Standing on your feet for extended periods, whether it’s a result of work or due to participation in physical activities and exercise, can cause a variety of health issues, including back pain. Patients discuss their symptoms as they describe how these have significantly affected their everyday lifestyles. Effective chiropractic care with Dr. Alex Jimenez has helped provide safe and effective pain relief for a variety of health issues. Patients highly recommend Dr. Alex Jimenez as the non-surgical choice for back pain, among other ailments.�
Chiropractic Therapy
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of every one of my patients.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
An individual’s everyday physical activities can be affected when confronted with debilitating symptoms. Patients clarify how their different injuries and conditions shifted their quality of life, interrupting their daily tasks. Dr. Alex Jimenez has helped provide patients with the pain relief they deserve for their particular health problems. The patients describe the improvements they have experienced through chiropractic care, recommending Dr. Alex Jimenez as the non-surgical selection for pain relief.
Chiropractic Treatment & Relief
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
The lumbar spine, or lower back, takes a lot of stress and strain throughout the day. The spine provides stabilization for the entire body, and the lumbar spine bears the brunt of much of the movement and activity. This wear and tear show up as lower back pain in many people. The American Chiropractic Association estimates that 31 million Americans have low back pain at some point in their lives. The leading cause of disability is low back pain � not only in the U.S. but worldwide.
What is the Lumbar Spine?
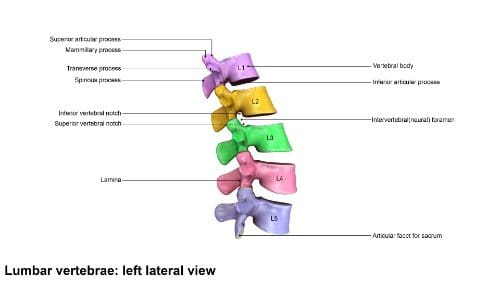
Located in the lower back area, the lumbar region is the portion of the spine that begins below the shoulder blades, about five or six inches, at the lordosis (where it curves in toward the abdomen). Five vertebrae make up the lumbar spine, L1 through L5 � which also happen to be the largest unfused vertebrae in the entire spinal column. The lower vertebrae bear more weight than the upper vertebrae, so they are constructed to be sturdier, but are also more prone to injury and degradation.
The L5 vertebra meets the S1 (the sacrum) at the lumbosacral joint. It is this joint that provides most of the range of motion including rotational flexibility of the hips and pelvis, allowing them to swing during movement such as running and walking.
The spinal cord ends at around the L1 and many nerve roots that originate at the spinal cord form what is called the cauda equine. These nerves travel down the spine, branching out to the legs, buttocks, and feet. The appearance resembles a horse�s tail, hence the name. Because the spinal cord does not extend into the lumbar area, the chance of a problem with the lower back resulting in paralysis or damage to the spinal cord is very rare.
Lower Back Pain
The most common causes�of lower back pain are soft tissue injuries and mechanical problems. Either of these can damage the intervertebral discs, compress the nerve roots, and inhibit the�correct function of the spinal joints so that they don�t move properly. Lower back pain is most commonly caused by a pulled or torn muscle or ligament, known as a sprain or strain. These injuries can have some causes, including:
Prolonged improper posture
Improper lifting of something heavy (without using your legs)
Sports injuries, particularly those where the player sustains high impact or where a lot of twisting is involved
Lifting while twisting the spine
A fall or movement that occurs suddenly and puts a great deal of stress on the lumbar area
Chiropractic Care for the Lumbar Spine
Chiropractic care is a prevalent, effective treatment for lower back pain. A chiropractor can help patients manage their back pain through spinal adjustments and lifestyle advice. They may recommend supplements, exercise, and dietary changes. The whole-body approach to chiropractic makes it an optimal choice for many people, especially those who don�t want to take medications or undergo invasive procedures.
The chiropractic treatment itself usually involves spinal manipulation and mobilization. Spinal manipulation is the technique that most people think of when they think of chiropractic. It of a short lever, high-velocity arm thrust applied directly to the vertebra that is injured or is causing the pain. This technique typically relieves pain, improves the function of the spine, and restores the back�s range of motion. Mobilization is a low-velocity movement performed by the chiropractor to manipulate the area, stretching and moving the joints and muscles.
These techniques typically restore range of motion and flexibility to the spine while reducing pain. For people with chronic lower back pain, chiropractic care can be a game changer.
Every year an estimated 3.8 million people in the United States sustain mild traumatic brain injuries (MTBI) or concussions. Many of these injuries are due to sports-related activities, work related injuries, motor vehicle accidents, and military operations. It is also estimated that as many as 50% of MTBIs are never reported because the patient does not seek medical attention. This makes it difficult to get a substantial number on how many there are, but it is a prevalent condition.
The Brain and Skull
A patient does not have to hit their head to sustain an MTBI. It can be caused by whiplash even though the person never hit their head. The reason for this lies in the construction of the brain and skull.
The brain is very soft; some experts compare the texture to that of soft butter. The skull is designed to protect the brain, and it is tough. If you run your hand over your head, you may feel some lumps and bumps, it may not feel entirely even, but the surface will be smooth.
The same cannot be said for the inside of the skull. There are boney ridges on the inside that are quite sharp. The design is intended to keep the brain in place.
When the head is hit or is jolted hard enough it caused the brain to shift inside of the skull, coming into contact with those boney ridges � sometimes forcefully. This can cause damage and the result in a brain injury. The harder the jolt, the more serious the injury may be.
Symptoms of Mild Traumatic Brain Injury
Part of the problem with MTBI is that the symptoms may not show up immediately. They could emerge weeks or even months after the incident making it unlikely that the symptoms will be tracked back and connected to it.
Often, MTBI is called a �silent epidemic� because the symptoms that it causes are usually not visible and may not be immediately connected to the injury. Depression, anxiety, angry outbursts, and impaired memory are more likely to be considered a psychiatric issue instead of a neurological one. The symptoms can be debilitating just the same.
Evaluation and diagnosis of an MTBI
Chiropractors routinely treat patients with Mild Traumatic Brain Injuries. When they are presented with a patient that they know has sustained a head injury, or if they suspect a brain injury based on specific symptoms, they use the Sports Concussion Assessment Tool 2 (SCAT2) to determine the severity. The SCAT2 helps the chiropractor create evaluate the physical signs, symptoms, sideline assessment using Maddocks score, Glasgow Coma Scale, coordination, balance, and cognitive.
As they evaluate the patient, they look for specific markers that indicate the patient is experiencing worsening neurological symptoms. These include:
Loss of consciousness
Vomiting
Headaches get�worse
Increased confusion
Weakness on one side or in one leg or arm
Blurred vision
Dilated pupils
Balance or coordination problems
Chiropractic Treatment for MTBI
A head injury usually involves a neck injury as well. The chiropractor may use a variety of techniques to treat the patient, including spinal manipulation, massage, and bracing. The patient will also be advised to avoid anti-inflammatory medication, aspirin, alcohol, and sleep aids, using acetaminophen for pain as needed. If the patient needs to see another doctor or specialist, the chiropractor will refer them.
Neck pain is one of the most common sources of pain and chronic pain worldwide. According to the International Association for the Study of Pain, each year, around 30% to 50% of the general population experiences neck pain and approximately 15% will, at some point in their lives, have chronic neck pain. Women seem to experience it more often than men, and it is most prevalent at around middle age. Neck pain can be debilitating, impacting a person home life as well as their work performance. It can also trigger migraines and limit the range of motion. Understanding the cervical spine is integral in understanding how to manage pain in that area.
What is the Cervical Spine?
Seven vertebrae make up the cervical spine: C1 through C7. They protect the spinal cord and are part of the system that makes up the neck.
C1 is located at the base of the skull and C7 sits at the beginning of the thoracic spine. While C1 is the smallest vertebrae, each subsequent one is slightly larger as you move down the spine. This is necessary because the farther down the spine, the more weight it must bear.
The vertebrae C3 through C6 are called �typical vertebrae.� Like other vertebrae in the spine, they have a similar construction. The top vertebrae, C1 and C2, are �atypical vertebrae.� Their construction is somewhat different from typical vertebrae due to their specialized function and location.
The atlas, C1, is the only vertebrae that have more of a ring shape than a shape resembling a vertebra. It is what connects the skull to the spine and is responsible for about half of the head�s backward and forward range of motion.
The axis, C2, is the second vertebra and has a unique construction that connects it to C1 at the atlanto-axial joint. It is responsible for around half of the head�s rotation. The vertebra prominens, C7, is much larger than the vertebrae that sit above it and its shape is different to facilitate its connection to T1, at the beginning of the thoracic spine.
Neck Pain
The cervical spine has several critical functions. It houses the spinal cord and protects it, supports the head and facilitates its movement, and facilitates the flow of blood to the brain.
The human head is around 10 to 13 pounds and the cervical spine, along with an intricate network of muscles, tendons, and ligaments support it. This is what also allows flexibility to the head so that it can move up and down, backward and forwards, rotational, and side bending. This job alone puts a great deal of stress on the neck and can lead to neck pain. Common causes of neck pain include:
Whiplash (whipping the head forwards and then backward very suddenly)
Degenerative disc disease
Pinched Nerve
Age-related conditions
Spinal stenosis
Sleeping in certain positions
Neck strain
Osteoarthritis
Keeping the neck in one spot too long, such as looking down at a mobile device
Herniated disc
Neck injury
Fibromyalgia
Chiropractic Care for the Cervical Spine
A chiropractor will typically treat a patient with neck pain using cervical spinal manipulation, cervical spinal mobilization, or a combination of the two techniques. Cervical spinal manipulation is what most people think of regarding chiropractic treatment. It involves short, quick thrusts that focus on a single joint at a time, so that range of motion is returned to that area. Cervical spinal mobilization is a gentler, lower impact adjustment that does not use as much force but does move the joint to its correct position.
Other treatments the chiropractor may employ include the application of cold or heat, massage, and exercises to strengthen and stretch the neck. The doctor will carefully consider the patient, their lifestyle, habits, and current level of fitness then create a plan that is tailored specifically for them that will help them manage their pain and return flexibility and range of motion as quickly as possible.
Back pain can be debilitating. A patient can find they have trouble moving or engaging in regular activities like lifting their children or even walking. Pain in the mid to upper back can be caused by a variety of issues, and it can have a significant impact on a person�s quality of life. Many people see chiropractors to get relief from their back pain, but there are some things that chiropractic patients should know so that they can get the most out of their treatments.
What is the Thoracic Spine?
Twelve vertebrae make up the thoracic spine which is located just above the lumbar spine and just below the cervical spine. It is often referred to as the upper back. This part of the spine has several essential functions. The ribs connect with this portion of the spine, and it also is responsible for protecting the spinal cord.
The thoracic spine also differs from the lumbar spine and cervical spine. Instead of curving inward (lordosis) as those areas do, it curves outward (kyphosis). This provides the freedom of movement that allows a person to bend forward and touch their toes. It does not allow for much bending backward; that typically comes from the lower back.
Many nerves extend from the thoracic spine. They control organ function for the major organs, including:
T1 to T4
Heart
Esophagus
Upper body muscles
Lungs
Larynx
Part of the arms
Trachea
Esophagus
T5 to T10
Gallbladder
Diaphragm
Small intestine
Appendix
Liver
Kidneys
Suprarenal gland
Stomach
Spleen
Adrenal gland
Pancreas
T11 to T12
Small intestines
Mid to upper body muscles
Lymph circulation
Colon
Solar plexus
Uterus
Mid to Upper Back Pain
Pain in the thoracic area of the spine is often caused by muscle strain, overuse, and injury to the discs, ligaments, and muscles that surround the spine and support it. Poor posture can also cause pain in that area. It is also very common for myofascial pain to affect the connective tissue of` muscle groups and individual muscles. These problems can occur due to a variety of causes:
Slouching or slumping while standing or sitting
Getting in a car accident where the patient is lurched forward or jolted
Lifting something that is too heavy
Yard work
Getting struck or hit in the back
Playing sports
Osteoarthritis can also occur in this area. It is caused by torn cartilage brought about by the everyday wear and teas and even the simple process of aging. Fractured vertebrae can also cause back pain in the thoracic area, as can a herniated disc, and a spine that is oddly shaped or misshapen. Degenerative disc disease and spinal stenosis can also be culprits.
Chiropractic Care for the Thoracic Spine
The goal of the chiropractor treating a patient for thoracic back pain will usually focus on reducing the pain and inflammation in the area. The treatments may include:
Spinal adjustments
Specialized exercise recommendations
Ergonomic training
Distraction
Heat or ice
Traction
Electrical stimulation
The chiropractor may also recommend nutritional supplements like proteolytic enzymes to aid in managing the swelling and pain that may be caused by disc herniation and some other back injuries. They may also recommend dietary changes or weight loss to help the patient manage their pain.
Chiropractic is a safe, effective, non-invasive treatment for mid to upper back pain. Many patients experience results immediately which is another draw for people. Most patients with back problems will be advised to maintain regular chiropractic visits to manage the pain and keep it at bay effectively.
If you are one of the seven out of 10 Americans who have back pain, you are probably looking for relief. What you probably aren�t looking for are injections or pills with harmful side effects. Your doctor may have told you that exercise is a great way to relieve pain naturally, but you aren�t sure where to start or even what activity is best.
Running and walking are both good exercises, but they aren�t for everyone. Some back pain patients can run with no problem with others have significant trouble. So, which is better for back pain sufferers? The answer might surprise you.
Benefits of running
When it comes to health benefits, running and walking, don�t differ much. Both help to decrease your risk of developing heart disease, diabetes, and hypertension as well as lower your cholesterol.
Running also has the added benefit of increasing the bone that connects the femur head to the shaft, substantially strengthening the hips and helping to prevent hip fractures. Both running and walking burn calories, facilitate weight loss and can help to make you healthier. However, one activity is a lot harder on the back, so if you have chronic back pain, there are some things you should know.
How running affects the back
Running puts repetitive impact and stress on the back. If you have a problem with your lower back, running can exacerbate it or lead to additional issues like sciatica.
You can experience back muscle spasms, muscular strain, and other centralized lower back pain. If you have disc problems, the high impact nature of running can make put a lot of stress on your spine and make your disc problems worse.
How walking benefits back pain sufferers
Walking is a much lower impact activity than running. Although some back problems can be made worse by walking, that is relatively rare.
Most back pain is relieved with walking, and you can enjoy other great benefits as well. By adopting a regular walking routine, you will strengthen your hips, legs, ankles, and feet as well as your core.
This helps to provide better stability for your spine. It also helps to increase circulation in the spinal structures, draining toxins, and pumping nutrients into the surrounding soft tissues.
Pain often restricts mobility. Walking helps to improve range of motion and flexibility. You will find that your posture improves as well as your mood. A stronger body and increased flexibility help to prevent injury.
Walking at least three times a week for at least 15 minutes is great for overall wellness and a strong body. Combine it with a healthy diet and stress relief techniques, and you will look, feel, and move better � and your pain will be easier to manage.
Make walking work
When you start your walking program, don�t push too hard too fast. Go at your own pace and start slow. If you have a higher fitness level, you may want to try speed walking. After a five-minute warm-up, walk as fast as you can for about 8 minutes then slow to a moderate pace for two minutes to cool down.
You can also engage your core muscles by using several techniques. Walk on an incline or using walking poles are excellent for strengthening the core. Pulling your abdominals in toward your spine while you walk is also a great move.
Running is beneficial for your health, but it isn�t for everyone. Walking is a far better choice for most patients with lower back pain. You may even find that your pain is alleviated altogether so get out there and get moving.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine