Sciatica can cause pain, discomfort, tingling sensations and numbness along the entire length of the sciatic nerve. Also known as sciatic nerve pain, is a collection of symptoms caused by a variety of health issues. Many people will turn to the use of drugs and/or medications as well as surgery to treat sciatica, however, research studies have demonstrated that functional medicine can help improve sciatic nerve pain. � As a matter of fact, a 2010 research study published in the Journal of Manipulative Physiological Therapies demonstrated that approximately 60 percent of patients with sciatica benefited from alternative treatment options, such as chiropractic care. Moreover, functional medicine approaches, including acupuncture, yoga, and massage therapy, among other alternative treatment options, have been demonstrated to help improve sciatic nerve pain. Functional medicine can help safely and effectively provide sciatica pain relief. �
Functional Medicine Approaches for Sciatica
Treatment for sciatica can depend largely on the underlying health issues causing the painful symptoms, therefore, it’s important for people to seek help from a healthcare professional. While many doctors choose to utilize drugs and/or medications, such as anti-inflammatory drugs, muscle relaxers, or steroids, to treat sciatic nerve pain, many research studies have demonstrated that alternative treatment options can help improve sciatica.� Below, we will discuss functional medicine approaches which can help improve sciatica symptoms. �
Sciatica is a collection of symptoms characterized by radiating pain, tingling sensations, and/or numbness which extends throughout the length of the sciatic nerve. Sciatica, also known as sciatic nerve pain, is generally diagnosed through its symptoms and depending on the type of painful symptoms, a healthcare professional can safely and effective treat sciatic nerve pain. Functional medicine approaches, such as chiropractic as well as nutrition and lifestyle modifications, can ultimately help improve sciatic nerve pain, or sciatica. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Chiropractic Care
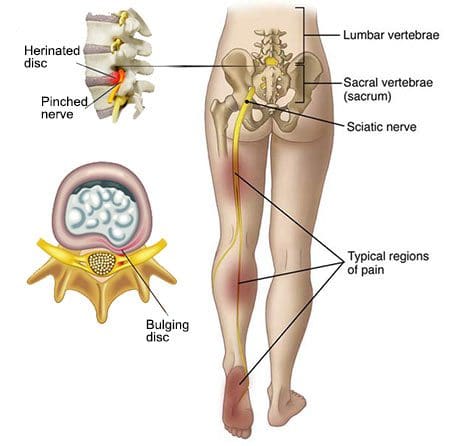
� One research study published in the Official Journal of the North American Spinal Society demonstrated that after comparing the results of 102 adults who suffered from sciatic nerve pain, those who received chiropractic care experienced less pain, fewer number of days with pain, and decreased instances moderate to severe pain compared to those adults who didn�t receive chiropractic care for their sciatica. � Disk herniations are some of the most common causes of sciatica.�There are several types of “ruptured” or herniated discs. Prolapse disc bulges are considered to be less severe because the outermost layer of the disc is still intact, however, extrusion or sequestration disc bulges are generally considered to be more painful. These types of ruptured or herniated discs cause damage to the outer layer of the spinal disc, which leads tissue to push through from where it�s normally constrained. This can compress the sciatic nerve and cause symptoms. �
For healthcare professionals, it�s important to know the patient’s symptoms in order to understand their health issues and follow the appropriate treatment approach. Sciatica can be diagnosed during a physical exam by a chiropractor or doctor of chiropractic. Doctors can also perform X-rays and other tests, such as magnetic resonance imaging, or MRI, test to diagnose the condition of the spine. After diagnosis, a chiropractor may utilize spinal adjustments and manual manipulations to correct the spine and relieve sciatic nerve pain. �
Yoga
Stretches and exercise can aggravate sciatica, however, yoga has been demonstrated to help relieve sciatic nerve pain. Some people have reported that sitting and/or standing for extended periods of time and then moving around suddently can aggravate sciatica. Scrunching or shortening the spine, such as raising the legs up and/or bringing the knees towards the chest in a squatting position can commonly affect symptoms. �
On the other hand, stretching and exercising the spine through yoga can help promote good posture while reducing stiffness, inflammation, and pain frequently associated with sciatic nerve pain. Research studies have demonstrated�that yoga is a safe and effective treatment for people with sciatica. Some of the most important movements for preventing sciatic nerve pain focus on building strength and relaxing stiffness. Stretches and exercises may even be utilized in rehabilitation settings for patients with sciatica following surgery.
Acupuncture and Massage Therapy
Acupuncture is a type of traditional Chinese medicine practice which is based on regulating overall health and wellness by opening the human body�s natural flow of energy. It utilizes small, virtually pain-free needles to target specific pathways in the human body. Acupuncture has been approved by the FDA as a treatment for back pain and it’s supported in a variety of research studies for relieving chronic pain, including sciatica. �
Massage therapy is another non-surgical, holistic approach which helps open muscles, tissues, and channels of energy within the human body to help improve blood flow and reduce painful symptoms. Massage therapy helps reduce back pain, improve muscle relaxation, and even promote the healthy release of endorphins, or the natural �feel good� substances of the human body which act as pain relievers to improve painful symptoms. �
Nutrition and Lifestyle Modifications
Approximately 5 to 10 percent of patients with low back pain also have sciatica, however, healthcare professionals have demonstrated that a patient’s nutrition and lifestyle can increase the risk of developing sciatic nerve pain. Also, factors like height, age, stress, being overweight or obese, sitting or standing for extended periods of time, and smoking, can also increase the risk of developing sciatica and other problems. �
Many of these risk factors cause inflammation, which makes it difficult to heal from injuries and conditions. To prevent inflammation and improve the odds of developing sciatica, make sure to eat a nutrient-dense healing diet, avoid smoking/using recreational drugs, and participate in exercise as well as get good sleep. Constipation may also cause toxicity and inflammation. As a matter of fact, anything which causes toxicity or inflammation can cause sciatica. Nutrition and lifestyle modifications can ultimately help improve sciatic nerve pain. �
Sciatica is a collection of symptoms caused by the compression or impingement of the spinal cord and/or nerve roots. Understanding the symptoms of sciatic nerve pain is essential towards obtaining a diagnosis in order to follow up with the best treatment. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions.
Chronic Back Pain Guidelines
To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.��
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
�
Formulas for Methylation Support
�
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
� Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care. � Please call our office in order for us to assign a doctor consultation for immediate access.
� If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
� * All of the above XYMOGEN policies remain strictly in force. �
� Sciatica, or sciatic nerve pain, is a collection of symptoms caused by the compression or impingement of the spinal cord and/or nerve roots, due to disk herniation, spinal health issues like osteoarthritis, spondylolisthesis, and spinal stenosis as well as intraspinal tumors and abscesses. Impingement or compression may typically occur along the spinal canal or intervertebral foramen. Health issues associated with the compression or impingement of the spinal cord and/or nerve roots may commonly occur in the lower back, pelvis, or buttocks. � �
Sciatica Symptoms
� The common symptoms of sciatic nerve pain include pain and discomfort which radiates along the lower back, down the buttocks and posterior aspect of the leg, into the knee and foot. The painful symptoms may affect one or both lower extremities and it may occur with or without low back pain. The pain and discomfort are described as burning, lancinating, or stabbing. Other common symptoms of sciatica include tingling sensations and numbness anywhere along the length of the sciatic nerve, particularly in the lower extremities. � Coughing or the Valsalva maneuver, a specific way of breathing which increases pressure in the chest, may worsen sciatic nerve pain symptoms. Moreover, the compression or impingement of the spinal cord and nerve roots can cause sensory, motor, or reflex deficits, among other health issues. Symptoms of sciatica may depend on which nerves are affected based on the segmental level of the spine. By way of instance, an L5 to S1 disk herniation may affect the ankle jerk reflex while an L3 to L4 disk herniation may affect the knee jerk reflex. �
Sciatica, or sciatic nerve pain, is a collection of symptoms rather than a single health issue, characterized by radiating pain, tingling sensations, and/or numbness which extends from the lower back and buttocks, down into the legs and feet. Sciatica is generally diagnosed through its symptoms and depending on the type of painful symptoms, a healthcare professional can safely and effective treat sciatic nerve pain. It’s important for patients to understand the symptoms of sciatica in order to continue with a diagnosis and follow-up with the appropriate treatment option. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
� Healthcare professionals have determined that straight leg raising may aggravate pain and discomfort which radiates down the length of the leg when gradually raised above 60 degrees or less. According to numerous research studies, this outcome measure is sensitive to sciatic nerve pain. Painful symptoms radiating down the affected leg when the contralateral leg is lifted, also known as crossed straight leg raising, is more common for sciatica. Furthermore, sciatica can ultimately be diagnosed through a series of tests and evaluations. � The straight leg raise test can be performed while patients are sitting with their hip joints flexed at 90 degrees. Then, their leg is carefully raised until the knee is fully extended. If the patient has sciatica, the painful symptoms will most often manifest as the leg is extended. The slump test can be performed like the straight leg raise test, but while the patient is slumping with the thoracic and lumbar spine flexed as well as the neck flexed. The slump test is more accurate but less specific, for disk herniation than the straight leg raise test. �
Sciatic Nerve Pain Diagnosis
� Sciatica is commonly diagnosed through its characteristic, painful symptoms. Once sciatic nerve pain is diagnosed, healthcare professionals should test a patient’s strength, sensations, and reflexes to determine any possible health issues. If painful symptoms persist for more than 6 weeks, or if there are neurologic deficits, imaging and electrodiagnostic studies should be performed. Structural and functional abnormalities which result in sciatica, such as spinal stenosis, can most accurately be diagnosed through MRI or CT scans. � Imaging and electrodiagnostic studies can help confirm the segmental level of the spinal cord and/or nerve root compression and/or impingement, which can exclude health issues that may mimic sciatica, such as polyneuropathy. These studies may help determine whether single or multiple regions of the spinal cord and/or nerve roots are being affected and whether the diagnosis correlates with MRI abnormalities. Abnormalities may not be obvious on imaging and electrodiagnostic studies for up to a few weeks after symptoms manifest. �
Sciatica Treatment
� Patients with sciatica, or sciatic nerve pain, can achieve relief from their painful symptoms through bed rest in a recumbent position with the head of the bed elevated about 30 degrees, also known as the semi-Fowler position. Treatment for low back pain can include nonopioid analgesics, such as NSAIDs and acetaminophen. Drugs and/or medications which decrease neuropathic pain, such as gabapentin or other anticonvulsants and low-dose tricyclic antidepressants, may also help relieve sciatic nerve pain, or sciatica, signs and symptoms. � Muscle spasm associated with low back pain or sciatica can be relieved through the utilization of heat or cold, physical therapy, and chiropractic care, among other alternative treatment options. Whether corticosteroids should be used to treat acute radicular pain remains controversial. Epidural corticosteroids can help achieve pain relief, however, these should not be utilized unless the patient’s painful symptoms are severe or persistent. Many healthcare professionals may utilize oral corticosteroids for these special occasions. � Surgery for sciatic nerve pain, or sciatica, is only recommended for cauda equina syndrome or for unequivocal disk herniation along with the presence of muscular weakness, progressive neurologic deficit and/or intolerable, intractable pain which interferes with regular physical activities in an emotionally stable patient which has not decreased after 6 weeks of conservative treatments. The standard procedure for sciatica caused by disk herniation is through classic diskectomy with a limited laminotomy. If the disk herniation is localized, a microdiscectomy may be performed, where the skin incision and laminotomy are smaller. Chemonucleolysis, which uses an intradiscal injection of chymopapain, is no longer utilized to help treat sciatic nerve pain. � Sciatica is a collection of symptoms caused by the compression or impingement of the spinal cord and/or nerve roots. Understanding the symptoms of sciatic nerve pain is essential towards obtaining a diagnosis in order to follow up with the best treatment. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions.
To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
�
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All of the above XYMOGEN policies remain strictly in force.
Individuals from all walks of life offer testimonials about their back pain and how their lives suffered from it. Each testimonial describes what they went through being affected by piriformis syndrome and how it limited their ability to take part in their jobs and home life. The patients clarify how El Paso, chiropractor, Dr. Alex Jimenez helped them find relief from their debilitating symptoms. They are all thankful for the treatment Dr. Jimenez has provided, and recommend his team for any type of injury you may have.
El Paso Back Clinic
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
It’s going very, very well. I do feel a lot of relief. What I like about here is that he genuinely cares about his patients and he educates you. He’s constantly talking to you about why he’s doing what he’s doing. He’s very good as a doctor, he’s awesome. – Araceli Norte
Low back pain is a common health issue for many people. Nearly everybody will experience lower back pain at any moment in their own lives. This pain can differ from mild to severe and it might be short-term or long-term. When it happens, low back pain can make many everyday tasks difficult to participate and engage in. That all too familiar annoyance, however, can tremendously limit time spent relaxing, working, and even that of relationships.
Moreover, low back pain might also lead to irritability as well as a whole onslaught of additional medical health issues if not treated appropriately. The prevalence of low back pain has become a common problem, amounting to one of the most common reasons for doctor office visits each year. Before considering what type of treatment approach to follow for your back pain, it’s important to understand the anatomy of the spine and how low back pain occurs.
Understanding the Spine
The World Health Organization estimates that in the United States alone, approximately 149 million days of work are lost as a consequence of low back pain. Back pain is considered to be one of the main sources of disability and shortage of work, and it appears in 60 to 70 percent of people in industrialized nations. Understanding your spine and the way it works can help you know some of the problems which exist from aging or injury, including spinal conditions.
Many demands are placed on your own spine. It holds up your head, shoulders, and upper body. It supplies you with the necessary components to help the human body stand up right, and provides flexibility and mobility to bend and twist. Furthermore, it protects your spinal cord. Back pain differs from one person to another. The pain might have a slow beginning or come on suddenly. The pain may be continuous or irregular. Usually, back pain resolves on its own in a few weeks. However, if you’re experiencing persistent low back pain, then you may have already realized how important it is to look for treatment. Chiropractic care is a well-known treatment option which can help offer relief from your low back pain.
What is Chiropractic Care?
Chiropractic care is a popular, alternative treatment approach which primarily focuses on the diagnosis, treatment and prevention of a variety of injuries and/or conditions, associated with the musculoskeletal and nervous systems. Through the use of specific treatment modalities, including spinal adjustments and manual manipulations, among others, a qualified and experienced chiropractor can help relieve low back pain by carefully correcting spinal misalignments, or subluxations.
By realigning the spine, chiropractic care can help promote the human body’s natural healing capabilities, without the need for drugs and/or medications as well as surgical interventions. Although low back pain can happen due to a variety of causes, chiropractic care can include various treatment modalities which are devoted to the management of numerous injuries and disabilities or conditions, including low back pain.
A chiropractor will perform specific treatments based on the individual’s needs, treating the body as a whole rather than simply reducing the symptoms. Many healthcare professionals recommend seeking chiropractic care for low back pain first before considering other, more aggressive treatment approaches. There are two components for chiropractic care techniques and methods: passive treatments to lower the patient’s pain in sequence to it becoming more manageable, and active treatments that the patient participates in independently.
Passive Treatment
If you’re experiencing low back pain, then it could be debilitating, making it difficult for you to go about your day normally. For that reason, it’s very important to seek immediate medical attention from a qualified and experienced healthcare professional, such as a chiropractor or physical therapist, to reduce your pain as much as possible so that you can actively participate in your treatment. These tools are often referred to as passive treatment because they are performed to a patient by the healthcare professional, including:
Electrical stimulation, such as TENS Units
Heat/ice packs
Ultrasound
Iontophoresis
Dry needling
Manual remedies
Massage
Hydrotherapy
Healthcare professionals use some of the methods, such as hot/cold packs and massage therapy, to improve blood flow to the affected area, thus reducing swelling and stiffness. Additionally, a chiropractor may utilize electric stimulation therapy, a painless remedy that gives miniature electric waves through your nervous system to relieve pain, reduce muscle strain, and encourage your body to create hormones which are anabolic. A variety of patients may also benefit from hydrotherapy. This involves executing low-intensity moves in water which alleviates strain on muscles while allowing you to move your joints without any distress.
Active Treatment
Active treatment involves exercises performed by the person and are often utilized at the following phases of chiropractic and passive treatments following the very low back pain has subsided enough so that the patient may perform them without any excessive distress. There are numerous different kinds of exercises that a chiropractor or professional physical therapist may recommend, like extending, balance training, and strength training. A variety of them can assist you with your strength, flexibility, mobility and range of motion, but a few help build the muscles around the painful region to provide those regions of the human body collectively with support to reduce low back pain.
Dr. Alex Jimenez’s Insight
A doctor of chiropractic, or chiropractor, will make sure to properly evaluate a patient before making any form of diagnosis or developing a treatment plan. An assessment can include analyzing the patient’s health history, a physical examination, including orthopedic and neurological tests, as well as advanced diagnostic tests. A chiropractor, or doctor of chiropractic, will then perform a variety of treatment modalities to treat a patient’s low back pain, depending on the specific cause of their symptoms.
What to Expect During a Chiropractor Visit
After you initially visit a chiropractor’s office, your doctor may ask you a couple of questions concerning your health, history, and lower back pain particularly. With this information, you will help your chiropractor provide you with the best treatment plan possible so that you see long-term results for your low back pain as quickly as possible.
Your doctor of chiropractic, or chiropractor, can also offer you an extensive examination. Depending upon your symptoms, your chiropractor may assess your own strength, coordination, flexibility, balance, posture, blood pressure, and heart and respiration rates. This may include using their hands to palpate your spine and surrounding area, along with a visual analysis of your movements.
You are going to learn excellent exercises to perform in your home so you may decrease your low back pain, stop re-injury, decrease strain, and accelerate your healing period. Your chiropractor will recommend specific equipment and will devote a good deal of time educating you about your source of pain and pain management plans. They’ll also implement hands-on exercises to supply you immediate relief.
When you’re well prepared to alleviate or remove your own pain, then seek immediate medical attention, so that a qualified and experienced chiropractor or professional physical therapist can help you live a pain-free life. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
I came to him (Dr. Alex Jimenez) and he’s been doing work on me and it’s been like, we’re going on 7 days, and I seem to be improving a lot more with him than what I’ve done with other therapists that I’ve been going to in almost a year. I would recommend him very highly, he’s good at what he does. – Leticia
According to the National Institute of Neurological Diseases and Stroke, or NINDS, lower back pain is one of the most common reasons for premature disability, often amounting to many doctor office visits and missed days at work. Based on these statistics, at least 80 percent of individuals in the world will experience low back pain at some point in their lifetimes, a majority of which could have been prevented.
Most lower back pain results from an injury, such as muscle sprains or strains due to abrupt movements or poor body mechanics while lifting heavy things. Low back pain may also be caused by certain ailments, such as a ruptured or herniated disc, sciatica, arthritis, kidney infections, diseases of the spinal column or cancer of the spinal cord,. Acute back pain can last anywhere from a few days to a few weeks while chronic back pain can last over three weeks to even months.
Low back pain is significantly more likely to happen in people between the ages of 30 and 50. This is partly as a consequence of changes that develop within the whole body with age. As you grow older, the fluid-like substance of the intervertebral discs in the spine reduces. This means that the discs in the spine experience stress more easily. You also lose muscle tone, which makes the spine more vulnerable to harm.
Ask any healthcare professional and you’ll get confirmation that low back pain is the most frequent health issue they are asked to look after. Strengthening your muscles and using good body mechanics are beneficial in preventing lower back pain. Often back pain can decrease on its own, especially through the use of the “RICE” treatment. But whilst rest, ice, compression and elevation can reduce back pain, its important to also seek treatment from a healthcare professional to treat the true underlying cause of your lower back pain.
What are the Symptoms of Low Back Pain?
Low back pain can be different for everyone. It might be sharp or stabbing. It may be dull, achy, or feel as a sort of cramp. The kind of pain you have will be based on the root cause of your low back pain. Many individuals discover that reclining or lying down can enhance their lower back pain, regardless of the underlying reason. Individuals with low back pain might experience a number of these, including:
Back pain that worsens with lifting and bending.
Worsening symptoms when sitting down.
Symptoms that become worse when walking.
Back pain which comes and goes, frequently following an up and down path.
Pain that extends from the back to the buttocks or outer hip, and travels down the leg.
Sciatica, including buttock and leg pain which travels into the foot, along with numbness, weakness or tingling sensations. It’s likely to get sciatica without low back pain.
Because low back pain can develop due to a variety of underlying health issues, symptoms commonly associated with lower back pain may differ from person to person. Irrespective of your age or symptoms, even if your low back pain doesn’t get better over a couple weeks, or is associated with fever, chills, or sudden weight loss, it’s fundamental for you to contact a healthcare professional immediately.
How is Low Back Pain Diagnosed?
Most doctors begin by conducting a physical examination to determine where you’re feeling the pain. A physical exam may also ascertain whether pain is affecting other structures and functions of your body. Your doctor may check your reflexes and your response to certain senses. This determines if your low back pain is affecting your nerves. If you do not have such debilitating symptoms, your doctor will probably monitor your condition before sending you for testing.
Certain symptoms like lack of bowel control, fever, fatigue, and weight loss might demand additional testing. Likewise, if your low back pain persists following home treatment, your doctor may also most likely want to send you for tests. Seek medical attention immediately at the event you observe any of these symptoms in addition to lower back pain.
Imaging evaluations such as X-rays, CT scans, ultrasound, and MRI may be needed in order for your doctor to evaluate bone issues, disk difficulties, or problems with the joints and ligaments in your spine. If your doctor suspects a matter with all the bones in your spine, they could send you to have a bone loss or bone density test. Electromyography, or EMG, as well as nerve conduction tests can help identify a problem with your own nerves.
How Can I Prevent Low Back Pain?
There are plenty of methods to prevent lower back pain. Practicing prevention techniques may also help reduce the seriousness of the symptoms once you have lower back pain. Prevention involves exercising the muscles in your core and back, losing weight if you are overweight or obese, lifting items properly by bending at the knees and lifting with the legs, and maintaining proper posture. Among the most common causes of lower back pain is a misalignment of the spine, or a subluxation, originating from improper posture.
Most office setups don’t provide ergonomic or support positioning desk chairs, while poor work habits prevents us from providing our spines with the much-needed relief we deserve throughout the day. Non-desk jobs also have their own perils. Standing daily, especially when combined with heavy lifting or routine bending, may also cause low back pain. The muscles surrounding the lumbar spine may not acquire the support they need when bending and lifting, resulting in low back pain. In either circumstance, strengthening these back muscles is fundamental to reducing the probability of chronic lower back pain.
Insist on an ergonomic desk chair, or have the opportunity to stand and move around more frequently. If you’re a cashier, invest in shoes with good arch support, which may help keep your entire body aligned. If needed, put on a technical brace to help support heavy lifting. Good habits at home to prevent low back pain can involve sleeping on a firm surface and having seats that are in the proper height. Steer clear from high-heeled shoes. If you smoke, then you may need to quit. Smoking causes the degeneration of spinal discs and reduces blood flow. But when you already have low back pain, a variety of treatment options, such as chiropractic care, can help treat lower back pain.
Dr. Alex Jimenez’s Insight
Many health issues can ultimately affect the spine, causing low back pain. Because of this, an individual’s symptoms are always different, often characterized by the underlying problem affecting them. A chiropractor can diagnose the source of a patient’s symptoms over a series of tests and evaluations, to determine the best treatment approach for the individual’s cause of low back pain. Chiropractic care focuses on naturally correcting any spinal misalignments, or subluxations, to reduce low back pain.
How Can Chiropractic Care Treat Low Back Pain?
Chiropractic care is one of the most well-known treatment options for relieving lower back pain. Medical practitioners normally recommend their patients to consider alternative treatment options before turning to prescription drugs and/or medications or surgery. The reasons are obvious: Many medications and/or drugs can have long-term health consequences. Whatever the advantages of providing temporary pain relief may be, these carry risks of complication throughout the recovery period.
Chiropractic care is a treatment approach which focuses on the diagnosis, treatment and prevention of a variety of injuries and/or conditions associated with the musculoskeletal and nervous system. Through the use of spinal adjustments and manual manipulations, a chiropractor can carefully restore the natural alignment of the spine, reducing stress in the complex structures of the spine and improving function. Chiropractic care may also include other treatment techniques and methods to help reduce low back pain.�Lower back pain may also need the two-pronged way of using both active and passive physical therapeutics, unless the healthcare professional has a reason to recommend one over another.
Passive treatments includes using ice packs and heating pads. The healthcare professional may also use many different forms of pulsing equipment, which triggers nerves and releases pain.
Active treatments comprises the individual to perform stretches and exercises that build the type of flexibility and strength necessary to stop future flare-ups and reduce current pain. Lots of them are done with a chiropracto’s supervision, on specialized equipment, though some might be performed at the patient’s home after they learns the principles.
Chiropractic care can help treat low back pain through the treatment approaches mentioned above. Furthermore, a chiropractor may suggest lifestyle modifications to help promote a faster recovery, including physical activities and nutritional guidelines. It you’re experiencing low back pain, make sure to seek immediate medical attention, in order to receive a proper diagnosis and be able to continue with treatment. Moreover, preventing lower back pain can help avoid future episodes. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
I go back to normal after seeing him (Dr. Alex Jimenez) and I know I can go back to doing whatever I can. But I’m now more careful. I would recommend him. It’s hard to find someone that knows their job and has a love for their job. That’s why I always come back. If I’ve got pain, I’m gonna look for him. – Mike Melgoza
Low back pain is one of the most prevalent reasons why people visit the doctor’s office and miss days from work. Approximately 80 percent of people will experience back pain at some point throughout their lifetime. Low back pain can range from moderate to severe and it can be acute, short-term, or chronic, long-term.�Because back pain can be caused by a variety of factors, the symptoms may also vary from one person to the other.
Most of the time, low back pain is more of an annoyance than anything else.�If an individual’s low back pain becomes intense and persistent, it can be tremendously debilitating and it can ultimately make it a challenge to participate as well as engage in many everyday activities. It’s essential to seek immediate medical attention to receive a proper diagnosis and continue with the best treatment option for each patient’s specific health issue.
Causes of Low Back Pain
Many potential causes can result in low back pain. In our modern world, spinal misalignments, or subluxations, caused by poor posture, have become one of the most common causes for low back pain, probably due to the simple fact that more and more people work in sedentary desk jobs than ever before. Without the appropriate back support from an ergonomic desk chair, low back pain can easily occur as a result of poor posture and due to the limited mobility of the spine throughout the day.
Even people who are up on their feet the vast majority of the day might suffer from low back pain due to a lack of spinal and abdominal support as well as a lack of proper coordination of the back muscles. While lower back pain can’t always be prevented, it’s possible to reduce the risk of suffering from lower back pain by practicing proper posture throughout the day to support the spine.
For individual’s who sit behind a computer screen for extended periods of time, this might mean investing in an ergonomic desk chair. For the more active individuals, it may mean purchasing a good pair of athletic shoes which can provide them with the right level of back and foot support throughout the day. Low back pain can also develop due to a variety of injuries and/or conditions. Fortunately, many treatment options are available to help treat low back pain, including chiropractic care and physical therapeutics.
Dr. Alex Jimenez’s Insight
The spine is made up of small bones, known as vertebrae, intervertebral discs, muscles, ligaments and nerves. With several factors, however, including poor posture, trauma from an injury, or an aggravated condition, the spine can become misaligned, ultimately affecting the complex structures surrounding the spine and resulting in back pain. Low back pain is among the most common types of back pain, particularly due to its increased role in supporting the weight of the human body.
Chiropractic Care for Low Back Pain
Chiropractic care is an alternative treatment option which focuses on the diagnosis, treatment and prevention of a variety of injuries and conditions associated with the musculoskeletal and nervous system, including back pain. Seeking chiropractic care as treatment for lower back pain is always recommended before you opt to start taking any prescription drugs and/or medications.
Pain and anti-inflammatory drugs and/or medications can relieve your low back pain, however, the results are usually temporary and these may also bring about undesirable side effects. Chiropractic care is a non-invasive and drug-free strategy for low back pain relief. It’s recommended to seek alternative treatment options, including chiropractic care and physical therapeutics, before turning to the use of drugs and/or medications as well as surgical interventions.
A doctor of chiropractic, or chiropractor, will commonly use spinal adjustments and manual manipulations to carefully correct any spinal misalignments, or subluxations, which may be causing the patient’s low back pain. Moreover, a chiropractor may utilize�passive and active treatments for low back pain and they often vary considerably in their techniques and methods. Passive and active treatments for low back pain are described as follows:
Passive treatments depend upon techniques and methods to be performed on the person. This may include anything from applying ice or heat packs to the affected area to stimulating the affected region with controlled electricity. Other treatment modalities used here may comprise of ultrasonography, TENS units, and iontophoresis.
Active treatments, on the other hand, describes measures that the patient will take, as instructed by a healthcare professional, to manage their low back pain. Typically, this comes from the type of stretches and exercises that are meant to reduce low back pain and minimize potential flare-ups too. Active treatments could include low-impact aerobic conditioning and back strengthening exercises. These may vary based upon the healthcare professional’s requirements.
Chiropractic care and physical therapeutics might be a wonderful solution for treating nearly any level of low back pain. Through the utilization of spinal adjustments and manual manipulations, as well as a combination of active and passive physical therapeutics, you’re in a position to work towards reducing your stress and increasing your body’s natural capability to prevent future health issues.
Contact a healthcare professional today to find out more about how you can manage your low back pain.The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
One of my friends recommended me, over and over, and just extended how good he�(Dr. Alex Jimenez, D.C.) was. So I gave it a shot. I had really bad sciatica and it was killing me, I couldn’t walk, but he has been helping me out, I can walk now… I couldn’t walk more than 25 yards, it (sciatica) was really affecting me. I had to get some help. I can’t say enough about Dr. Jimenez, he’s been helping me out, I can walk.
Edgar M. Reyes
According to the American Association of Neurological Surgeons, approximately 75 to 85 percent of individuals in the United States alone will experience some form of back pain throughout their lifetime, where 50 percent will suffer more than one episode within a year. Back pain is one of the most common complaints frequently reported among the general population and it is often a symptom which could indicate the presence of another underlying condition. Back pain can be caused by a variety of factors, some due to bad habits, such as improper posture, and others due to injuries from accidents. Other health issues, such as degenerative disc disease, or DDD, and arthritis can also result in back pain.�While the causes can vary, they share the same symptoms.
Bak pain can include upper back pain, middle back pain and lower back pain, often connected to sciatica, or sciatic nerve pain, a condition characterized by the compression or impingement of the sciatic nerve found in the low back. Back pain and sciatica have been closely associated with several common health issues. Often times, sciatica, or sciatic nerve pain, is caused by an underlying health issue along the lumbar spine. The sciatic nerve is the longest nerve in the human body, which connects to nerve roots in the region of the lower back and runs through the buttocks, down along the hips and into the back of each leg. Further sections of this nerve then branch out from the calf to the foot and into the toes. Sciatica can be identified by the following symptoms.
Low back pain which radiates down one or both legs
Leg and/or foot pain along with tingling and burning sensations
Numbness in the leg, feet and/or toes
Persistent pain and discomfort on one or both sides of the buttocks
Intense painful symptoms in the lower extremities
Having difficulties when sitting and while getting up
It’s essential to understand that back pain and sciatica are not generally considered to be a specific health issue themselves but rather, they are usually only considered to be a collection of several symptoms associated with an underlying injury and/or condition. A proper diagnosis of the root cause of your symptoms is additionally important in order to safely and effectively treat back pain and sciatica. As mentioned above, numerous factors can cause back pain and sciatica symptoms. Below, we will discuss some of the most common spine health issues which can cause back pain and sciatica, including degenerative disc disease, lumbar spinal stenosis, lumbar herniated disc and spondylolisthesis. Approximately 90 percent of sciatica cases are due to disc herniations.
Degenerative Disc Disease
The degeneration of the intervertebral discs, found between each vertebrae of the spine, is a natural process which often occurs with age, while for some individuals, however, it can begin to develop earlier than usual. In a healthy spine, the intervertebral discs function as shock absorbers between the bones of the spine, which ultimately provide height and allow the back to remain flexible while resisting forces. As we begin to get older, these rubbery discs begin to shrink and lose integrity. Almost everyone will demonstrate signs of wear-and-tear along their spinal discs over time, but not everyone will experience degenerative disc disease, or DDD. Although not actually a disease, DDD refers to a condition in which pain with the degeneration of the intervertebral discs.
One or more degenerated discs along the length of the spine may irritate a nerve root and cause sciatica. This condition is commonly characterized when a reduced disc becomes exposed. Bone spurs can also develop with disc degeneration and can lead to sciatica. Symptoms of degenerative disc disease, or DDD, frequently occur along the lower back, however, they can also develop in the neck, depending on the location of the degenerated discs. Common symptoms of DDD include, pain and discomfort, particularly when sitting, bending, lifting or twisting, tingling sensations and/or numbness in the extremities, and lessened symptoms when walking and moving, as in with changing positions or lying down. Weakness in the leg muscles or foot drop may be a sign that there is damage to the nerve root.
Lumbar Spinal Stenosis
Another common cause of back pain and sciatica is lumbar spinal stenosis. The natural degeneration of the spine which occurs with age can cause a variety of changes to the spine. Lumbar spinal stenosis is brought on by a gradual narrowing of the spinal canal that is common in the aging process and it generally affects people over the age of 50. When the space around the spinal cord narrows, it can place unnecessary amounts of pressure on the spinal cord and nerve roots. Additionally, it can be the result of a bulging disk, enlarged aspect joints, or an overgrowth of tissue. Only a small number of individuals are born with spine health issues which can develop into lumbar spinal stenosis. This is known as congenital spinal stenosis and it is frequently diagnosed in men.
Arthritis, or the degeneration of any joint in the body, has been attributed to be the most common cause of spinal stenosis. As the intervertebral discs begin to wear-and-tear naturally begin, they can lose water content and eventually dry out, ultimately losing height and even collapsing. This can place pressure on the facet joints, the joints which provide flexibility and movement to the spine, resulting in arthritis. As a result, the ligaments around the structures of the spine can increase in size, lessening the space for the nerves. Also, the human body may respond by growing new bone, additionally narrowing the space for the nerves to pass through. Symptoms of lumbar spinal stenosis may include, pain, tingling or burning sensations, numbness and weakness, as well as less painful symptoms when leaning forward or sitting.
Lumbar Herniated Disc
A herniated disc is a condition which can occur anywhere along the length of the spine, however, it most commonly affects the lower back or lumbar spine. It may also be referred to as a bulging, protruding or ruptured disc. A lumbar herniated disc is considered to be one of the most common causes of back pain in the lower back, as well as sciatica. An intervertebral disc begins to herniate when the soft, jelly-like nucleus, known as the nucleus pulposus, pushes against its outer ring, known as the annulus fibrosus, due to wear-and-tear or a sudden injury. With persistent pressure, the jelly-like nucleus may push through the disc’s outer ring or it may cause the ring to bulge, putting additional pressure on the spinal chord and its surrounding nerve roots.
Moreover, the intervertebral disc material can release chemicals and/or substances which may ultimately irritate the surrounding structures of the spine, contributing to nerve inflammation. When a nerve root becomes irritated, it can potentially lead to symptoms of pain and discomfort, numbness and weakness in one or both legs, otherwise referred to as sciatica, or sciatic nerve pain. An individual may also develop a herniated disc without ever experiencing any symptoms. A lumbar herniated disc is generally caused by the natural degeneration of the spine and discs, however, trauma and/or injury may also result in lumbar disc herniations. Symptoms of a lumbar herniated disc includes sciatica, tingling sensations, numbness, weakness, and loss of bladder or bowel control in severe cases. This last symptoms will require immediate medical attention.
Spondylolisthesis
Spondylolisthesis is another common cause of back pain and sciatica, particularly in young athletes. Repeated stress on the lower back, or lumbar spine, can create a crack or stress fracture in one of the vertebrae. In these cases, however, the stress fracture can often weaken the bone so much, to the point where it is unable to maintain its proper position in the spine, ultimately causing the vertebra to begin to shift or slip out of place. This condition is what is commonly known as spondylolisthesis. In children and adolescents, spondylolisthesis can occur through periods of rapid growth, by way of instance, during an adolescent growth spurt. This condition frequently occurs as a result of overuse, overstretching, or hyperextension, and even due to genetics.
Many healthcare professionals characterize spondylolisthesis as either low grade or high grade, depending on how much the vertebrae have shifted or slipped out of place. A high grade slip is generally identified when more than 50 percent of the width of the fractured vertebra slips forwards onto the vertebra beneath it. Individuals with high grade cases of spondylolisthesis will commonly describe experiencing significant levels of pain and discomfort as well as nerve injury. In the majority of instances, however, individuals with spondylolisthesis will not experience any obvious symptoms, as a matter of fact, most are unaware of the condition till an x-ray is taken for an unrelated injury and/or condition. Individuals with spondylolisthesis may experience back pain and sciatica, including muscle spasms, back stiffness and tight hamstrings.
Dr. Alex Jimenez’s Insight
Back pain is one of the most common reasons why individuals often miss days from work or go to the doctor, as it has also become one of the leading causes of disability worldwide. As a matter of fact, it has been statistically determined that approximately 80 percent of people will or have experienced back pain at least once throughout their life. Fortunately, a variety of treatments are available which can help ease the symptoms of back pain. It’s essential to understand back pain and sciatica, a collection of symptoms commonly associated with spine health issues along the lower back, in order to seek proper diagnosis and continue with an appropriate treatment plan in order to relieve your symptoms of back pain and sciatica.
Treatment for Back Pain and Sciatica
Chiropractic care is a well-known, alternative treatment option commonly utilized to help diagnose, treat and prevent back pain and sciatica. Since there are many factors which can contribute to symptoms of back pain and sciatic nerve pain, a doctor of chiropractic’s, or chiropractor’s, initial step would be to determine the root cause of the patient’s symptoms. Determining a diagnosis involves a thoughtful review of the patient’s health history, and a physical and neurological examination. Diagnostic testing may involve an x-ray, MRI, CT scan and/or electrodiagnostic tests, such as a nerve conduction speed evaluation or an electromyography. These examinations and tests help determine possible contraindications to treatment.
The aim of chiropractic care is to help promote the human body’s potential to heal itself. It is based on the scientific principle that limited spinal motion results in pain and reduced function and performance. Chiropractic care is non-invasive, or non-surgical, and drug-free. The type of chiropractic treatment provided is dependent upon the cause of the individual’s back pain and sciatica. A treatment program may include many distinct treatments and therapies, like ice/cold therapies, ultrasound, TENS, and spinal adjustments or manual manipulations. If the doctor of chiropractic decides that the patient’s spinal health issue requires treatment by a different kind of physician, then the individual may be referred to another healthcare professional.
Physical therapeutics for these conditions is also effective and generally has two components: active and passive. Passive physical therapeutics consist of ultrasound, electric stimulation, heat and ice packs as well as iontophoresis. Active physical therapeutics modalities include stretching exercises, back exercises and low-impact aerobic conditioning. Manual physical therapeutics, such as spinal adjustments and/or manual manipulations, might be integrated in part by a chiropractor. Physical therapists normally recommend 20 minutes of dynamic lumbar stabilization exercises every day. Core muscle strengthening is also important in treating back pain. Low-impact aerobics are also important and include water therapy, biking, and walking.
Physical therapeutics are an important element of treating spinal health issues. If you meet with a physical therapist, there will be a full assessment. Tests will be performed and an individualized treatment plan will be developed based on the patient’s goals. If you’re experiencing back pain or sciatica, don’t wait any longer for relief. Contact a healthcare professional to establish a one-on-one consultation and complete evaluation. Many chiropractors and physical therapists are certified, experienced and dedicated to helping you feel better. They have helped many others recover from spinal health issues and can help you too. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine



 �
�