Throbbing, dull and achy, sharp and excruciating. All of these words can be used to describe lower back pain.
Unfortunately, lower back pain is a common occurrence in adults. According to the American Chiropractic Association, low back pain is the single leading cause of disability worldwide, with millions of reported cases�every year.
What Treatment Should You Seek If You Experience Pain in Your Lower Back?
The good news is that it often heals on its own. A few days of over-the-counter pain meds, ice,�and taking it easy, and you could be back to normal.
However, those who continue to deal with the pain after a few weeks’ time may choose to look for other solutions. This is also true for people who experience repeated flare-ups, or chronic lower back pain.
One of the best and most popular options is chiropractic care.
Why?�
First of all, chiropractic care doesn’t focus solely on the pain but helps the body heal itself. Chiropractors understand the bones,�muscles, discs, and nerves�in the back, and can figure out the reason for the pain.
From there, they can create a customized treatment plan from compresses to spinal manipulation to exercises that help heal the area and reduces the pain.
Second, It’s A Drug-Free Solution.
Because of its healing, therapeutic approach, chiropractic treatment tends to the source of the pain, instead of simply dulling it. Spine Universe estimates 6 to 12 treatments are typically needed to treat low back pain, but each person’s requirement may vary.
Throughout these�treatments, spinal alignment begins�to balance the other parts of a person’s back and helps correct the issue causing the pain. Also, spinal manipulation helps improve mobility and function in many cases, whereas drugs alone do not.
Finally, Chiropractic Care for Lower Back Pain Also Helps Minimize Relapses
Patients who experience lower back pain never want to deal with it again, but�it can flare up periodically. According to the National Institute of Neurological Disorders and Stroke, roughly 20% of those who suffer from low back pain will eventually deal with it chronically. This can cause frustration, primarily when it affects mobility.
Before you run screaming in horror to the medicine cabinet, one of the best reasons to participate in chiropractic treatment is that it helps reduce the chance of a recurrence. By working on the total body and getting it in the best shape possible, the patient is stronger and more balanced to handle their workload and other strenuous activities. Chiropractors also impart advice on how to minimize the chances of re-aggravating the lower back.
Millions of people suffer from back pain each year, and some never visit a chiropractor. Those who do choose chiropractic treatment are privy to treatment that reduces their pain, increases healing, shortens their downtime and lessens their chances of a recurrence. If over the counter medication and ice packs haven’t worked within a few days, it’s time to make an appointment for a consultation with a licensed chiropractor. You will be happy you did.
With the increase of osteoporosis in older adults, the diagnosis and treatment�of abnormal hip fractures, such as�bisphosphonate-related proximal femoral fractures,�has become more important. According to Dr. Edward J. Fox, MD, obesity is often managed through the long-term�use of bisphosphonate treatment, which can inhibit�osteoclast-mediated bone regeneration. Over the prolonged utilization of bisphosphonate, patients� may develop atypical proximal femoral fractures.
Understanding Atypical Femur Fractures
Atypical femur fractures are characterized as stress fractures which commonly occur in the proximal one-third of the diaphyseal bone, although they might also occur more distally, developing in the lateral cortex and slowly progressing medially. “With irregular fractures, a small ‘beak’ of bone can form on the lateral surface of the femur and that is where the fracture generally begins,” explains Dr. Fox. This contrasts with stress fractures which occur laterally in the medial portion of the bone.
As a result, when a patient with osteoporosis reports feeling hip and knee pain without previous damage or injury, healthcare professionals will ask about bisphosphonate treatment. It is essential for the�doctor to request x-rays of the hip and femur shaft for proper diagnosis.�It is also important to request x-rays of the opposite femur, as atypical bisphosphonate-related proximal femoral fractures frequently occur bilaterally. Dr. Edward J. Fox urges patients to discontinue bisphosphonate use in the case of hip fractures,�followed by the subsequent use of crutches or a walker. Patients will eventually be able to resume regular physical activities.
Approximately more than 250,000 hip fractures occur in the United States, causing significant patient disability. The variety of hip fractures in older adults, including bisphosphonate-related proximal femoral fractures, often need several treatment approaches which depend on different considerations, such as the mechanism of injury, location and degree of the fracture, as well as the patient’s age and overall health and wellness.
Dr. Alex Jimenez D.C., C.C.S.T.
The precise mechanism of injury by which bisphosphonates cause atypical femur fractures is unknown. Research studies have demonstrated that the suppression of osteoclast activity prevents the clearance of bone fragments which build up on the bone surface during regular daily tasks; decreasing the strength of the bones which lead to fracture. “We all know that the threat of those fractures increases with the extended duration of bisphosphonate exposure, particularly after five decades. Bisphosphonates are stored with a half-life of at least eight decades in bone matrix. To reduce over-exposure and risk of atypical fracture, passing medication discontinuance has been speculated to be beneficial,” explained Dr. Fox
Dr. Edward J. Fox, MD, stated that until research studies find the exact mechanism of injury and treatment for bisphosphonate-related proximal femoral fractures, healthcare professionals should continue to determine the best treatment option for each patient, carefully weighing the benefits and risks of individual patients. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain is the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
X-radiography pitfalls: some undisplaced Garden 1 & 2 Fxs may be missed d/t pre-existing DJD and osteophytes along the femoral head-neck junction that may overly the Fx line
Fx line is incomplete and too small/subtle especially if the study is read by non-radiologists
Incomplete Fxs if left untreated will not heal and likely to progress to complete Fxs
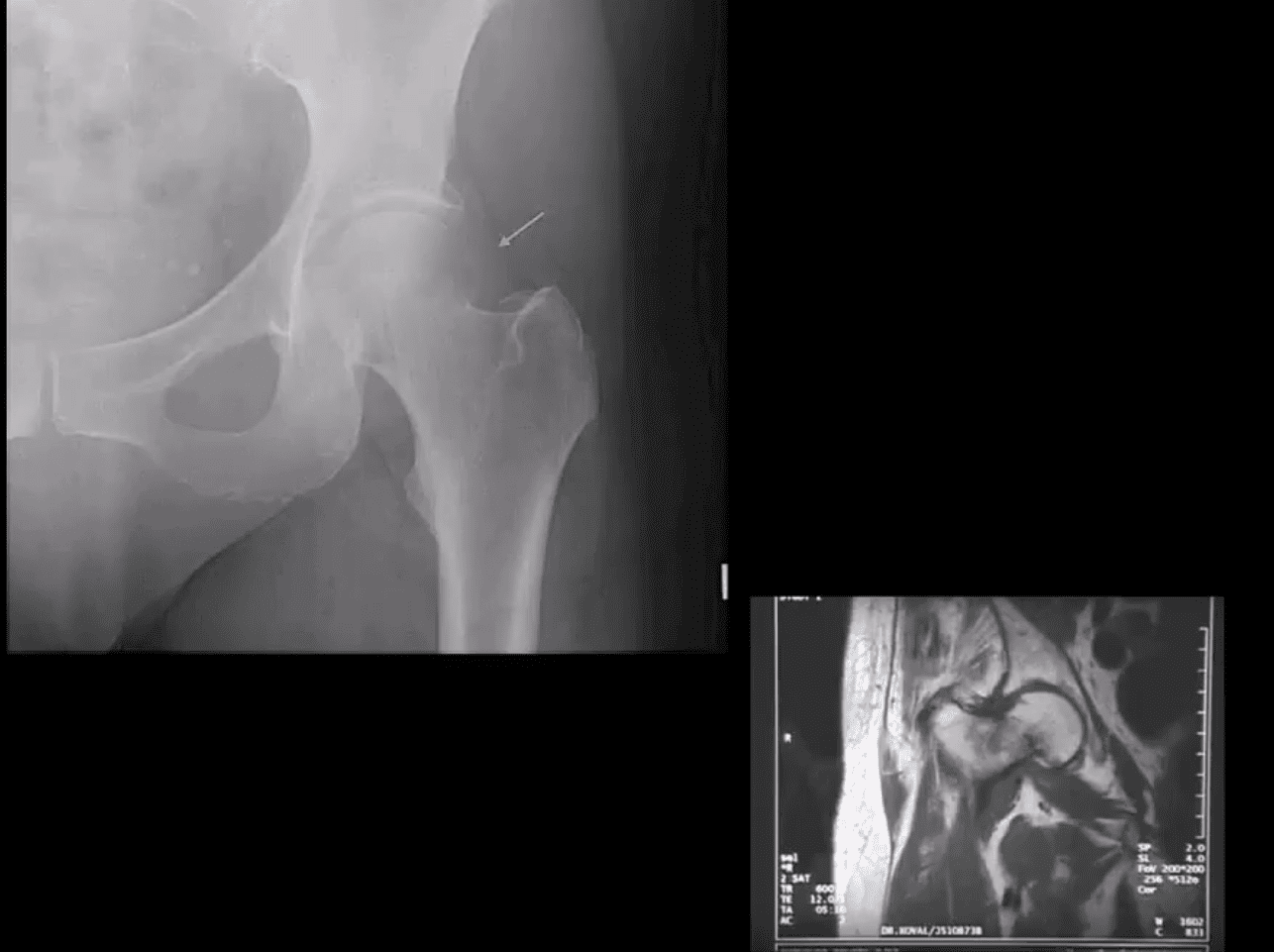
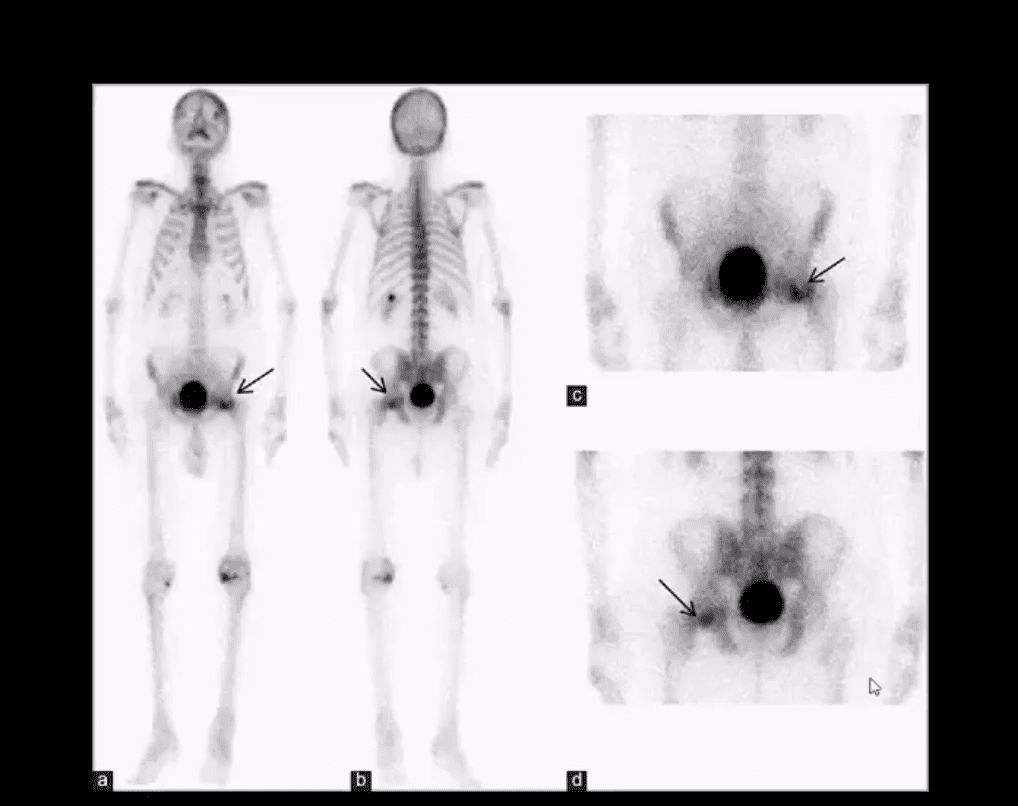
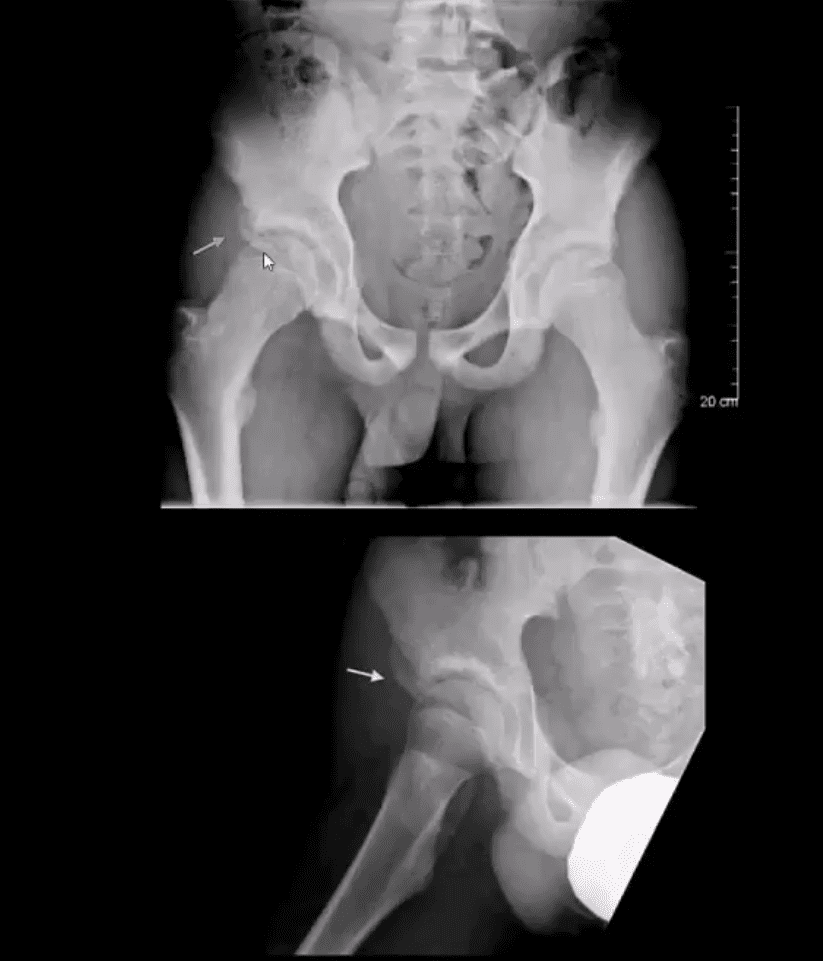
AP hip spot view: note valgus deformity of the head (above yellow arrow) with a small/subtle line of sclerosis in the sub-capital region representing Garden 1 Fx. MRI may help with Dx of subtle radiographic Fxs. If MRI contraindicated, Tc 99 radionuclide bone scan may help demonstrate high uptake of the radiopharmaceutical in Fx (below image)
Above – Tc99 Radionuclide Bone Scan Reveals Left Subcapital Femoral Neck Fx
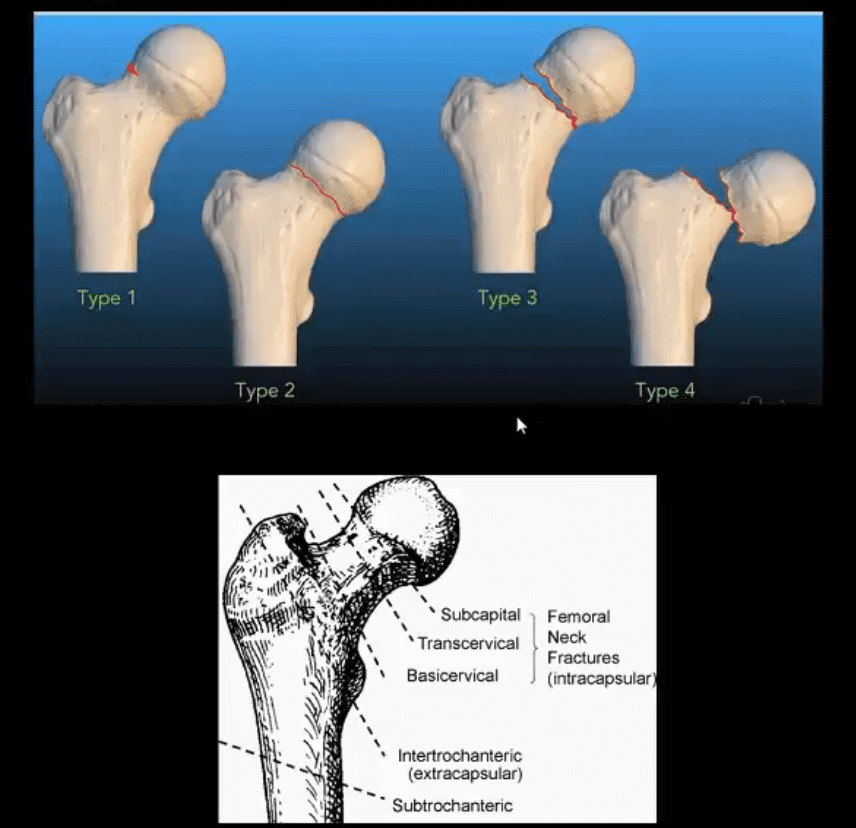
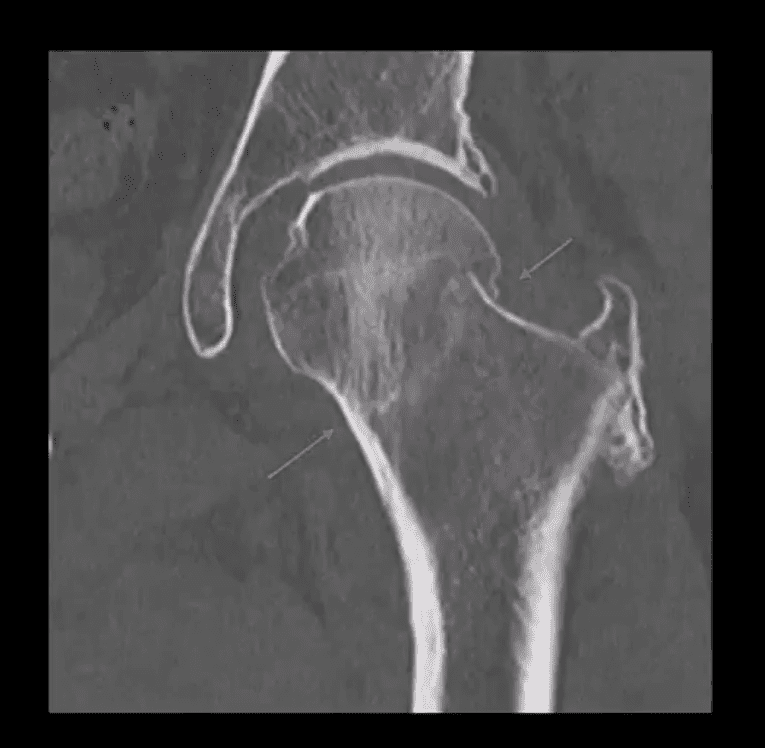
Garden 2 complete undisplaced (above green arrows) Fx
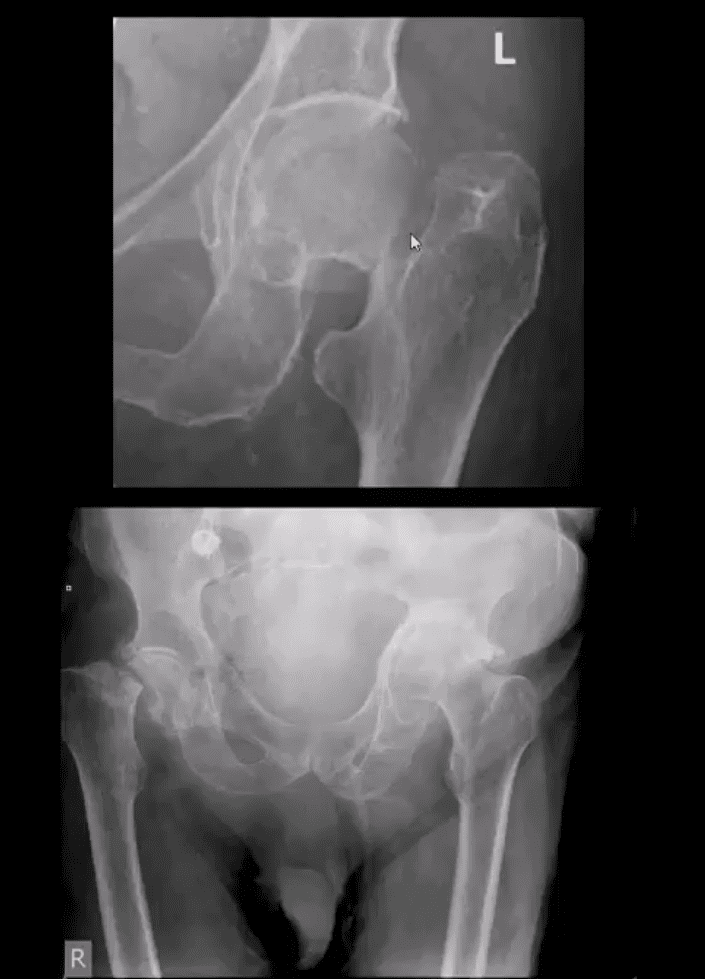
AP hip: Garden 3 complete partially displaced Fx (above the first image)
AP pelvis: complete displaced Garden 4 Fx (above the second image)
Clinical pearls: in some cases of Garden 4 Fx, DDx may be difficult to differentiate from OSP vs. pathologic fx d/t to bone Mets of Multiple myeloma (MM)
Management: depends on patients age and activity level
Garden 3 & 4� require total hip arthroplasty in patients <85-y.o.
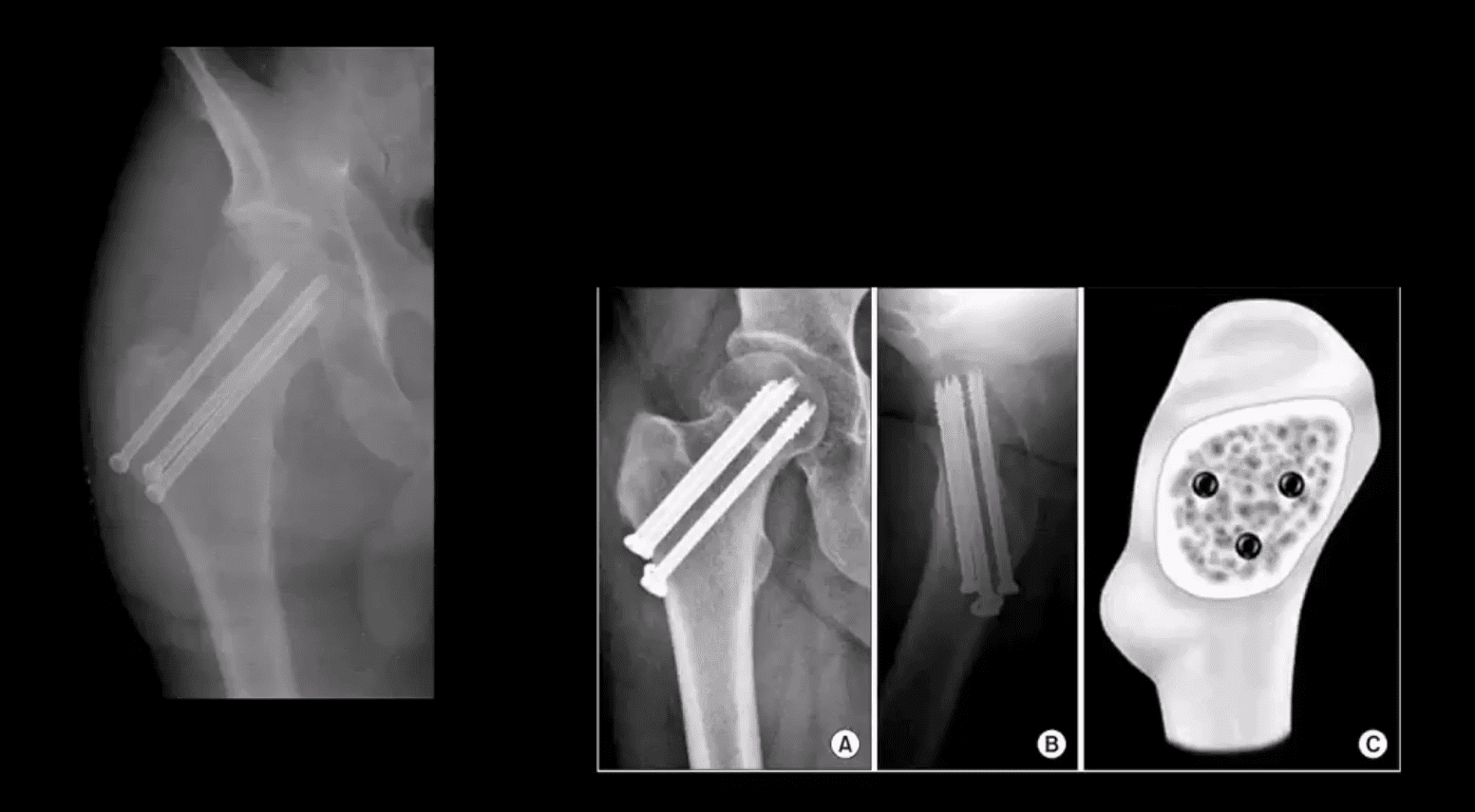
Garden 1 & 2 may be treated with closed reduction of fx and open capsule and 3-cannulated fixating screws
Pre-existing DJD may require total arthroplasty
Occasionally observation may be performed on patients who are not active and significant risks of surgery and depends on surgical centers
m/c Rx of Garden 1 & 2 undisplaced Fx with 3-screws. Screws proximity depends on the bone quality and Fx type
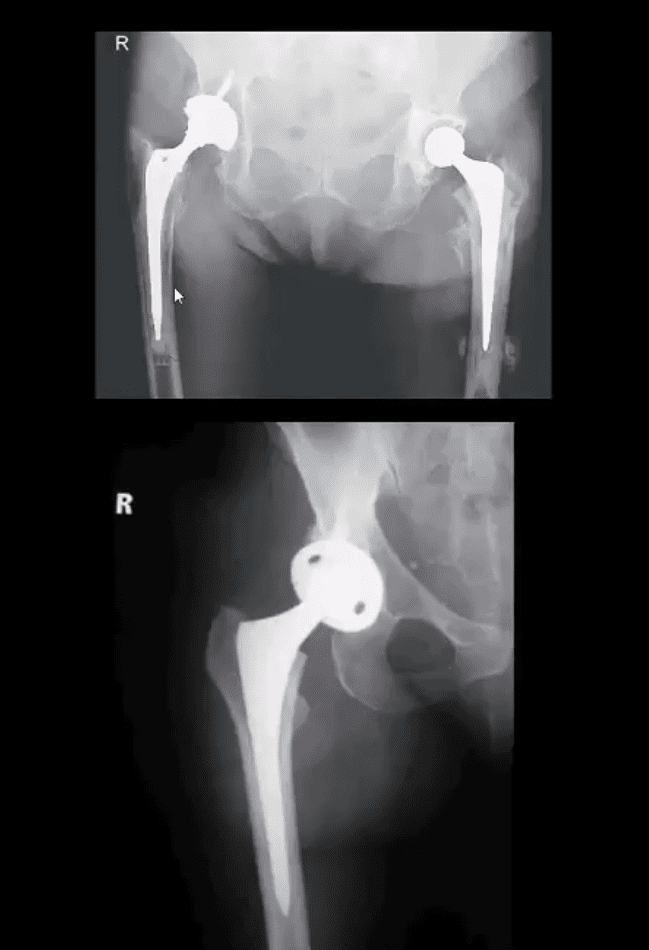
THA aka hip replacement: cemented THA with bone cement (above the first image) vs. non-cemented (biologic) that is used mostly in younger patients
2-types: metal on metal vs. metal on polyethylene
The femoral angle of the prosthesis should have slight valgus but never >140 degrees
The non-cemented component uses porous metal allowing the bone to integrate sometimes coating in bone cement from osteoconduction
THA has good outcome and prognosis
Occasionally cement failure, fractures, and infections may complicate this procedure
Hip fractures are characterized as any type of break in the upper region of the femur or thigh bone. The variety of broken bones generally depends on the circumstances and the force applied to the bone, where some can be more common than others. Impacted femoral neck fractures are common hip fractures which occur in many older adults in the United States.
Anatomy of Impacted Femoral Neck Fractures
The hip is a ball-and-socket joint which provides the femur the ability to bend and rotate at the pelvis. While any form of broken bones in the thigh bone or femur is considered a hip fracture, damage or injury to the socket, or acetabulum, itself is not considered a hip fracture. Below we will discuss hip fractures, particularly impacted femoral neck fractures, among others.
Causes, Symptoms and Diagnosis
Hip fractures frequently�occur due to a slip-and-fall accident or due�to a direct blow to the hip. Various health issues, including osteoporosis and stress injuries, as well as cancer, can sometimes weaken the bones and make the pelvis more vulnerable to fractures.�The neck of the femur is located under the ball of the hip joint. Impacted femoral neck fractures occur when a force presses against both ends of the femur at the femoral neck, pushing the broken ends of the bone together.
Patients with hip fractures experience symptoms of pain on the upper thigh or in the groin. They may also experience considerable discomfort with any attempt to flex or rotate the hip. In comparison to impacted femoral neck fractures, if the bone is completely broken, the leg may appear to be shorter than the non-injured leg. Also, the patient will hold the injured leg in a still position with the foot and knee turned outward in external rotation.
Diagnosis�for hip fractures commonly involves the use of x-rays of the hip, pelvis and/or femur. In several instances, if the patient experiences a slip-and-fall accident or a direct blow to the hip resulting in impacted femoral neck fractures, they may not be seen on a regular x-ray. Magnetic resonance imaging, or MRI, may be recommended to view some cases of hip fractures. The MRI scan will typically demonstrate any hidden hip fractures. Computed tomography, or CT, scans may also be utilized instead.
Impacted femoral neck fractures are hip injuries which occur just below the femoral head, or the ball-and-socket hip joint, where the broken ends of the bone are jammed together by the force of the injury. This area of the thigh bone, or femur, is known as the femoral neck. Treatment for impacted femoral neck fractures may include rest and physical rehabilitation. Diagnosis for impacted femoral neck fractures is important for treatment.
Dr. Alex Jimenez D.C., C.C.S.T.
Treatment of Impacted Femoral Neck Fractures
Once a healthcare professional has diagnosed the patient’s hip fracture, their overall health and wellness will also be evaluated.�Treatment for femoral neck stress fractures depends on the patient’s age and on the extent of the broken bone. Treatment for femoral neck stress fractures�include bed rest for several days followed by a physical rehabilitation program.
Many femoral neck stress fractures are treated with surgery. It’s essential for the patient to talk to their doctor to discuss the best treatment option.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Chiropractic for Athletes with Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain is the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Grateful for the treatment they have received for their injuries and conditions, many patients highly recommend Dr. Alex Jimenez, doctor of chiropractic, for a variety of health issues. Chiropractic care is an alternative treatment option which focuses on the diagnosis, treatment, and prevention of injuries and conditions associated with the musculoskeletal and nervous system. Dr. Alex Jimenez’s patients describe how much chiropractic care has improved their overall health and wellness, changing their quality of life for the best. Dr. Alex Jimenez is the recommended non-surgical treatment choice for a variety of health issues, including neck and back pain, among others.
El Paso, TX Chiropractor�Recommended
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
Unstable Fx: a result of high energy trauma with >50% d/t MVA
20% closed Fx and 50% of open Fx result in mortality
Mortality is associated with vascular and internal organs injuries
Vascular injury: 20% arterial 80% venous
Chronic morbidity/disability and prolonged pain
Unstable Fx are rarely seen in the outpatient setting and typically and present to the ED
Stable pelvic Fx are usually caused by muscles/tendons avulsions and more often seen in pediatric cases
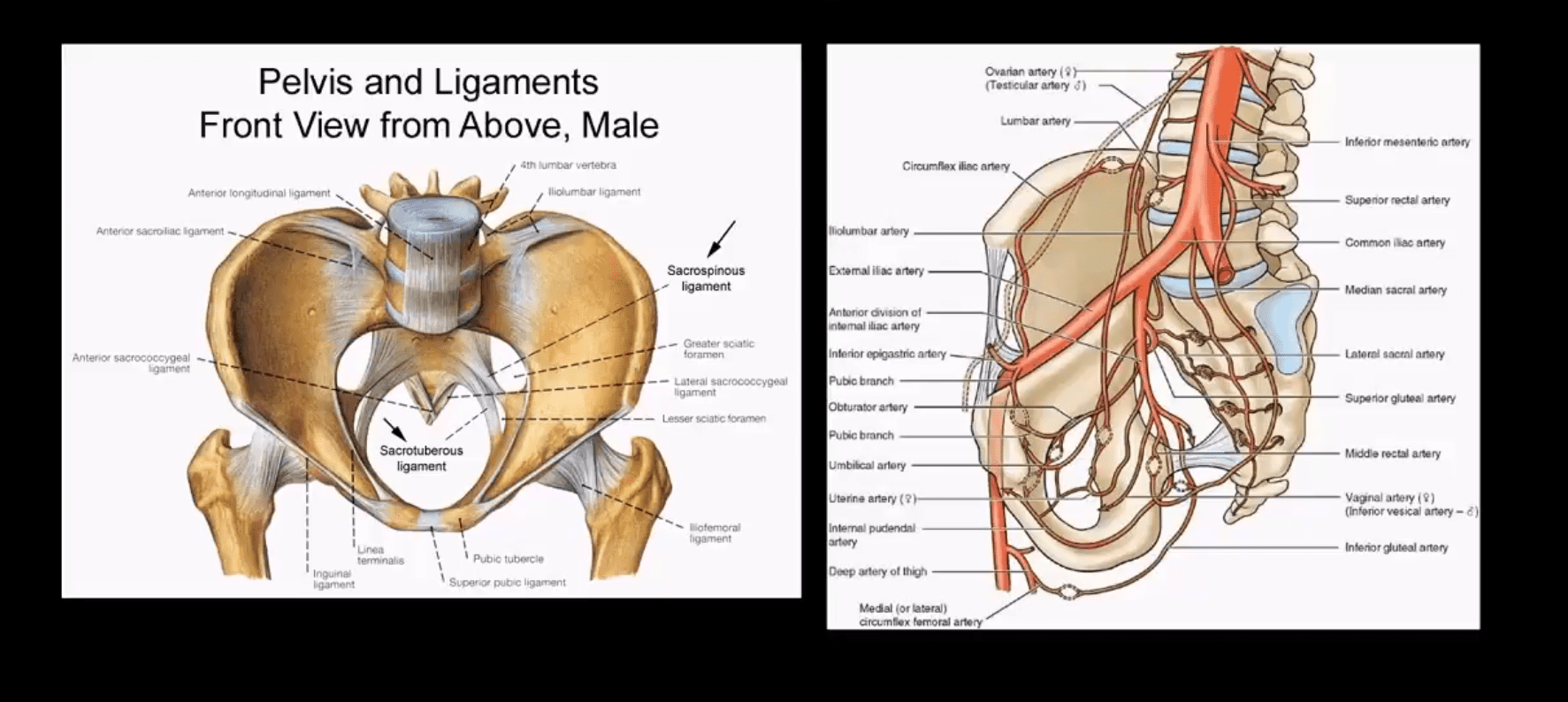
Understanding Pelvic Anatomy Is The Key To Successful Imaging Dx
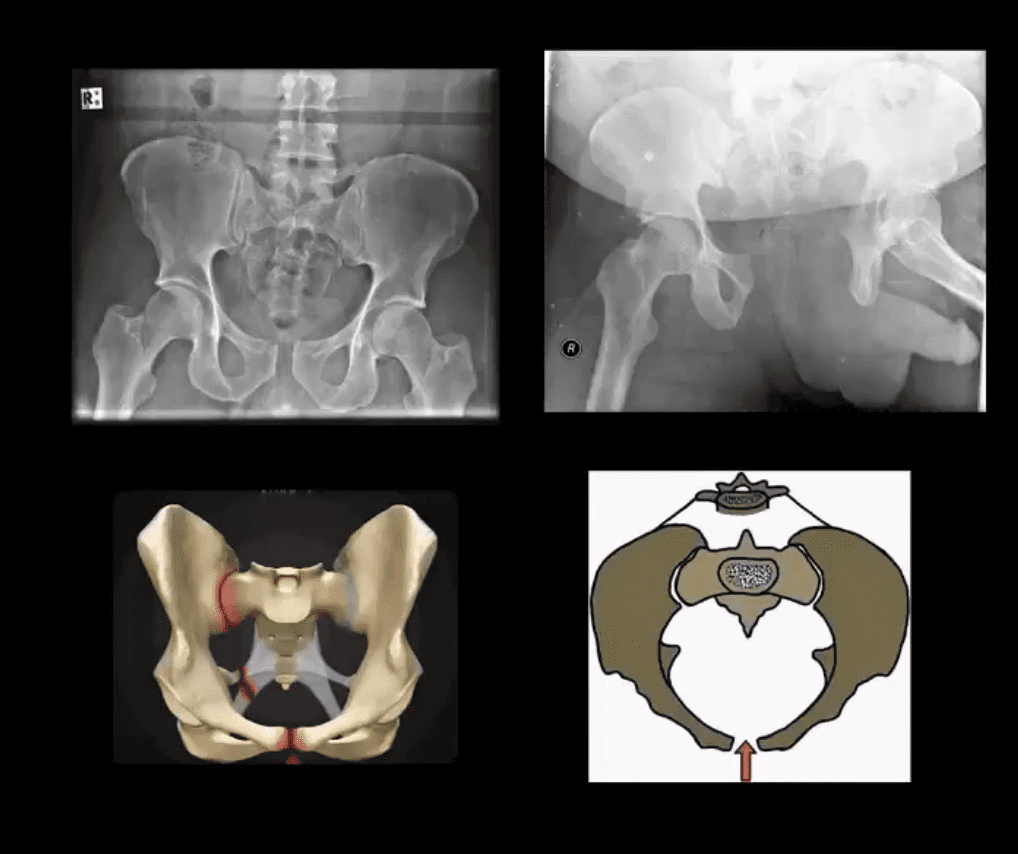
The bony pelvis is a continuous ring of bone held by strong ligaments
During significant impact, pelvic fractures may occur in more than one location because forces applied to one region of the ring will also correspond to injury on the other, usually the opposite side of the ring (above image)
Thus the majority of unstable pelvic Fx will typically demonstrate more than one break
Pelvic is seen as a ring of� bone connected by some of the strongest ligaments in the body
The pelvic ring comprises 2-semirings: anterior to the acetabulum and posterior to the acetabulum
The bony pelvis is in close proximity to major vessels carrying a greater chance of vascular injury
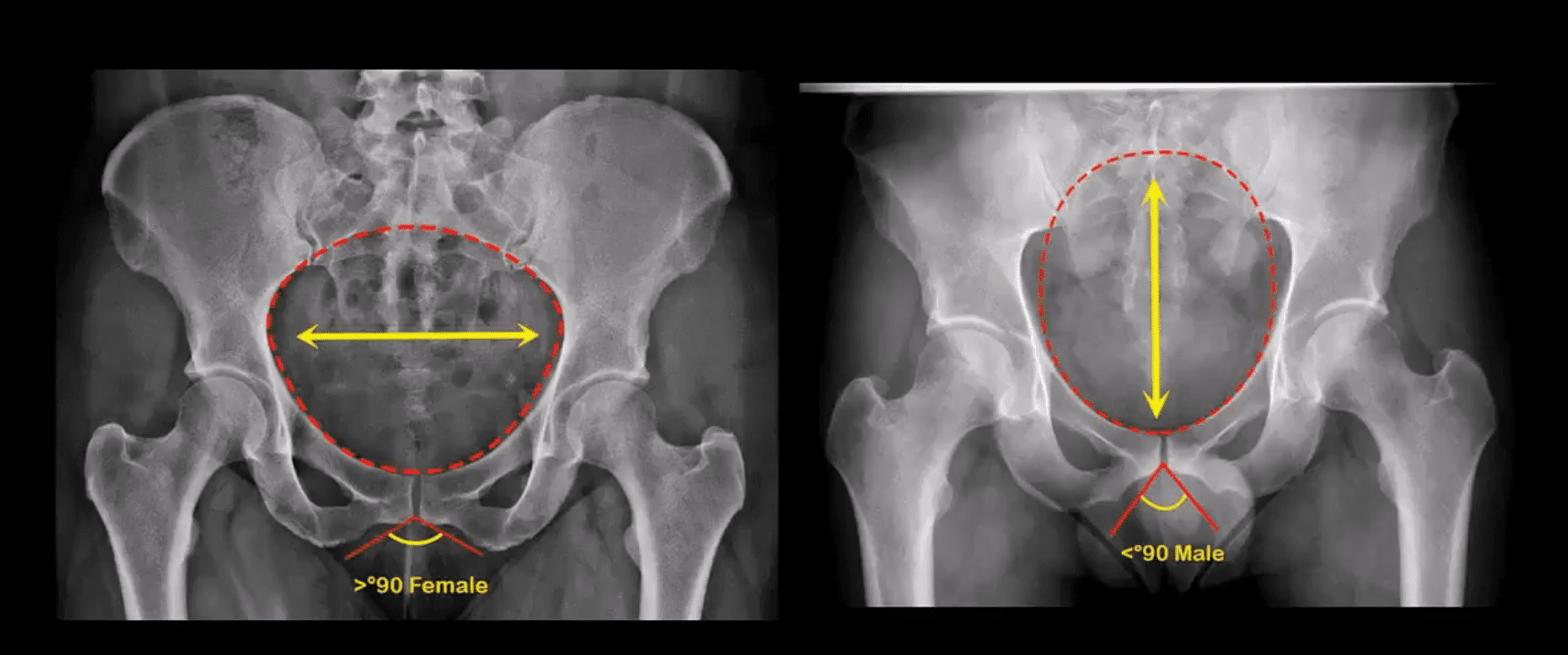
Anatomical Differences of The Female and Male Pelvis
Post-Traumatic Pelvic Views May Vary and Include:
Standard AP Pelvis (above images)
Judet views evaluating the acetabulo-pelvic region
Inlet/Outlet views helping with the symphysis and SIJ regions
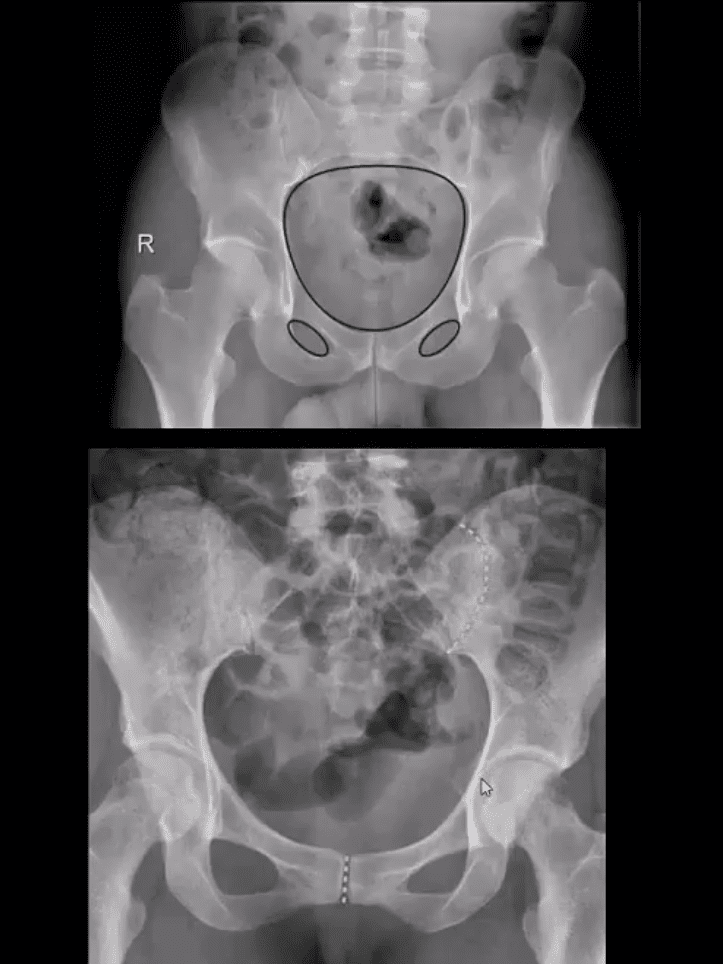
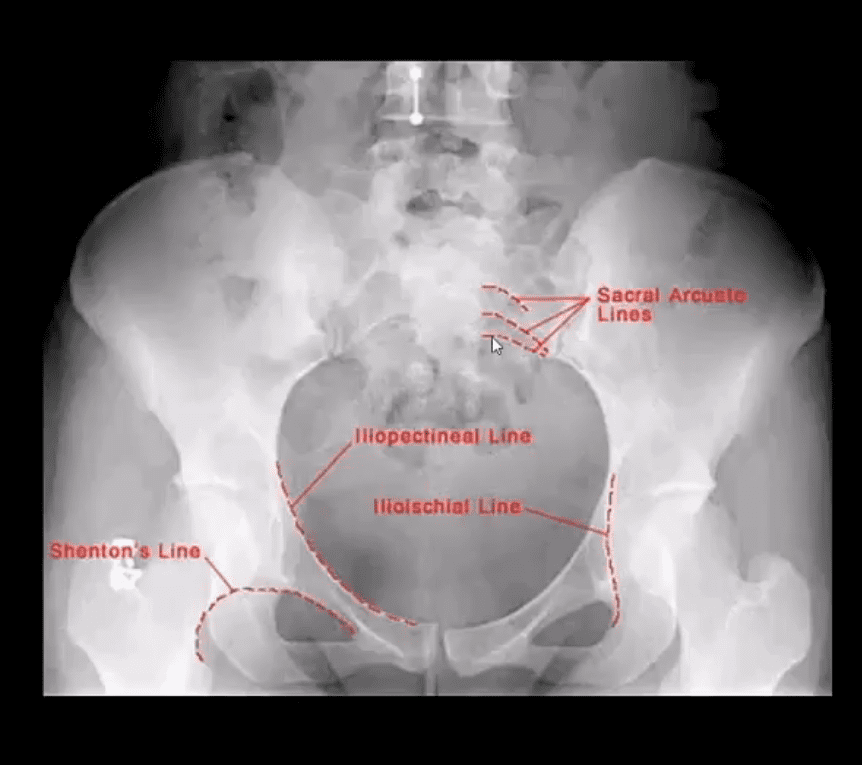
Rad survey of the pelvis should include evaluation of the continuity of pelvic rings:
Inlet/outlet, obturator rings (above the first image)
Symphysis pubis and SIJ for diastasis and post-trauma separation (above the second image)
Lumbosacral spine and hips should also be carefully examined
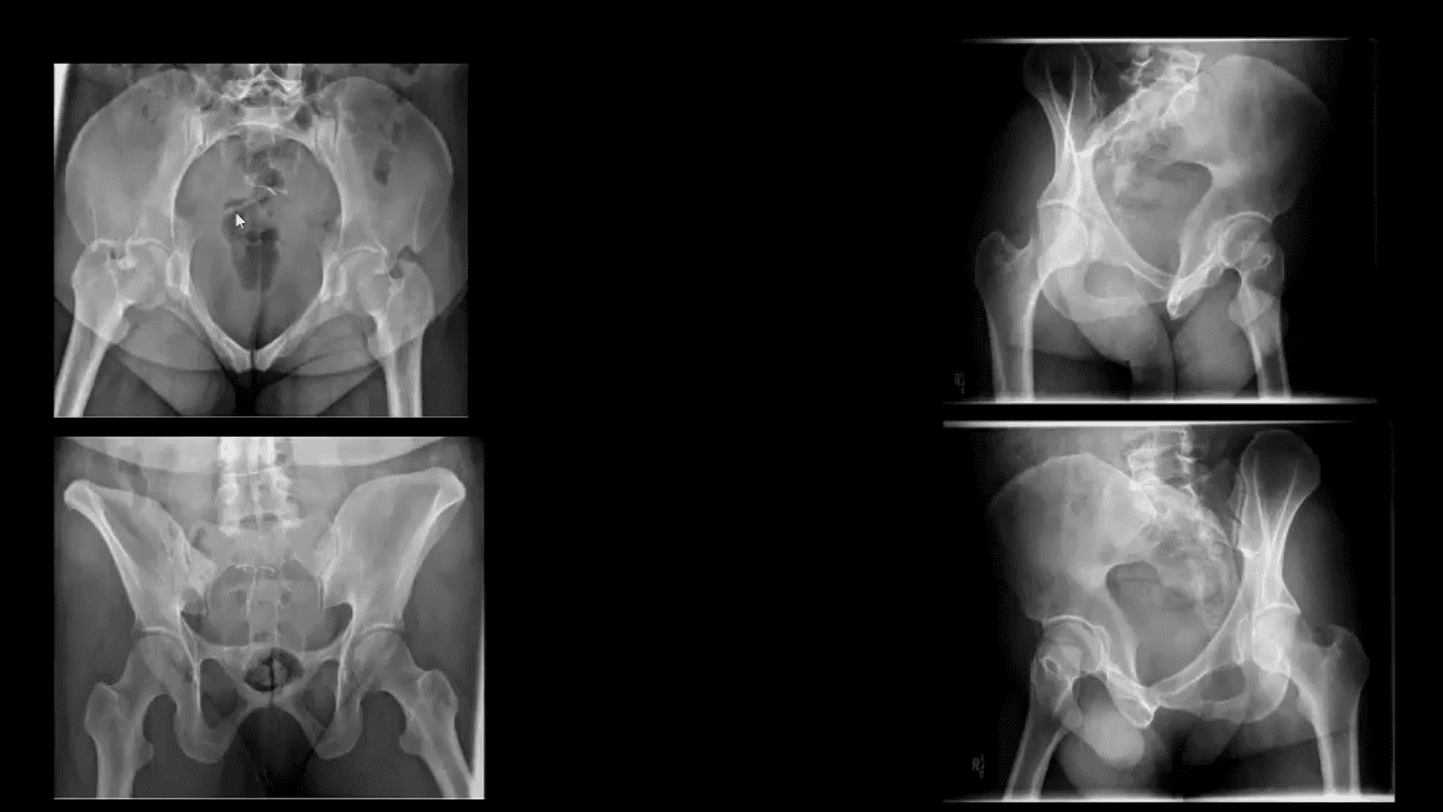
Pelvic inlet (above top left) and Outlet (above bottom left)
Judet views: left and right posterior oblique views
Additional Survey:
Iliopectineal, ilioischial, Shenton and Sacral arcuate lines will help detection of sacral, acetabular and hip fracture/dislocations
Stable Pelvic Fractures aka Avulsion Injury
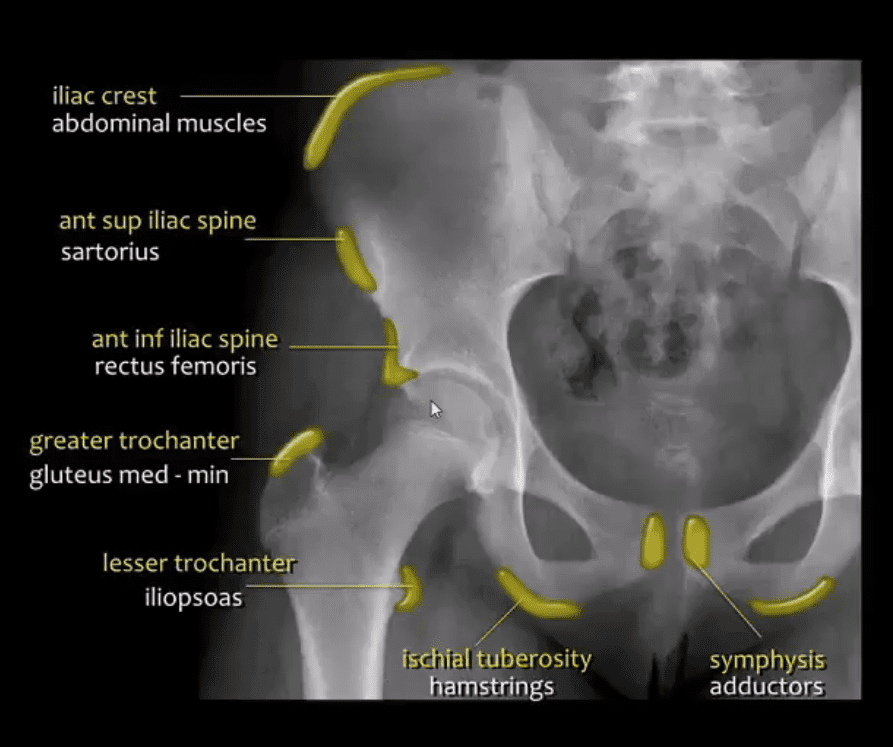
Appreciating anatomical sites of pelvic origin/insertion of different muscles will help Dx of pelvic avulsion Fx
Avulsion Fx of the AllS (origin of the direct head of Rectus femoris M)
Pelvic avulsions occur by sudden eccentric contraction especially during kicking or jumping
Imaging: x-radiography will suffice
Clinically: sudden snap or pop followed by local pain. Pt can weight bear
Care: non-operative with rest for 4-weeks. Non-union is rare. No major complications
DDx: key rad DDx feature is not to mistake an avulsion from an aggressive pediatric bone tumor-like osteosarcoma that may show some exuberant new bone formation d/t healing and bone callus
Commonly Encountered Unstable Pelvic Fractures
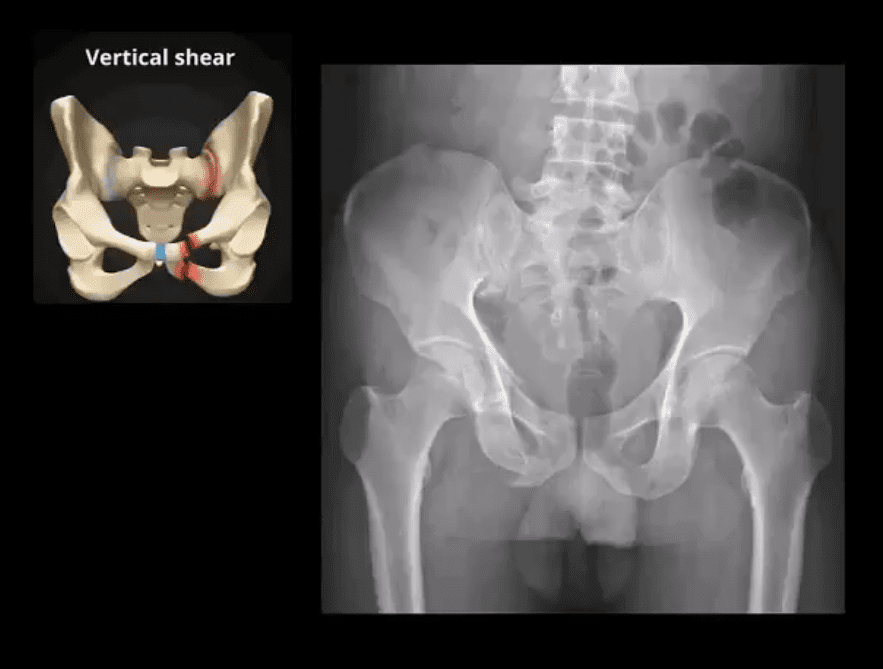
Malgaigne Fx: d/t vertical shear injury to the ipsilateral pelvis
Rad Dx: ipsilateral superior and inferior pubic rami Fx (anterior ring) with ipsilateral SIJ separation/Fx of the sacrum and adjacent ilium (posterior ring). Symphysis pubis diastasis can be seen. An additional clue is an avulsion of L4 and/or L5 TP that often signifies serious pelvic injury
Clinically: marked leg shortening, shock, inability to weight bear.
Damage to Superior Gluteal Artery can occur
Imaging: x-radiography followed by CT scanning w/o and with IV contrast esp. if visceral injury present
Care: surgical in most cases d/t significant instability. ORIF. Hemostasis, Pelvic stabilization
Prognosis: depends on the complexity, rate of visceral complications and stability. 10% Superior glut artery bleed requiring rapid hemostasis
Open Book Pelvis (major instability)
Mechanism: AP compression of different force magnitude (picture depiction)
Rad Dx: diastasis of symphysis pubis with diastasis of SIJ with and w/o adjacent Fx of the ala
Imaging steps: x-radiographic, CT scanning with and w/o contrast for vascular injury, cystography for acute urinary bladder rupture
Immediate and delayed complications may occur: vascular injury, urethral/bladder injury
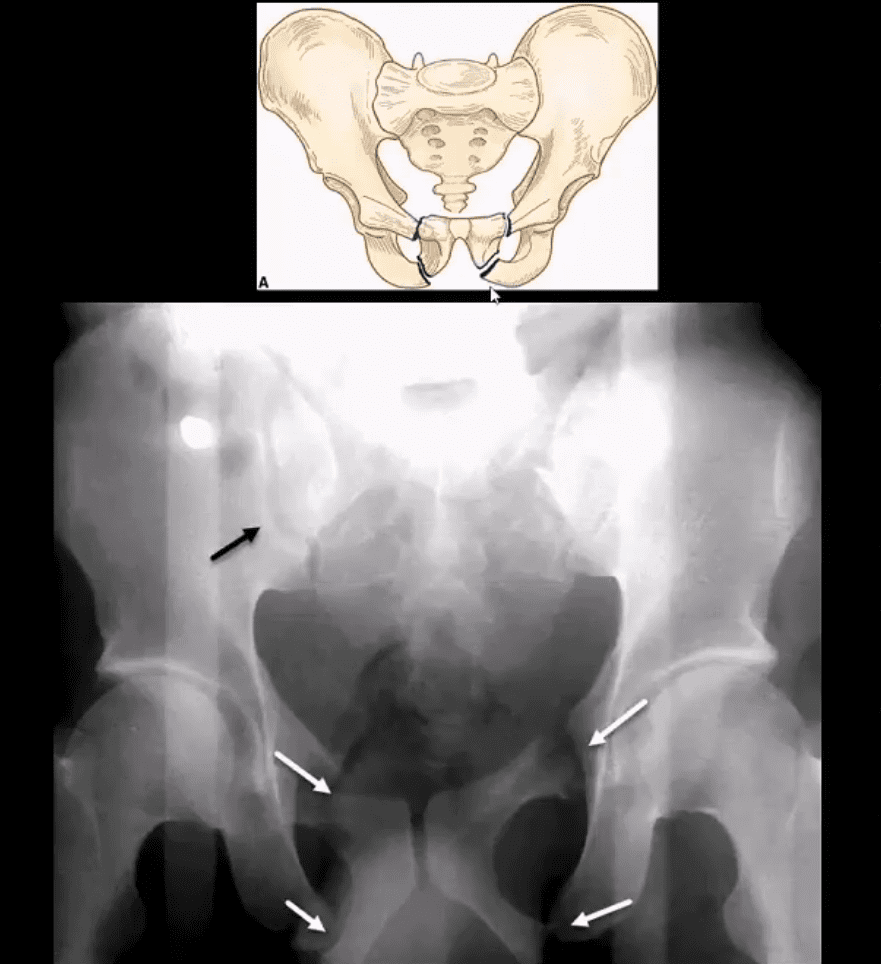
Straddle Injury: Unstable Fx
Mechanism: direct impact/collision
High risk of urinary bladder/urethral injury
Imaging: bilateral superior and inferior pubic rami Fx with or w/o diastasis and Fx of SIJ
CT with and w/o contrast for vascular injury
Cystourethrogram additionally evaluates a urogenital injury
2) Osteoporotic patients with low impact, trivial or no trauma (i.e., insufficiency Fx)
X-radiography is crucial to early Dx and prevention of complications which include:
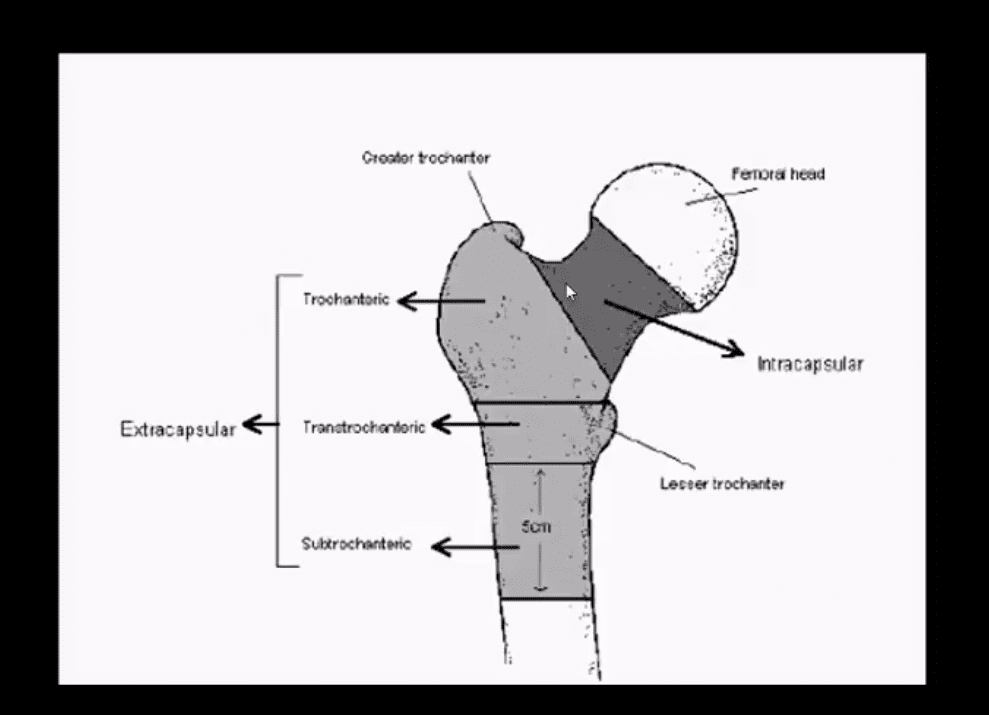
Dx: intra-capsular vs. extra-capsular Fx
Ischemic osteonecrosis aka avascular necrosis (AVN) of the femoral head and rapid disabling DJD
Epidemiology: USA has some of the highest rates of OSP hip Fx worldwide. Highest healthcare cost Fx to treat overall
Women>men, Caucasians>African-Americans
25-30% mortality within the 1st year. Mortality depends on co-morbidities and stat of activity prior Fx
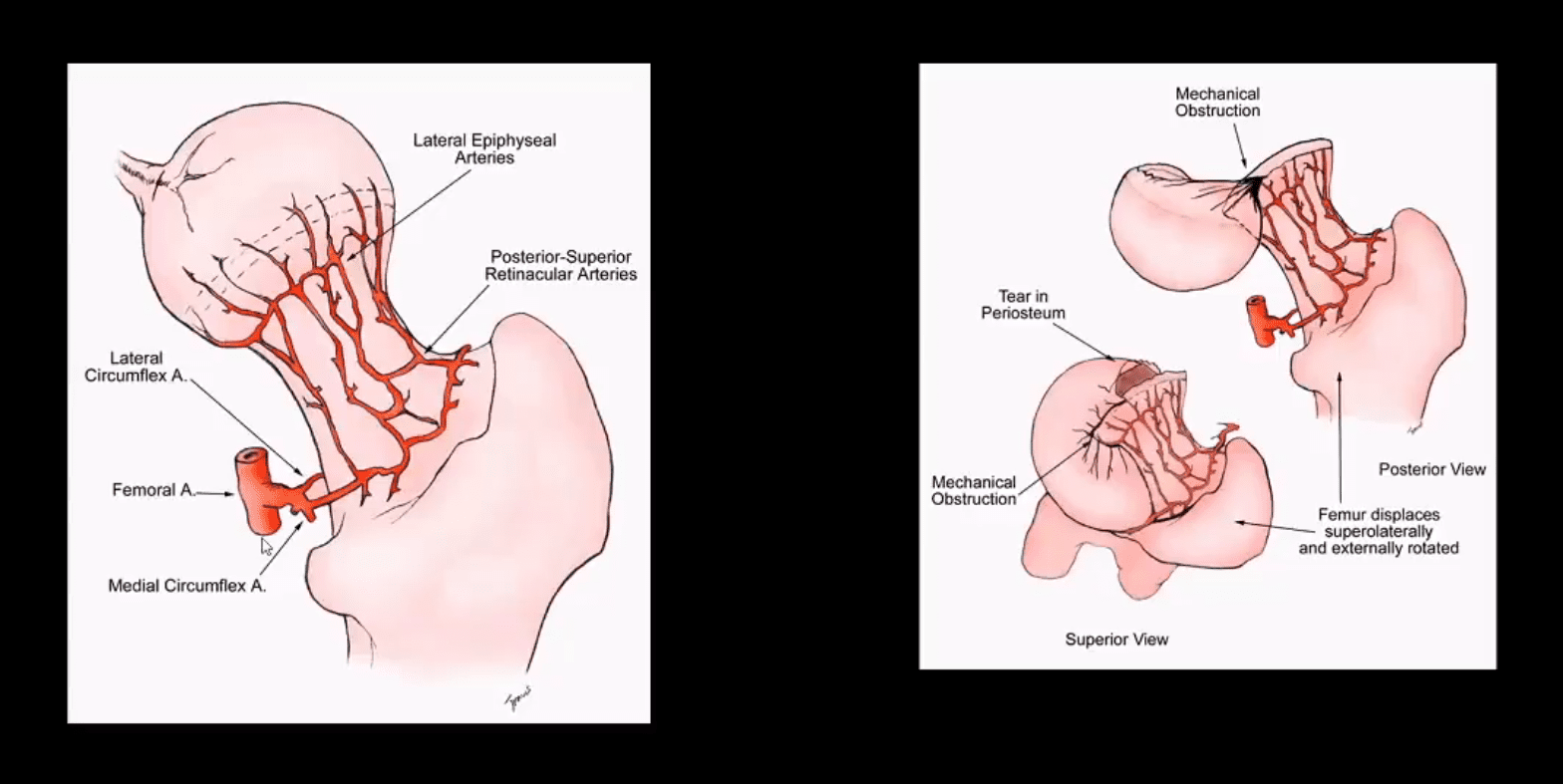
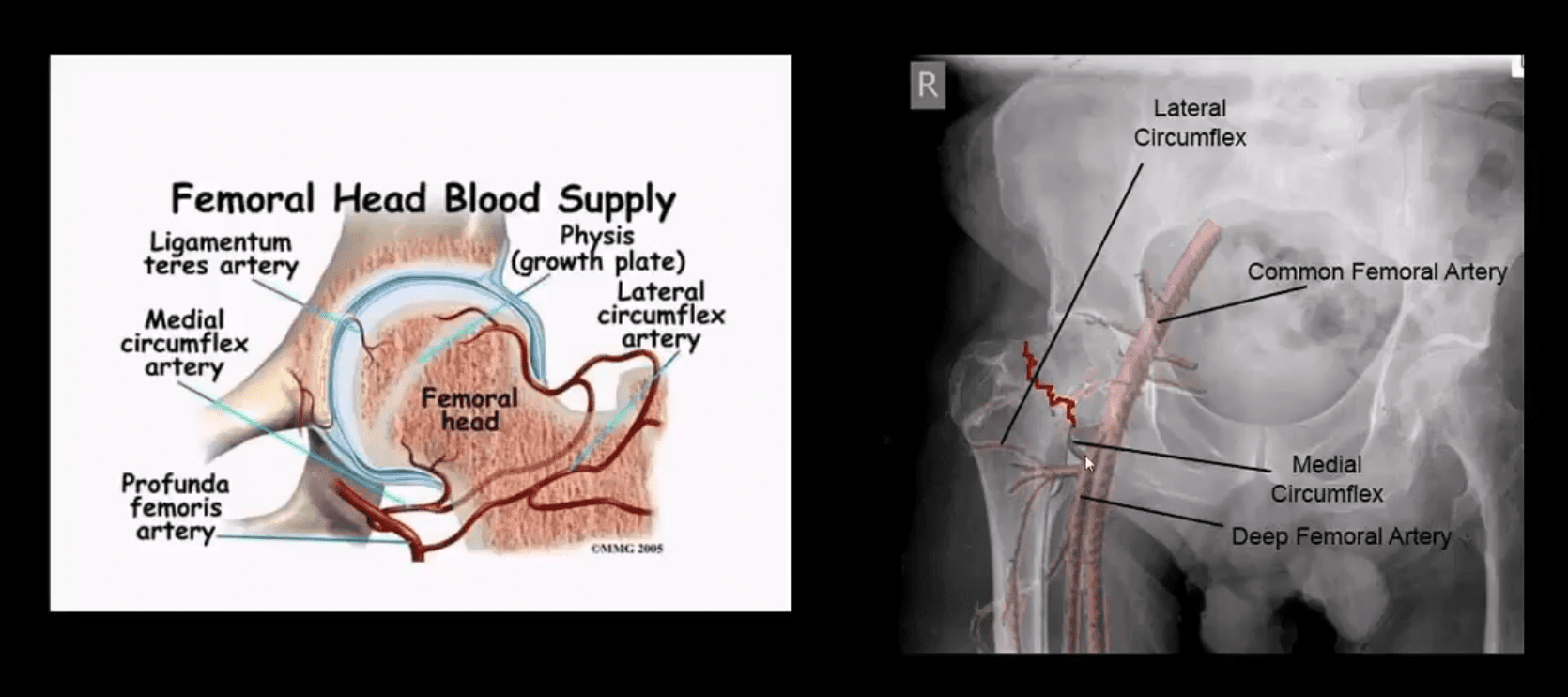
Pathophys: the femoral neck is intra-capsular and transmits arterial flow to the head. The neck is uncovered by the periosteum and unable to develop a good callus. The neck transmits maximum tensile forces through the proximal femur and prone to Fx and non-union
The hip is a ball-and-socket joint composed of the head of the thigh bone, or femur,�which acts as the ball and fits into the round socket of the hip bone, or acetabulum. The neck of the femur is located under the ball of the hip joint. Stress fractures to the femoral neck can entirely or partially detach the femoral head from the rest of the femur.
Femoral neck stress fractures can be either displaced, where the bone is transferred out of its normal position, or non-displaced, where the bone remains stable. These fractures may interrupt blood flow to the portion of the broken bone. In recovery, the blood supply prevents severely displaced femoral neck stress fractures from healing correctly.
Causes and Symptoms of Femoral Neck Stress Fractures
Femoral neck stress fractures can result due to: a small slip-and-fall accident or twisting of the hip in older adults, osteoporosis, a high-impact�injury, such as from an automobile accident, and�sudden strenuous physical activity or changes in physical activity in younger individuals unaccustomed to the events, including from sports injuries.�
The symptoms of femoral neck stress fractures generally include: pain and discomfort, radiating pain which extends to the knee, inability to bear weight on the affected lower extremity, shortening or sideways rotation of the leg, increased pain in the hip during the rotation of the leg, and inflammation on the side of the hip with the femoral neck stress fractures.
Diagnosis and Treatment of Femoral Neck Stress Fractures
A healthcare professional will diagnose femoral neck stress fractures based on the causes and symptoms of the health issue, followed by clinical evaluation. Many doctors order x-rays to diagnose femoral neck stress fractures. The doctor may also order�magnetic resonance imaging, or MRI, and computer tomography, or CT, scanning for a better diagnosis.
Treatment for femoral neck stress fractures depends on the patient’s age as well as on the extent of the broken bone. Treatment for femoral neck stress fractures may include�bed rest for several days followed by a physical rehabilitation program. A healthcare professional may prescribe drugs and/or medications to relieve pain, prevent blood clots and treat infection.
Many femoral neck stress fractures are treated through surgical interventions. Surgery for femoral neck stress fractures involves hip pinning if the bone is minimally displaced and the patient has�enough bone density. The surgeon performs this by making a small incision and then inserting several screws to stabilize the bones which are broken.
Hip hemiarthroplasty or partial hip replacement is utilized for displaced fractures where the surgeon will replace the�femoral head with a metal implant. The socket is not replaced in a partial hip replacement procedure. For total hip replacement, the surgeon will replace the socket of the hip joint, as well as the femoral head, with artificial metallic implants.
�
Femoral neck stress fractures are hip injuries which occur just below the femoral head, or the ball-and-socket hip joint. This area of the thigh bone, or femur, is known as the femoral neck. Femoral neck stress fractures happen when the ball is disconnected from the rest of the femur, or thigh bone. Treatment for this health issue includes rest and physical rehabilitation.
Dr. Alex Jimenez D.C., C.C.S.T.
Conclusion
Femoral neck stress fractures occur�in the hip area below the ball-and-socket joint of the hip. A healthcare professional will suggest treatment based on the severity of the femoral neck stress fractures and the patient’s age.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Chiropractic for Athletes with Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain is the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine