jimenez emphasizes early intervention to prevent these grim outcomes. His clinic’s comprehensive approach ensures that sciatica doesn’t overstay its welcome.
While we’ve danced with dark humor to make this journey through sciatica’s shadows more bearable, the condition itself is no laughing matter. Sciatica can profoundly impact your quality of life, turning simple tasks into daunting challenges. Dr. Alexander Jimenez and the El Paso Back Clinic offer a beacon of hope, using chiropractic care, advanced diagnostics, and holistic therapies to address the root causes of sciatica and related low back and hip pain. For personal injury victims in El Paso, Dr. Jimenez’s expertise ensures not only recovery but also the documentation needed for justice.
Disclaimer: This blog post is for informational purposes only and should not be taken as medical advice. Always consult a qualified healthcare provider, such as Dr. Jimenez, for a personalized diagnosis and treatment plan. Sciatica and its associated conditions require professional evaluation to ensure safe and effective care.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine